Expanding Genetic Screening in Obstetrical Practice
38
10/2/2017 1 Expanding Genetic Screening in Obstetrical Practice Michael T. Mennuti, M.D. Professor Emeritus Perelman School of Medicine University of Pennsylvania I do not have any financial relationships or other potential conflicts of interest to disclose related to this presentation or my participation in the luncheon conference.
Transcript of Expanding Genetic Screening in Obstetrical Practice
10/2/2017
1
Expanding Genetic Screeningin Obstetrical Practice
Michael T. Mennuti, M.D.Professor EmeritusPerelman School of MedicineUniversity of Pennsylvania
I do not have any financial relationships or other potential conflicts of interest to disclose related to this presentation or my participation in the luncheon conference.
10/2/2017
2
Cell free DNA testing
Parental carrier screening
Edmunde Burke
10/2/2017
3
Those who don't know history are destined to repeat it.
Edmunde Burke
Lo, YMD et.al. Presence of fetal DNA in maternal plasma and serum. Lancet 350:485-487, 1997

10/2/2017
4
Noninvasive prenatal diagnosis of fetal chromosomal aneuploidyby massively parallel genomic sequencing
of DNA in maternal plasma
Rossa W. K. Chiu, K. C. Allen Chana, Yuan Gaoc, et al. PNAS Dec 23, 2008
Noninvasive diagnosis of fetal aneuploidy by shotgunsequencing DNA from maternal blood
H. Christina Fan, Yair J. Blumenfeld, Usha Chitkara, et allPNAS Oct 21, 2008
10/2/2017
5
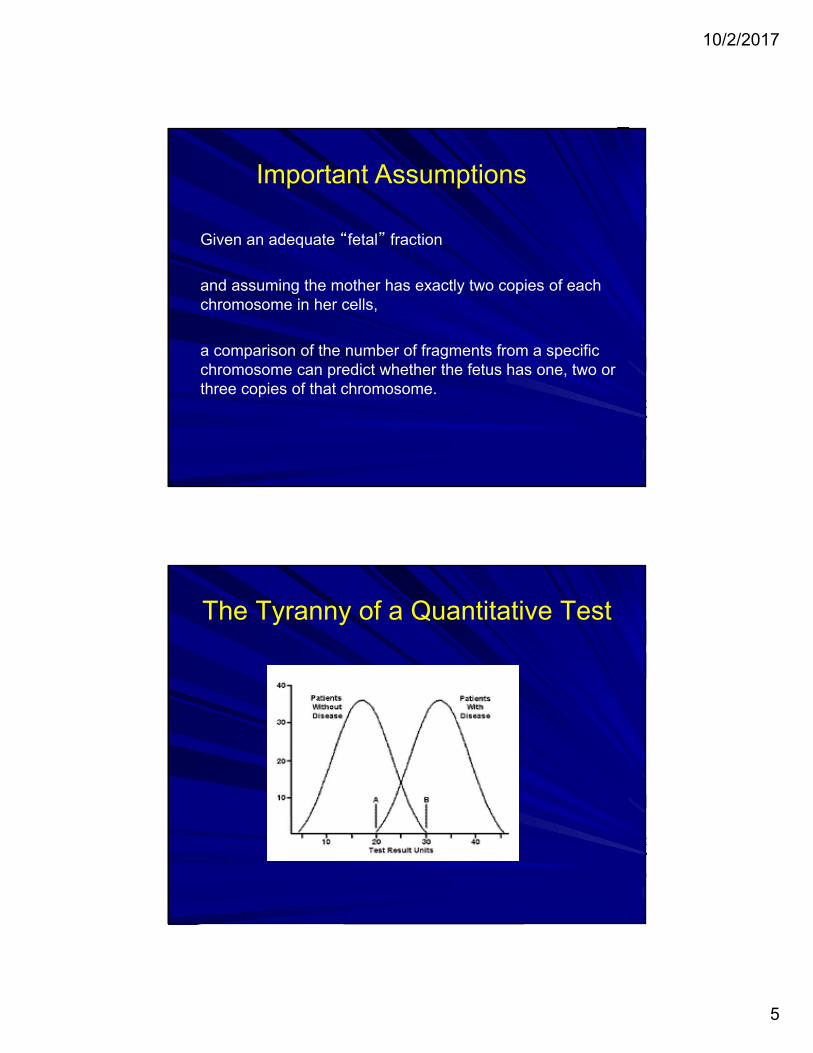
Given an adequate “fetal” fraction
and assuming the mother has exactly two copies of each chromosome in her cells,
a comparison of the number of fragments from a specific chromosome can predict whether the fetus has one, two or three copies of that chromosome.
Important Assumptions
The Tyranny of a Quantitative Test
10/2/2017
6
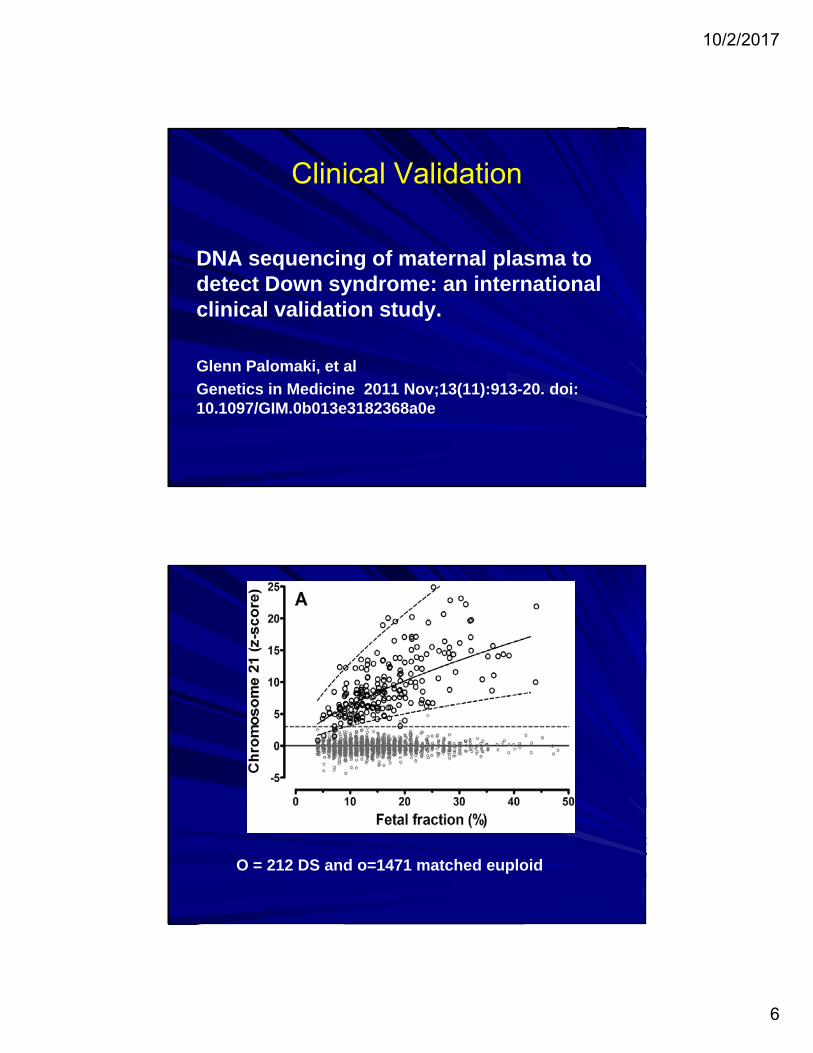
Clinical Validation
DNA sequencing of maternal plasma to detect Down syndrome: an international clinical validation study.
Glenn Palomaki, et al
Genetics in Medicine 2011 Nov;13(11):913-20. doi: 10.1097/GIM.0b013e3182368a0e
O = 212 DS and o=1471 matched euploid
10/2/2017
7
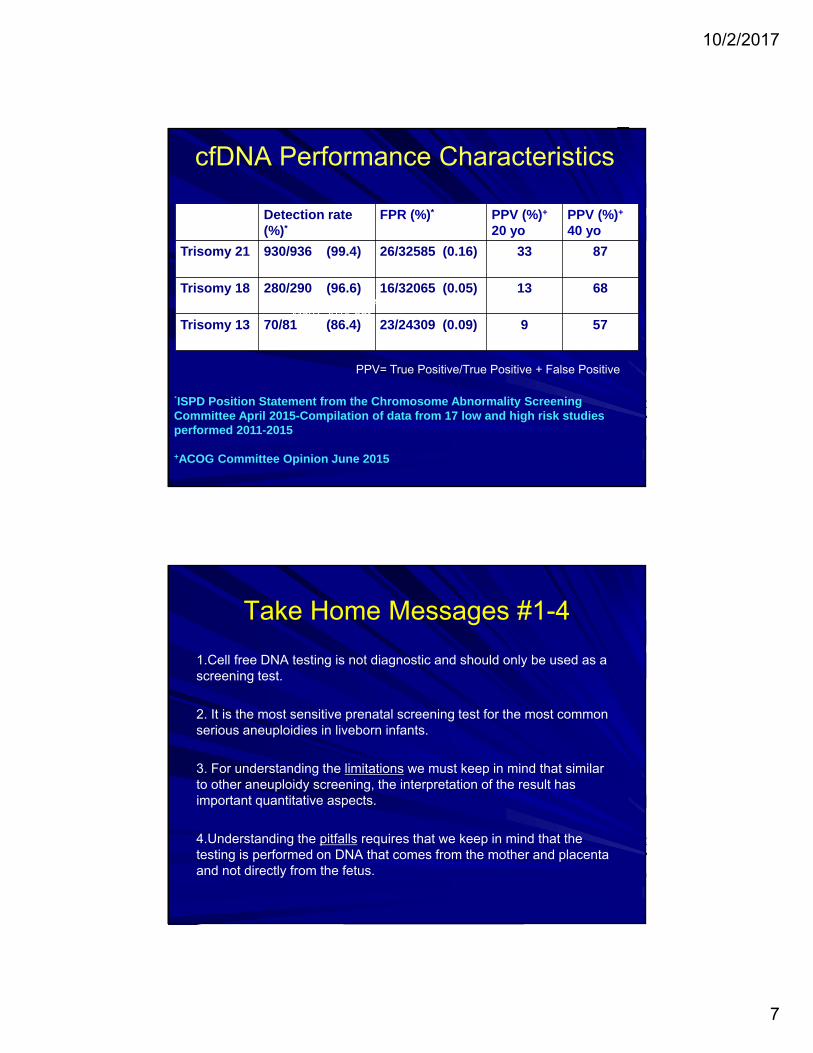
cfDNA Performance Characteristics
Detection rate (%)*
FPR (%)* PPV (%)+
20 yoPPV (%)+
40 yo
Trisomy 21 930/936 (99.4) 26/32585 (0.16) 33 87
Trisomy 18 280/290 (96.6) 16/32065 (0.05) 13 68
Trisomy 13 70/81 (86.4) 23/24309 (0.09) 9 57
*ISPD Position Statement from the Chromosome Abnormality Screening Committee April 2015-Compilation of data from 17 low and high risk studies performed 2011-2015
+ACOG Committee Opinion June 2015
PPV= True Positive/True Positive + False Positive
FINAL Philly Genetics MENNUTI May7,2015.ppt
Take Home Messages #1-4
1.Cell free DNA testing is not diagnostic and should only be used as a screening test.
2. It is the most sensitive prenatal screening test for the most common serious aneuploidies in liveborn infants.
3. For understanding the limitations we must keep in mind that similar to other aneuploidy screening, the interpretation of the result has important quantitative aspects.
4.Understanding the pitfalls requires that we keep in mind that the testing is performed on DNA that comes from the mother and placenta and not directly from the fetus.
10/2/2017
8
Biologic Factors that Influence Test Performance
“Fetal” fraction
Multiple gestation
Fetal and/or placental mosaicism/UPD
Genital discordance
Maternal aneuploidy or non-pathogenic CNV
Biologic Factors that Influence Test Performance
“Fetal” fraction
Multiple gestation
Fetal/placental mosaicism
Genital discordance
Maternal aneuploidy or benign CNV
10/2/2017
9
Case #1
A 40 yo G3P0 Ab2 with a BMI of 46 presents for US and counseling after cell free DNA testing drawn two weeks ago was reported as insufficient fetal fraction. Pt is on lovenoxfor Factor V Leiden.
On ultrasound there is a viable singleton pregnancy that confirms the patient was 8 weeks when the cfDNA test was drawn. The NT is 1.1 mm at 10 wks
The patient is anxious for a result because she has a gender reveal party scheduled for next week. What do you offer ?
Clinical correlations% fetal fraction (ff)
Rises as gestational age advances
Much higher in multiple gestations
Inversely related to maternal weight
(absolute weight cut-off for not offering not defined)
Insufficient ff may be increased in patients on heparin or lovenox.
Insufficient ff has been associated with increased risk of
aneuploidy (T13,T18)
10/2/2017
10
Biologic Factors that Influence Test Performance
“Fetal” fraction
Multiple gestation
Fetal/placental mosaicism
Genital discordance
Maternal aneuploidy or CNV
Twins (and other Multiples)
10/2/2017
11
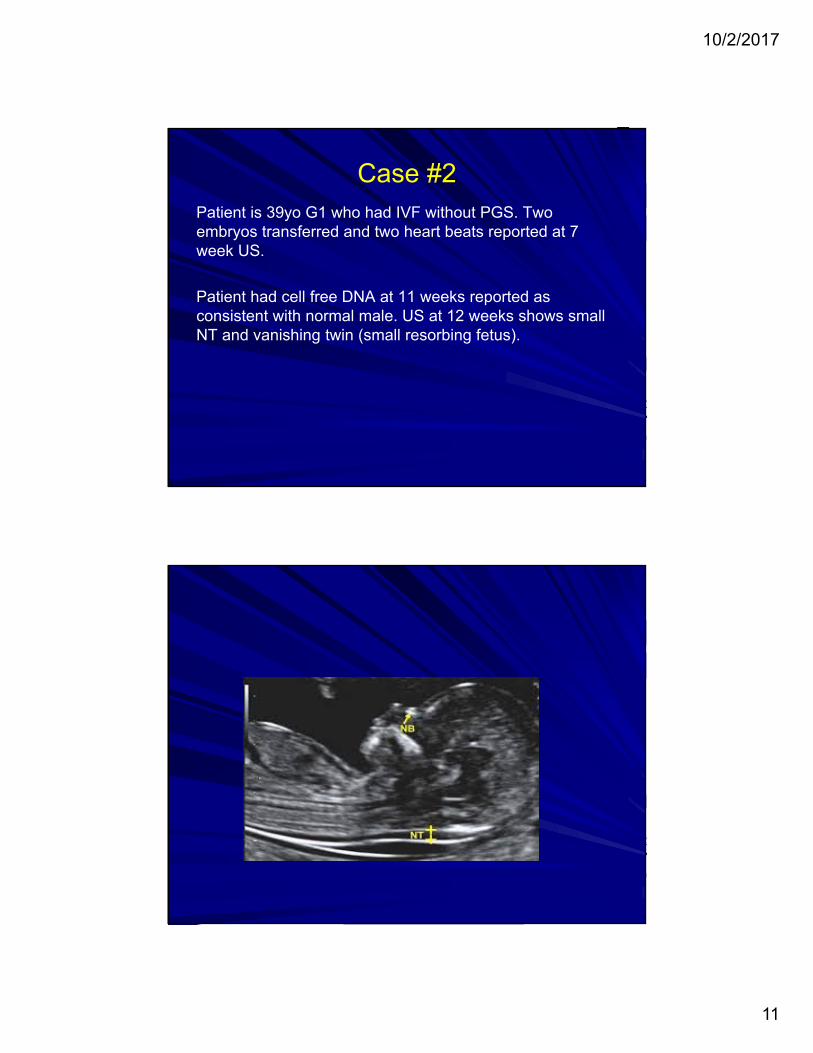
Case #2Patient is 39yo G1 who had IVF without PGS. Two embryos transferred and two heart beats reported at 7 week US.
Patient had cell free DNA at 11 weeks reported as consistent with normal male. US at 12 weeks shows small NT and vanishing twin (small resorbing fetus).

10/2/2017
12
Case #2Patient is 39yo G1 who had IVF without PGS. Two embryos transferred and two heart beats reported at 7 week US.
Patient had cell free DNA at 11 weeks reported as consistent with normal male. US at 12 weeks shows small NT and resorbing fetus.
US at 16 weeks shows normal anatomy survey and female genitalia
10/2/2017
13
Options
1. Repeat cell free DNA
2. Offer amnio with chromosome analysis
3. Offer serum screening
4. Repeat US at 20 weeks for abnormalities or markers
and check the genitals
5. No further testing
Options
1. Repeat cell free DNA
2. Offer amnio with chromosome analysis
3. Offer serum screening
4. Repeat US at 20 weeks for abnormalities or markers
and check the genitals
5. No further testing

10/2/2017
14
Biologic Factors that Influence Test Performance
“Fetal” fraction
Multiple gestation
Fetal/placental mosaicism
Genital discordance
Maternal aneuploidy or CNV
10/2/2017
15

10/2/2017
16
Why is this important ?(Back ground: CPM is seen in 1-2% of CVS and amniocentesis usually recommend to resolve it.)
Does maternal plasma provide a broader sampling of DNA from placental cells and detect more mosaicism than CVS ?
Are abnormal cell lines proportionately represented in cell free DNA ?
At what level do we detect clinically relevant true fetal mosaicism using cell free DNA ?
What are the consequences of placental and/or fetal mosaicism?
Case #3
28yo G1 declined aneuploidy screening. Noted to have 8 day growth lag at time of normal 20 week scan. Follow-up US at 28 weeks recommended.
Follow-up US for growth with EFW 7th percentile. Although no malformations are apparent the patient is offered and declines amniocentesis for genetic and infectious disease studies. The patient accepts cell free DNA screening, CMV serology

10/2/2017
17
Cell free DNA result consistent withtrisomy 7 mosaicism
Case #3What has been reported?
Pregnancies with mosaic trisomy 7 usually CPM without IUGR and with normal outcome
Pregnancies with maternal UPD 7 associated with Russell-Silver Syndrome
Russell Silver associated with characteristic facial features --- also, IUGR, failure to thrive, and adult short stature (male 4ft 11in; female 4ft 7in). Increased frequency of development delay, language delay and behavioral issues.
10/2/2017
18
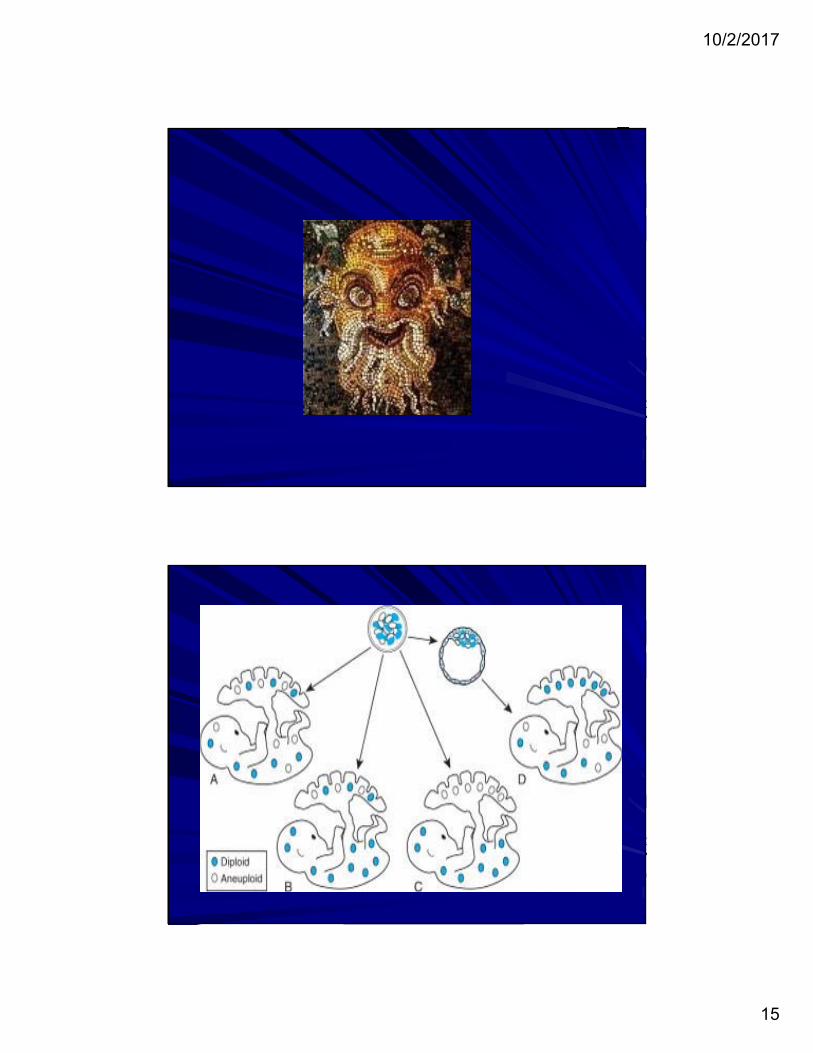
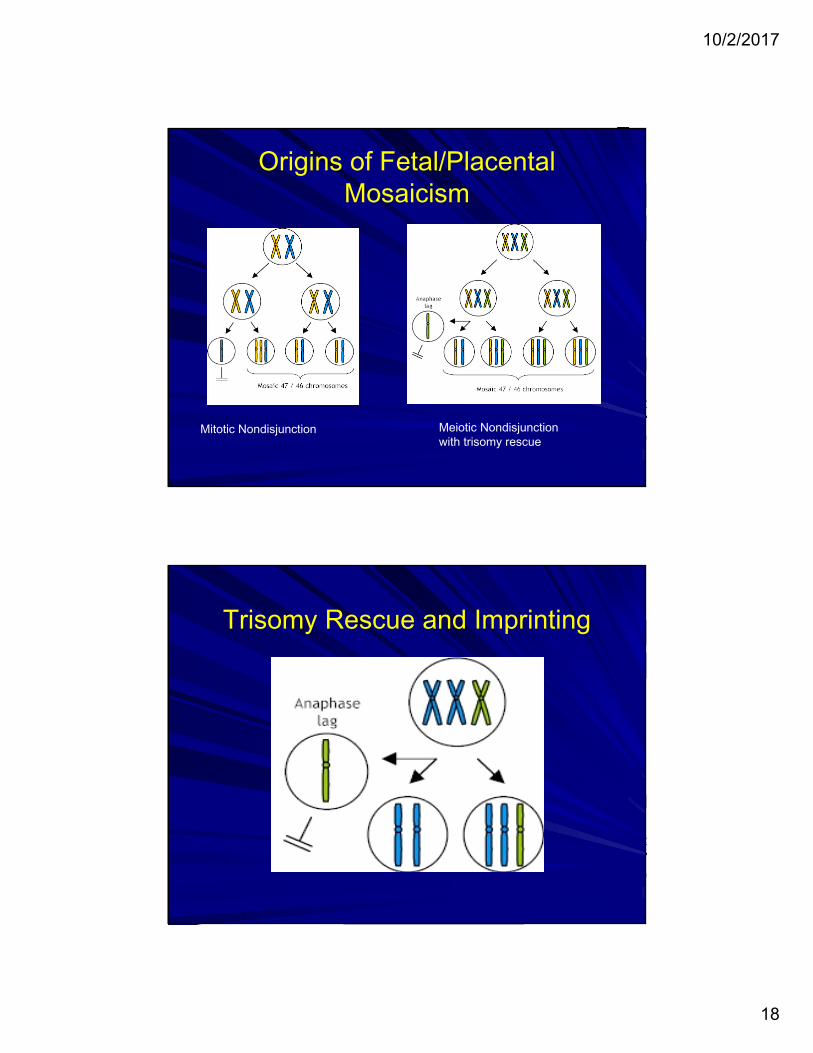
Origins of Fetal/Placental Mosaicism
Mitotic Nondisjunction Meiotic Nondisjunctionwith trisomy rescue
Trisomy Rescue and Imprinting
10/2/2017
19
Case #3What has been reported?
Pregnancies with mosaic trisomy 7 usually CPM without IUGR and with normal outcome
Pregnancies with maternal UPD 7associated with Russell-Silver Syndrome
Russell Silver associated with characteristic facial features --- also, IUGR, failure to thrive, and adult short stature (male 4ft 11in; female 4ft 7in). Increased frequency of development delay, language delay and behavioral issues.
Case #328yo G1 declined aneuploidy screening. Noted to have 8 day growth lag at time of normal 20 week scan. FU recommended
Follow-up US for growth at 27 weeks with EFW 7th
percentile. Although no malformations are apparent the patient is offered and declines amniocentesis for genetic and infectious disease studies. The patient accepts cell free DNA screening.
Subsequent follow-up US the EFW is 4th percentile.
SVD 38 weeks delivers 5lb 8 ½ ounce male.
10/2/2017
20
Laboratory Testing Result
10/2/2017
21
Take Home Messages #1-4
1.Cell free DNA testing is not diagnostic and should only be used as a screening test.
2. It is the most sensitive prenatal screening test for the most common serious aneuploidies in liveborn infants.
3. For understanding the limitations we must keep in mind that similar to other aneuploidy screening, the interpretation of the result has important quantitative aspects.
4.Understanding the pitfalls requires that we keep in mind that the testing is performed on DNA that comes from the mother and placenta and not directly from the fetus.
Take Home Message #5
5. Our assumption that normal placental chromosomes means normal fetal chromosomes and vice versa is usually, but not always, correct

10/2/2017
22
Biologic Factors that Influence Test Performance
“Fetal” fraction
Multiple gestation
Fetal/placental mosaicism
Genital discordance
Maternal aneuploidy or CNV
What is different about SCAs? SCAs are more common: 1/350-1/400 births
and mosaicism is more common with SCAs
cfDNA testing for SCA is associated with different test performance and fetal diagnosis is associated with unique counseling challenges
Parental decision making following identification of an SCA is substantially different than with other diagnoses
Analysis of sex chromosomes by cell free DNA was commercially driven but does have some value beyond gender reveal events
10/2/2017
23
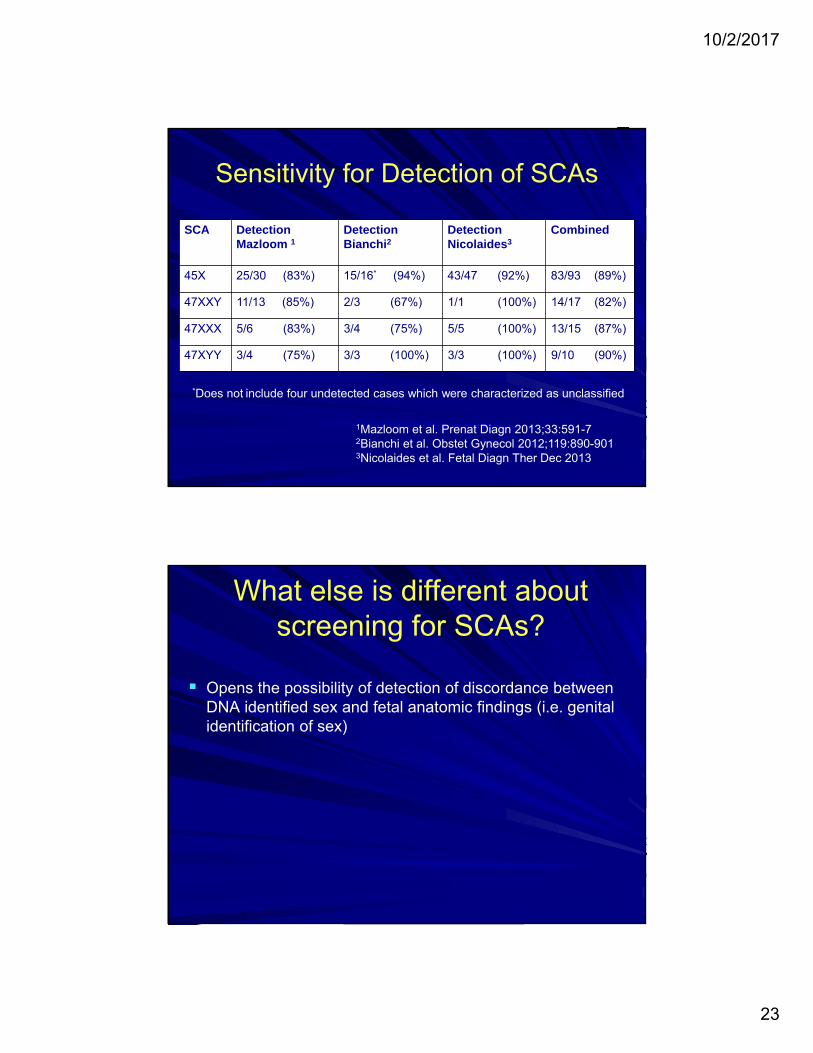
Sensitivity for Detection of SCAs
SCA Detection Mazloom 1
Detection Bianchi2
Detection Nicolaides3
Combined
45X 25/30 (83%) 15/16* (94%) 43/47 (92%) 83/93 (89%)
47XXY 11/13 (85%) 2/3 (67%) 1/1 (100%) 14/17 (82%)
47XXX 5/6 (83%) 3/4 (75%) 5/5 (100%) 13/15 (87%)
47XYY 3/4 (75%) 3/3 (100%) 3/3 (100%) 9/10 (90%)
1Mazloom et al. Prenat Diagn 2013;33:591-72Bianchi et al. Obstet Gynecol 2012;119:890-9013Nicolaides et al. Fetal Diagn Ther Dec 2013
*Does not include four undetected cases which were characterized as unclassified
What else is different about screening for SCAs?
Opens the possibility of detection of discordance between DNA identified sex and fetal anatomic findings (i.e. genital identification of sex)

10/2/2017
24
Experience with SCA testing by cfDNA Sequencing
Experience with 18,161 samples
SCA with Positive Screen - 204 ≅ 1:90
Frequency of False Positive – 0.26%-1.05%
Frequency of sex discordance - 32 ≅ 1:600
Bianchi et al. Obstet Gynecol 2015;125:375-82
Explanations for discordance
Human error- sample mix-up or lab error
Vanishing twin / co-twin demise
Inaccurate ultrasonographic imaging
Maternal organ transplant, transfusion
Fetal SCA or DSD

10/2/2017
25
Case # 4 38 yo G4P3 offered and accepts cf DNA screening
cfDNA: negative for trisomy 21, 18, 13 , female
Case #420 week Ultrasound
10/2/2017
26
Case #4
Repeat cfDNA test: confirmed original result
Follow-up US reconfirmed unambiguous male genitalia
Patient declined amniocentesis
DNA female / Ultrasound male
Sample mix-up or lab error
CAH, aromatase deficiency, maternal ovarian tumor, exogenous androgens
Translocation of SRY to an X chromosome or autosome
Mosaicism – 45,X/46,XY or 46,XX/46,XY
SOX 9 duplication
10/2/2017
27
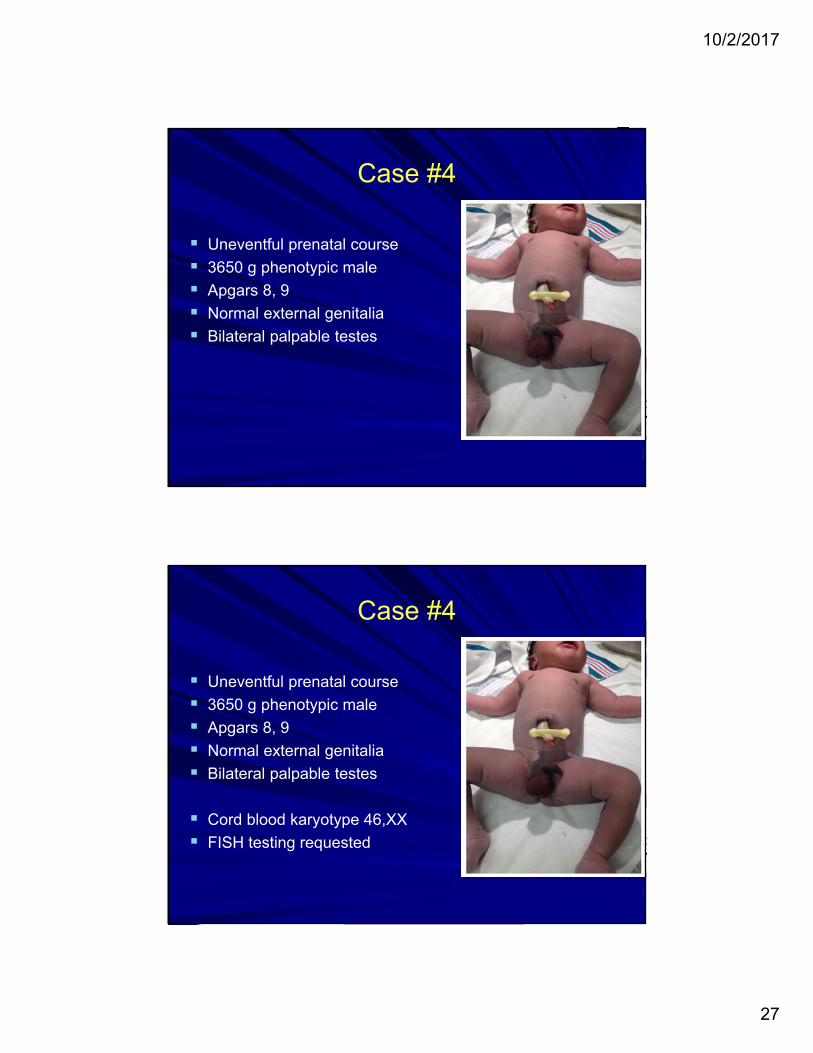
Case #4
Uneventful prenatal course
3650 g phenotypic male
Apgars 8, 9
Normal external genitalia
Bilateral palpable testes
Case #4
Uneventful prenatal course
3650 g phenotypic male
Apgars 8, 9
Normal external genitalia
Bilateral palpable testes
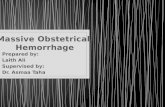
Cord blood karyotype 46,XX
FISH testing requested
10/2/2017
28
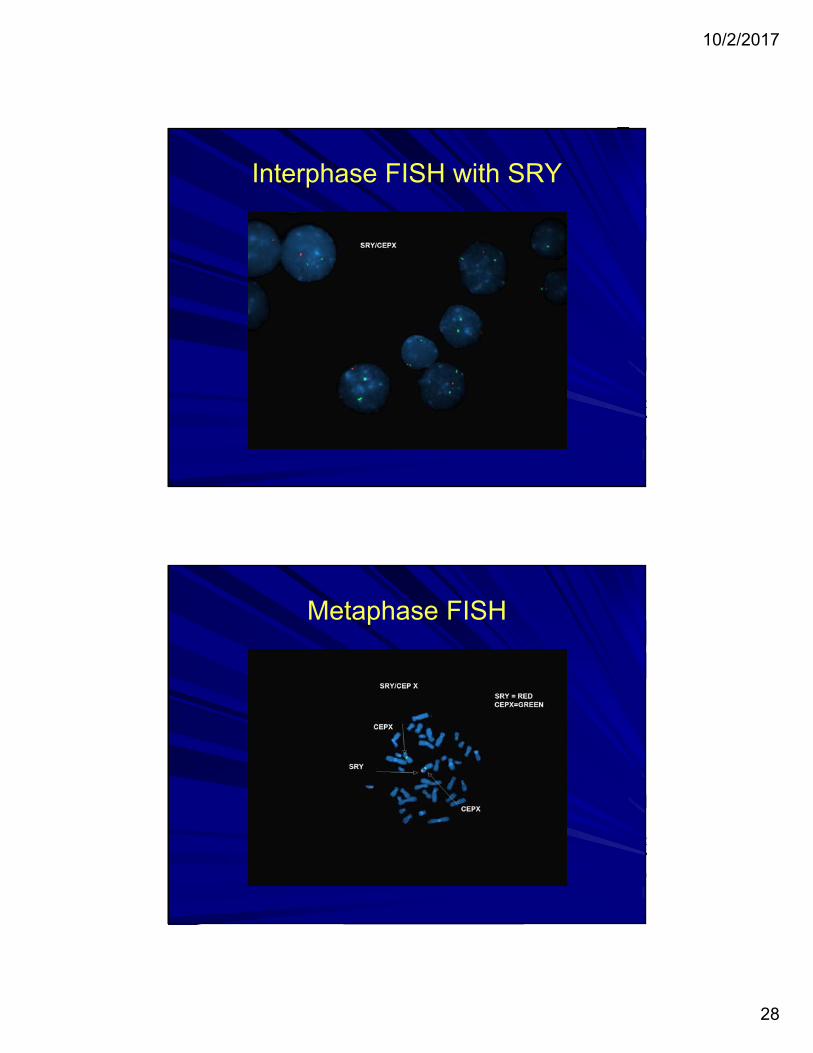
Interphase FISH with SRY
Metaphase FISH
10/2/2017
29
DNA male / Ultrasound female
Sample mix-up, lab error
Androgen receptor defect, 5-α reductase deficiency
Swyer syndrome – mutations SRY or other genes play a role in sexual development
Campomelic dysplasia – SOX 9 haploinsuff
45,X/46,XY or 46,XX/46,XY
Take Home Message #6
6. Always double check gender result from cell free DNA
with findings on the anatomy survey.
10/2/2017
30
Biologic Influences on Test Performance
“Fetal” fraction
Multiple gestation
Fetal/placental mosaicism
Genital discordance
Maternal aneuploidy or CNV
Maternal Aneuploidy
Constitutional
Constitutional aneuploidy
Mosaicism for constitutional aneuploidy
Acquired
Tumor - usually multiple aneuploidies
Transplant
Other
10/2/2017
31
Case #5
28 year old primigravida presented as transfer for high risk obstetrical care. Primary reason for transfer is “suspected connective disorder” and secondarily for fetus with “gastroschisis”.
Patient had a history of lax joints, double jointedness, tall stature and long limbs. Patient has been seen by a geneticist who raised suspicion of connective tissue disorder and referred to an expert in these diseases. Patient did not followed-up.
Case #5
At the time of dx of gastroschisis patient was offered and declined amniocentesis. Patient was then offered cfDNAscreening which was performed and was consistent with 47,XXX fetus.
Patient again declined amniocentesis and opted to continue the pregnancy. Patient had read about 47,XXX and concluded she would not terminate the pregnancy for gastroschisis or for 47,XXX.

10/2/2017
32
Case #5
Maternal karyotype performed and result 47,XXX.
Maternal response –
That’s great - it explains everything – I am very glad I had the test
Case #5
Maternal karyotype performed and result 47,XXX.
Maternal response –
That’s great - it explains everything – I am very glad I had the test
Newborn cord blood – 46,XX
10/2/2017
33
going the way of the dinosaurs
Only fortune tellers, weathermen and fools should pretend to predict the future.

10/2/2017
34
Increased use of cell free DNA testing as the primary screening method for fetal aneuploidy
A single assay for covering 6000 variants and 600 genes.

10/2/2017
35
Increased use of cell free DNA testing as the primary screening method for aneuploidy
Parental carrier screening for an greater and greater number of recessive disease traits to identify couples at risk
Increase marketing for detection of single gene disorders in the fetus by cfDNA
Use of whole exome or whole genome sequencing to evaluate fetus with US detected abnormalities
Parental carrier screening for a greater and greater number of recessive disease traits to identify pregnancies at risk
Increase marketing for detection of single gene disorders in the fetus by cfDNA
Use of whole exome or whole genome sequencing to evaluate fetus with US detected abnormalities
Technical ability to sequence the exome or genome of the fetus using cf DNA such that it will be clinically practical
Advances in capturing fetal cells from maternal blood
10/2/2017
36
Goals of Screening
Chinese Scientists Edit Genes of Human Embryos, Raising Concerns - NYT APR. 23, 2015
UK scientists gain licence to edit genes in human embryos - Nature Feb. 1 2016
Swedish scientist edits DNA of human embryo –
Sep. 22, 2016

10/2/2017
37
Editing the DNA of a human embryo to prevent a disease in a baby could be ethically allowable one day—but only in rare circumstances and with safeguards in place, says a widely anticipated report released today.
Report of international committee convened by the U.S. National Academy of Sciences (NAS) and the National Academy of Medicine in Washington, D.C.
Science Feb 14 2017
Chinese Scientists Edit Genes of Human Embryos, Raising Concerns - NYT APRIL 23, 2015
UK scientists gain licence to edit genes in human embryos - Nature feb 1 2016
Swedish scientist edits DNA of human embryo –
Sep. 22, 2016
First U.S. team to gene-edit human embryos revealed - Jul. 27, 2017

10/2/2017
38
Letting the Genomeout of the Bottle –
Will We Get Our Wish?
Thank you for your attention !