
Exploring and validating alternative methods of using ... · Exploring and validating alternative...
12
Exploring and validating alternative methods of using multiple databases to answer complex longitudinal research questions Is linking databases the only answer? ISPOR 19th Annual International Meeting June 3, 2014 Montreal, QC, Canada Presenters • Rolin Wade, RPh, MS − Principal, RWE/HEOR, IMS Health − US Practice Lead, Retrospective Database Research − Plymouth Meeting, NJ USA • David Macarios, MBA (HSM) − Vice President, HEOR, Lifecell Corporation − Bridgewater, NJ USA 2
Transcript of Exploring and validating alternative methods of using ... · Exploring and validating alternative...

Exploring and validating alternative methods of using multiple databases to answer complex longitudinal research questions
Is linking databases the only answer?
ISPOR 19th Annual International Meeting June 3, 2014 Montreal, QC, Canada
Presenters
• Rolin Wade, RPh, MS
− Principal, RWE/HEOR, IMS Health
− US Practice Lead, Retrospective Database Research
− Plymouth Meeting, NJ USA
• David Macarios, MBA (HSM)
− Vice President, HEOR, Lifecell Corporation
− Bridgewater, NJ USA
2

Background
• HEOR requires evaluating a longitudinal view of patient risk factors, details regarding medical interventions, and accurate cost/payment information
• Complete granular detail has been unavailable or inaccessible except for tedious and expensive chart abstraction, patient and provider interviews etc.
• These methods were not practical and had many limitations
• Our research is focused on implementing and validating methods of building a robust longitudinal view of the patient using multiple sources of retrospective data
3
“It’s Just A Hernia”
Hernia surgery gets no respect !!
3.2 billion $ in 2011 spent on ventral “hernias” in USA1
This does not include loss of work and disability issues
1 Poulose BK, Beck WC, Phillips SE, et al. The Chosen Few: Disproportionate Resource Use in Ventral Hernia Repair. Am Surg. 2013 Aug;79(8):815-8.

The Medical Challenge: Understanding A Subset Of
All Ventral Hernia Repairs
Over 335,000 ventral hernia repairs (VHR)
are performed in the US each year
• ~ 15% are considered ‘complex’
patients
The Complex Abdominal Wall Repair (CAWR)
procedure is complicated and often includes:
• A large defect size, Multiple
comorbidities, Prolonged OR time,
Concomitant procedures, Component
separation to restore ab wall function
• 5th most common procedure listed
in surgeons applying for board
recertification
≠
≠
No Consensus On Optimal Method Or Type Of Mesh In Specific Cases
Both Are Coded As “Umbilical Hernias!!”
Breuing, K., Butler, C., Ferzoco, S., et al . Surgery 2010
Impaired wound healing
• Previous wound infection
• Stoma present
• Violation of the gastrointestinal tract
Grade 3 Potentially
Contaminated
Grade 2 Co-Morbid
• Smoker
• Obese
• Diabetic
• Immunosuppressed
• COPD
Grade 1 Low Risk
• Low risk of
complications
• No history of wound infection
Grade 4 Infected
Increased risk of wound breakdown
Risk or presence of infection
• Infected mesh
• Septic dehiscence
There Is No Agreed Upon System To Characterize Patients

The Analytic Challenge: Insurance Claims Data Inadequate To Answer Analytic Challenge
• Cohort of interest not easily identifiable in claims records
− Claims records can approximate case complexity, but cannot accurately capture
• What technique of repair
• open, lap, CS, etc
• When is mesh needed ?
• Where to place the mesh ?
• What type of mesh ? Biologic vs synthetic mesh ? Permanent vs absorbable ?
– Can you even identify the type of mesh consistently in claims records?
• What is optimal post op management ?
• What to do with infected mesh ?
• Timing of repair following removal infected mesh ?
• Do all hernias really need to be repaired ?
• Is “watchful waiting” ok for some ventral hernias ?
• Is hernia repair economically feasible for hospitals ?
Making the Correct Decision !!
• Right operation
• Right patient
• Right timing
• Right mesh Hernia Surgery Decision Making
The Current Fiscal Environment Demands We Guide Administers and Surgeons Regarding Choices in Optimal Patient Care

$0
$10,000
$20,000
$30,000
$40,000
$50,000
$60,000
$70,000
$80,000
May-12 May - June 2012 Sep-12 Oct-12 Apr-13
Cost per event Cumulative hospital cost
Case example provided by George DeNoto III, MD, FACS, Chief, Division of General Surgery at St. Francis Hospital, Roslyn, NY & Clinical Associate Professor of Surgery, Hofstra North Shore-Long Island Jewish School of Medicine.
Index event: 46-year-old male
undergoes primary
epigastric hernia repair with
composite mesh
Composite mesh explanted and repaired
with lightweight synthetic mesh in the
retrorectus plane Post op infection managed outpatient
Infected lightweight
synthetic mesh explanted
Patient develops a postoperative
enteroccocal wound infection with chronic wound
drainage
Understand Longterm Consequences Critical, Starting With the Index Inpatient Surgery
3. Reynolds D, Davenport DL, Korosec RL, Roth JS. Financial Implications of Ventral Hernia Repair: A Hospital Cost Analysis. J Gastrointest Surg. 2012 Sep 11.
Illustrative example: Total cost of care is ~$74K due to multiple surgeries of increasing
complexity (excludes QoL and Productivity)1, 2, 3
The Research Question
• Primary Objective: What is the overall cost of care in patients with ventral hernia repair using surgical mesh implant?
• Are there differences in outcomes based on the type of mesh used?
• How should patient risk factors influence choices?
10
• What is the prevalence of post-operative complications and their costs?
• Should we focus only on Grade 3 and 4 hernia repair (potentially contaminated or infected)

Previous Research on this Subject
• Used open source OP claims and hospital charge master data
• 4332 patients (grade 2=2875, Grade 3=171, grade 4=488)
• Compared synthetic mesh and biologic implant
• Tracked complication rates through 90 days post-discharge
• Overall complication rates and costs were higher with biologic implant
• Results were mixed in grade 4 patients
• Limitations: grading based on billing codes, unknown missing data, charge versus cost estimates, long-term complications unknown
11
Lifecell/IMS (data on file, 2012)
Previous Research on this Subject
• Use of a very large US claims data set
• 744 patients with grade 3 (n=538) or 4 (n=206) hernia repair
• Compared primary repair, synthetic mesh and xenograft
• Complication rates
− Grade 3: Synthetic mesh > primary repair > xenograft
− Grade 4: Xenograft = primary repair
• Overall costs (hospital perspective)
− Grade 3: $33K – 36K, NS difference between groups
− Grade 4: $46K - $50K, NS difference between groups
• Limitations: grading approximated, specific product unknown, specifics of surgery unknown, uncertain coding of complications, no visibility to IP services used
12
DeNoto et.al. Open Access Surgery 2013:6 23-32
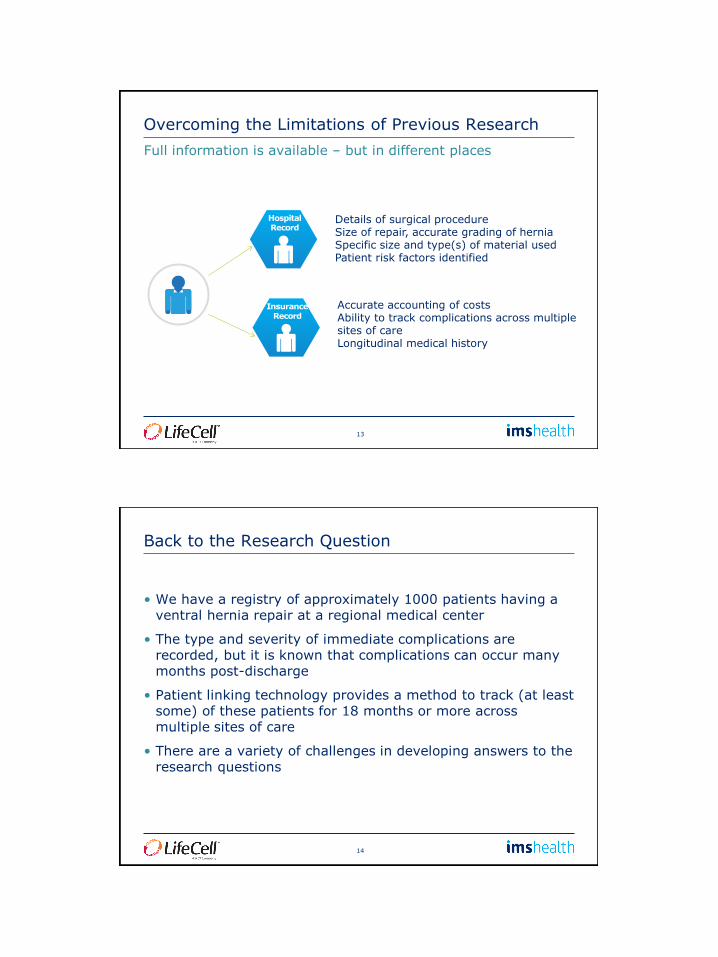
Overcoming the Limitations of Previous Research
13
Full information is available – but in different places
Insurance Record
Hospital Record
Details of surgical procedure Size of repair, accurate grading of hernia Specific size and type(s) of material used Patient risk factors identified
Accurate accounting of costs Ability to track complications across multiple sites of care Longitudinal medical history
Back to the Research Question
• We have a registry of approximately 1000 patients having a ventral hernia repair at a regional medical center
• The type and severity of immediate complications are recorded, but it is known that complications can occur many months post-discharge
• Patient linking technology provides a method to track (at least some) of these patients for 18 months or more across multiple sites of care
• There are a variety of challenges in developing answers to the research questions
14

Approach #1 – Direct Patient Linking
• Synthetic identifiers will be created for the 1000 patients in the ventral hernia repair registry
• These identifiers can be linked to a variety of longitudinal data assets
− PharMetrics Plus Administrative Claims database
− IMS Patient-centric data warehouse (OP claims, Rx claims, Charge master)
− Social Security Death Index
• A longitudinal analysis of the linked patients will be conducted
− Pre-surgical history
− Resource utilization and costs
− Relevant medical events (infection, bowel obstruction, re-admission)
− death
15
Data Linking Technology
16
MULTIPLE CHANNELS
Each interaction is captured at the de-identified patient level in the same manner across channels
PATIENT PROFILE
A singular view of the patient experience is represented
DE-IDENTIFICATION
All interactions are combined upon the common algorithm in place across channels
Patient XYZQJL
HIPAA-compliant De-identification
Process
PATIENT
A single patient interacts with the healthcare system across multiple entry points
Health plan claims
Consumer OTC
medication
Consumer demographic & behavioral
Hospital
EMR
Lab data
Customer data
Open sourced med and Rx
claims

IMS utilizes a patented HIPAA compliant algorithm for linking patients across data sources
17
Trusted Third Party
Name DOB ZIP Data
Source Data with PHI from Data Supplier
IMS Encryption
Engine
Pt XYZQJL Data
Pt XYZQJL Data
source 3
Pt XYZQJL Data
Source 1 Pt XYZQJL Data
source 2
De-identified patient data undergo a deterministic matching process to be
assigned to a unique and persistent IMS Patient ID
IMS and its technology partners deploy proprietary
encryption tools to de-identify patient data at the
source
1
2
Patient data with persistent IMS Patient ID’s are
available from across sources for use in IMS products and services to inform
patient-centric insights across
“linkable” IMS data assets
3
Issued and pending patents: System and Method for Generating De-Identified Health Care Data (US Patents 6,732,113/7,376,677), Anonymously Linking a Plurality of Data Records, (US Patent 6,397,224).
Approach #2 – Population Matching
• The 1000 registry patients will be characterized by:
− Age, Gender, Geography, Payer type
− Index quarter of ventral incisional hernia repair
− Index procedure codes, Secondary diagnoses for hernia repair
− Primary/Secondary diagnosis at admission/discharge diagnosis
− Length of index hospital stay, total allowed costs ($2500 increment)
• These patients will then be matched (versus linked) to patients in the longitudinal claims database
• A longitudinal analysis will be conducted as specified in Approach #1
• Can matching be a practical surrogate for linking?
18

Comparison of the Methods
• Patients from one database are directly linked to a 2nd database
• Expected match rate is low (5-20%)
• Sample size is small and may not be generalizable
• Outcome measures can be directly associated with clinical specifics
• Can provide a validation reference for alternative methods
• Patients in the 2nd database are chosen on multiple characteristics
• Matching elements are limited to administrative elements
• The sample size is large and may be generalizable
• Some outcome measures (re-admission, death) may statistically approximate the linked population outcomes
19
Linking Matching
What Can We Learn in Further Analysis?
• What outcome measures can be credibly estimated when using a matched population?
• How influential are un-matchable confounders (such as hernia size) on our outcome estimates?
• Does using a combination of techniques to estimate outcomes provide a more robust answer or just add confusion?
• How many statistical consults will we need to satisfy the peer-reviewers ????
20
Matched Population
Linked Population
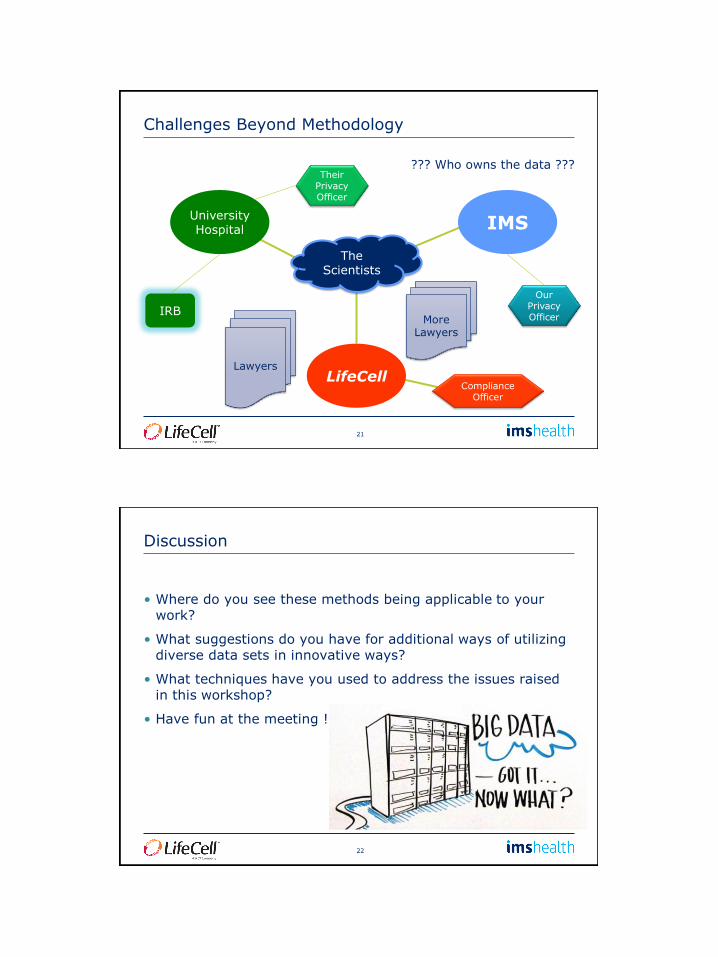
Challenges Beyond Methodology
21
The Scientists
University Hospital
LifeCell
IMS
Our Privacy Officer
Their Privacy Officer
Lawyers
IRB More
Lawyers
??? Who owns the data ???
Compliance Officer
Discussion
• Where do you see these methods being applicable to your work?
• What suggestions do you have for additional ways of utilizing diverse data sets in innovative ways?
• What techniques have you used to address the issues raised in this workshop?
• Have fun at the meeting !
22

Contact Information
•Rolin Wade
•David Macarios
23


















