
Examination of theof the Knee - Foundation for … of the Knee zThis is an article that we published...
19
5/25/2016 1 Thank You Thank You z Thanks to Thanks to RUSH 2016 SPORTS RUSH 2016 SPORTS MEDICINE SYMPOSIUM MEDICINE SYMPOSIUM for the for the kind invitation to present at this kind invitation to present at this course course z It is indeed an honor and privilege It is indeed an honor and privilege to be invited to participate and to be invited to participate and share information. share information. George J. Davies, DPT, MED, PT, SCS, ATC, LAT, CSCS, NASM-PES, NASM-CES, ACSM-CET, APTA-CCI, SMAC, (REMT), FAPTA Professor of Physical Therapy, AASU, Savannah, GA. (2004- ) Professor Emeritus UW-LaCrosse, WI. (1975-2004) Consultant, Clinician, Co-Director Clinical and Research Services– Sports PT Residency Program , GLSM, La Crosse, WI. (1995-present) Sports PT, Coastal Therapy, Savannah, GA. (2004- present) Past President Sports Physical Therapy Section – APTA (1992-1998) JOSPT - Co-Founder & Co-Editor, 1979 JOSPT - GJD-JAG Excellence in Clinical Research Award, 2004 Fellow, APTA, 2005, Hall of Fame Award, SPTS-APTA, 2006 NATA, President’s Award, 2007, NATA, Most Distinguished Athletic Trainer, 2009 Sports Health Sports Health - Co-Founder & Co-Editor, 2009 AOSSM AOSSM – Hall of Fame Award, 2013 Disclosures: Disclosures: Associate Editor, Associate Editor, Sports Health Sports Health PUBMED Elsevier Elsevier-Book Royalties Book Royalties Human Kinetics Human Kinetics-Book Royalties Book Royalties Williams & Wilkins Williams & Wilkins-Book Royalties Book Royalties North American Seminars North American Seminars-DVD DVD Royalties Royalties No Conflicts No Conflicts INDEX MEDICUS 2015 Disclosures: Disclosures: Editor Editor Elsevier Elsevier- Book Royalties Book Royalties Conflicts Conflicts 2015 2015 Disclosures: Disclosures: The following companies have The following companies have provided research equipment provided research equipment support to Biodynamics & Human support to Biodynamics & Human Performance Center Performance Center-AASU: AASU: Arthrometrics Arthrometrics, Atlanta, GA. , Atlanta, GA. Biodex, Shirley, N.Y. Biodex, Shirley, N.Y. CDM Sport/Monitored Rehab CDM Sport/Monitored Rehab Systems, Fort Worth, TX. Systems, Fort Worth, TX. DS2 Rehab Systems, Missouri City, DS2 Rehab Systems, Missouri City, TX TX ERMI, Atlanta, GA. ERMI, Atlanta, GA. ExerTools ExerTools, Petaluma, CA. , Petaluma, CA. Innovative Sports Inc, Chicago, IL. Innovative Sports Inc, Chicago, IL. TheraBand TheraBand, , Hygenic Hygenic Corporation, Corporation, Akron, OH. Akron, OH. No Conflicts No Conflicts Disclosures: Disclosures: “Gladly accept “Gladly accept money from money from anyone for anyone for Institutional Institutional Research Research Support….” Support….” No Conflicts No Conflicts Examination of the of the Knee Casual interest in the Casual interest in the knee knee for the last for the last 51 years 51 years since I since I 51 years 51 years since I since I started as a student started as a student athletic trainer in 1965 athletic trainer in 1965 !!! !!!
Transcript of Examination of theof the Knee - Foundation for … of the Knee zThis is an article that we published...
5/25/2016
1
Thank YouThank YouThanks to Thanks to RUSH 2016 SPORTS RUSH 2016 SPORTS MEDICINE SYMPOSIUM MEDICINE SYMPOSIUM for the for the kind invitation to present at this kind invitation to present at this coursecourse
It is indeed an honor and privilege It is indeed an honor and privilege to be invited to participate and to be invited to participate and
share information. share information.
George J. Davies, DPT, MED, PT, SCS, ATC, LAT, CSCS, NASM-PES, NASM-CES, ACSM-CET, APTA-CCI, SMAC, (REMT), FAPTA
Professor of Physical Therapy, AASU, Savannah, GA. (2004- )
Professor Emeritus UW-LaCrosse, WI. (1975-2004)
Consultant, Clinician, Co-Director Clinical and Research Services–Sports PT Residency Program , GLSM, La Crosse, WI. (1995-present)
Sports PT, Coastal Therapy, Savannah, GA. (2004- present)
Past President Sports Physical Therapy Section – APTA (1992-1998)
JOSPT - Co-Founder & Co-Editor, 1979
JOSPT - GJD-JAG Excellence in Clinical Research Award, 2004
Fellow, APTA, 2005, Hall of Fame Award, SPTS-APTA, 2006
NATA, President’s Award, 2007, NATA, Most Distinguished Athletic Trainer, 2009
Sports Health Sports Health - Co-Founder & Co-Editor, 2009
AOSSMAOSSM – Hall of Fame Award, 2013
Disclosures:Disclosures:
Associate Editor, Associate Editor, Sports HealthSports HealthElsevierElsevier--Book RoyaltiesBook RoyaltiesPUBMED ElsevierElsevier--Book RoyaltiesBook RoyaltiesHuman KineticsHuman Kinetics--Book RoyaltiesBook RoyaltiesWilliams & WilkinsWilliams & Wilkins--Book RoyaltiesBook RoyaltiesNorth American SeminarsNorth American Seminars--DVDDVDRoyalties Royalties
No ConflictsNo Conflicts
INDEX MEDICUS2015
Disclosures:Disclosures:
Editor Editor ElsevierElsevier--Book RoyaltiesBook Royalties
ConflictsConflicts
20152015
Disclosures:Disclosures:The following companies have The following companies have provided research equipment provided research equipment support to Biodynamics & Human support to Biodynamics & Human Performance CenterPerformance Center--AASU:AASU:
ArthrometricsArthrometrics, Atlanta, GA. , Atlanta, GA. Biodex, Shirley, N.Y.Biodex, Shirley, N.Y.CDM Sport/Monitored Rehab CDM Sport/Monitored Rehab Systems Fort Worth TXSystems Fort Worth TXSystems, Fort Worth, TX.Systems, Fort Worth, TX.DS2 Rehab Systems, Missouri City,DS2 Rehab Systems, Missouri City,TXTXERMI, Atlanta, GA.ERMI, Atlanta, GA.ExerToolsExerTools, Petaluma, CA., Petaluma, CA.Innovative Sports Inc, Chicago, IL. Innovative Sports Inc, Chicago, IL. TheraBandTheraBand, , HygenicHygenic Corporation,Corporation,Akron, OH. Akron, OH.
No ConflictsNo Conflicts
Disclosures:Disclosures:
“Gladly accept “Gladly accept money from money from anyone for anyone for Institutional Institutional Research Research Support….”Support….”
No ConflictsNo Conflicts
Examination of theof the Knee
Casual interest in the Casual interest in the knee knee
for the last for the last 51 years51 years since Isince I51 years 51 years since I since I
started as a student started as a student athletic trainer in 1965 athletic trainer in 1965
!!!!!!

5/25/2016
2
P & SM, 1978P & SM, 1978
Examination of the KneeExamination of the KneeThis is an article that we published This is an article that we published 38 years ago38 years ago in the Physician and in the Physician and SportsMedicineSportsMedicine that was that was used for used for CME’s for physicians.CME’s for physicians.CME s for physicians. CME s for physicians. At that time it was “At that time it was “state of the state of the artart”, and it’s interesting how much ”, and it’s interesting how much of that that art has stayed the of that that art has stayed the same, with of course, some same, with of course, some changes!changes!
Examination of Examination of the Knee:the Knee:
How do we doHow do we doHow do we do How do we do it?it?
Subjective,
Objective
Subjective,
Objective
&
Functional Examination
&
Functional Examination
Subjective Examination and History of the Knee
Complex
Subjective Examination and History of the Knee
Complex
KneeKneeMechanism of InjuryMechanism of Injury
Subjective Exam Subjective Exam ComponentsComponents
Demographic informationLocation of symptomsD i tDominant armMOIHistory: present & pastBehavior of symptoms: rest, ADL’s, work, sports, AM/PM
SubjectiveSubjectiveExam ComponentsExam Components
Diagnostic tests & Imaging StudiesLab tests
Medical systems review: questionnaire and interview (Differential DX.)MedsMedsPrevious treatmentsPrevious functional statusPatient’s goals
Differential DiagnosisDifferential DiagnosisDifferential DiagnosisDifferential Diagnosis
Systems reviewSystems review and differential diagnosis

5/25/2016
3
Functional Testing Algorithm –Knee -2016
Sport Specific TestingLower Extremity Functional Tests Functional Hop TestsFunctional Jump Tests
Competitive Competitive AthletesAthletes
RecreationalRecreationalFunctional Jump TestsOKC Isokinetic testing CKC Isokinetic TestingSensorimotor System Testing: Balance/Proprioceptive TestingKT 1000/2000 Basic MeasurementsBasic Measurements
RecreationalRecreationalAthletesAthletes
GeneralGeneralOrthopaedicOrthopaedic
PatientsPatients
Functional Testing AlgorithmFunctional Testing AlgorithmSports Specific Tests Sports Specific Tests Lower Extremity Functional Tests Lower Extremity Functional Tests Functional Hop Tests Functional Hop Tests Functional Jump Tests Functional Jump Tests OKC Isokinetic TestsOKC Isokinetic TestsOKC Isokinetic Tests OKC Isokinetic Tests CKC Isokinetic Tests CKC Isokinetic Tests Kinesthetic/Balance Tests Kinesthetic/Balance Tests KT 1000 TestsKT 1000 TestsSpecial Tests Special Tests –– ONLY 175 + 1ONLY 175 + 1Basic MeasurementsBasic Measurements
FTA Specific GuidelinesFTA Specific GuidelinesLEFT LEFT –– MM--1:30; F1:30; F--2:00 minutes2:00 minutesHOP HOP -- < 10%Ht.; < 10%Ht.; < 10% < 10% bilatbilat. Comp.; . Comp.; Norms/various hops Norms/various hops JUMP JUMP -- < 15%/Ht.; Norms< 15%/Ht.; NormsOKC Isokinetics OKC Isokinetics -- < 25% bilateral < 25% bilateral comparison/other criteriacomparison/other criteriacomparison/other criteriacomparison/other criteriaCKC Isokinetics CKC Isokinetics -- < 30% bilateral < 30% bilateral comparisoncomparisonKinesthetic/Balance Testing Kinesthetic/Balance Testing –– BilatBilatcompcompKT 1000 KT 1000 -- < 3 mm bilateral comparison< 3 mm bilateral comparisonBasic Measurements Basic Measurements -- < 10% bilateral < 10% bilateral comparisoncomparison
Basic MeasurementsBasic MeasurementsBasic MeasurementsBasic MeasurementsTime/soft tissue healingTime/soft tissue healingVAS (0VAS (0--10 scale)10 scale)Anthropometric Anthropometric measurementsmeasurementsmeasurementsmeasurementsAROM, PROMAROM, PROMSpecial TestsSpecial TestsQualitative & Quantitative Qualitative & Quantitative Movement AssessmentMovement AssessmentKnee Rating scales: IKDC, etc.Knee Rating scales: IKDC, etc.
Basic MeasurementsBasic MeasurementsBasic MeasurementsBasic MeasurementsMD Clearance & Approval MD Clearance & Approval Time/soft tissue healingTime/soft tissue healingVAS (0VAS (0--10 scale)10 scale)Anthropometric measurementsAnthropometric measurementsAROM, PROMAROM, PROMSpecial TestsSpecial TestsQualitative & Quantitative Qualitative & Quantitative Movement AssessmentMovement AssessmentKnee Rating scales: IKDC, etc.Knee Rating scales: IKDC, etc.
Functional Testing AlgorithmFunctional Testing Algorithm
TIME:TIME:
Soft tissue healing Soft tissue healing from th i jthe injury or
from a
post-surgical condition
ACL Quad Tendon ACL Quad Tendon Graft HealingGraft Healing
Dark Quad Dark Quad Tendon PreTendon Pre--
OpOp
6 months PO6 months PO1 month PO1 month POTime ZeroTime Zero
We still have not We still have not answered this Question?answered this Question?
Biologics and “mother nature” Biologics and “mother nature” d thd thand the:and the:
NeoangiogenesisMaturationLigamentization

5/25/2016
4
Functional Testing AlgorithmFunctional Testing Algorithm
TIME:TIME: Soft Soft tissue healingtissue healingWe need similar types of outcomesWe need similar types of outcomesWe need similar types of outcomes We need similar types of outcomes regarding the regarding the biology of healingbiology of healing
We can’t hurry We can’t hurry “mother nature”;“mother nature”;
Although we are trying with all the Although we are trying with all the biologics!!!biologics!!!
Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making
Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making
HamstringsHamstrings
BTBBTB
Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making
Perhaps wait for 3-6 more months to allow the biologics to “do“dothe biologics to do do their job”….their job”….
Basic MeasurementsBasic MeasurementsBasic MeasurementsBasic Measurements
Time/soft Time/soft tissuetissuetissue tissue healinghealing
ACL Quad Tendon ACL Quad Tendon Graft HealingGraft Healing
Dark Quad Dark Quad Tendon PreTendon Pre--
OpOp
6 months PO6 months PO 1 year PO1 year PO1 month PO1 month POTime ZeroTime Zero
Clinical Decision Making Clinical Decision Making Clinical Decision Making Clinical Decision Making
Then we return Then we return him back tohim back tohim back to him back to sports sports
5/25/2016
5
Physical Physical ((ObjectiveObjective) )
E i tiE i tiExamination Examination of the Kneeof the Knee
Physical Examination/Physical Examination/Tests & MeasurementsTests & Measurements
Observation/posture
Gait EvaluationQ & Q Movement Assessment Referral/related
Physiological PROMAccessory/Jt. Play PROMKT 1000Flexibility TestsReferral/related
jointsNeurological ExamSensation, reflexesKinesthetic/proprioceptiveBalance Neural TT
PalpationAROM
RROM (MMT/HHD)Special TestsComputerized isokinetic testing Functional TestingFunctional TestingImaging StudiesLab Studies
Physical Examination of the Physical Examination of the KneeKnee
1)1) Most physical exam tests should Most physical exam tests should be referenced back to the original be referenced back to the original descriptiondescription2)2) SensitivitySensitivity3)3) SpecificitySpecificity4) 4) Likelihood ratiosLikelihood ratios5) 5) PPVPPV6) 6) NPVNPV
Functional Testing Algorithm –Knee -2016
Sport Specific TestingLower Extremity Functional Tests Functional Hop TestsFunctional Jump Tests
Competitive Competitive AthletesAthletes
RecreationalRecreationalFunctional Jump TestsOKC Isokinetic testing CKC Isokinetic TestingSensorimotor System Testing: Balance/Proprioceptive TestingKT 1000/2000 Basic MeasurementsBasic Measurements
RecreationalRecreationalAthletesAthletes
GeneralGeneralOrthopaedicOrthopaedic
PatientsPatients
Functional Testing Algorithm Functional Testing Algorithm ––KneeKnee
Objective, quantitative (and Objective, quantitative (and qualitative), systematic qualitative), systematic testing and rehabilitation testing and rehabilitation methodmethod to safely and rapidlyto safely and rapidlymethod method to safely and rapidly to safely and rapidly progress a patient from progress a patient from immediate post injury/postimmediate post injury/post--op to return to full functional op to return to full functional activities and return to play in activities and return to play in sports sports
Functional Testing Algorithm Functional Testing Algorithm ––KneeKnee
Progression to the next higher level of testing difficulty is predicated upon passing the prior test in the series…
Each successive test and its associated training regimen places increasing stress on the patient while at the same time decreasing clinical control
So how does it really work?So how does it really work?
CKC Power CKC Power TestingTesting
Within Within 10%10%--YESYES
Within Within 30%30%--YESYES
Focused Focused RehabRehab--CKC CKC ExercisesExercises
Focused Focused RehabRehab--BalanceBalance
NOT NOT Within Within 10%10%
NOT NOT Within Within 30%30%
Basic Basic MeasureMeasure--mentsments
SensoriSensori--motor motor testingtesting
Within Within 10%10%--YESYES
NOT NOT Within Within 10%10%
FocusedFocusedRehab Rehab
Specificity Specificity Testing Testing
Within Within NormsNorms--
Within Within 10%10%--YESYES
DC to DC to SportsSports
NOT NOT Within Within
NOT NOT Within Within NormsNorms
FocusedFocusedRehabRehab--FunctionalFunctional
Focused Focused Specificity Specificity RehabRehab
OKC OKC TestingTesting
Functional Functional Testing Testing
Within 25%Within 25%--YESYES
YESYES
NOT NOT Within Within 25%25%
NormsNorms
Focused Focused RehabRehab--OKC OKC Exercises Exercises
Functional Functional Jump/Jump/HopHopExercisesExercises
Functional Testing Algorithm Functional Testing Algorithm ––KneeKnee
We can rehabilitate patients faster than ever because by testing themtesting them, we always know
h th ti t i i thwhere the patient is in the rehab program and can focus focus the interventions the interventions specifically on the patient’s particular condition and status
5/25/2016
6
Physical Examination/Physical Examination/Tests & MeasurementsTests & MeasurementsObservation/posture
Gait EvaluationQ & Q Movement Assessment Referral/related
Physiological PROMAccessory/Jt. Play PROMKT 1000Flexibility TestsReferral/related
jointsNeurological ExamSensation, reflexesKinesthetic/proprioceptiveBalance Neural TT
PalpationAROM
RROM (MMT/HHD)Special TestsComputerized isokinetic testing Functional TestingFunctional TestingImaging StudiesLab Studies
ObservationObservation
& Posture& Posture
KT 1000 TestsKT 1000 TestsKT 1000 TestsKT 1000 Tests
Gait EvaluationGait EvaluationGait EvaluationGait Evaluation Q & Q Q & Q Movement Movement
A tA tAssessmentAssessmentQualitative Movement Qualitative Movement Analysis of the Entire Analysis of the Entire Kinematic Chain in all Kinematic Chain in all Planes of Motion Planes of Motion
Regional InterdependencyRegional Interdependency
TOTAL BODY INTERDEPENDENCYTOTAL BODY INTERDEPENDENCYIf movement is one integrated If movement is one integrated
pattern, regardless of its pattern, regardless of its complexity, complexity,
then we mustthen we mustevaluate and treat evaluate and treat The The TOTAL PATIENTTOTAL PATIENT
Basic MeasurementsBasic MeasurementsBasic MeasurementsBasic MeasurementsQualitative & Quantitative Qualitative & Quantitative Movement Assessment:Movement Assessment:Step Down Tests:Step Down Tests:
Performance TestsPerformance TestsSingle Leg Step Single Leg Step DownDown AnalysisAnalysis

5/25/2016
7
Axial Spinal “Clearing” Tests
• Lumbar Spine
• AROM
• PROM End ROM• PROM – End ROM
• MMT – Mid ROM
• Special Tests
• SI Joint
Appendicular Peripheral Joint “Clearing” Tests
Hip
Proximal Tib-Fib Joint
Ankle
Foot
Neurological ExamNeurological Exam--Sensorimotor Sensorimotor System TestingSystem Testing
••BalanceBalance
••Sensation Sensation –– dermatomes etc.dermatomes etc.
••ReflexesReflexes••ReflexesReflexes
••NeurodynamicNeurodynamic testingtesting
••MMTMMT
••Kinesthesia/ProprioceptionKinesthesia/Proprioception
Knee Kinesthetic TestingKnee Kinesthetic Testing
•Balance
•Angular Joint Replication•Angular Joint Replication
•End ROM Reproduction
•Threshold to Sensation of
Movement
BiodexBiodexBalance Balance
StabilometerStabilometerIt has been my It has been my clinical clinical
observation observation (performance (performance motion assessment) motion assessment) that that
after a LE injury, after a LE injury, individuals individuals do not bear weight equally do not bear weight equally during doubleduring double--leg exercises, leg exercises,
especially on the especially on the
injured leginjured leg
ClinicalClinicalBiomechanicsBiomechanics17:55117:551--554,554,
20022002
5/25/2016
8
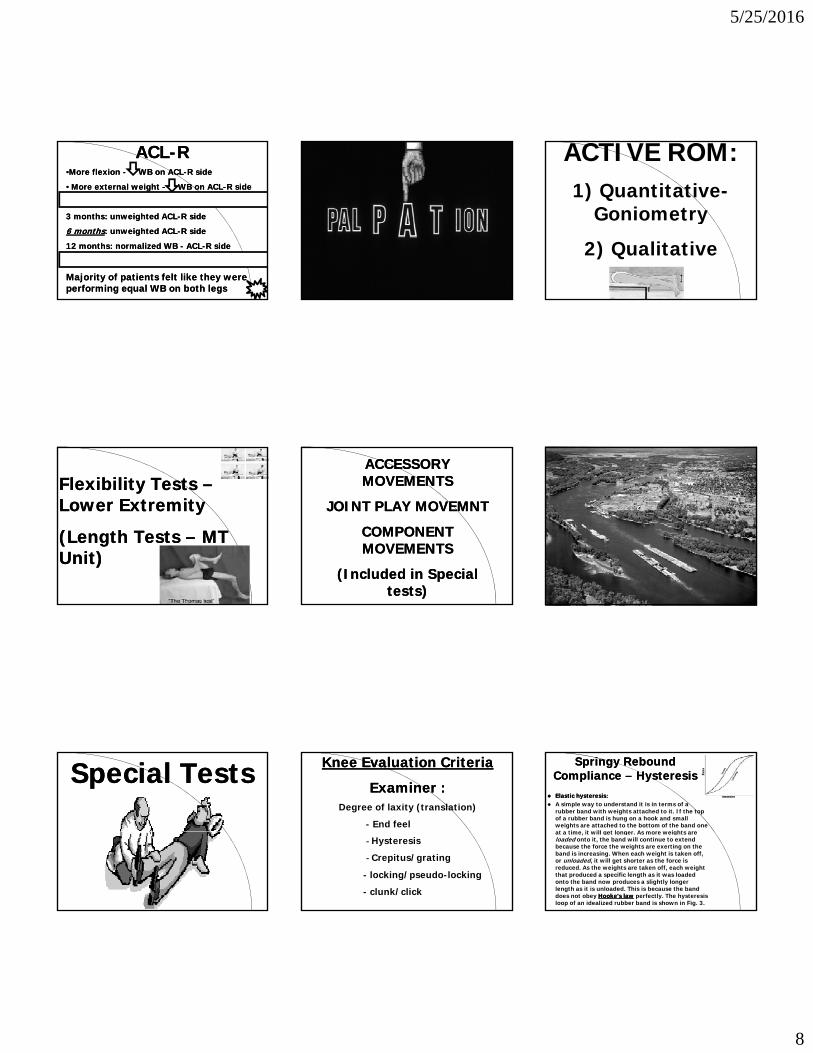
ACLACL--RR••More flexion More flexion -- WB on ACLWB on ACL--R sideR side
•• More external weight More external weight -- WB on ACLWB on ACL--R sideR side
3 months: 3 months: unweightedunweighted ACLACL--R sideR sidegg
6 months6 months: : unweightedunweighted ACLACL--R sideR side
12 months: 12 months: normalized WB normalized WB -- ACLACL--R sideR side
Majority of patients felt like they were Majority of patients felt like they were performing equal WB on both legs performing equal WB on both legs
ACTIVE ROM:1) Quantitative-
GoniometryGo o et y
2) Qualitative
Flexibility Tests Flexibility Tests ––Lower Extremity Lower Extremity
(Length Tests (Length Tests –– MT MT Unit)Unit)
ACCESSORY ACCESSORY MOVEMENTSMOVEMENTS
JOINT PLAY MOVEMNTJOINT PLAY MOVEMNT
CO OCO OCOMPONENT COMPONENT MOVEMENTSMOVEMENTS
(Included in Special (Included in Special tests)tests)
Special TestsSpecial Tests Knee Evaluation CriteriaKnee Evaluation Criteria
Examiner Examiner ::Degree of laxity (translation)
- End feel
- Hysteresis
- Crepitus/grating
- locking/pseudo-locking
- clunk/click
Springy Rebound Springy Rebound Compliance Compliance –– HysteresisHysteresisElastic hysteresis:Elastic hysteresis:A simple way to understand it is in terms of a rubber band with weights attached to it. If the top of a rubber band is hung on a hook and small weights are attached to the bottom of the band one at a time it will get longer As more weights areat a time, it will get longer. As more weights are loaded onto it, the band will continue to extend because the force the weights are exerting on the band is increasing. When each weight is taken off, or unloaded, it will get shorter as the force is reduced. As the weights are taken off, each weight that produced a specific length as it was loaded onto the band now produces a slightly longer length as it is unloaded. This is because the band does not obey Hooke's lawHooke's law perfectly. The hysteresis loop of an idealized rubber band is shown in Fig. 3.

5/25/2016
9
Knee Evaluation Knee Evaluation CriteriaCriteria
Patient –Patient c/o pain( e od tio of the(reproduction of the symptoms)
Patient c/o apprehension(feeling that the PFJ is ready to subluxate/dislocate)
Special TestsSpecial Tests
Orthopedic Physical Orthopedic Physical AssessmentAssessmentMagee, DJMagee, DJ> 175 special tests for the > 175 special tests for the Knee ?????????????Knee ?????????????We’ll discuss and demonstrate We’ll discuss and demonstrate an algorithman algorithm--based exam for based exam for the special tests which is the special tests which is clinically efficientclinically efficient
CorroborationCorroboration of of multiple testsmultiple tests
to identify to identify consistency in the consistency in the yyclusters of signs & clusters of signs &
symptoms =symptoms =clinical diagnosisclinical diagnosis
CategoryCluster of S & S YES
+ - NO
Category
Algorithm Based ExamAlgorithm Based Exam
CategoryClusters of S & S
CategoryCluster of S & S
NO
YES
YES
+ -
Physical Examination of the Physical Examination of the KneeKnee--Effusion Tests Effusion Tests -- 66
Physical Examination of the Physical Examination of the KneeKnee--Effusion Tests Effusion Tests
Ballottement Test/Ballotable Patella or Patella Tap Test (SEN:83)(SP:49)(+LR:1.6)
Sweep Test (Wipe Brush Bulge StrokeSweep Test (Wipe, Brush, Bulge, Stroke Test)
Fluctuation TestIndentation TestPeripatellar Swelling TestPalpable fluid wave
Physical Examination of the Physical Examination of the KneeKnee--Milking Test/Fluid WaveMilking Test/Fluid Wave
Physical Examination of the Physical Examination of the KneeKnee--PF PF BallotmentBallotment TestTest
(SEN:83)(SEN:83)(SP:49)(SP:49)(+LR:1.6)(+LR:1.6)
Physical Examination of the Physical Examination of the KneeKnee--PF Tests PF Tests -- 3232
5/25/2016
10
Physical Examination of the KneePhysical Examination of the Knee--PatelloPatello--Femoral TestsFemoral Tests
Patellar Apprehension test (Fairbank’s Apprehension Test) (SEN:7-37)(70-92)(+LR:0.87-2.3)
Patellar Grinding Compression Test (Clarke’s sign) (SEN:29-49)(SP:67-95)(+LR:0.88-7.4)
Active Patellar Grind TestPF Medial Tilt (SEN:43)(SP:92)(+LR:5.4)PF Lateral Tilt PF Superior Tilt (SEN:19)(SP:83)(+LR:1.1)PF P t i TiltPF Posterior TiltMedial PF Glides (SEN:54)(SP:69)(+LR:1.8)Lateral PF Glides (SEN:54)(SP:69)(+LR:1.8)Caudal PF Glides (SEN:63)(SP:56)(+LR:1.4)Cephalic PF GlidesPatellar Mobility TestingPF RotationsPF Passive Tracking TestPF Active Tracking TestLateral Pull Test (SEN:25)(SP:100)Waldron Test (SEN:18-45)(SP:68-83)(+LR:1.05-1.41)Patella Alta Test (SEN:49)(SP:72)(+LR:1.75)VMO Coordination Test (PF Tracking Test) (SEN:17)(SP:93)(+LR:2.26)
Physical Examination of the Physical Examination of the KneeKnee--PatelloPatello--Femoral TestsFemoral Tests
VMO Coordination Test (PF Tracking Test) (SEN:17)(SP:93)(+LR:2.26)
Eccentric Step Test (SEN:42)(SP:82)(+LR:2.34)McConnell Test for patellar OrientationMcConnell Test for Chondromalacia patella Z hl ’ SiZohler’s SignTubercle Sulcus TestQ-angle (SEN:76)(SP:63)(+LR:2.05)Palpation Tests: (SEN:27-83)(SP:68-76)(+LR:1.11-1.5)Resisted Knee Extension (SEN:21-39)(SP:82-95)(+LR:2.2-4.2)Pain with Functional Testing (SEN:75-94)(SP:43-50)(+LR:1.3-1.8)Step Up TestFrund’s SignDynamic Apprehension Test (SEN: 100)(SP: 88)
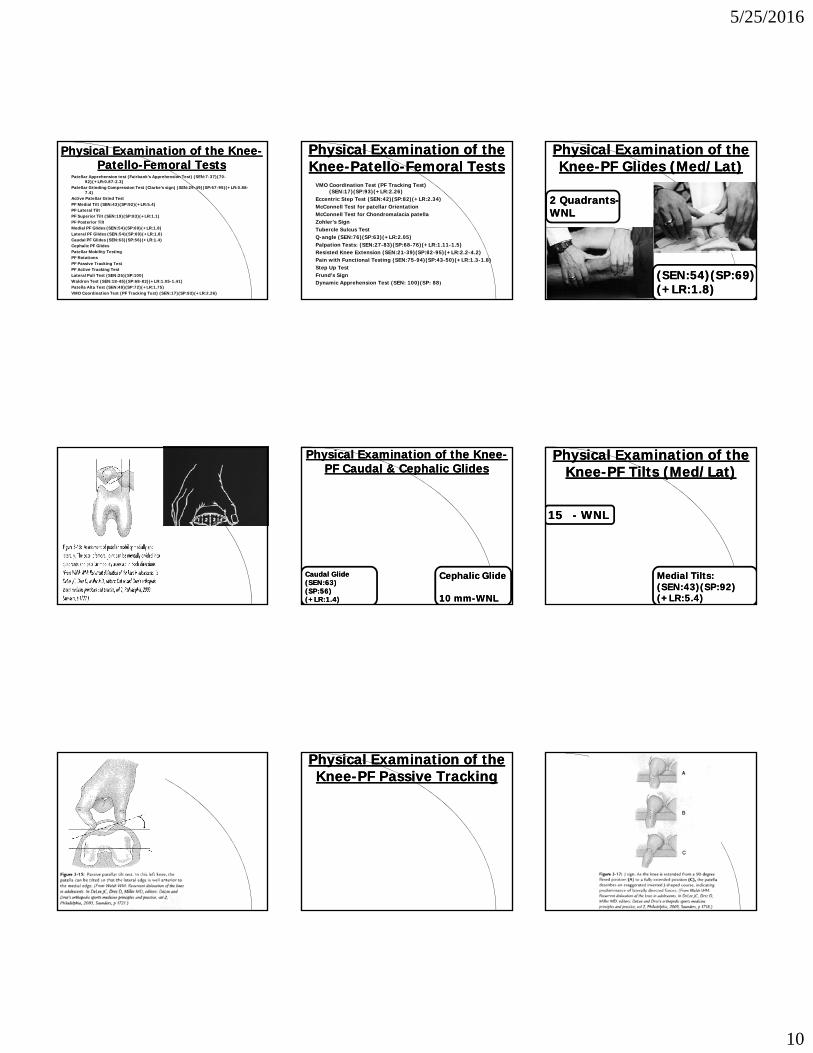
Physical Examination of the Physical Examination of the KneeKnee--PF Glides (Med/Lat)PF Glides (Med/Lat)
2 Quadrants2 Quadrants--WNLWNL
(SEN:54)(SP:69)(SEN:54)(SP:69)(+LR:1.8)(+LR:1.8)
Physical Examination of the KneePhysical Examination of the Knee--PF Caudal & Cephalic Glides PF Caudal & Cephalic Glides
Caudal GlideCaudal Glide(SEN:63)(SEN:63)(SP:56)(SP:56)(+LR:1.4)(+LR:1.4)
Cephalic GlideCephalic Glide
10 mm10 mm--WNLWNL
Physical Examination of the Physical Examination of the KneeKnee--PF Tilts (Med/Lat)PF Tilts (Med/Lat)
1515 -- WNLWNL
Medial Tilts:Medial Tilts:(SEN:43)(SP:92)(SEN:43)(SP:92)(+LR:5.4)(+LR:5.4)
Physical Examination of the Physical Examination of the KneeKnee--PF Passive Tracking PF Passive Tracking

5/25/2016
11
Physical Examination of the Physical Examination of the KneeKnee--PF Active Tracking PF Active Tracking
(SEN:25)(SEN:25)(SP:100)(SP:100)
Physical Examination of the Physical Examination of the KneeKnee--PF CKCPF CKC--AROM Tracking AROM Tracking
Physical Examination of Physical Examination of the Kneethe Knee--PCL Tests PCL Tests -- 1919
Physical Examination of the KneePhysical Examination of the Knee--Posterior Instability TestsPosterior Instability Tests
Posterior Drawer Test (SEN:22-100)(SP:99)(+LR:90)External Rotation - Recurvatum test (SEN:3-39)(SP:99)(+LR:3.0)Valgus test at 0° knee extension (SEN:59-94)(SP:100)Varus test at 0° knee extensionPosterior Sag Sign (Gravity Drawer Test) (SEN:46-100)(SP:100)Godfrey’s 90/90 TestClancy’s Step-off Test/Thumb SignQ d i A ti D T t (S 54 98%) (S 97 100%)(+LR 18)Quadriceps Active Drawer Test (Sen-54-98%) (Spec-97-100%)(+LR:18)Reverse Pivot Shift (Jakob Test)(PLRI) (SEN:26-58)(SP:94-95)(+LR:5.2-9.67)Posterior (Reverse) Lachman’s Test/Trillat’s Test (SEN:62)(SP:89)(+LR:5.64)Dial Test (Tibial External Rotation Test) Anterior Abrasion Sign (SEN:7-14)(SP:NA)Fixed Posterior SubluxationProximal Tibial Percussion TestPosterior Functional Drawer TestLoomer’s Test (PLRI)Dial Test (PLRI/PCL)Standing Apprehension TestPosterior Medial Displacement Test (PMRI)
Physical Examination Physical Examination of the Kneeof the Knee
PCL TESTSPCL TESTS
Posterior Drawer TestPosterior Drawer Test
NoulisNoulis’ Thesis, 1875’ Thesis, 1875
Physical Examination of the Physical Examination of the KneeKnee--RecurvatumRecurvatum TestTest
(SEN:3(SEN:3--39)39)(SP:99)(SP:99)(+LR:3.0)(+LR:3.0)
Physical Examination of the Physical Examination of the KneeKnee--SAG/Godfrey’s TestSAG/Godfrey’s Test
(SEN:46(SEN:46--100)100)(SP:100)(SP:100)
Physical Examination Physical Examination of the Kneeof the Knee
PCL TESTSPCL TESTSIt is important to establish the It is important to establish the
ta ti efe e e o itio o e dota ti efe e e o itio o e dostarting reference position so we do starting reference position so we do not not mismis--interpret the interpret the tibialtibialtranslation translation
(10mm = Normal)(10mm = Normal)(Step(Step--up is lost = + PCL injury)up is lost = + PCL injury)
Physical Examination of the Physical Examination of the KneeKnee--Clancy’s Step Clancy’s Step -- Up TestUp Test
10 mm10 mmStepStep--Up Up --WNLWNL
5/25/2016
12
Physical Examination Physical Examination of the Kneeof the Knee
PCL TESTSPCL TESTS
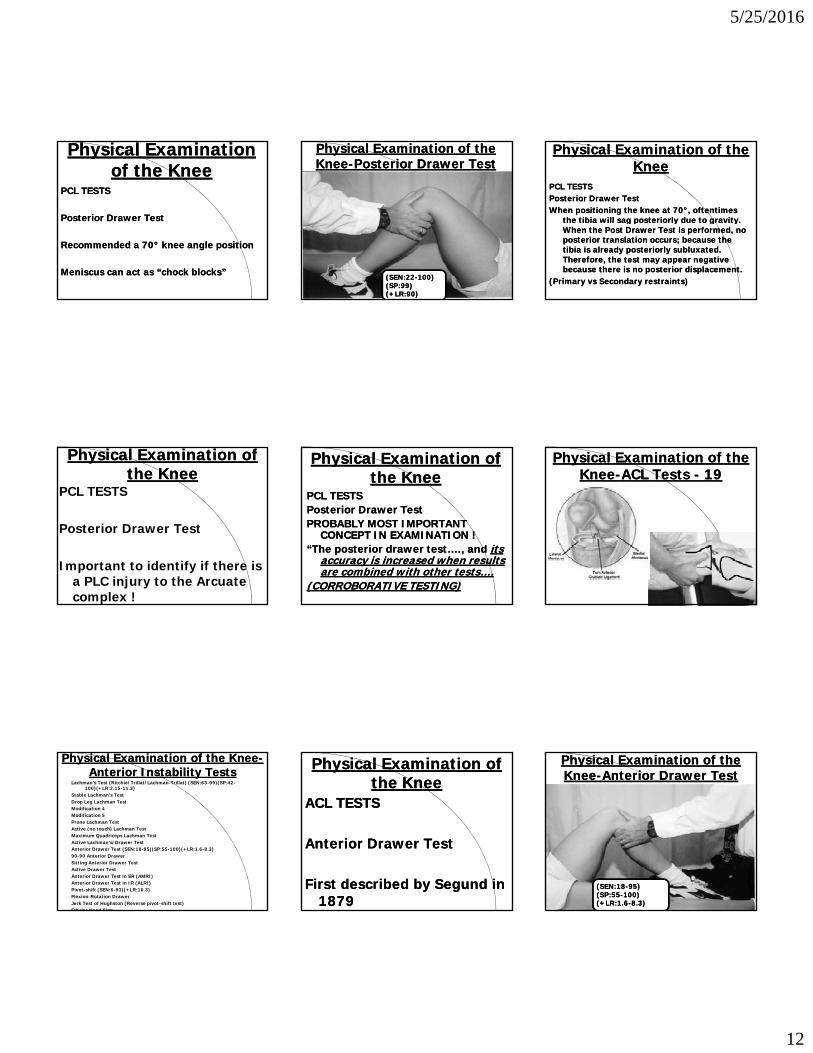
Posterior Drawer TestPosterior Drawer TestPosterior Drawer TestPosterior Drawer Test
Recommended a 70Recommended a 70°° knee angle positionknee angle position
Meniscus can act as Meniscus can act as “chock blocks”“chock blocks”
Physical Examination of the Physical Examination of the KneeKnee--Posterior Drawer TestPosterior Drawer Test
(SEN:22(SEN:22--100)100)(SP:99)(SP:99)(+LR:90)(+LR:90)
Physical Examination of the Physical Examination of the KneeKnee
PCL TESTSPCL TESTSPosterior Drawer TestPosterior Drawer TestWhen positioning the knee at 70When positioning the knee at 70°°, oftentimes , oftentimes
the tibia will sag posteriorly due to gravitythe tibia will sag posteriorly due to gravitythe tibia will sag posteriorly due to gravity. the tibia will sag posteriorly due to gravity. When the Post Drawer Test is performed, no When the Post Drawer Test is performed, no posterior translation occurs; because the posterior translation occurs; because the tibia is already posteriorly tibia is already posteriorly subluxatedsubluxated. . Therefore, the test may appear negative Therefore, the test may appear negative because there is no posterior displacement. because there is no posterior displacement.
(Primary vs Secondary restraints)(Primary vs Secondary restraints)
Physical Examination of Physical Examination of the Kneethe Knee
PCL TESTS
Posterior Drawer TestPosterior Drawer Test
Important to identify if there is a PLC injury to the Arcuate complex !
Physical Examination of Physical Examination of the Kneethe Knee
PCL TESTSPCL TESTSPosterior Drawer TestPosterior Drawer TestPROBABLY MOST IMPORTANTPROBABLY MOST IMPORTANTPROBABLY MOST IMPORTANT PROBABLY MOST IMPORTANT
CONCEPT IN EXAMINATION !CONCEPT IN EXAMINATION !“The posterior drawer test…., and “The posterior drawer test…., and its its
accuracy is increased when results accuracy is increased when results are combined with other tests….are combined with other tests….
(CORROBORATIVE TESTING)(CORROBORATIVE TESTING)
Physical Examination of the Physical Examination of the KneeKnee--ACL Tests ACL Tests -- 1919
Physical Examination of the KneePhysical Examination of the Knee--Anterior Instability TestsAnterior Instability Tests
Lachman’s Test (Ritchie/Trillat/Lachman-Trillat) (SEN:63-99)(SP:42-100)(+LR:2.15-11.3)
Stable Lachman’s TestDrop Leg Lachman TestModification 4Modification 5Prone Lachman TestActive (no touch) Lachman TestMaximum Quadriceps Lachman TestActive Lachman’s/Drawer Test Anterior Drawer Test (SEN:18-95)(SP:55-100)(+LR:1.6-8.3)90-90 Anterior DrawerSitting Anterior Drawer TestActive Drawer TestAnterior Drawer Test in ER (AMRI)Anterior Drawer Test in IR (ALRI) Pivot-shift (SEN:6-93)(+LR:10.3)Flexion-Rotation DrawerJerk Test of Hughston (Reverse pivot-shift test)Fibular Head Sign
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTS
Anterior Drawer TestAnterior Drawer Test
First described by First described by SegundSegund in in 18791879
Physical Examination of the Physical Examination of the KneeKnee--Anterior Drawer TestAnterior Drawer Test
(SEN:18(SEN:18--95)95)(SP:55(SP:55--100)100)(+LR:1.6(+LR:1.6--8.3)8.3)

5/25/2016
13
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSAnterior Drawer TestAnterior Drawer TestIt is important to establish theIt is important to establish theIt is important to establish the It is important to establish the
starting reference position so we starting reference position so we do not do not mismis--interpret the interpret the tibialtibialtranslation translation (false positives with (false positives with PCL insufficiencies) PCL insufficiencies)
(10 mm step(10 mm step--up)up)
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSACL TESTSKnee Knee -- 7070°°Anterior Drawer TestAnterior Drawer Test -- limitationslimitationsAnterior Drawer Test Anterior Drawer Test limitationslimitationsMeniscus can act as “chock blocks”Meniscus can act as “chock blocks”EffusionEffusionPainPainPatient comfortPatient comfortOnly checks the AMB of ACLOnly checks the AMB of ACL
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSACL TESTSAnterior Drawer TestAnterior Drawer Test
The data suggest that the anterior The data suggest that the anterior drawer test becomes drawer test becomes increasingly more sensitive as increasingly more sensitive as the the secondary restraintssecondary restraints of of anterior stability are lost anterior stability are lost
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSACL TESTSAnterior Drawer TestAnterior Drawer TestS iti itS iti it A t i j i 22%A t i j i 22% 70%70%Sensitivity:Sensitivity: Acute injuries: 22%Acute injuries: 22%--70%70%
Chronic injuries: 54%Chronic injuries: 54%--97%97%
Under anesthesia:Under anesthesia: 80%80%--91%91%Specificity:Specificity: Acute & Chronic injuries: Acute & Chronic injuries:
97%97%
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSLachman Test
Noulis’ Thesis, 1875 Century
Torg, et.al. AJSM, 1976 later !!!
Physical Examination of the Physical Examination of the KneeKnee--Lachman’s TestLachman’s Test
(SEN:63(SEN:63--99)99)(SP:42(SP:42--100)100)(+LR:2.15(+LR:2.15--11.3)11.3)
<3 mmWNL
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSLachman TestLachman TestSensitivity:Sensitivity: Acute injuries: 80%Acute injuries: 80%--99%99%Sensitivity:Sensitivity: Acute injuries: 80%Acute injuries: 80% 99%99%
Chronic injuries: 94%Chronic injuries: 94%--99%99%
Under anesthesia:Under anesthesia: 85%85%--99%99%Specificity:Specificity: Acute & Chronic injuries: Acute & Chronic injuries: Under anesthesia:Under anesthesia: 95%95%
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSLachman TestLachman TestClinical interpretation:Clinical interpretation:Visual anterior translation of tibia Visual anterior translation of tibia
to femurto femurProprioceptive anterior translationProprioceptive anterior translation“Soft” or “mushy” end point“Soft” or “mushy” end point
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSLachman TestLachman Test
Several “Hybrid variations”:Several “Hybrid variations”:8 modifications8 modifications of the Lachman’s of the Lachman’s
Test:Test:

5/25/2016
14
Physical Examination of Physical Examination of the Kneethe Knee--Pivot Shift Pivot Shift
(SEN:6(SEN:6--93)93)(+LR:10.3)(+LR:10.3)
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSACL TESTSPivot Shift TestPivot Shift TestThe pivot shift is both aThe pivot shift is both a clinicalclinicalThe pivot shift is both a The pivot shift is both a clinical clinical
phenomenonphenomenon that results in a that results in a complaint of a giving way of the complaint of a giving way of the knee and a knee and a physical signphysical sign that can that can be elicited on examination of the be elicited on examination of the injured knee.injured knee.
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSPivot Shift TestPivot Shift Test
At approximately 20At approximately 20--3030°° ROM, ROM, there is a pivoting of the tibia there is a pivoting of the tibia on the femur on the femur (ALRI).(ALRI).ITB “slips” over the lateral ITB “slips” over the lateral
femoral epicondyle.femoral epicondyle.
Physical Examination Physical Examination of the Kneeof the Knee
ACL TESTSACL TESTSPivot Shift TestPivot Shift Test
Sensitivity:Sensitivity: Acute & Chronic injuries: Acute & Chronic injuries: 35%35%--98%98%
Under anesthesia:Under anesthesia: 98%98%Specificity:Specificity: Acute & Chronic injuries: Acute & Chronic injuries:
98%98%
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSPivot Shift TestPivot Shift Test
Several modifications: hip Several modifications: hip positions, knee positions, positions, knee positions, tibialtibial rotationsrotations
Physical Examination of Physical Examination of the Kneethe Knee
ACL TESTSACL TESTSPivot Shift TestPivot Shift TestA positive pivot shift test in aA positive pivot shift test in aA positive pivot shift test in a A positive pivot shift test in a
conscious patient may reflect the conscious patient may reflect the patient’s inability to protect the patient’s inability to protect the knee, which may suggest that knee, which may suggest that these patients are less likely to these patients are less likely to respond to nonrespond to non--operative operative treatmenttreatment
Physical Examination of the Physical Examination of the KneeKnee--Jerk TestJerk Test
Physical Examination of the Physical Examination of the KneeKnee--FlexionFlexion--Rotation Drawer Rotation Drawer
Physical Examination of the KneePhysical Examination of the Knee--Rotary Instability Tests Rotary Instability Tests -- 3030

5/25/2016
15
Physical Examination of the KneePhysical Examination of the Knee--AnteromedialAnteromedial Rotary Instability TestsRotary Instability Tests
Slocum Test with External Tibial Rotation (AMRI)
Lemaire’s anteromedialLemaire s anteromedial Jolt Test (T Drawer, Y Test)
Dejour Test
Physical Examination of the KneePhysical Examination of the Knee--AnterolateralAnterolateral Rotary Instability TestsRotary Instability Tests
Slocum Test with Internal Tibial Rotation (ALRI)
Lateral Pivot Shift Test of MacintoshActive Pivot Shift TestLosee TestJerk Test of HughstonCrossover Test of ArnoldLemaire’s Jolt TestNakajima TestNoyes flexion-rotation drawer testFlexion-extension valgus testMartens Test
Physical Examination of the KneePhysical Examination of the Knee--PosteromedialPosteromedial Rotary Instability TestsRotary Instability Tests
Hughston Postermedial Drawer Test
Posteromedial pivot shift test
Physical Examination of the KneePhysical Examination of the Knee--PosterolateralPosterolateral Rotary Instability TestsRotary Instability Tests
Pivot Shift TestJakob Test (Reverse pivot shift
maneuver)External Rotation Recurvatum TestJerk TestLoomer’s PLRI TestLoomer s PLRI TestBousquet external hypermobility testTibial External Rotation TestsHughston Posterolateral Drawer TestDial Test (Tibial External Rotation Test)Dynamic posterior shift testActive posterolateral drawer signArcuate Spin TestStanding Apprehension TestFrog Leg Maneuver Frog Leg Maneuver
Physical Examination of the KneePhysical Examination of the Knee--MCL Valgus Stress Tests MCL Valgus Stress Tests -- 77
Physical Examination of the Physical Examination of the Medial Stability TestsMedial Stability Tests
Valgus stress test at 0°Valgus stress test at 30° (SEN:78-
100)(SP:49-100)(+LR:.1.8-2.3)H h t ’ V l t t 0°Hughston’s Valgus stress at 0°Hughston’s Valgus stress at 30°Swain TestApley’s Distraction Test with ERApley’s Distraction Test with ER with DDV
(Davies Dynamic Version)
Physical Examination of Physical Examination of the Kneethe Knee
VALGUS STRESS TESTSVALGUS STRESS TESTS
Palmer, Palmer, ActaActa ChirChirScand Suppl, 1938
Physical Examination of the KneePhysical Examination of the Knee--MCL Valgus Stress TestMCL Valgus Stress Test--00
Physical Examination of Physical Examination of the Kneethe Knee
VALGUS STRESS TESTSVALGUS STRESS TESTS
00°° Extension: MCL, capsule, Extension: MCL, capsule, ACL,PCL, PMOL, etc. ACL,PCL, PMOL, etc. (MCL(MCL--57%)57%)
3030°° Flexion: MCL Flexion: MCL (MCL(MCL--78%)78%)

5/25/2016
16
Physical Examination of the KneePhysical Examination of the Knee--MCL Valgus Stress TestMCL Valgus Stress Test--3030
(SEN:78(SEN:78--100)100)(SP:49(SP:49--100)100)(+LR:1.8(+LR:1.8--2.3)2.3)
Physical Examination of the Physical Examination of the KneeKnee--ApleysApleys Distraction TestDistraction Test
Physical Examination of the Physical Examination of the KneeKnee--Apley’sApley’s DistractionDistraction--DDVDDV
AMA Nomenclature AMA Nomenclature --Knee Instability TestingKnee Instability Testing
Classification of knee instability testing:Grade I: mild sprainGrade I: mild sprainGrade II: moderate sprain
1+ - 1-5 mm more laxity2+ - 6-10 mm more laxity
Grade III: severe sprain3+- > 10 mm more laxity
Clinical Pearl Clinical Pearl MCL Valgus Stress TestingMCL Valgus Stress Testing
Clinical Pearl Clinical Pearl MCL Valgus Stress TestingMCL Valgus Stress TestingWhen performing a valgus stress When performing a valgus stress test, test, Start by Start by “closing the joint”“closing the joint” first first ––yy g jg j
To perform the valgus stress test, To perform the valgus stress test, actually begin by moving toward actually begin by moving toward varusvarus first to approximate the tibia first to approximate the tibia to the femurto the femur
MCL Valgus Stress TestMCL Valgus Stress Test
Closing the jointClosing the joint is is analogous to identifying analogous to identifying g y gg y gthe starting reference the starting reference position just like when position just like when performing a PCL/ACL performing a PCL/ACL test test
Clinical Pearl Clinical Pearl ––MCL Valgus Stress TestingMCL Valgus Stress Testing
Clinical Pearl Clinical Pearl ––MCL Valgus Stress TestingMCL Valgus Stress TestingWhen performing a valgus stress When performing a valgus stress test, test, Start by Start by “closing the joint”“closing the joint” first first ––
Reason is to approximate the joint Reason is to approximate the joint surfaces so one can surfaces so one can palpatepalpate the the joint line opening and joint line opening and kinesthetically feelkinesthetically feel the amount of the amount of motion motion
Clinical PearlClinical PearlClinical PearlClinical PearlMCL Valgus Stress InjuryMCL Valgus Stress Injury
Think about a Think about a PF PF subluxationsubluxation also as a also as a potential additional injury potential additional injury and a coand a co--morbidity morbidity
5/25/2016
17
Physical Examination of the KneePhysical Examination of the Knee--LCL LCL VarusVarus Stress Tests Stress Tests -- 66
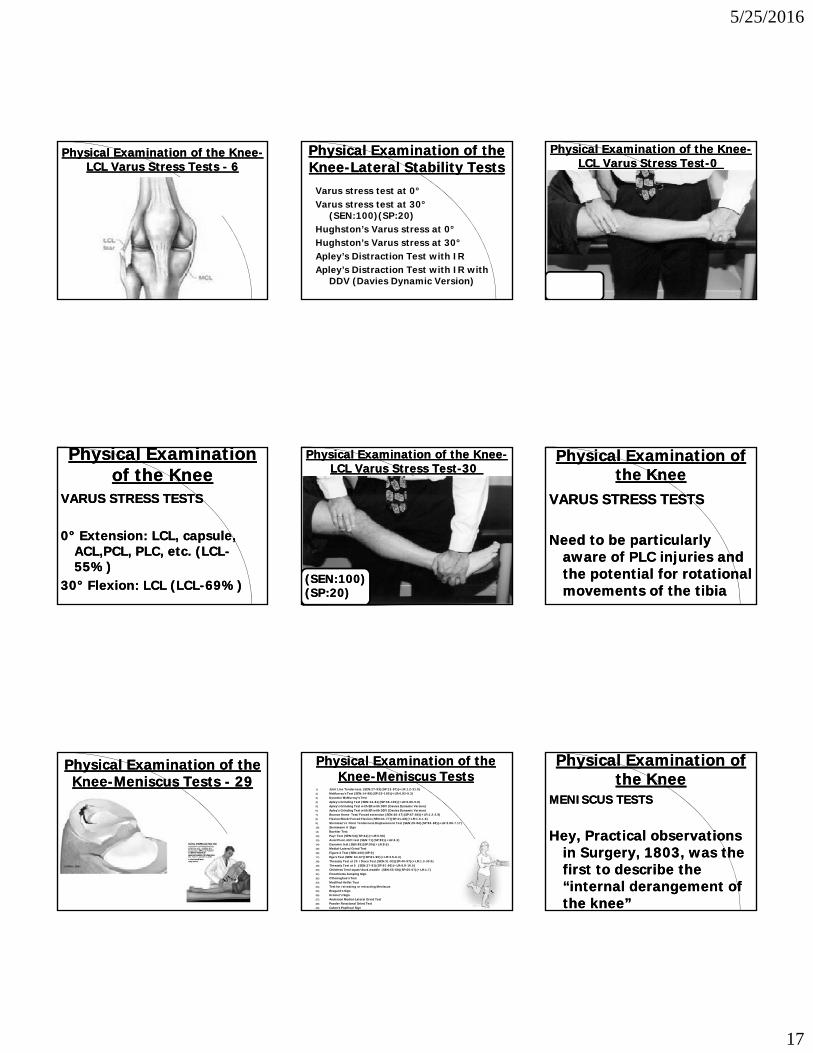
Physical Examination of the Physical Examination of the KneeKnee--Lateral Stability TestsLateral Stability Tests
Varus stress test at 0°Varus stress test at 30°
(SEN:100)(SP:20)( )( )Hughston’s Varus stress at 0°Hughston’s Varus stress at 30°Apley’s Distraction Test with IRApley’s Distraction Test with IR with
DDV (Davies Dynamic Version)
Physical Examination of the KneePhysical Examination of the Knee--LCL LCL VarusVarus Stress TestStress Test--00
Physical Examination Physical Examination of the Kneeof the Knee
VARUS STRESS TESTSVARUS STRESS TESTS
00°° Extension: LCL, capsule, Extension: LCL, capsule, ACL,PCL, PLC, etc. ACL,PCL, PLC, etc. (LCL(LCL--55%)55%)
3030°° Flexion: LCL Flexion: LCL (LCL(LCL--69%)69%)
Physical Examination of the KneePhysical Examination of the Knee--LCL LCL VarusVarus Stress TestStress Test--3030
(SEN:100)(SEN:100)(SP:20)(SP:20)
Physical Examination of Physical Examination of the Kneethe Knee
VARUS STRESS TESTSVARUS STRESS TESTS
Need to be particularly Need to be particularly aware of aware of PLC injuriesPLC injuries and and the potential for rotational the potential for rotational movements of the tibiamovements of the tibia
Physical Examination of the Physical Examination of the KneeKnee--Meniscus Tests Meniscus Tests -- 2929
Physical Examination of the Physical Examination of the KneeKnee--Meniscus TestsMeniscus Tests
1) Joint Line Tenderness (SEN:27-93)(SP:13-97)(+LR:1.2-31.0)2) McMurray’s Test (SEN:14-88)(SP:20-100)(+LR:0.82-9.3)3) Dynamic McMurray’s Test4) Apley’s Grinding Test (SEN:13-81)(SP:56-100)(+LR:0.80-5.9)5) Apley’s Grinding Test with ER with DDV (Davies Dynamic Version)6) Apley’s Grinding Test with ER with DDV (Davies Dynamic Version) 7) Bounce Home Test/Forced extension (SEN:36-47)(SP:67-86)(+LR:1.2-2.9)8) Flexion Block/Forced Flexion (SEN:44-77)(SP:41-68)(+LR:1.0-1.6)9) Steinman’s I Point Tenderness Displacement Test (SEN:29-86)(SP:83-88)(+LR:3.88-7.17)10) Steinmann II Sign11) Boehler Test11) Boehler Test 12) Payr Test (SEN:54)(SP:44)(+LR:0.96)13) Axial Pivot-shift test (SEN:71)(SP:83)(+LR:4.2)14) Dynamic test (SEN:85)(SP:90)(+LR:8.5)15) Medial-Lateral Grind Test16) Figure 4 Test (SEN:100)(SP:0)17) Ege’s Test (SEN: 64-67)(SP:81-90)(+LR:3.5-6.4)18) Thessaly Test at 20 /Disco Test (SEN:31-92)(SP:40-97)(+LR:1.3-30.0)19) Thessaly Test at 5 (SEN:27-81)(SP:91-96)(+LR:6.8-16.5)20) Childress Test/squat/duck waddle (SEN:55-68)(SP:60-67)(+LR:1.7)21) Finochietto Jumping Sign22) O’Donoghue’s Test23) Modified Helfet Test 24) Test for retreating or retracting Meniscus25) Bragard’s Sign26) Kromer’s Sign27) Anderson Medial-Lateral Grind Test28) Passler Rotational Grind Test29) Cabot’s Popliteal Sign
Physical Examination of Physical Examination of the Kneethe Knee
MENISCUS TESTSMENISCUS TESTS
H P ti l b tiH P ti l b tiHey, Practical observations Hey, Practical observations in Surgery, 1803, was the in Surgery, 1803, was the first to describe the first to describe the “internal derangement of “internal derangement of the knee”the knee”

5/25/2016
18
Physical Examination of the Physical Examination of the KneeKnee--RecurvatumRecurvatum TestTest
(SEN:36(SEN:36--47)47)(SP:67(SP:67--86)86)(+LR:1.2(+LR:1.2--2.9)2.9)
Physical Examination of the KneePhysical Examination of the Knee--Steinman’s Point Pressure TestSteinman’s Point Pressure Test
(SEN:29(SEN:29--86)86)(SP:83(SP:83--88)88)(+LR:3.88(+LR:3.88--7.17)7.17)
Physical Examination of the Physical Examination of the KneeKnee--Mc Murray’s TestMc Murray’s Test
(SEN:14(SEN:14--88)88)(SP:20(SP:20--100)100)(+LR:0.82(+LR:0.82--9.3)9.3)
Physical Examination of the Physical Examination of the KneeKnee--McMurray’s Dynamic TestMcMurray’s Dynamic Test
Physical Examination of the Physical Examination of the KneeKnee--Apley’sApley’s Compression TestCompression Test
(SEN:13(SEN:13--81)81)(SP:56(SP:56--100)100)(+LR:0.80(+LR:0.80--5.9)5.9)
Physical Examination of Physical Examination of the Kneethe Knee
MENISCUS TESTSApley Grind Test
“Surgeon leans well over the patient and with his whole body weight, compresses the tibia downward onto the couch. Again he rotates powerfully….”
OUCH !!!!
Physical Examination of the KneePhysical Examination of the Knee--Apley’sApley’s CompressionCompression--DDVDDV
Physical Examination of the Physical Examination of the KneeKnee
Predictive Value of Clinical Signs in Evaluation of Predictive Value of Clinical Signs in Evaluation of Meniscal Pathology; Fowler, et.al. Meniscal Pathology; Fowler, et.al. ArthroscopyArthroscopy, , 5:184,19895:184,1989No one testNo one test is predictive for diagnosis of is predictive for diagnosis of meniscal tearmeniscal tearmeniscal tearmeniscal tearPresence of ACL pathology will render test less Presence of ACL pathology will render test less effectiveeffectiveJoint line tenderness, pain with forced Joint line tenderness, pain with forced hyperflexion (Steinman’s Test), and positive hyperflexion (Steinman’s Test), and positive Mc Murray’s together provide best predictor Mc Murray’s together provide best predictor of meniscal tearof meniscal tear
Physical Examination Physical Examination of the Kneeof the Knee
Very few tests by themselves are Very few tests by themselves are absolutely accurate, therefore absolutely accurate, therefore thethe “clusters of signs and“clusters of signs andthe the clusters of signs and clusters of signs and symptoms”symptoms” and using the and using the constellation of exam findings constellation of exam findings and the and the corroboration of testscorroboration of testsare the key to a good are the key to a good examination and diagnosisexamination and diagnosis

5/25/2016
19
Physical Examination of the Physical Examination of the KneeKnee--PlicaPlica Syndrome Tests Syndrome Tests -- 99
Medial Patellar Plica Test (SEN:90)(SP:89)(+LR:8.18)
Medial Plica Shelf Test Medial Plica TestRotation Valgus TestHolding TestPlica/Patellar Stutter TestHughston’s Plica TestPatellar Bowstring TestMediopatellar Plica Test (Mital-Hayden Test)
Physical Examination of the Physical Examination of the KneeKnee--Miscellaneous TestsMiscellaneous TestsTests for Tests for OsteochondralOsteochondral LesionsLesionsWilson’s test
Proximal Proximal TibiofibularTibiofibular Joint InstabilityJoint InstabilityFibular Head Translation Test
Patella tendon/ligament length testPatella tendon/ligament length test
ITB Syndrome ITB Syndrome Noble’s Compression Test Renne’s Test
Hoffa’s Syndrome TestHoffa’s Syndrome Test
Physical Examination of the Physical Examination of the KneeKnee--Miscellaneous TestsMiscellaneous Tests
Flexibility TestsFlexibility Tests--Cross knee Cross knee Thomas TestOber’s TestModified Ober’s TestEly’s testKnee Angle MeasurementsKnee Angle MeasurementsggQ-Angle/Patellofemoral Angle TestTubercle Sulcus Angle (Q-Angle at 90 )A-AngleDaniel’s Quadriceps Neutral Angle TestBayonet Sign
Functional test for Quadriceps Contusion Functional test for Quadriceps Contusion
Test for knee Extension Contracture (Heel Height Difference)Test for knee Extension Contracture (Heel Height Difference)
Corroboration of Corroboration of tests tests to implicate to implicate or rule out or rule out various injuries various injuries or injured or injured structuresstructures
Functional Testing Algorithm –Knee -2016
Sport Specific TestingLower Extremity Functional Tests Functional Hop TestsFunctional Jump Tests
Competitive Competitive AthletesAthletes
RecreationalRecreationalFunctional Jump TestsOKC Isokinetic testing CKC Isokinetic TestingSensorimotor System Testing: Balance/Proprioceptive TestingKT 1000/2000 Basic MeasurementsBasic Measurements
RecreationalRecreationalAthletesAthletes
GeneralGeneralOrthopaedicOrthopaedic
PatientsPatients
SummarySummary
AndAnd
ConclusionsConclusionsConclusionsConclusions
Functional Testing Algorithm –Knee -2016
Sport Specific TestingLower Extremity Functional Tests Functional Hop TestsFunctional Jump Tests
Competitive Competitive AthletesAthletes
RecreationalRecreationalFunctional Jump TestsOKC Isokinetic testing CKC Isokinetic TestingSensorimotor System Testing: Balance/Proprioceptive TestingKT 1000/2000 Basic MeasurementsBasic Measurements
RecreationalRecreationalAthletesAthletes
GeneralGeneralOrthopaedicOrthopaedic
PatientsPatients
Thanks to Thanks to RUSH Sports RUSH Sports
MedicineMedicineSymposiumSymposium
Th k YTh k YThank YouThank You













![HYDRAULIC MOTORS EPM - EIBL- DHT · 2018-10-24 · Max. Oil Flow, cont. 405060 60 60 60 60 60 60 [lpm] int.* 455570 75 75 75 75 75 75 Max. Inlet cont. 175 175 175 175 175 175 175](https://static.fdocuments.us/doc/165x107/5e92874e36e2be41131fa132/hydraulic-motors-epm-eibl-dht-2018-10-24-max-oil-flow-cont-405060-60-60.jpg)



