Exercise Progression Strategies for the Knee & Shoulder · Rest: 30-90 seconds ... Tip: Add towel...
27
8/28/2013 1 Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach Eric J. Chaconas Morey J. Kolber Exercise Progression Strategies for the Knee & Shoulder Eric J. Chaconas, PT, DPT, CSCS, FAAOMPT Morey J. Kolber, PT, PhD, OCS,CSCS Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach Eric J. Chaconas Morey J. Kolber Course Objectives • Recall evidence-based implications for incorporating specific exercise strategies to the shoulder and knee in clinical practice. • Discuss the principles of exercise dosing and prescription. • Examine clinical and basic science research related to exercise progression at the shoulder and knee. • Recognize appropriate rehabilitation exercises for the shoulder and knee. Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach Eric J. Chaconas Morey J. Kolber Exercise • Load placed on the body in order to achieve a physiological response • Goal: functional movement pattern improvement – Motor Control – “Timing” “Activation” – Strength: eccentric, concentric, isometric – Hypertrophy – Power – Speed – Endurance
-
Upload
trinhduong -
Category
Documents
-
view
216 -
download
1
Transcript of Exercise Progression Strategies for the Knee & Shoulder · Rest: 30-90 seconds ... Tip: Add towel...
8/28/2013
1
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Exercise Progression Strategies
for the Knee & Shoulder
Eric J. Chaconas, PT, DPT, CSCS, FAAOMPT
Morey J. Kolber, PT, PhD, OCS,CSCS
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Course Objectives
• Recall evidence-based implications for incorporating specific exercise strategies to the shoulder and knee in clinical practice.
• Discuss the principles of exercise dosing and prescription.
• Examine clinical and basic science research related to exercise progression at the shoulder and knee.
• Recognize appropriate rehabilitation exercises for the shoulder and knee.
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Exercise• Load placed on the body in order to achieve a
physiological response
• Goal: functional movement pattern improvement
– Motor Control
– “Timing” “Activation”
– Strength: eccentric, concentric, isometric
– Hypertrophy
– Power
– Speed
– Endurance
8/28/2013
2
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber 4
Other Benefits to Consider
• Reversing pathophysiology
• Stress/injury tolerance
• Desensitization
• Reduce fear of movement
• Reducing systemic disease risk factors
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Treatment Progression
Mobility and Palliative Care
Motor Control, Strength, Proprioception
Endurance, Power, Functional
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber 6
Considerations
• Patient goals
• Tissue healing
• Bio-psychosocial variables (coping skills)
• Limitations (i.e. number of treatment sessions)
8/28/2013
3
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Exercise Order
• Complex movements first– Fatigue will impair movement patterns
– Warm up exercises should be very short in duration
• Exercise order example: ACL rehab 6 weeks post surgery– Squat 2 x 8
– Leg Press 3 x 15
– Single leg proprioception training 3 x 45 seconds
– Side stepping with resistance band 30 feet x 4
– Side plank 2 x 1 minute
– Straight leg raise 3 x 25
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Intensity
• Inversely related to duration of rest period
• Can not increase intensity without sacrificing
some other parameter
– i.e. higher intensity = lower volume
• Intensity should be modified based upon
specific exercise goal
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Frequency
• Most common parameter that is arbitrarily chosen
– i.e. 3 times per week, home exercise program every day
• Total session volume
• Frequency must match the goal of the exercise
program
– Reversing inhibition
– Motor control/movement re-learning
– Strength development
– Power development

8/28/2013
4
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Dosing Strategies
• What are your goals?
–Timing or activation?
–Strength vs. endurance vs. power vs. hypertrophy?
– Is there atrophy?
–What muscle fiber type needs to be recruited?
–What about bioenergetics?
–How will you know you are dosing correctly?
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Resistance Training Variables
Power Intensity:75-90% 1RM
Sets: 3-5
Repetitions: 1-5
Rest: 2-5 min
Strength Intensity:> 85%1RM
Sets: 2-6
Repetition: 6
Rest: 2-5 min
Hypertrophy Intensity:67-85%1RM
Sets: 3-6
Repetition: 6-12
Rest: 30-90 seconds
Endurance Intensity:< 67%1RM
Sets: 2-3
Repetition: 12
Rest: 30 sec
*Rest = between sets & exercises
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Muscle Performance Impairments
Ideal goals for exercise selection:
•Maximal activation
•Maximal isolation
Reality:
• Exercises that maximally activate: perpetuate imbalances
Early rehabilitation needs:
• Exercises that activate (timing) key muscles
• Minimize undesirable recruitment
Late rehabilitation:
• Maximal activation
8/28/2013
5
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
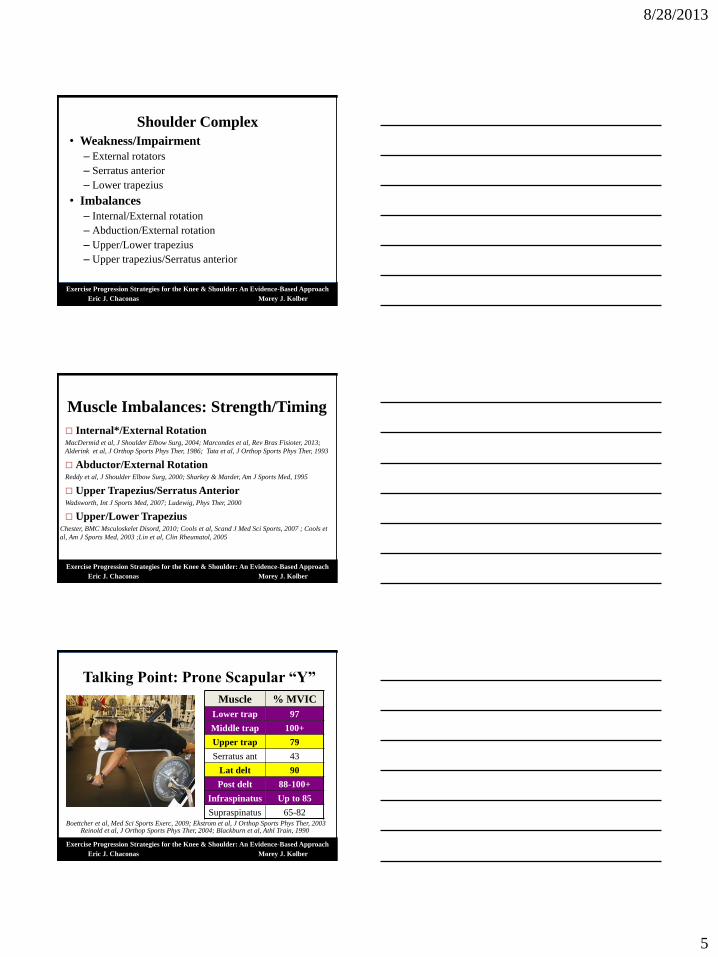
Shoulder Complex
• Weakness/Impairment
– External rotators
– Serratus anterior
– Lower trapezius
• Imbalances
– Internal/External rotation
– Abduction/External rotation
– Upper/Lower trapezius
– Upper trapezius/Serratus anterior
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Muscle Imbalances: Strength/Timing
Internal*/External RotationMacDermid et al, J Shoulder Elbow Surg, 2004; Marcondes et al, Rev Bras Fisioter, 2013;
Alderink et al, J Orthop Sports Phys Ther, 1986; Tata et al, J Orthop Sports Phys Ther, 1993
Abductor/External RotationReddy et al, J Shoulder Elbow Surg, 2000; Sharkey & Marder, Am J Sports Med, 1995
Upper Trapezius/Serratus AnteriorWadsworth, Int J Sports Med, 2007; Ludewig, Phys Ther, 2000
Upper/Lower TrapeziusChester, BMC Msculoskelet Disord, 2010; Cools et al, Scand J Med Sci Sports, 2007 ; Cools et
al, Am J Sports Med, 2003 ;Lin et al, Clin Rheumatol, 2005
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Talking Point: Prone Scapular “Y”
Muscle % MVIC
Lower trap 97
Middle trap 100+
Upper trap 79
Serratus ant 43
Lat delt 90
Post delt 88-100+
Infraspinatus Up to 85
Supraspinatus 65-82Boettcher et al, Med Sci Sports Exerc, 2009; Ekstrom et al, J Orthop Sports Phys Ther, 2003
Reinold et al, J Orthop Sports Phys Ther, 2004; Blackburn et al, Athl Train, 1990

8/28/2013
6
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Impairment: External Rotator Weakness
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
External Rotator Muscle Performance
ER at side:
Teres minor 84% MVIC
Infraspinatus 46-73% MVIC
Supraspinatus 20-51% MVIC
Lower trapezius 48% MVIC
Lateral deltoid 8-21% MVIC
Posterior deltoid 31% MVIC
Myers et, J Athl Train, 2005; Hintermeister, Am J Sports Med, 1998 Dark et al, Phys Ther, 2007 Andersen et al, Phys Ther, 2010
Tip: Add towel roll & consider EMS
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
External Rotator Muscle Performance
ER at 90°:
Teres minor 89% MVIC
Infraspinatus 51% MVIC
Supraspinatus 50% MVIC
Lower trapezius 88% MVIC
Lateral deltoid 50% MVIC
Posterior deltoid 60% MVIC
Myers et, J Athl Train, 2005; Hintermeister, Am J Sports Med, 1998 Dark et al, Phys Ther, 2007 Andersen et al, Phys Ther, 2010

8/28/2013
7
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
External Rotation: Sidelying
Infraspinatus 62-85% MVIC
Lat. deltoid < 40% MVIC
Posterior deltoid 64% MVIC
Supraspinatus 51% MVIC
Teres minor 67-80% MVIC Reinold et al, J Orthop Sports Phys Ther, 2004; Townsend et al, Am J Sports Med, 1991
*De Mey et al, J Orthop Sports Phys Ther, 2013; Andersen et al, Phys Ther, 2010
Consideration:
-Conscious scapular correction
leads to ↑ LT activity (13%)*
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
External Rotation: Prone
Muscle % MVIC
Infra Up to130
Supra 68
Low Trap 79
Up Trap 20
Serratus Ant 57
Post Delt 79
Lat Delt 49
Reinold et al, J Orthop Sports Phys Ther, 2009; Ekstrom et al,J Orthop Sports Phys Ther, 2003
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Impairment: Lower Trapezius Weakness
8/28/2013
8
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
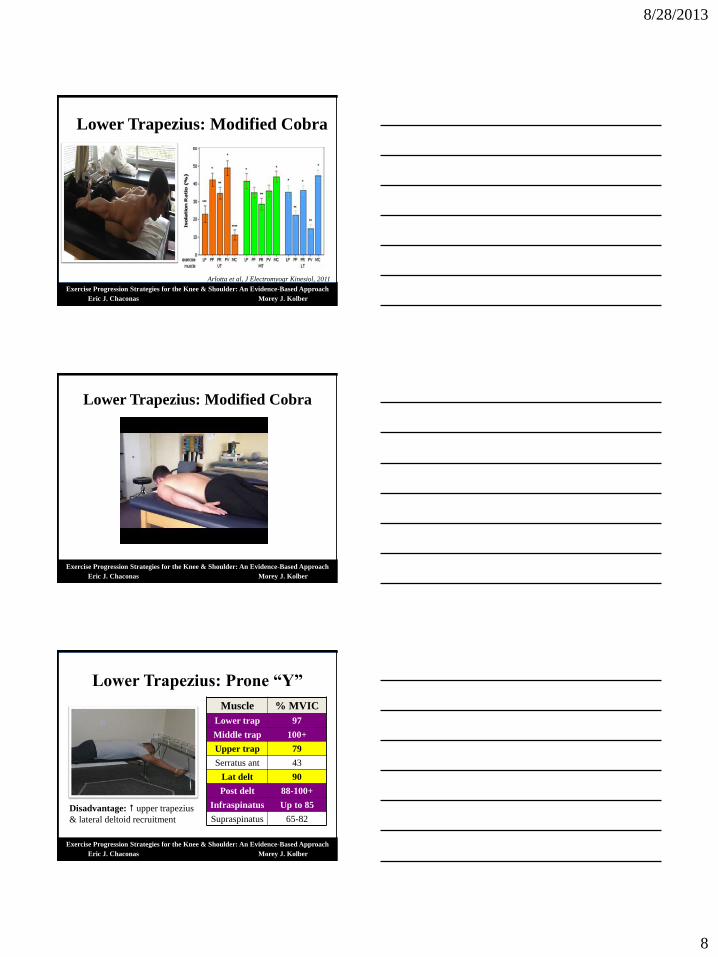
Lower Trapezius: Modified Cobra
Arlotta et al, J Electromyogr Kinesiol, 2011
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Lower Trapezius: Modified Cobra
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Lower Trapezius: Prone “Y”
Muscle % MVIC
Lower trap 97
Middle trap 100+
Upper trap 79
Serratus ant 43
Lat delt 90
Post delt 88-100+
Infraspinatus Up to 85
Supraspinatus 65-82
Disadvantage: upper trapezius
& lateral deltoid recruitment

8/28/2013
9
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Impairment: Serratus Anterior Weakness
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Serratus Anterior
•Punches:50-80% MVIC
*UT activation 7% MVICDecker et al, Am J Sports Med, 2003
Myers et al, J Athl Train, 2005
Ekstrom et al, J Orthop Sports Phys Ther, 2003
•Push up plus:73-80% MVIC
* UT activation 8-19% MVIC
Ludewig et al, Am J Sports Med, 2004
Moseley et al, Am J Sports Med, 1992
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Serratus Anterior
Scaption above 120°
Ludewig et al, Am J Sports Med, 2004; Moseley et al, Am J Sports Med, 1992Ekstrom et al, J Orthop Sports Phys Ther, 2003
Serratus ant. MVIC 96%Upper trap MVIC 79%
Upper Cut
Serratus ant. MVIC 100%Upper trap MVIC 66%
8/28/2013
10
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
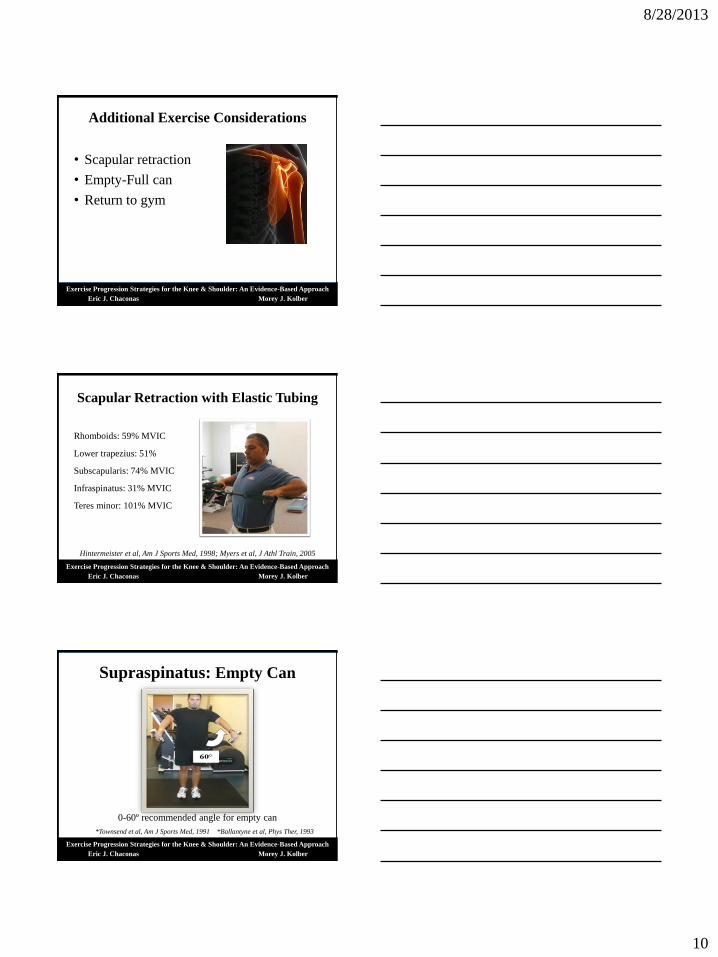
Additional Exercise Considerations
• Scapular retraction
• Empty-Full can
• Return to gym
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Scapular Retraction with Elastic Tubing
Rhomboids: 59% MVIC
Lower trapezius: 51%
Subscapularis: 74% MVIC
Infraspinatus: 31% MVIC
Teres minor: 101% MVIC
Hintermeister et al, Am J Sports Med, 1998; Myers et al, J Athl Train, 2005
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Supraspinatus: Empty Can
0-60º recommended angle for empty can
*Townsend et al, Am J Sports Med, 1991 *Ballantyne et al, Phys Ther, 1993

8/28/2013
11
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Supraspinatus: Full Can
*Improved isolation
compared to empty can
*Potentially less activation
than empty can
*Possibly Anterior
scapular tilting compared
to empty can
*↓ concern over improper
form
Kelly et al, Am J Sports Med, 1996
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Supraspinatus Considerations–Empty can: possible AHD - anterior tilt - poor form (SIS)
–Full can: alternative to empty can
–Empty & full can both have significant deltoid recruitment
• Both may perpetuate imbalance of force couples & impingement
–Prone scapular Y activates supraspinatus (> 65% MVIC) although significantly activates lateral deltoid (90% MVIC) & upper trap
• Alternatives:–Sidelying external rotation • Significantly anterior & lateral deltoid (< 40% MVIC) activity• Supraspinatus activity: 51% MVIC (Empty/Full/Y 64-85%)
–Prone external rotation• Significantly anterior & lateral deltoid (49% MVIC) activity• Supraspinatus activity: 68% MVIC
Dark et al, Phys Ther, 2007; Boettcher et al, Med Sci Sports Exerc, 2009
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Exercise Program Design
List key exercises for each muscle in a 3-stage progression
Acute Sub-acute Sport Return
Subscapularis Stand IR T-band Push-up plus Rebounder
Infraspinatus
Serratus Ant
Lower Trap

8/28/2013
12
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Exercise Program Design
• Secondary Impingement with supra/infra tendinosis
• Patient does not play sports or exercise
List 5 key exercises for muscle performance
First week Discharge
1.
2.
3.
4.
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Return to Gym and/or Sport
• Considerations: Gym
•Adjustment/advancement of volume & load
• Atrophy is common…..consider………
• Rehabilitation vs. Post rehabilitation volume & load
• Rest between sets?
•Gym/exercises: require consideration of biomechanics
•Rotator cuff disorders
•Anterior instability
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Weight-Training Injuries
– Descriptive epidemiological reports comprise majority of literature
pertaining to WT injuries
– Injury surveillance (NEISS) ER
• 35% injury rate in past two decades
• Males comprise > 80% injuries Jones et al, Phys Sportsmed, 2000
– Injury surveillance (NEISS) ER 1990 -2007
• Males > 80% with “48.4% from 1996 to 2006”
Kerr et al, Am J Sports Med, 2010
– Primary site of injury: Shoulder complex
Goertzen et al, Sportverletz Sportschaden,1989; Raske & Norlin, Am J Sports Med,
2002; Van der Wall, Clin Nucl Med, 1999; Koegh et al, J Strength Cond Res, 2006
8/28/2013
13
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
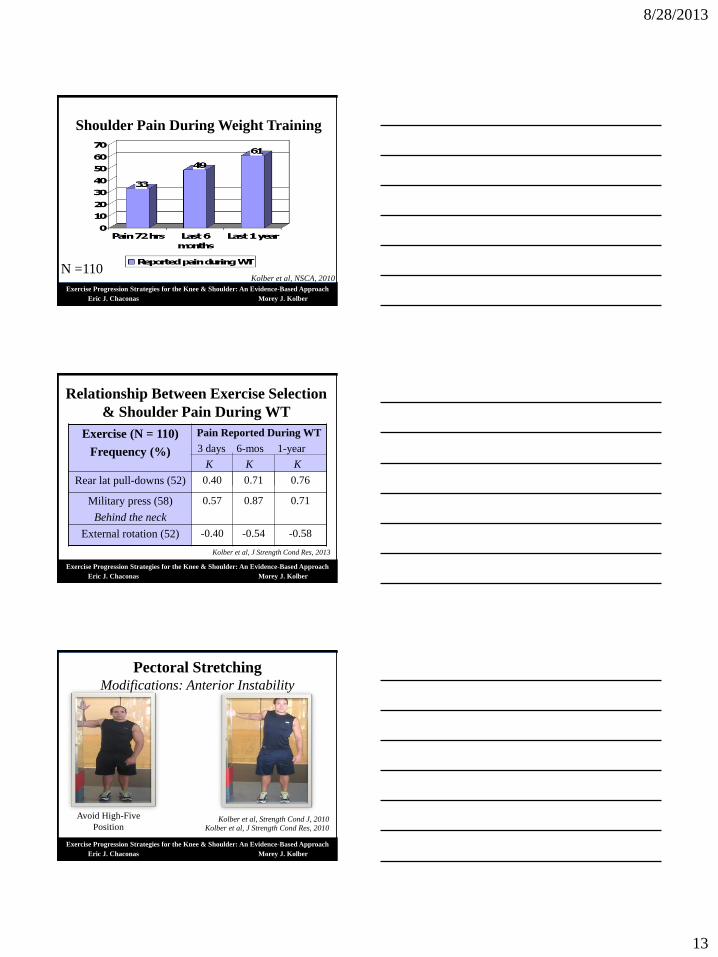
Shoulder Pain During Weight Training
N =110Kolber et al, NSCA, 2010
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Relationship Between Exercise Selection
& Shoulder Pain During WT
Exercise (N = 110)
Frequency (%)
Pain Reported During WT
3 days 6-mos 1-year
K K K
Rear lat pull-downs (52) 0.40 0.71 0.76
Military press (58)
Behind the neck
0.57 0.87 0.71
External rotation (52) -0.40 -0.54 -0.58
Kolber et al, J Strength Cond Res, 2013
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Pectoral StretchingModifications: Anterior Instability
Avoid High-Five
PositionKolber et al, Strength Cond J, 2010
Kolber et al, J Strength Cond Res, 2010

8/28/2013
14
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Seated Barbell Press: Deltoids (A &L)Modification: Anterior Instability
What we know: Both behind the neck pull-downs & military press
have a significant association with shoulder pain & clinical symptoms
of anterior shoulder instability Kolber et al, J Strength Cond Res, 2013
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Machine Chest Fly: Pectorals Modification: Anterior Instability
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Seated Dumbbell Press: Deltoids (A&L) Modification: Anterior Instability & SIS

8/28/2013
15
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Chest Fly: PectoralsModification: Anterior Instability
Dumbbell Chest Fly Dumbbell Chest Press
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Shoulder Press: Deltoids (A/L)Modifications: Anterior Instability & SIS
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Bench Press: Pectorals & TricepsModifications: Anterior Instability & AC Disorder

8/28/2013
16
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Seated Bench Press: Pectoral & TricepsModification: Anterior Instability & AC Disorders
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Latissimus Pull-Downs: Posterior Musculature
Modifications: Anterior Instability
Considerations:
1. Wide grip to front instead of rear
-Increase activation of latissimus
Lehman et al, Dyn Med, 2004
Signorile et al, J Strength Cond Res, 2002
-↓ propensity for anterior instability/pain
Kolber et al, J Strength Cond Res, 2013
2. Add scapular depression to ↑ LT activity
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Consideration:
-Scapular retraction may mildy* middle trap, lats & rhomboid activity
Lehman et al, Dyn Med, 2004
Seated Rows: Posterior Musculature
8/28/2013
17
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
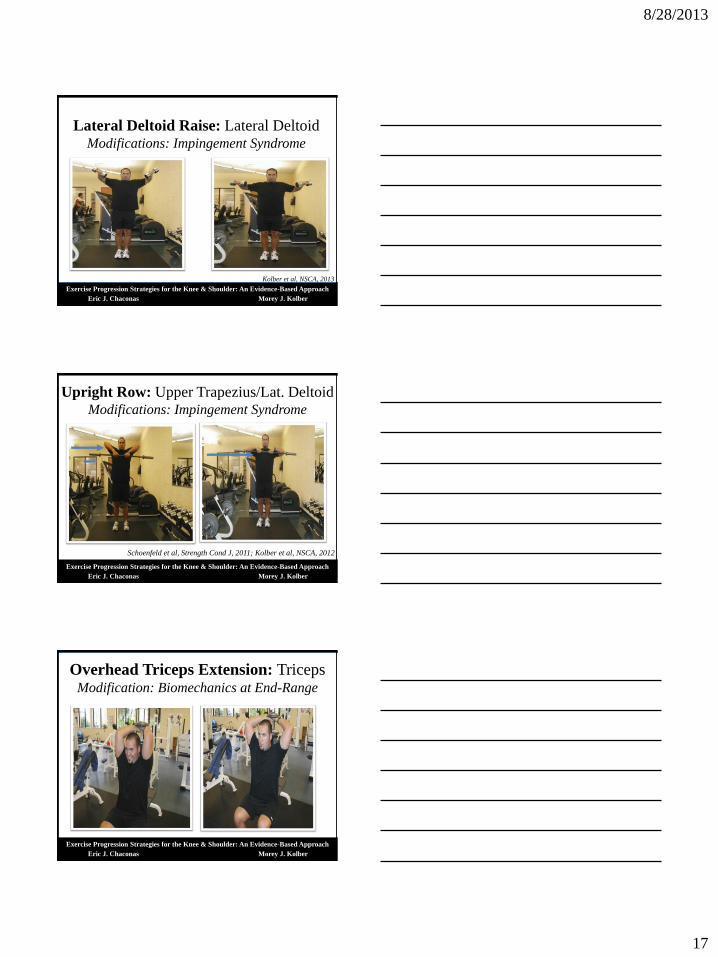
Lateral Deltoid Raise: Lateral DeltoidModifications: Impingement Syndrome
Kolber et al, NSCA, 2013
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Schoenfeld et al, Strength Cond J, 2011; Kolber et al, NSCA, 2012
Upright Row: Upper Trapezius/Lat. DeltoidModifications: Impingement Syndrome
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Overhead Triceps Extension: TricepsModification: Biomechanics at End-Range
8/28/2013
18
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber 52
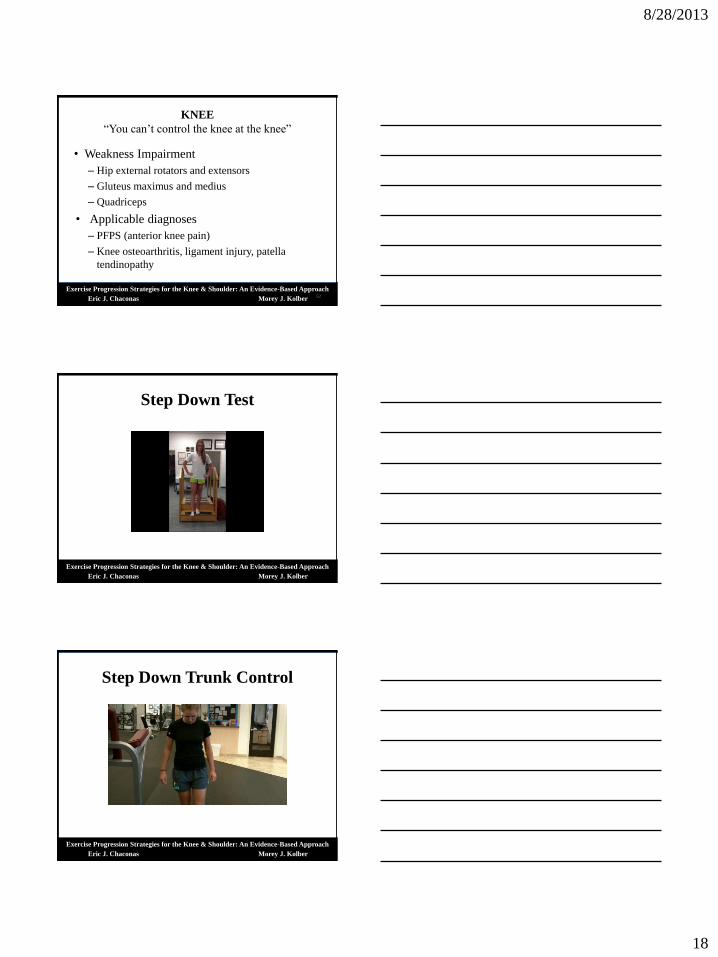
KNEE
“You can’t control the knee at the knee”
• Weakness Impairment
– Hip external rotators and extensors
– Gluteus maximus and medius
– Quadriceps
• Applicable diagnoses
– PFPS (anterior knee pain)
– Knee osteoarthritis, ligament injury, patella
tendinopathy
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Step Down Test
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Step Down Trunk Control
8/28/2013
19
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
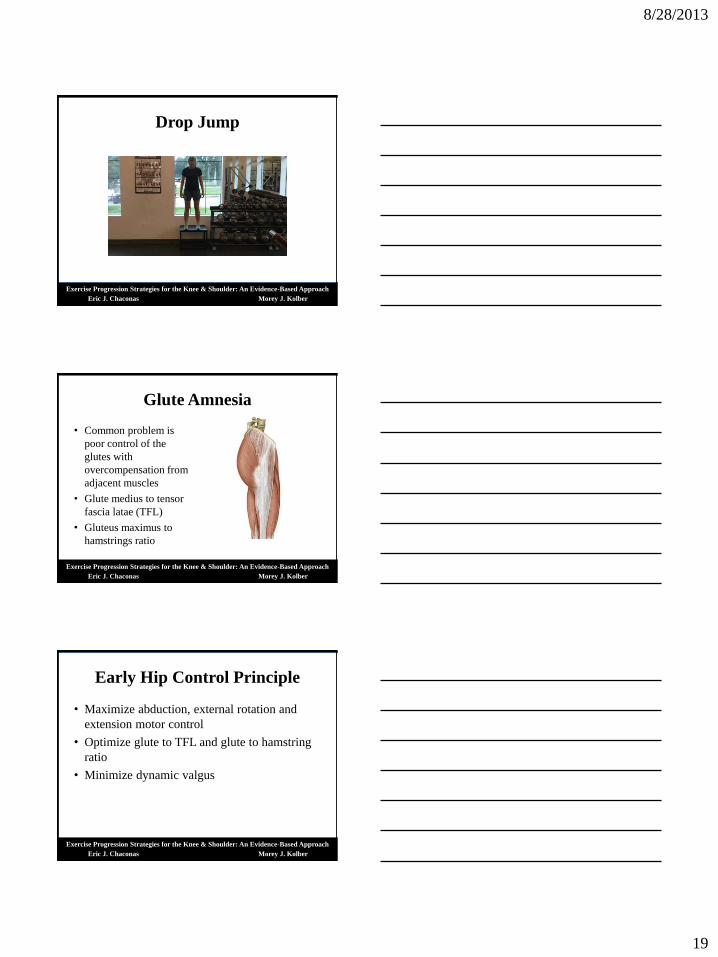
Drop Jump
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Glute Amnesia
• Common problem is
poor control of the
glutes with
overcompensation from
adjacent muscles
• Glute medius to tensor
fascia latae (TFL)
• Gluteus maximus to
hamstrings ratio
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Early Hip Control Principle
• Maximize abduction, external rotation and
extension motor control
• Optimize glute to TFL and glute to hamstring
ratio
• Minimize dynamic valgus
8/28/2013
20
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
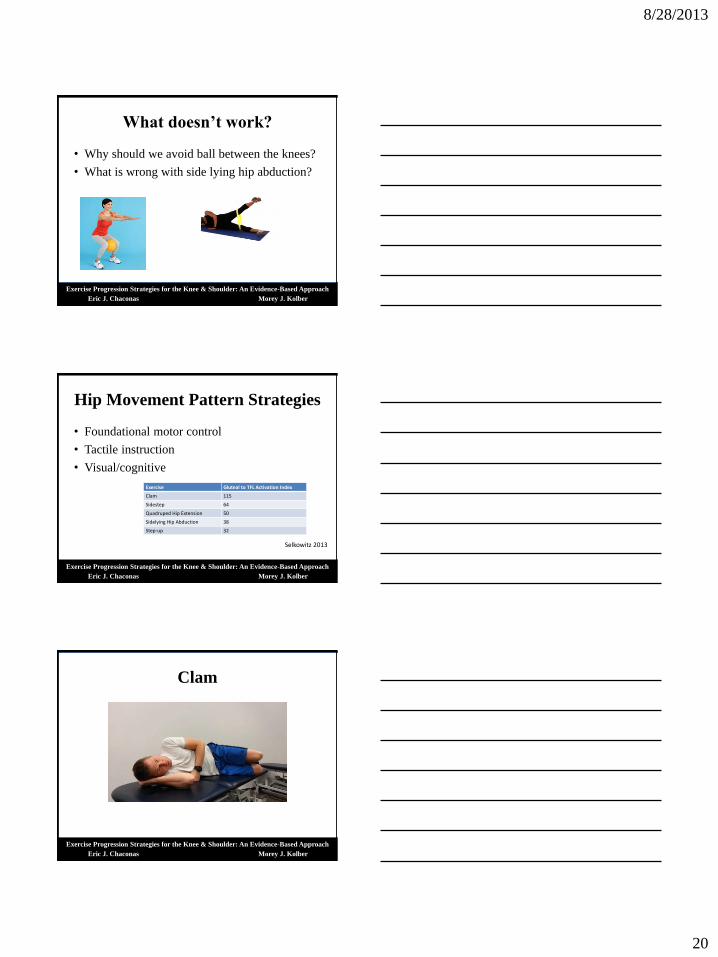
What doesn’t work?
• Why should we avoid ball between the knees?
• What is wrong with side lying hip abduction?
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Hip Movement Pattern Strategies
• Foundational motor control
• Tactile instruction
• Visual/cognitive
Exercise Gluteal to TFL Activation Index
Clam 115
Sidestep 64
Quadruped Hip Extension 50
Sidelying Hip Abduction 38
Step-up 32
Selkowitz 2013
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Clam

8/28/2013
21
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Clam Plus
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Early Phase Gluteus Medius
• Side bridge (side plank)
– Endurance holds
• Side step progression
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Slow Eccentric

8/28/2013
22
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Early Phase Gluteus Maximus
• Bridge with abduction
of hips to improve
glute/hamstring ratio
• Add resistance
• Unilateral
Kang 2013
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Extension Diagonals
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
8/28/2013
23
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
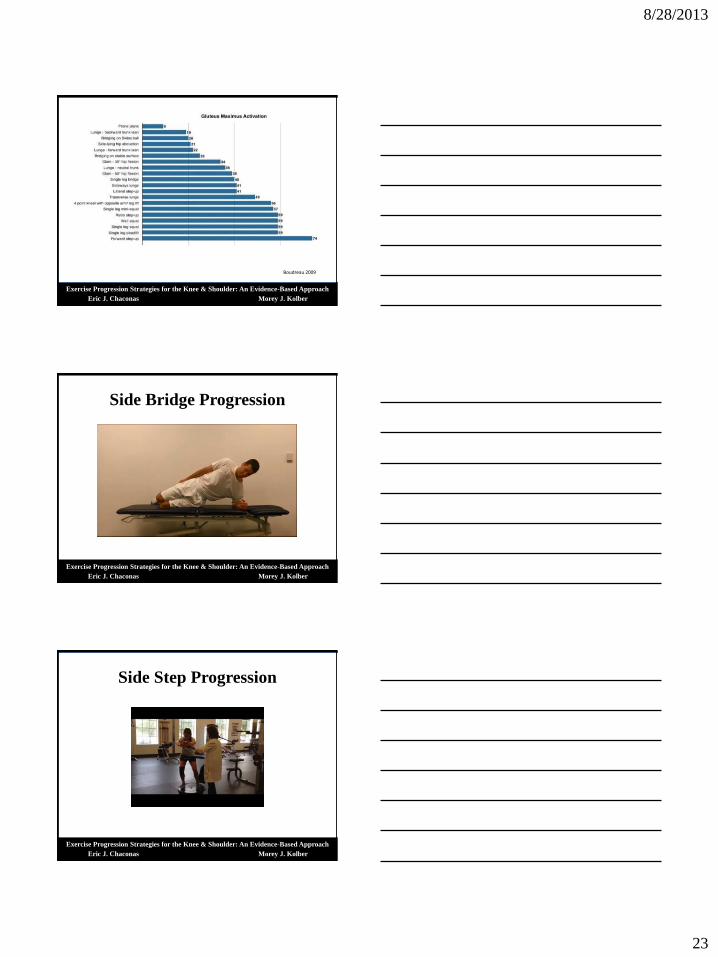
Boudreau 2009
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Side Bridge Progression
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Side Step Progression

8/28/2013
24
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Single Leg Squat
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Single Leg Squat
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Single Leg Deadlift

8/28/2013
25
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Squat Progression
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Step Up/Down
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Quadriceps
• Quadriceps inhibition in the presence of knee
pain
– Knee osteoarthritis
– Ligament Injury
– Knee joint effusion
– Patella femoral pain syndrome
– Most knee surgical procedures
• Does quadriceps weakness cause knee pain?

8/28/2013
26
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Quadriceps Rehabilitation
• Open kinetic chain: straight leg raise, knee
extension
• Closed kinetic chain: Deeper knee flexion
angle = greater quadriceps activation
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Quadriceps
• NMES is effective
• Consider
– Electrode size
– Motor point
– Max intensity tolerated
• Diagnoses
– Total knee Stevens-Lapsley 2012
– Knee OA Vaz 2013
– ACL Kim 2010
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber 78
Home Program
• Patient adherence is the #1 concern
• Less is more
• Instruction: video, patient smartphone
• Adherence to an exercise program directly
associated with level of Self-determination
theory

8/28/2013
27
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
Self-determination Continuum
Lonsdale, 2012
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
5 A’s to Maximize Patient Self-
Determination
• Ask: Open ended questions, paraphrase, empathize– Gauge patient readiness to accept advice
• Advise: Provide rationale, request patient input and use autonomy focused phrases
– “Here are some things that will help you overcome”
• Agree: Active participation in goal setting, decide on objective, measurable and time based goals
• Assist: Identify barriers, identify solutions
• Arrange: Provide patient with a rehabilitation diary, follow up appointment and contact information for questions
Exercise Progression Strategies for the Knee & Shoulder: An Evidence-Based Approach
Eric J. Chaconas Morey J. Kolber
References (Lower Quarter)• Boudreau, S.N., M.K. Dwyer, C.G. Mattacola, C. Lattermann, T.L. Uhl, and J.M. McKeon: Hip-muscle activation during
the lunge, single-leg squat, and step-up-and-over exercises. J Sport Rehabil 2009;18(1)91-103.
• Cambridge, E.D., N. Sidorkewicz, D.M. Ikeda, and S.M. McGill: Progressive hip rehabilitation: the effects of resistance band placement on gluteal activation during two common exercises. Clin Biomech 2012;27(7)719-724.
• Kang SY, Jeon HS, Kwon O, Cynn HS, Choi B. Activation of the gluteus maximus and hamstring muscles during prone hip extension with knee flexion in three hip abduction positions. Man Ther 2013 Jan 8. [Epub ahead of print]
• Kim KM, Croy T, Hertel J, Saliba S. Effects of neuromuscular electrical stimulation after anterior cruciate ligament reconstruction on quadriceps strength, function, and patient-oriented outcomes: a systematic review. J Orthop Sports Phys Ther. 2010;40:383-391.
• McBeth, J.M., J.E. Earl-Boehm, S.C. Cobb, and W.E. Huddleston: Hip muscle activity during 3 side-lying hip-strengthening exercises in distance runners. J Athl Train 2012;47(1)15-23.
• McCurdy, K., E. O'Kelley, M. Kutz, G. Langford, J. Ernest, and M. Torres: Comparison of lower extremity EMG between the 2-leg squat and modified single-leg squat in female athletes. J Sport Rehabil 2010;19(1)57-70.
• Reiman MP, Bolgla LA, Loudon JK. A literature review of studies evaluating gluteus maximus and gluteus mediusactivation during rehabilitation exercises. Physiother Theory Pract 2012;28(4)257-268.
• Selkowitz, D.M., G.J. Beneck, and C.M. Powers: Which Exercises Target the Gluteal Muscles While Minimizing Activation of the Tensor Fascia Lata? Electromyographic Assessment Using Fine-Wire Electrodes. J Orthop Sports Phys Ther201243(2):54-64.
• Stevens-Lapsley JE, Balter JE, Wolfe P, Eckhoff DG, Kohrt WM. Early neuromuscular electrical stimulation to improve quadriceps muscle strength after total knee arthroplasty: a randomized controlled trial. Phys Ther 2012;92(2):210-26.
• Vaz MA, Baroni BM, Geremia JM, Lanferdini FJ, Mayer A, Arampatzis A, Herzog W. Neuromuscular electrical stimulation (NMES) reduces structural and functional losses of quadriceps muscle and improves health status in patients with knee osteoarthritis. J Orthop Res 2013;31(4):511-6.