
EW ORK–PRESBYTERIAN Neuroscience · for invading into multiple anatomi-cal compartments,...
8
P hysicians at NewYork- Presbyterian Hospital and its affiliated medical schools—Columbia University College of Physicians & Surgeons and Weill Medical College of Cornell University—have devel- oped an approach to skull base sur- gery that allows personalized atten- tion to the disease process and the emotional aspects of patient care. “Skull base tumors are notorious for invading into multiple anatomi- cal compartments, including the skull, brain, nasal sinuses, orbit, and neck,” said Jeffrey N. Bruce, MD. “Our ability to draw on the expertise of a diverse group of surgeons, a multi- disciplinary skull base team, enables us to handle even the most complex problems.” With a team of world-renowned experts striving to improve patient outcomes, the Hospital’s program offers state-of-the-art treatment for a wide variety of tumors and vascular abnormalities, including acoustic neuromas, pituitary adenomas, chordomas, and carcinomas of the head and neck. “There is nothing we can’t handle,” said Philip E. Stieg, PhD, MD. Intensive microsurgery is frequently used to treat the skull base lesion. However, according to Susan Pannullo, MD, radiosurgical options may be the best modality for addressing a particular patient’s pathology. That is why the treatment algorithm is developed based on the specific needs of each patient. “We can choose from a variety of approaches,” Dr. Pannullo said. “Physicians may be less comfortable treating with radiosurgery if their hospital doesn’t have this great treatment option and a team to design the best way for treating that patient.” D uring the past decade, Gamma Knife radiosurgery has made possible a considerable num- ber of advances in the field of neuro- surgery. Researchers at NewYork- Presbyterian Hospital and its affiliated medical schools—Columbia University College of Physicians & Surgeons and Weill Medical College of Cornell University—continue to be at the fore- front of the trend, applying this target- ed modality to an ever-widening range of indications. Gamma Knife comple- ments other radiosurgical options avail- able through the Hospital, which has one of the most comprehensive radio- surgical programs in the country. “Since our first radiosurgical treat- ment in 1989, we have continuously expanded our technology and experi- ence,” said Steven Isaacson, MD. “The goal is to improve the health of our patients and the well-being of their families.” Gamma Knife surgery is a safe and noninvasive modality. It is capable of delivering up to 201 beams of gamma radiation, which converge, with pin- point accuracy, on the targeted abnor- mality in the brain. Because of the con- vergence of the rays, enough radiation is provided to treat the diseased area, yet the low intensity of each individual beam ensures the safety of surrounding healthy tissue. Treatment with the Gamma Knife greatly reduces the incidence of com- plications after treatment in compari- son with conventional therapy, and Gamma Knife Expands Treatment Options see Gamma Knife, page 7 TABLE of CONTENTS Image-Guided Neurosurgery 2 Information-rich images of the brain allow surgerons to perform sophisticated procedures with unprecedented precision. Attacking Brain Tumors Directly 4 Researchers are exploring the advantages of convection-enhanced therapy in the treatment of brain tumors. Evaluating Tumor Response 6 Magnetic resonance spectroscopy complements magnetic resonance imaging. Personalizing Patient Care In Skull Base Surgery Navigation technologies allow neurosurgeons to navigate with precision. see Skull Base, page 5 Neuroscience Spring 2004 N EW Y ORK –P RESBYTERIAN Upcoming CME Events 2004 • Neurostimulation in Neurology and Psychi- atry—May 15; please call (212) 746-2625 • Neuro-Oncology Update—October 8th • Brain Attack and Cerebrovascular Disease Update 2004—November 19th Affiliated with COLUMBIA UNIVERSITY COLLEGE OF PHYSICIANS & SURGEONS and WEILL MEDICAL COLLEGE OF CORNELL UNIVERSITY
Transcript of EW ORK–PRESBYTERIAN Neuroscience · for invading into multiple anatomi-cal compartments,...
Physicians at NewYork-Presbyterian Hospital andits affiliated medical
schools—Columbia UniversityCollege of Physicians & Surgeonsand Weill Medical College ofCornell University—have devel-oped an approach to skull base sur-gery that allows personalized atten-tion to the disease process and theemotional aspects of patient care.
“Skull base tumors are notoriousfor invading into multiple anatomi-cal compartments, including theskull, brain, nasal sinuses, orbit,and neck,” said Jeffrey N. Bruce,MD. “Our ability to draw on the expertise of a diverse group of surgeons, a multi-disciplinary skull base team, enables us to handle even the most complex problems.”
With a team of world-renowned experts striving to improve patient outcomes, theHospital’s program offers state-of-the-art treatment for a wide variety of tumors andvascular abnormalities, including acoustic neuromas, pituitary adenomas, chordomas,and carcinomas of the head and neck.
“There is nothing we can’t handle,” said Philip E. Stieg, PhD, MD.Intensive microsurgery is frequently used to treat the skull base lesion. However,
according to Susan Pannullo, MD, radiosurgical options may be the best modalityfor addressing a particular patient’s pathology. That is why the treatment algorithmis developed based on the specific needs of each patient.
“We can choose from a variety of approaches,” Dr. Pannullo said. “Physicians maybe less comfortable treating with radiosurgery if their hospital doesn’t have this greattreatment option and a team to design the best way for treating that patient.”
During the past decade, GammaKnife radiosurgery has madepossible a considerable num-
ber of advances in the field of neuro-surgery. Researchers at NewYork-Presbyterian Hospital and its affiliatedmedical schools—Columbia UniversityCollege of Physicians & Surgeons andWeill Medical College of CornellUniversity—continue to be at the fore-front of the trend, applying this target-ed modality to an ever-widening rangeof indications. Gamma Knife comple-ments other radiosurgical options avail-able through the Hospital, which hasone of the most comprehensive radio-surgical programs in the country.
“Since our first radiosurgical treat-ment in 1989, we have continuouslyexpanded our technology and experi-ence,” said Steven Isaacson, MD. “Thegoal is to improve the health of ourpatients and the well-being of theirfamilies.”
Gamma Knife surgery is a safe andnoninvasive modality. It is capable ofdelivering up to 201 beams of gammaradiation, which converge, with pin-point accuracy, on the targeted abnor-mality in the brain. Because of the con-vergence of the rays, enough radiationis provided to treat the diseased area,yet the low intensity of each individualbeam ensures the safety of surroundinghealthy tissue.
Treatment with the Gamma Knifegreatly reduces the incidence of com-plications after treatment in compari-son with conventional therapy, and
Gamma KnifeExpands TreatmentOptions
see Gamma Knife, page 7
TAB
LEo
fC
ON
TEN
TS Image-Guided Neurosurgery
2Information-rich images of the brain allowsurgerons to perform sophisticated procedures with unprecedented precision.
Attacking Brain Tumors Directly
4Researchers are exploring the advantages of convection-enhanced therapy in the treatment of brain tumors.
Evaluating Tumor Response
6Magnetic resonance spectroscopycomplements magnetic resonanceimaging.
Personalizing Patient Care In Skull Base Surgery
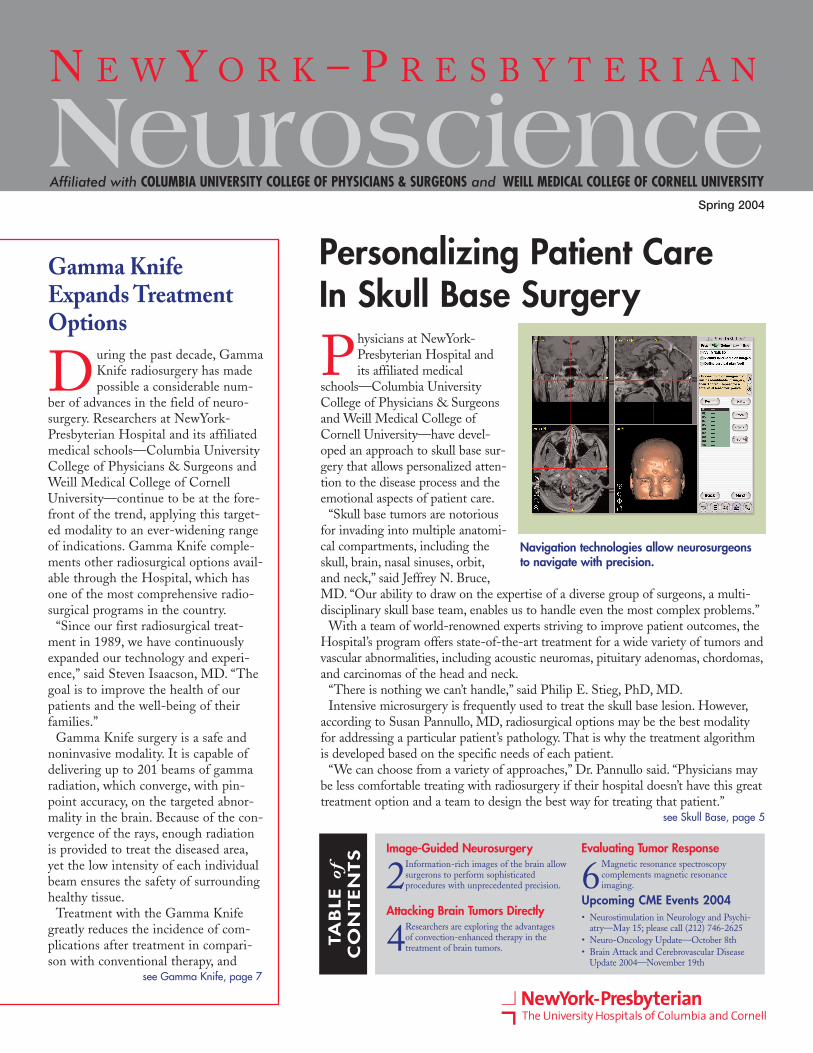
Navigation technologies allow neurosurgeonsto navigate with precision.
see Skull Base, page 5
NeuroscienceSpring 2004
N E W Y O R K – P R E S B Y T E R I A N
Upcoming CME Events 2004• Neurostimulation in Neurology and Psychi-
atry—May 15; please call (212) 746-2625• Neuro-Oncology Update—October 8th• Brain Attack and Cerebrovascular Disease
Update 2004—November 19th
Affiliated with COLUMBIA UNIVERSITY COLLEGE OF PHYSICIANS & SURGEONS and WEILL MEDICAL COLLEGE OF CORNELL UNIVERSITY
2 Spring 2004
U sing information-rich imagesof the brain obtained duringsurgery, neurosurgeons at
NewYork-Presbyterian Hospital andWeill Medical College of CornellUniversity can perform sophisticatedprocedures with unprecedentedprecision. Called intraoperative mag-netic resonance imaging, this processenables surgeons to visualize intra-cerebral lesions in real time, facilitatingtheir complete resection and improvingoutcome.
“With intraoperative magnetic reso-nance imaging, we can acquire imagesin the operating room while we areworking and adjust our surgical planbased on the updated information,”said Theodore Schwartz, MD.
According to Dr. Schwartz, intraoper-ative magnetic resonance imaging allowsthe fullest possible resection of manybrain tumors with maximum safety. It isalso an option in cases of intractableepilepsy. The Department ofNeurosurgery at NewYork-Presbyterian/Weill Cornell owns 1 of just 17 unitscurrently available in the United States.
Determining tumor margins anddelineating brain structures precisely isalways a challenge, and neurosurgeonshave employed a variety of ingenioustechnologies over the years, rangingfrom computed tomography to conven-tional magnetic resonance imaging, tovisualize the brain before surgery.
During procedures, they have used theoperating microscope and computer-assisted surgical navigation. All suchsystems are limited, however, becausefunctional brain structures may shiftslightly during surgery (thoughstereotactic methods can be used todevelop accurate spatial coordinatesand localize brain regions with a fair
degree of precision).One consequence of even minor
alterations in the position of the brainparenchyma is that in the interest ofavoiding harm to the patient, surgeonsmay perform resections that fail toinclude some portion of the lesion. Agrowing body of evidence indicatesthat incomplete resections are responsi-ble for less-than-optimal results inabout one third of cases in which onlypreoperative images are used. Fluo-roscopy and computed tomography,other methods that can be used intra-operatively, in principle, lack the reso-lution of magnetic resonance imagingand have the practical disadvantage ofexposing patients to ionizing radiation.
Developed in the mid-1990s and firstreported in 1997, intraoperative mag-netic resonance imaging was designed
Expanding the Range of Image-Guided NeurosurgeryNeuroscienceN E W Y O R K – P R E S B Y T E R I A N
“With intraoperative magnetic resonance imaging, we can acquire images in the operating room while we areworking and adjust our surgical plan....”
—Theodore Schwartz, MD
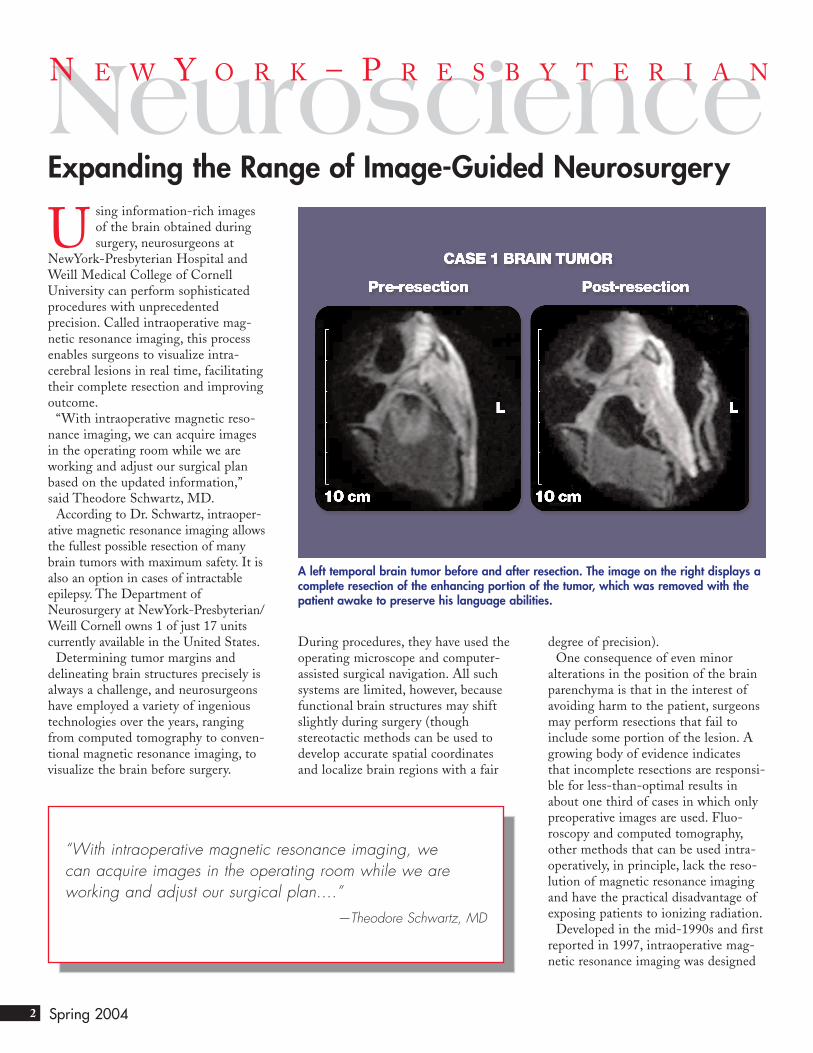
A left temporal brain tumor before and after resection. The image on the right displays acomplete resection of the enhancing portion of the tumor, which was removed with thepatient awake to preserve his language abilities.

3
in an attempt to address this problem.Because intraoperative magnetic resonanceimaging works by analyzing radio waves, amobile radio frequency shield is placedaround the patient’s head. The magnet of thescanner is weak enough that it does notaffect the use of instruments.
Once an image is acquired, noted Dr.Schwartz, “we can use that information forwhat we call ‘intraoperative navigation’—thatis, we can point anywhere in the brain, andthe computer will tell us exactly where we’repointing, from the intraoperative magneticresonance imaging scan that we just took.”
With its capacity to visualize tumor mar-gins, intraoperative magnetic resonanceimaging has been applied with great successin resecting various types of primary braintumors, including lower-grade, slowly grow-ing gliomas and higher-grade gliomas, whichgrow faster and are more often malignant.Transsphenoidal surgery for pituitary adeno-mas (benign neoplasms of the pituitarygland, which can be removed through thenose) is also greatly enhanced with the use ofintraoperative magnetic resonance imaging.
In a recently published study (Epilepsia2002;43:430-436), Dr. Schwartz and otherresearchers found that intraoperative mag-netic resonance imaging appears to be usefulin cases that call for a radical amygdalohip-pocampectomy. In this procedure, used totreat intractable medial temporal lobe epilep-sy, surgeons remove the amygdala, hip-pocampus, and parahippocampal gyrus.Retrospective imaging studies indicate ahigher rate of postoperative seizures if anyportion of these structures escapes resection.Dr. Schwartz and colleagues followed 5 con-secutive patients who underwent this proce-dure with the use of intraoperative magneticresonance imaging and demonstrated post-operatively that the hippocampectomy wascomplete in all cases. These patients haveremained seizure-free.
“We’re doing the same operations wealways did,” said Dr. Schwartz. “We’re justdoing them better.”
Theodore Schwartz, MD, is Director, Center for Epilepsy Surgery at NewYork-PresbyterianHospital/Weill Cornell Medical Center, and isAssistant Professor of Neurological Surgery atWeill Medical College of Cornell University.E-mail: [email protected].
NewYork-Presbyterian Neuroscience is a publication of the Neuroscience Centers ofNewYork-Presbyterian Hospital. The Neuroscience Centers are at the forefront ofresearch and practice in the diagnosis, treatment, and rehabilitation of neurologic dis-ease. NewYork-Presbyterian Hospital is located at Columbia University Medical Centerand NewYork Weill Cornell Medical Center. The Neuroscience Centers include theNeurological Institute at NewYork-Presbyterian Hospital/Columbia University MedicalCenter and the Weill Cornell Neuroscience Institute at NewYork-PresbyterianHospital/Weill Cornell Medical Center, which are respectively affiliated with ColumbiaUniversity College of Physicians & Surgeons and the Weill Medical College of CornellUniversity.
NewYork-Presbyterian Neuroscience Editorial Board M.Flint Beal, MDNeurologist-in-Chief,NewYork-Presbyterian/Weill Cornell Anne Parrish Titzel Professor of Neurologyand Chairman, Department of Neurology,Weill Medical College of Cornell [email protected]
Y. Pierre Gobin, MDDirector, Division of InterventionalNeuroradiology,NewYork-Presbyterian/Weill CornellProfessor of Radiology in NeurologicalSurgery, Weill Medical College of Cornell [email protected]
Sean Lavine, MDCo-Director, Neuroendovascular Services,NewYork-Presbyterian/ColumbiaAssistant Professor of Neurological Surgeryand Radiology, Columbia University Collegeof Physicians & [email protected]
James Lieberman, MDPhysiatrist-in-Chief,NewYork-Presbyterian/Columbia H.K. Corning Professor and Chairman,Department of Rehabilitation Medicine,Columbia University College of Physicians & SurgeonsProfessor of Rehabilitation Medicine andChief, Division of Rehabilitation Medicine,Weill Medical College of Cornell [email protected]
Philip Meyers, MDCo-Director, Neuroendovascular Services,NewYork-Presbyterian/Columbia Assistant Professor of Neurological Surgeryand Radiology, Columbia University Collegeof Physicians & [email protected]
Michael O’Dell, MDAssociate Chief, Department ofRehabilitation Medicine,NewYork-Presbyterian/Weill CornellAssociate Chief and Professor ofRehabilitation Medicine, Weill MedicalCollege of Cornell [email protected]
Timothy Pedley, MDNeurologist-in-Chief,NewYork-Presbyterian/ColumbiaHenry and Lucy Moses Professor ofNeurology and Chairman, Department ofNeurology, Columbia University College of Physicians & [email protected]
Howard Riina, MDAttending Neurosurgeon,NewYork-Presbyterian/Weill Cornell Assistant Professor of Neurological Surgery,Neurology and Radiology, Weill MedicalCollege of Cornell [email protected]
Robert Solomon, MDChairman and Director of Service,Department of Neurological Surgery,NewYork-Presbyterian/Columbia Byron Stookey Professor of NeurologicalSurgery, Columbia University College of Physicians & [email protected]
Philip Stieg, PhD, MDNeurosurgeon-in-Chief, Department ofNeurological Surgery,NewYork-Presbyterian/Weill Cornell Professor and Chairman, Department ofNeurological Surgery, Weill Medical Collegeof Cornell [email protected]
Steven Isaacson, MDCo-Director, Center for RadiosurgeryDepartment of Radiation OncologyNewYork-Presbyterian/ColumbiaAssistant Professor of Clinical NeurologicalSurgery & Clinical Otolaryngology,Columbia University College of Physicians & [email protected]
Susan Pannullo, MDDirector of Neuro-OncologyDepartment of Neurological SurgeryNewYork-Presbyterian/Weill CornellAssistant Professor of Neurological SurgeryWeill Medical College of Cornell [email protected]
Guest Editors:
4 Spring 2004
Can brain tumors defend them-selves against a direct attack aswell as they do against systemic
(ie, intravenous) drug delivery?Researchers at the Herbert IrvingComprehensive Cancer Center atNewYork-Presbyterian Hospital/Columbia University Medical Center areseeking to learn just that as part of anongoing Phase I clinical trial.
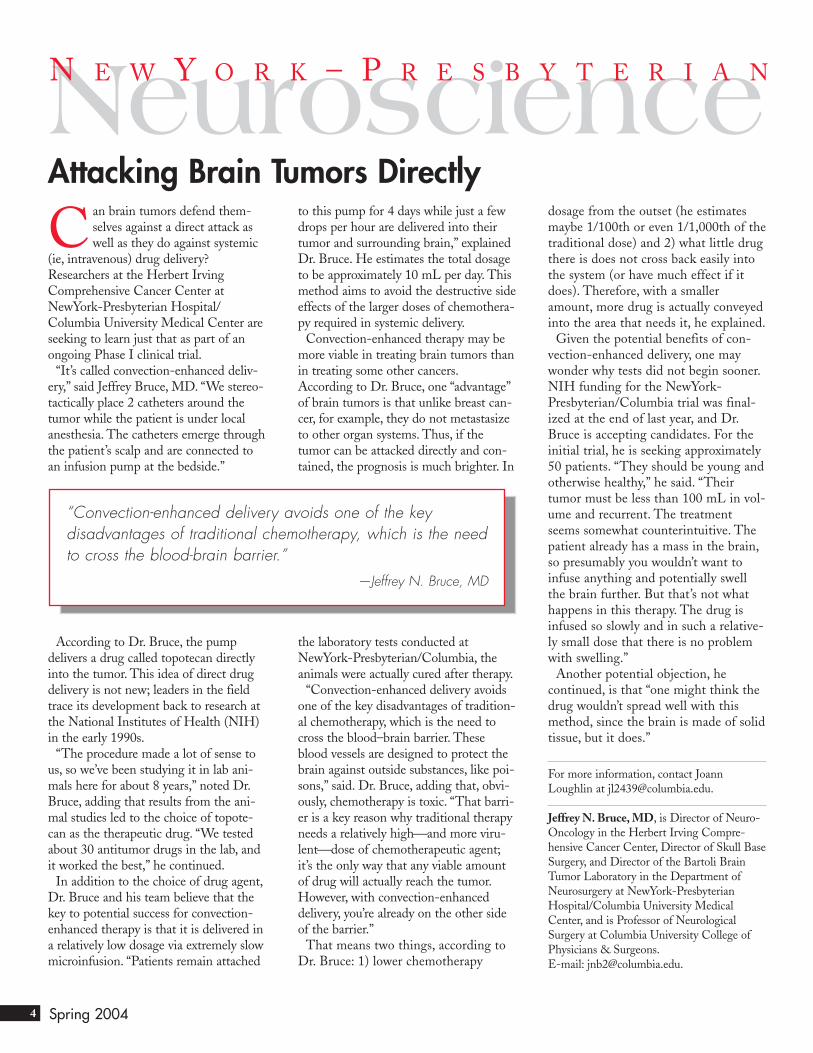
“It’s called convection-enhanced deliv-ery,” said Jeffrey Bruce, MD. “We stereo-tactically place 2 catheters around thetumor while the patient is under localanesthesia. The catheters emerge throughthe patient’s scalp and are connected toan infusion pump at the bedside.”
According to Dr. Bruce, the pumpdelivers a drug called topotecan directlyinto the tumor. This idea of direct drugdelivery is not new; leaders in the fieldtrace its development back to research atthe National Institutes of Health (NIH)in the early 1990s.
“The procedure made a lot of sense tous, so we’ve been studying it in lab ani-mals here for about 8 years,” noted Dr.Bruce, adding that results from the ani-mal studies led to the choice of topote-can as the therapeutic drug. “We testedabout 30 antitumor drugs in the lab, andit worked the best,” he continued.
In addition to the choice of drug agent,Dr. Bruce and his team believe that thekey to potential success for convection-enhanced therapy is that it is delivered ina relatively low dosage via extremely slowmicroinfusion. “Patients remain attached
to this pump for 4 days while just a fewdrops per hour are delivered into theirtumor and surrounding brain,” explainedDr. Bruce. He estimates the total dosageto be approximately 10 mL per day. Thismethod aims to avoid the destructive sideeffects of the larger doses of chemothera-py required in systemic delivery.
Convection-enhanced therapy may bemore viable in treating brain tumors thanin treating some other cancers.According to Dr. Bruce, one “advantage”of brain tumors is that unlike breast can-cer, for example, they do not metastasizeto other organ systems. Thus, if thetumor can be attacked directly and con-tained, the prognosis is much brighter. In
the laboratory tests conducted atNewYork-Presbyterian/Columbia, theanimals were actually cured after therapy.
“Convection-enhanced delivery avoidsone of the key disadvantages of tradition-al chemotherapy, which is the need tocross the blood–brain barrier. Theseblood vessels are designed to protect thebrain against outside substances, like poi-sons,” said. Dr. Bruce, adding that, obvi-ously, chemotherapy is toxic. “That barri-er is a key reason why traditional therapyneeds a relatively highand more viru-lentdose of chemotherapeutic agent;it’s the only way that any viable amountof drug will actually reach the tumor.However, with convection-enhanceddelivery, you’re already on the other sideof the barrier.”
That means two things, according toDr. Bruce: 1) lower chemotherapy
dosage from the outset (he estimatesmaybe 1/100th or even 1/1,000th of thetraditional dose) and 2) what little drugthere is does not cross back easily intothe system (or have much effect if itdoes). Therefore, with a smalleramount, more drug is actually conveyedinto the area that needs it, he explained.
Given the potential benefits of con-vection-enhanced delivery, one maywonder why tests did not begin sooner.NIH funding for the NewYork-Presbyterian/Columbia trial was final-ized at the end of last year, and Dr.Bruce is accepting candidates. For theinitial trial, he is seeking approximately50 patients. “They should be young andotherwise healthy,” he said. “Theirtumor must be less than 100 mL in vol-ume and recurrent. The treatmentseems somewhat counterintuitive. Thepatient already has a mass in the brain,so presumably you wouldn’t want toinfuse anything and potentially swellthe brain further. But that’s not whathappens in this therapy. The drug isinfused so slowly and in such a relative-ly small dose that there is no problemwith swelling.”
Another potential objection, hecontinued, is that “one might think thedrug wouldn’t spread well with thismethod, since the brain is made of solidtissue, but it does.”
For more information, contact JoannLoughlin at [email protected].
Jeffrey N. Bruce, MD, is Director of Neuro-Oncology in the Herbert Irving Compre-hensive Cancer Center, Director of Skull BaseSurgery, and Director of the Bartoli BrainTumor Laboratory in the Department ofNeurosurgery at NewYork-PresbyterianHospital/Columbia University MedicalCenter, and is Professor of NeurologicalSurgery at Columbia University College ofPhysicians & Surgeons.E-mail: [email protected].
Attacking Brain Tumors DirectlyNeuroscienceN E W Y O R K – P R E S B Y T E R I A N
“Convection-enhanced delivery avoids one of the key disadvantages of traditional chemotherapy, which is the needto cross the blood-brain barrier.”
—Jeffrey N. Bruce, MD

5
The emotional aspects of treatment areaddressed by support personnel, includ-ing a team of nurse practitioners, physi-cian assistants and administrative staff.“We don’t just view the patient as havinga disease process we can treat surgically,”said Dr. Stieg. “Because skull basesurgeries are often extremely complexand difficult, time must be taken toexplain the diagnosis, treatment options,and risks.”
At NewYork-Presbyterian Hospital,neurological surgeons, otorhinolaryngol-ogists, plastic surgeons, vascular surgeons,interventional neuroradiologists, andpediatric surgeons work in close collabo-ration with the patient to develop multi-modal approaches for improving patientsurvival and quality of life. Surgeons haveincorporated unique surgical approaches.For example, pituitary adenomas can betreated endoscopically in conjunctionwith intraoperative magnetic resonanceimaging. This minimally invasive proce-dure eliminates the need for postopera-tive packing. Early results suggest theprocedure shortens hospitalization timeand achieves equivalent resections com-pared with an open procedure. “Intra-operative magnetic resonance imagingallows us to confirm complete removal ofthe tumor, while the endoscope allows usto do the procedure in a minimally inva-sive fashion,” said Dr. Stieg.
Skull base lesion treatment can be facil-itated by an image guidance system thatallows surgeons to confirm the anatomiclocation of the tumor before operating.This “stealth” image guidance systemuses magnetic resonance imaging orcomputed tomography scans takenpresurgically to produce a 3-dimensionalmodel of the skull. Surgeons use the 3-dimensional image as a navigationalmap during tumor resection. Thus, asafer and more complete excision of thetumor can be achieved, possibly offeringthe patient a better long-term prognosis.
When the risks of aggressive micro-surgery are deemed too great, theHospital has one of the country’s most
comprehensive radiosurgical programs.These procedures have been “very effec-tive and safe for treatment of many typesof skull base tumors that cannot beresected without irreversible damage,”said Michael Sisti, MD.
Radiosurgery options available topatients include Gamma Knife; 3-dimensional intensity modulated radia-tion therapy, in which radiation isshaped to correspond precisely to thetarget site, using varying beam-intensitymodulation technology; and linear accel-erator-based radiosurgery, which utilizesa single, highly focused beam, applied inmultiple passes.
“These techniques in combination areexcellent adjuncts to the noninvasivemanagement of skull base tumors,” Dr.Sisti said. “We can recommend a treat-ment course more evenhandedly thanmight be the case in institutions whereonly one technology is available.”
The complexity of the skull base regiononce rendered many tumors inoperable.However, because of advances in micro-surgery and radiological imaging, manymore tumors are treatable than in thepast. At the same time, improvements insurgical technique and adoption of radio-surgical modalities have dramaticallyreduced complication rates. Despite theprogress, skull base surgery remains com-plicated and risky for many patients.Thus, the skill and experience of thetreating clinician is an important factorto consider. According to StevenIsaacson, MD, NewYork-PresbyterianHospital provides an “unprecedentedlevel of service” to patients and referringphysicians. “We have neurosurgeons,radiation oncologists, clinical neuro-psychologists, diagnostic neuroradiolo-gists, and others, all of whom enjoy ahealthy clinical relationship. We believe
this translates into better outcomes forour patients.”
Jeffrey N. Bruce, MD, is Director of Neuro-Oncology in the Herbert Irving Compre-hensive Cancer Center, Director of Skull BaseSurgery, and Director of the Bartoli BrainTumor Laboratory in the Department ofNeurosurgery at NewYork-PresbyterianHospital/Columbia University MedicalCenter, and is Professor of NeurologicalSurgery at Columbia University College ofPhysicians & Surgeons.E-mail: [email protected].
Steven Isaacson, MD, is Co-Director, of theCenter for Radiosurgery in the Departmentof Radiation Oncology at NewYork-Presbyterian Hospital/Columbia UniversityMedical Center, and is Associate Professor ofClinical Radiation Oncology & ClinicalOtolaryngology at Columbia UniversityCollege of Physicians & Surgeons.E-mail: [email protected].
Susan Pannullo, MD, is Director of Neuro-Oncology in the Department of NeurologicalSurgery at NewYork-Presbyterian Hospital/Weill Cornell Medical Center, and isAssistant Professor of Neurological Surgery atWeill Medical College of Cornell University.E-mail: [email protected].
Michael B. Sisti, MD, is Co-Director of theCenter for Radiosurgery in the Departmentof Neurological Surgery at NewYork-Presbyterian Hospital/Columbia UniversityMedical Center, and is Assistant Professor ofNeurological Surgery at Columbia UniversityCollege of Physicians & Surgeons.E-mail: [email protected].
Philip E. Stieg, PhD, MD , isNeurosurgeon-in-Chief of the Department of Neurological Surgery at NewYork-Presbyterian Hospital/Weill Cornell MedicalCenter, and is Professor and Chairman of theDepartment of Neurological Surgery at WeillMedical College of Cornell University.E-mail: [email protected].
Skull Basecontinued from page 1
“We have neurosurgeons, radiation oncologists, clinicalneuropsychologists, diagnostic neuroradiologists... [The hospital provides] an unprecedented level of service.”
— Steven Isaacson, MD

6 Spring 2004
NewYork-Presbyterian Hospital investigators are movingforward with research that may help establish magneticresonance spectroscopy as an imaging modality com-
plementary to magnetic resonance imaging, for evaluating cere-bral tumor response to therapy.
“Potentially, the efficacy of different types of therapy could beevaluated based on metabolite changes seen with magnetic reso-nance spectroscopy,” said Casilda Balmaceda, MD. Magneticresonance spectroscopy has also been proven successful at con-sistently identifying metabolic changes in cerebral tumors,according to Pina Sanelli, MD.
Metabolites commonly observed in magnetic resonance spec-troscopy include choline (Cho), the levels of which areincreased in tumor regions. High levels of choline indicate highlevels of cell membrane production or breakdown in the regionof interest. Other common metabolites observed in magneticresonance spectroscopy are creatine (Cr), lactate (Lac) and N-acetyl-aspartate (NAA), the latter of which is thought to existonly in neurons and is decreased in regions of viable tumor.Lactate may also be increased in tumor as a result of increasedanaerobic glycolysis, a preferred metabolic pathway for glucosein tumor tissue.
“Magnetic resonance spectroscopy will provide information onthe heterogeneity patterns of these metabolic levels in tumors,”Dr. Sanelli said. “The spectral pattern may also give usefulinformation in estimating tumor regression or progression, byfollowing changes in the metabolic peaks over the time courseof the treatment.”
Currently, magnetic resonance imaging with contrast materialis the gold standard for assessing treatment efficacy in centralnervous system cancers. However, it may underestimate the trueextent of a tumor; in some studies, abnormal magnetic reso-nance spectroscopy findings have been detected outside of con-trast-enhanced tumor boundaries delineated by standard imag-ing. In addition, magnetic resonance imaging is relatively insen-sitive in distinguishing recurrent tumor from normal postopera-tive changes (ie, edema or radiation-induced necrosis). Thus,NewYork-Presbyterian Hospital researchers believe magneticresonance spectroscopy may enhance the clinical decision-mak-
ing ability of physicians.“By evaluating metabolite levels and anatomical structure, it
can provide information on whether or not a tumor is activelymetabolizing,” said Dr. Balmaceda.
Magnetic resonance spectroscopy can predict tumor change—prior to change evident on magnetic resonance imaging—inglioma patients treated with chemotherapy. They also found thatan increase in a specific metabolic ratio seen on magnetic reso-nance spectroscopy, was a significant predictor of poor outcome.
Dr. Balmaceda helped plan a clinical trial that will be the firstto use magnetic resonance spectroscopy to evaluate response toGliadel wafer implantation, in malignant glioma patients.Magnetic resonance spectroscopy will be used as a primary indi-cator of therapeutic response to Gliadel in patients with newlydiagnosed high-grade malignant glioma. Patients will be evalu-ated with magnetic resonance imaging and magnetic resonancespectroscopy at 21 days and 12 weeks after Gliadel insertion,with follow-up continuing until disease progression or death.
“In the past, the focus has been on what’s going on in thetumor, not in the area where the tumor has been removed,”said Susan Pannullo, MD. “We want to figure out what’sgoing on in the area around where the tumor was taken out,and see what we can do to prevent it from coming back.”
Clinical studies suggest that Gliadel may improve survival insome early-stage glioma patients. Now, the results of magneticresonance spectroscopy studies may help determine specificallywhich patients may benefit from this particular therapy.
This is not the first time NewYork-Presbyterian Hospital
New Technologies for Evaluating Tumor ResponseNeuroscienceN E W Y O R K – P R E S B Y T E R I A N
Magnetic resonance spectroscopy has been proven successful atconsistently identifying metabolic changes in cerebral tumors.Further, the efficacy of different types of therapy could potentiallybe evaluated based on metabolite changes seen with magneticresonance spectroscopy.
Direct Infusion Brain Tumor Chemotherapy
“In the past, the focus has been on what’sgoing on in the tumor, not in the area where thetumor has been removed.”
—Susan Pannullo, MD

7
areas of the brain can be treated inwhich surgery would be ineffective.Many conditions that were once con-sidered inoperable can now be treatedwithout an incision and with little or nopain. Indications include primary braintumors, such as glioblastomas, benignbrain tumors, such as meningiomas, andtumors involving other areas of the cen-tral nervous system, such as acousticneuromas. The modality is particularlyuseful for patients with tumors that arenot amenable to open surgery, patientsfor whom surgery is contraindicatedbecause they have comorbid conditionsor are taking specific medications, andthose who simply are unwilling toundergo an open procedure. “It is anexcellent treatment modality for brainmetastases, allowing cancer patients tomove on quickly to treatment of theirsystemic disease,” said Susan Pannullo,MD. Arteriovenous malformations(AVMs) and trigeminal neuralgia canalso be treated successfully in selectedpatients. The uses of the Gamma Knifeare expanding further. Gamma Knife
surgery is being investigated byNewYork-Presbyterian Hospitalresearchers as an alternative to conven-tional epilepsy surgery. In addition, themodality may one day prove useful totreat obsessive compulsive disorder,chronic pain syndromes, obesity, andother disorders.
At the initial consult, the radiationoncologist and/or neurosurgeon deter-mines whether Gamma Knife treatmentis appropriate for the patient. A regis-tered nurse reviews the procedure withthe patient and provides a tour of theunit. The patient also meets theGamma Knife staff and is given theopportunity to ask questions before theactual treatment date.
Patients undergoing treatment arefirst fitted with a stereotactic headframe, which allows precise localizationof the tumor or other target. Then,imaging is performed to determine thesize and position of the abnormality.With this data, the multidisciplinaryteam plans the treatment, including thetarget area and the radiation dosage tobe administered.
The patient’s head, still secured in thestereotactic head frame, is positioned ina collimator helmet, which directs radi-ation to predetermined points in thebrain. The patient is then slid into alarge, shielded sphere containing thesource of radiation. A series of short
investigators have evaluated magneticresonance spectroscopy for centralnervous system tumor progression andresponse to therapy. One recent studyincluded malignant glioma patientsreceiving temozolomide chemotherapy.Investigators, including Dr. Balmaceda,Dr. Pannullo, and Dr. De La Paz,found that magnetic resonance spec-troscopy may be complementary tomagnetic resonance imaging; for exam-ple, in one patient, magnetic resonanceimaging remained stable over time,while magnetic resonance spectroscopyrevealed improvement in regions ofinterest. Now, Robert De La Paz, MD,in collaboration with neurosurgeonJeffrey Bruce, MD, plans to use mag-netic resonance spectroscopy to evalu-ate infusion of topotecan chemotherapy
directly to the brain tumor.“The rationale is that we can deliver a
higher dose of chemotherapy to thetumor, while limiting its effect on thenormal brain,” Dr. De La Paz said.
Investigators are also looking at longer-term response to therapy in braintumors, using magnetic resonance spec-troscopy. In one recent group of patients,increased lactate was thought to be anearly predictor of tumor recurrence ortreatment failure.
Casilda Balmaceda, MD, is AssistantAttending Neurologist, Neurology Serviceat NewYork-Presbyterian Hospital/Columbia University Medical Center, andis Assistant Professor of Neurology,Columbia University College of Physicians& Surgeons.E-mail: [email protected].
Robert De La Paz, MD, is Director ofNeuroradiology at NewYork-PresbyterianHospital/Columbia University MedicalCenter, and is Professor of Radiology atColumbia University College of Physicians &Surgeons. E-mail: [email protected].
Susan Pannullo, MD, is Director of Neuro-Oncology in the Department of NeurologicalSurgery at NewYork-Presbyterian Hospital/Weill Cornell Medical Center, and isAssistant Professor of Neurological Surgery atWeill Medical College of Cornell University.E-mail: [email protected]
Pina C. Sanelli, MD, is Assistant AttendingPhysician at NewYork-PresbyterianHospital/Weill Cornell Medical Center, andis Assistant Professor of Radiology,Neuroradiology Division at Weill MedicalCollege of Cornell University.E-mail: [email protected].
Gamma Knifecontinued from page 1
“Our commitment is to provide all the possibilities of modernmedicine to help our patients. Through close, personalattention to individual patient needs, we have created anenvironment dedicated to providing complete supportive careand promoting optimum healing.”
— Michael Sisti, MD
see Gamma Knife, page 8

Nonprofit Org.U.S. Postage Paid
Permit No. 117
New York, NY
NewYork-Presbyterian Hospital425 East 61st StreetNew York, NY 10021
Important news from
the NewYork-
Presbyterian
Neuroscience
Centers—current
research projects,
clinical trials, and
advances in the
diagnosis, treatment,
and rehabilitation of
neurologic disease.
SERVICE LINE ADMINISTRATOR: Richard Fenton, 627 West 165th Street, New York, NY 10032, 212.305.1389 E-mail: [email protected]
exposures (approximately 10 minuteseach) are applied with little or no dis-comfort to the patient, who can typical-ly go home the same day.
Gamma Knife surgery is notappropriate for every neurosurgerypatient and every indication. ThusNewYork-Presbyterian Hospital hasadopted a multidisciplinary, multi-modality approach to patient care.“Whereas most hospitals have eitherGamma Knife or linear acceleratorradiosurgery, we have both options,”said Michael Sisti, MD.
The Gamma Knife technology canprovide outstanding results in a widevariety of indications. However, the
technology is “the means and not theend” of efforts taken to improvepatients’ lives, according to Dr. Sisti.
"We remain dedicated to the beliefthat the quality of the physician-patientrelationship defines the excellence ofcare we wish to practice," he said. "Ourcommitment is to provide all the possi-bilities of modern medicine to help ourpatients. Through close, personal atten-tion to individual patient needs, wehave created an environment dedicatedto providing complete supportive careand promoting optimum healing."
Steven Isaacson, MD, is Co-Director ofthe Center for Radiosurgery, Department ofRadiation Oncology, at NewYork-Presbyterian Hospital/Columbia UniversityMedical Center, and is Associate Professorof Clinical Radiation Oncology and Clinical
Otolaryngology at Columbia UniversityCollege of Physicians & Surgeons.E-mail: [email protected].
Susan Pannullo, MD, is Director of Neuro-oncology, Department of NeurologicalSurgery, at NewYork-Presbyterian Hospital/Weill Cornell Medical Center, and isAssistant Professor of Neurological Surgeryat Weill Medical College of CornellUniversity.E-mail: [email protected].
Michael B. Sisti, MD, is Co-Director, theCenter for Radiosurgery, Department ofNeurological Surgery, at NewYork-Presbyterian Hospital/Columbia UniversityMedical Center, and is Assistant Professorof Neurological Surgery, ColumbiaUniversity College of Physicians &Surgeons. E-mail: [email protected].
neuro
scie
nce
NE
WY
OR
K–
PR
ES
BY
TE
RI
AN
Gamma Knifecontinued from page 7


















