Facial Plastics and Rhinoplasty Assessment · FACIAL PLASTICS AND RHINOPLASTY ASSESSMENT ....
116
Bhaskar Ram Aberdeen Royal Infirmary Dundee FRCSENT VIVA course www.frcsentvivacourse.co.uk FACIAL PLASTICS AND RHINOPLASTY ASSESSMENT
Transcript of Facial Plastics and Rhinoplasty Assessment · FACIAL PLASTICS AND RHINOPLASTY ASSESSMENT ....
Bhaskar Ram
Aberdeen Royal Infirmary
Dundee FRCSENT VIVA course
www.frcsentvivacourse.co.uk
FACIAL PLASTICS AND RHINOPLASTY ASSESSMENT

Aesthetic Principles • Ensure Complete Excision
• Consider Moh’s surgery • Replace tissue with like tissue ▫ Replace all missing components • Restore units and aesthetics • Evaluate tissue surrounding donor and recipient sites
Nasal Reconstruction • What does the patient want?
Expectations REMEMBER KIS • Patient Factors Health of patient, health of skin, smoker • Diagnose the nasal defect Subunits, tissue layer, internal structures • Evaluate donor materials for missing surface and tissue layers
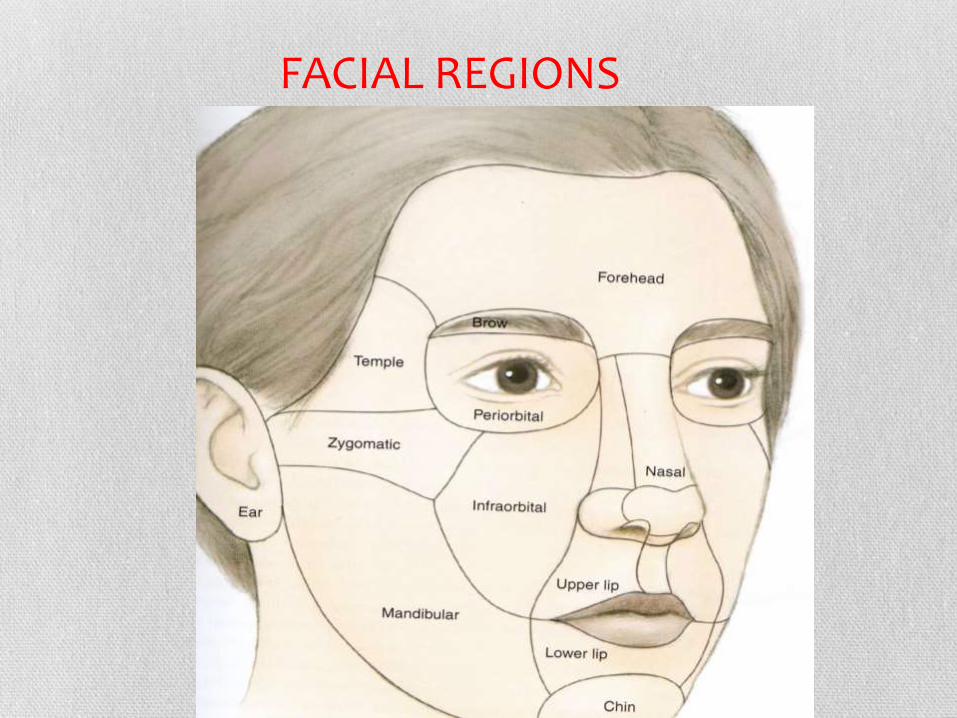
FACIAL REGIONS
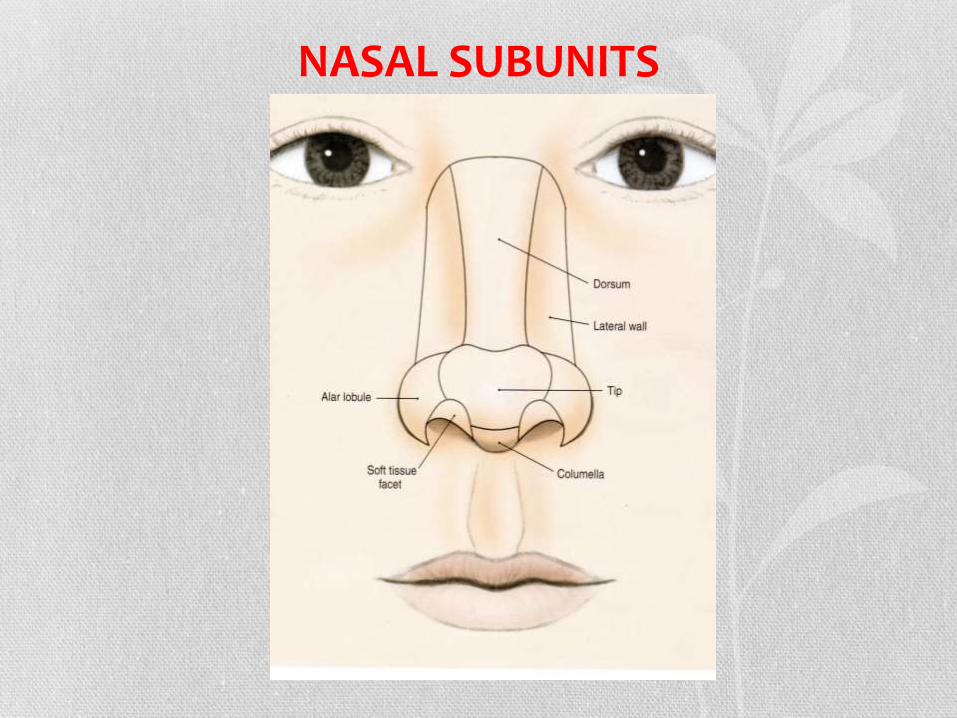
NASAL SUBUNITS
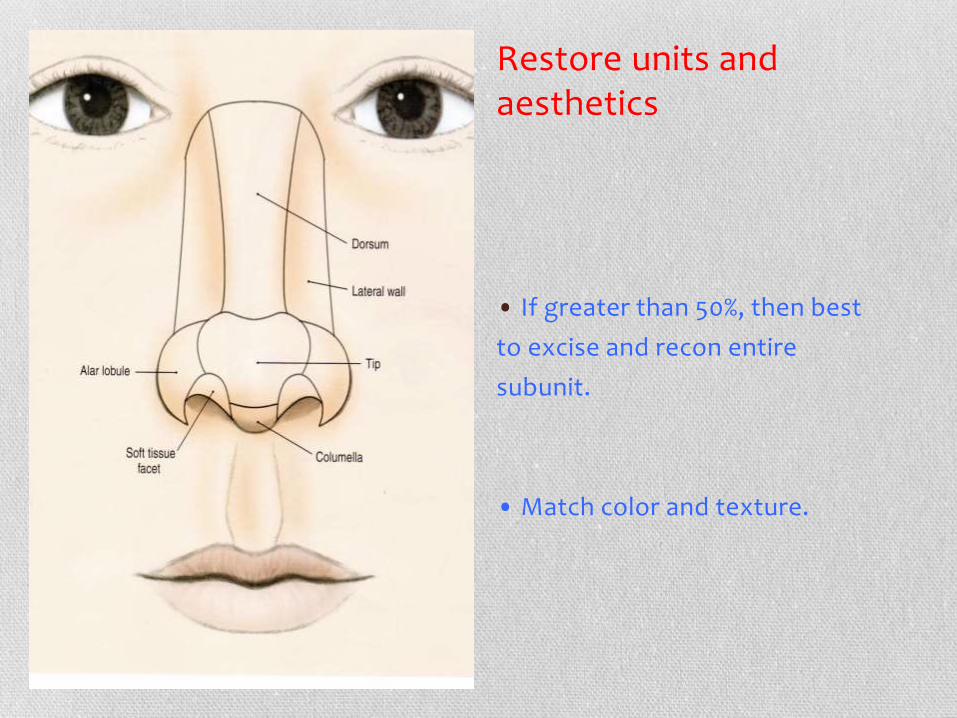
Restore units and aesthetics
• If greater than 50%, then best
to excise and recon entire
subunit.
• Match color and texture.
Replace tissue with like tissue • Cutaneous cover
Full thickness skin graft
Local or regional flaps
Structural support
Septal cartilage
Auricular or rib cartilage
Calvarial bone
• Lining flaps
▫ Septal mucoperichondrial flaps
Vestibular or turbinate mucosal flaps
HOW TO RECONSTRUCT
• START from the THE BASE
• BUILD the SUPPORT next
• COMPLETE with COVERING the defect with the skin

NASAL LINING FLAPS
• Bipedicled vestibular flap (Aka bucket handle flap)
(must be defect <1.5cm in
vertical height)
▫ Make intercartilagenous incision between upper and lower lats
Elevate the flap, sufficiently to mobilize
• Auricular cartilage can serve as framework to attach to.
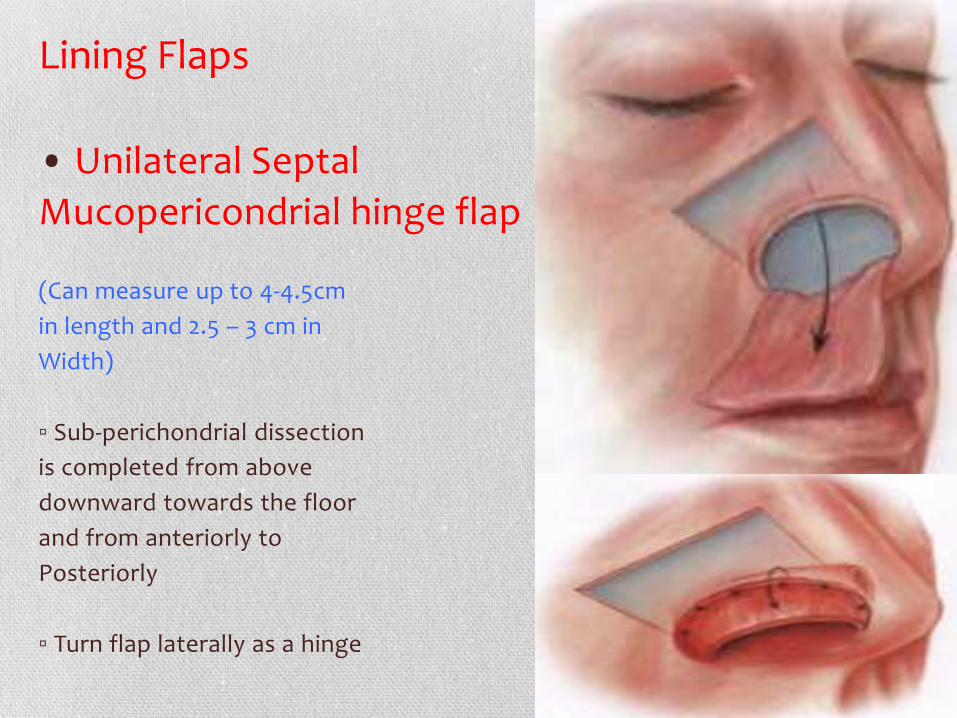
Lining Flaps
• Unilateral Septal
Mucopericondrial hinge flap
(Can measure up to 4-4.5cm
in length and 2.5 – 3 cm in
Width)
▫ Sub-perichondrial dissection
is completed from above
downward towards the floor
and from anteriorly to
Posteriorly
▫ Turn flap laterally as a hinge

Framework
Framework
• Cephalic Dorsum – cranial bone.
▫ These are secured to frontal bone with miniplates.
• Caudal Dorsum – septal or auricular cartilage.
• Lateral Sidewall – may be replaced with bone or
cartilage.
• Alar defects – cartilage (usually contralateral
concha cymba).
Nasal Reconstruction – CUTANEOUS DEFECTS-Ladder • Primary closure
• Healing by secondary intention
• Dermabrasion
• Full thickness skin grafts (FTSG)
• Composite grafts
• Random Flaps
• Pedicled Flaps

Secondary Intention
Typically for medial canthal defects
• Results in contraction
and distortion of nose
• Poor aesthetic
outcomes on most
defects of nose
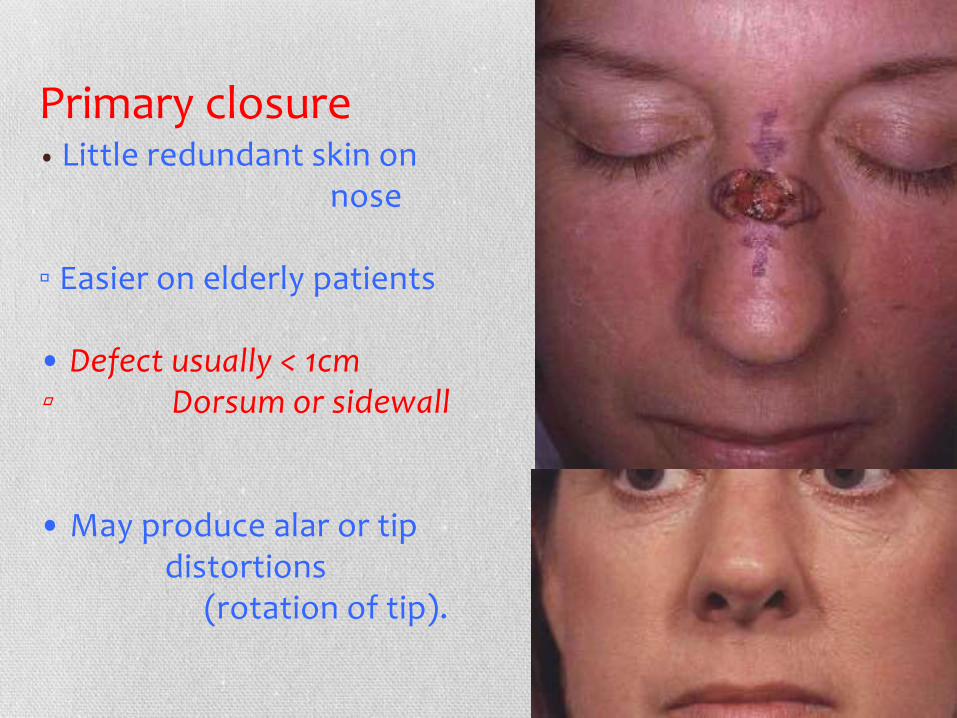
Primary closure • Little redundant skin on nose ▫ Easier on elderly patients • Defect usually < 1cm ▫ Dorsum or sidewall • May produce alar or tip distortions (rotation of tip).
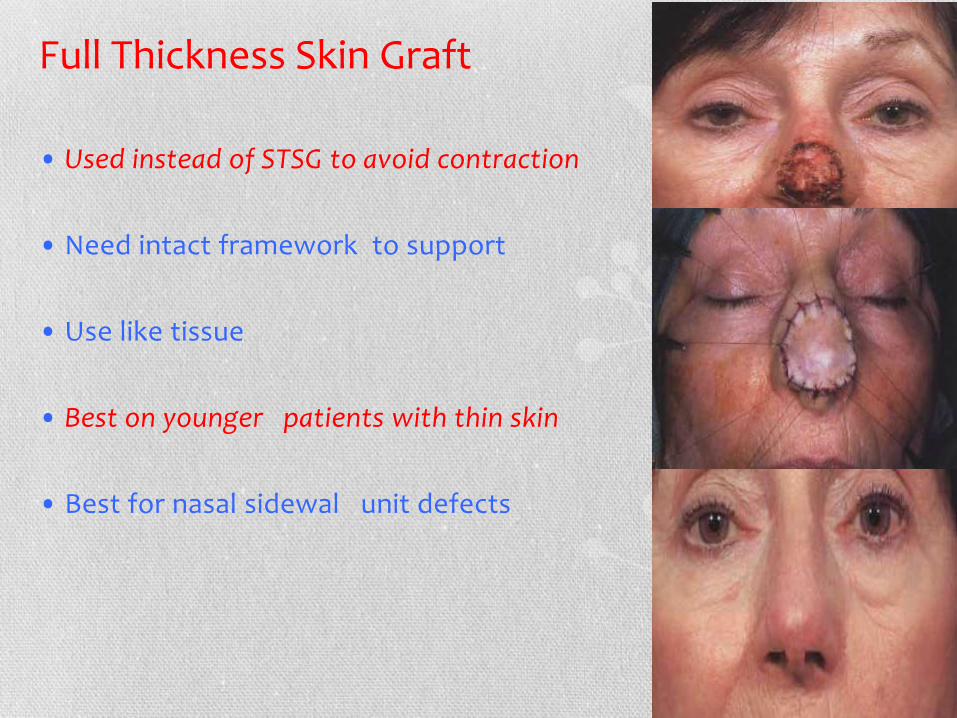
Full Thickness Skin Graft • Used instead of STSG to avoid contraction
• Need intact framework to support
• Use like tissue
• Best on younger patients with thin skin
• Best for nasal sidewal unit defects
Local Flaps
LOCAL FLAPS Types of Flaps: Defined by direction of
tissue movement
• Advancement flaps: Linear movement
▫ Y-V advancement
• Rotational Flaps: Radial movement
• Transposition Flaps: Raised from donor sites
and rotated over to defect
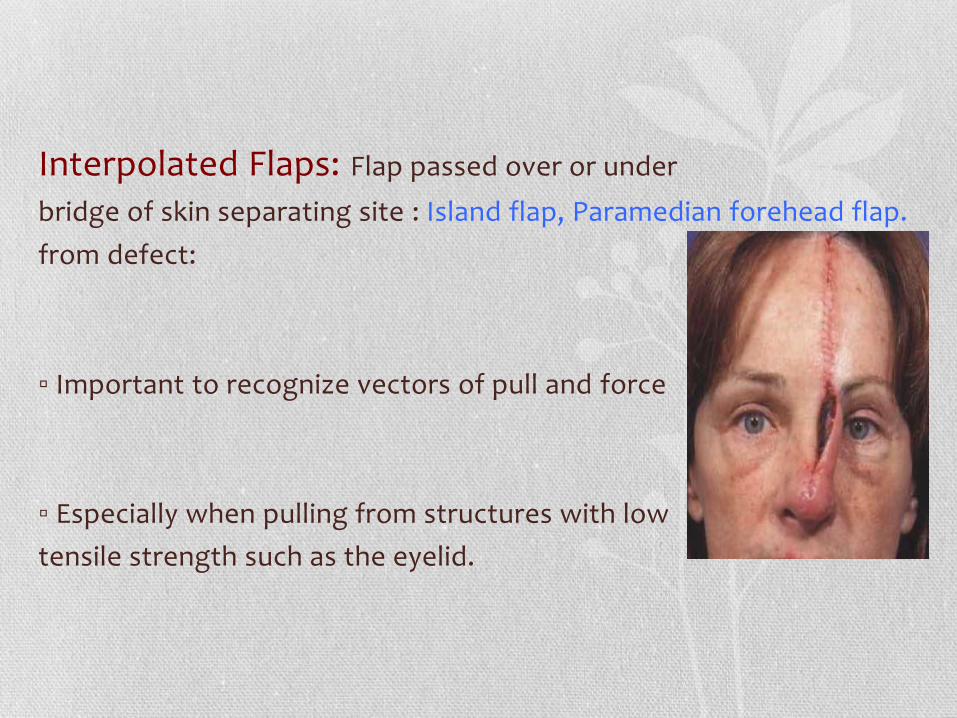
Interpolated Flaps: Flap passed over or under
bridge of skin separating site : Island flap, Paramedian forehead flap.
from defect:
▫ Important to recognize vectors of pull and force
▫ Especially when pulling from structures with low
tensile strength such as the eyelid.


What flap to use and Where
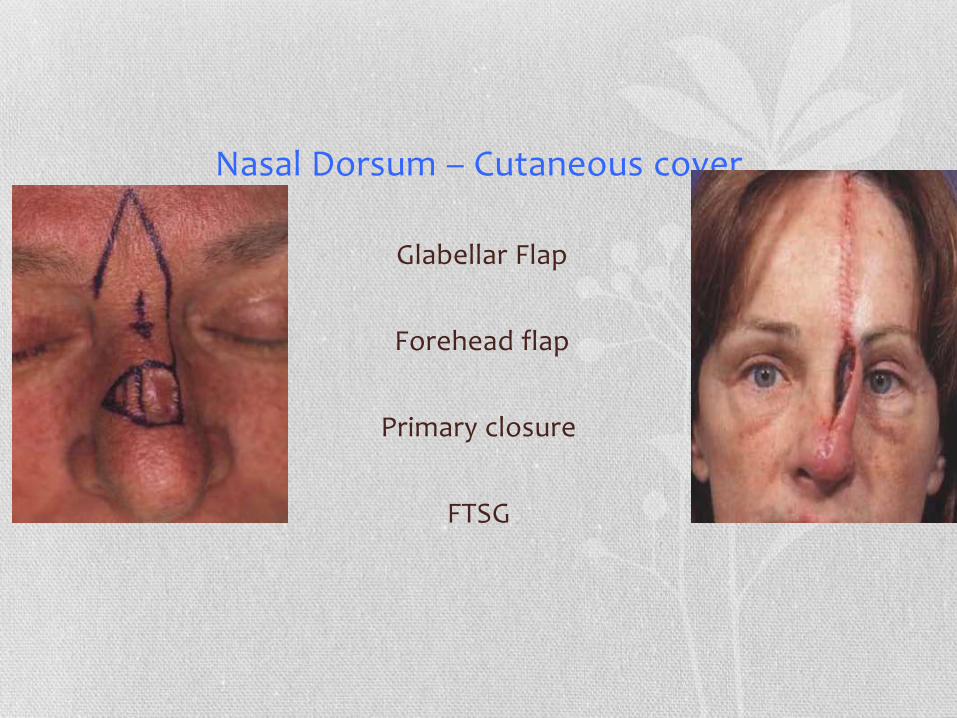
Nasal Dorsum – Cutaneous cover
Glabellar Flap
Forehead flap
Primary closure
FTSG

Nasal Sidewall- Cutaneous Cover
FTSG
Transposition Flap
Bilobed Flap
Forehead Flap
Nasal Tip Lobule – Cutaneous cover
• Bilobe flap • Forehead flap • FTSG
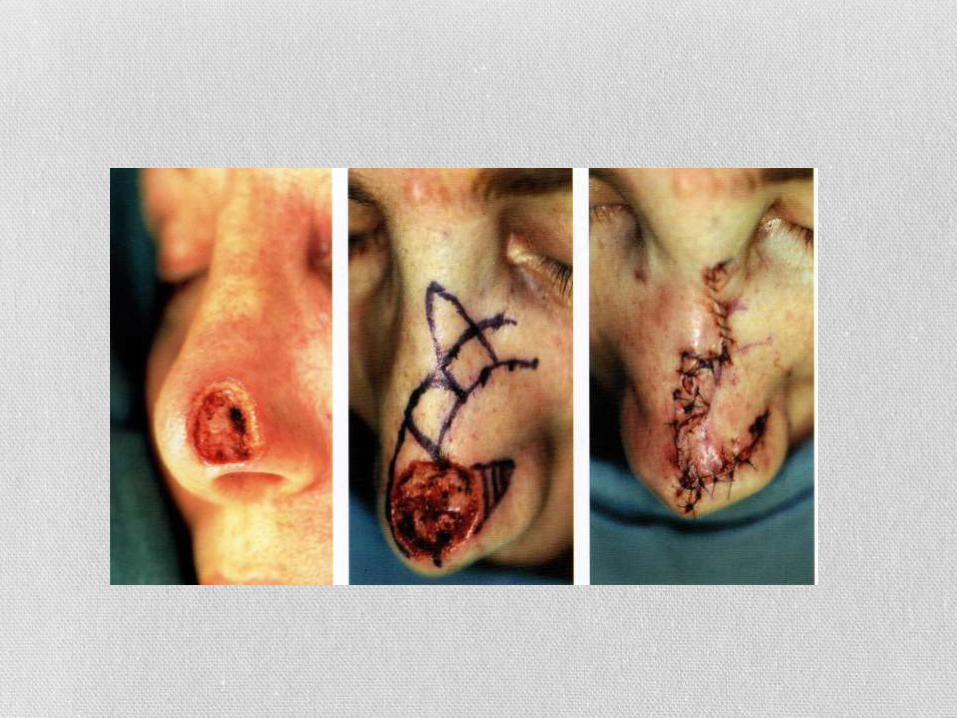
Tip Lobule – Bilobe Flap
• Original design by Esser (1918)
Total transposition of ‹100°
• Ideal for defects:
1.5 - 2.0cm
▫ Best of ›5mm from margin of
nostril

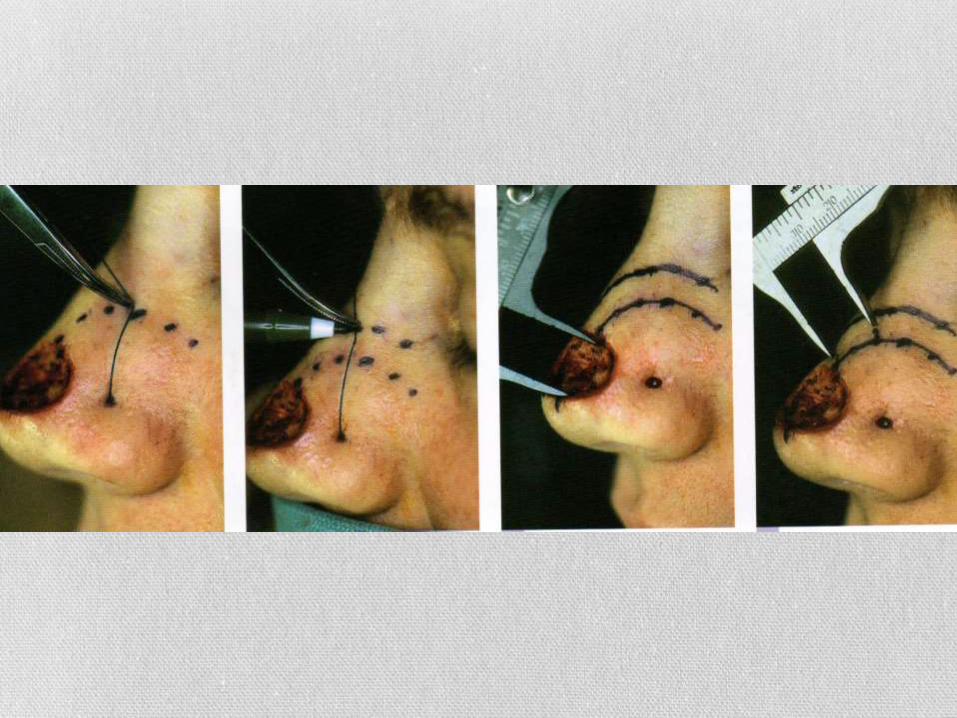
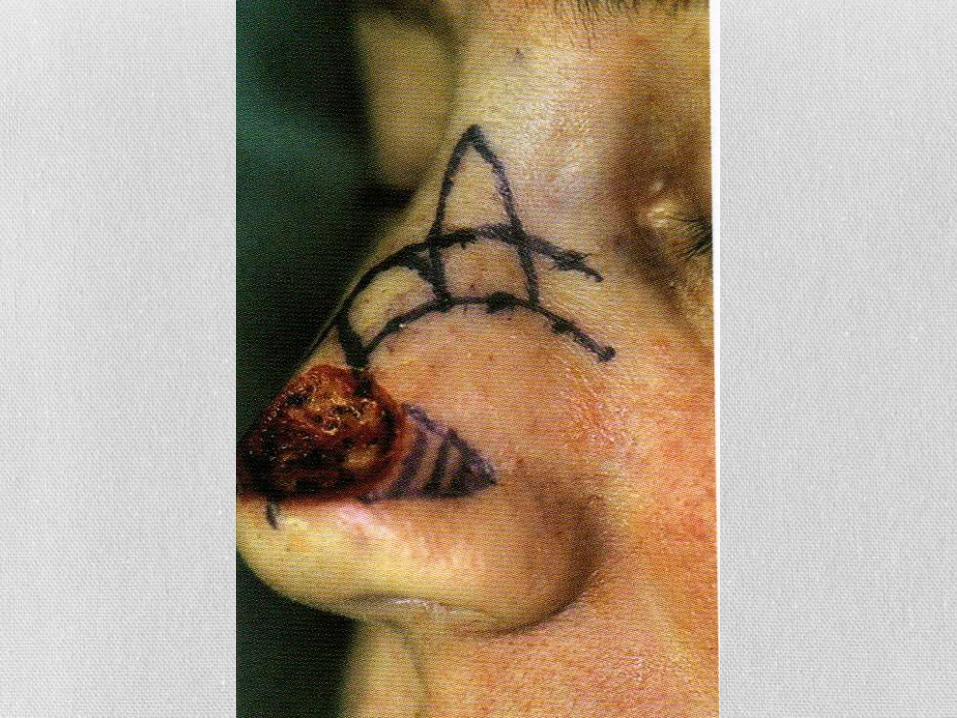

Preferably laterally based
Most common nasal local flap Double transposition flap Little distortion of alar rim
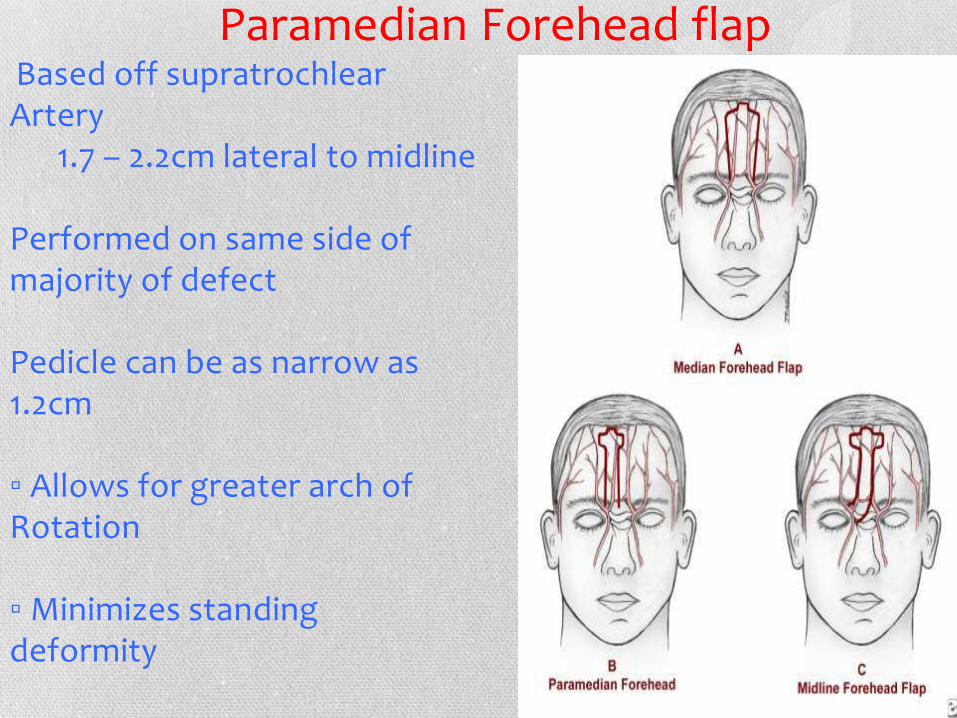
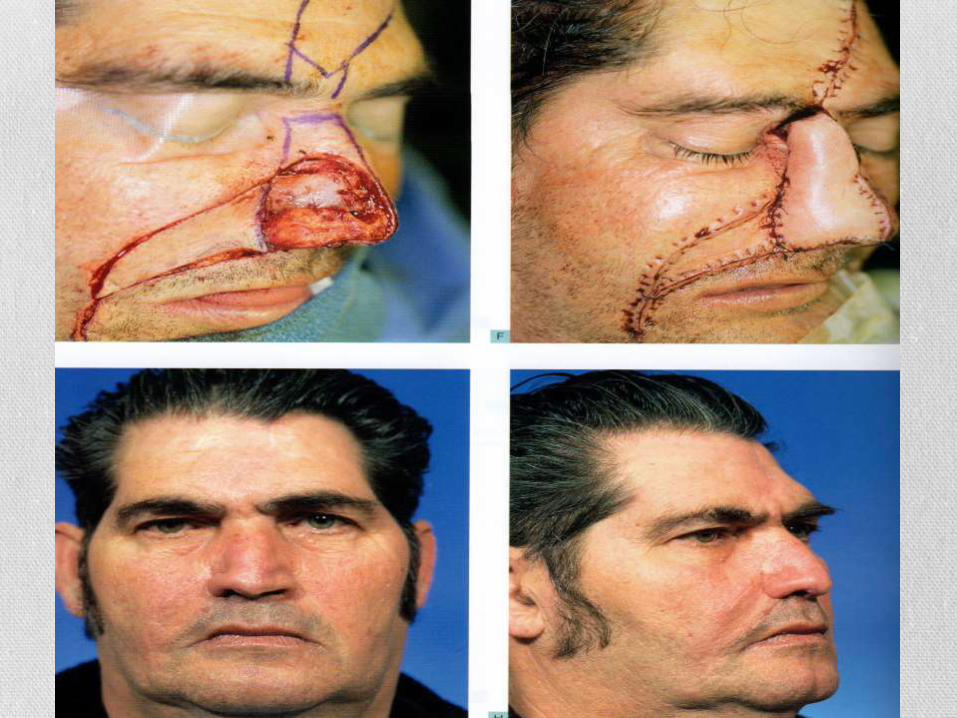
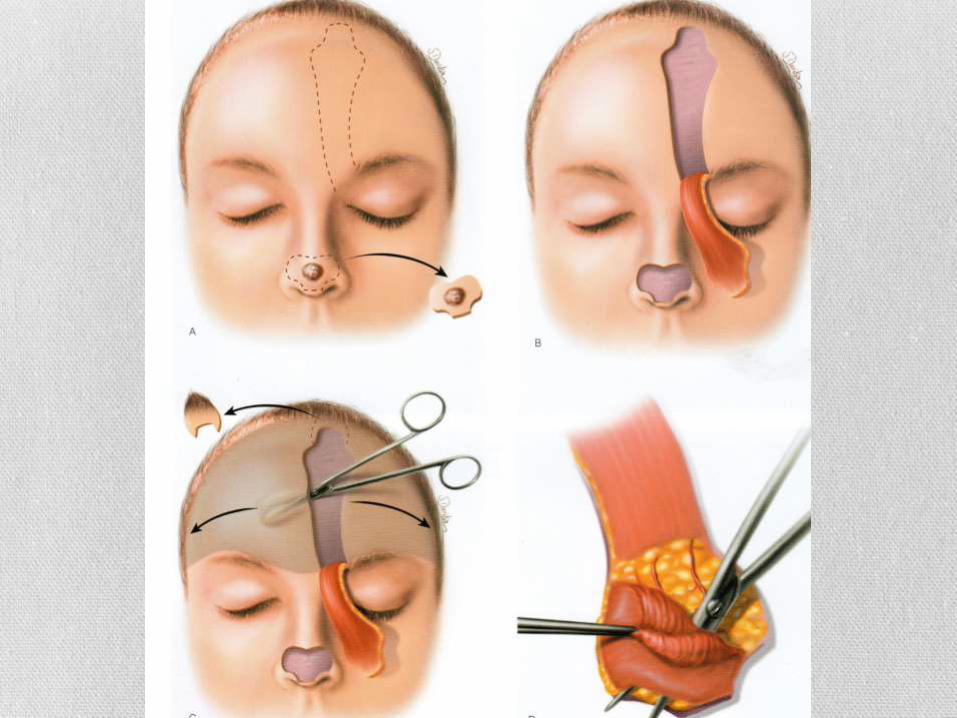
Paramedian Forehead flap Based off supratrochlear Artery 1.7 – 2.2cm lateral to midline Performed on same side of majority of defect Pedicle can be as narrow as 1.2cm ▫ Allows for greater arch of Rotation ▫ Minimizes standing deformity
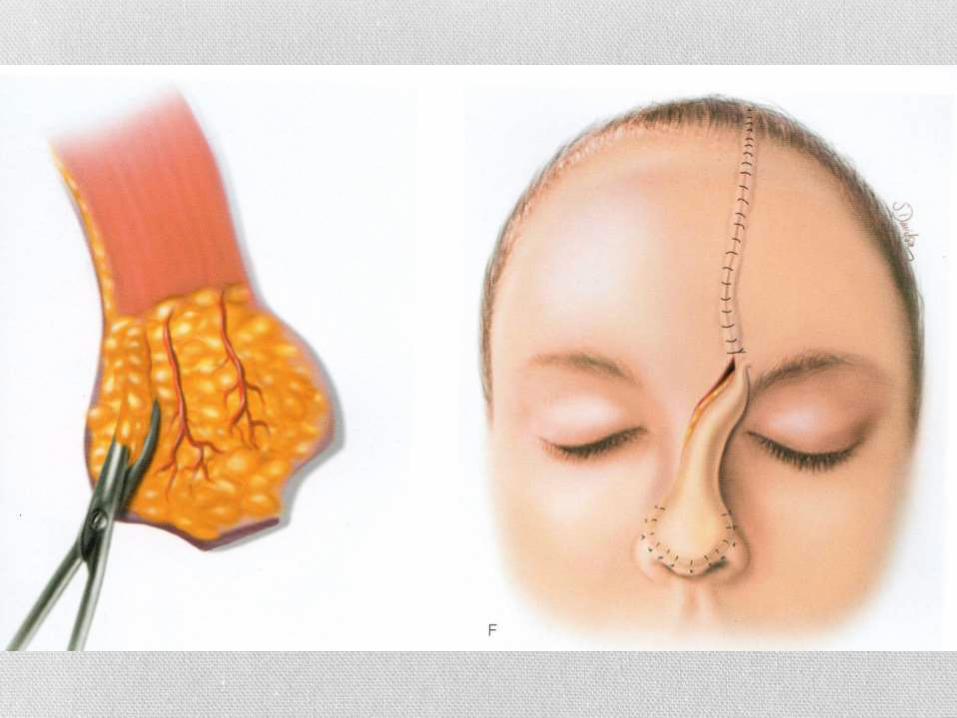


Columella – Cutaneous cover FTSG (superficial)
Composite graft (<1.5cm)
Melolabial flap
Forehead flap
Alar rim – Cutaneous cover
• Melolabial flap
• Forehead flap
• Composite graft
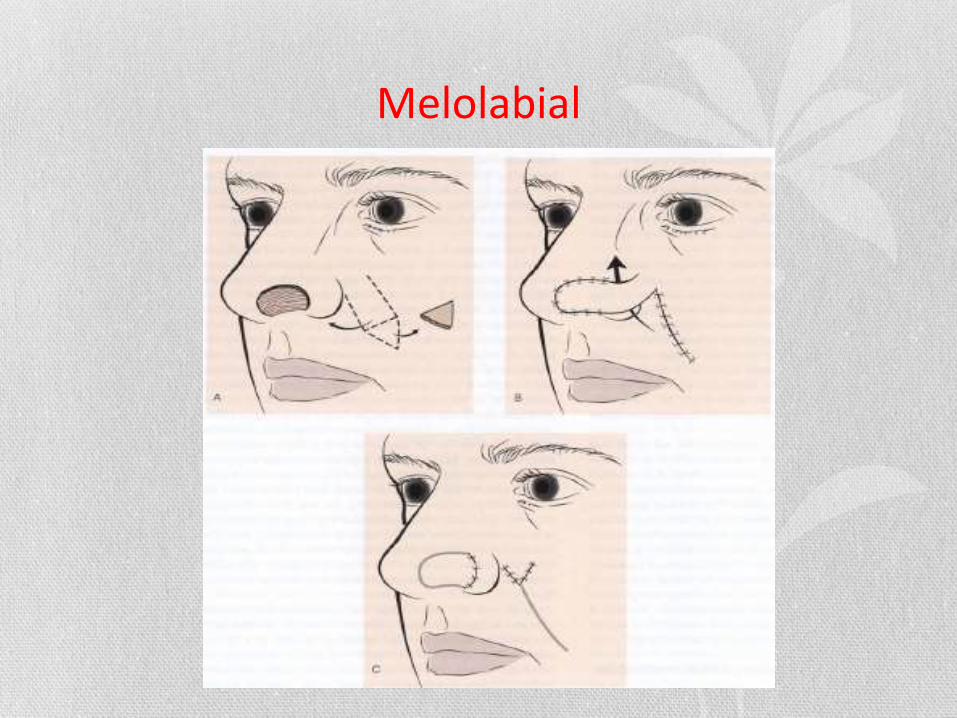
Melolabial
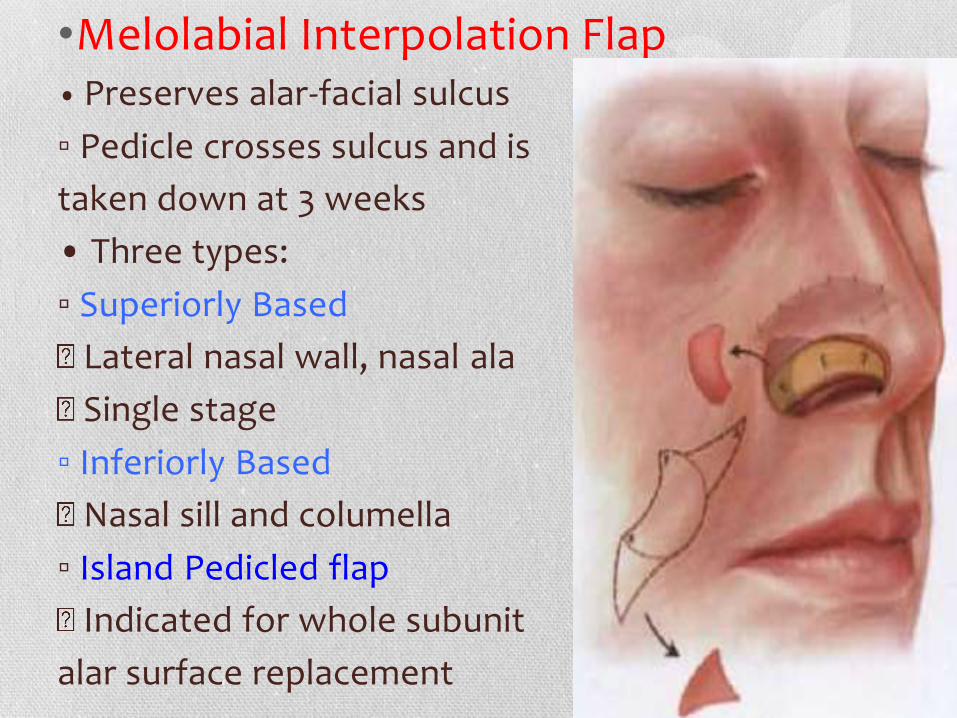
•Melolabial Interpolation Flap • Preserves alar-facial sulcus
▫ Pedicle crosses sulcus and is
taken down at 3 weeks
• Three types:
▫ Superiorly Based
Lateral nasal wall, nasal ala
Single stage
▫ Inferiorly Based
Nasal sill and columella
▫ Island Pedicled flap
Indicated for whole subunit
alar surface replacement
TEMPLE AND FOREHEAD DEFECTS

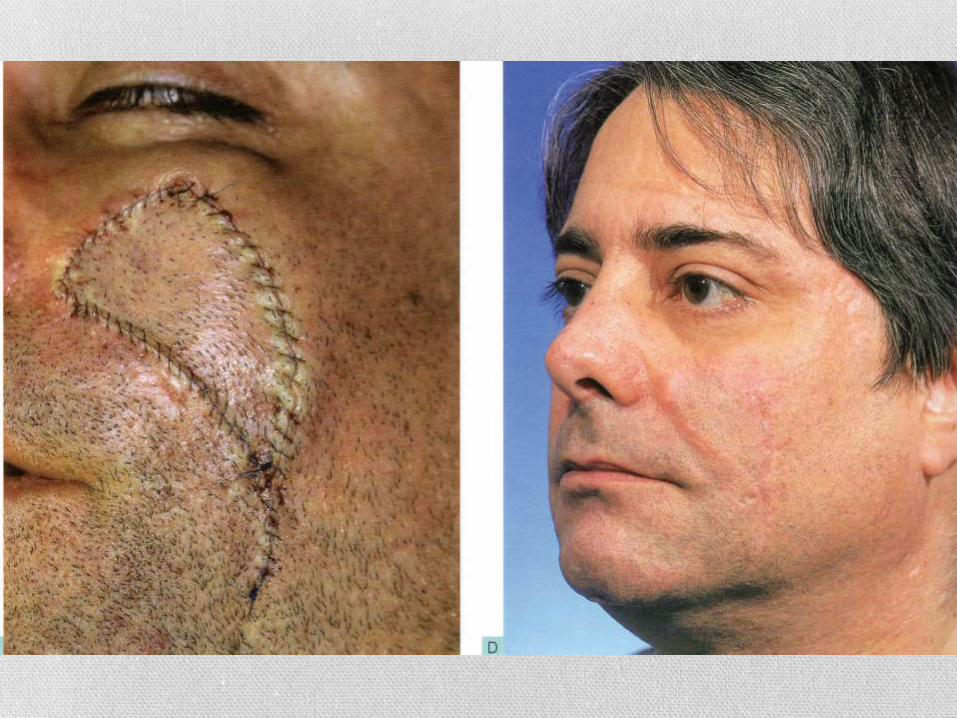
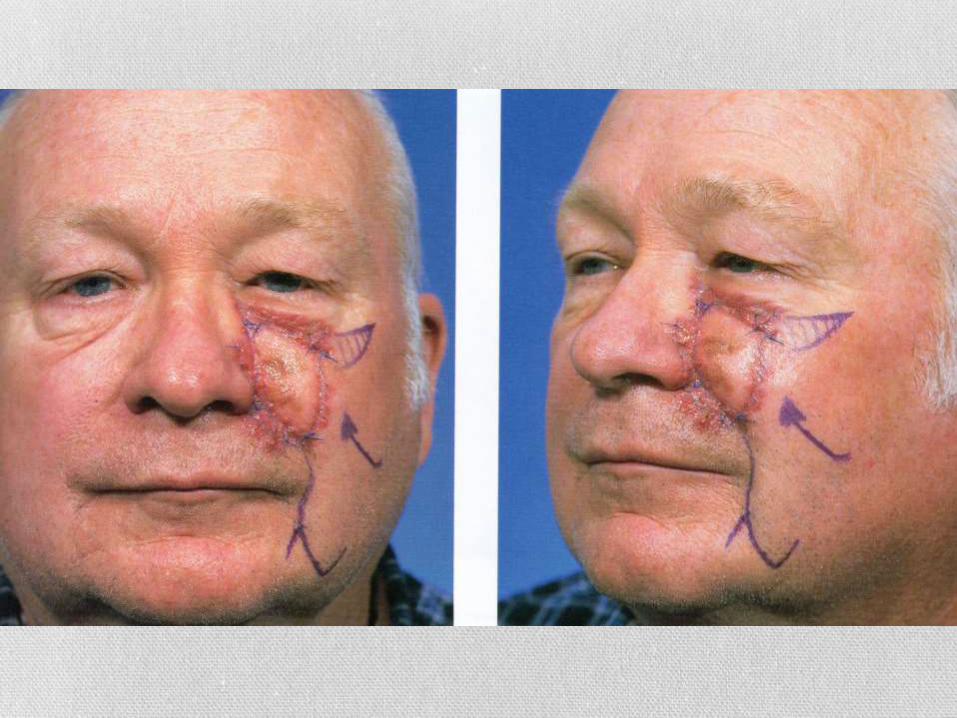
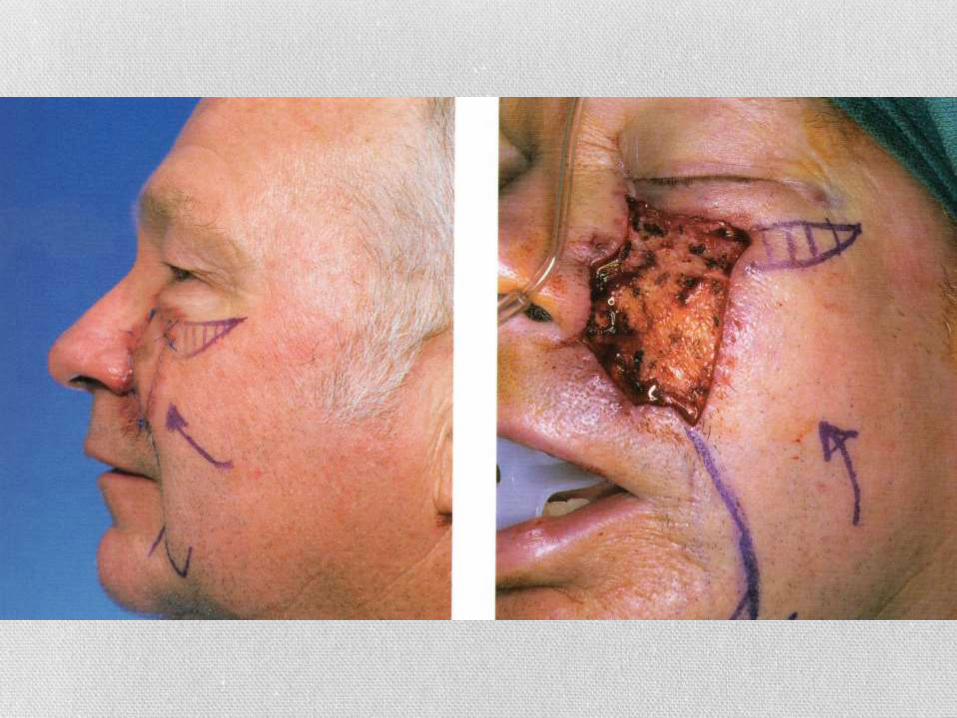
CHEEK DEFECTS



Take home points Mohs Surgery – Principles
Reconstruction of Mohs Defects
Cosmetic Principles
Healing by Secondary Intent
Skin Graft
Primary closure
Flap Reconstruction
Reconstruction of specific locations
FACIAL ANALYSIS OF THE RHINOPLASTY PATIENT
Bhaskar Ram
Consultant Otolaryngologist
The standard attractive face
Symmetry
Proportions
Angles
Relationships
Correction of what is askew determines the surgical plan
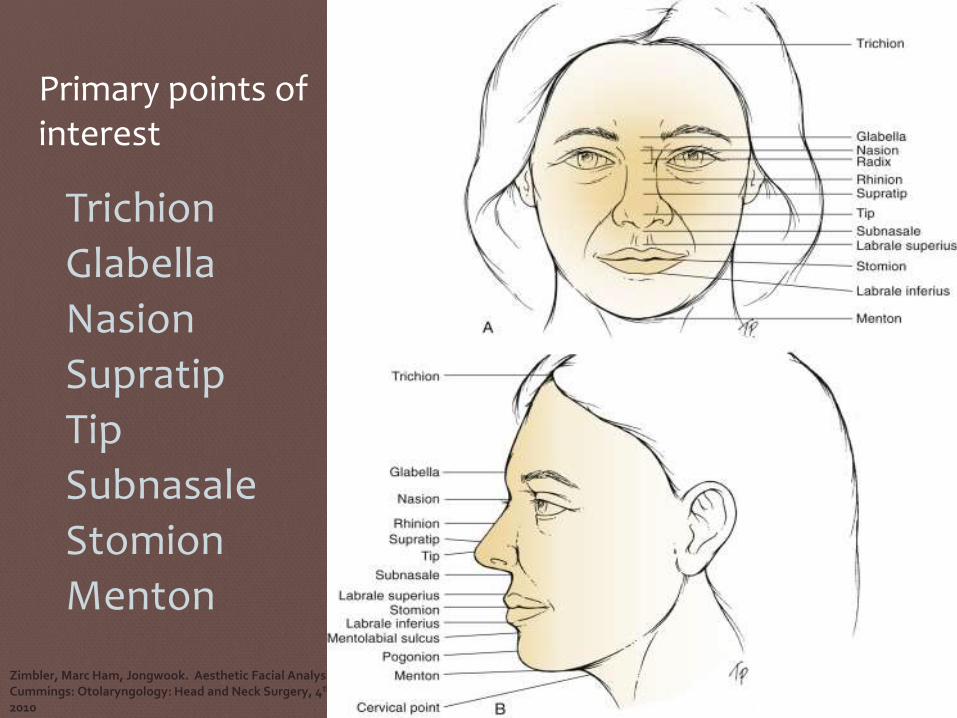
Primary points of interest
Trichion
Glabella
Nasion
Supratip
Tip
Subnasale
Stomion
Menton
Zimbler, Marc Ham, Jongwook. Aesthetic Facial Analysis, Cummings: Otolaryngology: Head and Neck Surgery, 4th ed 2010
•Trichion: Anterior hairline in the midline
•Glabella: Most prominent midline point of forehead, well appreciated on lateral view
•Nasion: Most posterior midline point of forehead, typically corresponds to nasofrontal suture
•Rhinion: Soft-tissue correlate of osseocartilaginous junction of nasal dorsum
• Supratip: Point cephalic to the tipTip: Ideally,
• Subnasale: Junction of columella and upper lip
•Menton: Most inferior point on chin
•Pogonion: Most anterior midline soft-tissue
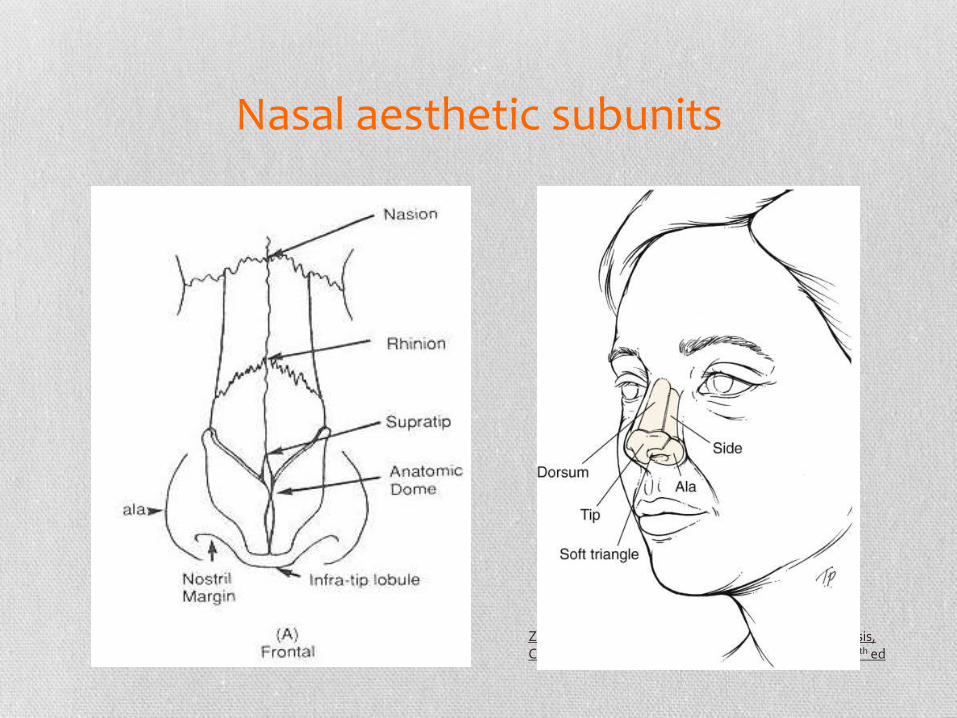
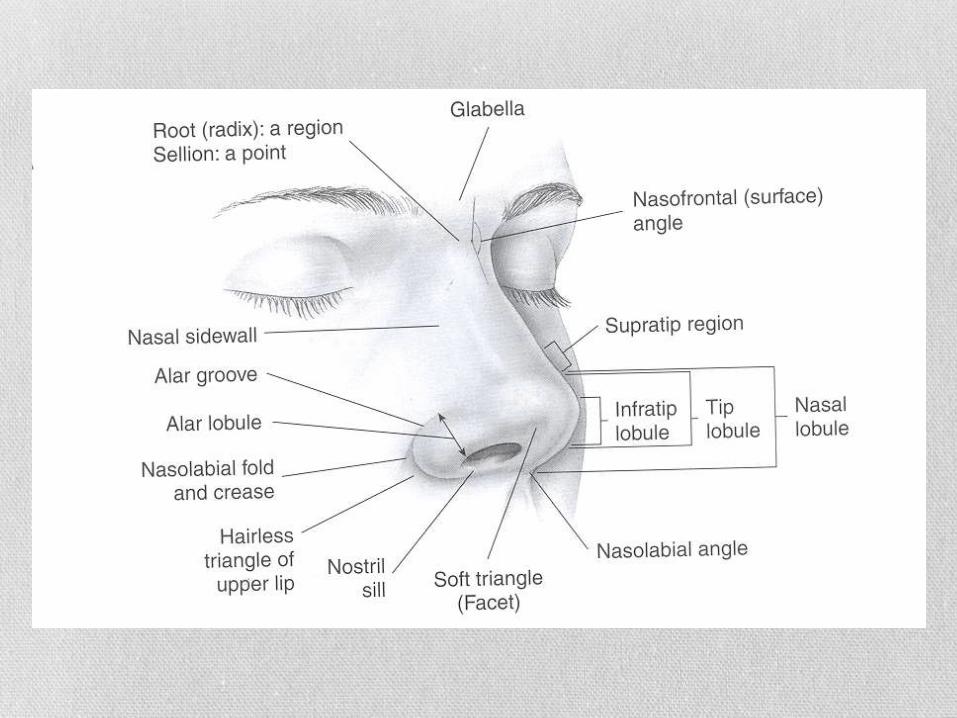
Nasal aesthetic subunits
Zimbler, Marc Ham, Jongwook. Aesthetic Facial Analysis, Cummings: Otolaryngology: Head and Neck Surgery, 4th ed
Tip Support
•Major
•LLC size and shape
•LLC attachment to ULC
•LLC attachment to caudal spine
•Minor
•Interdomal ligament
•Soft tissue envelope
•Cartilagenous dorsum membranous septum
•Nasal spine
Rhinoplasty consultation
• First Consultation
• Understand patients wants
• Are they genuine, realistic
• Understand what you can realistically achieve
•
• Will the pt be happy with the outcome
•
BEWARE • Intranasal substance abuse (eg, cocaine)
• Psychological or psychiatric instability
• SIMON (single, immature, male, overly expectant, narcissistic) personality traits
• Patient refusal of external scar
• Very thick nasal skin
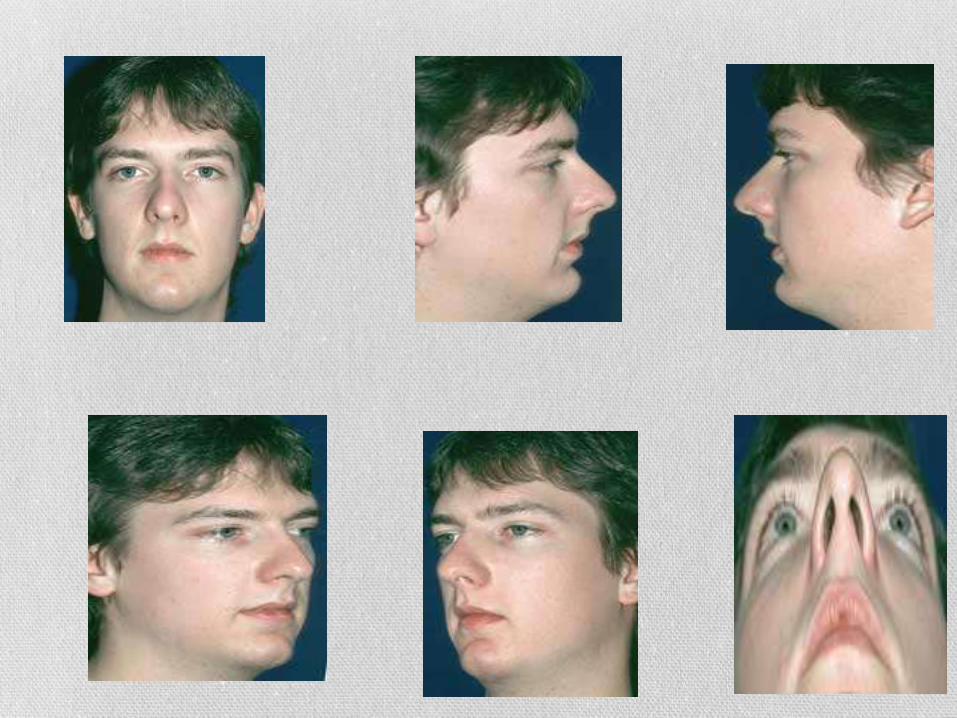
STANDARD FACIAL PHOTOGRAPHS

Facial Analysis
Horizontal 1/3s
Trichion glabella
Glabella subnasale
Subnasalementon
Lower 1/3 may be subdivided
Upper lip 1/3
Lower lip + chin 2/3
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.
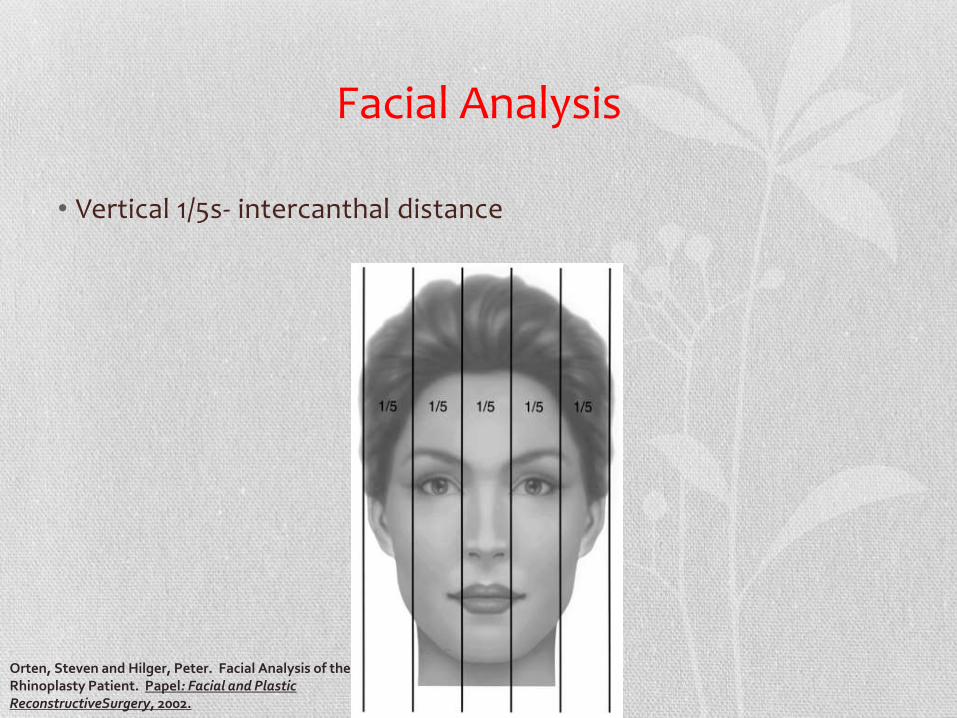
Facial Analysis
• Vertical 1/5s- intercanthal distance
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.

Frontal View •Twisted
•Dorsal width
•Alar base
•Tip defining
points
•Asymmetry of
domes
Rhinoplasty DominicMCastellanoM.D. Castellano&HowardSpecialtyCenter Tampa,Fl , Osler Review Course
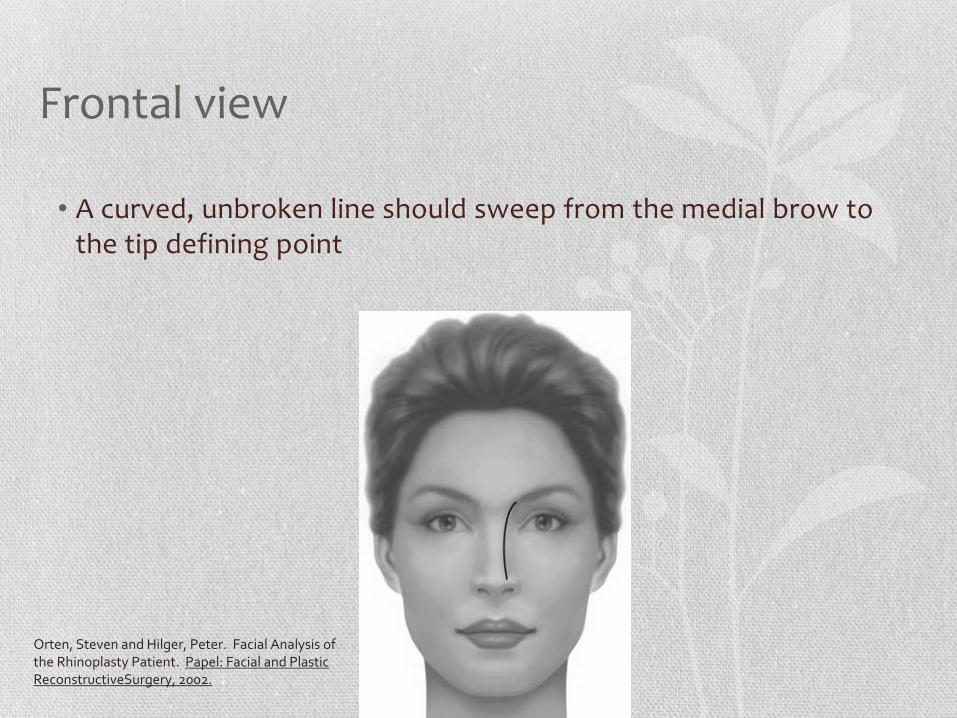
Frontal view
• A curved, unbroken line should sweep from the medial brow to the tip defining point
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.
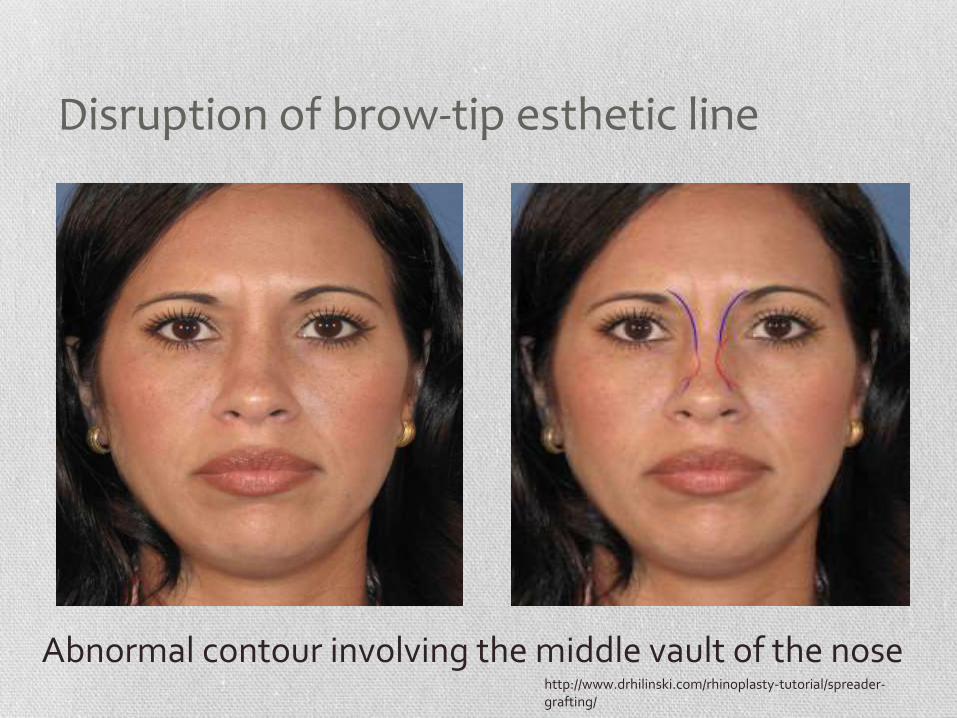
Disruption of brow-tip esthetic line
http://www.drhilinski.com/rhinoplasty-tutorial/spreader-grafting/
Abnormal contour involving the middle vault of the nose
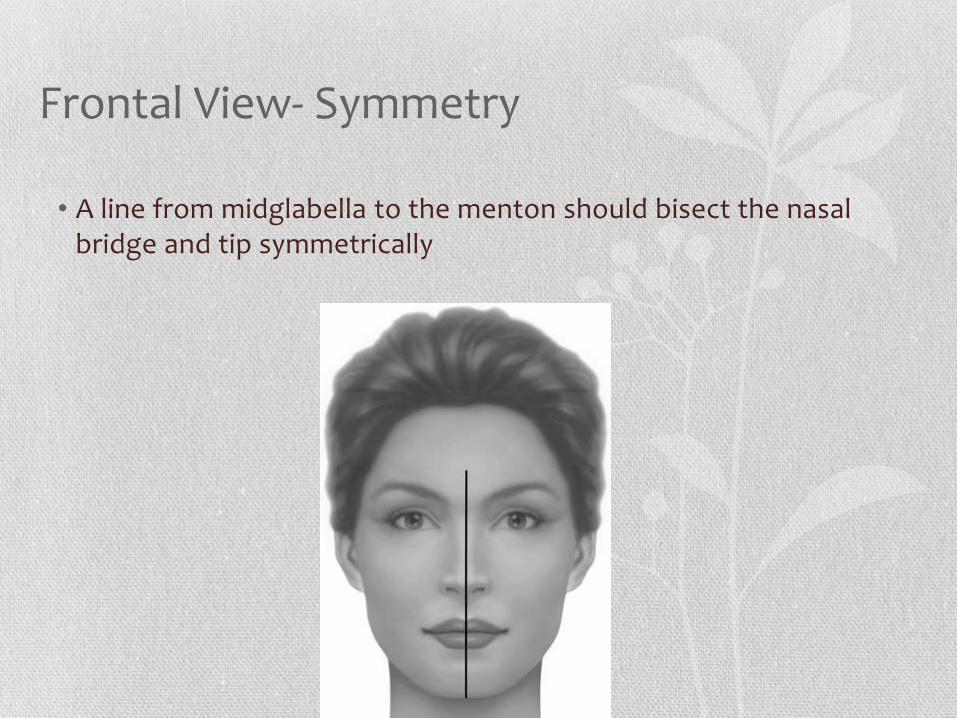
Frontal View- Symmetry
• A line from midglabella to the menton should bisect the nasal bridge and tip symmetrically
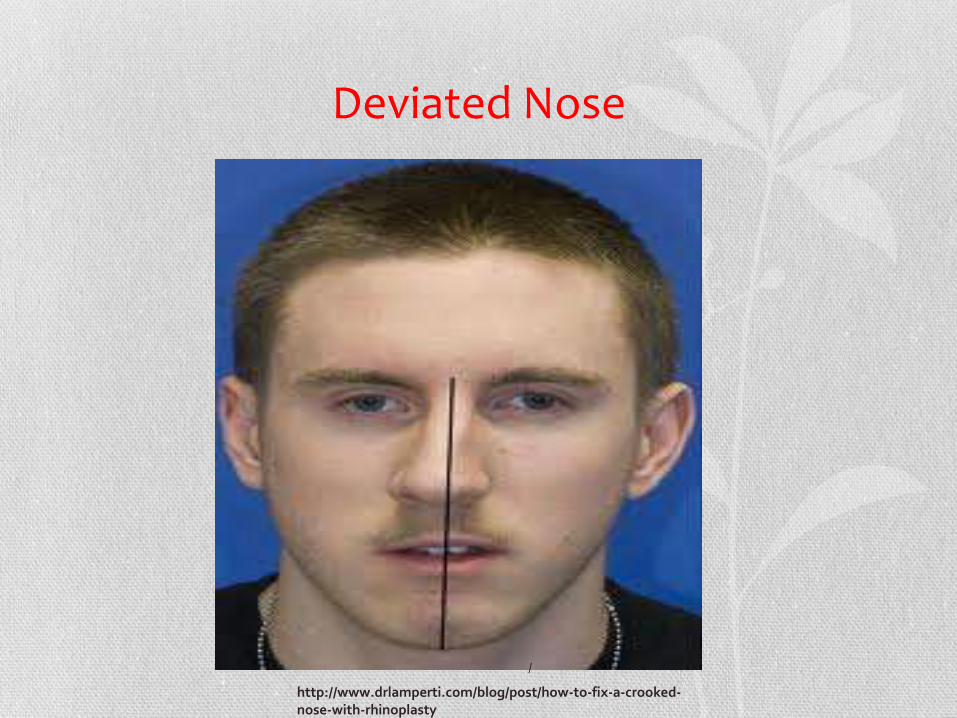
Deviated Nose
/
http://www.drlamperti.com/blog/post/how-to-fix-a-crooked-nose-with-rhinoplasty
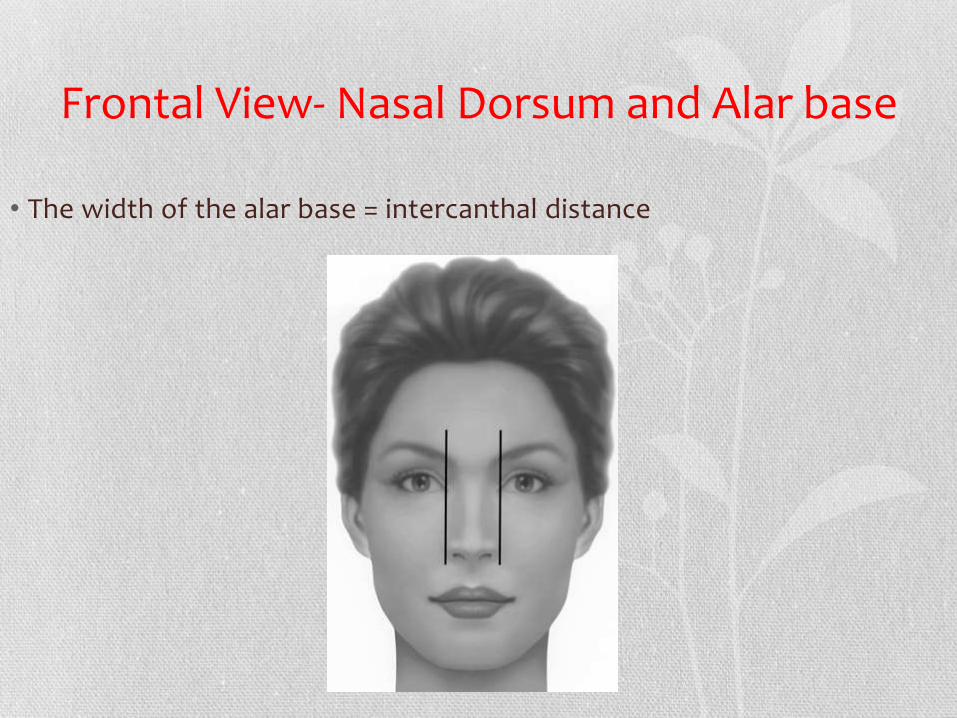
Frontal View- Nasal Dorsum and Alar base
• The width of the alar base = intercanthal distance

Alar base Reduction
http://www.plasticsurgerypractice.com/issues/articles/2011-01_02.asp
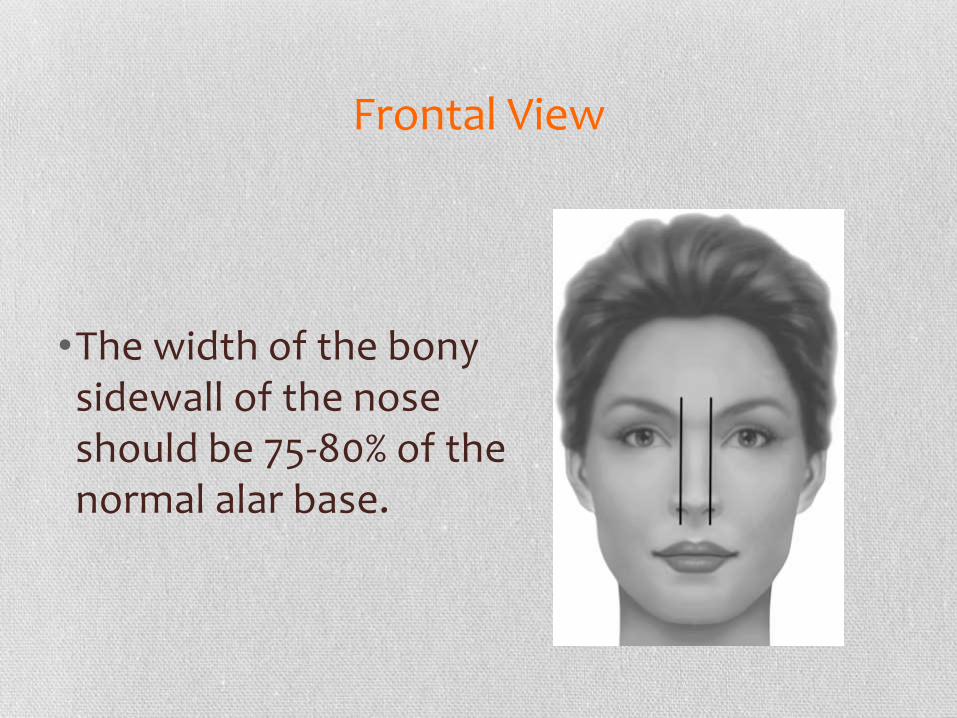
Frontal View
•The width of the bony sidewall of the nose should be 75-80% of the normal alar base.
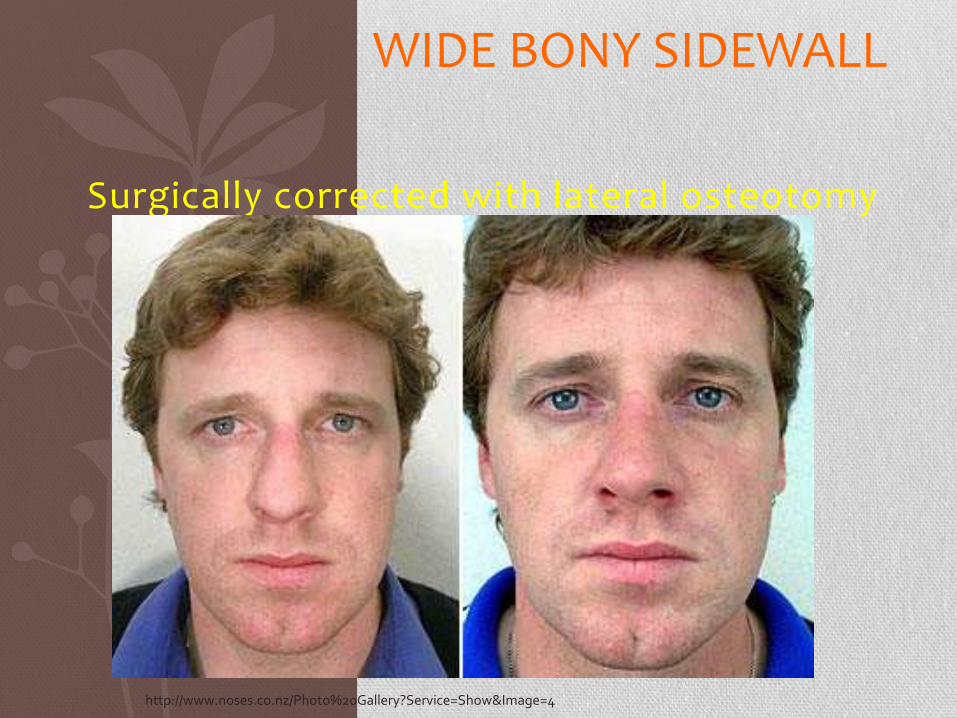
WIDE BONY SIDEWALL
Surgically corrected with lateral osteotomy
http://www.noses.co.nz/Photo%20Gallery?Service=Show&Image=4
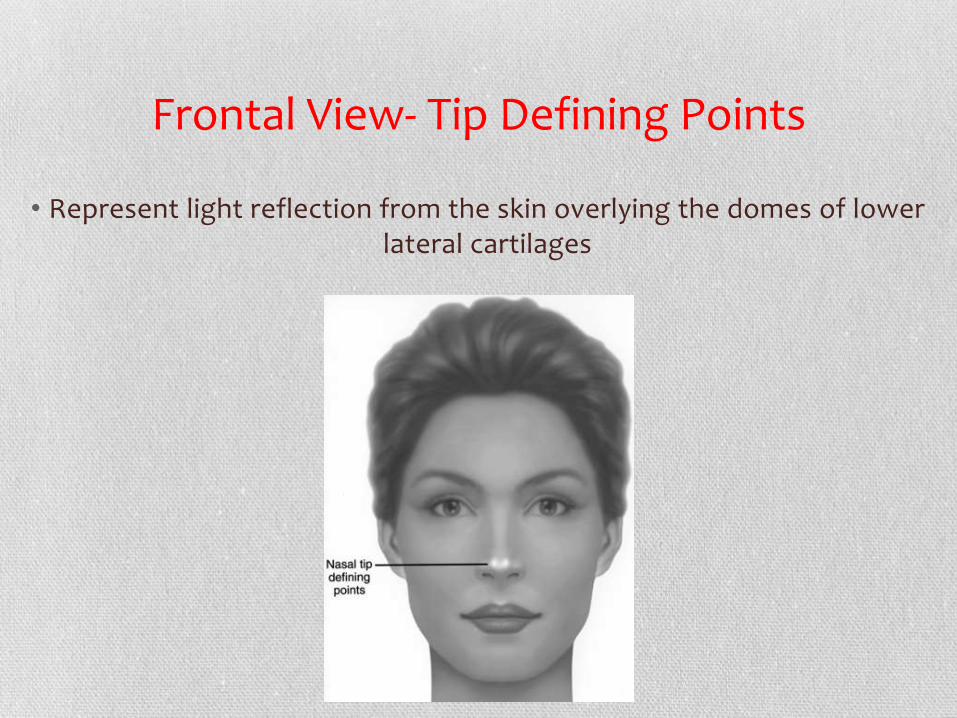
Frontal View- Tip Defining Points
• Represent light reflection from the skin overlying the domes of lower lateral cartilages
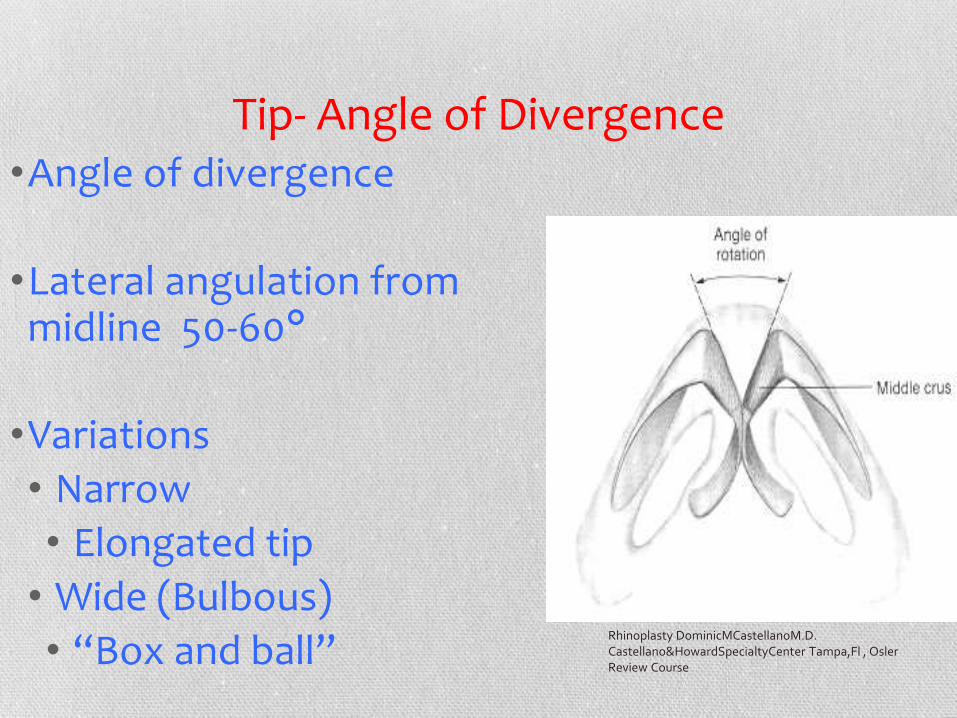
Tip- Angle of Divergence •Angle of divergence
•Lateral angulation from midline 50-60°
•Variations
• Narrow
• Elongated tip
• Wide (Bulbous)
• “Box and ball” Rhinoplasty DominicMCastellanoM.D. Castellano&HowardSpecialtyCenter Tampa,Fl , Osler Review Course
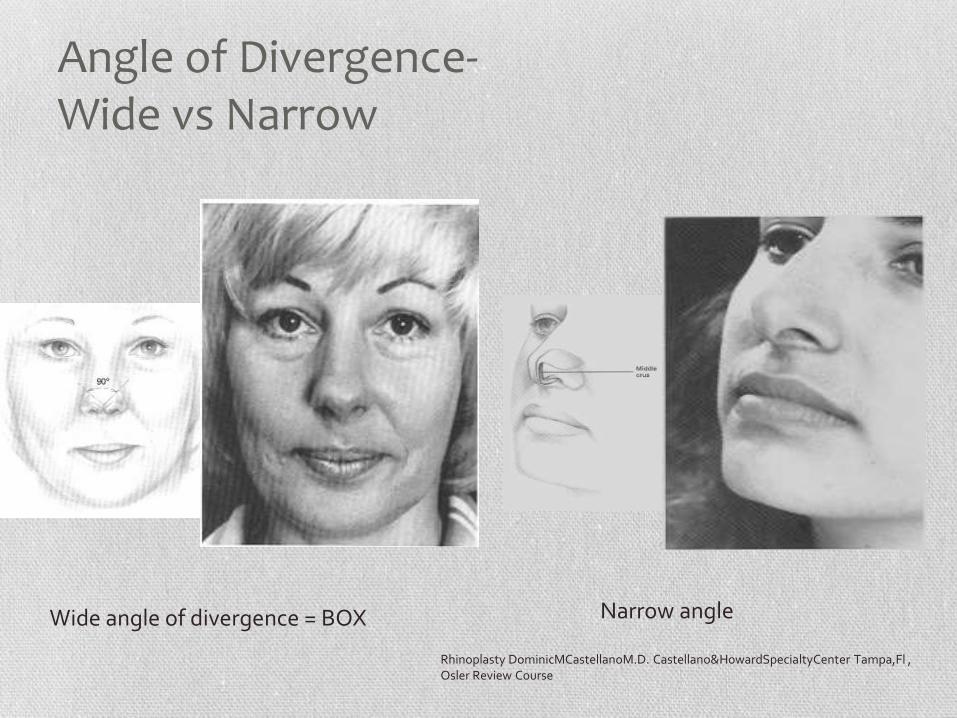
Angle of Divergence- Wide vs Narrow
Wide angle of divergence = BOX Narrow angle
Rhinoplasty DominicMCastellanoM.D. Castellano&HowardSpecialtyCenter Tampa,Fl , Osler Review Course

Frontal View- Columella Columella should hang
just inferior to alar rims
Infratip lobule should be a gentle “gull in flight”
Too much-reduction
Retracted-augmentation Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic
ReconstructiveSurgery, 2002.
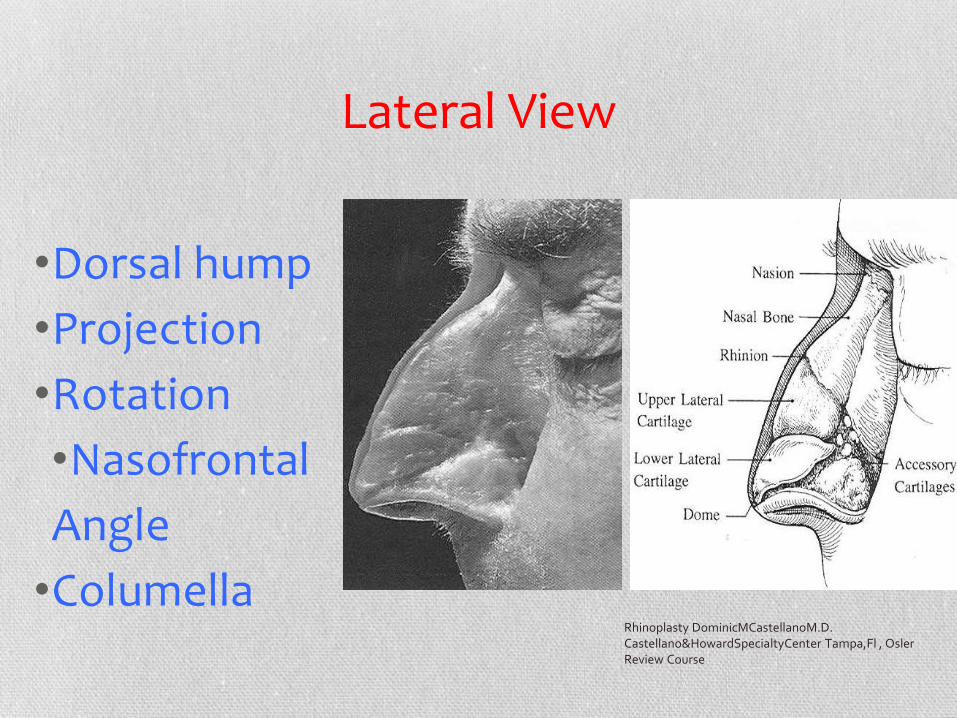
Lateral View
•Dorsal hump
•Projection
•Rotation
•Nasofrontal
Angle
•Columella Rhinoplasty DominicMCastellanoM.D. Castellano&HowardSpecialtyCenter Tampa,Fl , Osler Review Course
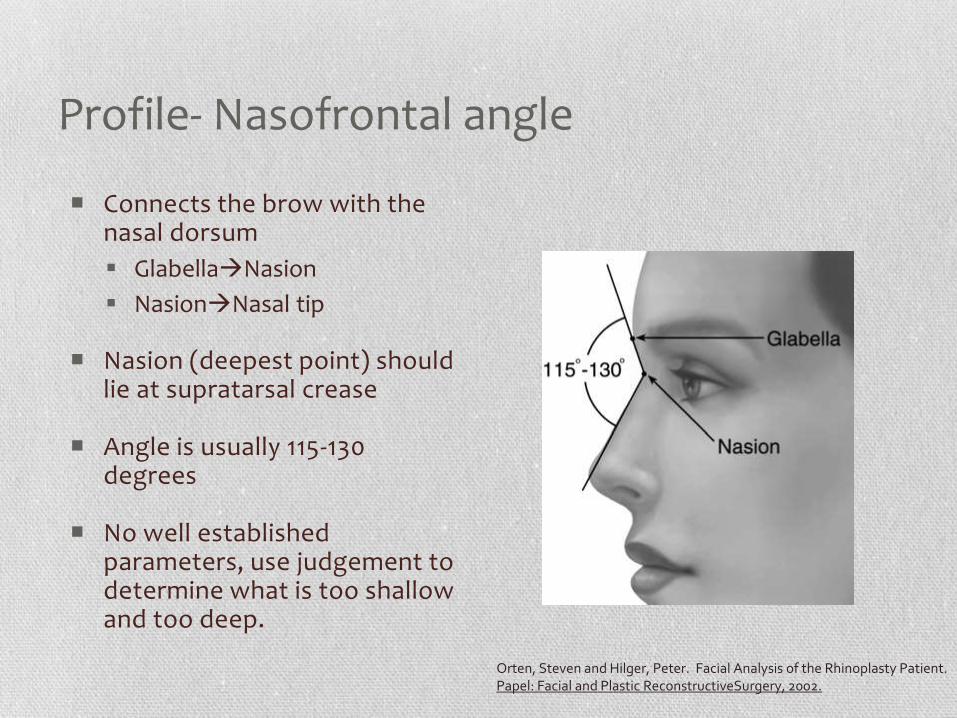
Profile- Nasofrontal angle
Connects the brow with the nasal dorsum
GlabellaNasion
NasionNasal tip
Nasion (deepest point) should lie at supratarsal crease
Angle is usually 115-130 degrees
No well established parameters, use judgement to determine what is too shallow and too deep.
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.
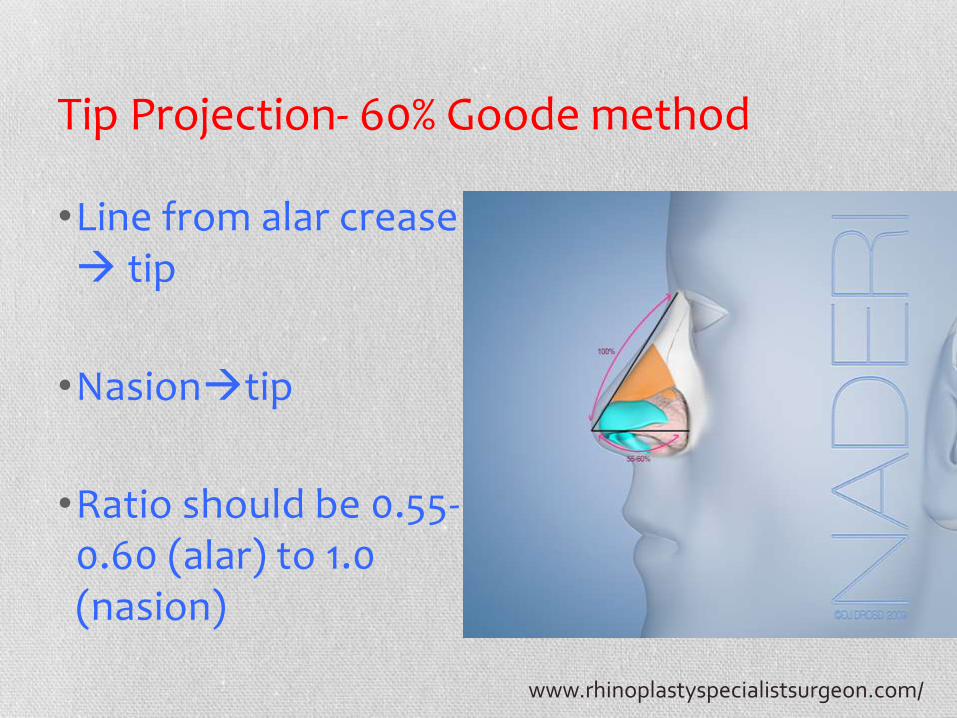
Tip Projection- 60% Goode method
•Line from alar crease tip
•Nasiontip
•Ratio should be 0.55-0.60 (alar) to 1.0 (nasion)
www.rhinoplastyspecialistsurgeon.com/
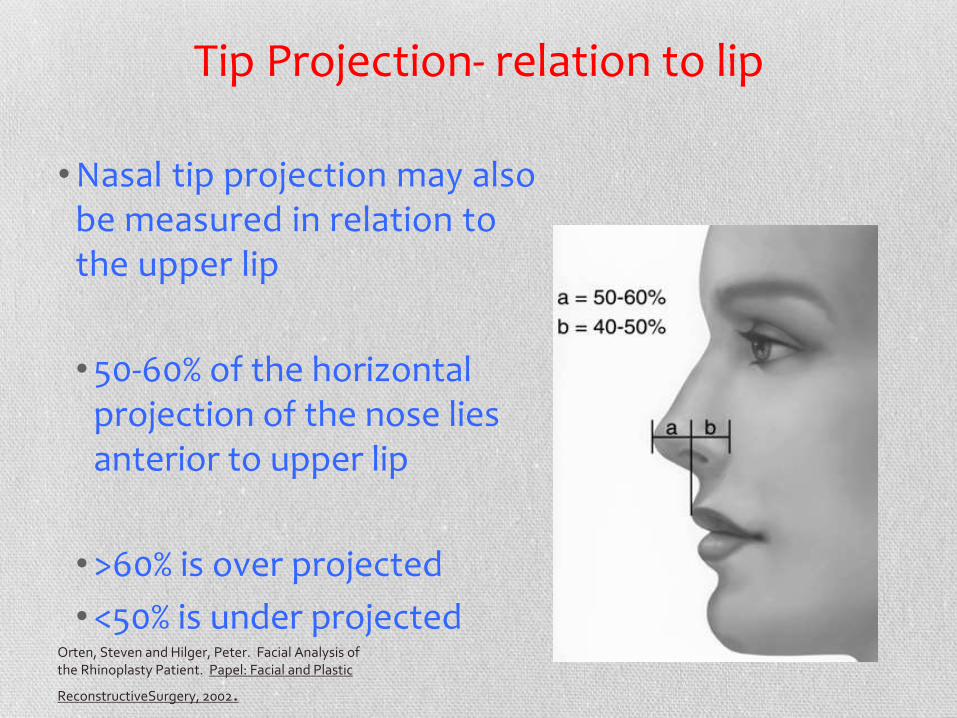
Tip Projection- relation to lip
•Nasal tip projection may also be measured in relation to the upper lip
•50-60% of the horizontal projection of the nose lies anterior to upper lip
•>60% is over projected
•<50% is under projected Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic
ReconstructiveSurgery, 2002.

Lateral View- Dorsum
Line from Nasion to desired tip projection
Nasal dorsum should lie at or slightly (1-2mm) posterior and parallel to this line
Slight supratip break of dorsum gives definition and helps distinguish dorsum from tip
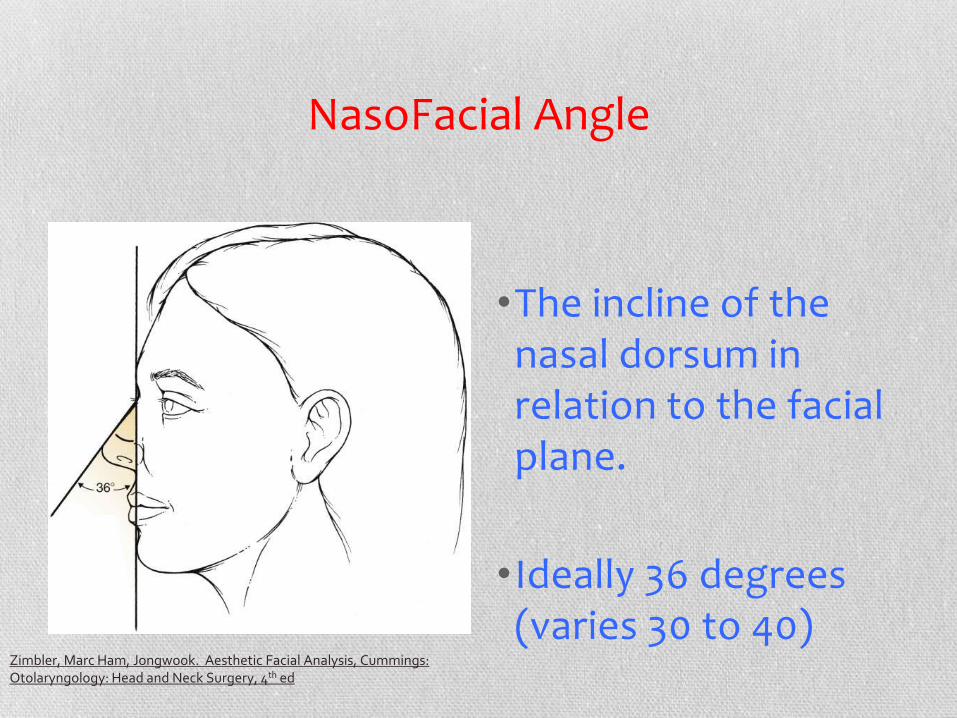
NasoFacial Angle
•The incline of the nasal dorsum in relation to the facial plane.
•Ideally 36 degrees (varies 30 to 40)
Zimbler, Marc Ham, Jongwook. Aesthetic Facial Analysis, Cummings: Otolaryngology: Head and Neck Surgery, 4th ed

Tip rotation- Nasolabial Angle
•Line anterior to posterior point of nostril
•Vertical line perpendicular to Frankfurt plane, dropped along upper lip
•Men 90-95
•Women 95-115
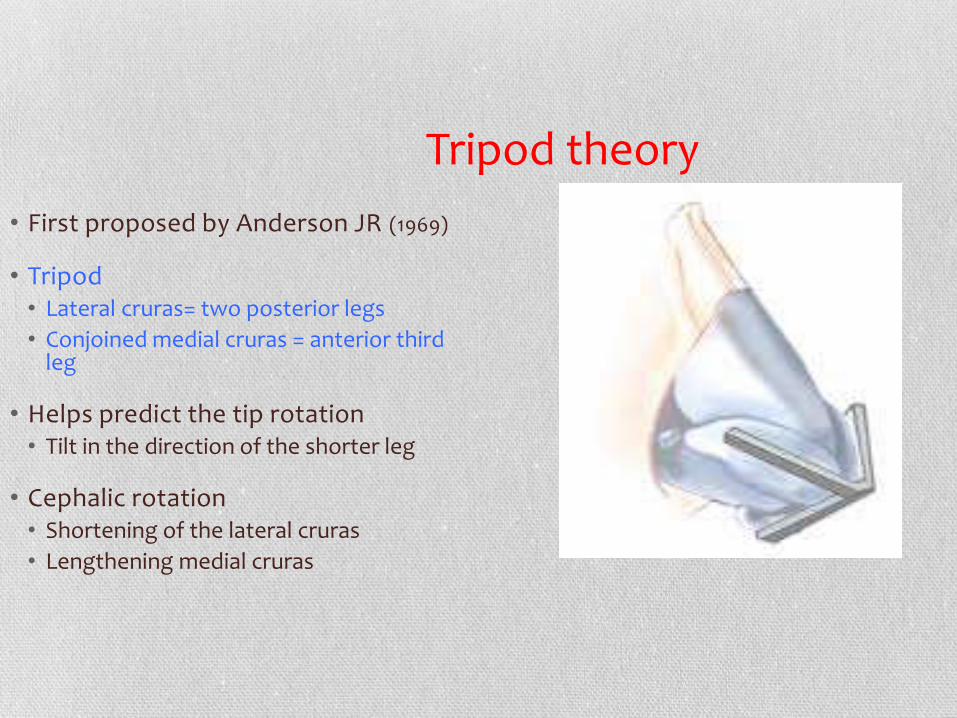
Tripod theory
• First proposed by Anderson JR (1969)
• Tripod • Lateral cruras= two posterior legs
• Conjoined medial cruras = anterior third leg
• Helps predict the tip rotation • Tilt in the direction of the shorter leg
• Cephalic rotation • Shortening of the lateral cruras
• Lengthening medial cruras
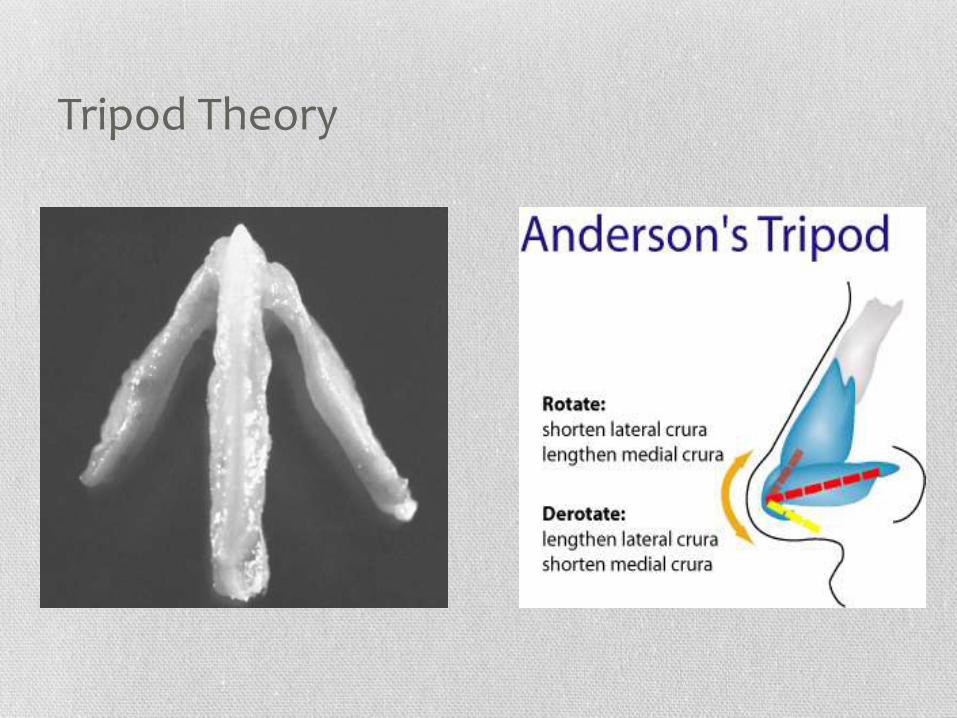
Tripod Theory
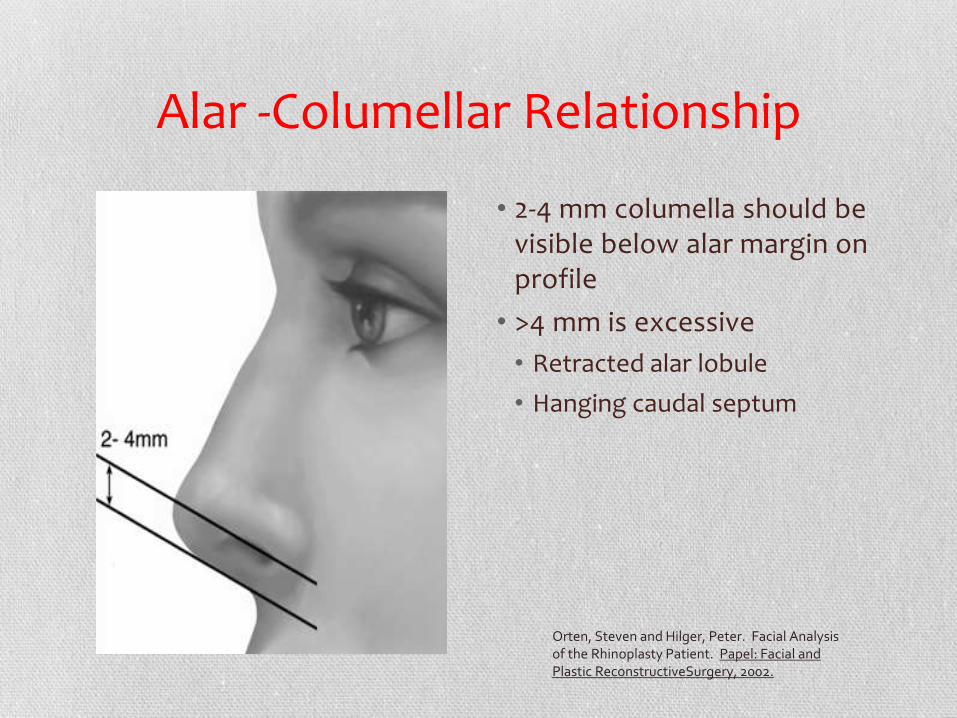
Alar -Columellar Relationship
• 2-4 mm columella should be visible below alar margin on profile
• >4 mm is excessive
• Retracted alar lobule
• Hanging caudal septum
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.
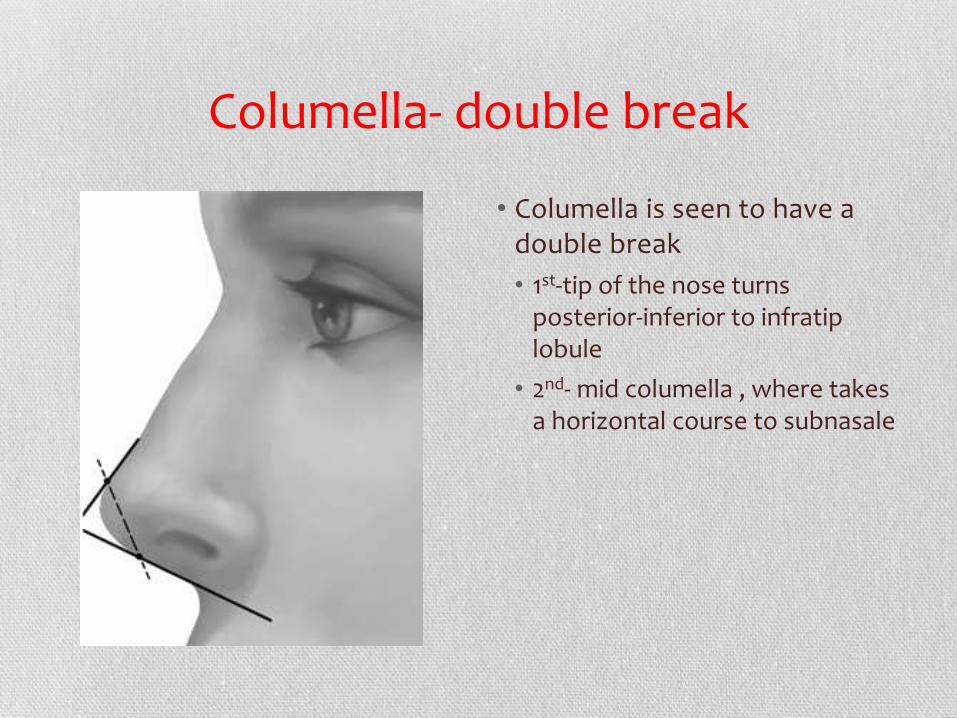
Columella- double break
• Columella is seen to have a double break
• 1st-tip of the nose turns posterior-inferior to infratip lobule
• 2nd- mid columella , where takes a horizontal course to subnasale
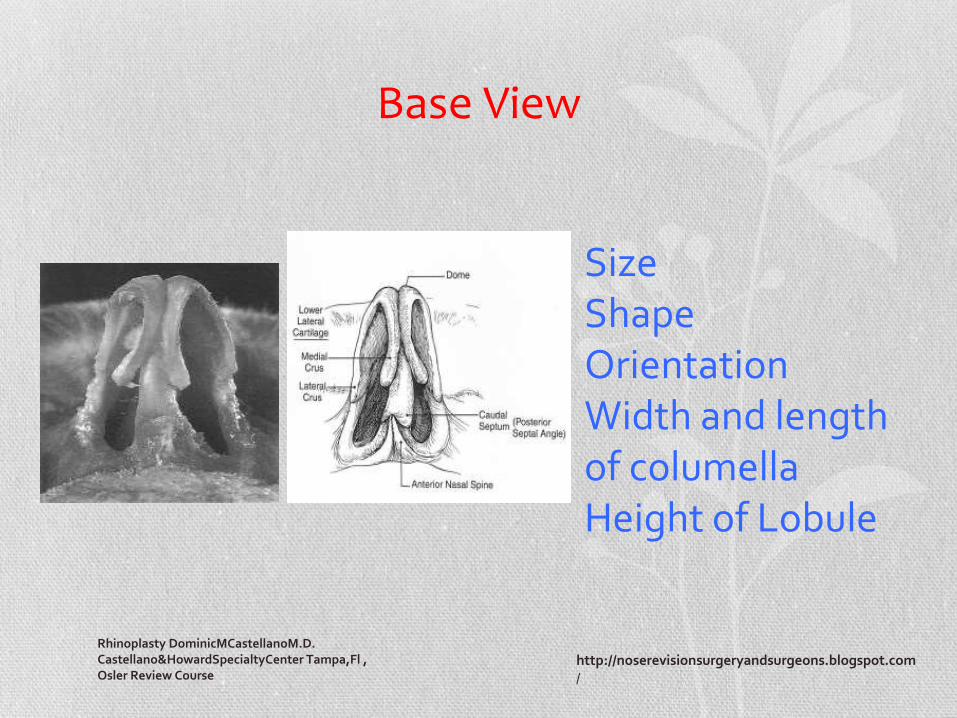
Base View
Rhinoplasty DominicMCastellanoM.D. Castellano&HowardSpecialtyCenter Tampa,Fl , Osler Review Course
Size Shape Orientation Width and length of columella Height of Lobule
http://noserevisionsurgeryandsurgeons.blogspot.com/

Base View
•Isosceles Triangle
•Lobule 1/3
•Columella 2/3
•Nostrils
•Symmetric
•Pear shaped
•Columella flare at base and at infratip lobule
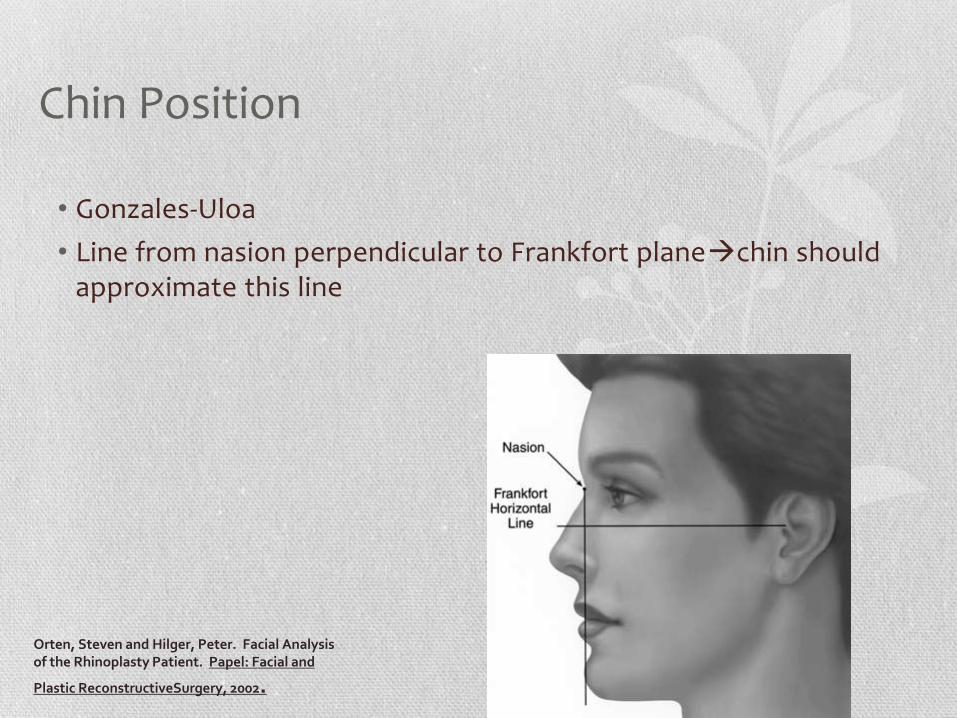
Chin Position
• Gonzales-Uloa
• Line from nasion perpendicular to Frankfort planechin should approximate this line
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and
Plastic ReconstructiveSurgery, 2002.
Inadequate Chin
Microgenia
Underdeveloped mental portion of mandible
Micrognathia
Underdeveloped mandible with class II occlusion
Retrognathia
Mandible is normal in size but retruded with class II occlusion
Micrognathia or retrognathia= orthognathic surgery
Microgenia or doesn’t desire orthognathic surgery=augmentation mentoplasty
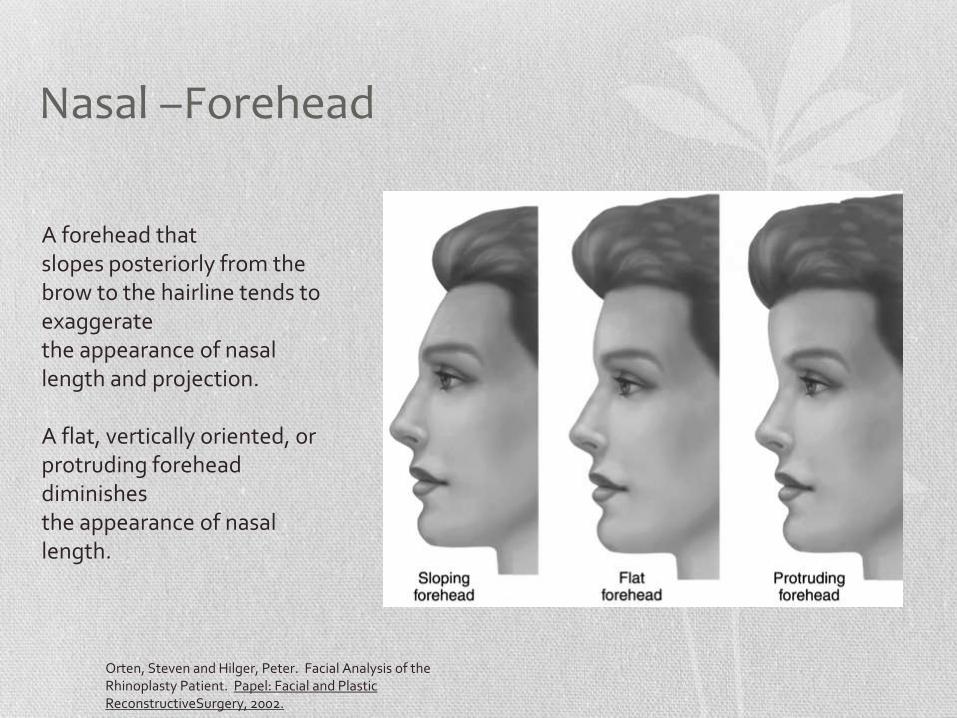
Nasal –Forehead
Orten, Steven and Hilger, Peter. Facial Analysis of the Rhinoplasty Patient. Papel: Facial and Plastic ReconstructiveSurgery, 2002.
A forehead that slopes posteriorly from the brow to the hairline tends to exaggerate the appearance of nasal length and projection. A flat, vertically oriented, or protruding forehead diminishes the appearance of nasal length.
Summary- Frontal View
Frontal View
Divide the face
▪ Horizontal 1/3
▪ Vertical 1/5
Look for asymmetry
Dorsal width
▪ 75% of alar base
Alar width
▪ Intercanthal distance
Shape and asymmetry of tip
Note abnormalities in the dental occlusal relations
Summary-Lateral View
• Nasal length
• Tip projection
• Goode 1: 0.6 ratio
• Crumley 3,4,5
• Tip Rotation
• Nasolabial angle 90-95 men
• 950-115 in women

Nasal Relation
• All analysis of lips should include assessment of forehead, brow, lips, chin, dentition.
• Forehead- Nasofrontal angle
• Chin- Vermillion borders to chin (should be within 2-3 mm)
THE END
Now that I have your attention, let’s practice!
LIP DEFECTS
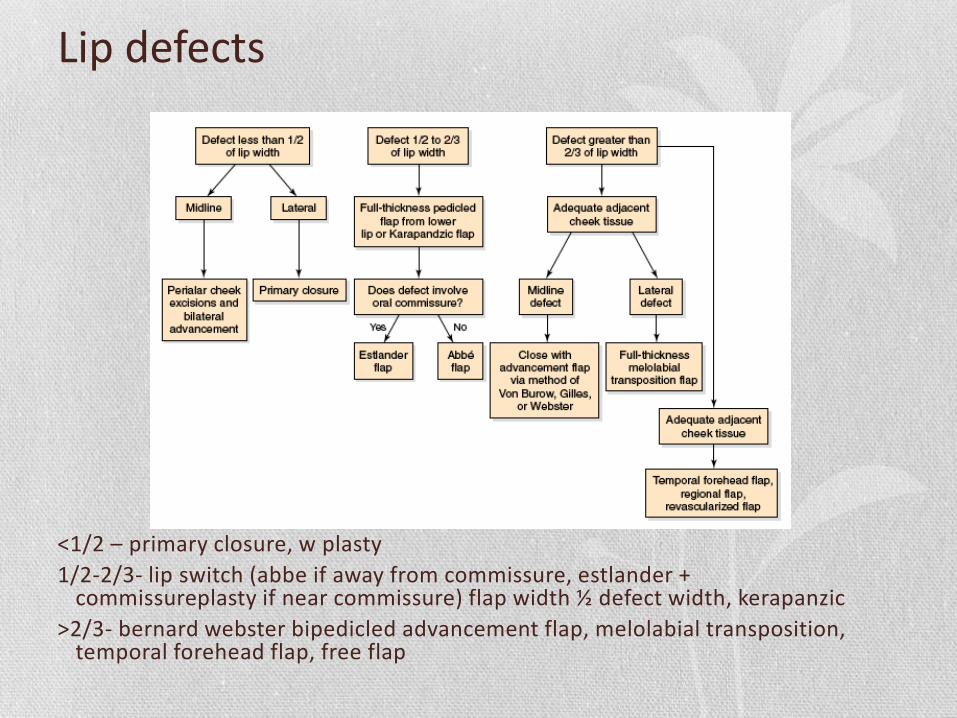
Lip defects
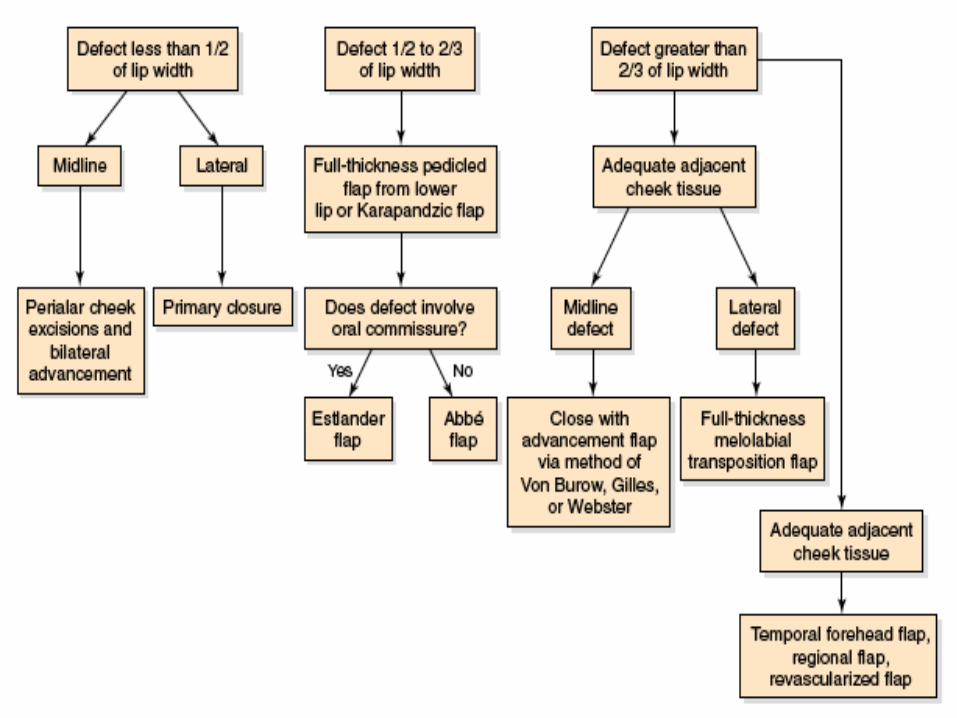
<1/2 – primary closure, w plasty
1/2-2/3- lip switch (abbe if away from commissure, estlander + commissureplasty if near commissure) flap width ½ defect width, kerapanzic
>2/3- bernard webster bipedicled advancement flap, melolabial transposition, temporal forehead flap, free flap
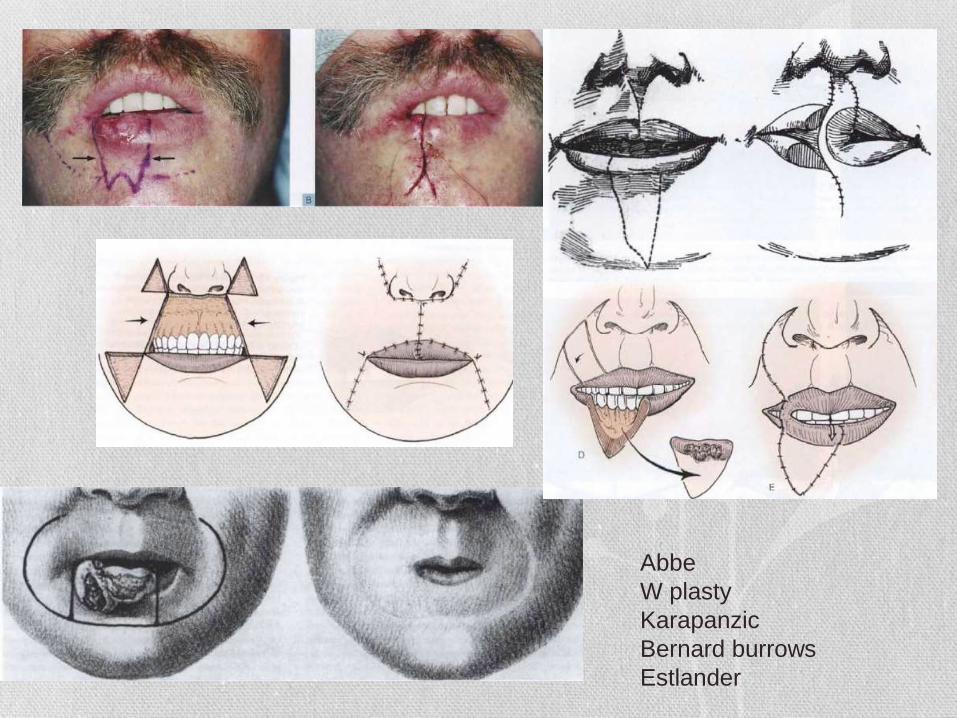
Abbe
W plasty
Karapanzic
Bernard burrows
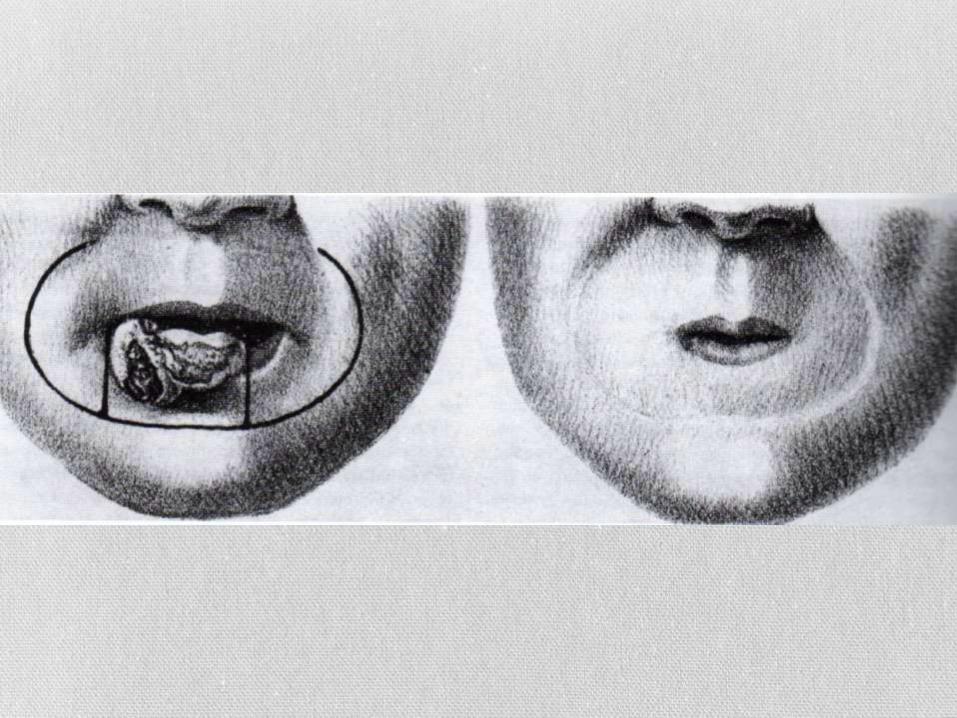
Estlander

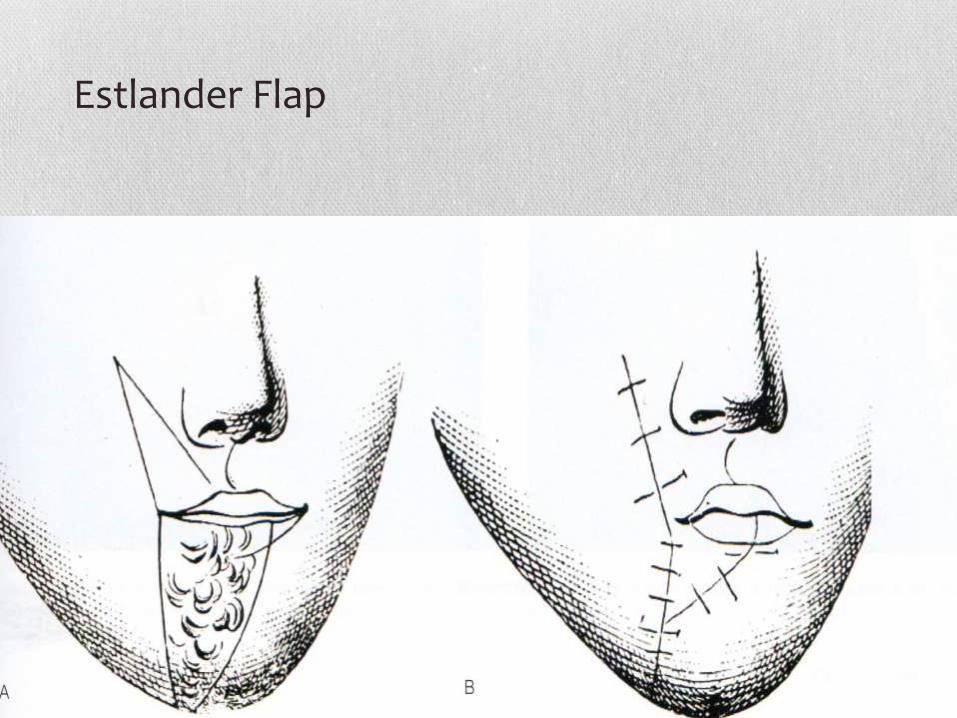
Estlander Flap

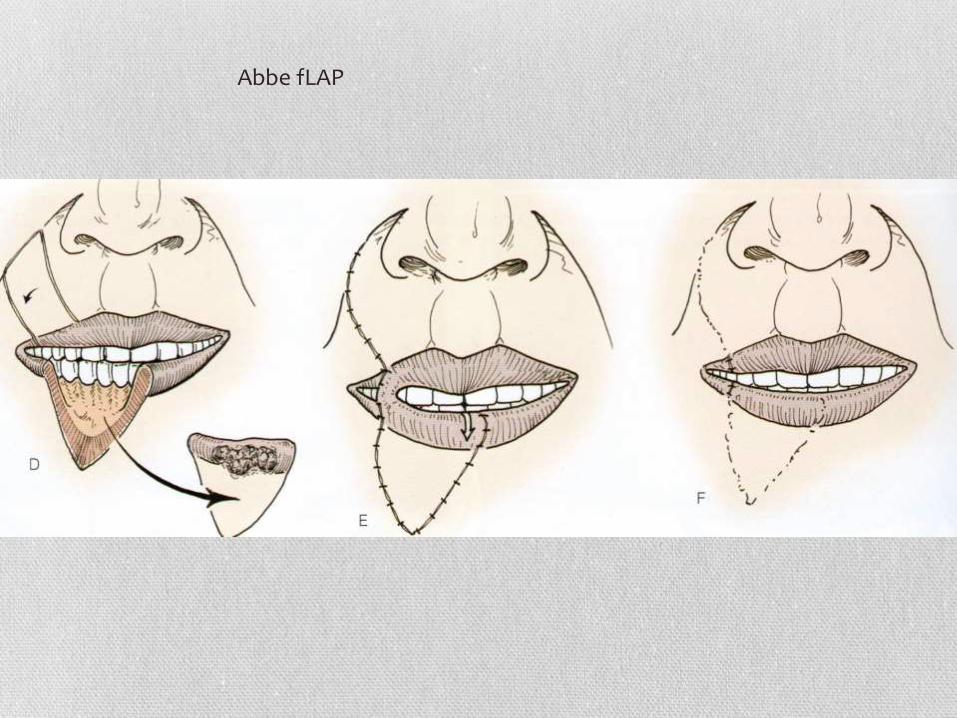
Abbe fLAP