NEEP 541 – Swelling Fall 2002 Jake Blanchard. Outline Swelling.
Upload
doctorniravCategory
view
76download
8description
EXAMINATION OFSWELLING
DR.K.SUGUNAKAR
HISTORY
how long is the lump present?
when was the lump first noticed?
There is a heaven and hell difference
between these two questions.
Pain less lump may present for along time
with out patients knowledge.
SHORTDURATION&PAIN: INFLAMMATORY
SINCE BIRRTH:CONGENITAL
LONGER DURATIONWITH OUT PAIN :BENIGN
LONGER DURATION WITH PAIN AND SHORT DURATION-------------MAYBE MALIGNANT
MODEOF ONSET
HAVE APPEARED AFTER TRAUMA ;fractured displacement of bone,dislocation of joint,haematoma
DEVELOPED SPONTANEOUSLY AND GROWN RAPIDLY WITH PAIN: inflammatory
GRADULLY INCREASING INSIZE: neoplasm
SWELLING APPEARED IN PRE EXISTING CONDITION: keloid from previous scar, malignant melanoma from previous benign nevus
OTHER SYMPTOMS
PAIN----inflammatory or involving nerves
DIFFICULTY IN RESPIRATION---pressure on trachea
DIFFICULTY IN SWALLOWING--- pressure on esophagus
INTERFFERING WITH MOVEMENT—swellings near joint
DISFIGURATION
pain
Nature of pain: throbbing pain suggests inflammation
leading to suppuration.pain may be burning,stabbing,aching.
Site:most offen pain is localised to the site of swelling. referred
pain may be present
Time of onset: in inflammatory swellings.pain appears even
before the swelling.but in case of tumors swelling appears long
before pain.in malignant conditions pain is due to involvement of
nerves,fungation,ulceration,deepinfiltration,which indicates
inoperability
PROGRESS OF THE SWELLING
GROWING SLOWLY-------benign swellings
GROWING QUICKLY--------malignant swellings
SUDDENLY INCREASING IN SIZE AFTER REMAINING
STATIONERY FOR SOME TIME----malignant transformation of
benign swellings
DECREASING IN SIZE------inflammatory swellings
EXACT SITE: site of the swelling tells from
which organ the swelling was originated.
PSENCEOF OTHER LUMPS:
neurofibromatosis,diaphysial
aclasia,hodgkins lymphoma may present
with multiple swellings.
PSENCE OF OTHER LUMPS:
neurofibromatosis,diaphysial
aclasia,hodgkins lymphoma may present
with multiple swellings.
EXACT SITE: site of the swelling tells from
which organ the swelling was originated.

SUB MANDIBULAR REGION
SUB MANDIBULAR GLAND
LYMPH NODE
PLUNGING RANULA

Swelling present since
birth
Neck swelling in posterior and anterior
triangle of neck
Cystic swelling
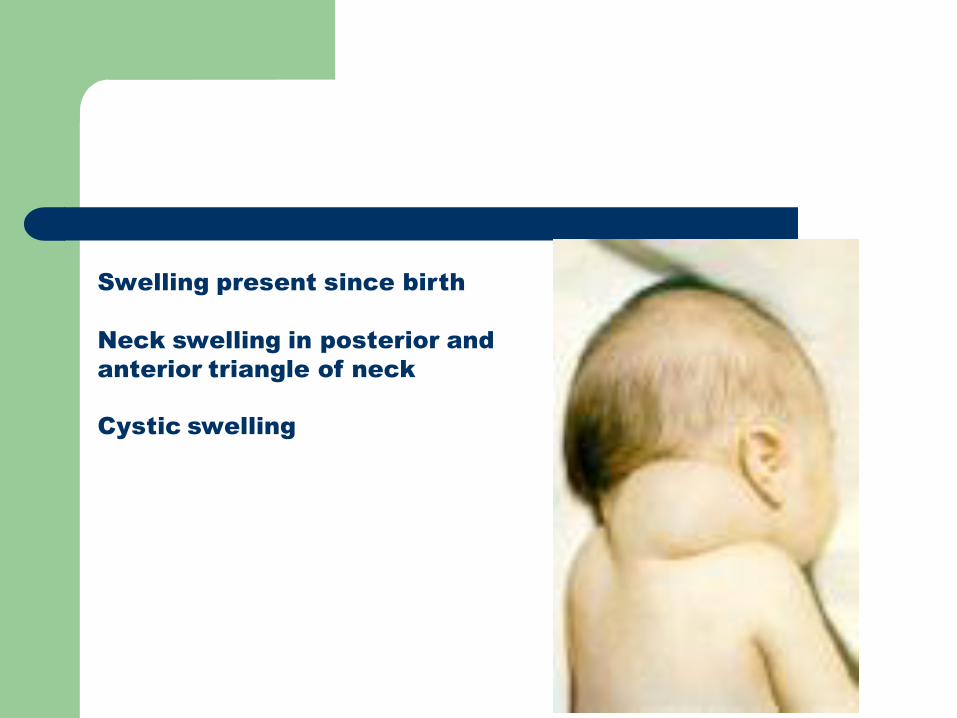
Swelling present since birth
Neck swelling in posterior and
anterior triangle of neck
Cystic swelling
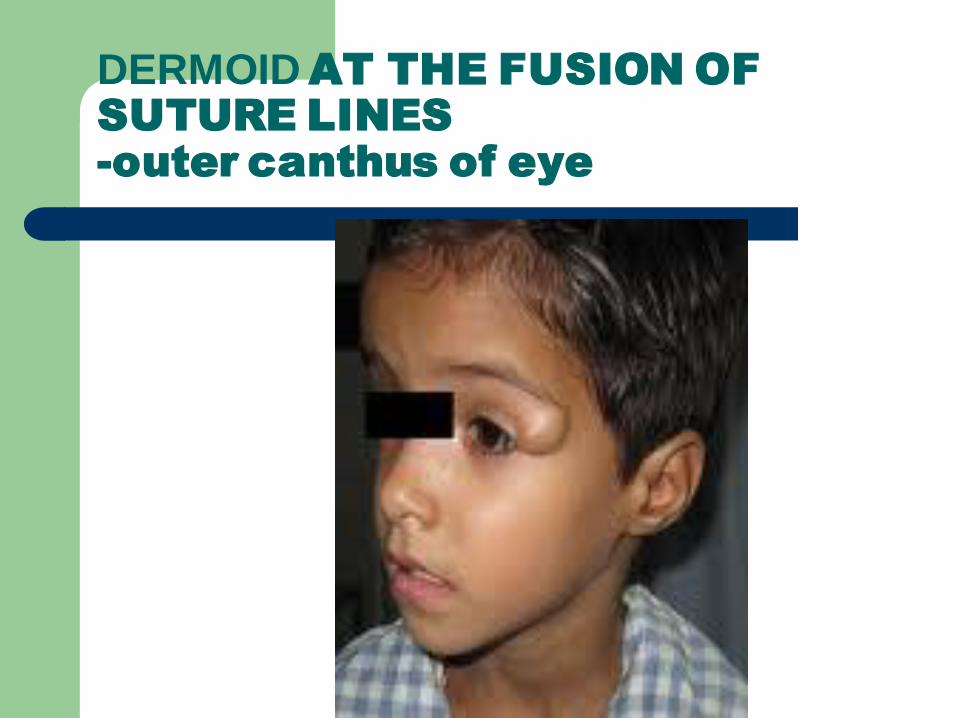
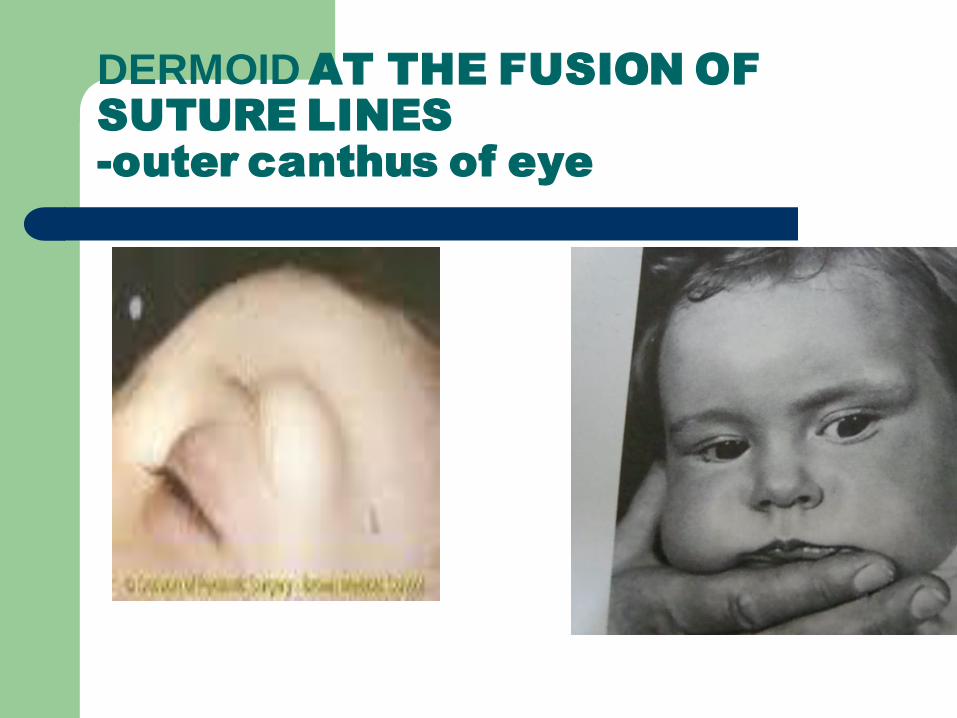
DERMOID AT THE FUSION OF
SUTURE LINES
-outer canthus of eye
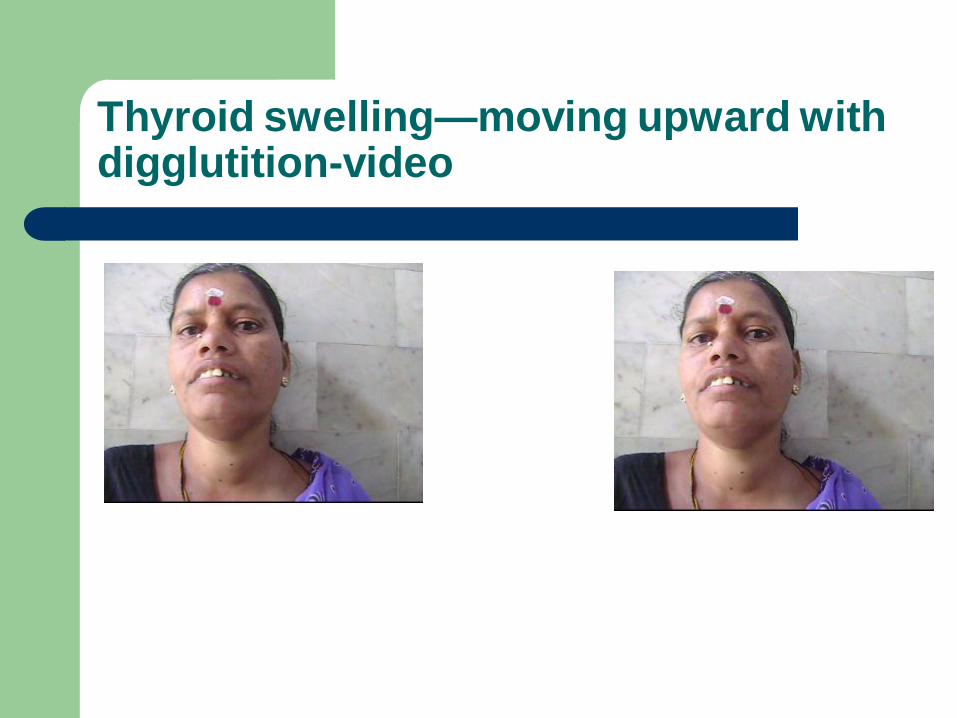
Thyroid swelling—moving upward with digglutition-video
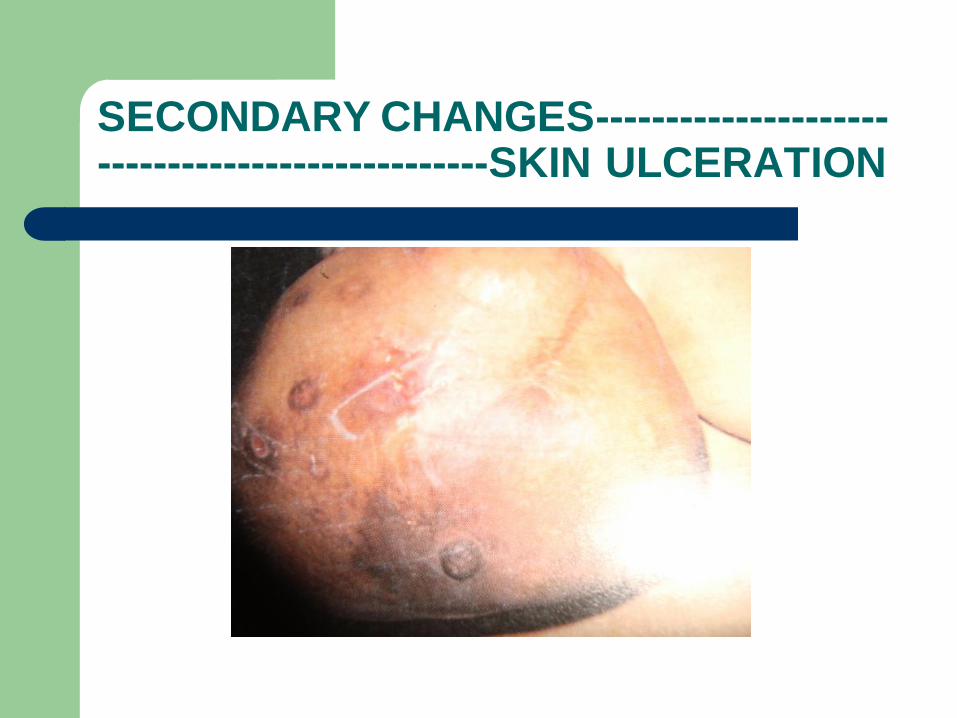
SECONDARY CHANGES LIKE
SOFTENING,ULCERATION,FUNGATION,IN
FLAMMATORY CHANGES----malignant
swellings &T.B.lymphadenitis
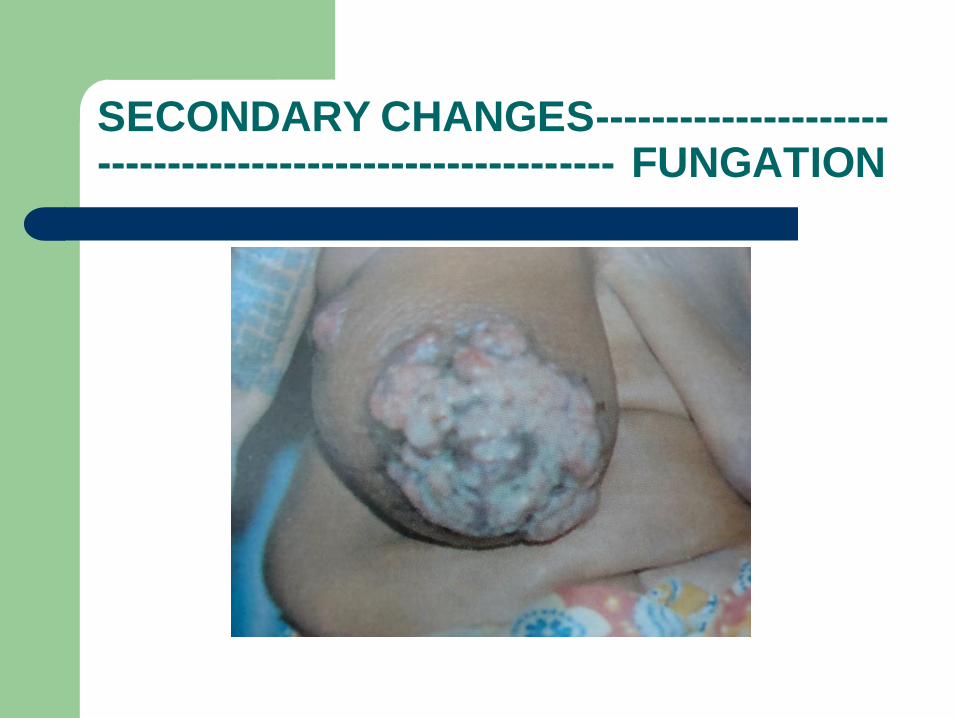
SECONDARY CHANGES---------------------------------------------------------- FUNGATION

SECONDARY CHANGES-------------------------------------------------SKIN ULCERATION
SECONDARY CHANGES-------------------------------------------------SKIN ULCERATION
RECURRENT SWELLINGS---malignant
swellings, malignant growth in benign
swellings.certain swellings like pagets
recurrent fibroid,known for recurrence.cystic
swellings may recur if they are not removed
completely.
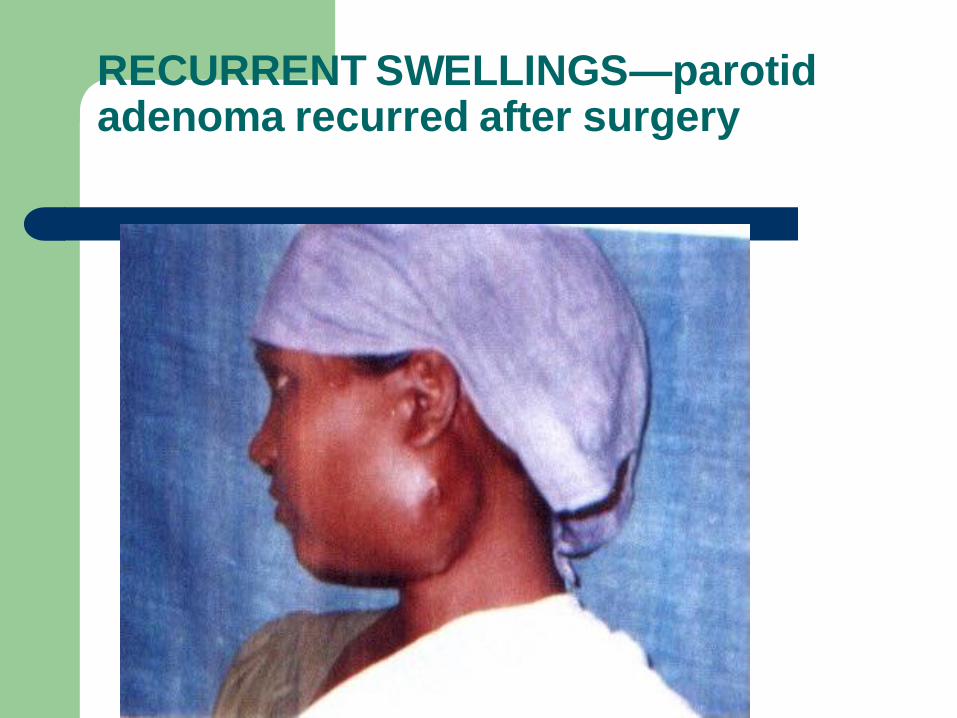
RECURRENT SWELLINGS—parotid adenoma recurred after surgery
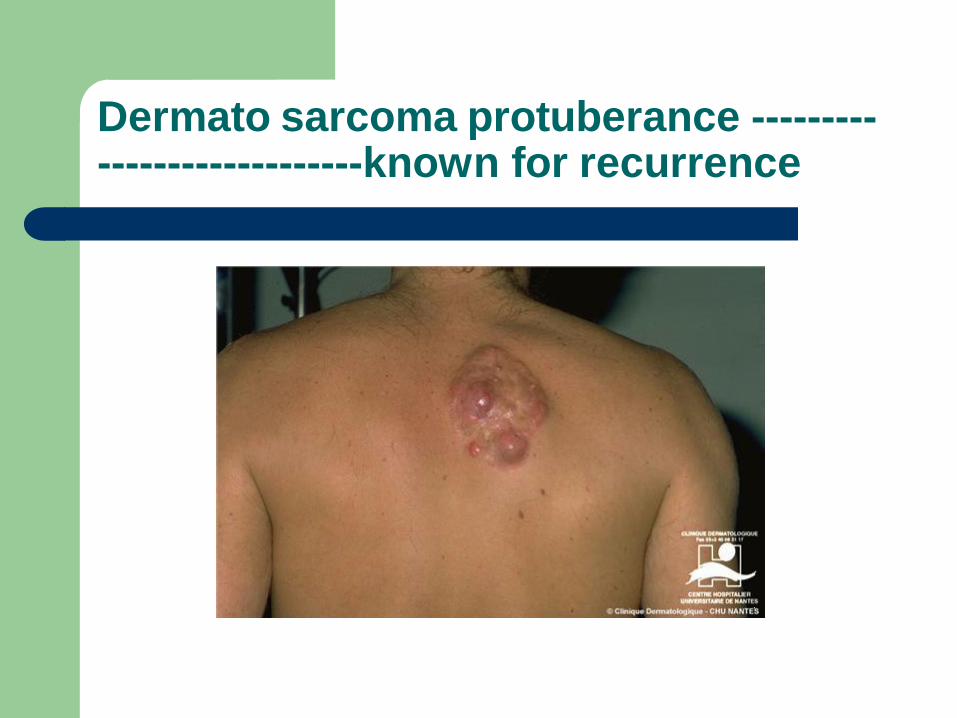
Dermato sarcoma protuberance ----------------------------known for recurrence
LOSS OF BODYWEIGHT--
malignant&tuberculosis
LOSS OF APPETITE--
malignant&tuberculosis -
HISTORY OF FEVER—acute& chronic,
inflammatory swellings, malignant swellings,
lymphomas
PAST HISTORY; important in tuberculosis
FAMILY HISTORY: important in carcinoma breast,medullary carcinoma thyroid,
PERSONAL HISTORY: smoking and alcoholism are risk factures for several malignancies
LOCAL EXAMINATION
SITE OF THE SWELLING: a few swellings are peculiar in their positions such as dermoid cyst are mostly seen in the mid line of the body or on the line of the fusion of embryonic processes.eg.at the outer canthus of eye---that means on the line of fusion between the fronto-nasal process and the maxillary process.or behind the ear (post auricular dermoid)---on the line of fusion of the mesodermal hillocks which form the pinna.
SHAPE OF THE SWENG;ovoid,sperical,irregular
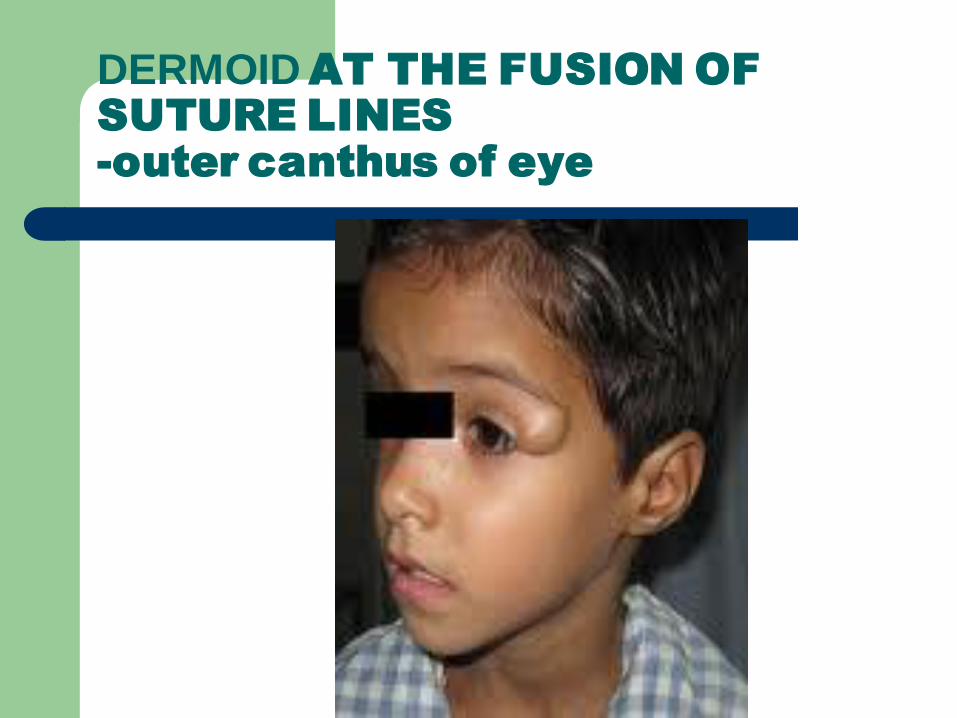
DERMOID AT THE FUSION OF
SUTURE LINES
-outer canthus of eye
DERMOID AT THE FUSION OF
SUTURE LINES
-outer canthus of eye
COLOUR OF THE SWELLING:colour of the
swelling give a definitive hint to the
diagnosis. black color of benign nevus and
malignant melanoma, red/purple color of
haemangioma.
bluish color of ranula are obvious and diagnostic

SURFACE: in certain swellings suface may
be very much obvious and diagnostic.
cauliflower surface of squamous cell
carcinoma, irregular numerous branched
surface of papilloma.
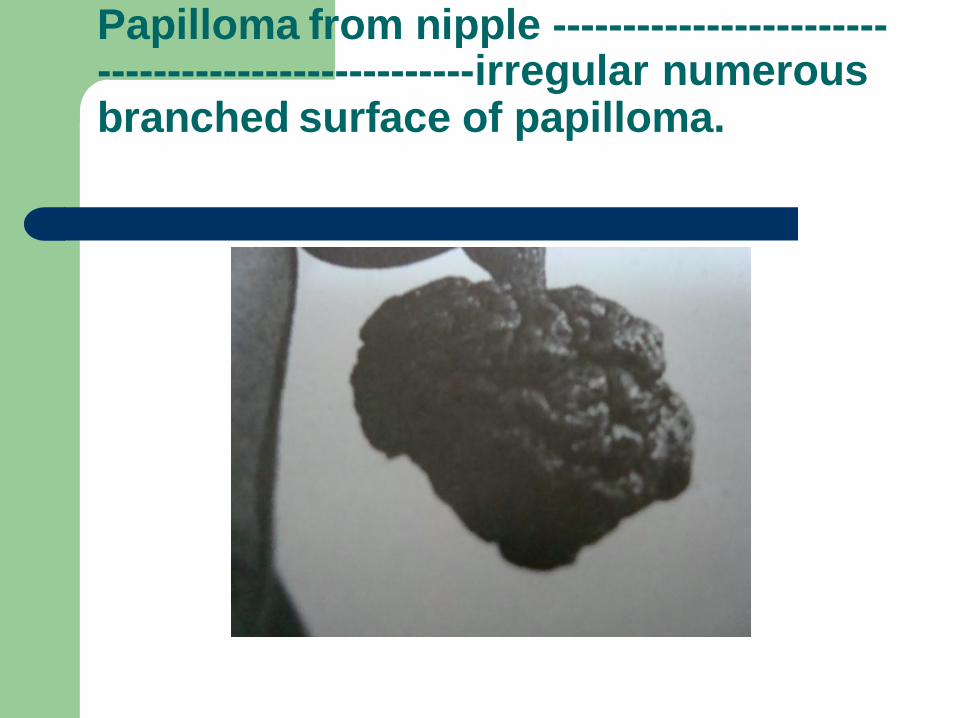
Papilloma from nipple ---------------------------------------------------irregular numerous branched surface of papilloma.
NUMBER: this is important as this may give
a clue to the diagnosis. some swellings are
always multiple such as
neurofibromatosis,diaphysial
aclasia,hodgkins lymphoma
some swellings are more known to be
solitary ,eg.lipoma,dermoid cysts

MULTIPLE SWELLINGS-------------------------------------------NEUROFIBROMATOSIS

MULTIPLE SWELLINGS-
Sebaceous cysts
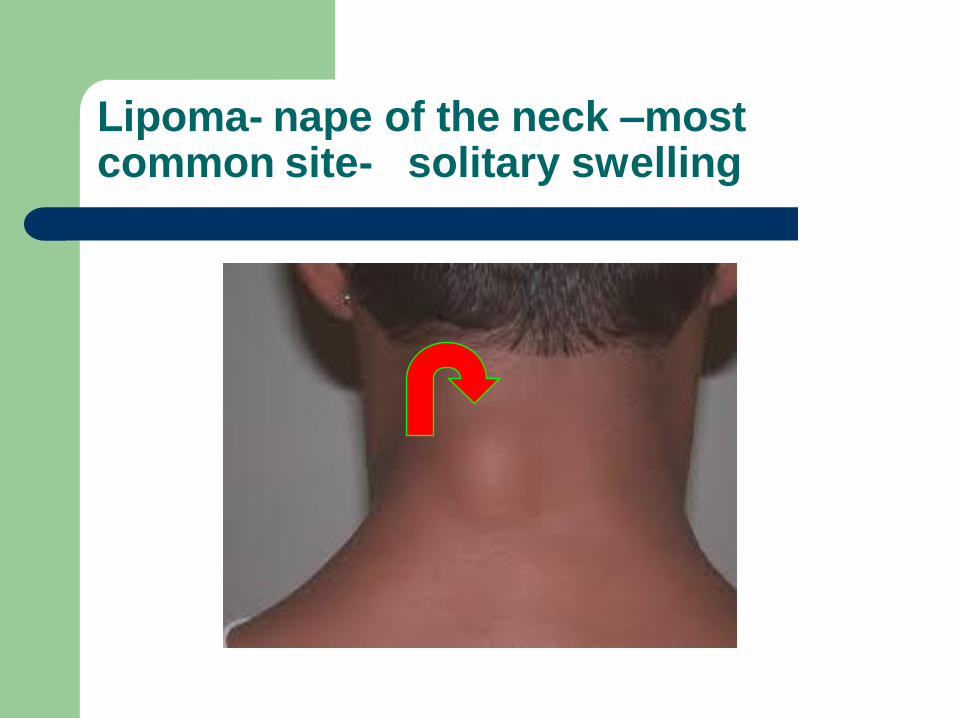
Lipoma- nape of the neck –most common site- solitary swelling

DERMOID---solitary swelling
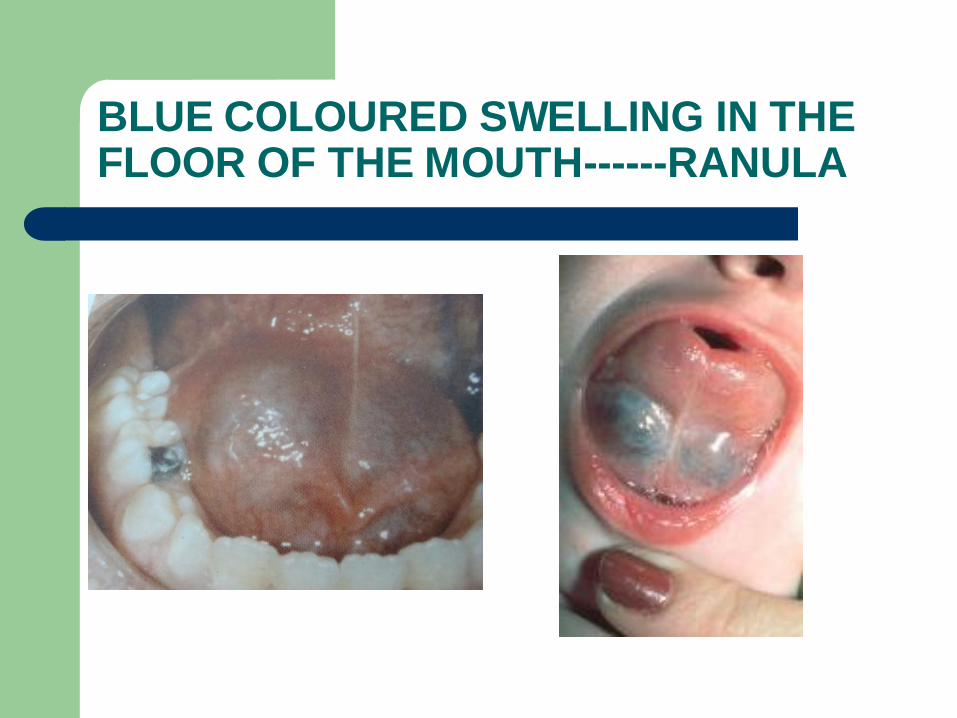
BLUE COLOURED SWELLING IN THE FLOOR OF THE MOUTH------RANULA

Redness,oedema,&pain---inflammatory swellings
PULSATION: swellings arising from the arteries are pulsatile,eg.aneurysm and vasculargrowth such as carotid body tumor. These give expansile pulsations.some swellings present over the arteries will be pulsatile.these will give transmitted pulsations
SKIN OVER THE SWELLING: red edematous in inflammatory swellings.tense,glossy with venous prominence in sarcoma with rapid growth. presence of black punctum in sebaceous cyst.presence of scar indicates previous operation(when the scar is linear with suture marks) previous injury(regular scar),previous suppuration(puckered,broad,irregular scar)

Redness,oedema,&pain---inflammatory swellings

Skin------tense,glossy with venous prominence in sarcoma with rapid growth
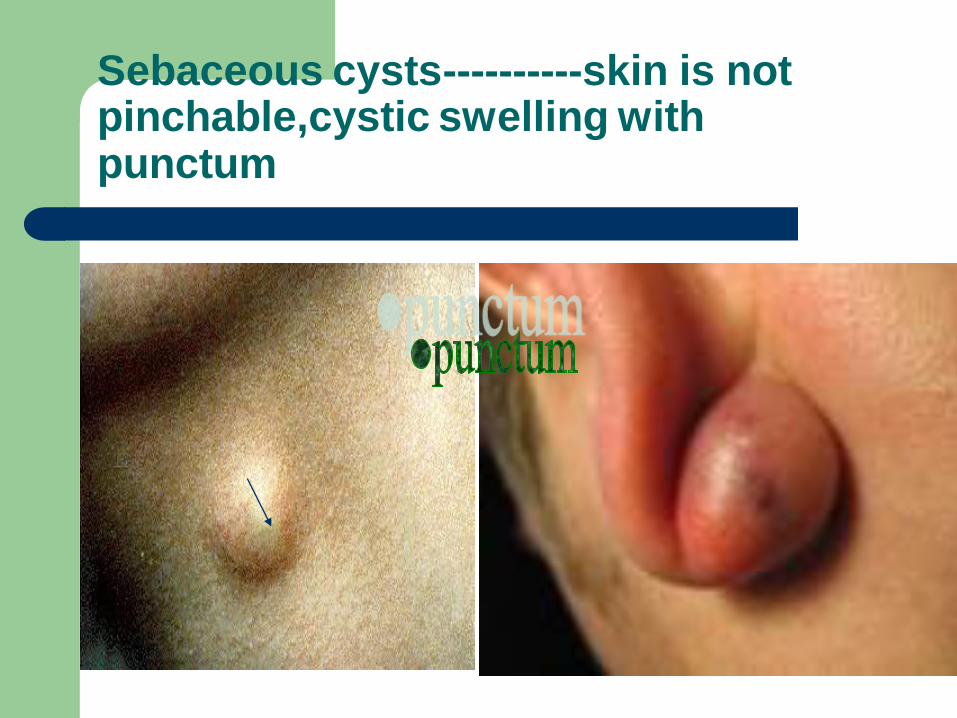
Sebaceous cysts----------skin is not pinchable,cystic swelling with punctum

Scar---previous surgery
PALPATION
LOCAL RISE OF
TEMPERATURE:
DUE TO INCREASED
VASCULARITY
MAYBE
INFLAMMATORYOR
VASCLAR TUMOR LIKE
SARCOMA
TENDERNESS
GENTLE PRESSURE
OVER SWELLING
SHOULD SEE THE FACIAL
EXPRESSION
INFLAMMATORYSWELLIN
GS ARE TENDER
NEOPLSTIC SWELLINGS
ARE NON TENDER
SIZE ,SHAPE ,EXTENT CAN BE CLEALRY KNOWN WITH
PALPATION
IT IS BETTER TO MENTION IN VERTCAL AND HORIZONTAL
DIAMETRES
SURFACE
SMOOTH
NODULAR
LOBULAR
IRREGULAR
CYSTIC
LYMPHNODAL MASS
LIPOMA
MALIGNANT

SMOOTH SURFACE
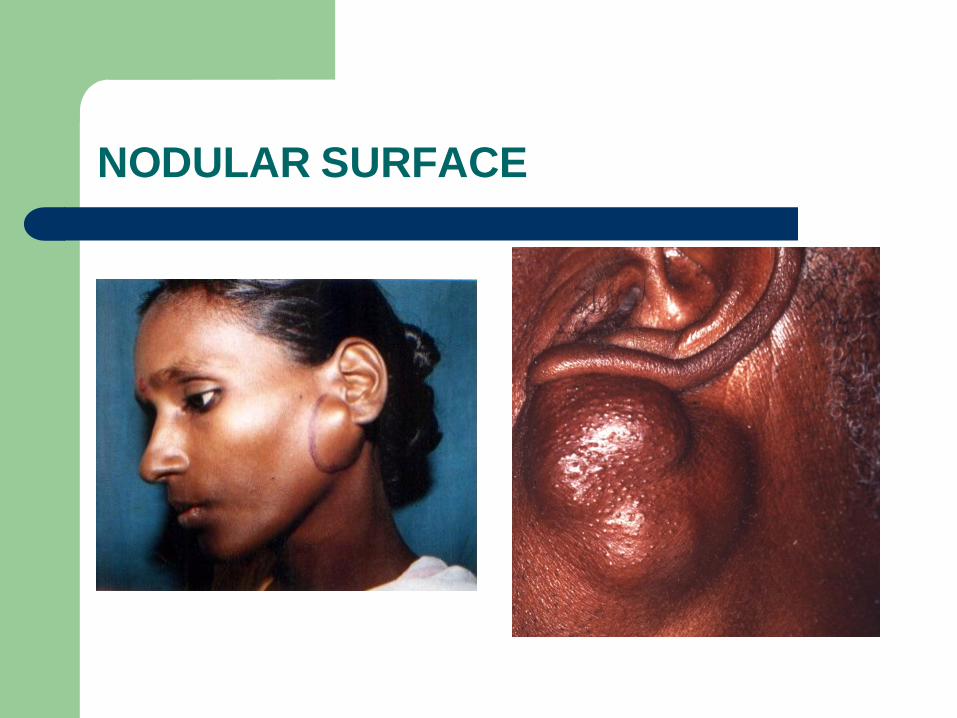
NODULAR SURFACE
EDGE
WELLDEFFINED
SMOOTH
IRREGULAR
ILLDEFINED
NEOPLSTIC,CHR.INFL
BENIGN
MALIGNANT
ACUTE
INFFLAMMATORY
SLIP SIGN
BOTH LIPOMA AND CYST
HAVE SMOOTH
MARGINNS
LIPOMA SLIPS AWAY ON
PALPATION
CYST YIELDS ON
PALPATION
CONSISTANCY
IT DEPENDS ON WHAT IT IS MADE UP OF
CYSTIC
FIRM
HARD
UNIFORM IN COSISTACY OR VARIABLE IN CONSISTACY
FLUCTUATION
SWELLING FLUCTUATES WHEN IT HAS FLUID
FIRST TO FIX THE SWELLING
THIS TEST SHOULD BE PERFORMED IN TWO PLANES
PAGETS TEST
TRANSLUSENCY
THIS MEANS SWELLING TRASMITS LIGHT WHEN IT HAS CLEAR FLUID LIKE WATER,LYMPH,SERUM,PLASMA
NOT TRANSULANT WHEN IT CONTAINS OPAQUE FLUID LIKE BLOOD,PUS,PULTAEOUS MATERIOL
Translucency brilliantly Positiveinhydrocele,ranula
,cystic hygroma
IMPULSE ON COUGHING
SWELINGS WHICH HAVE CONTINUITY WITH ABDOMINAL CAVITY-HERNIA
SWELLINGS WHICH HAVE CONTINUITY WITH SPINAL CORD-MENINGOCELE
WHICH HAVE CONTINUITY WITH PLEURAL CAVITY-EMPYEMA NECESSITANCE
SWELLING IS PALPATED IN FINGURES AND ASKED TO COUGH AN IMPULSE WILL BE FELT DUE TO INCREASE PRESSURE IN THESE CAVITIES
INCASE OF CHILDREN THIS IS PERFORMED WHEN THEY CRY
I
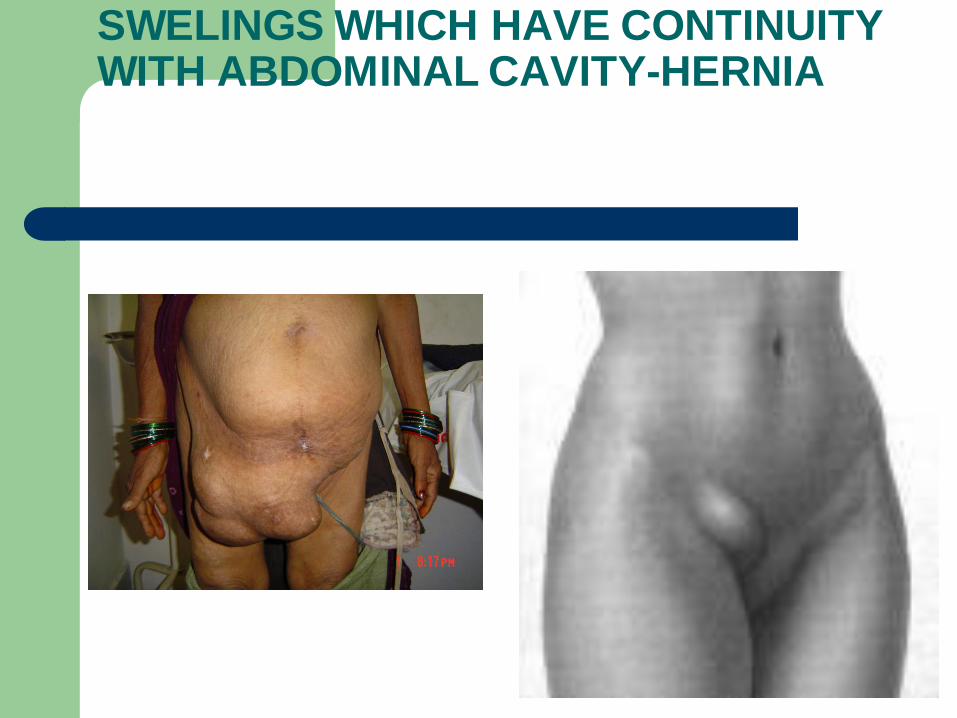
SWELINGS WHICH HAVE CONTINUITY WITH ABDOMINAL CAVITY-HERNIA
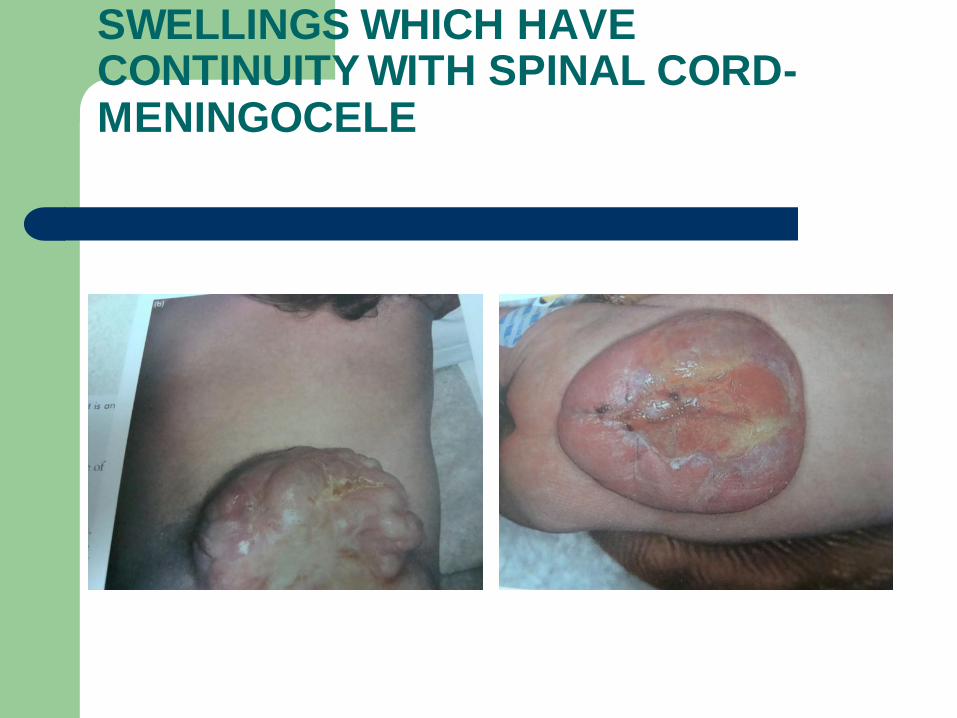
SWELLINGS WHICH HAVE CONTINUITY WITH SPINAL CORD-MENINGOCELE
REDUCIBILITY
SWELLING REDUCES AND ULTIMATELY DISSAPPEARS AS
SOON AS PRESS UP ON
Does not appear on removal of swelling
Appears after increase in counter pressure
THIS IS A FEATURE OF HERNIA
LYMH VARIX,VARICOCELE,SAPHENA
VARIX,MENINGOCELE ARE REDUCIBLE PARTLY OR
COMPLETELY
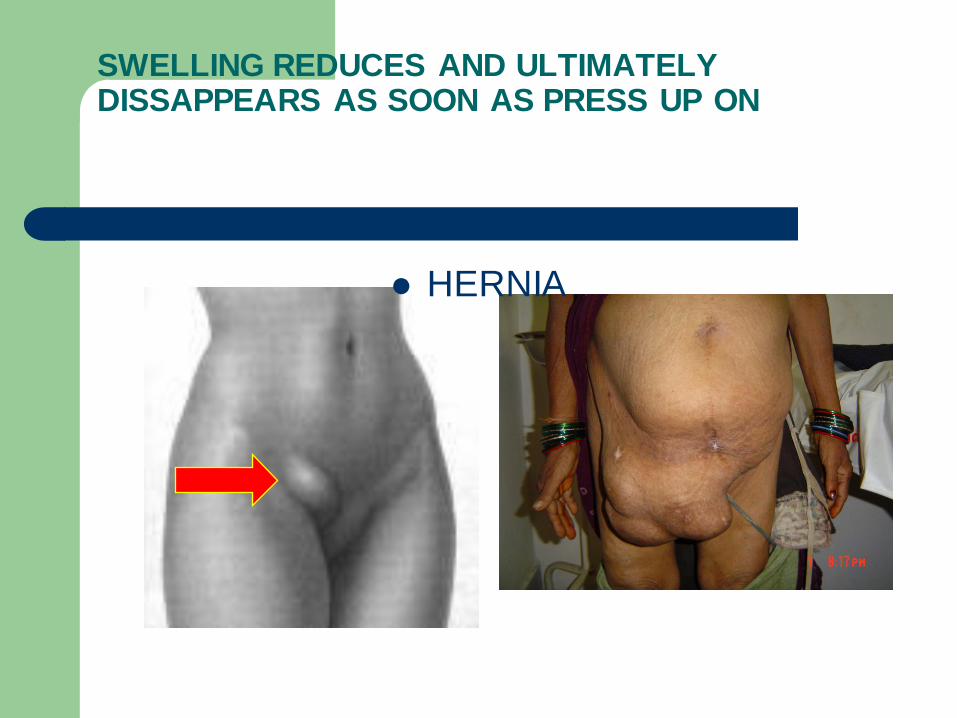
SWELLING REDUCES AND ULTIMATELY DISSAPPEARS AS SOON AS PRESS UP ON
HERNIA
COMPRESSIBILITY
THE SWELLING CAN BE COMPRESSED BUT NOT BE
DISSAPPEARED COMPLETELY
THE SWELLING REAPPEAS WHEN PRESSURE IS TAKEN
OFF
HAEMANGIOMA,LYMPHANGIOMA

HAEMANGIOMA
PULSATILITY
ARISING FROM ARTERY--EXPANSILE PULSATION-
ANEURISM
VERY CLOSE TO ARTEY---TRANSMITTED PULSATION
SWELLING IS HIGHLY VASCULAR-----------
TELANGIECTATIC SARCOMA
FIXITY TO THE SKIN
SHOULD TEST WHETHER SKIN OVER THE SWELLING
PINCHABLE OR NOT
SEBACEOUS CYST, PAPILLOMA,EPITHELIOMA ARISE
FROM SKIN THEY MOVE WITH SKIN
IN MALIGNANT SELLINGS IF SKIN IS INFILTRATED SKIN IS
NOT PINCHABLE

SEBACEOUS CYST, ARISE FROM SKIN THEY MOVE WITH SKIN
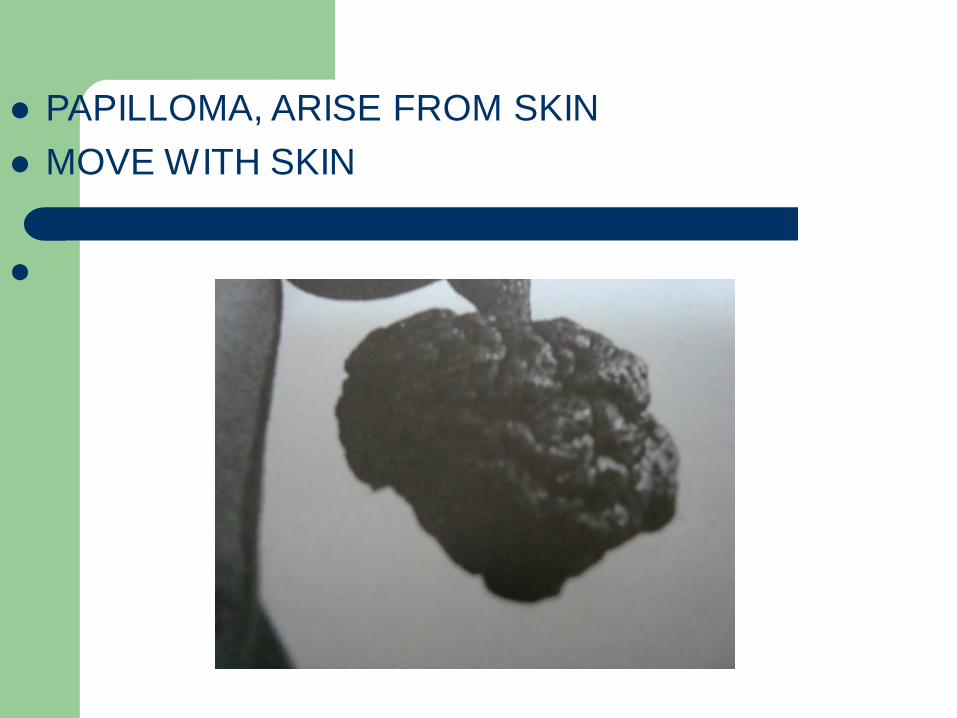
PAPILLOMA, ARISE FROM SKIN
MOVE WITH SKIN
PLANE OF THE SWELLING
SKIN---SKIN IS NOT MOVED OVER THE SWELLING
SUBCUTANEOU TISSUE----the tumors arising from subcutaneous are free from both skin and underlying contracted muscle.SKIN IS PINCHABLE&SWELLING PROMINENT WHEN MUSCLE IS contracted & MOVES freely over contracted muscle
Swellings arising from the deep fascia are not as mobile as those arising from the sub cutaneous tissue.but it is very difficult to find out whether the tumor is fixed to deep fascia or not as the fascia can not be made taught separately from muscle.
When the tumor arises from sub cutaneous tissue and fixed to
muscle, the tumor will be more prominent and cannot be moved
along the fibres of muscle when the muscle is contracted.
If the tumor incorporated in the muscle, it will be fixed and
decreases in size when the muscle is contracted. If the tumor lies deep to muscle, it virtually disappears as soon
as muscle become taught
Some times swelling appears when the muscle is taught. this is
due to tear in the tendon concerned.
Swellings in connection with the tendon of muscle moves along
with the tendon and become fixed when the muscle is made
taught against resistance.
Swelling in connection with the vessels and nerves don't move
along the line of the said vessel , the but moves a little extent at
right angles to their axes
Swellings arising from bone or absolutely fixed even when the
muscle is relaxed and cannot be moved apart from bone.
Secondary changes to the swelling-----seen in malignant swellings,tuberculous lymph nodal mass
REGIONAL LYMPH NODES—no examination is complete with out the examination of draining lymph nodes. When regional lymph nodes are enlarged it is good practice to examine other group of lymph nodes. to exclude generalized lymphadenopathy.-
PERCUSSION :the importace of this examination is not that much important in swelling. its sole place is to find out the presence of resonant note on percussion over hernia. or to elicit tender ness in brodies abscess.
Auscultation: all pulsatile swellings should be
Auscultated.machinary murmer is heard in an aneurysmal varix.
Movements: joints nearby swelling should be examined for
movements to find out whether the joint is involvedd or not.
Examine for pressure effects: 1)the arterial pulse distal to
swelling some times swelling may press upon main artery of the
limb and cause weak pulse distally.2)the nerves may be
effected by the pressure of swelling, this cause wasting of
muscle,paresis,paralysis.3)swelling may exert pressure on
bone eroding it as in aneurysm,dermoidcyst.
General examination in malignant swellings
Examine the chest for consolidation, pleural effusion
Liver for secondaries
General examination of abdomen to find out peritoneal metastases
The spine,pelvis,the trochanters of femurs,skull to exclude metastases
If one group of lymph nodes are enlarged examine other group of lymph nodes
If swelling is suspected of gumma or condyloma, examine for other syphilitic stigmata
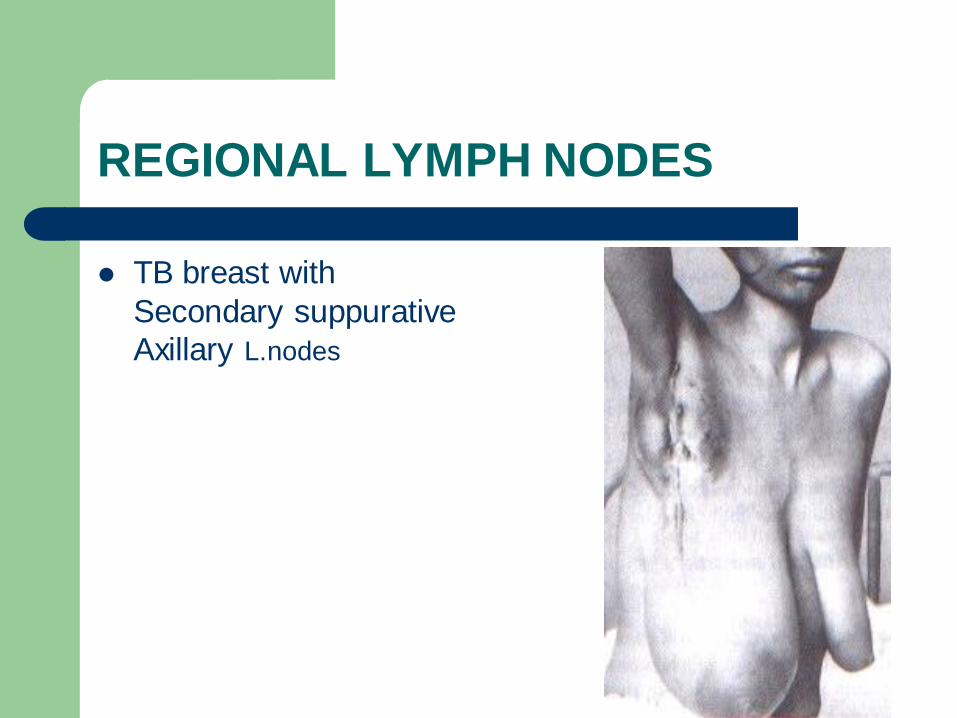
REGIONAL LYMPH NODES
TB breast with
Secondary suppurative
Axillary L.nodes