Ex Utero Intrapartum Treatment Procedure (EXIT) Bhavani Shankar Kodali MD Anesthesiologist-in-Chief,...
25
Ex Utero Intrapartum Treatment Procedure (EXIT) Bhavani Shankar Kodali MD Anesthesiologist-in-Chief, Interim Chairman Brigham and Women’s Hospital Associate Professor Harvard Medical School
-
Upload
clinton-barton -
Category
Documents
-
view
226 -
download
0
Transcript of Ex Utero Intrapartum Treatment Procedure (EXIT) Bhavani Shankar Kodali MD Anesthesiologist-in-Chief,...

Ex Utero Intrapartum Treatment Procedure (EXIT)
Bhavani Shankar Kodali MDAnesthesiologist-in-Chief, Interim Chairman
Brigham and Women’s Hospital
Associate ProfessorHarvard Medical School

Why this session?
• Full term • Fetal anomaly• No time to referral• Your facility can undertake corrective
surgery

Fetal Surgery
• Open Fetal Surgery
• Minimally Invasive Fetal Surgery
• EXIT


Goals
• Correct and improve fetal anomaly
• Minimize the risk to the mother

Open Fetal Surgery

Minimally Invasive Fetal Surgery


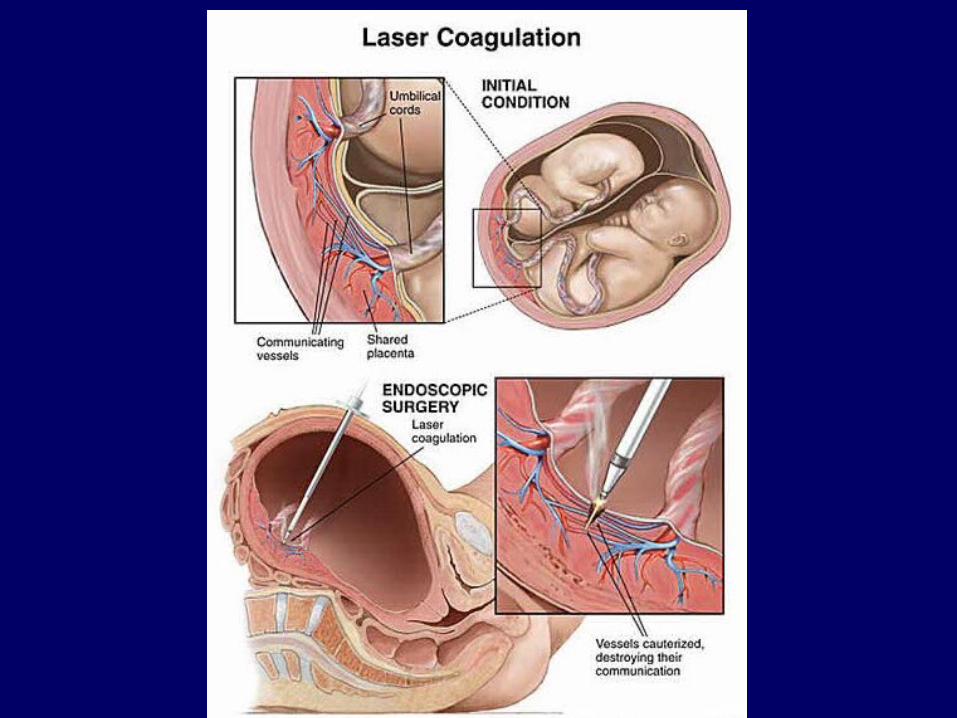
Minimally Invasive Fetal Surgery• Twin-Twin Transfusion syndrome• Obstructive uropathy: shunt insertion and
valve ablation• Aortic or pulmonary stenosis: Valvoplasty• Cyanotic heart disease: atrial septostomy• Congenial diaphragm hernia: tracheal
balloon occlusion• Spina bifida: fetoscopic closure of the defect



Anesthesia
• General anesthesia
• Epidural analgesia
• Combined spinal anesthesia
• Fetal analgesia and relaxation


EXIT
• A modification of cesarean delivery.
• Baby is partially (head and upper torso) or, less often, completely delivered.
• Placental support is maintained and the baby oxygenated via placental blood flow

What should you know?
• Not an intra-partum procedure
• You may have a baby that may require EXIT until pediatric surgeons secure the oxygenation via other means
• Most procedures last a matter of minutes (eg, tracheal intubation)

When Do You Perform
• Not at preterm
• At, or close to term
• Ideally should not be in labor

What is the requirement?
• Uterine relaxation is important not only to facilitate delivery of fetal head but also to prevent placental separation and to preserve utero-placental flow during the procedure

Management
• Usual Cesarean Delivery
• Uterine relaxation


Procedure
• Arterial line
• Spinal with Duramorph (Hydromorphone)
• General anesthesia

ECMO – 32 weeks - CHD• Arterial Line• Spinal in the labor room with Duramorph• General Anesthesia• Isoflurane, Sevoflurane, Desflurane• Phenylephrine boluses• Decreased inhalational agent to 0.5 mac• BIS is a good idea• Uterotonics may be necessary• Hemorrhage• Reversal and extubation

Regional Anesthesia
• Uterine relaxation – Nitroglycerine