Expanded Newborn Screening: Public Health Policy and Clinical Impact Nutrition 526 October 18, 2010...
73
Expanded Newborn Expanded Newborn Screening: Screening: Public Health Policy Public Health Policy and Clinical Impact and Clinical Impact Nutrition 526 Nutrition 526 October 18, 2010 October 18, 2010 Beth Ogata, MS, RD, CSP, Beth Ogata, MS, RD, CSP, [email protected] [email protected] Cristine M Trahms, MS, RD, FADA Cristine M Trahms, MS, RD, FADA
-
date post
22-Dec-2015 -
Category
Documents
-
view
215 -
download
0
Transcript of Expanded Newborn Screening: Public Health Policy and Clinical Impact Nutrition 526 October 18, 2010...

Expanded Newborn Expanded Newborn Screening: Screening:
Public Health Policy and Public Health Policy and Clinical ImpactClinical Impact
Nutrition 526Nutrition 526October 18, 2010October 18, 2010
Beth Ogata, MS, RD, CSP, Beth Ogata, MS, RD, CSP, [email protected]@uw.eduCristine M Trahms, MS, RD, FADACristine M Trahms, MS, RD, FADA

Newborn ScreeningNewborn Screening
A state mandated A state mandated public health program public health program that begins with a that begins with a “heel poke” “heel poke” for every for every baby before hospital dischargebaby before hospital discharge
First screen must be taken 24-48 hours First screen must be taken 24-48 hours of life regardless of feeding status or of life regardless of feeding status or weightweight
Blood Sample on Guthrie Filter Paper Card

Who is screened?Who is screened?
Washington State law requires that every Washington State law requires that every newborn be tested prior to discharge from newborn be tested prior to discharge from the hospital or within five days of agethe hospital or within five days of age
Second screen strongly recommended Second screen strongly recommended between 7 and 14 days of age)between 7 and 14 days of age)
Third screen recommended for sick and Third screen recommended for sick and premature infantspremature infants

Why do newborn screening?Why do newborn screening?
Screen a presumably Screen a presumably healthy newborn healthy newborn populationpopulation
Detect disease before Detect disease before symptoms present symptoms present clinicallyclinically
Goal: Prevent or reduce Goal: Prevent or reduce morbidity and mortalitymorbidity and mortality

Criteria for Newborn ScreeningCriteria for Newborn Screening
Important conditionImportant condition
Acceptable treatment availableAcceptable treatment available
Facilities for diagnosis and treatmentFacilities for diagnosis and treatment
Difficult to recognize earlyDifficult to recognize early
Suitable screening testSuitable screening test
Natural history knownNatural history known
Cost-effective to diagnose and treatCost-effective to diagnose and treat
Wilson & Jungner, 1968

Tandem Mass Spectrometry (MS/MS) Tandem Mass Spectrometry (MS/MS) High Impact and High ThroughputHigh Impact and High Throughput
One disease, one test is not cost-effectiveOne disease, one test is not cost-effective
Many diseases, one test is cost-effectiveMany diseases, one test is cost-effective
MS/MS allows for rapid, simultaneous MS/MS allows for rapid, simultaneous analysis and detection of many disorders analysis and detection of many disorders of amino acid, organic acid, and fatty acid of amino acid, organic acid, and fatty acid metabolismmetabolism

Tandem Mass Spectrometer (MS/MS)

MS/MS MethodologyMS/MS Methodology
Blood spots punched (3/16Blood spots punched (3/16thth inch disc) inch disc)Stable isotope internal standards added Stable isotope internal standards added (deuterated)(deuterated)Butyl esters derivatives madeButyl esters derivatives madeAutomatic injection into MS/MS via 96 well Automatic injection into MS/MS via 96 well platesplatesSample set up determines which masses and Sample set up determines which masses and therefore which compounds are detectedtherefore which compounds are detected2 minute analysis time2 minute analysis timeAutomated data processing for resultsAutomated data processing for results

MS/MS Methodology – continued MS/MS Methodology – continued
Compounds analyzed are amino acids Compounds analyzed are amino acids and acylcarnitinesand acylcarnitines Amino acids – to identify PKU, MSUD, Amino acids – to identify PKU, MSUD,
homocystinuriahomocystinuria Acylcarnitine – carnitine (vehicle) + fatty Acylcarnitine – carnitine (vehicle) + fatty
acid for identification of organic acid for identification of organic acidurias and fatty acid oxidation acidurias and fatty acid oxidation disordersdisorders

+Prec (85.10): 0.401 to 1.202 min from Sample 9 (BADER) of AC 101003 DATA.wiff (Turbo Spray... Max. 3.5e4 cps.
260 280 300 320 340 360 380 400 420 440 460 480 500m/z, amu
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Re
l. In
t. (%
)
*
* * * *
*
C2
100%
Inte
ns
ity
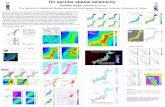
* internal standards
Control
+Prec (85.10): 0.401 to 1.202 min from Sample 8 (PATE) of AC 101003 DATA.wiff (Turbo Spray) Max. 3.8e4 cps.
260 280 300 320 340 360 380 400 420 440 460 480 500m/z, amu
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Re
l. In
t. (%
)
Inte
ns
ity
100%
*
* * *
*
*
MCAD
C2
C16
C8
C10:1C6
MS/MS Plasma Acylcarnitines MS/MS Plasma Acylcarnitines

MS/MS Plasma Amino AcidsMS/MS Plasma Amino Acids

What is the scope of newborn screening?What is the scope of newborn screening?
Screen ~80,000 newborns
Receive ~160,000 specimens
Track ~3000 infants with abnormal results
Prevent ~140 babies from death or disability
For example: In WA State

Which disorders should be Which disorders should be identified?identified?
NBS mandates are under state controlNBS mandates are under state control Some states screened for 3 diseases, others Some states screened for 3 diseases, others
40+40+
2002 Maternal and Child Health Bureau 2002 Maternal and Child Health Bureau commissioned ACMGcommissioned ACMG Analyze literatureAnalyze literature Develop consensus on which disordersDevelop consensus on which disorders Recommend a core panel to create uniform Recommend a core panel to create uniform
NBS across all statesNBS across all states





Historical Harm (?)Historical Harm (?)Early PKU screening led to cases of over-Early PKU screening led to cases of over-restriction and/or implementation of diet restriction and/or implementation of diet prior to confirmation of diagnosisprior to confirmation of diagnosis Today, diagnosis is quite rapidToday, diagnosis is quite rapid 40 years ago, it took much longer so more 40 years ago, it took much longer so more
potential for harmpotential for harm
However, no published evidence of wide-However, no published evidence of wide-spread physical/medical harmspread physical/medical harmBUT the cases do underscore need for BUT the cases do underscore need for expertise and resources for managementexpertise and resources for management

Amino Acid DisordersAmino Acid Disorders
AA that are not used to AA that are not used to make proteins are make proteins are recycled by their specific recycled by their specific metabolic pathways. metabolic pathways.
Enzymatic deficiencies in Enzymatic deficiencies in these pathways lead to these pathways lead to various clinical various clinical phenotypes.phenotypes.
Diagnosed by plasma Diagnosed by plasma amino acids, urine amino amino acids, urine amino acids, and/or urine acids, and/or urine organic acids (takes 2-5 organic acids (takes 2-5 days)days)
PKU: severe, permanent IDPKU: severe, permanent IDMSUD: ID, hallucinations, MSUD: ID, hallucinations, ataxiaataxiaHCY: connective tissue HCY: connective tissue damage (joints, heart), ID, damage (joints, heart), ID, psychiatric disturbancespsychiatric disturbancesCIT: risk of hyperammonemia CIT: risk of hyperammonemia ID, coma, death ID, coma, deathASA: brittle hair, liver disease ASA: brittle hair, liver disease IDIDTYR I: acute or chronic liver TYR I: acute or chronic liver disease, liver cancer, disease, liver cancer, neurologic pain crisesneurologic pain crises

Organic Acid DisordersOrganic Acid Disorders
Organic acids are Organic acids are breakdown products of breakdown products of protein and fatty acid protein and fatty acid metabolism. Defects in metabolism. Defects in their breakdown lead to their breakdown lead to (generally):(generally):
Vomiting, metabolic Vomiting, metabolic acidosis, elevated acidosis, elevated ammonia in crisesammonia in crises
ID, motor delay, ataxia, ID, motor delay, ataxia, cardiac/renal/pancreatic cardiac/renal/pancreatic problemsproblems
Diagnosed by urine Diagnosed by urine organic acids and/or organic acids and/or plasma acylcarnitinesplasma acylcarnitines
IVA: Isovaleric acidemiaIVA: Isovaleric acidemiaGA I: Glutaric acidemia type IGA I: Glutaric acidemia type IHMG: 3-OH 3-CH3 glutaric HMG: 3-OH 3-CH3 glutaric aciduriaaciduriaMCD: Multiple carboxylase MCD: Multiple carboxylase deficiencydeficiencyMUT: Methylmalonic acidemia MUT: Methylmalonic acidemia (mutase deficiency)(mutase deficiency)3MCC: 3-Methylcrotonyl-CoA 3MCC: 3-Methylcrotonyl-CoA carboxylase deficiencycarboxylase deficiencyCbl A,B: Methylmalonic Cbl A,B: Methylmalonic acidemiaacidemiaPROP: Propionic acidemiaPROP: Propionic acidemiaBKT: Beta-ketothiolase BKT: Beta-ketothiolase deficiencydeficiency

Fatty acid disorders lead Fatty acid disorders lead to impaired energy to impaired energy productionproduction
Hypoglycemia, Hypoglycemia, cardiomyopathy, muscle cardiomyopathy, muscle weakness can be seenweakness can be seen
Diagnosed by plasma Diagnosed by plasma acylcarnitines, and urine acylcarnitines, and urine organic acids can be organic acids can be helpfulhelpful
MCAD: Medium-chain MCAD: Medium-chain acyl-CoA dehydrogenase acyl-CoA dehydrogenase deficiencydeficiencyVLCAD: Very long-chain VLCAD: Very long-chain acyl-CoA dehydrogenase acyl-CoA dehydrogenase deficiencydeficiencyLCHAD: Long-chain L-3-LCHAD: Long-chain L-3-OH acyl-CoA OH acyl-CoA dehydrogenase dehydrogenase deficiencydeficiencyTFP: Trifunctional protein TFP: Trifunctional protein deficiencydeficiencyCUD: Carnitine uptake CUD: Carnitine uptake defectdefect
Fatty Acid DisordersFatty Acid Disorders

Who is identified?Who is identified?
1.1. Patients who need active managementPatients who need active management Symptomatic at diagnosisSymptomatic at diagnosis Strong evidence of pathology if untreatedStrong evidence of pathology if untreated Examples: PKU, classic galactosemia, Examples: PKU, classic galactosemia,
MSUD, PROP, etc.MSUD, PROP, etc.

Who is identified?Who is identified?
2.2. Patients with disorders known to pose Patients with disorders known to pose risk but reduced penetrancerisk but reduced penetrance
i.e., probably not everyone needs to be i.e., probably not everyone needs to be treatedtreated
HPHE, MCADHPHE, MCAD Both are/have mild ends of the spectrum Both are/have mild ends of the spectrum
that have only been identified through NBSthat have only been identified through NBS MCAD mutation c.199 C>TMCAD mutation c.199 C>T
Never seen in patients picked up clinicallyNever seen in patients picked up clinically

Who is identified?Who is identified?
3.3. Patients who may not need any Patients who may not need any managementmanagement
Disorders considered extremely rare but Disorders considered extremely rare but seen in large numbers via NBS programsseen in large numbers via NBS programs
Reported cases have significant morbidityReported cases have significant morbidity
NBS pickups are mostly mildNBS pickups are mostly mild
3MCC, SCAD3MCC, SCAD Biochemical phenotypeBiochemical phenotype

Proceeding with CautionProceeding with Caution(Reasons to be Thoughtful)(Reasons to be Thoughtful)
Proceeding with caution Proceeding with caution Not screening Not screening
Core diseases vs. secondary targets / Core diseases vs. secondary targets / unintended targetsunintended targets What is reported vs. withheld?What is reported vs. withheld? Will we pick up untreatable conditions?Will we pick up untreatable conditions? What is the impact of false positives on families?What is the impact of false positives on families?
No long-term outcome data – consider research No long-term outcome data – consider research paradigmparadigm
Consider infrastructure needed for follow-upConsider infrastructure needed for follow-up

What are we screening for?What are we screening for?
9 OA 9 OA 5 FAO5 FAO 6 AA6 AA 3 Hb Pathies3 Hb Pathies 6 Others6 Others
CORE PANELCORE PANEL
IVAIVAGA IGA IHMGHMGMCDMCDMUTMUT3MCC3MCCCbl A,BCbl A,BPROPPROPBKTBKT
MCADMCADVLCADVLCADLCHADLCHADTFPTFPCUDCUD
PKUPKUMSUDMSUDHCYHCYCITCITASAASATYR ITYR I
Hb SSHb SSHb S/ßThHb S/ßThHb S/CHb S/C
CHCHBIOTBIOTCAHCAHGALTGALTHEARHEARCFCF

How many infants does NBS identify?How many infants does NBS identify?
20062006 20072007 Infants DiagnosedInfants Diagnosed
22 11 Biotinidase deficiencyBiotinidase deficiency
55 55 Congenital adrenal hypoplasia (CAH)Congenital adrenal hypoplasia (CAH)
4545 4545 Congenital hypothyroidism (CH)Congenital hypothyroidism (CH)
1212 1414 Cystic fibrosisCystic fibrosis
66 00 GalactosemiaGalactosemia
11 00 HomocystinuriaHomocystinuria
00 00 Maple syrup urine diseaseMaple syrup urine disease
33 66 Medium chain acyl coA dehydrogenase (MCAD) def.Medium chain acyl coA dehydrogenase (MCAD) def.
77 77 Phenylketonuria (PKU)Phenylketonuria (PKU)
1313 2323 Sickle cell and other HGSickle cell and other HG
9595 112112 TOTALTOTAL

EmmaEmma
13 months old, healthy13 months old, healthyNormal pregnancy and deliveryNormal pregnancy and deliveryNormal eating pattern, no allergies or Normal eating pattern, no allergies or intolerancesintolerancesFeb 2008: Feb 2008: Vomited 4-5 times throughout the weekendVomited 4-5 times throughout the weekend No feverNo fever Sleeping for extended periods – parents concerned, Sleeping for extended periods – parents concerned,
but previous fever had same patternbut previous fever had same pattern Parents gave PedialyteParents gave Pedialyte

EmmaEmma
4½ yo brother, parents sick on 4½ yo brother, parents sick on Sunday/Monday; same symptomsSunday/Monday; same symptoms
Monday night 9:30 checked on EmmaMonday night 9:30 checked on Emma Raspy breathing – thought respiratory Raspy breathing – thought respiratory
problem but not worriedproblem but not worried
Tuesday morning 11 am she was found Tuesday morning 11 am she was found motionless in her crib and pronounced motionless in her crib and pronounced dead at the scenedead at the scene

EmmaEmma
Autopsy revealed fatty changes to liverAutopsy revealed fatty changes to liver
Coroner requested newborn screening Coroner requested newborn screening blood spot be sent for acylcarnitine profileblood spot be sent for acylcarnitine profile
Diagnostic for very long chain acyl-co A Diagnostic for very long chain acyl-co A dehydrogenase deficiency (VLCAD) dehydrogenase deficiency (VLCAD)

VLCADVLCAD
Disorder of long chain fatty acid Disorder of long chain fatty acid breakdownbreakdown
C14, C14:1C14, C14:1 C16, C18 C16, C18
Normal beta oxidation occurs in Normal beta oxidation occurs in mitochondriamitochondria

http://www.genomeknowledge.org/figures/saturatedbetao.jpg
Fatty Acid OxidationFatty Acid Oxidation

Hypertrophic cardiomyopathy, with Hypertrophic cardiomyopathy, with hypoglycemia and skeletal myopathy, lethargy, hypoglycemia and skeletal myopathy, lethargy, failure to thrivefailure to thrive Usually present birth to 5 monthsUsually present birth to 5 months
Hypoglycemia, hepatomegaly, muscle weakness Hypoglycemia, hepatomegaly, muscle weakness without cardiac manifestationswithout cardiac manifestations Late infancy – older childhoodLate infancy – older childhood
Muscle weakness/pain, rhabdomyolysis with Muscle weakness/pain, rhabdomyolysis with exercise or illness. No hypoglycemia or cardiacexercise or illness. No hypoglycemia or cardiac Teens to adulthoodTeens to adulthood
VLCAD PresentationsVLCAD Presentations

Diet low in long-chain fats (Portagen, Diet low in long-chain fats (Portagen, Monogen = 87%, 90% of fats as MCT)Monogen = 87%, 90% of fats as MCT)
Additional medium chain fats (MCT oil, Additional medium chain fats (MCT oil, walnut oil)walnut oil)
Carnitine 100 mg/kg/day Carnitine 100 mg/kg/day
Avoidance of fastingAvoidance of fasting
Treating illness with IV glucose supportTreating illness with IV glucose support
VLCAD TreatmentVLCAD Treatment

Newborn screeningNewborn screening
Plasma acylcarnitine profilePlasma acylcarnitine profile
Urine organic acids (should be normal)Urine organic acids (should be normal)
DNA sequencingDNA sequencing
VLCAD DiagnosisVLCAD Diagnosis

Family referred to genetics by coronerFamily referred to genetics by coroner
Parents requested testing for older brother Parents requested testing for older brother (Zach)(Zach)
Acylcarnitine orderedAcylcarnitine ordered
DNA sequencing of ACADVL gene DNA sequencing of ACADVL gene orderedordered
Emma’s FamilyEmma’s Family

C14:1
C16:1- nl
C14 C16 - nl
Acylcarnitine – Zach (5 yo)Acylcarnitine – Zach (5 yo)

Reported: mild elevation of C14 and C14:1 Reported: mild elevation of C14 and C14:1 with low free carnitine. VLCAD cannot be with low free carnitine. VLCAD cannot be ruled out ruled out Recommend supplementing with carnitine Recommend supplementing with carnitine and retest in 1 weekand retest in 1 weekDNA testing results back before AC DNA testing results back before AC repeat: Zach’s DNA testing reveals he is repeat: Zach’s DNA testing reveals he is affectedaffectedFamily seen in clinic, started on treatmentFamily seen in clinic, started on treatment
Zach TestingZach Testing

5 yo5 yoHealthyHealthyNo symptoms of muscle weaknessNo symptoms of muscle weakness
CPK = 315U/L (35-230)CPK = 315U/L (35-230)
No hepatomegalyNo hepatomegaly AST= 49 (5-41)AST= 49 (5-41) ALT= 23 ALT= 23 Bilirubin conj, unconj = normal (0.0, 0.4)Bilirubin conj, unconj = normal (0.0, 0.4)
No evidence of cardiac involvementNo evidence of cardiac involvementHas had several viral illnesses in his lifetime without Has had several viral illnesses in his lifetime without difficultydifficultyOnce on carnitine, AC profile was classic for VLCADOnce on carnitine, AC profile was classic for VLCAD
Zach – Clinical PictureZach – Clinical Picture

Sampling Sampling hospital partnershipshospital partnerships
Screening Screening State LabState Lab
Reporting Reporting to health care providerto health care provider
Referral Referral to specialty care providerto specialty care provider
Short term follow-up Short term follow-up diagnosisdiagnosis
Long term follow-up Long term follow-up ongoing treatment & monitoringongoing treatment & monitoring
Components of Newborn ScreeningComponents of Newborn Screening

Birth
Day 1 First Screen
+NL ++
DX
TX
Long term Follow up
2nd Sample
+
DX
TX
NL
Primary Care Doctor/ Biochem ClinicASAP
•Timely/urgent•Systematic process
Primary Doctor
Primary Care DoctorBiochem Clinic
Long term Follow up
Washington StateWashington StateNewborn ScreeningNewborn Screening

Informed Informed ConsentConsent
Effective NBS requires a close working relationship between hospitals, newborn screening program, and follow-up program

Supporting understanding for Supporting understanding for familiesfamilies

Nutrition Involvement in NBSNutrition Involvement in NBS
PolicyPolicy
Diagnostic/coordinationDiagnostic/coordination
ClinicalClinical
CommunityCommunity

Example: infant with galactosemiaExample: infant with galactosemia
Symptoms in newborn, if Symptoms in newborn, if untreateduntreated
Vomiting, diarrheaVomiting, diarrhea Hyperbilirubinemia, hepatic Hyperbilirubinemia, hepatic
dysfunction, hepatomegalydysfunction, hepatomegaly Renal tubular dysfunctionRenal tubular dysfunction CataractsCataracts EncephalopathyEncephalopathy E. coli septicemia resultE. coli septicemia result Death within 6 weeks, if Death within 6 weeks, if
untreateduntreated
AlsoAlso Duarte variantDuarte variant galactokinase deficiencygalactokinase deficiency uridine diphosphate-uridine diphosphate-
galactose-4-epimerase galactose-4-epimerase deficiencydeficiency
Galactose-1-phosphate uridyl transferase (GALT) deficiency

Example: infant with galactosemiaExample: infant with galactosemia
Primary source is milk Primary source is milk (lactose= galactose + (lactose= galactose + glucose)glucose)
Secondary sources are Secondary sources are legumeslegumes
Minor? sources are fruits Minor? sources are fruits and vegetablesand vegetables
Food labelsFood labels milk, casein, milk solids, milk, casein, milk solids,
lactose, whey, hydrolyzed lactose, whey, hydrolyzed protein, lactalbumin, protein, lactalbumin, lactostearin, caseinatelactostearin, caseinate
Medications Medications (lactose is often (lactose is often an inactive ingredient)an inactive ingredient)
Dietary supplementsDietary supplements
Artificial sweetenersArtificial sweeteners
Monitoring: galactose-1-phosphate levels <3-4 mg/dlMonitoring: galactose-1-phosphate levels <3-4 mg/dl
Treatment: eliminate all galactose from dietTreatment: eliminate all galactose from diet

Example: Infant with galactosemiaExample: Infant with galactosemia
POLICY
RD participated on State Advisory Board to select disorders, including galactosemia
DIAGNOSIS & COOORDINATION
“Presumptive positive” RD in contact with family and local providers to discuss appropriate feeding practices and arrange clinic appointment
CLINICAL MANAGEMENT
RD provides nutrition care as member of the Biochemical Genetics Team:
•Initiation of formula
•Guidelines for monitoring intake
•Plans for follow-up
RD as case manager
COMMUNITY
RD at local health department provides ongoing education to family, local care providers

Nutrition and NBS: PolicyNutrition and NBS: Policy
Screening process (disorders, procedures) Screening process (disorders, procedures) RD participated in Advisory Board meetings, providing input about RD participated in Advisory Board meetings, providing input about nutrition-related treatmentnutrition-related treatment
Services and reimbursementServices and reimbursementNutrition consultant to state CSHCN ProgramNutrition consultant to state CSHCN Program
RD provides input about relevant state Medicaid policiesRD provides input about relevant state Medicaid policies
Training and educationTraining and educationRD provides information about management of metabolic disorders RD provides information about management of metabolic disorders to local WIC agenciesto local WIC agencies

Nutrition and NBS: Clinical Nutrition and NBS: Clinical Management – PKUManagement – PKU
PhenylketonuriaPhenylketonuria Phenylalanine hydroxylasePhenylalanine hydroxylase Dihydropteridine reductaseDihydropteridine reductase Biopterin synthetaseBiopterin synthetase
Establish diagnosisEstablish diagnosis Presumptive positive Presumptive positive
NBS resultsNBS results> 3 mg/dL, >24 hrs of age> 3 mg/dL, >24 hrs of age
Differential diagnosisDifferential diagnosis serum phe, nl tyrserum phe, nl tyr
r/o DHPR, biopterin r/o DHPR, biopterin defectsdefects

Current Treatment GuidelinesCurrent Treatment Guidelines
With effective NBS, children are identified With effective NBS, children are identified by 7 days of ageby 7 days of age
Initiate treatment immediatelyInitiate treatment immediately
Maintain phe levels 1-6 mg/dl (60-360 Maintain phe levels 1-6 mg/dl (60-360 umol/L)umol/L)
Lifelong treatmentLifelong treatment

Outcome ExpectationsOutcome Expectations
With NBS and blood With NBS and blood phenylalanine levels phenylalanine levels consistently in the consistently in the treatment rangetreatment range
Normal IQ and physical Normal IQ and physical growth are expectedgrowth are expected
With delayed diagnosis or With delayed diagnosis or consistently elevated consistently elevated blood levelsblood levels
IQ is diminished and IQ is diminished and physical growth is physical growth is compromisedcompromised

Clinical Management: PKUClinical Management: PKU
Goals of Nutrition TherapyGoals of Nutrition Therapy
Normal growth rateNormal growth rate
Normal physical Normal physical developmentdevelopment
Normal cognitive Normal cognitive developmentdevelopment
Normal nutritional statusNormal nutritional status

Clinical Management: PKUClinical Management: PKU
Correct substrate Correct substrate imbalanceimbalance Restrict phenylalanine Restrict phenylalanine
intake to normalize intake to normalize plasma concentrationplasma concentration
Supply product of Supply product of reactionreaction Supplement tyrosine Supplement tyrosine
to maintain normal to maintain normal plasma tyrosine levelsplasma tyrosine levels
Phenylalanine -------------------//----------------------- Tyrosine
(substrate) phenylalanine hydroxylase (product)

Phe Levels from NBS to TxPhe Levels from NBS to Tx
Blood levels every 2 daysbecause of rapid growth
Equilibrium achieved by 14 days of age
Diagnostic levels

Adjustments necessary to maintain Adjustments necessary to maintain “safe” blood phe levels“safe” blood phe levels
Usual intake of pheUsual intake of phe Newborn on formulaNewborn on formula
20 oz x 22 mg phe/oz = 20 oz x 22 mg phe/oz = 440 mg phe440 mg phe 1 yo child on “regular” diet1 yo child on “regular” diet
30 g protein = 30 g protein = 1500 mg phe1500 mg phe (DRI = 13.5 g) (DRI = 13.5 g) 7 yo child on “regular” diet7 yo child on “regular” diet
50 g protein = 50 g protein = 2500 mg phe2500 mg phe (DRI = 19 g) (DRI = 19 g)
Phenylalanine requirementPhenylalanine requirement 250 mg/d250 mg/d

Management ToolsManagement Tools
Specialized formula Specialized formula providesprovides 80-90% energy intake80-90% energy intake 89-90% protein intake89-90% protein intake tyrosine supplementstyrosine supplements no phenylalanineno phenylalanine
Phenylalanine to meet Phenylalanine to meet requirement from infant requirement from infant formula or foodsformula or foods

Food Choices for PKUFood Choices for PKU

Effect of a single amino acid Effect of a single amino acid deficiency on growthdeficiency on growth

Effective Blood Level Management Effective Blood Level Management in Childhoodin Childhood
Blood levels once per month, or more frequently if needed for good management

Age of Child Tasks for Children and Parents 0-6 months Parents learn about and adjust to PKU 6 months Start low-protein solid foods 6-7 months Introduce cup 8-9 months Introduce finger foods 10-15 months Consider weaning from bottle (discuss transition with clinic staff) 2-3 years Learn the concept of “formula first”
Learn to distinguish “yes” and “no” foods 4-5 years Begin to learn to count foods – “how many”
Begin to use scale – “how much” 5-6 years Assist in formula preparation
Teach children how to deal with other children’s curiosity about PKU 7-10 years Prepare formula with decreasing supervision
Choose after school snack Learn to pack school lunch Begin to list foods on food record Begin weighing food regularly on scale
10-12 years Begin to prepare and consume formula independently each day (with parental monitoring)
Prepare simple entrees independently Know what blood levels are ideal
13-14 years Increasing self-monitoring (with continued parent support) in formula preparation and consumption
Independently manage total phenylalanine intake for the day Learn menu planning Responsible for food records
15-17 years Responsible for all aspects of self-management Able to do ‘finger poke’ for blood test Able to explain basics of PKU – “What is it?” Responsible for remembering recent blood levels Continued parent support
18 years Transition to adult-based clinic care Ready to live independently, including: -formula preparation and consumption -food preparation and records -monthly serum phenylalanine levels
PKU PKU Management Management
GuidelinesGuidelines
Self-Self-management management
SkillsSkills

Goal of Lifetime Management of Goal of Lifetime Management of PKUPKU
To maintain metabolic To maintain metabolic balance while providing balance while providing adequate nutrients and adequate nutrients and energy for normal energy for normal physical and intellectual physical and intellectual growthgrowth

Maternal PKU Concerns/OutcomesMaternal PKU Concerns/Outcomes
Women with PKU are at high risk for delivering a Women with PKU are at high risk for delivering a damaged infantdamaged infant Placenta concentrates phe 2-4xPlacenta concentrates phe 2-4x
MicrocephalyMicrocephaly
Cardiac problemsCardiac problems
Infant IQ directly related to maternal blood phe Infant IQ directly related to maternal blood phe levellevel
Outcome improved with maternal blood phe <2 Outcome improved with maternal blood phe <2 mg/dl prior to conception and during pregnancymg/dl prior to conception and during pregnancy

Nutrition and NBS: CommunityNutrition and NBS: Community
PHN and interpreter make PHN and interpreter make monthly visits to family of monthly visits to family of young child with MSUD. young child with MSUD.
Through pre-arranged Through pre-arranged phone calls, we can discuss phone calls, we can discuss formula composition and formula composition and preparation, and solid foods.preparation, and solid foods.
This helps provide This helps provide information between regular information between regular clinic visits.clinic visits.

Nutrition and NBS: CommunityNutrition and NBS: Community
A woman with PKU is enrolled in the First Steps A woman with PKU is enrolled in the First Steps program (WA State MSS).program (WA State MSS).
The RD with PKU Clinic provides consultation to The RD with PKU Clinic provides consultation to the First Steps RD, about management of amino the First Steps RD, about management of amino acid levels.acid levels.

Metabolic TeamMetabolic TeamChildChild Age-appropriate self-management skillsAge-appropriate self-management skills
ParentsParents Monitoring health status, teaching, advocacyMonitoring health status, teaching, advocacy
NutritionistNutritionist Nutrition therapy, feeding skillsNutrition therapy, feeding skills
GeneticistGeneticist Medical monitoringMedical monitoring
Social WorkerSocial Worker Family support, counselingFamily support, counseling
LabLab Laboratory monitoringLaboratory monitoring
Medical HomeMedical Home Well child care, family supportWell child care, family support
PsychologistPsychologist Developmental monitoring, counselingDevelopmental monitoring, counseling
PHN, othersPHN, others Family support in communityFamily support in community
SchoolSchool Educational programs, treatment monitoringEducational programs, treatment monitoring
CommunityCommunity Support of family and friendsSupport of family and friends
Therapists (OT, Therapists (OT, PT, SLP, etc.)PT, SLP, etc.)
Developmental monitoring, interventionDevelopmental monitoring, intervention

NBS and the Community: NBS and the Community: ChallengesChallenges
Understand the implications of the results Understand the implications of the results of newborn screening testsof newborn screening tests
Develop a communication system Develop a communication system between the community providers and the between the community providers and the metabolic team for support of treatmentmetabolic team for support of treatment
Interact with PCPs and families as Interact with PCPs and families as needed, to support appropriate MNTneeded, to support appropriate MNT

NBS and the Community:NBS and the Community:What you need to knowWhat you need to know
Which disorders are identified by NBS in your Which disorders are identified by NBS in your state? Where do you find this information?state? Where do you find this information?
What is the difference between What is the difference between screening screening and and diagnostic resultsdiagnostic results??
What is the system for follow-up of presumptive What is the system for follow-up of presumptive positive NBS results?positive NBS results?
How do you make referrals to regional genetics How do you make referrals to regional genetics clinics and specialty care clinics?clinics and specialty care clinics?

Scenes from the Scenes from the Annals of Reporting Annals of Reporting and Acting on NBS Resultsand Acting on NBS Results
A primary care physician telephones are reports A primary care physician telephones are reports there is a new baby with PKU and asks that you there is a new baby with PKU and asks that you please start the infant on formula ASAP.please start the infant on formula ASAP.
What additional information do What additional information do you need?you need?
What would you do?What would you do?

Scenes from the Scenes from the Annals of Reporting Annals of Reporting and Acting on NBS Resultsand Acting on NBS Results
You are on-call for the weekend for your local You are on-call for the weekend for your local hospital and you receive an order from the hospital and you receive an order from the newborn nursery on an infant with presumptive newborn nursery on an infant with presumptive galactosemia and a request for the initiation of galactosemia and a request for the initiation of treatment.treatment.
What additional information What additional information do you need?do you need?
What would you do?What would you do?

SummarySummary
NBS is the first part of a process NBS is the first part of a process of care that requires strong of care that requires strong partnerships for optimal partnerships for optimal outcomes outcomes
NBS outcomes are only as good NBS outcomes are only as good as the follow-up providedas the follow-up provided
Families should have access to Families should have access to the best treatment and care for the best treatment and care for their childtheir child

SummarySummary
Specific diagnosis must be confirmed Specific diagnosis must be confirmed in coordination with the state Newborn Screening in coordination with the state Newborn Screening
ProgramProgram
Careful monitoring of medical and nutritional Careful monitoring of medical and nutritional status must be on-going status must be on-going by the metabolic teamby the metabolic team
Nutritional intervention Nutritional intervention must be specific to the disorder must be specific to the disorder specific to the childspecific to the child

Additional InformationAdditional Information
Washington State Newborn Screening Washington State Newborn Screening http://http://www.doh.wa.gov/ehsph/phl/newborn/default.htmwww.doh.wa.gov/ehsph/phl/newborn/default.htm National Newborn Screening and Genetics Resource Center National Newborn Screening and Genetics Resource Center http://genes-http://genes-r-us.uthscsa.edur-us.uthscsa.eduStar G-Screening, Technology, and Research in Genetics Star G-Screening, Technology, and Research in Genetics http://newbornscreening.infohttp://newbornscreening.info
Building Block for LifeBuilding Block for Life (PNPG) (PNPG) Expanded NBS – 27(1)Expanded NBS – 27(1) Genetics and Expanded NBS – 30(3)Genetics and Expanded NBS – 30(3)
Nutrition FocusNutrition Focus Overview nutr assessment of children with metabolic disorders – 24(5)Overview nutr assessment of children with metabolic disorders – 24(5) Genetics – 22(6)Genetics – 22(6)
Journal of Developmental and Behavioral PediatricsJournal of Developmental and Behavioral Pediatrics Levy PA. An overview of newborn screening. 2010;31(7):622.Levy PA. An overview of newborn screening. 2010;31(7):622.

Why do we do newborn screening?Why do we do newborn screening?
So Super Girl can be So Super Girl can be whoever she wants to whoever she wants to be….be….