Examining discharge outcomes and health status of critically ill patients: some practical...
12
Intensive and Critical Care Nursing (2004) 20, 366—377 ORIGINAL ARTICLE Examining discharge outcomes and health status of critically ill patients: some practical considerations Doug Elliott a,∗ , Yugan Mudaliar b , Carolyn Kim b a Prince of Wales Hospital, Randwick and Department of Clinical Nursing, The University of Sydney, Sydney, NSW 2006, Australia b Intensive Care Unit, Westmead Hospital, Sydney, Australia KEYWORDS Health status; Intensive care; Outcome; Proxy responses Summary This prospective observational study examined the outcomes of 200 consecutive admissions to an adult tertiary level Intensive Care Unit (ICU). Eligible and consenting participants were also involved in a sub-study that examined health status at four measurement points from pre-illness to 6 months post- discharge. Of the 189 individual patients admitted, 23% died in ICU and 57% were discharged home. The health status sub-study enrolled 34 participants (39% of eligible patients) who were representative of the ICU population for demographic and clinical vari- ables. Surviving participants returned to a similar, though not identical state of health at 6 months post-discharge, when compared to their pre-ICU health-state us- ing the 15D and SF-36 instruments. Health status at ICU discharge was significantly impaired when compared to other measurement points, particularly for mobility, breathing, eating, usual activities and vitality. A number of methodological challenges were evident, particularly for the health status sub-study, including prospective subject recruitment and retention, losses to follow-up and instrument responsiveness. Despite the limitations noted, the study provided useful findings and recommendations for the continued development of methods to examine the health status of critically ill patients. © 2004 Elsevier Ltd. All rights reserved. Introduction Evidence of the effectiveness of clinical interven- tions, in terms of patient functional outcomes, is necessary in the current health care environment. This is particularly the case for critical care units, * Corresponding author. Tel.: +61 2 9382 2305/9351 0657; fax: +61 2 9382 3035/9351 0654. E-mail address: [email protected] (D. Elliott). where management is expensive and patient out- comes (other than mortality and morbidity) have historically not been well measured (Angus and Carlet, 2003). However methodologically desirable, ran- domised controlled trials cannot often be ethically performed with critically ill patients (Rubenfeld et al., 1999). Hence, other study designs including comparisons of matched groups of critically ill patients treated in different ways are important in 0964-3397/$ — see front matter © 2004 Elsevier Ltd. All rights reserved. doi:10.1016/j.iccn.2004.07.001
-
Upload
doug-elliott -
Category
Documents
-
view
215 -
download
0
Transcript of Examining discharge outcomes and health status of critically ill patients: some practical...

Intensive and Critical Care Nursing (2004) 20, 366—377
ORIGINAL ARTICLE
Examining discharge outcomes and health statusof critically ill patients: some practicalconsiderations
Doug Elliotta,∗, Yugan Mudaliarb, Carolyn Kimb
a Prince of Wales Hospital, Randwick and Department of Clinical Nursing, The University of Sydney,Sydney, NSW 2006, Australiab Intensive Care Unit, Westmead Hospital, Sydney, Australia
KEYWORDSHealth status;Intensive care;Outcome;Proxy responses
Summary This prospective observational study examined the outcomes of 200consecutive admissions to an adult tertiary level Intensive Care Unit (ICU). Eligibleand consenting participants were also involved in a sub-study that examinedhealth status at four measurement points from pre-illness to 6 months post-discharge.Of the 189 individual patients admitted, 23% died in ICU and 57% were discharged
home. The health status sub-study enrolled 34 participants (39% of eligible patients)who were representative of the ICU population for demographic and clinical vari-ables. Surviving participants returned to a similar, though not identical state ofhealth at 6 months post-discharge, when compared to their pre-ICU health-state us-ing the 15D and SF-36 instruments. Health status at ICU discharge was significantlyimpaired when compared to other measurement points, particularly for mobility,breathing, eating, usual activities and vitality.A number of methodological challenges were evident, particularly for the health
status sub-study, including prospective subject recruitment and retention, losses tofollow-up and instrument responsiveness. Despite the limitations noted, the studyprovided useful findings and recommendations for the continued development ofmethods to examine the health status of critically ill patients.© 2004 Elsevier Ltd. All rights reserved.
Introduction
Evidence of the effectiveness of clinical interven-tions, in terms of patient functional outcomes, isnecessary in the current health care environment.This is particularly the case for critical care units,
* Corresponding author. Tel.: +61 2 9382 2305/9351 0657;fax: +61 2 9382 3035/9351 0654.
E-mail address: [email protected] (D. Elliott).
where management is expensive and patient out-comes (other than mortality and morbidity) havehistorically not been well measured (Angus andCarlet, 2003).
However methodologically desirable, ran-domised controlled trials cannot often be ethicallyperformed with critically ill patients (Rubenfeldet al., 1999). Hence, other study designs includingcomparisons of matched groups of critically illpatients treated in different ways are important in
0964-3397/$ — see front matter © 2004 Elsevier Ltd. All rights reserved.doi:10.1016/j.iccn.2004.07.001

Examining discharge outcomes and health status of critically ill patients 367
evaluating intensive care management (Angus andCarlet, 2003). Subsequent observational outcomestudies have evolved from using coarse, unvali-dated and imprecise measures to the applicationof valid generic instruments or the developmentof setting-specific questionnaires (Chaboyer andElliott, 2000; Elliott, 1999). This process hasimproved the generalisability of results, but therecontinues to be some methodological concerns,including the use of relevant measuring instru-ments and lack of control of extraneous variables(Heyland et al., 1998).
A generic instrument that measures baselinehealth related quality of life (HRQOL) and exhibitsresponsiveness in the recovering critically ill pa-tient with demonstrated reliability and validity hasbeen elusive (Ridley, 1999), although more recentreview papers have identified some useful instru-ments (Angus and Carlet, 2003; Black et al., 2001),including the SF-36, Sickness Impact Profile (SIP),Nottingham Health Profile (NHP), and EuroQol 5-D (Chaboyer and Elliott, 2000; Mendelsohn andChelluri, 2003). SF-36 in particular is well validated(Angus and Carlet, 2003; Chrispin et al., 1997) andis the most common instrument used for assessingt(
scoparsmrrIrG1apwbeaC
(addco
haviours, such as physical functioning had higheragreement than less overt concepts such as men-tal health or vitality (Badia et al., 1996; Hofhuis etal., 2003; Rogers et al., 1997)—–an inherently logi-cal finding. However, it was also the case that prox-ies systematically underrate a patient’s functionalstatus or quality of life (Hofhuis et al., 2003; Rogerset al., 1997).
The purpose of this study was to examine theoutcomes of a group of critically ill patients ad-mitted to an adult general ICU. In addition, twohealth status instruments and related procedureswere tested for evaluating the health outcomes ofa sub-sample of the above patients. The specificstudy objectives were to:
1. examine the discharge outcomes of 200 consec-utive admissions to an adult general ICU
2. evaluate the procedure for prospective mea-surement of health status with this group ofcritically ill patients, including the use of proxyrespondents
3. test the 15D Quality of Life Questionnaire andthe SF-36 health survey for applicability ashealth outcome instruments for patients duringand following a critical illness that required ad-
M
Tcstsaowitpp
S
AfhIphIs(
he functional status of the post-Intensive Care UnitICU) population (Elliott, 1999).The measurement of pre-illness or injury health
tatus is also an integral component of this pro-ess to provide a baseline measure. However, tobtain these measures on all potential critical careatients is obviously not possible. An alternativepproach is to examine the usefulness of proxyespondents or retrospective recall in this clinicaletting. Although the majority of studies did noteasure pre-crisis health status, studies that dideported that a substantial proportion of survivorseturned to a state of health similar to their pre-CU status (Elliott, 1999). These studies used eitheretrospective review (Gardner and Sibthorpe, 2002;raf et al., 2003; Ridley et al., 1997; Welsh et al.,999) or proxies (Hofhuis et al., 2003; Rogers etl., 1997). Both approaches have limitations. Theotential for recall bias is an important limitationhen using retrospective recall. As the timeframeetween the event and the recall point length-ns, an individual’s memory becomes more flawed,nd guesses increase in frequency (Guadagnoli andleary, 1995; Herrman, 1995).The reported level of agreement between index
the patient) and proxy respondents (usually a rel-tive) for a critical illness is variable. One studyemonstrated fair agreement at 6 months post-ischarge, but significant differences at ICU dis-harge using SF-36 (Rogers et al., 1997). A numberf studies found that observable activities or be-
mission to a general ICU.
ethods
he study design was descriptive and observational,onducted prospectively for 200 consecutive admis-ions to a 13-bed general ICU of a 900-bed ter-iary referral hospital in Sydney, Australia. Cardiacurgical patients were managed in a separate ICU,nd high dependency units were located through-ut the hospital. All patients admitted to the ICUeremechanically ventilated. Eligible and consent-ng participants were also involved in assessment ofhe patient’s health status, using four measurementoints (pre-crisis health; at ICU discharge; at hos-ital discharge; 6 months post-discharge).
ample
convenience sample was recruited and followedor their outcome on discharge from the ICU,ospital discharge and 6 months post-discharge.n addition, eligible patients were approachedrospectively for in-depth examination of theirealth status before, during and after their currentCU admission. The inclusion criteria for the healthtatus sub-study were: (1) aged 16 years or older;2) admitted to ICU for a period greater than 24 h;

368 D. Elliott et al.
(3) death not obviously imminent; (4) not for pal-liative management; (5) a relative available for ini-tial study consent and instrument completion; (6)not for transfer to another ICU or hospital; (7) nodiagnosed mental illness; and (8) suitable Englishcomprehension skills (for patients and/or next-of-kin) to enable completion of the questionnaire.
Patients admitted to the ICU for periods less than24 h were commonly only for close monitoring fol-lowing a surgical procedure. Relatives visiting pa-tients who were not expected to live or relativeswho were acutely distressed about the patient’scondition were not approached to participate in thestudy. In practice, this was a substantial propor-tion of the overall population. Repeat admissionswere enrolled once on their first admission to theICU. Proxy respondents (next-of-kin) were asked tocomplete the instruments at the first measurementpoint because of the critical clinical condition ofthe index respondent (patient) on admission to theICU. Completion of subsequent questionnaires byproxy respondents was dependent on the clinicalcondition and cognition of the index respondent.
Measuring instruments
levels, and takes approximately 5—10min to com-plete. The dimensions assessed are: mobility, vi-sion, hearing, breathing, sleeping, eating, speech,elimination, usual activities, mental function, dis-comfort, distress, depression, vitality, and sexualactivity. The response statements move in orderfrom full function through to minimal or no func-tion for that health dimension. For example, usualactivities is assessed by the 5-level statement: (1) Iam able to perform my usual activities (e.g. em-ployment, studying, housework, free-time activi-ties) without difficulty; (2) I am able to performmy usual activities slightly less effectively or withminor difficulty; (3) I am able to perform my usualactivities much less effectively with considerabledifficulty, or not completely; (4) I can only managea small proportion of my previously usual activities;or (5) I am unable to manage any of my previouslyusual activities.
The instrument is similar to the EuroQol 5-D(Brooks, 1996), although EQ-5D uses only three re-sponse levels to assess mobility, self-care, usual ac-tivities, pain/discomfort, and anxiety/depression.The benefits of 15D are in its face validity, rangeof dimensions, brevity, and ease of completion be-cor
rstnvscltaTRtiva(s2
P
Hgst
Two commonly used ICU-based instruments — AcutePhysiology and Chronic Health Evaluation (APACHE)(Knaus et al., 1985); Therapeutic InterventionScoring System (TISS) (Keene and Cullen, 1983) —assessed the patients’ severity of illness and clini-cal interventions, respectively. APACHE II scores aregrouped into low (0—10 points); medium (11—20points); and high (>21 points). Four classes (IV:≥40points; III: 20—39 points; II: 10—19 points; I: <10points) are used for TISS scores (Keene and Cullen,1983). However, TISS does not accurately measureindependent nursing activities related to patienthygiene, sensory deficits, continuous observations,or technical problem-solving. These deficiencieshave been addressed in the recently developedNursing Activity Scale (Reis Miranda et al., 2003).APACHE and TISS scores were used to examine thehomogeneity of the sub-study participants in rela-tion to the study population. The instruments are,however, of minimal benefit in determining inter-mediate and long-term outcomes in terms of pa-tients’ functional status or quality of life followinga critical illness.
The questionnaires completed by the healthstatus sub-study participant were the 15D Qual-ity of Life Questionnaire (Sintonen and Pekurinen,1993) and SF-36 (Ware and Sherbourne, 1992; Ware,2000). 15D is a closed-ended 15-item questionnaireassessing health status using five ordinal response
ause of the standard response format. However,ne item per dimension may limit sensitivity andesponsiveness to changes in health status.SF-36 is a closed-ended 36-item questionnaire
eflecting eight health concepts and a health tran-ition question, and takes approximately 5—10mino complete (Ware and Sherbourne, 1992). Asoted earlier, SF-36 is widely accepted as aalid and reliable instrument for measuring healthtatus in populations and clinical samples, in-luding critically ill patients. The 36 items col-apse into eight health-state scales, a healthransition item, and physical component (PCS)nd mental component summary (MCS) measures.he PCS is a summary of Physical Functioning,ole—–Physical, Bodily Pain, and General Health;he MCS is summed from Vitality, Social Function-ng, Role—–Emotional, and Mental Health. Loweralues on a 0—100 scale indicate poorer functioningnd higher values better functioning for all scalesWare et al., 1993; Ware, 2000). See http://www.f-36.org/tools/sfsurveys.aspx (accessed 11 June004) for a sample of the instrument.
rocedure
uman Research Ethics Committee approval wasranted prior to study commencement. A pilottudy using a convenience sample was conducted toest the procedure (see below). For the main study,

Examining discharge outcomes and health status of critically ill patients 369
all patients admitted to the general ICU during thedata collection period were indirectly tracked bythe hospital information system, with no direct con-tact between the researchers and the patients orrelatives during this process. Informed consent wasobtained for the health status sub-study by thenext-of-kin and patient (when cognisant), includinga guarantee of confidentiality.
The next-of-kin (proxy respondent) completedthe questionnaire on the patient’s general healthstatus prior to their critical illness and subsequentadmission to ICU. At discharge from the ICU, thesurviving patient (or next-of-kin, depending on thepatient’s functional and cognitive abilities) com-pleted a repeat questionnaire assessing their cur-rent health status (15D only) was administered. Athospital discharge and 6 months post-discharge, thequestionnaire was mailed out with a reminder let-ter. Non-responders were followed up by telephonetwice, after which a decision was made to discon-tinue follow-up attempts. Other patient data werecollected from a variety of sources, as complete pa-tient information was not integrated into a hospitalclinical information system.
D
Sdaanpplntppc
prsdrced(
P
Tm
participants. The sample consisted of 16 males and14 females, with an average age of 50 years (me-dian: 56; range: 16—81 years). The median ICU LOSwas 8 days (range: 27—850 h). The hospital LOS av-eraged 27 days (range: 2—101 days). The medianAPACHE score was 17 (95% CI: 16—22%), with themajority of patients (73%) grouped in the mediumacuity category (11—20 points). The most commondiagnoses were surgery, trauma and sepsis. The ma-jority of the pilot sample was discharged home(70%), while one died in ICU and two died in hospi-tal. A substantial number of survivors (33%) were re-admitted to the same hospital within 7—12 months,with four patients re-admitted twice during thatperiod.
The next-of-kin (proxy respondent) was pre-dominantly a spouse (n = 17). Proxy respondentscompleted all the patients’ pre-admission healthstatus measurements, as expected. The index re-spondents (patients) completed 23, 92 and 80% ofthe following measures, respectively. Ten partici-pants completed all four measures, with a furtherfive completing all but the hospital discharge mea-sure and another three completing all but the lastmeasure. Five participants completed the first andlms
H
S(eiaufthwserfr
arc(wafF
ata analysis
ummary statistics (means, frequencies) were pro-uced for the demographic and clinical variables:ge, ICU length of stay (LOS), hospital LOS, APACHEnd TISS scores. For the health status sub-study, allon-participants were grouped together for com-arison with participants using t tests. Specific non-articipant groups (refusals, deaths, transfers out,ess than 24 h, re-admissions, non-English speaking,o relatives, and mental illness) were compared tohe participants using Analysis of Variance (ANOVA)rocedures. Variables using frequencies and pro-ortions (gender, admission source, discharge out-ome) were analysed by chi-square procedures.Differences in 15D scores between measurement
oints was tested by one-way ANOVA proceduresather than a repeated-measures design, as sampleizes for each measurement point were differentue to loss to follow-up (non-equivalent responseates). Scaled scores for the eight health con-epts and the two component summary scores werexamined using t tests to detect any significantifferences between the two measurement pointspre-ICU and 6 months post-discharge).
ilot study
he study procedure for the health status instru-ents was tested with a convenience sample of 30
ast measures, three completed only the hospitaleasures, and four completed only the first mea-ure.
ealth status of pilot participants
cores for 15D at ICU discharge were lower than:1) all other measurement points for mobility andating (P < .001); (2) pre-admission for breath-ng and mental function (P < .05); and (3) pre-dmission and 6 months post-discharge for speech,sual activities (P < .001) and vitality (P < .05)or 15D. In addition, pre-ICU scores were higherhan hospital discharge for usual activities. Pre-ICUealth status and hospital discharge health statusere not significantly different for the other dimen-ions. All dimensions were not significantly differ-nt at pre-admission and 6 months post-discharge,eflecting a return to a similar health statusollowing the critical illness, hospitalisation andecovery.Using SF-36, Physical Function, Role—–Physical
nd Role—–Emotional scores at 6 months had noteturned to pre-admission levels, but were signifi-antly higher than ICU and hospital discharge scoresP < .001). Similarly, Bodily Pain and Mental Healthere lowest at ICU discharge and highest at pre-dmission (P < .05). There were no significant dif-erences for General Health, Vitality, and Socialunctioning.

370 D. Elliott et al.
Pilot study discussion
The pilot demonstrated some difficulties with par-ticipant recruitment, losses to follow-up and re-sponses to some instrument items. It was initiallyproposed for the ICU medical consultants to intro-duce the study to relatives at the first meeting fol-lowing the patient’s admission to ICU. However, inpractice, the consultants found it difficult to intro-duce the study at such a stressful time for the rela-tives. A poor response to prospective participantrecruitment was evident in similar studies (e.g.Graf et al., 2003) but not others (e.g. Mata et al.,1992).
It also became clear that a number of SF-36 itemswere difficult to answer for patients who had justbeen transferred from the ICU or were for dischargefrom hospital. These items related to everyday do-mestic or work activities that were not possiblefor the participant, given their clinical conditionand the physical constraints of the hospital envi-ronment. By contrast, the item content and facevalidity of the 15D questions made them easier forthe patients and/or their next-of-kin to understandand answer.
sions
cipan34)
6)))))5)
2))4%)00%)
Results
Patient characteristics
The 200 consecutive admissions to the general ICUwere completed in 17 weeks and resulted in a to-tal of 189 patients being screened for follow-up.Twenty percent of admissions died prior to recruit-ment to the health status sub-study (n = 39), andtwo recruited participants died prior to the firstmeasurement point. In addition, 63 (32%) did notsatisfy the study inclusion criteria. Just over half ofthe hospital survivors were discharged home (57%),and 12 patients required transfer to a rehabilitationhospital (see Table 1). The proportions who weredischarged home or who died in ICU differed be-tween the participants and non-participants. Over-all, there were 52 patients who died in hospital (28%of the entire sample) during the study period.
Health status sub-study
Of the patients eligible for the sub-study, 53 re-fused and 34 were recruited (response rate: 39%).Tmmsars(S
Changes to the study procedure following evalu-ation of the pilot study were: (1) relatives of po-tential participants were approached by the re-searchers personally or by letter, not by the ICUconsultants and (2) SF-36 was completed at pre-crisis and 6 months post-discharge, but not at ICUdischarge or hospital discharge. This was supportedby other studies (e.g. Kvale et al., 2003; McCarthyet al., 1995).
Table 1 ICU sample discharge outcomes and re-admis
Discharge outcome Parti(n =
Survived hospital n (%)Discharged home 26 (7Transferred to rehabilitation hospital 2 (6Transferred to other hospital 1 (3
Died in ICU 3 (9Died in hospital 2 (6Cumulative hospital mortality 5 (1
Re-admissions within 12 monthsNone 21 (7Within 1 month 2 (72—6 months 4 (17—12 monthsDay-only admission 3 (1
.
ts Non-participants(n = 155)
All patients(n = 189)
n (%) %93 (60) 6310 (6) 65 (3) 341 (26) 236 (4) 447 (30) 28
78 (50) (52%)15 (10) (9%)13 (8) (10%)2 (1)9 (9%) (6%)
he participants comprised 19 males and 15 fe-ales, with an average age of 56 years (S.D.: 18;edian: 60; range: 16—82). The common admis-ion diagnoses were surgery (42%), respiratory (24%)nd neurological (9%). A high proportion of respi-atory disorders in this sample reflected the sea-onal factors evident with general ICU admissionsdata collection during the Australian Winter/Earlypring—–July to October).

Examining
dischargeoutcom
esand
healthstatus
ofcritically
illpatients
Table 2 Health status sub-study participant and non-participant characteristics.Variables Participants
(n = 34)Non-participants
Overall(n = 155)
Refusals(n = 53)
Deaths(n = 39)
Transferout(n = 5)
Less than24 hs(n = 33)
Re-admission(n = 11)
Non-English(n = 10)
Norelatives(n = 2)
Mentalillness(n = 2)
AgeMean (S.D.) 56.1 (17.6) 54.9 (18.7) 52.8 (18.7) 56.4 (20.1) 46.6 (19.5) 59.0 (17.3) 56.7 (22.5) 55.4 (16.4) 37.5 (19.1) 46.5 (23.3)Median 59.5 60.5 59 63 52 66 67 59 37.3 46.5
GenderMales (%) 19 (56) 92 (64) 36 (68) 20 (51) 3 (60) 22 (67) 10 (91) 8 (80) 2 (100) 2 (100)Females (%) 15 (44) 52 (36) 17 (32) 19 (49) 2 (40) 11 (33) 1 (9) 2 (20) 0 0
ICU LOS (hours)Median 95 46 142 19 67 22 97 94 115 273
Hospital LOS (days)Mean (S.D.) 31 (26) 24 (28) 38 (34) 9 (15) 7 (5) 18 (16) 57 (32) 41 (36) 31 (9) 29 (15)Median 22 15 25 2 8 12 56 22 31 29
APACHEMean 17 (7) 19 (8) 17 (7) 25 (6) 12 (8) 14 (6) 19 (4) 19 (7) 26 (16) 14 (6)Median 16 18 17 25 11 14 21 21 26 13.5
TISSMean/day 29 (15) 30 (20) 26 (8) 32 (19) 22 (5) 36 (34) 29 (14) 24 (6) 30 (1) 21 (5)Median 28 27 27 29 20 26 28 25 30 21
Admitted from (%)Emergency department 15 (44) 65 (45) 27 (51Operating suite 9 (26) 48 (34) 15 (28Cardiothorcic ICU 0 5 (4) 4 (8)High dependency 5 (15) 19 (13) 5 (9)General ward 2 (6) 3 (2) 2 (4)Imaging department 3 (9) 3 (2) 0
371
) 14 (35) 2 (40) 17 (52) 0 5 (50) 0 1) 15 (39) 2 (40) 10 (30) 2 (18) 4 (40) 1 (50) 2 (100)
1 (3) 0 0 0 0 0 07 (18) 1 (20) 5 (15) 3 (28) 1 (10) 0 01 (3) 0 0 5 (46) 0 0 01 (3) 0 1 (3) 1 (9) 0 1 (50) 0

372 D. Elliott et al.
Table 2 outlines the demographic and clinicalvariables for the sub-study participants and non-participants. Mean age, ICU LOS, hospital LOS,APACHE II, and TISS all demonstrated homogene-ity, and the proportions for gender and admissionsource were also found to be equivalent. No signifi-cant differences were found inmale:female propor-tions for the participant group and non-participantgroups. A significant difference was found in theadmission source (χ2 = 67.99; P = .004), althoughsome of this difference may be accounted for bysmall and zero cell sizes. The participant group wasrepresentative of all groups for patient acuity (mea-sured by APACHE), except the ‘deaths’ group. Thesefindings indicated that the participant group wasrepresentative of the overall ICU patient popula-tion.
Approximately half of the participants com-pleted all measurement points (n = 17), but sevencompleted only one measurement. Two recruitedpatients died prior to completing the first measure-ment, leaving 32 participants at the pre-admissionmeasurement. Seventeen participants completedall four measures, with a further two complet-ing all but the hospital discharge measure and an-
eas
spectively. It was not clear why this decrease oc-curred between the final two measurements. In-structions to the respondents were for the indexrespondent to complete the questionnaires person-ally if able. The proxy carer may have disregardedthis instruction so as not to inconvenience the indexrespondent.
Using 15D, participants reported a similarhealth status at 6 months post-discharge to thatindicated by their proxy respondents at thepre-ICU measure (see Table 3). The ICU dis-charge measure was statistically significantly lowerthan other measurement points for: (1) mobil-ity;breathing;eating;speech;elimination;usual ac-tivities;vitality; and sexual activity when com-pared to pre-admission status; (2) breathingand eating when compared to hospital dis-charge; (3) mobility, eating, usual activities,and vitality when compared to 6 months post-discharge.
In general, the participants returned to anequivalent or slightly better state of health at 6months post-discharge when compared to their pre-crisis health state, as measured by SF-36. Thatis, no statistically significant differences for theemssmcmw
other three completing all but the last measure.Two completed only the hospital measures, and sixcompleted only the first measure. Proxy respon-dents completed all but one of the patients’ pre-admission health status measurements. Completionby index respondents increased to 26, 70 and 42%for the ICU discharge, hospital discharge and 6months post-hospital discharge measurements, re-
Table 3 One-way ANOVA Table for 15D scores across m
Variable Statistical significance
F P
Mobility 6.30 .0006Vision 1.98 .12Hearing 0.96 .42Breathing 5.44 .0017Sleeping 2.24 .0889Eating 9.10 .0000Speech 4.70 .0042Elimination 4.84 .0035Usual activities 5.57 .0015Mental function 2.94 .0372Discomfort/symptoms 0.90 .0444Depression 2.28 .0848Distress 1.69 .1754Vitality 5.76 .0012Sexual activity 3.73 .0145
ures.
Differences
Pre-ICU Post-ICU Hospitaldischarge
6 monthspost
Post-ICU Post-ICU
Post-ICU Post-ICU
Post-ICU Post-ICU Post-ICUPost-ICUPost-ICUPost-ICU Post-ICU
Post-ICU Post-ICUPost-ICU
ight health concepts and two component sum-ary scales of SF-36 when the pre-ICU healthtate and the 6 months post-discharge health-statecores were examined (see Table 4). At the 6-onth measure, one third of participants indi-ated that their health was about the same as 12onths ago, whilst 47% were somewhat or muchorse.

Examining discharge outcomes and health status of critically ill patients 373
Table 4 SF-36 scores for two measures.
Dimensions Pre-ICU, mean (S.D.) 6 months post-discharge,mean (S.D.)
Significance
n = 32 n = 19 t P
Physical Functioning (PF) 50 (39) 57 (38) 0.582 .563Role Functioning—–Physical (RP) 56 (44) 54 (44) 0.133 .895Bodily Pain (BP) 68 (25) 75 (25) −0.997 .324General Health (GH) 46 (24) 54 (24) −1.198 .237Vitality (VT) 48 (19) 49 (20) −0.240 .812Social Functioning (SF) 68 (21) 70 (21) −0.257 .798Role Functioning—–Emotional (RE) 66 (42) 65 (42) 0.055 .957Mental Health (MH) 53 (26) 52 (27) 0.182 .857Physical Component Summary (PCS) 40 (15) 44 (13) −0.936 .354Mental Component summary (MCS) 44 (11) 43 (10) 0.407 .686
Health Transition (HT)Frequency (%)Much better 0 0Somewhat better 2 (6) 4 (21)About the same 17 (53) 6 (32)Somewhat worse 7 (22) 8 (42)Much worse 6 (19) 1 (5)
Discussion
Major findings
This study examined the discharge outcomes of 200consecutive admissions to a general ICU. Of the189 individual patients, 23% died in ICU. Eligiblepatients (and their proxies) also participated in asub-study assessing health status, with 34 agreeingto be involved. Participants were representative ofgeneral ICU patients in this sample.
Surviving participants returned to a similar stateof health at hospital discharge and 6 months post-discharge when compared to their pre-ICU healthcrisis state as measured by 15D and SF-36. The par-ticipants’ health status at ICU discharge was sig-nificantly impaired when compared to the othermeasurement points, particularly in terms ofmobil-ity, breathing, eating, usual activities, and vitality.This was a logical finding, given the subjects’ clin-ical condition, but does highlight the dimensionsmost affected by an episode of critical illness.These specific dimensions could be targeted for im-proved management of patients after their ICU stay(Hurel et al., 1997). There were no significant dif-fdt
sln
were reported for the majority of patients 12months after a critical illness (Badia et al., 2001).However, in another study approximately half thepatients reported moderate to extreme problemswith usual activities, pain/discomfort, and anxi-ety/depression at 6 months post-illness (Granja etal., 2002).
Of interest in this study was the finding of littlechange in measured health status for 15D betweenhospital discharge and 6 months post-discharge.The reason for this is not clear. It would seem rea-sonable that some improvement would occur overthat 6-month period. This finding may have beenbecause patients had already reached their optimalfunction. Alternatively, 15D may not demonstrateadequate responsiveness to measure the functionalchange in individuals. This does occur with instru-ments that have minimal items per dimension. Un-fortunately, other similar studies did not assesspost-hospital discharge status (Badia et al., 2001;Granja et al., 2002).
Pre-illness SF-36 scores were similar to otherstudies conducted in Europe and North America(Graf et al., 2003; Ridley et al., 1997; Welsh et al.,1999). When compared to age-matched AustralianpBSaNsa
erences across measurement points for the 15Dimensions vision, hearing, sleeping, mental func-ion, discomfort/symptoms, depression or distress.Whilst direct comparison with other critical care
tudies was not possible with 15D, the equiva-ent concepts in EQ-5D provide some opportu-ity for exploration. Similar findings to this study
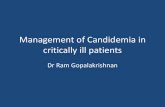
opulation norms (ABS, 1995), all domains exceptodily Pain were substantially lower (see Fig. 1).tudies using SF-36 in Australia (Boyle et al., 2004)nd other countries (Canada, Finland, Germany,orway, United Kingdom) have also demonstratedignificantly lower scores for critically ill patientst pre-ICU or 6—12 months post-illness, when

374 D. Elliott et al.
Figure 1. SF-36 mean scores compared to population norms.
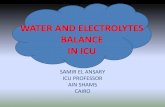
Figure 2. Comparison of 6-month SF-36 mean scores with similar studies.

Examining discharge outcomes and health status of critically ill patients 375
compared to population normative data (Eddlestonet al., 2000; Graf et al., 2003; Herridge et al., 2003;Kvale et al., 2003; Pettila et al., 2000; Wehler etal., 2003). Another study also found similar find-ings when using a different HR-QOL questionnaireand a community group comparison (Brooks et al.,1997).
Fig. 2 displays the 6-month SF-36 scores for thisstudy and similar studies that provided enough datato enable comparisons. Two studies are Australian(Boyle et al., 2004; Chaboyer et al., 2002), whilstthe others are British (Ridley et al., 1997) and Cana-dian (Herridge et al., 2003). One study noted im-provements in functional status for patients withpre-existing illnesses, at 6 months after their ICUadmission. In contrast, those previously well pa-tients who suffered an acute critical illness hadsignificant poorer HRQOL (Ridley et al., 1997). Asnoted, similar scores are evident for most domainswith the exception of Mental Health and PhysicalRole limitations. It is unclear why Mental Healthis substantially lower in this study compared toother studies, but it was equivalent to the pre-ICUscore (these scores were even lower for the pilotstudy). The Physical Role score for the HerridgesAtm
ss2(Se2Sevi
L
Aicis
STcai
to the sub-study was however problematic. Patientswere critically ill on initial presentation and usuallyunable to respond. The next-of-kin were dealingwith the crisis of the patient’s illness and admis-sion that may well have affected their willingnessto participate. Some studies exclude patients whoare not able to respond whilst in ICU or step-downward (Badia et al., 1996; Welsh et al., 1999), al-though this then creates a problem with generalis-ability.
For this study, prospective recruitment of rela-tives whilst visiting the ICU was difficult. Visitingwas an emotionally traumatic time for the rela-tives, and direct approaches by the researchers wasoften met with the reply of ‘Can I look at this or doit later?’. Study packages were given to relativeswho did not refuse outright, but these approacheswere often not rewarded with completed responsesdespite follow-up. It was also difficult to see therelatives because of their varied visiting times andthe open visiting policy of the ICU.
In addition, the physical environment of the ICUwas not conducive to participant recruitment, as itwas difficult to speak privately with relatives withinthe highly technical, busy and noisy setting (Grafatfmwevptloea
fp2cioSo2
USpedos
tudy (2003) can be explained by their sample ofRDS patients with characteristics quite differento the comparative studies (APACHE II score: 23,edian ICU LOS: 25 days, average age: 45 years).Other studies using SF-36 generally demon-
trated similar findings, but used different mea-urement points—–3 months (Eddleston et al.,000); 9 months (Graf et al., 2003); 12 monthsPettila et al., 2000), or did not provide specificF-36 domain scores to allow comparisons (Jonest al., 2003; Kvale et al., 2003; Chelluri et al.,004). Studies using different instruments such asIP (Gardner and Sibthorpe, 2002) or NHP (Niskanent al., 1999) also demonstrated satisfactory butariable recovery of HR-QOL for survivors of a crit-cal illness.
imitations
number of important methodological issues weredentified during the conduct of this study involvingritically ill patients, and are discussed below tonform any future critical review or design of healthtatus studies with survivors of a critical illness:
ubject recruitment and retentionhe difficulties with prospective participant re-ruitment were not apparent in the pilot study, asconvenience sample was used rather than all el-gible consecutive patient admissions. Recruitment
nd Munro, 2003). To counteract this, personal let-ers were sent to the relatives’ home address, withollow-up phone-calls. This assumed that relativesay have felt more inclined to be involved if theyere introduced to the study in their familiar homenvironment, and not when they were focused onisiting their ill relative. This modification did im-rove the response rate slightly, although still noto an optimal level. Others have noted similar prob-ems (Graf and Munro, 2003). It is therefore rec-mmended that recruitment be delayed until thepisode of critical illness has passed and patientsre ready for or have been discharged from the ICU.Subject loss to follow-up is a common problem
or longitudinal studies, and particularly when thearticipants have a critical illness (Jones and Lyons,003). Both ICU/hospital mortality and persistentognitive or psychomotor dysfunction were evidentn this ICU sample, as indicated by the proportionf proxy respondents completing those measures.imilar losses to follow-up have been reported inther studies (Boyle et al., 2004; Chaboyer et al.,002).
se of proxy respondentsome previous studies of ICU patients that usedroxy respondents (e.g. Konopad et al., 1995; Matat al., 1992) assumed direct correlation with the in-ex respondent and did not discuss the issue of levelf agreement. More recent studies have demon-trated that proxy respondents provide fair but not

376 D. Elliott et al.
identical agreement (Badia et al., 1996; Hofhuis etal., 2003; Rogers et al., 1997). Despite this, the useof proxies to measure concurrent health status ofpatients, rather than retrospective assessment, ap-pears to be feasible and appropriate in this clinicalsample.
Instrument responsivenessThe finding of no significant differences in 15Dscores between hospital discharge and 6 monthspost-discharge may indicate a lack of appropriateprecision in this instrument. SF-36 currently has thebenefit of population normative data, findings fromsimilar clinical samples for comparative analysis,and has been identified as appropriate for follow-upof survivors of a critical illness (Black et al., 2001;Chrispin et al., 1997; Elliott, 1999), although notduring the post-ICU hospital period (Kvale et al.,2003). Perhaps 1—4 weeks after hospital dischargewould be a useful measurement point to examineinstrument responsiveness (Graf et al., 2003).
Conclusions
Acknowledgements
This study was supported in part by funds from theWestmead Hospital Charitable Trusts. Our thanks goto the patients and their next-of-kin for their in-volvement at a time of personal and family crisis.
References
Angus DC, Carlet J. Surviving intensive care: a report from the2002 Brussels Roundtable. Intens Care Med 2003;29:368—77.
Australian Bureau of Statistics (ABS). National Health Survey:SF-36 Population Norms. Sydney: Australia Pub. 4399.0, ABS;1995.
Badia X, Diaz-Prieto A, Rue M, Patrick DL. Measuring health andhealth-state preferences among critically ill patients. IntensCare Med 1996;22:1379—84.
Badia X, Diaz-Prieto A, Gorriz MT, Herdman M, Torrado H, FarreroE, et al. Using the EuroQol-5D to measure changes in qualityof life 12 months after discharge from an intensive care unit.Intens Care Med 2001;27:1901—7.
Black NA, Jenkinson C, Hayes JA, Young D, Vella K, Rowan KM, etal. Review of outcome measures used in adult critical care.Crit Care Med 2001;29:2119—24.
Boyle M, Murgo M, Adamson H, Gill J, Elliott D, CrawfordM. The effect of chronic pain on health related qualityof life amongst intensive care survivors. Aust Crit Care
B
B
C
C
C
C
E
E
G
G
G
G
The majority of patients admitted to this ICU duringthe study period were discharged home, althoughthere was cumulative hospital mortality of 28%. Thesurvivors in the health status sub-study returned totheir pre-crisis health status at hospital dischargeand 6 months post-discharge, although this was sub-stantially lower than population norms for most do-mains. The study demonstrated that generic healthstatus instruments can be used in the study of out-comes of patients who are admitted to a generalICU in a critical condition. It is recommended thatlarger studies be conducted, with procedures de-veloped to ensure a higher response rate, to verifythe findings presented here.
Routine use of valid HRQOL instruments mayprovide important information when managing theentire episode of critical illness, including whensurvivors are transferred from ICU. Patient-basedinformation, in functional terms that patientsand their families can readily understand, canhighlight specific areas of health status that aresubstantially affected during the patient’s criticalillness, hospitalization, and recovery period. Thisinformation can assist nurses (including ICU liaisonroles), doctors and allied health staff involved inthe continued management of patients followingICU discharge, and in guiding patient and fam-ily expectations regarding their recovery post-hospitalization.
2004;17:104—13.rooks R. EuroQol: the current state of play. Health Policy1996;37:53—72.
rooks R, Kerridge R, Hillman K, Bauman A, Daffurn K. Qual-ity of life outcomes after intensive care: comparison with acommunity group. Intens Care Med 1997;23:581—6.
haboyer W, Elliott D. Health-related quality of life of ICUsurvivors: a review of the literature. Intens Crit Care Nurs2000;16:88—97.
haboyer W, Foster M, Creamer J. Health status of ICU survivors:a pilot study. Aust Crit Care 2002;15:21—6.
helluri L, Kyung AI, Belle SH, Schulz R, Rotondi AJ, Donahoe MP,et al. Long-term mortality and quality of life after prolongedmechanical ventilation. Crit Care Med 2004;32:61—9.
hrispin PS, Scotton H, Rogers J, Lloyd D, Ridley SA. Shortform 36 in the intensive care unit: assessment of acceptabil-ity, reliability and validity of the questionnaire. Anaesthesia1997;52:15—23.
ddleston JM,White P, Guthrie E. Survival, morbidity, and qualityof life after discharge from intensive care. Crit Care Med2000;28:2293—9.
lliott D. Measuring the health outcomes of general ICU patients:a systematic review of methods and findings. Aust Crit Care1999;12:132—40.
ardner A, Sibthorpe B. Will he get back to normal? Survivaland functional status after intensive care therapy. Intens CritCare Nurs 2002;18:138—45.
raf J, Koch M, Dujardin R, Kersten A, Janssens U. Health-relatedquality of life before, 1 month after, and 9 months after in-tensive care in medical cardiovascular and pulmonary pa-tients. Crit Care Med 2003;31:2163—9.
ranja C, Teixeira-Pinto A, Cost-Pereira A. Quality of life afterintensive care: evaluation with EQ5-D questionnaire. IntensCare Med 2002;28:898—907.
raf MJ, Munro CL. Subject recruitment in critical care nursingresearch: a complex task in a complex environment. HeartLung 2003;32:162—8.

Examining discharge outcomes and health status of critically ill patients 377
Guadagnoli E, Cleary PD. How consistent is patient-reported pre-admission status when collected during and after hospitalstay? Med Care 1995;33:106—12.
Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F, et al. One-year outcomes in survivorsof the acute respiratory distress syndrome. N Engl J Med2003;348:683—93.
Herrman D. Reporting current, past, and changed health status:what we know about distortion. Med Care 1995;33:AS89—94.
Heyland DK, Guyatt G, Cook DJ, Meade M, Juniper E, CroninL, et al. Frequency and methodologic rigor of quality-of-life assessments in the critical care literature. Crit Care Med1998;26:591—8.
Hofhuis J, Hautvast JLA, Schrijvers AJP, Bakker J. Quality of lifeon admission to the intensive care: can we query the rela-tives? Intens Care Med 2003;29:974—9.
Hurel D, Loirat P, Saulnier F, Nicolas F, Brivet F. Quality of life sixmonths after intensive care: results of a prospective multi-center study using a generic health status scale and a satis-faction scale. Intens Care Med 1997;23:331—7.
Jones C, Lyons C. Researching the experience of being criticallyill: some methodological difficulties. Intens Crit Care Nurs2003;19:365—9.
Jones C, Skirrow P, Griffiths RD, Humphris GH, Ingleby S, Eddle-ston J, et al. Rehabilitation after critical illness: a random-ized, controlled trial. Crit Care Med 2003;31:2456—61.
Keene AR, Cullen DJ. Therapeutic intervention scoring system:update. Crit Care Med 1983;11:1—3.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II:a severity of disease classification system. Crit Care Med
K
K
M
M
McCarthy MJ, Shroyer AL, Sethi GK, Moritz TE, HendersonWG, Grover FL, et al. Self-report measures for assessingtreatment outcomes in cardiac surgery patients. Med Care1995;33:OS76—85.
Niskanen M, Ruokonen E, Takala J, Rissanen P, Kari A. Qual-ity of life after prolonged intensive care. Crit Care Med1999;27:1132—9.
Pettila V, Kaarlola A, Makelainen A. Health-related quality of lifeof multiple organ dysfunction patients one year after inten-sive care. Intens Care Med 2000;26:1473—9.
Reis Miranda D, Nap R, de Rijk A, Schaufeli W, Iapichino G. Nurs-ing activities score. Crit Care Med 2003;31:374—82.
Ridley SA. Survival and quality of life after intensive care. ClinIntens Care 1999;10:117—23.
Ridley SA, Chrispin PS, Scotton H, Rogers J, Lloyd D. Changesin quality of lafter intensive care: comparison with normaldata. Anaesthesia 1997;52:195—200.
Rogers J, Ridley S, Chrispin P, Scotton H, Lloyd D. Reliability ofthe next of kins’ estimates of critically ill patients’ qualityof life. Anaesthesia 1997;52:1137—43.
Rubenfeld GD, Angus DC, Pinsky MR, Curtis JR, Connors AF,Bernard GR. Outcomes research in critical care. Am J RespirCrit Care Med 1999;160:358—67.
Sintonen H, Pekurinen M. A fifteen-dimensional measure ofhealth-related quality of life (15D) and its applications. In:Walker S, Rosser R, editors. Quality of life assessment: keyissues in the 1990s. Dordrecht: Kluwer Academic Publishers;1990. p. 185—95.
Ware JE. SF-36 health survey update. Spine 2000;24:3130—9.Ware JE, Sherbourne CD. The MOS 36-item short-form health
W
W
W
1985;13:818—29.onopad E, Noseworthy TW, Johnston R, Shustack A, Grace M.Quality of life measures before and one year after admissionto an intensive care unit. Crit Care Med 1995;23:1653—9.
vale R, Ulvik A, Flaatten H. Follow-up after intensive care: asingle center study. Intens Care Med 2003;29:2149—56.
ata G, Fernendez R, Carmona A, Delgado-Rodriguez M, Ruiz J,Pugnaire A, et al. Factors related to quality of life 12 monthsafter discharge from an intensive care unit. Crit Care Med1992;20:1257—62.
endelsohn AB, Chelluri L. Interviews with intensive care unitsurvivors: assessing post-intensive care quality of life and pa-tients’ preferences regarding intensive care and mechanicalventilation. Crit Care Med 2003;31:S400—6.
survey (SF-36): I. Conceptual framework and item selection.Med Care 1992;30:473—83.
are JE, Snow KK, Kosinski M, Gandek B. SF-36 health sur-vey manual and interpretation guide. Boston: Nimrod Press;1993.
ehler M, Geise A, Hadzionerovic D, Aljukic E, Reulbach U,Hahn EG, et al. Health-related quality of life of patients withmultiple organ dysfunction: individual changes and compari-son with normative population. Crit Care Med 2003;31:1094—101.
elsh CH, Thompson K, Long-Krug S. Evaluation of patient-perceived health status using the Medical Outcomes SurveyShort-Form 36 in an intensive care unit population. Crit CareMed 1999;27:1466—71.