
Exploring the adoption of telemedicine and virtual ...
10
REVIEW ARTICLE Exploring the adoption of telemedicine and virtual software for care of outpatients during and after COVID-19 pandemic Anthony Jnr. Bokolo 1 Received: 16 June 2020 /Accepted: 1 July 2020 # The Author(s) 2020 Abstract As the novel coronavirus disease 2019 (COVID-19) continues to spread across countries, the need for innovative measures to provide high-quality patient care and manage its spread has become more imperative. Software-based systems such as medical software applications could provide valuable suggestion on health-related information to physicians towards improving quality of life, especially for outpatients (e.g., elderly, immunosuppressed, pregnant women). The use of telemedicine and virtual software offers promising potential in the fight against COVID-19. Accordingly, by means of expedited literature and document review, this paper provides implication on the opportunities, application, and challenges of telemedicine and existing virtual software currently adopted as suitable initiatives for reducing the spread of COVID-19. More importantly, findings present factors that impact adoption of telemedicine. The findings suggest that telemedicine and virtual software are capable of decreas- ing emergency room visits, safeguarding healthcare resources, and lessening the spread of COVID-19 by remotely treating patients during and after the COVID-19 pandemic. Keywords Coronavirus 2019 . COVID-19 . Outpatient . Pandemic . Telemedicine adoption . Virtual software platforms Introduction On March 11, 2020, the World Health Organization (WHO) declared the coronavirus disease 2019 (COVID-19) outbreak as a pandemic, with more than 720,000 cases reported over 203 countries as of March 31, 2020. The novel COVID-19 pandemic has altered our society, economy, and healthcare system [1, 2]. Residents were advised to quarantine them- selves, and countries have closed their doors to visitors to protect their citizens [3]. Due to the spread of COVID-19, the need for innovative approaches to be employed in control- ling the spread has become more imperative [4]. Additionally, COVID-19 pandemic has placed unprecedented reduction on medical resource and increased risk of occupational exposure for medical practitioners [ 5]. Although addressing the COVID-19 pandemic is multifaceted, one important method that has not yet been fully explored is to leverage information and communications technology (ICT) to support optimal care delivery while lessening the risk of direct human-to- human exposure [6]. Telemedicine which is the deployment of ICT to deliver healthcare digitally can adopted to limit physical human inter- action [4]. Telemedicine use has been increasing during the COVID-19 pandemic, being a tool that reaches patients’ home. In this context, telemedicine and virtual software plat- forms offer affordable, effective, and attractive option. Thus, they can be utilized to manage the pandemic [7]. While this crisis has presented the medical care delivery system with unparalleled challenges [8], COVID-19 has catalyzed rapid use of ICT such as telemedicine and virtual software platforms to deliver healthcare at a distance [9, 10]. Although, telemed- icine and virtual software platforms have been used to greatly monitor patients across different medical facilities, it has had fewer applications in larger setting [11]. In the present COVID-19 pandemic, social distancing and quarantine have been adopted as effective methods to reduce the spread of COVID-19. Also, due to the current stay at home measure put in place by governments, telemedicine and virtual soft- ware platforms are suggested to provide health services in this study [12]. Telemedicine could also be employed also within hospital wards (for instance, to help attending nurses in intensive care * Anthony Jnr. Bokolo [email protected] 1 Department of Computer Science, Norwegian University of Science and Technology, NTNU, NO-7491 Trondheim, Norway https://doi.org/10.1007/s11845-020-02299-z / Published online: 8 July 2020 Irish Journal of Medical Science (1971 -) (2021) 190:1–10
Transcript of Exploring the adoption of telemedicine and virtual ...

REVIEW ARTICLE
Exploring the adoption of telemedicine and virtual software for careof outpatients during and after COVID-19 pandemic
Anthony Jnr. Bokolo1
Received: 16 June 2020 /Accepted: 1 July 2020# The Author(s) 2020
AbstractAs the novel coronavirus disease 2019 (COVID-19) continues to spread across countries, the need for innovative measures toprovide high-quality patient care and manage its spread has become more imperative. Software-based systems such as medicalsoftware applications could provide valuable suggestion on health-related information to physicians towards improving qualityof life, especially for outpatients (e.g., elderly, immunosuppressed, pregnant women). The use of telemedicine and virtualsoftware offers promising potential in the fight against COVID-19. Accordingly, by means of expedited literature and documentreview, this paper provides implication on the opportunities, application, and challenges of telemedicine and existing virtualsoftware currently adopted as suitable initiatives for reducing the spread of COVID-19. More importantly, findings presentfactors that impact adoption of telemedicine. The findings suggest that telemedicine and virtual software are capable of decreas-ing emergency room visits, safeguarding healthcare resources, and lessening the spread of COVID-19 by remotely treatingpatients during and after the COVID-19 pandemic.
Keywords Coronavirus 2019 . COVID-19 . Outpatient . Pandemic . Telemedicine adoption . Virtual software platforms
Introduction
On March 11, 2020, the World Health Organization (WHO)declared the coronavirus disease 2019 (COVID-19) outbreakas a pandemic, with more than 720,000 cases reported over203 countries as of March 31, 2020. The novel COVID-19pandemic has altered our society, economy, and healthcaresystem [1, 2]. Residents were advised to quarantine them-selves, and countries have closed their doors to visitors toprotect their citizens [3]. Due to the spread of COVID-19,the need for innovative approaches to be employed in control-ling the spread has become more imperative [4]. Additionally,COVID-19 pandemic has placed unprecedented reduction onmedical resource and increased risk of occupational exposurefor medical practitioners [5]. Although addressing theCOVID-19 pandemic is multifaceted, one important methodthat has not yet been fully explored is to leverage informationand communications technology (ICT) to support optimal
care delivery while lessening the risk of direct human-to-human exposure [6].
Telemedicine which is the deployment of ICT to deliverhealthcare digitally can adopted to limit physical human inter-action [4]. Telemedicine use has been increasing during theCOVID-19 pandemic, being a tool that reaches patients’home. In this context, telemedicine and virtual software plat-forms offer affordable, effective, and attractive option. Thus,they can be utilized to manage the pandemic [7]. While thiscrisis has presented the medical care delivery system withunparalleled challenges [8], COVID-19 has catalyzed rapiduse of ICT such as telemedicine and virtual software platformsto deliver healthcare at a distance [9, 10]. Although, telemed-icine and virtual software platforms have been used to greatlymonitor patients across different medical facilities, it has hadfewer applications in larger setting [11]. In the presentCOVID-19 pandemic, social distancing and quarantine havebeen adopted as effective methods to reduce the spread ofCOVID-19. Also, due to the current stay at home measureput in place by governments, telemedicine and virtual soft-ware platforms are suggested to provide health services in thisstudy [12].
Telemedicine could also be employed also within hospitalwards (for instance, to help attending nurses in intensive care
* Anthony Jnr. [email protected]
1 Department of Computer Science, Norwegian University of Scienceand Technology, NTNU, NO-7491 Trondheim, Norway
https://doi.org/10.1007/s11845-020-02299-z
/ Published online: 8 July 2020
Irish Journal of Medical Science (1971 -) (2021) 190:1–10

units treating COVID-19 patients in the rehabilitation pro-gramme guided by physiotherapists). Therefore, the objectiveof this study is to provide guidance for treatment of outpatientsto help guide medical practitioners as they provide care duringand after the COVID-19 pandemic. This paper provides im-plications on the opportunities, application, and factors thatimpact adoption of telemedicine and virtual software plat-forms to reduce the spread of COVID-19 pandemic.Likewise, findings from this paper provide invaluable recom-mendations related to the impact of telemedicine and virtualsoftware platforms on flattening the infection curve ofCOVID-19. The remainder of the paper is structured as fol-lows: “Methodology,” “Findings,” “Discussion and implica-tions,” and, lastly, “Conclusion.”
Methodology
This study adopts an expedited literature review similar toprior study Grimes et al. [13] as a research method based onrecommendations from Jnr [14] to guide this study as seen inFig. 1.
Figure 1 depicts the research design which comprises of sixactivities: research questions, search strategies, inclusion andexclusion criteria, quality assessment criteria, data extractionand synthesis, and lastly findings and discussion. Each ofthese activities is briefly discussed below.
Research questions
Accordingly, this research aims to address the following re-search questions:
& RQ1: How can telemedicine and virtual software plat-forms be adopted for treating outpatients during and afterCOVID-19 pandemic?
& RQ2: What are the telemedicine and virtual software plat-forms that are adopted during and after COVID-19pandemic?
& RQ3: What factors impact adoption of telemedicine andvirtual software platforms during and after COVID-19pandemic?
Search strategy
To extensively search for studies related to telemedicine andvirtual software platforms during COVID-19 pandemic, thesearch strategy was carried out using online databases/librar-ies. The search was carried out from May 2, 2020 and endedon May 7, 2020 in Google Scholar, ScienceDirect, PubMed,ProQuest, Springer, Wiley, IEEE Xplore, ACM, Emerald,Taylor & Francis, ISI Web of Science, Sage, Inderscience,and Scopus. These online libraries were selected as they areconsidered appropriate search engines for studies in medical/health science, social science, and information systems re-search. Additionally, they provide options of carrying out ad-vanced search filtering by keywords and by publication year,type, and research area. Figure 2 depicts the PreferredReporting Items for Systematic Reviews and Meta-Analysis(PRISMA) flowchart which was employed to search and se-lect papers.
Using these online databases, studies related to telemedi-cine and virtual software platforms during COVID-19 pan-demic were collected from document reports, journal papers,and conference proceedings. Furthermore, in executing thesearch, specifying keywords or search terms was used tosearch online electronic databases. To confirm review quality,search keywords were formulated by using Boolean AND/ORoperators to combine the search terms to improve the rele-vance of the search procedure. The main search terms com-pose of “telemedicine,” “telehealth,” “virtual software plat-forms,” “digital health,” “virtual medicine,” “e-health,”“COVID-19,” “corona virus 2019,” and “pandemic.”Moreover, a list of search strings which included “digital care,health application, medical application, and e-medicine” wasused to search for relevant papers.
As seen in Fig. 2, the search results retrieved 98 articlesusing the abovementioned keywords. Eleven papers werefound as duplicates and were removed. Hence, the total num-ber of remaining papers becomes 87. Next, 23 studies wereremoved based on title and abstract check assessing if thepapers were aligned to the research questions being explored(see “Research questions” section) resulting to 64 papers. Theremaining papers were evaluated against the inclusion andexclusion criteria (see “Inclusion and exclusion criteria”
Fig. 1 Research design employedin this study
2 Ir J Med Sci (2021) 190:1–10

section). Therefore, 34 articles were found to meet the inclu-sion criteria. After which 1 paper was added based on cross-referencing resulting to 35 papers.
Inclusion and exclusion criteria
After retrieving the papers from the online libraries, each pa-per was examined based on the inclusion and exclusioncriteria as seen in Table 1.
Quality assessment criteria
One of the important criteria that is required to be checkedalong with the inclusion and exclusion criteria is the qual-ity assessment. A higher level of rigorousness of studies isemployed to check quality of papers. Thus, a quality as-sessment checklist confirmed that more than 50% of theselected papers are indexed in ISI Web of Science orScopus database.
Table 1 Inclusion and exclusion criteria
Inclusion criteria Exclusion criteria
Studies published in English language. Studies that are not written in English language.
Journal articles, conference proceedings, and document reports. Not journal articles, conference proceedings, and document reports.
Published between 2020 till date. Published before 2020.
Studies that provide possible answers to research questions based on title andabstract content.
Remove duplicate/similar studies by retaining the most current andcomprehensive version.
Conceptual, literature review, quantitative, qualitative, and experimental studiesthat provide evidence.
Studies that do not provide any theoretical, empirical, or statisticalevidence.
Studies generally related to virtual software platforms and COVID-19 pan-demic.
Studies not related to virtual software platforms and COVID-19 pan-demic.
Studies related to related to role of ICT to manage COVID-19 pandemic. Studies not related to role of ICT to manage COVID-19 pandemic.
Fig. 2 PRISMA flowchart forsearch process
3Ir J Med Sci (2021) 190:1–10

Data extraction and synthesis
This stage of the review aims to synthesize and categorize theselected papers based on their scope as related to telemedicineand virtual software platforms during COVID-19 pandemic.Thus, the selected studies were reviewed in detail and relevantdata were extracted, analyzed, and synthesized to provide an-swers to the research questions (see “Research questions”section).
Findings
Opportunities of adopting telemedicine and virtualsoftware platforms
Several approaches have been considered by different coun-tries to manage and control COVID-19 pandemic.Telemedicine and virtual software platforms are one of themethods to manage COVID-19 pandemic [15, 16]. Giventhe high risk of transmission of the virus through person-to-person contact, telemedicine can be beneficial in reducingdirect contact and helps for patient follow-up [17].Telemedicine and virtual software platforms overcome phys-ical barriers to provide physicians and patients access to med-ical care [1]. Adoption of virtual software platforms with tele-medicine sustains the continuity of outpatient care during andbeyond the COVID-19 pandemic in the midst of social dis-tancing measures, quarantine, and stay at home orders whilereducing spread of the virus [5, 13].
Telemedicine also proves useful, in particular, to help con-serve personal protective equipment and provide isolated pa-tients connection to friends and family [18]. Accordingly, fewmedical centers have resorted adopting virtual software plat-forms such as Microsoft Teams, Zoom, Google Hangouts,Skype, Facebook Messenger, Apple Facetime, and others tofacilitate telemedicine care during the pandemic [1].Respectively, according to Chauhan et al. [6], Doshi et al.[15], and Vidal-Alaball et al. [16], adoption of telemedicineand virtual software platforms aids in the following;
& Decrease the time required to get a diagnosis and initiatetreatment, stabilize, or quarantine a patient
& Facilitates close follow-up with patients who can be mon-itored from their home to avoid oversaturation of healthfacilities
& Reducing movement of people, minimizing the risk ofintra-hospital infection
& Supports co-ordination of medical resources utilized indistant locations
& Prevent the risk of contagion, particularly for medicalpractitioners, who are key assets
& Aids in informing the general public
& Saves costs on disposable robes, antiseptic material,gloves, disinfecting of hospital spaces, etc.
& Training of medical practitioners who are new to the treat-ment of pandemic
& Monitoring of real-world data, for example, JohnsHopkins COVID-19 website (https://coronavirus.jhu.edu/map.html) and the VG live corona website update(https://www.vg.no/spesial/2020/corona/) which provideregularly updated information on COVID-19
Adoption of telemedicine and virtual softwareplatforms for treating outpatients
Telemedicine and virtual software platforms have been previ-ously adopted in providing medical care during public healthemergencies [5]. Adoption of telemedicine and virtual soft-ware platforms provides medical practitioners with reliableinformation platform that outlines factual information,allowing attending physician to obtain authenticate informa-tion in real time [19]. In response to the current COVID-19pandemic, medical centers are adopting telemedicine and vir-tual software platforms to provide after hours health coveragefrom 6 pm to 8 am [5]. An illustration on the application oftelemedicine is shown in Fig. 3.
Figure 3 depicts telemedicine process applied for treat-ment. Thus, telemedicine helps for storage of relevant data,such as physical findings or patient complaints, through trans-fer of stored video or static images, which can be transferred tothe receiving physician to review at a later time [20, 21].Outpatients can adopt either asynchronous (not same timeusing e-mail, patient portal messages, health apps, e-consults,etc.) [2, 22, 23] or synchronous (same time using telephone,videoconferencing, etc.) telemedicine and virtual softwareplatforms [10, 11, 18]. As stated by Doshi et al. [15], medicalcenters are deploying on-site commercial telemedicine carts atmedical centers and hospital-provided laptops at home. Theyalso use video software such as Google Duo, Zoom, andMicrosoft teams and commercially provided digital stetho-scopes and web cameras.
Evidence from Banskota et al. [24], Grimes et al. [13], andShokri and Lighthall [5] mentioned that patients are happywith the virtual medical experience and appreciate the conti-nuity of obtaining medical care without having to risk theirhealth leaving home during the COVID-19 pandemic. Also,Shokri and Lighthall [5] stated that currently patients are seenin real time using audiovisual appointments, including prelim-inary consultations, and future follow-ups. However, patientsthat require urgent medical care are still being examined inperson with physicians donning of proper PPE [22]. Thus,telemedicine is not meant to replace in-person healthcare. Itallows for protecting patient and physicians from exposure to
4 Ir J Med Sci (2021) 190:1–10

potential infections and fostering compliance of quarantineand social distancing initiatives [5].
Telemedicine and virtual software platforms adoptedduring and after COVID-19 pandemic
As the world faces the impact of COVID-19, several virtualsoftware platforms are being adopted. As recommended byKeesara et al. [25], beyond video consultation software andmobile phone applications, other software platforms such aschatbots and wearable devices are being adopted. These vir-tual software platforms are deployed to provide asynchronousand synchronous support both for outpatients. Also, these vir-tual software platforms provide synchronous real-time audio-visual-enabled visits and are easy to use for physicians, pa-tients, and attending staff scheduling appointments, allowing
for patient treatment via smart phone computer, or tablet, andconforms to patient privacy laws [5]. Additionally, otheremerging virtual software platforms such as voice-interfacesystems (e.g., Google Voice, Amazon Alexa, Apple Siri) ormobile sensors such as thermometers, smartwatches, or oxy-gen monitors can be adopted for treatment at home [25].
Although adopting these virtual software platforms in se-vere situation poses difficulties, many medical-based healthsystems are already leveraging existing telemedical platformsin their response for treatment of patients [5]. As suggested byDoshi et al. [15], physicians use virtual software platforms,specifically synchronous audio and video applicationsequipped with high definition videos and digital otoscopes,stethoscopes, dermatoscopes, and ophthalmoscopes used forexamining and monitoring patients. In adopting telemedicineand virtual software platforms, physicians must get patient
Fig. 3 Telemedicine processapplication
5Ir J Med Sci (2021) 190:1–10

consent for online consultation (mostly automated in virtualsoftware platforms privacy statement seen during installationof the software), document the type of consultation (e.g., syn-chronous or asynchronous), location of patient and physician,identity confirmation, and documentation of medical serviceperformed (date, time, and duration) [5].
Factors that impact adoption of telemedicine andvirtual software platforms
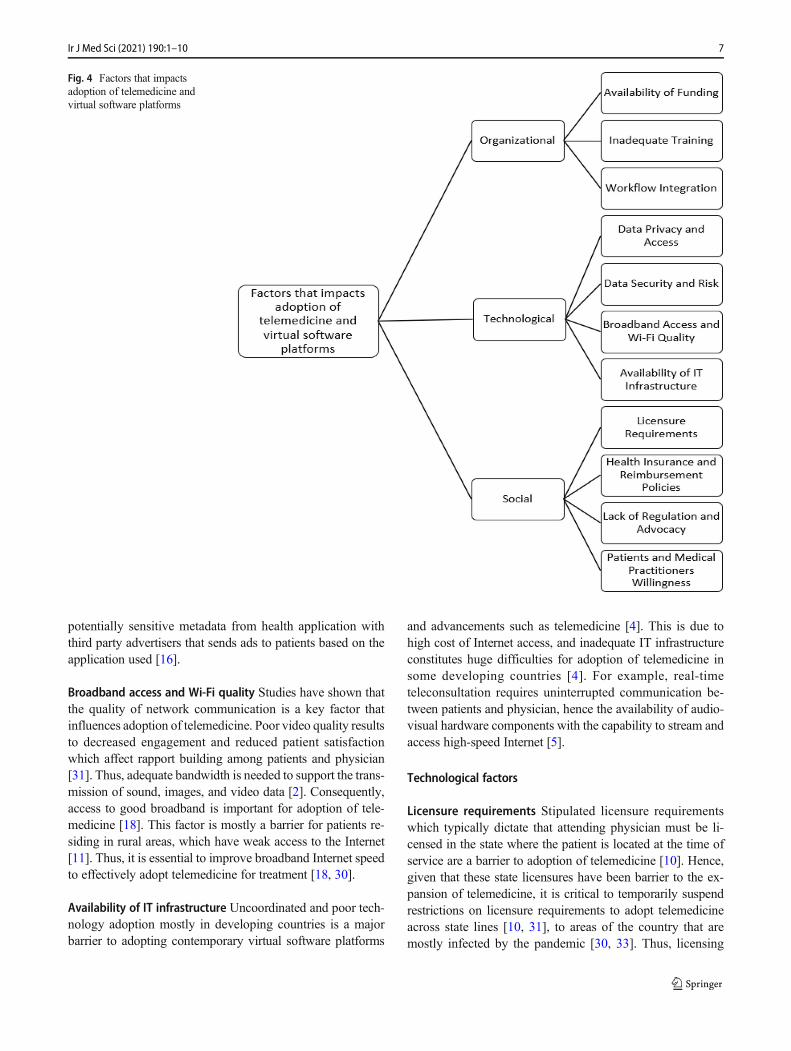
Telemedicine and virtual software platforms are practicallyfeasible and appropriate for the support of medical practi-tioners and patients during and after this pandemic via syn-chronous and asynchronous mediums such as smartphone ap-plication, telephone, videoconference, and e-mail [26].Although the adoption of telemedicine and virtual softwareplatforms holds promise for managing pandemic response,its adoption has limitations such as the availability of robustIT infrastructure, licensing and regulatory services, equipmentcosts, training of both physicians and nurses, and alterations tointegrate within current hospital workflows [3, 15, 27].Among others, ethical considerations must be taken into ac-count [5]. Accordingly, this study discusses the social, orga-nizational, and technological factors that impact the wide-spread adoption of telemedicine and virtual software plat-forms by patients and medical practitioners. The factors de-rived from the literature are shown in Fig. 4.
Figure 4 depicts the social, organizational, and technolog-ical factors that impact the widespread adoption of telemedi-cine and virtual software platforms by patients and medicalpractitioners during and after the pandemic. Each of the fac-tors is discussed below.
Organizational factors
Availability of funding The deployment of telemedicine andvirtual software platforms takes time and does not happensuddenly. It requires funding to purchase resources needed.Also, it involves cost of developing the virtual software plat-form with expenditures for equipment, medical practitioners’salaries, information technology (IT) support, and training[15]. As mentioned by Keesara et al. [25], there is need for abroader strategy to cover technical fees that support deploy-ment of needed infrastructures. Thus, the lack of funding is abarrier for adoption of telemedicine [4, 28]. At the moment, afew countries such as the USA, Australia, and China havealready invested in telemedicine and are getting promisingresults. Also, virtual software platforms had been previouslyadopted by few hospitals in the USA such as University ofPittsburgh, Jefferson Health, and Cleveland Clinic [12]. Chinahas also adopted real-time virtual consultation solution thataddresses medical care needs for patients at home [12].
Inadequate training Medical practitioners who interact withpatients through virtual care solutions should be trained [5,29]. Thus, training sessions should be provider and madeavailable when needed [3], either virtually or physically.Similarly, adoption of telemedicine and virtual software plat-forms might be challenging for some citizens as they will needtraining in adopting digital technologies [11, 20]. Findingsfrom prior studies [18] suggest that unfamiliarity with virtualsoftware platforms is a key barrier to adoption of telemedicineservices [2, 5, 23].
Workflow integration Integrating telemedicine to existinghealthcare practice adopted in the hospital that leads to issueson how to manage the use of virtual software platforms formedical treatment of patients by medical practitioners canresult to low uptake by both patients and physicians [23].Thus, workflows for adoption of virtual software platformsshould be drafted to minimize burden [30]. Thus, the adoptedof telemedicine and virtual software platforms should empow-er medical practitioners with flexibility in usage for providingmedical care [31].
Technological factors
Data privacy and access Data privacy and security protectionis a critical factor needed for success of telemedicine [32]. Theprotection and privacy of patient’s data must be important asthis has been an issue in the past [11]. Given recent warningsby Federal Bureau of Investigation (FBI) regarding vulnera-bility of some virtual software platforms, telemedicine mustnot sacrifice data privacy protections and access measures[18]. But, presently, countries such as China and Singaporehave initiated a strict Global Positioning System (GPS) track-ing during quarantine raising issues about infringing on citi-zens liberties and use of private data. Also, adoption ofGeneral Data Protection Regulation (GDPR) during and afterthe pandemic can provide some flexibility as regards to theaccess and use of citizens’ personal medical data [18]. But forthe safety of citizens due to COVID-19, personal medical dataof patients could be accessed without the need to obtain theirconsent. But telemedicine should guarantee data privacy andaccess protection [16].
Data security and risk The adoption of telemedicine and vir-tual software platforms involves digital collection and use ofsensitive medical information among patients and medicalpractitioners [5], which could lead to security risk, for thecollection, use, and disclosure of sensitive personal data[18]. Findings from recent studies [25, 32] revealed that94% of participants highlighted data protection regulationsas one of the factors that limits adoption of virtual softwareplatforms in health sector. This is true because for instance amobile medical application may be sponsored by sharing
6 Ir J Med Sci (2021) 190:1–10
potentially sensitive metadata from health application withthird party advertisers that sends ads to patients based on theapplication used [16].
Broadband access and Wi-Fi quality Studies have shown thatthe quality of network communication is a key factor thatinfluences adoption of telemedicine. Poor video quality resultsto decreased engagement and reduced patient satisfactionwhich affect rapport building among patients and physician[31]. Thus, adequate bandwidth is needed to support the trans-mission of sound, images, and video data [2]. Consequently,access to good broadband is important for adoption of tele-medicine [18]. This factor is mostly a barrier for patients re-siding in rural areas, which have weak access to the Internet[11]. Thus, it is essential to improve broadband Internet speedto effectively adopt telemedicine for treatment [18, 30].
Availability of IT infrastructure Uncoordinated and poor tech-nology adoption mostly in developing countries is a majorbarrier to adopting contemporary virtual software platforms
and advancements such as telemedicine [4]. This is due tohigh cost of Internet access, and inadequate IT infrastructureconstitutes huge difficulties for adoption of telemedicine insome developing countries [4]. For example, real-timeteleconsultation requires uninterrupted communication be-tween patients and physician, hence the availability of audio-visual hardware components with the capability to stream andaccess high-speed Internet [5].
Technological factors
Licensure requirements Stipulated licensure requirementswhich typically dictate that attending physician must be li-censed in the state where the patient is located at the time ofservice are a barrier to adoption of telemedicine [10]. Hence,given that these state licensures have been barrier to the ex-pansion of telemedicine, it is critical to temporarily suspendrestrictions on licensure requirements to adopt telemedicineacross state lines [10, 31], to areas of the country that aremostly infected by the pandemic [30, 33]. Thus, licensing
Fig. 4 Factors that impactsadoption of telemedicine andvirtual software platforms
7Ir J Med Sci (2021) 190:1–10

policy changes should be established during and after the pan-demic without geographical borders or boundaries to physi-cians [4, 5, 29].
Health insurance and reimbursement policiesCurrently, mostmedical insurance does not cover telemedicine treatment andas such do not provide reimbursement for patients. Although, inthe USA, all 50 states and the District of Columbia cover someform of fee medical service for live video with Medicaid [33].Most healthcare insurance coverage such asMedicare has histor-ically had restrictions limiting coverage of telemedicine servicesto specific geographic areas [33]. But, due to the CoronavirusPreparedness and Response Supplemental Appropriations Act of2020, geographic restrictions have currently been waived forMedicare reimbursement [10, 15]. Similarly, both the CMSand a few local commercial payers have revised payment policiesin response to COVID-19 [3, 13].
Lack of regulation and advocacy As supported from the liter-ature, telemedicine and virtual software platforms can beadopted as an effective tool in helping to manage the currentpandemic. However, existing policies are also a barrier thatlimit how, where, and when telemedicine can be adopted [33].Findings from a survey conducted by Price WaterhouseCooper in 2019 revealed that 38% of chief executive officersin US medical care systems reported have no virtual compo-nent in their general strategic plan [11, 25]. Moreover, theexistence of fewer advocacy bodies such as the physicianadvocacy groups, the associations for telemedicine, and pa-tient also contributes to the lower adoption of telemedicineand virtual software platforms for treatment [4].
Patients’ and medical practitioners’ willingness The limitedadoption of telemedicine and virtual software platforms ismostly attributable to physicians’ unwillingness to adopt tele-medicine [24]. Telemedicine is mostly complex and disrup-tive and thus requires physicians to learn new approach ofconsulting [28]. Physicians’ acceptance of telemedicine relieson their perception of telemedicine as being normal, safe, andeffective. Hence, they may not be familiar and aware of tele-medicine, due to limited telemedicine training provided [28].Likewise, many hospitals are not adopting telemedicine be-cause many patients are not well-versed in virtual softwareplatforms and are initially apprehensive of it leading to resis-tance and apathy to technological change [4]. Furthermore, inadopting telemedicine and virtual software platforms for treat-ment, the patient must consent to use of audio and video [13].
Discussion and implications
The COVID-19 pandemic is rapidly transforming the medicalcare system, with telemedicine or virtual telemedicine and
virtual software platforms being one of the crucial drivers ofchange [15, 25]. As the health sector continues to be on thefront lines, medical centers can leverage on telemedicine tosupport their patients, protect their staffs, and conserve scarcemedical resources [3]. In recent years, growth in telemedicinehas been incremental in the world, for example, in the USA, ithas been adopted by only 8% as at 2019 [34]. Findings fromthis study suggest key organizational, technological, and so-cial factors required to improve adoption of telemedicine bypatients and medical practitioners.
Additionally, findings from this study depict telemedicine’stransformative impact on healthcare delivery and the rapid shiftin virtual software platforms adoption among outpatients andmedical practitioners. Thus, telemedicine provides outpatientsof all ages access to asynchronous sharing of biometric data viatheir patient portal and answering pre-set screening question ontheir mobile devices before audio/video consultation [34]. Aspointed out byMann et al. [34] during the COVID-19 pandem-ic, outpatients such as pregnant women are routinely synchro-nizing their home monitoring devices to their physicianthrough electronic health record (HER) and are having ad-vanced post-partum results enabled by telemedicine and virtualsoftware platforms for remote monitoring. This experiencemay likely create future opportunities of healthcare accessibil-ity and convenience that will be difficult to reverse after theCOVID pandemic. Likewise, the regulatory changes raised tosupport easily accessible adoption of telemedicine may beequally hard to reverse [34].
Evidently, patients and medical practitioners across theworld are already adopting telemedicine and virtual softwareplatforms, experiencing their potentials, and establishing ex-pectations and comfort of these software tools for early diag-nosis and follow-up [35]. Accordingly, telemedicine and as-sociated virtual software platforms can help to reduce spreadof COVID-19 during quarantine and social distancing.Possibly, telemedicine should be adopted as a proactive mea-sure to improve medical care and should not only be seen as atemporary fix in times of emergency; rather, it is a convenient,safe, scalable, effective, and green method of providing med-ical care [30]. Although, adoption of telemedicine cannotcompletely solve all the issues caused by COVID-19, it canhelp flatten the infection curve of COVID-19.
Conclusion
Telemedicine should be adopted as a proactive measure toimprove medical care and should not only be seen as a tem-porary fix in times of emergency; rather, it is a convenient,safe, scalable, effective, and green method of providing med-ical care. Therefore, this study explores the significant role oftelemedicine and virtual software platforms in managingCOVID-19 and provides implications of virtual software
8 Ir J Med Sci (2021) 190:1–10

platforms during the pandemic outbreak and beyond.Accordingly, by means of expedited literature and documentreview, this paper discusses the opportunities, application oftelemedicine, and existing virtual software adopted as suitableinitiatives for reducing the spread of COVID-19. More impor-tantly, findings present the social, technological, and organi-zational factors that influence the adoption of telemedicine.Findings from this article suggest that technological advancesin telemedicine have proven to possess huge potentials insupporting social distancing and quarantine towards control-ling the spread COVID-19. The main limitations to this studyare aligned to the rapid nature of the review and use of sec-ondary data from existing literature and document reports.Thus, primary data was not employed to validate the social,technological, and organizational factors. Also, the expeditedreview methods may have inevitably missed some salientstudies on COVID-19. Future work will be directed in provid-ing empirical evidence on the identified factors based on pri-mary data from case studies through interview.
Acknowledgements Open Access funding provided by NTNUNorwegian University of Science and Technology (incl St. OlavsHospital - Trondheim University Hospital).
Data availability Not applicable.
Compliance with ethical standards
Conflict of interest The authors declare that they have no conflict ofinterest.
Code availability Not applicable.
Open Access This article is licensed under a Creative CommonsAttribution 4.0 International License, which permits use, sharing, adap-tation, distribution and reproduction in any medium or format, as long asyou give appropriate credit to the original author(s) and the source, pro-vide a link to the Creative Commons licence, and indicate if changes weremade. The images or other third party material in this article are includedin the article's Creative Commons licence, unless indicated otherwise in acredit line to the material. If material is not included in the article'sCreative Commons licence and your intended use is not permitted bystatutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of thislicence, visit http://creativecommons.org/licenses/by/4.0/.
References
1. Kaminski J (2020) Informatics in the time of COVID-19. Can JNurs Inform. https://cjni.net/journal/?p=6820
2. Rao SS, Loeb AE, Amin RM et al (2020) Establishing telemedicinein an academic total joint arthroplasty practice: needs and opportu-nities highlighted by the COVID-19 pandemic. Arthroplast Today.https://doi.org/10.1016/j.artd.2020.04.014
3. Hollander JE, Carr BG (2020) Virtually perfect? Telemedicine forCOVID-19. N Engl J Med 382:1679–1681
4. Okereafor K, Adebola O, Djehaiche R (2020) Exploring the poten-tials of telemedicine and other non-contact electronic health tech-nologies in controlling the spread of the novel coronavirus disease(COVID-19). IJITE 8(4):1–13
5. Shokri T, Lighthall JG (2020) Telemedicine in the era of theCOVID-19 pandemic: implications in facial plastic surgery.Facial Plast Surg Aesthetic Med 22(3):155–157. https://doi.org/10.1089/fpsam.2020.0163
6. Chauhan V, Galwankar S, Arquilla B et al (2020) Novel coronavi-rus (COVID-19): leveraging telemedicine to optimize care whileminimizing exposures and viral transmission. J Emerg TraumaShock 13(1):20
7. Hakim AA, Kellish AS, Atabek U et al (2020) Implications for theuse of telehealth in surgical patients during the COVID-19 pandem-ic. Am J Surg 220(1):48–49. https://doi.org/10.1016/j.amjsurg.2020.04.026
8. Pan XB (2020) Application of personal-oriented digital technologyin preventing transmission of COVID-19, China. Ir J Med Sci.https://doi.org/10.1007/s11845-020-02215-5
9. O’Reilly MF, Merghani K, Sheehan E (2020) Virtualised care andCOVID-19. Ir J Med Sci. https://doi.org/10.1007/s11845-020-02269-5
10. Wright JH, Caudill R (2020) Remote treatment delivery in responseto the COVID-19 pandemic. Psychother Psychosom 89(3):1–3.https://doi.org/10.1159/000507376
11. Leite H, Hodgkinson IR, Gruber T (2020) New development:‘healing at a distance’—telemedicine and COVID-19. PublicMoney Manag 40(6):483–485. https://doi.org/10.1080/09540962.2020.1748855
12. Moazzami B, Razavi-Khorasani N, Moghadam AD, Farokhi E,Rezaei N (2020) COVID-19 and telemedicine: immediate actionrequired for maintaining healthcare providers well-being. J ClinVirol 126:1–2. https://doi.org/10.1016/j.jcv.2020.104345
13. Grimes CL, Balk EM, Crisp CC et al (2020) A guide forurogynecologic patient care utilizing telemedicine during theCOVID-19 pandemic: review of existing evidence. IntUrogynecol J 31:1063–1089. https://doi.org/10.1007/s00192-020-04314-4
14. Jnr Bokolo A (2020) Use of telemedicine and virtual care for re-mote treatment in response to COVID-19 pandemic. JMed Syst 44:132. https://doi.org/10.1007/s10916-020-01596-5
15. Doshi A, Dressen JR, SFHM JCS (2020) Keep calm and log on:telemedicine for COVID-19 pandemic response. 15(5):302–304
16. Vidal-Alaball J, Acosta-Roja R, Pastor N, Sanchez U, Morrison D,Narejos S et al (2020) Telemedicine in the face of the COVID-19pandemic. Aten Primaria 52:418–422
17. Aslani N, Garavand A (2020) The role of telemedicine to controlCoVID-19. Arch Clin Infect Dis. https://doi.org/10.5812/archcid.102949
18. Wosik J, FudimM, Cameron B, Gellad ZF, Cho A, Phinney D et al(2020) Telehealth transformation: COVID-19 and the rise of virtualcare. J Am Med Inform Assoc 27:957–962
19. Song X, Liu X, Wang C (2020) The role of telemedicine during theCOVID-19 epidemic in China—experience from Shandong prov-ince. Crit Care 24(1):178. https://doi.org/10.1186/s13054-020-02884-9
20. Christianson J, Christianson E (2020) White paper: using telehealthin the emergency department to minimize risk to health care pro-viders and conserve resources during the COVID-19 response.InDoc, PA:1–4
21. Khairat S, Meng C, Xu Y, Edson B, Gianforcaro R (2020)Interpreting COVID-19 and virtual care trends: cohort study.JMIR Public Health Surveill 6(2):e18811
22. Kapoor A, Guha S, Das MK, Goswami KC, Yadav R (2020)Digital healthcare: the only solution for better healthcare duringCOVID-19 pandemic? Indian Heart J 72:61–64
9Ir J Med Sci (2021) 190:1–10

23. Torous J, Myrick KJ, Rauseo-Ricupero N, Firth J (2020) Digitalmental health and COVID-19: using technology today to acceleratethe curve on access and quality tomorrow. JMIR Ment Health 7(3):e18848
24. Banskota S, HealyM, Goldberg EM (2020) 15 smartphone apps forolder adults to use while in isolation during the COVID-19 pan-demic. West J Emerg Med: Integrating Emergency Care withPopulation Health. 21(3):514–525. https://doi.org/10.5811/westjem.2020.4.47372
25. Keesara S, Jonas A, SchulmanK (2020) Covid-19 and health care’sdigital revolution. N Engl J Med 382:e82
26. Zhou X, Snoswell CL, Harding LE, Bambling M, Edirippulige S,Bai X, Smith AC (2020) The role of telehealth in reducing themental health burden from COVID-19. Telemed J E Health 26(4):377–379
27. Pappot N, Taarnhøj GA, Pappot H (2020) Telemedicine and e-health solutions for COVID-19: patients’ perspective. Telemed JE Health 26(7):1–3. https://doi.org/10.1089/tmj.2020.0099
28. Smith AC, Thomas E, Snoswell CL et al (2020) Telehealth forglobal emergencies: implications for coronavirus disease 2019(COVID-19). J Telemed Telecare 26(5):309–313. https://doi.org/10.1177/1357633X20916567
29. Gutierrez J, Kuperman E, Kaboli PJ (2020) Using telehealth as atool for rural hospitals in the COVID-19 pandemic response. JRural Health. https://doi.org/10.1111/jrh.12443
30. Whaibeh E, Mahmoud H, Naal H (2020) Telemental health in thecontext of a pandemic: the COVID-19 experience. Curr TreatOptions Psychiatry 7:198–202. https://doi.org/10.1007/s40501-020-00210-2
31. Humphreys J, Schoenherr L, Elia G et al (2020) Rapid implemen-tation of inpatient telepalliative medicine consultations duringCOVID-19 pandemic. J Pain Symptom Manag 60(1):54–59.https://doi.org/10.1016/j.jpainsymman.2020.04.001
32. Cho H, Ippolito D, Yu YW (2020) Contact tracing mobile apps forCOVID-19: privacy considerations and related trade-offs. https://arxiv.org/pdf/2003.11511.pdf
33. Sodhi M (2020) Telehealth policies impacting federally qualifiedhealth centers (FQHCs) in face of COVID-19. J Rural Health.https://doi.org/10.1111/jrh.12445
34. Mann DM, Chen J, Chunara R et al (2020) COVID-19 transformshealth care through telemedicine: evidence from the field. J AmMed Inform Assoc. https://doi.org/10.1093/jamia/ocaa072
35. Machado RA, de Souza NL, Oliveira RM et al (2020) Social mediaand telemedicine for oral diagnosis and counselling in the COVID-19 Era. Oral Oncol. https://doi.org/10.1016/j.oraloncology.2020.104685
Publisher’s note Springer Nature remains neutral with regard to jurisdic-tional claims in published maps and institutional affiliations.
10 Ir J Med Sci (2021) 190:1–10






![Exploring The Cloud – A Global Study Of Government’S Adoption Of Cloud[1]](https://static.fdocuments.us/doc/165x107/5465d073af79596f338b4edf/exploring-the-cloud-a-global-study-of-governments-adoption-of-cloud1.jpg)










![Alliance for Telemedicine Registry and Evaluation · Alliance for Telemedicine Registry and Evaluation 3 while adoption was tele consultation was limited in India [3]. Post (and with](https://static.fdocuments.us/doc/165x107/5ffde34d0fb9982ca04d860c/alliance-for-telemedicine-registry-and-evaluation-alliance-for-telemedicine-registry.jpg)