Expert Review ajog - endometriozisdernegi.org€¦ · HealthSystem and Pritzker School of Medicine...
11
Nonsteroidal antiinflammatory drug resistance in dysmenorrhea: epidemiology, causes, and treatment Q6 Folabomi A. Oladosu, PhD; Frank F. Tu, MD, MPH; Kevin M. Hellman, PhD Q1 Introduction The scope of the clinical problem of menstrual pain was effectively commu- nicated by former First Lady Michelle Obama, when she tweeted, “Why are girls still missing so many days of school because of their menstrual cycles?” 1 Too many women hide this personal stigma, and experience a physical and psycho- logical burden of frequent, severely painful cramps occurring over several days every month, persisting for decades. The transcultural impact of this problem was highlighted when Chinese Olympic medalist Fu Yuanhui acknowledged that menstrual pain affected her Olympic swimming performance. 2 The etiology of menstrual pain remains inadequately characterized, 3 and this limited scientific understanding hinders adequate treat- ment for women who are unresponsive to first-line options including nonste- roidal antiinflammatory drug (NSAID) therapy. To optimize the management of menstrual pain, further studies of its pathophysiology are needed. This review summarizes current scientific knowledge and associated critical gaps in menstrual pain unresponsive to NSAIDs (Figure 1 ½F1 ). Epidemiology of NSAID-resistant dysmenorrhea Menstrual pain, also known as dysmen- orrhea, is common and affects nearly half of reproductive-age girls Q2 and women. 4-6 Before the advent of NSAID therapy, it was observed that 10% of high school girls in Los Angeles missed classes because of dysmenorrhea. 7 The devel- opment of NSAIDs in 1969 heralded a new era of pain management, and over- the-counter availability of this medica- tion class in 1983 held the promise of resolving dysmenorrhea for many women. Indeed, for most women, NSAIDs are effective for treating dysmenorrhea as demonstrated by a meta-analysis of 35 randomized controlled trials. 8 However, dysmenor- rhea still causes 10-20% of US female high school students to miss class during their menses. 9,10 This phenomenon is also seen internationally, 11 with men- strual pain-induced absenteeism occur- ring at similar or greater rates. 12-14 Further, a review of 51 different clinical trials found that 18% of women report minimal or no relief of menstrual pain with NSAIDs. 15 This failure to relieve pain suggests multiple pathological mechanisms may contribute to treat- ment unresponsiveness. Clarifying these mechanisms is an obvious critical need in gynecological research. What causes menstrual pain? Preclinical research studies suggest prostaglandin (PG)-dependent mecha- nisms drive dysmenorrhea in a majority of women (reviewed by Maia et al 16 in 2005). The start of menstruation is marked by the simultaneous decrease in circulating progesterone and estradiol, initiating increased transcription of endometrial collagenases, matrix metal- loproteinases (MMPs), and inflamma- tory cytokines (Figure 2 ½F2 ). Up-regulated MMPs specifically target and break down endometrial tissue, freeing phos- pholipids from the cellular membrane. Uterine phospholipases convert available phospholipids to arachidonic acid, which is then synthesized into PG, prostacyclins, and thromboxane-2a via cyclooxygenase (COX)-1 and COX-2. Notably, COX-2 expression is highest during menses. 16 Although it is unclear whether increased COX-2 expression occurs in dysmenorrhea, the end prod- ucts PGE 2 and PGF 2a are elevated in the menstrual effluent in dysmenorrheic From the Department of Obstetrics and Gynecology, NorthShore University HealthSystem and Pritzker School of Medicine University of Chicago, Evanston, IL. Received May 29, 2017; revised Aug. 14, 2017; accepted Aug. 31, 2017. supported by Eunice Kennedy Shriver National Institute of Child Health and Human Development HD081709, National Institute of Diabetes and Digestive and Kidney Diseases DK100368, and NorthShore University HealthSystem. F.F.T. was a consultant for AbbVie Pharmaceuticals. The remaining authors report no conflict of interest. Corresponding author: Kevin M. Hellman, PhD. [email protected] 0002-9378/$36.00 ª 2017 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.ajog.2017.08.108 Although nonsteroidal antiinflammatory drugs can alleviate menstrual pain, about 18% of women with dysmenorrhea are unresponsive, leaving them and their physicians to pursue less well-studied strategies. The goal of this review is to provide a background for treating menstrual pain when first-line options fail. Research on menstrual pain and failure of similar drugs in the antiplatelet category suggested potential mechanisms underlying nonsteroidal antiinflammatory drug resistance. Based on these mechanisms, alternative options may be helpful for refractory cases. This review also identifies key pathways in need of further study to optimize menstrual pain treatment. Key words: adenomyosis, endometriosis, menstrual pain, nonsteroidal antiinflammatory drugs, oral contraception, primary dysmenorrhea, secondary dysmenorrhea MONTH 2017 American Journal of Obstetrics & Gynecology 1 Expert Review ajog.org REV 5.5.0 DTD ĸ YMOB11822_proof ĸ 15 September 2017 ĸ 7:05 pm ĸ ce 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110
Transcript of Expert Review ajog - endometriozisdernegi.org€¦ · HealthSystem and Pritzker School of Medicine...

Q6Q1
Expert Review ajog.org
12345678910111213141516171819202122232425262728293031323334353637383940414243444546474849505152535455
56575859606162
Nonsteroidal antiinflammatory drug resistancein dysmenorrhea: epidemiology, causes,and treatmentFolabomi A. Oladosu, PhD; Frank F. Tu, MD, MPH; Kevin M. Hellman, PhD
½F1�
2
Although nonsteroidal antiinflammatory drugs can alleviate menstrual pain, about 18% ofwomen with dysmenorrhea are unresponsive, leaving them and their physicians topursue less well-studied strategies. The goal of this review is to provide a background fortreating menstrual pain when first-line options fail. Research on menstrual pain andfailure of similar drugs in the antiplatelet category suggested potential mechanismsunderlying nonsteroidal antiinflammatory drug resistance. Based on these mechanisms,alternative options may be helpful for refractory cases. This review also identifies keypathways in need of further study to optimize menstrual pain treatment.
Key words: adenomyosis, endometriosis, menstrual pain, nonsteroidal antiinflammatorydrugs, oral contraception, primary dysmenorrhea, secondary dysmenorrhea
636465666768697071727374757677787980818283848586878889
IntroductionThe scope of the clinical problem ofmenstrual pain was effectively commu-nicated by former First Lady MichelleObama, when she tweeted, “Why aregirls still missing so many days of schoolbecause of their menstrual cycles?”1 Toomany women hide this personal stigma,and experience a physical and psycho-logical burden of frequent, severelypainful cramps occurring over severaldays every month, persisting for decades.The transcultural impact of this problemwas highlighted when Chinese Olympicmedalist Fu Yuanhui acknowledged thatmenstrual pain affected her Olympicswimming performance.2 The etiologyof menstrual pain remains inadequatelycharacterized,3 and this limited scientificunderstanding hinders adequate treat-ment for women who are unresponsiveto first-line options including nonste-roidal antiinflammatory drug (NSAID)therapy. To optimize the managementof menstrual pain, further studies ofits pathophysiology are needed. This
½F2�
From the Department of Obstetrics andGynecology, NorthShore UniversityHealthSystem and Pritzker School of MedicineUniversity of Chicago, Evanston, IL.
Received May 29, 2017; revised Aug. 14, 2017;accepted Aug. 31, 2017.
supported by Eunice Kennedy Shriver NationalInstitute of Child Health and HumanDevelopment HD081709, National Institute ofDiabetes and Digestive and Kidney DiseasesDK100368, and NorthShore UniversityHealthSystem.
F.F.T. was a consultant for AbbViePharmaceuticals. The remaining authors reportno conflict of interest.
Corresponding author: Kevin M. Hellman, [email protected]
0002-9378/$36.00ª 2017 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.ajog.2017.08.108
REV 5.5.0 DTD
90919293949596979899100101102103104105106107108109110
review summarizes current scientificknowledge and associated critical gaps inmenstrual pain unresponsive to NSAIDs(Figure 1).
Epidemiology of NSAID-resistantdysmenorrheaMenstrual pain, also known as dysmen-orrhea, is common and affects nearlyhalf of reproductive-age girls andwomen.4-6 Before the advent of NSAIDtherapy, it was observed that 10% of highschool girls in Los Angeles missed classesbecause of dysmenorrhea.7 The devel-opment of NSAIDs in 1969 heralded anew era of pain management, and over-the-counter availability of this medica-tion class in 1983 held the promise ofresolving dysmenorrhea for manywomen. Indeed, for most women,NSAIDs are effective for treatingdysmenorrhea as demonstrated by ameta-analysis of 35 randomizedcontrolled trials.8 However, dysmenor-rhea still causes 10-20% of US femalehigh school students to miss class duringtheir menses.9,10 This phenomenon isalso seen internationally,11 with men-strual pain-induced absenteeism occur-ring at similar or greater rates.12-14
Further, a review of 51 different clinicaltrials found that 18% of women reportminimal or no relief of menstrual pain
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
Q
with NSAIDs.15 This failure to relievepain suggests multiple pathologicalmechanisms may contribute to treat-ment unresponsiveness. Clarifying thesemechanisms is an obvious critical needin gynecological research.
What causes menstrual pain?Preclinical research studies suggestprostaglandin (PG)-dependent mecha-nisms drive dysmenorrhea in a majorityof women (reviewed by Maia et al16 in2005). The start of menstruation ismarked by the simultaneous decrease incirculating progesterone and estradiol,initiating increased transcription ofendometrial collagenases, matrix metal-loproteinases (MMPs), and inflamma-tory cytokines (Figure 2). Up-regulatedMMPs specifically target and breakdown endometrial tissue, freeing phos-pholipids from the cellular membrane.Uterine phospholipases convert availablephospholipids to arachidonic acid,which is then synthesized into PG,prostacyclins, and thromboxane-2a viacyclooxygenase (COX)-1 and COX-2.Notably, COX-2 expression is highestduring menses.16 Although it is unclearwhether increased COX-2 expressionoccurs in dysmenorrhea, the end prod-ucts PGE2 and PGF2a are elevated in themenstrual effluent in dysmenorrheic
American Journal of Obstetrics & Gynecology 1
7:05 pm � ce

½T1�
print&web4C=FPO
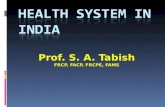
FIGURE 1---
Q4
Proposed pathway examining nonsteroidal antiinflammatory drug (NSAID)-resistant dysmenorrhea.
Many complex mechanisms contribute to development of NSAID-resistant dysmenorrhea. NSAIDs
normally reduce menstrual pain via suppression of peripheral and systemic prostaglandins (PG) and
corresponding downstream effects (shown in black). Elements on left branch highlight uterine
mechanisms while right branch highlights central and peripheral neural mechanisms. Various
physiological factors, ranging from poor medical adherence to involvement of PG-independent
cascades, may disrupt NSAID efficacy to ameliorate menstrual pain and promote NSAID resis-
tance (shown in red).
COX, cyclooxygenase; CYP, cytochrome P450.
Oladosu. NSAID-resistant dysmenorrhea. Am J Obstet Gynecol 2017.
Expert Review ajog.org
111112113114115116117118119120121122123124125126127128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160161162163164165166
167168169170171172173174175176177178179180181182183184185186187188189190191192193194195196197198199200201202203204205206207208209210211212213214215216217218219220221222
women when compared to healthycontrols.17,18
The identification of elevated PGE2and PGF2a in dysmenorrhea supportedthe strategy of inhibiting COX-2 with
2 American Journal of Obstetrics & Gynecology M
REV 5.5.0 DTD
NSAIDs to treat menstrual pain.Nonspecific NSAIDs (Table) bind toboth COX-1 and COX-2 to inhibit PGsynthesis. More selective NSAIDs knownas COX-2 inhibitors alleviate menstrual
ONTH 2017
� YMOB11822_proof � 15 September 2017 �
pain by specifically inhibiting COX-2activity. Unlike COX-1, which is consti-tutively expressed, COX-2 is up-regulated by stimuli associated withinflammation19 and during progester-one withdrawal,20,21 thus making COX-2 inhibitors an appropriate alternativeto nonspecific NSAIDs.
Although it is possible that PGs couldexcite nociceptors and cause pain, it isbelieved that PGs indirectly causecramping pain by stimulating uterinecontractility.22 Preclinically, we recentlyconfirmed that PGF2a administrationincreases uterine contractility and elicitsvisceral pain.23 Conversely, drugs thatinhibit PG synthesis, such as ibuprofen24
and naproxen,25 reduce uterine contrac-tility in dysmenorrheic women. Thesefindings suggest that PGs increase uterinecontractility and produce cramping painvia temporary elevations in uterine pres-sure.22 Since not all women withdysmenorrhea have alterations in uterinepressure,26 other mechanisms mightcontribute to menstrual pain. Forexample, impaired uterine perfusion wasobserved in dysmenorrhea27; ischemiamay also cause cramping pain. In ourmousemodel of dysmenorrhea, impaireduterine perfusion and hypoxemia alsooccurred.23 Although these studiescollectively suggest physiological mecha-nisms underlying dysmenorrhea, they failto clarify why some women do notrespond to NSAIDs.
Anatomical factorsA subset of women with dysmenorrhea,particularly those with delayed presen-tation after menarche, may harborseparate contributing anatomical factorssuch as endometriosis, leiomyoma, oradenomyosis; these cases are examples of“secondary dysmenorrhea” that couldunderlie NSAID resistance. Undoubt-edly, surgical interventions for thesestructural issues address dysmenorrhea.For example, in a meta-analysis, lapa-roscopic excision of endometriosis wasshown to reduce menstrual pain.28 Themolecular contributions of anatomicalfactors to secondary dysmenorrhea arelimited. Immunohistological studiesinvestigating endometriosis demon-strated that lesions have increased
7:05 pm � ce

print&web4C=FPO
FIGURE 2---
Production of prostaglandins (PG) via onset of menstruation. Decreased progesterone and estrogen
levels at end of luteal phase initiate cascade that results in breakdown of endometrial tissues, release
of cellular phospholipids, and subsequent production of PG.
COX, cyclooxygenase; MMP, matrix metalloproteinases; NSAID, nonsteroidal antiinflammatory drug; TX, thromboxane.
Oladosu. NSAID-resistant dysmenorrhea. Am J Obstet Gynecol 2017.
ajog.org Expert Review
223224225226227228229230231232233234235236237238239240241242243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278
279280281282283284285286287288289290291292293294295296297298299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334
COX-2 expression,29 which led to cor-responding increased PG30 and aroma-tase activity.31 Ectopic endometriumfrom adenomyosis patients expressedincreased levels of transient receptorpotential vanilloid 1 (a pain signalingprotein) and oxytocin receptor.32 Geneexpression of myometrial regulatorsmyostatin and MMP14 from leiomyomabiopsies were positively correlated tosevere dysmenorrhea.33 These in vitrostudies provide insight into mechanismsthat promote secondary dysmenorrhea,but more research is needed to unmaskthe complex pathophysiology associatedwith these anatomical factors.
The causal contribution of anatomicalfactors to dysmenorrhea, particularlythose that exhibit NSAID unrespon-siveness, is unclear. A meta-analysisestimated as many as 29% of dysmen-orrheic women may have moderate tosevere endometriosis.34 However, sincemany women do not undergo laparo-scopic evaluation, it is difficult to identifythe proportion of women with NSAID-resistant dysmenorrhea who have endo-metriosis. A small clinical study foundthat among 31 women with NSAID-resistant dysmenorrhea, 35% hadendometriosis.35 In a larger study (n ¼654), 25% of participants with NSAID-resistant dysmenorrhea had ultrasoundor magnetic resonance imaging sugges-tive of endometriosis.36 Conversely, it isimportant to note that dysmenorrheasymptoms are nonspecific for endome-triosis,37 and NSAIDs can be effective inrelieving some cases of menstrual pain inwomen with endometriosis.38,39 In oneobservational study of leiomyomas, 70%of women with fibroids used NSAIDsand 51% reported a reduction in symp-toms.40 It is uncertain whether NSAIDsare useful for adenomyosis.41 Since it isunknown whether anatomical factorscontribute to NSAID unresponsiveness,further research is needed to determinewhether treatment strategies targetinganatomical factors are sufficient foraddressing the causes of NSAID-resistant dysmenorrhea.
Molecular mechanismsTherapeutic alternatives for NSAID-resistant dysmenorrhea will be
REV 5.5.0 DTD
developed quicker once mechanisticcharacterization progresses. NSAIDscollectively elicit nonspecific inhibitionof COX isoforms (Table). COX-1 andCOX-2 are homologous, share 63%identical amino acid sequences and havea similar catalytic binding site.19
Although NSAIDs bind nonselectivelyto both COX isoforms, they vary inisoform-specific inhibition. As seen inthe Table, NSAIDs such as aspirin andibuprofen are more selective for COX-1,while diclofenac preferentially targetsCOX-2.42 Genetic polymorphisms wereshown to disrupt COX-1 inhibition withaspirin. For example, Ulehlova et al43
demonstrated that COX-1 poly-morphism rs10306114 was correlatedwith high platelet aggregation in aspirin-resistant individuals. Although multiplesingle nucleotide polymorphisms(SNPs) that contribute to aspirin resis-tance were identified, they were onlyreplicated in some studies and remain anactive area of research (reviewed by
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
Weng and colleagues44). Although thereare no documented COX poly-morphisms directly associated withNSAID binding, there are several COXSNPs within the promoter regions thatmay alter NSAID efficacy.45 Notably,rs20417 is a SNP in the promoter regionof COX-2 associated with aspirin resis-tance.41 Further research is needed todetermine if the identified SNPs have atranscriptional effect contributing toNSAID-resistant dysmenorrhea.
Another molecular factor that con-tributes to treatment resistance is drugbioavailability. The drug formulationalongside an individual’s metabolicprofile may alter the efficacy of bothantiplatelet and NSAID therapy. Onestudy found a significant relationshipbetween total naproxen serum levels anda reduction in rheumatoid arthritissymptoms46; the range of oral dosagesused (250, 500, and 1500 mg), however,makes it difficult to determine whethervariable absorption significantly
American Journal of Obstetrics & Gynecology 3
7:05 pm � ce

TABLECommonly used nonsteroidalQ5 antiinflammatory drugs andconcentrations that inhibit cyclooxygenase activity in blood
NSAID COX-1 IC50, mmol/L COX-2 IC50, mmol/L COX-1:COX-2 IC50 ratioa
Diclofenac 0.26 0.01 0.05
Aspirin 4.45 13.88 3.12
Ketorolac 0.27 0.18 0.68
Naproxen 32.01 28.19 0.88
Ibuprofen 5.90 9.90 1.69
COX, cyclooxygenase; NSAID, nonsteroidal antiinflammatory drug.
a Ratios >1 indicate drug is more selective for COX-1 and ratios <1 indicate drug is more selective for COX-2.
Oladosu. NSAID-resistant dysmenorrhea. Am J Obstet Gynecol 2017.
Expert Review ajog.org
335336337338339340341342343344345346347348349350351352353354355356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390
391392393394395396397398399400401402403404405406407408409410411412413414415416417418419420421422423424425426427428429430431432433434435436437438439440441442443444445446
contributed to inadequate pain relief.Other mechanisms affecting NSAIDmetabolism could also greatly impactCOX inhibition. Cytochrome P450(CYP) enzymes, specifically CYP1A2,CYP2C8, and CYP2C9, are responsiblefor metabolizing NSAIDs. CYP gain-of-function variants are associated withincreased metabolism, resulting indecreased drug effect.47 For example, theCYP2C9*2/*2 polymorphism was asso-ciated with increased total clearance ofcelecoxib and diclofenac.48 Moreresearch is necessary to determine ifother gain-of-function variants exist andalter NSAID metabolism.
Other molecular contributors toNSAID-resistant dysmenorrheaIn addition to COX and PG-mediatedpathways, other molecular mechanismscould drive NSAID-resistant dysmenor-rhea. Leukotrienes, a class of eicosanoidssynthesized via 5-lipoxygenase, shouldbe considered candidate mediators,49 astheir increased expression is found in theendometrium,50 urine,51 and menstrualeffluent52 of womenwith dysmenorrhea.However, leukotriene receptor inhibi-tion did not successfully alleviatemenstrual pain.53,54 Another potentialCOX-independent mechanism is theplatelet activating factor (PAF) pathway.PAF mediates inflammatory states un-affected by NSAIDs and is elevated in themenstrual effluent of women withNSAID-resistant dysmenorrhea.52 Al-terations in PAF synthesis were found inwomen with endometriosis.55,56 In a
4 American Journal of Obstetrics & Gynecology M
REV 5.5.0 DTD
mouse model, we recently confirmed aPAF receptor agonist is capable ofincreasing uterine hypercontractility andimpairing perfusion, causing uterinehypoxemia and pain.23 The effects onuterine physiology were blocked with aPAF receptor antagonist in our mousemodel, but PAF-targeting treatmentshave not yet been conducted in womenwith dysmenorrhea. Additional researchis needed to elucidate the possible rolesof leukotrienes and PAF in NSAID-resistant dysmenorrhea.
Peripheral and central sensitizationwithin dysmenorrheaThe aforementionedmolecules are readilyimplicated in mechanisms that wouldincrease peripheral nerve sensitivity. PGcan sensitize primary afferents57 via themodulation of tetrodotoxin-resistant so-dium channels58 and transient receptorpotential vanilloid 1 receptors.59 Localneurogenesis is another element of pe-ripheral sensitization, and was demon-strated to contribute to secondarydysmenorrhea.32,60-62 However, the roleof local neurogenesis in NSAID-resistantdysmenorrhea has not yet beendemonstrated.Alternatively, widespread increases in
pain sensitivity known as central sensi-tization could contribute dysmenor-rhea.63 Although it has not beendemonstrated directly, evidence of cen-tral sensitization within dysmenorrheaincludes increased referred pain,64 andheightened experimentally evoked ther-mal, ischemic, muscular, and pressure
ONTH 2017
� YMOB11822_proof � 15 September 2017 �
pain sensitivity.65-68 Dysmenorrheicwomen also exhibit altered gray mattervolume in key cortical regulatory painregions.69-71 Since NSAIDs are notknown to affect central sensitization,72
further research is needed to confirmwhether dysfunctional central sensitiza-tion occurs in NSAID-resistantdysmenorrhea.
Mechanisms driving peripheral orcentral sensitization could also lead toincreased referred pain. In rat models,uterine inflammation led to neurogenicplasma extravasation the abdominalmusculature and adjacent organs.73,74
Although some women with dysmen-orrhea may also have superficialabdominal muscular pain, it is notpredictive of endometriosis.75 Thus, itremains unclear whether women withabdominal muscle cramps duringmenses are more or less likely torespond to NSAIDs.
The importance of medical adherenceMedication adherence likely contributesto NSAID-resistant dysmenorrhea. Aquarter to half of dysmenorrheic womendo not take the correct medication ordosage.10,12 Side effects associated withNSAIDs such as gastrointestinaldiscomfort also limit medication adher-ence.8 Along with medication type,dosage, and side effects, the timing ofNSAID administration may affect effi-cacy. Notably, biochemical analysesdemonstrated that naproxen adminis-tration prior to initiating the COX-2cascade results in nearly complete sup-pression of PG synthesis; attempting toblock synthesis afterwards only pro-duced a gradual and incomplete sup-pression.76 However, a single, butunderpowered trial, comparing men-strual pain relief between prophylactic vsabortive treatment with ibuprofen didnot find a difference.77 It is possible thatdifferences in prophylactic use of nap-roxen and ibuprofen could be due todifferent preferential binding to COX-1and COX-2 (Table). Aside from thistrial, clinical investigators have notsufficiently investigated prophylacticNSAIDs use prior to the onset ofmenses.Although an educational trial regardingprophylaxis did demonstrate increased
7:05 pm � ce

3
ajog.org Expert Review
447448449450451452453454455456457458459460461462463464465466467468469470471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502
503504505506507508509510511512513514515516517518519520521522523524525526527528529530531532533534535536537538539540541542543544545546547548549550551552553554555556557558
patient knowledge, reduction of men-strual pain was not evaluated.78
Treatments for NSAID-resistantdysmenorrheaUntil it can be determined why somewomen with dysmenorrhea are unre-sponsive to NSAIDs, it is essential thatclinicians be aware of adequate alterna-tive treatments. Below, we present a listof candidate pharmacological and non-pharmacological treatments previouslyinvestigated for use in dysmenorrhea.We noted where generic medications areavailable, but insurance coverage for off-label use needs to be considered in termsof patient costs.
Hormone-based treatmentsHormonal treatments, specifically oralcontractive pills (OCPs), are widely usedfor NSAID-resistant dysmenor-rhea.22,79,80 OCPs thin the endometriallining, resulting in reduced COX-2 andPG production.16,81 The bulk of researchexamining OCPs and dysmenorrhea fo-cuses on the effect of different hormonalregimens and combinations. A system-atic review suggested continuous regi-mens are generally more effective atreducing dysmenorrhea symptoms thancyclic regimens.82 Cyclic regimens oftenimprove dysmenorrhea, but studiesrarely found differences betweendifferent hormone combinations.83
Nomegestrol acetate/17b-estradiol wasmore effective in treating menstrual painwhen compared to drospirenone/ethi-nylestradiol oral contraceptive.84 Acomparison of 20 mg ethinyl estradiol/150 mg desogestrel to 20 mg ethinylestradiol/100 mg levonorgestrel sug-gested each improved dysmenorrheasimilarly (23% and 26% of women,respectively).85 Combination OCPs withestradiol valerate/dienogest and ethinylestradiol/levonorgestrel both reducedexperienced time of dysmenorrhea painby 4 days, but significant differencesbetween the regimens were notobserved.86 A systematic reviewconcluded that levonorgestrel-releasingintrauterine devices are as effective asOCPs at alleviating menstrual pain.87 Acritical limitation of the above studies ofcomparing hormonal regimens and
REV 5.5.0 DTD
combinations in primary dysmenorrheais that they have not specifically evalu-ated their utility in NSAID-resistantdysmenorrhea.Hormonal treatments are also used
for women with secondary dysmenor-rhea unresponsive to NSAIDs and whodo not wish to undergo surgery. A ran-domized placebo-controlled trialdemonstrated that OCPs were an effec-tive treatment for secondary dysmenor-rhea associated with endometrosis.88
Continuous OCP regimens improvedysmenorrhea better than cyclical regi-mens after surgery for endometriosis,89
although there are concerns that theestradiol component of OCPs couldexacerbate endometriosis.90 In any case,hormonal suppression is still recom-mended for treatment of dysmenorrheain current consensus guidelines.91
Other studies on secondary dysmenor-rhea treatment focused on gonadotropin-releasing hormone (GnRH) agonists. Arandomized placebo-controlled trialshowed GnRH agonist leuprolide almostcompletely eliminated menstrual pain in44 patients with suspected endometri-osis.92 Although effective in treating sec-ondary dysmenorrhea, GnRH agonist-induced reduction of estrogen promotesbone density loss over time.93,94 PairingGnRH agonists with add-back orreplacement estrogen therapy95-97 or uti-lizing low GnRH agonist dosages98 arecapable of alleviating menstrual painassociated with endometriosis withoutbone loss. The utilization of these drugs isrecommended by the American Societyfor ReproductiveMedicine guidelines onlyafter laparoscopic diagnosis of endome-triosis, given these risks.99 Alongside itsside-effect profile, patients may findmonthly injections of GnRH agonistsinconvenient.A recent review suggested that oral
progestins may be a better first-line op-tion for menstrual and pelvic pain asso-ciated with endometriosis.90 Oralprogestins such as norethindrone acetateand dienogest target the progesteronereceptor, and have regulatory approvalfor endometriosis. A randomizedplacebo-controlled trial demonstratedthat dienogest reduced dysmenorrhea inwomen with endometriosis.100
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
Dienogest was also as effective inreducing menstrual pain whencompared to the GnRH agonist leupro-lide.101 An open-label study foundnorethindrone acetate was as effective atreducing menstrual pain as OCPs.102
Despite their efficacy, it is important toconsider the frequent irregular bleedingassociated with oral progestins.103
Although a meta-analysis supports oralprogestin usage for endometriosis,104 itremains to be investigated whether it isan effective empirical option for NSAID-resistant dysmenorrhea.
Another class of hormonal treatmentused for secondary dysmenorrhea isaromatase inhibitors.105 Aromatase is anenzyme that is expressed in the ovarianfollicle and endometriotic stromal cellsand converts androgens to estrogen.106
Aromatase inhibitors, primarily used toreduce endometriomas107 and my-omas108 in women, may be beneficial forsecondary dysmenorrhea by renderingpatients amenorrheic. Due to concernregarding its effects on bone mineraldensity and other adverse side effects,add-back regimens may be necessary.109
Further research is needed to determineif aromatase inhibitors are Qappropriateof NSAID-resistant dysmenorrhea.
Surgical interventionsAlthough excision of endometriotic le-sions are routinely recommended,99 somesymptomatic patients who do not haveidentified anatomical factors followingdiagnostic surgical evaluation may benefitfrom alternative surgical strategies. Lapa-roscopic uterine nerve ablation (LUNA)and laparoscopic presacral neurectomy(PSN) are 2 surgical interventions histor-ically employed for the treatment of sec-ondary dysmenorrhea (reviewed byProctor and colleagues110 and Latthe andcolleagues111). However, a large multisiterandomized controlled trial conducted byDaniels and colleagues112 determined thatLUNA for chronic pelvic pain did not havea significant effect on dysmenorrhea,regardless of time accrued following sur-gery, and led to this procedure largely be-ing abandoned. However, this trial andmany of the other negative trials did notstudy the effects of LUNA or PSN inNSAID-resistant dysmenorrhea inwomen
American Journal of Obstetrics & Gynecology 5
7:05 pm � ce

Expert Review ajog.org
559560561562563564565566567568569570571572573574575576577578579580581582583584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614
615616617618619620621622623624625626627628629630631632633634635636637638639640641642643644645646647648649650651652653654655656657658659660661662663664665666667668669670
without chronic pelvic pain andendometriosis.
Clinical trials examined the efficacy ofsurgical interventions on primarydysmenorrhea. A double-blinded ran-domized controlled trial of LUNAdemonstrated menstrual pain relief in halfof womenwith primary dysmenorrhea.113
A trial comparing LUNA and LUNA plusPSN reported 69% and 73% of primarydysmenorrhea patients, respectively, hadimprovements inmenstrual pain.114 Chenand Soong115 found that 77% of primarydysmenorrhea patients benefited fromPSN. Although it is unknown whetherthese patients with primary dysmenorrheawere NSAID-resistant, it is quite possiblethat surgery was performed since NSAIDmanagement was not feasible. Thus,further research is needed to clarify theutility of LUNA and PSN as treatments forNSAID-resistant dysmenorrhea, particu-larly in the absence of endometriosis andchronic pelvic pain.
VasodilatorsAnother potential treatment fordysmenorrhea is sildenafil citrate. Sil-denafil specifically blocks cyclic guano-sine monophosphate degradation, thuspromoting smooth muscle relaxation inthe uterus and surrounding bloodvessels.116 In a randomized placebo-controlled trial, sildenafil reduced men-strual pain in women with primarydysmenorrhea.117 Similar to sildenafil,nitric oxide donor drugs also promotevasodilation and myometrial musclerelaxation, and are capable of reducingmenstrual pain. Transdermal nitroglyc-erin or glyceryl trinitrate administrationon the first day of menstruation was suf-ficient to reduce reported menstrual painfor the duration ofmenses.118,119Glyceryltrinitrate andnitroglycerin are available asgeneric medications. A limiting factor ofglyceryl trinitrate and similar vasodilatorsare their side effects that impair tolera-bility including headaches.120 Therefore,the utility of glyceryl trinitrate or othervasodilators for NSAID-resistantdysmenorrhea remains to be determined.
Calcium channel blockersCalcium channel blockers, available asgeneric medications, are primarily
6 American Journal of Obstetrics & Gynecology M
REV 5.5.0 DTD
indicated to treat hypertension byreducing contractility in vascular smoothmuscle and cardiac muscles; they alsoinhibit uterine contractions in pregnantand nonpregnant women.121 Observa-tional studies from the late 1970sdemonstrated that 20-40 mg of calciumchannel blocker nifedipine providedmenstrual pain relief but was associatedwith side effects such as tachycardia,flushing, and headache.122,123 Thesefindings are supported in a controlledtrial showing that 14 of 19 patients ob-tained menstrual pain relief with nifedi-pine.124 Although one research studysuggested efficacy of nifedipine inwomenunresponsive to salicylates,125 futureresearch is needed to establish efficacy forwomen unresponsive to NSAIDs.
Vasopressin and oxytocin receptorantagonistsVasopressin and oxytocin, hormonesknown to stimulate myometrial con-tractions, were also implicated in pri-mary dysmenorrhea.126 There isconflicting evidence, however, on theeffects of vasopressin/oxytocin receptorantagonists on dysmenorrhea. Severalstudies showed that vasopressin-inducedcontractions in dysmenorrheic womenwere reduced by vasopressin/oxytocinreceptor antagonists atosiban127,128 andSR49059.129 In contrast, Valentin andcolleagues130 demonstrated that whencompared to healthy controls, dysmen-orrheic women did not show elevatedlevels of vasopressin and that the intra-venous administration of atosiban didnot attenuate menstrual pain or uterinecontractility. It is important to note thatthe study of Valentin and colleagues130
administered atosiban intravenously af-ter menses onset, while the study ofBrouard et al129 administered SR49059orally at least 4 hours prior to mensesonset. Thus, more evidence is needed toexamine how the time and type ofadministration impacts the efficacy ofvasopressin/oxytocin receptor antago-nists on NSAID-resistant dysmenorrhea.
AntispasmodicsAlthough infrequently used in theUnited States, antispasmodics such ashyoscine butylbromide are used globally
ONTH 2017
� YMOB11822_proof � 15 September 2017 �
to treat abdominal pain, includingmenstrual pain. Hyoscine butylbromideis an anticholinergic drug that targetsmuscarinic receptors to relax smoothmuscle.131 In the United States, a similardrug, hyoscyamine sulfate, is available asa generic medication. Common adverseeffects include dry mouth, constipation,and dizziness. Although it is frequentlyprescribed for visceral spasms, it is notFood and Drug Administration indi-cated for dysmenorrhea.
In a double-blind crossover study,Kemp132 demonstrated that hyoscinebutylbromide was just as effective asaspirin in treating dysmenorrhea.Questionnaire-based studies showedthat women used hyoscine butylbromideto self-treat their dysmenorrhea with asimilar frequency as paracetamol andNSAIDs.133-136 A randomized controlledtrial compared a combination of anantispasmodic (drotaverine) and NSAID(aceclofenac) vs aceclofenac alone, andfound the combination provided supe-rior pain relief for primary dysmenor-rhea.137 Since the addition of drotaverineprovided better pain relief than aceclo-fenac alone, these results support the useof an adjunct antispasmodic to treat re-fractory menstrual pain. These findingsalso suggest that muscle spasm pain indysmenorrhea may contribute toNSAID-resistant pain.
Complementary andnonpharmacological medicaltreatmentsHerbal and dietary supplements wereproposed as alternative treatments fordysmenorrhea. Although many varietiesare currently used to treat dysmenorrhea,inconsistencies between various studiesmake it difficult to determine the efficacyof supplements (reviewed by Pattanittumand colleagues138). Ginger, the mostcommonly reported effective remedy inrandomized controlled trials, onlyreduced pain 1.5 cm on a 10-cm visualanalog scale.139 Thus, more high-qualitytrials demonstrating superior effective-ness of herbal and dietary supplementsare needed to provide viable options forpatients unresponsive to NSAIDs.
Many nonpharmacological remediesfor dysmenorrhea were investigated.
7:05 pm � ce

ajog.org Expert Review
671672673674675676677678679680681682683684685686687688689690691692693694695696697698699700701702703704705706707708709710711712713714715716717718719720721722723724725726
727728729730731732733734735736737738739740741742743744745746747748749750751752753754755756757758759760761762763764765766767768769770771772773774775776777778779780781782
Limited evidence suggests acupunc-ture,140 hot water bottles,141 yoga,142
massage,143 physiotherapy,144 and exer-cise145 may be helpful formenstrual pain,but as with many traditional pharma-ceuticals, effects were not consistentlyrepeated or verified with large random-ized controlled trials. In contrast, trans-cutaneous electrical nerve stimulation(TENS) was shown to reduce menstrualpain in several randomized146-148 andobservational149,150 trials. Since trans-abdominal application of TENS has noeffect on uterine contractility,25 TENSmay affect associated abdominal musclecontractility instead. The role of abdom-inal muscle cramping in dysmenorrheawould be consistent with the utility ofantispasmodic agents described above.The findings obtained with TENS areconsistent with the hypothesis that PG-independent pathways contribute todysmenorrhea, and suggest that theattenuation of these alternative pathwaysmay be effective.
Future directionsAs mentioned above, most studiesinvestigating various treatments fordysmenorrhea have not examined theprevalence of NSAID resistance amongtheir participants. Since dysmenorrheapatients may choose treatments based onpreference rather than previous NSAIDtreatment failure, the overall efficacy oftreatments for NSAID-resistant dysmen-orrhea is unknown. Validated electronictools that track menstrual pain and theuse of rescue medication151 would beuseful for clinical trials. It is likely thatmultiple phenotypes of dysmenorrheaexist reflecting different underlying cau-ses. However, since the abandonment ofclassifying spasmodic and congestivemenstrual pain phenotypes,152 areplacement classification scheme wasnot popularly accepted, and shouldpossibly be reconsidered for the diagnosisfor NSAID-resistant dysmenorrhea.
Pharmacological and gene assays couldhelp identify forms of NSAID-resistantdysmenorrhea that may respond toalternative treatment strategies. A similarresearch strategy revolutionized the un-derstanding of aspirin resistanceobserved in antiplatelet therapy. The
REV 5.5.0 DTD
utilization of ex-vivo assays that detectmechanisms of aspirin resistance led tothe identification of polymorphisms,43,44
absorption impairments,153 or otherfactors that limit drug bioavail-ability.46,154 The translation of these testsfor NSAID-resistant pain could similarlyclarify why some patients are unrespon-sive and provide avenues for adequatetherapeutic development.
ConclusionA significant proportion of women withdysmenorrhea obtain no relief fromNSAIDs. Opportunities to characterizeNSAID resistance with diagnostic testingand enroll women with resistance phe-notypes into novel clinical trials were notpursued. We suggest that future studiesexplore molecular targets that couldexplain resistance and evaluate noveltherapies in these patients. Given thatCOX are implicated in other acute (eg,muscle soreness, inflammation, burnpain) and chronic (eg, migraine,arthritis) pain conditions, studying themechanisms of NSAID resistance has thebroad potential to improve pain relief inpatients with multiple types of refractorypain conditions.Prior treatment algorithms suggest
that symptomatic patients with NSAID-resistant dysmenorrhea who do notrespond to OCPs undergo diagnosticlaparoscopic examination.22,79 Recentconsensus guidelines suggest trials oflevonorgestrel-releasing intrauterine de-vices, with surgery being the last diag-nostic and therapeutic option.91
Although surgery for symptomatic pa-tients is often effective and recom-mended,155-157 some patientsmay be notwilling to undergo surgery. For thesepatients, until research establishes theunderlying mechanisms, some of theoptions described here could partiallyameliorate their unremitting monthlypain. -
ACKNOWLEDGMENT
Wewould like to thank Dr Gerald Gebhart for hisassistance with the manuscript.
REFERENCES
1. @FLOTUS44. “Why are girls still missing somany days of school because of their menstrual
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
cycles?” The First Lady on the barriers to girls’education. April 13, 2016. Available at: https://twitter.com/flotus44/status/720275882040885248. Accessed September 11, 2017.2. Feng E. Uninhibited Chinese swimmer, dis-cussing her period, shatters another barrier.New York Times. Available at: http://www.nytimes.com/2016/08/17/world/asia/china-fu-yuanhui-period-olympics.html?_r¼0. AccessedAug. 16, 2016.3. Berkley KJ, McAllister SL. Don’t dismissdysmenorrhea! Pain 2011;152:1940-1.4. Zondervan KT, Yudkin PL, Vessey MP, et al.The community prevalence of chronic pelvic painin women and associated illness behavior. Br JGen Pract 2001;51:541-7.5. Westling AM, Tu FF, Griffith JW, Hellman KM.The association of dysmenorrhea with noncyclicpelvic pain accounting for psychological factors.Am J Obstet Gynecol 2013;209:422.e1-10.6. Grace VM, ZondervanKT. Chronic pelvic painin New Zealand: prevalence, pain severity, di-agnoses and use of the health services. Aust N ZJ Public Health 2004;28:369-75.7. Goldwasser M. Primary dysmenorrhea: a localmanifestation of a constitutional disease and itstreatment. Cal West Med 1938;48:418-21.8. Marjoribanks J, Ayeleke RO, Farquhar C,ProctorM. Nonsteroidal anti-inflammatory drugsfor dysmenorrhea. CochraneDatabaseSyst Rev2015;7:CD001751.9. Klein JR, Litt IF. Epidemiology of adolescentdysmenorrhea. Pediatrics 1981;68:661-4.10. O’Connell K, Davis AR, Westhoff C. Self-treatment patterns among adolescent girls withdysmenorrhea. J Pediatr Adolesc Gynecol2006;19:285-9.11. McGettiganP,HenryD.Use of non-steroidalanti-inflammatory drugs that elevate cardiovas-cular risk: an examination of sales and essentialmedicines lists in low-,middle-, and high-incomecountries. PLoS Med 2013;10:e1001388.12. Hillen TI, Grbavac SL, Johnston PJ,Straton JA, Keogh JM. Primary dysmenorrhea inyoung Western Australian women: prevalence,impact, and knowledge of treatment. J AdolescHealth 1999;25:40-5.13. Ozerdogan N, Sayiner D, Ayranci U,Unsal A, Giray S. Prevalence and predictors ofdysmenorrhea among students at a university inTurkey. Int J Gynaecol Obstet 2009;107:39-43.14. Ortiz MI. Primary dysmenorrhea amongMexican university students: prevalence, impactand treatment. Eur J Obstet Gynecol ReprodBiol 2010;152:73-7.15. Owen PR. Prostaglandin synthetase in-hibitors in the treatment of primary dysmenor-rhea. Outcome trials reviewed. Am J ObstetGynecol 1984;148:96-103.16. Maia H, Maltez A, Studard E, Zausner B,Athayde C, Coutinho E. Effect of the menstrualcycle and oral contraceptives on cyclooxygenase-2 expression in the endometrium. Gynecol Endo-crinol 2005;21:57-61.17. Chan WY. Prostaglandins and nonsteroidalantiinflammatory drugs in dysmenorrhea. AnnuRev Pharmacol Toxicol 1983;23:131-49.
American Journal of Obstetrics & Gynecology 7
7:05 pm � ce

Expert Review ajog.org
783784785786787788789790791792793794795796797798799800801802803804805806807808809810811812813814815816817818819820821822823824825826827828829830831832833834835836837838
839840841842843844845846847848849850851852853854855856857858859860861862863864865866867868869870871872873874875876877878879880881882883884885886887888889890891892893894
18. Lundström V, Green K. Endogenous levelsof prostaglandin F 2a and its main metabolites inplasma and endometrium of normal anddysmenorrheic women. Am J Obstet Gynecol1978;130:640-6.19. Vane JR, Bakhle YS, Botting RM. Cyclo-oxygenases 1 and 2. Annu Rev PharmacolToxicol 1998;38:97-120.20. Marx SG, Wentz MJ, MacKay LB, et al. Ef-fects of progesterone on iNOS, COX-2, andcollagen expression in the cervix. J HistochemCytochem 2006;54:623-39.21. Tamura I, Taketani T, Lee L, et al. Differentialeffects of progesterone on COX-2 and Mn-SODexpressions are associated with histone acety-lation status of the promoter region in humanendometrial stromal cells. J Clin EndocrinolMetab 2011;96:E1073-82.22. Dawood MY. Primary dysmenorrhea: ad-vances in pathogenesis and management.Obstet Gynecol 2006;108:428-41.23. Hellman KM, Yu PY, Oladosu FA, et al. Theeffects of platelet-activating factor on uterinecontractility, perfusion, hypoxia, and pain inmice. Reprod Sci 2017. 1933719117715122.24. Milsom I, Andersch B. Effect of ibuprofen,naproxen sodium and paracetamol on intra-uterine pressure and menstrual pain indysmenorrhea. Br J Obstet Gynaecol 1984;91:1129-35.25. Milsom I, Hedner N, Mannheimer C.A comparative study of the effect of high-intensity transcutaneous nerve stimulation andoral naproxen on intrauterine pressure andmenstrual pain in patients with primarydysmenorrhea. Am JObstet Gynecol 1994;170:123-9.26. Woodbury RA, Torpin R. Myometrial physi-ology and its relation to pelvic pain. J Am MedAssoc 1947;134:1081-5.27. Dmitrovi�c R. Transvaginal color Dopplerstudy of uterine blood flow in primary dysmen-orrhea. Acta Obstet Gynecol Scand 2000;79:1112-6.28. Pundir J, Omanwa K, Kovoor E, Pundir V,Lancaster G, Barton-Smith P. Laparoscopicexcision versus ablation for endometriosis-associated pain: an updated systematic reviewand meta-analysis. J Minim Invasive Gynecol2017;24:747-56.29. Ota H, Igarashi S, Sasaki M, Tanaka T.Distribution of cyclooxygenase-2 in eutopicand ectopic endometrium in endometriosisand adenomyosis. Hum Reprod 2001;16:561-6.30. TamuraM, Deb S, Sebastian S, Okamura K,Bulun SE. Estrogen up-regulates cyclo-oxygenase-2 via estrogen receptor in humanuterine microvascular endothelial cells. FertilSteril 2004;81:1351-6.31. Noble LS, Takayama K, Zeitoun KM, et al.Prostaglandin E2 stimulates aromatase expres-sion in endometriosis-derived stromal cells.J Clin Endocrinol Metab 1997;82:600-6.32. Nie J, Liu X, Guo S-W. Immunoreactivity ofoxytocin receptor and transient receptor po-tential vanilloid type 1 and its correlation with
8 American Journal of Obstetrics & Gynecology M
REV 5.5.0 DTD
dysmenorrhea in adenomyosis. Am J ObstetGynecol 2010;202:346.e1.33. Tsigkou A, Reis FM, Ciarmela P, et al.Expression levels of myostatin and matrix met-alloproteinase 14 mRNAs in uterine leiomyomaare correlated with dysmenorrhea. Reprod Sci2015;22:1597-602.34. Johannesson U, de Boussard CN, BroddaJansen G, Bohm-Starke N. Evidence of diffusenoxious inhibitory controls (DNIC) elicited by coldnoxious stimulation in patients with provokedvestibulodynia. Pain 2007;130:31-9.35. Stavroulis AI, Saridogan E, Creighton SM,Cutner AS. Laparoscopic treatment of endo-metriosis in teenagers. Eur J Obstet GynecolReprod Biol 2006;125:248-50.36. Ragab A, Shams M, Badawy A,Alsammani MA. Prevalence of endometriosisamong adolescent school girls with severedysmenorrhea: a cross sectional prospectivestudy. Int J Health Sci (Qassim) 2015;9:273-81.37. Vercellini P, Fedele L, Aimi G, Pietropaolo G,Consonni D, Crosignani PG. Association be-tween endometriosis stage, lesion type, patientcharacteristics and severity of pelvic painsymptoms: a multivariate analysis of over 1000patients. Hum Reprod 2007;22:266-71.38. Kauppila A, Puolakka J, Ylikorkala O. Pros-taglandin biosynthesis inhibitors and endome-triosis. Prostaglandins 1979;18:655-61.39. Kauppila A, Rönnberg L. Naproxen sodiumin dysmenorrhea secondary to endometriosis.Obstet Gynecol 1985;65:379-83.40. Jacoby VL, Jacoby A, Learman LA, et al.Use of medical, surgical and complementarytreatments among women with fibroids. Eur JObstet Gynecol Reprod Biol 2014;182:220-5.41. Streuli I, Dubuisson J, Santulli P, deZiegler D, Batteux F, Chapron C. An update onthe pharmacological management of adeno-myosis. Expert Opin Pharmacother 2014;15:2347-60.42. Cryer B, Feldman M. Cyclooxygenase-1and cyclooxygenase-2 selectivity of widely usednonsteroidal anti-inflammatory drugs. Am JMed1998;104:413-21.43. Ulehlova J, Slavik L, Kucerova J, Krcova V,Vaclavik J, Indrak K. Genetic polymorphisms ofplatelet receptors in patients with acutemyocardial infarction and resistance to anti-platelet therapy. Genet Test Mol Biomarkers2014;18:599-604.44. Weng Z, Li X, Li Y, Lin J, Peng F, Niu W.The association of four common poly-morphisms from four candidate genes (COX-1, COX-2, ITGA2B, ITGA2) with aspirininsensitivity: a meta-analysis. PLoS One2013;8:e78093.45. Agúndez JA, Blanca M, Cornejo-García JA,García-Martin E. Pharmacogenomics of cyclo-oxygenases. Pharmacogenomics 2015;16:501-22.46. Hundal O, Rugstad HE, Husby G. Naproxenfree plasma concentrations and unbound frac-tions in patients with osteoarthritis: relation toage, sex, efficacy, and adverse events. TherDrug Monit 1991;13:478-84.
ONTH 2017
� YMOB11822_proof � 15 September 2017 �
47. Zanger UM, Schwab M. Cytochrome P450enzymes in drug metabolism: regulation of geneexpression, enzyme activities, and impact ofgenetic variation. Pharmacol Ther 2013;138:103-41.48. Kirchheiner J, Brockmoller J. Clinical con-sequences of cytochrome P450 2C9 poly-morphisms. Clin Pharmacol Ther 2005;77:1-16.49. Shapiro H, Singer P, Ariel A. Beyond theclassic eicosanoids: Peripherally-actingoxygenated metabolites of polyunsaturatedfatty acids mediate pain associated with tissueinjury and inflammation. Prostaglandins LeukotEssent Fatty Acids 2016;111:45-61.50. Rees MC, DiMarzo V, Tippins JR,Morris HR, Turnbull AC. Leukotriene release byendometrium and myometrium throughout themenstrual cycle in dysmenorrhea and menor-rhagia. J Endocrinol 1987;113:291-5.51. Harel Z, Lilly C, Riggs S, Vaz R, Drazen J.Urinary leukotriene (LT) E(4) in adolescents withdysmenorrhea: a pilot study. J Adolesc Health2000;27:151-4.52. Nigam S, Benedetto C, Zonca M, Leo-Rossberg I, Lübbert H, Hammerstein J.Increased concentrations of eicosanoids andplatelet-activating factor in menstrual blood fromwomen with primary dysmenorrhea. Eicosa-noids 1991;4:137-41.53. Fujiwara H, Konno R, Netsu S, et al. Efficacyof montelukast, a leukotriene receptor antago-nist, for the treatment of dysmenorrhea: aprospective, double-blind, randomized,placebo-controlled study. Eur J Obstet GynecolReprod Biol 2010;148:195-8.54. Harel Z, Riggs S, VazR, FlanaganP, Harel D.The use of the leukotriene receptor antagonistmontelukast (Singulair) in the management ofdysmenorrhea in adolescents. J Pediatr AdolescGynecol 2004;17:183-6.55. Simoni J, Simoni G, Lox CD,McGunegle DE, Feola M. Cytokines and PAFrelease from human monocytes and macro-phages: effect of hemoglobin and contaminants.Artif Cells Blood Substit Immobil Biotechnol1994;22:525-34.56. Hemmings R, Miron P, Falcone T,Bourque J, Lepage N, Langlais J. Platelet-acti-vating factor acetylhydrolase activity in perito-neal fluids of women with endometriosis. ObstetGynecol 1993;81:276-9.57. Davies P, Bailey PJ, Goldenberg MM, Ford-Hutchinson AW. The role of arachidonic acidoxygenation products in pain and inflammation.Ann Rev Immunol 1984;2:335-57.58. England S, Bevan S, Docherty R. PGE2modulates the tetrodotoxin-resistant sodiumcurrent in neonatal rat dorsal root ganglionneurones via the cyclic AMP-protein kinase Acascade. J Physiol 1996;495:429-40.59. Moriyama T, Higashi T, Togashi K, et al.Sensitization of TRPV1 by EP 1 and IP revealsperipheral nociceptive mechanism of prosta-glandins. Mol Pain 2005;1:3.60. Tokushige N, Markham R, Russell P,Fraser I. High density of small nerve fibers in thefunctional layer of the endometrium in women
7:05 pm � ce

ajog.org Expert Review
895896897898899900901902903904905906907908909910911912913914915916917918919920921922923924925926927928929930931932933934935936937938939940941942943944945946947948949950
9519529539549559569579589599609619629639649659669679689699709719729739749759769779789799809819829839849859869879889899909919929939949959969979989991000100110021003100410051006
with endometriosis. Hum Reprod 2005;21:782-7.61. Zhang G, Dmitrieva N, Liu Y, McGinty KA,Berkley KJ. Endometriosis as a neurovascularcondition: estrous variations in innervation,vascularization, and growth factor content ofectopic endometrial cysts in the rat. AmJPhysiolRegul Integr Comp Physiol 2008;294:R162-71.62. Zhang X, Lu B, Huang X, Xu H, Zhou C,Lin J. Innervation of endometrium and myome-trium in women with painful adenomyosis anduterine fibroids. Fertil Steril 2010;94:730-7.63. Iacovides S, Avidon I, Baker FC. What weknow about primary dysmenorrhea today: acritical review. Hum Reprod Update 2015;21:762-78.64. Arendt-Nielsen L, Madsen H, Jarrell J,Gregersen H, Drewes AM. Pain evoked bydistension of the uterine cervix in women withdysmenorrhea: evidence for central sensitiza-tion. Acta Obstet Gynecol Scand 2014;93:741-8.65. Iacovides S, Baker FC, Avidon I, Bentley A.Women with dysmenorrhea are hypersensitiveto experimental deep muscle pain across themenstrual cycle. J Pain 2013;14:1066-76.66. Bajaj P, Bajaj P, Madsen H, Arendt-Nielsen L. A comparison of modality-specificsomatosensory changes during menstruationin dysmenorrheic and nondysmenorrheicwomen. Clin J Pain 2002;18:180-90.67. Slater H, Paananen M, Smith AJ, et al.Heightened cold pain and pressure pain sensi-tivity in young female adults with moderate-to-severe menstrual pain. Pain 2015;156:2468-78.68. Iacovides S, Avidon I, Baker F. Women withdysmenorrhea are hypersensitive to experi-mentally induced forearm ischemia duringpainful menstruation and during the pain-freefollicular phase. Eur J Pain 2015;19:797-804.69. As-Sanie S, Harris RE, Napadow V, et al.Changes in regional gray matter volume inwomen with chronic pelvic pain: a voxel-basedmorphometry study. Pain 2012;153:1006-14.70. Tu C-H, Niddam DM, Yeh T-C, et al. Men-strual pain is associated with rapid structuralalterations in the brain. Pain 2013;154:1718-24.71. Liu P, Yang J,WangG, et al. Altered regionalcortical thickness and subcortical volume inwomen with primary dysmenorrhea. Eur J Pain2016;20:512-20.72. Okkerse P, van Amerongen G, de Kam ML,et al. The use of a battery of pain models todetect analgesic properties of compounds: atwo-part four-way crossover study. Br J ClinPharmacol 2017;83:976-90.73. Winnard KP, Dmitrieva N, Berkley KJ.Cross-organ interactions between reproductive,gastrointestinal, and urinary tracts: modulationby estrous stage and involvement of the hypo-gastric nerve. Am J Physiol Regul Integr CompPhysiol 2006;291:R1592-601.74. Wesselmann U, Lai J. Mechanisms ofreferred visceral pain: uterine inflammation inthe adult virgin rat results in neurogenicplasma extravasation in the skin. Pain1997;73:309-17.
REV 5.5.0 DTD
75. Hsu AL, Sinaii N, Segars J, Nieman LK,Stratton P. Relating pelvic pain location to sur-gical findings of endometriosis. Obstet Gynecol2011;118:223-30.76. Duggan KC, Walters MJ, Musee J, et al.Molecular basis for cyclooxygenase inhibition bythe non-steroidal anti-inflammatory drug nap-roxen. J Biol Chem 2010;285:34950-9.77. Chan WY, Dawood MY, Fuchs F. Prosta-glandins in primary dysmenorrhea. Comparisonof prophylactic and nonprophylactic treatmentwith ibuprofen and use of oral contraceptives.Am J Med 1981;70:535-41.78. Chiou M-H, Wang H-H, Yang Y-H. Effect ofsystematic menstrual health education ondysmenorrheic female adolescents’ knowledge,attitudes, and self-care behavior. Kaohsiung JMed Sci 2007;23:183-90.79. Harel Z. Dysmenorrhea in adolescents andyoung adults: an update on pharmacologicaltreatments and management strategies. ExpertOpin Pharmacother 2012;13:2157-70.80. Latthe PM, Champaneria R. Dysmenorrhea.BMJ Clin Evid 2014;2014.81. Bieglmayer C, Hofer G, Kainz C,Reinthaller A, Kopp B, Janisch H. Concentra-tions of various arachidonic acid metabolites inmenstrual fluid are associated with menstrualpain and are influenced by hormonal contra-ceptives. Gynecol Endocrinol 1995;9:307-12.82. Edelman A, Micks E, Gallo MF, Jensen JT,Grimes DA. Continuous or extended cycle vscyclic use of combined hormonal contraceptivesfor contraception. Cochrane Database Syst Rev2014;7:CD004695.83. Wong CL, Farquhar C, Roberts H,Proctor M. Oral contraceptive pill for primarydysmenorrhea. Cochrane Database Syst Rev2009;4:CD002120.84. Witjes H, Creinin MD, Sundström-Poromaa I, Martin Nguyen A, Korver T.Comparative analysis of the effects of nome-gestrol acetate/17 b-estradiol and drospir-enone/ethinylestradiol on premenstrual andmenstrual symptoms and dysmenorrhea. Eur JContracept Reprod Health Care 2015;20:296-307.85. Winkler UH, Ferguson H, Mulders JA. Cyclecontrol, quality of life and acne with two low-dose oral contraceptives containing 20 microgethinylestradiol. Contraception 2004;69:469-76.86. Petraglia F, Parke S, Serrani M, Mellinger U,Römer T. Estradiol valerate plus dienogestversus ethinylestradiol plus levonorgestrel for thetreatment of primary dysmenorrhea. Int JGynaecol Obstet 2014;125:270-4.87. Imai A, Matsunami K, Takagi H, Ichigo S.Levonorgestrel-releasing intrauterine deviceused for dysmenorrhea: five-year literature re-view. Clin Exp Obstet Gynecol 2014;41:495-8.88. Harada T, Momoeda M, Taketani Y,Hoshiai H, Terakawa N. Low-dose oral contra-ceptive pill for dysmenorrhea associated withendometriosis: a placebo-controlled, double-blind, randomized trial. Fertil Steril 2008;90:1583-8.
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
89. Muzii L, Di Tucci C, Achilli C, et al. Contin-uous versus cyclic oral contraceptives afterlaparoscopic excision of ovarian endome-triomas: a systematic review and metaanalysis.Am J Obstet Gynecol 2016;214:203-11.90. Casper RF. Progestin-only pills may be abetter first-line treatment for endometriosis thancombined estrogen-progestin contraceptivepills. Fertil Steril 2017;107:533-6.91. Burnett M, Lemyre M. Primary dysmenor-rhea consensus guideline. J Obstet GynaecolCan 2017;39:585-95.92. Ling FW. Randomized controlled trial ofdepot leuprolide in patients with chronic pelvicpain and clinically suspected endometriosis.Pelvic Pain Study Group. Obstet Gynecol1999;93:51-8.93. Dawood MY, Lewis V, Ramos J. Corticaland trabecular bone mineral content in womenwith endometriosis: effect of gonadotropin-releasing hormone agonist and danazol. FertilSteril 1989;52:21-6.94. Dodin S, Lemay A, Maheux R, Dumont M,Turcot-Lemay L. Bone mass in endometriosispatients treated with GnRH agonist implant ordanazol. Obstet Gynecol 1991;77:410-5.95. Leather A, Studd J, Watson N, Holland E.The prevention of bone loss in young womentreated with GnRH analogues with “add-back”estrogen therapy. Obstet Gynecol 1993;81:104-7.96. Hornstein MD, Surrey ES, Weisberg GW,Casino LA. Leuprolide acetate depot and hor-monal add-back in endometriosis: a 12-monthstudy. Lupron Add-Back Study Group. ObstetGynecol 1998;91:145-8.97. Zupi E, Marconi D, Sbracia M, et al. Add-back therapy in the treatment ofendometriosis-associated pain. Fertil Steril2004;82:1303-8.98. Tahara M, Matsuoka T, Yokoi T, Tasaka K,Kurachi H, Murata Y. Treatment of endometri-osis with a decreasing dosage of agonadotropin-releasing hormone agonist(nafarelin): a pilot study with low-dose agonisttherapy (“draw-back” therapy). Fertil Steril2000;73:799-804.99. Practice Committee of the American Societyfor Reproductive Medicine. Treatment of pelvicpain associated with endometriosis: a commit-tee opinion. Fertil Steril 2014;101:927-35.100. Strowitzki T, Faustmann T, Gerlinger C,Seitz C. Dienogest in the treatment ofendometriosis-associated pelvic pain: a 12-week, randomized, double-blind, placebo-controlled study. Eur J Obstet Gynecol ReprodBiol 2010;151:193-8.101. Strowitzki T, Marr J, Gerlinger C,Faustmann T, Seitz C. Dienogest is as effectiveas leuprolide acetate in treating the painfulsymptoms of endometriosis: a 24-week, ran-domized, multicenter, open-label trial. HumReprod 2010;25:633-41.102. Al-Jefout M, Nawaiseh N. Continuousnorethisterone acetate versus cyclical drospir-enone 3 mg/ethinyl estradiol 20 mg for themanagement of primary dysmenorrhea in young
American Journal of Obstetrics & Gynecology 9
7:05 pm � ce

Expert Review ajog.org
10071008100910101011101210131014101510161017101810191020102110221023102410251026102710281029103010311032103310341035103610371038103910401041104210431044104510461047104810491050105110521053105410551056105710581059106010611062
10631064106510661067106810691070107110721073107410751076107710781079108010811082108310841085108610871088108910901091109210931094109510961097109810991100110111021103110411051106110711081109111011111112111311141115111611171118
adult women. J Pediatr Adolesc Gynecol2016;29:143-7.103. Zigler RE, McNicholas C. Unscheduledvaginal bleeding with progestin-only contra-ceptive use. Am J Obstet Gynecol 2017;216:443-50.104. Vercellini P, Cortesi I, Crosignani PG. Pro-gestins for symptomatic endometriosis: a criticalanalysis of the evidence. Fertil Steril 1997;68:393-401.105. Pavone ME, Bulun SE. Aromatase in-hibitors for the treatment of endometriosis. FertilSteril 2012;98:1370-9.106. Attar E, Bulun S. Aromatase and othersteroidogenic genes in endometriosis: trans-lational aspects. Hum Reprod Update 2006;12:49-56.107. Agarwal AK, Garg R, Ritch A, Sarkar P.Postural orthostatic tachycardia syndrome.Postgrad Med J 2007;83:478-80.108. Gurates B, Parmaksiz C, Kilic G, Celik H,Kumru S, Simsek M. Treatment of symptomaticuterine leiomyoma with letrozole. Reprod Bio-med Online 2008;17:569-74.109. Berlanda N, Somigliana E, Viganò P,Vercellini P. Safety of medical treatments forendometriosis. Expert Opin Drug Saf 2016;15:21-30.110. Proctor M, Latthe P, Farquhar C, Khan K,Johnson N. Surgical interruption of pelvic nervepathways for primary and secondary dysmen-orrhea. Cochrane Database Syst Rev 2005;4:CD001896.111. Latthe P, Proctor M, Farquhar C,Johnson N, Khan K. Surgical interruption ofpelvic nerve pathways in dysmenorrhea: a sys-tematic review of effectiveness. Acta ObstetGynecol Scand 2007;86:4-15.112. Daniels J, Gray R, Hills RK, et al. Laparo-scopic uterosacral nerve ablation for alleviatingchronic pelvic pain: a randomized controlledtrial. JAMA 2009;302:955-61.113. Lichten EM, Bombard J. Surgical treat-ment of primary dysmenorrhea with laparo-scopic uterine nerve ablation. J Reprod Med1987;32:37-41.114. Juang C-M, Chou P, YenM-S, Horng H-C,Twu N-F, Chen C-Y. Laparoscopic uterosacralnerve ablation with and without presacral neu-rectomy in the treatment of primary dysmenor-rhea: a prospective efficacy analysis. J ReprodMed 2007;52:591-6.115. Chen FP, Soong YK. The efficacy andcomplications of laparoscopic presacral neu-rectomy in pelvic pain. Obstet Gynecol 1997;90:974-7.116. Nehra A, Colreavy F, Khandheria B,Chandrasekaran K. Sildenafil citrate, a selectivephosphodiesterase type 5 inhibitor: urologic andcardiovascular implications. World J Urol2001;19:40-5.117. Dmitrovic R, Kunselman AR, Legro RS.Sildenafil citrate in the treatment of pain in pri-mary dysmenorrhea: a randomized controlledtrial. Hum Reprod 2013;28:2958-65.118. Ali A, Bipozzi MA, Burgos RA, et al.Transdermal nitroglycerine in the management
10 American Journal of Obstetrics & Gynecology
REV 5.5.0 DTD
of pain associatedwith primary dysmenorrhea: amultinational pilot study. The TransdermalNitroglycerine/Dysmenorrhea StudyGroup. J IntMed Res 1997;25:41-4.119. Moya RA, Moisa CF, Morales F, Wynter H,Ali A, Narancio E. Transdermal glyceryl trinitratein themanagement of primary dysmenorrhea. IntJ Gynaecol Obstet 2000;69:113-8.120. Facchinetti F, Sgarbi L, Piccinini F, Volpe A.A comparison of glyceryl trinitrate with diclofe-nac for the treatment of primary dysmenorrhea:an open, randomized, cross-over trial. GynecolEndocrinol 2002;16:39-43.121. Fenakel K, Lurie S. The use of calciumchannel blockers in obstetrics and gynecology;a review. Eur J Obstet Gynecol Reprod Biol1990;37:199-203.122. Andersson KE, Ulmsten U. Effects ofnifedipine on myometrial activity and lowerabdominal pain in women with primarydysmenorrhea. Br J Obstet Gynaecol 1978;85:142-8.123. Sandahl B, Ulmsten U, Andersson KE. Trialof the calcium antagonist nifedipine in the treat-ment of primary dysmenorrhea. Arch Gynecol1979;227:147-51.124. Mondero NA. Nifedipine in the treatment ofdysmenorrhea. J Am Osteopath Assoc1983;82:704-8.125. Ulmsten U. Calcium blockade as a rapidpharmacological test to evaluate primarydysmenorrhea. Gynecol Obstet Invest 1985;20:78-83.126. Akerlund M. Involvement of oxytocin andvasopressin in the pathophysiology of pretermlabor and primary dysmenorrhea. Prog BrainRes 2002;139:359-65.127. Akerlund M. Can primary dysmenorrheabe alleviated by a vasopressin antagonist? Re-sults of a pilot study. Acta Obstet GynecolScand 1986;66:459-61.128. Liedman R, Grant L, Igidbashian S, et al.Intrauterine pressure, ischemia markers, andexperienced pain during administration of avasopressin V1a receptor antagonist in sponta-neous and vasopressin-induced dysmenorrhea.Acta Obstet Gynecol Scand 2006;85:207-11.129. Brouard R, Bossmar T, Fournié-Lloret D,Chassard D, Akerlund M. Effect of SR49059, anorally active V1a vasopressin receptor antago-nist, in the prevention of dysmenorrhea. BJOG2000;107:614-9.130. Valentin L, Sladkevicius P, Kindahl H,Broeders A, Marsal K, Melin P. Effects of avasopressin antagonist in women withdysmenorrhea. Gynecol Obstet Invest 2000;50:170-7.131. Pomeroy A, Rand M. Anticholinergic ef-fects and passage through the intestinal wall ofN-butylhyoscine bromide. J Pharm Pharmacol1969;21:180-7.132. Kemp J. “Buscopan” in spasmodicdysmenorrhea. Curr Med Res Opin 1972;1:19-25.133. Moawed S. Indigenous practices of Saudigirls in Riyadh during theirmenstrual period. EastMediterr Health J 2001;7:197-203.
MONTH 2017
� YMOB11822_proof � 15 September 2017 �
134. Ogunfowokan AA, Babatunde OA. Man-agement of primary dysmenorrhea by schooladolescents in ILE-IFE, Nigeria. J Sch Nurs2010;26:131-6.135. Aziato L, Dedey F, Clegg-Lamptey JNA.Dysmenorrheamanagement and coping amongstudents in Ghana: a qualitative exploration.J Pediatr Adolesc Gynecol 2015;28:163-9.136. Enck P, Koehler U, Weigmann H, Mueller-Lissner S. Abdominal pain, cramping ordiscomfort impairs quality of life in women: anInternet-based observational pilot studyfocusing on impact of treatment.Z Gastroenterol 2017;55:260-6.137. Pareek A, Chandurkar NB, Patil RT,Agrawal SN, Uday RB, Tambe SG. Efficacy andsafety of aceclofenac and drotaverine fixed-dose combination in the treatment of primarydysmenorrhea: a double-blind, double-dummy,randomized comparative study with aceclofe-nac. Eur J Obstet Gynecol Reprod Biol2010;152:86-90.138. Pattanittum P, Kunyanone N, Brown J. Di-etary supplements for dysmenorrhea. CochraneDatabase Syst Rev 2016;3:CD002124.139. Chen CX, Barrett B, Kwekkeboom KL.Efficacy of oral ginger (Zingiber officinale) fordysmenorrhea: a systematic review and meta-analysis. Evid Based Complement Alternat Med2016;2016:6295737.140. Smith CA, Armour M, Zhu X, Li X, Lu ZY.Acupuncture for dysmenorrhea. CochraneDatabase Syst Rev 2016;4:CD007854.141. Chaudhuri A, Singh A, Dhaliwal L.A randomized controlled trial of exercise and hotwater bottle in the management of dysmenor-rhea in school girls of Chandigarh, India. Indian JPhysiol Pharmacol 2013;57:114-22.142. Yang N-Y, Kim S-D. Effects of a yogaprogram on menstrual cramps and menstrualdistress in undergraduate students with primarydysmenorrhea: a single-blind, randomizedcontrolled trial. J Altern Complement Med2016;22:732-8.143. Azima S, Bakhshayesh HR, Kaviani M,Abbasnia K, Sayadi M. Comparison of the effectof massage therapy and isometric exercises onprimary dysmenorrhea: a randomized controlledclinical trial. J Pediatr Adolesc Gynecol 2015;28:486-91.144. Ortiz MI, Cortés-Márquez SK, Romero-Quezada LC, Murguía-Cánovas G, Jaramillo-Díaz AP. Effect of a physiotherapy program inwomen with primary dysmenorrhea. Eur JObstet Gynecol Reprod Biol 2015;194:24-9.145. Brown J, Brown S. Exercise for dysmen-orrhea. Cochrane Database Syst Rev 2010;2:CD004142.146. Lauretti GR, Oliveira R, Parada F,Mattos AL. The new portable transcutaneouselectrical nerve stimulation device was effica-cious in the control of primary dysmenorrheacramp pain. Neuromodulation 2015;18:522-7.147. Wang S-F, Lee J-P, Hwa H-L. Effect oftranscutaneous electrical nerve stimulation onprimary dysmenorrhea. Neuromodulation2009;12:302-9.
7:05 pm � ce

ajog.org Expert Review
11191120112111221123112411251126112711281129113011311132113311341135113611371138113911401141114211431144114511461147114811491150115111521153115411551156115711581159116011611162116311641165116611671168116911701171117211731174
1175117611771178117911801181118211831184118511861187
148. Dawood MY, Ramos J. Transcutaneouselectrical nerve stimulation (TENS) for the treat-ment of primary dysmenorrhea: a randomizedcrossover comparison with placebo TENS andibuprofen. Obstet Gynecol 1990;75:656-60.149. Schiøtz HA, Jettestad M, Al-Heeti D.Treatment of dysmenorrhea with a new TENSdevice (OVA). J Obstet Gynaecol 2007;27:726-8.150. Kaplan B, Rabinerson D, Lurie S, Peled Y,Royburt M, Neri A. Clinical evaluation of a newmodel of a transcutaneous electrical nervestimulation device for the management of pri-mary dysmenorrhea. Gynecol Obstet Invest1997;44:255-9.
REV 5.5.0 DTD
151. Nguyen AM, Arbuckle R, Korver T, et al.Psychometric validation of the dysmenorrheadaily diary (DysDD): a patient-reported outcomefor dysmenorrhea. Qual Life Res 2017;26:2041-55.152. Webster SK, Martin HJ, Uchalik D,Gannon L. The menstrual symptom question-naire and spasmodic/congestive dysmenor-rhea: measurement of an invalid construct.J Behav Med 1979;2:1-19.153. Grosser T, Fries S, Lawson JA,Kapoor SC, Grant GR, FitzGerald GA. Drugresistance and pseudoresistance: an unin-tended consequence of enteric coating aspirin.Circulation 2013;127:377-85.
MONTH 2017 A
� YMOB11822_proof � 15 September 2017 �
154. Eikelboom JW, Hankey GJ. Over-expression of the multidrug resistance protein-4transporter in patients undergoing coronary ar-tery bypass graft surgery. J Am Coll Cardiol2011;58:762-4.155. Kennedy S, Bergqvist A, Chapron C, et al.ESHRE guideline for the diagnosis and treat-ment of endometriosis. Hum Reprod 2005;20:2698-704.156. Management of endometriosis. Practicebulletin no. 114. Obstet Gynecol 2010;116:223-36.157. Falcone T, Lebovic DI. Clinical manage-ment of endometriosis. Obstet Gynecol2011;118:691-705.
merican Journal of Obstetrics & Gynecology 11
7:05 pm � ce
1188118911901191119211931194119511961197119811991200120112021203120412051206120712081209121012111212121312141215121612171218121912201221122212231224122512261227122812291230