Eyelid Plastic Surgery Reconstructive Center, LLC REGISTRATION · Eyelid Plastic Surgery...
4
. .., REGISTRATION (PLEASE PAINn Eyelid Plastic Surgery & Reconstructive Center, LLC 185 Greenbriar Blvd. Covington, La. 70433 Telephone: (985) 898-2001 Mobile/Cell Number _ Date _ Home Phone _ Patient ~~~----------------~--- Last Name ;"SI Name Imbal Responsible Party (if a minor) _ Street Address _ City State Zip _ Sex 0 M 0 F Age Birthdate 0 Single 0 Married 0 Widowed 0 Separated 0 Divorced Patient Employed By _ Business Address _ occucanoru; Business Phone _ Spouse (or responsibleparty) Name Birthdate --'- Business Name and Address _ occupation Business Phone _ Who is responsible for this account? Relationship to Patient _ Social Security # Spouse's Social Security # _ Do you have Medical Insurance? 0 No 0 Yes ~ NameofPrima~lnsurer------------------------------------ _ If yes. Contract # Group # Subscriber # _ Name of Secondary Insurer (if any) _ Contract # Group # Subscriber # _ o Medicare o Medicaid Claim 10 # _ If Welfare. your number County 01'- _ In case of emergency,who should be notified? Phone _ How did you leam of our practice? _ Slgnal1Jre 01 tnsuree/Guardran Dale ASSIGNMENT AND RELEASE I. the undersiqned. have Insurance coverage With , ame 01 Ir surance Company and assign directly to Dr. all medical benefits. If any. otherwise payable to me for services rendered. I understand that I am financially responsible for all charges whether or not paid by Insurance. I hereby authonze the doctor to release all information necessary to secure the payment of benefits. I authonze the use of this signature on all my Insurance submissions. MEDICARE AUTHORIZATION I -equest that payment of authorized Medicare benefits be made either to me or on my behalf to Dr. for any services furnished me by that physician. I authonze any holder of medical mtormanon about me to release to the Health Care Financing Administration and ItS agents any Information needed to determine these benefits or the benefits payable for related services. I understand my Signature requests that payment be made and authorizes release of medical information necessary to pay the claim. If "other health insurance" is Indicated In Item 9 of the HCFA-1500 form. or elsewhere on other approved claim forms or electronically submitted claims. my signature authorizes releasing of the Information to the Insurer or agency shown. In Medicare assigned cases. the phystcian or supplier agrees to accept the charge determination of the Medicare earner as the full charge. and the patient IS responsible only for the deductible. comsurance, and noncovered ser- vices. Coinsurance and the deductible are based upon the charge determination of the Medicare earner, geneflc1ary S'gnalure Jale
Transcript of Eyelid Plastic Surgery Reconstructive Center, LLC REGISTRATION · Eyelid Plastic Surgery...
. ..,
REGISTRATION(PLEASE PAINn
Eyelid Plastic Surgery & Reconstructive Center, LLC185 Greenbriar Blvd.Covington, La. 70433Telephone: (985) 898-2001
Mobile/Cell Number _
Date _ Home Phone _
Patient ~~~----------------~---Last Name ;"SI Name Imbal
Responsible Party (if a minor) _
Street Address _
City State Zip _
Sex 0 M 0 F Age Birthdate 0 Single 0 Married 0 Widowed 0 Separated 0 Divorced
Patient EmployedBy _
Business Address _
occucanoru; Business Phone _
Spouse (or responsibleparty) Name Birthdate --'-
Business Nameand Address _
occupation Business Phone _
Who is responsible for this account? Relationship to Patient _
Social Security # Spouse's Social Security # _
Do you have Medical Insurance? 0 No 0 Yes ~
NameofPrima~lnsurer------------------------------------ _
If yes.
Contract # Group # Subscriber # _
Name of Secondary Insurer (if any) _
Contract # Group # Subscriber # _
o Medicare o Medicaid Claim 10# _
If Welfare. your number County 01'- _
In case of emergency,who should be notified? Phone _
How did you leam of our practice? _
Slgnal1Jre 01 tnsuree/Guardran Dale
ASSIGNMENT AND RELEASE
I. the undersiqned. have Insurance coverage With, ame 01 Ir surance Company
and assign directly to Dr. all medical benefits. If any. otherwise payable to mefor services rendered. I understand that I am financially responsible for all charges whether or not paid by Insurance. I hereby authonze the doctorto release all information necessary to secure the payment of benefits. I authonze the use of this signature on all my Insurance submissions.
MEDICARE AUTHORIZATION
I -equest that payment of authorized Medicare benefits be made either to me or on my behalf to Dr.for any services furnished me by that physician. I authonze any holder of medical mtormanon about me to release to the Health Care FinancingAdministration and ItS agents any Information needed to determine these benefits or the benefits payable for related services. I understand mySignature requests that payment be made and authorizes release of medical information necessary to pay the claim. If "other health insurance"is Indicated In Item 9 of the HCFA-1500 form. or elsewhere on other approved claim forms or electronically submitted claims. my signature authorizesreleasing of the Information to the Insurer or agency shown. In Medicare assigned cases. the phystcian or supplier agrees to accept the chargedetermination of the Medicare earner as the full charge. and the patient IS responsible only for the deductible. comsurance, and noncovered ser-vices. Coinsurance and the deductible are based upon the charge determination of the Medicare earner,
geneflc1ary S'gnalure Jale
DATE: NAME: _
PLEASE ANSWER THE FOLLOWING QUESTIONS ABOUT YOUR HEALTH
1. PLEASE LIST ALL MEDICATIONS, INCLUDING EYE MEDICATIONS, ANDASPIRIN IF TAKEN EVERY DAY.
2. PLEASE LIST ALL MEDICATIONS TO WHICH YOU ARE ALLERGIC?
3. PLEASE LIST ALL ACCIDENTS OR INJURIES:
YEAR ACCIDENTIINJURY
4. PLEASE LIST ALL HOSPITIALIZATIONS OR OPERATIONS:
YEAR HOSPIT ALIZA TION/OPERA TION
5. HAVE YOU EVER BEEN EXPOSED TO OR HAD CLOSE CONTACT WITHANYONE WITH HEPATITIS, TUBERCULOSIS, OR mv INFECTION (AIDS)?
NO YES
NAME OF REFERRING PHYSICIAN: _
ADDRESS: CITY/ZIP: _
PHONE: _
NAME OF CARDIOLOGYIINTERNAL PHYSICIAN:
NAME: _
ADDRESS: CITY/ZIP: _
PHONE: _
pAGE 2
6. HAVE YOU EVER HAD A Y OF THE FOLLOWI G?NO YES
HIGH BLOOD PRESSURE .HEART DISEASE .ABNORMAL HEART BEAT.STROKE .DIABETES .
CANCER .ASTHMA OR BRONCHITIS ..THYROID DISEASE .MIGRAINE HEADACHES .ARE YOU PREGNANT .
7. HAS YOU OR ANYONE IN YOUR FAMIL Y HAD ANY OF THE FOLLOWING:NO YES NO YES
BLINDNESS .GLAUCOMA... _MACULAR DEGENERATION. _
RETINAL DETACHMENT .OTHER EYE DiSEASES .
8. HAS ANYONE IN YOUR FAMILY (BLOOD RELATIVE) EVER HAD ANY OF THEFOLLOWING?
HIGH BLOOD PRESSURE .HEART DISEASE .ABNORMAL HEART BEAT ..STROKE .DIABETES .
ASTHMA OR BRONCHITIS .THYROID DiSEASE .MIGRAINE HEADACHES .INHERITED DISEASE ORMENTAL IMPAIRMENT ...
9. DO YOU USE DRUGS, OTHER THAN THOSE PRESCRIBED? __ 0 YESDO YOU SMOKE CIGARETTES? 0 YES
10. DO YOU CONSUME ALCOHOL? NO
11. DO YOU HAVE PROBLEMS WITH ANY OF THE FOLLOWING?
YES
OTOALL
FEVER, WEIGHT LOSS, OR TIREDNESS .EARS, NOSE, MOUTH, OR THROAT .HEART OR BLOOD VESSELS .
NONONONOoo
NONONONONOoo
LUNGS .ESOPHAGUS, STOMACH, OR INTESTINES .KIDNEYS, BLADDER, ORGENITAL SySTEM .MUSCLES, BONES, OR JOINTS .SKIN OR BREASTS .NERVOUS SySTEM .PSYCHIATRIC SySTEM .ENDOCRINE (GLANDULAR) SySTEM .BLOOD OR LYMPH SySTEM .ALLERGIES OR IMMUNE SySTEM .
THE FOLLOWING FOR OFFICE USE ONLY
YESYESYESYESYESYESYESYESYESYESYESYESYES
UPDATE INFORMATION:
PHYSICIANDATE TECH DATE PHYSICIAN TECH
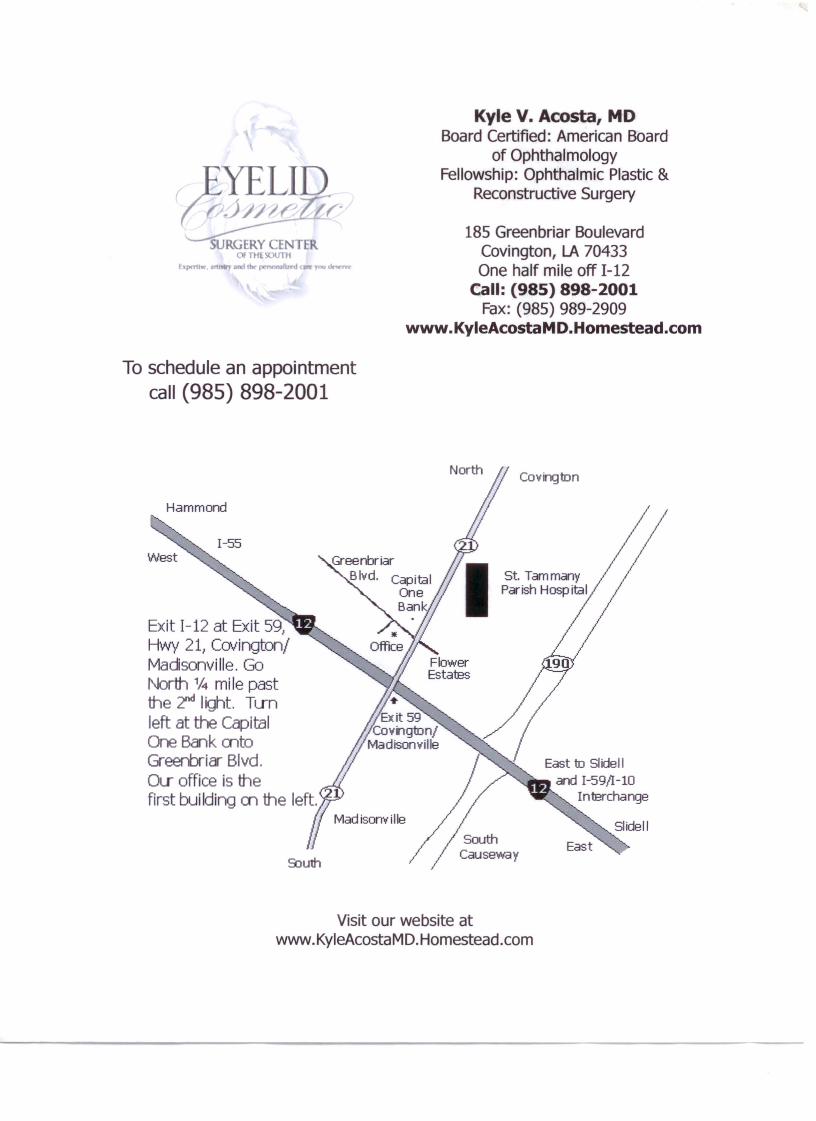
Kyle V. Acosta, MDBoard Certified: American Board
of OphthalmologyFellowship: Ophthalmic Plastic &
Reconstructive Surgery
185 Greenbriar BoulevardCovington, LA 70433One half mile off 1-12
Call: (985) 898-2001Fax: (985) 989-2909
www.KyleAcostaMD.Homestead.com
To schedule an appointmentcall (985) 898-2001
North Covington
St. TammanyPar ish Hasp ita I
Exit 1-12 at Exit 591
Hwy 211 Covington/Madisonvi lie. GoNorth % miIe pastthe ~ Iight. Tunleft at the CapitalOne Bank mtoGreenbriar Blvd.OLI office is thefirst building m the left.
East to Slidelland 1-59/1-10
Interchange
Visit our website atwww.KyleAcostaMD.Homestead.com