Evolving Strategies in HIV Diagnosis and Treatment
60
Evolving Evolving Strategies in HIV Strategies in HIV Diagnosis and Diagnosis and Treatment Treatment Rob Smith Rob Smith September 27,2013 September 27,2013
description
Evolving Strategies in HIV Diagnosis and Treatment. Rob Smith September 27,2013. Current Success Rate for cART. Undetectable viral load in 85% of treated patients Reasons for treatment failure: adherence (co-morbidities), access, drug resistance (
Transcript of Evolving Strategies in HIV Diagnosis and Treatment

Evolving Strategies in Evolving Strategies in HIV Diagnosis and HIV Diagnosis and
TreatmentTreatment
Rob SmithRob Smith
September 27,2013September 27,2013




Current Success Rate for cARTCurrent Success Rate for cART
Undetectable viral load in 85% of Undetectable viral load in 85% of treated patientstreated patients
Reasons for treatment failure: Reasons for treatment failure: adherence (co-morbidities), access, adherence (co-morbidities), access, drug resistance (<5% of pts)drug resistance (<5% of pts)
Not all treated patients achieve Not all treated patients achieve immune reconstitution (especially if immune reconstitution (especially if CD4 nadir <200)CD4 nadir <200)

NEJM Mar., 2010

HIV Stats in the USHIV Stats in the US
50,000 new cases/yr; 18,000 50,000 new cases/yr; 18,000 deaths/yrdeaths/yr
20-30% do not know HIV status20-30% do not know HIV status These 20% account for ½ of new These 20% account for ½ of new
casescases By 2015, ½ of all HIV cases will be By 2015, ½ of all HIV cases will be
>50 yo>50 yo

HIV in MaineHIV in Maine 1800 HIV positive; prevalence 0.1%1800 HIV positive; prevalence 0.1% 300-500 do not know their HIV status 300-500 do not know their HIV status 50 new cases per year; >50% “late 50 new cases per year; >50% “late
stage”stage” 60% MSM; 10% hetero w known 60% MSM; 10% hetero w known
positive partner; 16% hetero w/o positive partner; 16% hetero w/o known at risk partner; 12% IVDUknown at risk partner; 12% IVDU

Why Do We Still See AIDS in the Why Do We Still See AIDS in the US?US?
““Late testers”: 30-40% present with AIDS Late testers”: 30-40% present with AIDS or develop in one year –this is true in or develop in one year –this is true in Maine as well as nationally (NEJM Maine as well as nationally (NEJM 2006;354:438).2006;354:438).
Retention in care, adherence to medsRetention in care, adherence to meds
(Psychiatric disease, substance use, other (Psychiatric disease, substance use, other barriers to ongoing treatment—CID barriers to ongoing treatment—CID 2007:44:1493)2007:44:1493)

CID Sept. 15, 2010

Recent MMC CaseRecent MMC Case
50 yo man seen in MMC ER w 50 yo man seen in MMC ER w “difficulty breathing”. “difficulty breathing”.
Evaluated w BMP, CXR (“interstitial Evaluated w BMP, CXR (“interstitial infiltrates”). Rx albuterol.infiltrates”). Rx albuterol.
3 wks later: Admit to MMC - hypoxic. 3 wks later: Admit to MMC - hypoxic. Relevant Hx: 25 lb weight loss since Relevant Hx: 25 lb weight loss since
Jan; cough x 3-4 months. Single Jan; cough x 3-4 months. Single male. Not currently sexually active.male. Not currently sexually active.


Exam: thrush; oral hairy leucoplakia; Exam: thrush; oral hairy leucoplakia; circular dermatophytic rash in axilla.circular dermatophytic rash in axilla.
CT: bilat ground glass opacities in CT: bilat ground glass opacities in upper and lower lobesupper and lower lobes
BAL: Pneumocystis; CMVBAL: Pneumocystis; CMV HIV VL 200,000; CD4 45HIV VL 200,000; CD4 45

Another Recent MMC CaseAnother Recent MMC Case
55 yo married man with fatigue, weight loss, 55 yo married man with fatigue, weight loss, intermittent fever x 6 months. Rx for “chronic intermittent fever x 6 months. Rx for “chronic Lyme” with 3 months oral doxycycline.Lyme” with 3 months oral doxycycline.
Refer to dermatology for Rx psoriasis with Refer to dermatology for Rx psoriasis with topical steroidstopical steroids
Refer to surgery for rectal fissureRefer to surgery for rectal fissure Develops right facial droop, arm weakness; Develops right facial droop, arm weakness;
thalamic brain mass on CT scan--?tumor. thalamic brain mass on CT scan--?tumor. Admit to MMC.Admit to MMC.
HIV positive; CD4 40HIV positive; CD4 40

Newer Testing StrategiesNewer Testing Strategies CDC proposals (2006): CDC proposals (2006): Routine testing on adults (13-64)Routine testing on adults (13-64) Annual testing in those at riskAnnual testing in those at risk Pregnancy, contemplated pregnancyPregnancy, contemplated pregnancy “ “Opt out provision”; implied consentOpt out provision”; implied consent Rapid Diagnostic Tests: 6 approvedRapid Diagnostic Tests: 6 approved “ “Point of care”Point of care” Home testingHome testing Confirm Positives!Confirm Positives! (NEJM 2006;354:438;PLOS ONE (NEJM 2006;354:438;PLOS ONE
2012 ;7(9): e44417)2012 ;7(9): e44417)

Maine HIV Testing Law 2007Maine HIV Testing Law 2007 Changes in state law:Changes in state law: No pre-test counseling requiredNo pre-test counseling required No written informed consent…..BUTNo written informed consent…..BUT Does requireDoes require “ “A patient must be informed orally or in writing A patient must be informed orally or in writing
that an HIV test will be performed unless (they) that an HIV test will be performed unless (they) decline”decline”
“ “Information must include an explanation of Information must include an explanation of what an HIV infection involves, and the meaning what an HIV infection involves, and the meaning of positive and negative test results”of positive and negative test results”
“ “If a test is positive, post-test counseling must If a test is positive, post-test counseling must be provided”be provided”

Barriers to Routine HIV TestingBarriers to Routine HIV Testing
Lack of knowledge of CDC Lack of knowledge of CDC recommendationsrecommendations
USPHT DID not endorse –DOES as of USPHT DID not endorse –DOES as of 20132013
Assumptions re: patient risk Assumptions re: patient risk Low priority—lack of timeLow priority—lack of time Uncertainty re: informed consent lawUncertainty re: informed consent law

Traditional Diagnostic Tests-HIV 1Traditional Diagnostic Tests-HIV 1
ELISA plus Western BlotELISA plus Western Blot Sensitivity: 99.5% post 3 months Sensitivity: 99.5% post 3 months
diseasedisease
Specificity: 99.99%Specificity: 99.99%
False negatives: Window period; False negatives: Window period; agammaglobulinemia; SubType O,Nagammaglobulinemia; SubType O,N
False Positives: “autoantibodies”False Positives: “autoantibodies”

New HIV Diagnostic Algorithm-New HIV Diagnostic Algorithm-20122012
HIV 1/2 Immunoassay screen (includes HIV 1/2 Immunoassay screen (includes antibody screen and p24 antigen)antibody screen and p24 antigen)
If positive, reflex to Multispot (HIV 1 vs 2 If positive, reflex to Multispot (HIV 1 vs 2 assay) and HIV RNA (viral load)assay) and HIV RNA (viral load)
If initial screen is negative, no additional If initial screen is negative, no additional testing UNLESS clinical concern of acute testing UNLESS clinical concern of acute HIV disease; in this event, do HIV RNAHIV disease; in this event, do HIV RNA
Adapted from CLSI consensus guideline Adapted from CLSI consensus guideline (June 2011)(June 2011)

HPIHPI
22 y.o. female with no hx illness who experienced 22 y.o. female with no hx illness who experienced HA and fever 1 week after returning from HA and fever 1 week after returning from vacation to resort in Caribbean. Symptoms vacation to resort in Caribbean. Symptoms progressed to severe fatigue and fainting.progressed to severe fatigue and fainting.
9/19 went to ER. Febrile with UA showing 3-5 9/19 went to ER. Febrile with UA showing 3-5 WBC. Diagnosed with UTI and given ciprofloxacin.WBC. Diagnosed with UTI and given ciprofloxacin.
9/22 back to ER for worsening dizziness, fever, 9/22 back to ER for worsening dizziness, fever, HA, fatigue. WBC 4.8 with 29% bands. Monospot HA, fatigue. WBC 4.8 with 29% bands. Monospot negative. Given IV hydration and sent home for negative. Given IV hydration and sent home for unspecified viral illness.unspecified viral illness.

HPI continuedHPI continued 9/24 Returned to ER. Fever, fatigue, dizziness, new 9/24 Returned to ER. Fever, fatigue, dizziness, new
right inguinal LAD, dry cough and mild diarrhea. right inguinal LAD, dry cough and mild diarrhea. Febrile to 101.4, marked orthostatic hypotension. Febrile to 101.4, marked orthostatic hypotension. WBC 2.6, platelets 105, CRP 3, CMP WNLWBC 2.6, platelets 105, CRP 3, CMP WNL
Admitted to an outside hospital with ? PID versus Admitted to an outside hospital with ? PID versus
Lyme. ID and Gyn consulted and started on empiric Lyme. ID and Gyn consulted and started on empiric Piperacillin/Tazobactam and Doxycycline.Piperacillin/Tazobactam and Doxycycline.
Exam unremarkable --- ultrasound with 2 cm Exam unremarkable --- ultrasound with 2 cm inguinal node. CT abd/pelvis negative except a inguinal node. CT abd/pelvis negative except a question of inflammation in the right inguinal node. question of inflammation in the right inguinal node. Cardiac echo negative. CXR LLL infiltrate versus Cardiac echo negative. CXR LLL infiltrate versus atelectasis.atelectasis.

HPI continuedHPI continued Further workup revealed:Further workup revealed:
• Erhlichia serology negativeErhlichia serology negative• Lyme ELISA equivocalLyme ELISA equivocal• Rapid strep negativeRapid strep negative• HIV ELISA (antibody) test negativeHIV ELISA (antibody) test negative• VDRL negativeVDRL negative• C-diff and cryptosporidium negativeC-diff and cryptosporidium negative• Chlamydia swab positiveChlamydia swab positive• Blood, stool, and urine cultures showed no growth.Blood, stool, and urine cultures showed no growth.
WBC and platelet count improved and sent home WBC and platelet count improved and sent home 9/27 to complete a 2 week course of doxycycline 9/27 to complete a 2 week course of doxycycline for presumptive chlamydia/LGV, ? atypical PNA, ? for presumptive chlamydia/LGV, ? atypical PNA, ? LymeLyme
Continued to feel lightheaded so saw her family Continued to feel lightheaded so saw her family
physcian on 10/2. Afebrile: WBC 5.6 (21% physcian on 10/2. Afebrile: WBC 5.6 (21% reactive lymphs), HCT 37, plat 354, ALT 69. reactive lymphs), HCT 37, plat 354, ALT 69. Doxycycline extended 3 weeks. ID consulted.Doxycycline extended 3 weeks. ID consulted.

DDx ExpandedDDx Expanded
Hx of unprotected sexual intercourse while on Hx of unprotected sexual intercourse while on vacation. No new findings on exam. Doxycycline vacation. No new findings on exam. Doxycycline discontinued.discontinued.
HIV viral load >750,000 copies/mLHIV viral load >750,000 copies/mL Repeat HIV testing showed + ELISA and Western Repeat HIV testing showed + ELISA and Western
blotblot Pan-sensitive genotypePan-sensitive genotype Pt started on anti-retroviral Rx for “Acute Pt started on anti-retroviral Rx for “Acute
retroviral syndrome’ or “Primary HIV”retroviral syndrome’ or “Primary HIV”

Acute Retroviral Syndrome- Acute Retroviral Syndrome- SymptomsSymptoms
Fever (96%)Fever (96%) Lymphadenopathy Lymphadenopathy
(74%)(74%) Pharyngitis (70%)Pharyngitis (70%) Rash (70%)Rash (70%) Myalgia/arthralgia Myalgia/arthralgia
(54%)(54%)
HeadacheHeadache DiarrheaDiarrhea Nausea and Nausea and
vomitingvomiting HepatosplenomegalHepatosplenomegal
yy Weight lossWeight loss ThrushThrush Neurologic Neurologic
symptomssymptoms

Baseline Tests –HIV DxBaseline Tests –HIV Dx
HIV viral load, CD4 countHIV viral load, CD4 count HIV genotypeHIV genotype CBC, CMP, RPR, Hep B/C serologies, CBC, CMP, RPR, Hep B/C serologies,
RPR, Toxo IgG (if CD4,200)RPR, Toxo IgG (if CD4,200) PPD (>5mm) or IGRA assayPPD (>5mm) or IGRA assay Immunizations: PCV13 (Prevnar) Immunizations: PCV13 (Prevnar)
followed 8 wks later by PPSV23 followed 8 wks later by PPSV23 (Pneumovax); Hep A/B if indicated(Pneumovax); Hep A/B if indicated

OI Prevention Guidelines (CDC OI Prevention Guidelines (CDC 2009)2009)
• CD4<200 (or 14%): PCP—TM/SZ (daily), CD4<200 (or 14%): PCP—TM/SZ (daily), dapsone (+/-pyrimethamine for toxo), dapsone (+/-pyrimethamine for toxo), atovoquone ($$), aerosol pentamidineatovoquone ($$), aerosol pentamidine
• CD4<100: Toxoplasmosis—if seropositive; CD4<100: Toxoplasmosis—if seropositive; tm/sz or dapsone plus tm/sz or dapsone plus pyrimethamine/leucovorinpyrimethamine/leucovorin
• CD4<50: MAI—azithromycin weekly or CD4<50: MAI—azithromycin weekly or clarithromycin dailyclarithromycin daily

Who to Rx: DHHS Guidelines 2012Who to Rx: DHHS Guidelines 2012
Rx recommended for all HIV-infected Rx recommended for all HIV-infected individuals. Strength of individuals. Strength of recommendation varies on the basis recommendation varies on the basis of preRx CD4 count.of preRx CD4 count.
CD4 <350 AICD4 <350 AI CD4 350 to 500 AIICD4 350 to 500 AII CD4 >500 BIII CD4 >500 BIII
A=strong evidence;B=moderateA=strong evidence;B=moderate

Why Rx Everyone with HIVWhy Rx Everyone with HIV
Rx reduces HIV-related events, HIV-Rx reduces HIV-related events, HIV-unrelated events and malignanciesunrelated events and malignancies
(Note that CD4 nadir and “viremia copy (Note that CD4 nadir and “viremia copy years” predict adverse outcomes)years” predict adverse outcomes)
Public health benefit with reduced HIV Public health benefit with reduced HIV transmission (HPTN 052; Nejm 2011)transmission (HPTN 052; Nejm 2011)
Timing may depend on presence of Timing may depend on presence of opportunistic infectionsopportunistic infections
(Inconclusive evidence for “elite (Inconclusive evidence for “elite controllers, long-term non-progressors”)controllers, long-term non-progressors”)

Preferred Regimens (DHHS-2012)Preferred Regimens (DHHS-2012)
Efavirenz/tenofovir/emtricitabineEfavirenz/tenofovir/emtricitabine Ritonavir-boosted atazanavir and Ritonavir-boosted atazanavir and
tenofovir/emtricitabine (“truvada”)tenofovir/emtricitabine (“truvada”) Ritonavir-boosted darunavir and Ritonavir-boosted darunavir and
tenofovir/emtricitabine tenofovir/emtricitabine Raltegravir and tenofovir/emtricitabineRaltegravir and tenofovir/emtricitabine
((http://www.aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf)andAdolescentGL.pdf)

Alternative Regimens Alternative Regimens
Rilpivirine/tenofovir/emtricitabine Rilpivirine/tenofovir/emtricitabine Eltegravir/cobicistat/tdf/ftc Eltegravir/cobicistat/tdf/ftc Lopinavir/r (“Kaletra”)/tdf/ftcLopinavir/r (“Kaletra”)/tdf/ftc May substitute abacavir/lamivudine May substitute abacavir/lamivudine
(“Epzicom”) for (“Epzicom”) for tenofovir/emtricitabine in patients tenofovir/emtricitabine in patients with renal disease, osteoporosiswith renal disease, osteoporosis

Factors to ConsiderFactors to Consider
Underlying drug resistance Underlying drug resistance Potential adverse effects of drugs, drug-Potential adverse effects of drugs, drug-
drug interactionsdrug interactions Pregnancy or significant child bearing Pregnancy or significant child bearing
potentialpotential Co-morbid conditions (Hepatitis B/C, Co-morbid conditions (Hepatitis B/C,
psychiatric, substance abuse)psychiatric, substance abuse) Post-menopausal women or other risk Post-menopausal women or other risk
osteoporosisosteoporosis ConvenienceConvenience

Always check for drug resistance Always check for drug resistance firstfirst
HIV genotype for everyone, as a HIV genotype for everyone, as a baseline and if there is viral baseline and if there is viral breakthrough (>500 copies HIV)breakthrough (>500 copies HIV)
If treatment is failing, obtain If treatment is failing, obtain genotype while on their regimen to genotype while on their regimen to detect resistance mutationsdetect resistance mutations
HIV phenotype for known or HIV phenotype for known or suspected complex drug resistance suspected complex drug resistance mutation patterns ($$)mutation patterns ($$)

Management of HIV (DHHS 2011)Management of HIV (DHHS 2011)
Goal is “undetectable” (<48 Goal is “undetectable” (<48 copies/mL) HIV viral load (Assays copies/mL) HIV viral load (Assays vary on limit of detection from <75 vary on limit of detection from <75 to <20 copies/mL) to <20 copies/mL)
Monitor the HIV viral load q 3 months Monitor the HIV viral load q 3 months once goal is achievedonce goal is achieved
CD4 counts can be repeated q 6-12 CD4 counts can be repeated q 6-12 months if viral load controlledmonths if viral load controlled

Continue to Monitor For…Continue to Monitor For…
New STDs (annual RPR/syphilis New STDs (annual RPR/syphilis screen)screen)
New onset Hep C (annual)New onset Hep C (annual) TB (Risk dependent on community TB (Risk dependent on community
context)context) Metabolic disorders—ie fasting Metabolic disorders—ie fasting
glucose, lipids; creatinine and glucose, lipids; creatinine and urinalysis; testosterone in urinalysis; testosterone in symptomatic males; ?bone densitysymptomatic males; ?bone density

Be Aware of….Be Aware of….
Increased CAD riskIncreased CAD risk Increased risk for liver disease (fatty Increased risk for liver disease (fatty
liver)liver) Increased risk for renal diseaseIncreased risk for renal disease Neuro-cognitive disorders-10x Neuro-cognitive disorders-10x
reduction in HIV dementia with ARVs, reduction in HIV dementia with ARVs, but ?increased risk over timebut ?increased risk over time
AIDS (lymphoma, cervical) and Non-AIDS (lymphoma, cervical) and Non-AIDS malignancies (anal, lung, liver)—AIDS malignancies (anal, lung, liver)—related to CD4related to CD4

NEJM 352:1 January 6, 2005

Post-Exposure ProphylaxisPost-Exposure Prophylaxis
Occupational—CDC algorithm; UCSF Occupational—CDC algorithm; UCSF PEPline (888-448-4911 or PEPline (888-448-4911 or www.nccc.ucsf.edu/Hotlines/PEPline.html); www.nccc.ucsf.edu/Hotlines/PEPline.html); risk if needlestick exposure to an HIV risk if needlestick exposure to an HIV infected pt=0.33%; if mucosal, 0.09% riskinfected pt=0.33%; if mucosal, 0.09% risk
Needlestick risk factors: index patient Needlestick risk factors: index patient status; hollow vs solid needle; visible status; hollow vs solid needle; visible blood; deep puncture; needle into vesselblood; deep puncture; needle into vessel
Treat ASAP (within 2 hours if possible)Treat ASAP (within 2 hours if possible) Risk reduction of 80%Risk reduction of 80%

Post-Exposure Prophylaxis: Non-Post-Exposure Prophylaxis: Non-OccupationalOccupational
CDC recommends nPEP if:CDC recommends nPEP if: ““Substantial risk of exposure w/in 72 Substantial risk of exposure w/in 72
hrs”hrs” Mucosal or non-intact skin exposed to Mucosal or non-intact skin exposed to
“body fluids” (not saliva, urine etc “body fluids” (not saliva, urine etc unless visibly contaminated w blood) unless visibly contaminated w blood) from known HIV source from known HIV source
Case by case if HIV status unknownCase by case if HIV status unknown Should not be used as a frequent Should not be used as a frequent
intervention for any one patientintervention for any one patient

PEP:Choice of MedsPEP:Choice of Meds
New recommendations (2013): New recommendations (2013): truvada plus raltegravir (well truvada plus raltegravir (well tolerated—J AIDS 2012)tolerated—J AIDS 2012)
If source pts viral resistance pattern If source pts viral resistance pattern is known, choose effective is known, choose effective alternatives alternatives
Do not use abacavir/3TCDo not use abacavir/3TC 28d course of treatment28d course of treatment

Pre-Exposure Prophylaxis Pre-Exposure Prophylaxis (“PrePEP”)?(“PrePEP”)?
Effectiveness demonstrated in MSM trial: Effectiveness demonstrated in MSM trial: 44% overall, 73% if adherent; 66% in 44% overall, 73% if adherent; 66% in heterosexual femalesheterosexual females
Cost effective (<$100K per QALY)—but Cost effective (<$100K per QALY)—but could result in annual expenditures of $4 could result in annual expenditures of $4 billion (Ann Intern Med 2012; 156: 541)billion (Ann Intern Med 2012; 156: 541)
Concerns: How to stratify risk; who pays; Concerns: How to stratify risk; who pays; drug resistance; long term risks of Rxdrug resistance; long term risks of Rx
CDC interim guidelines for MSM (2011), CDC interim guidelines for MSM (2011), heterosexuals at high risk (2012); IVDUheterosexuals at high risk (2012); IVDU

Real or Functional Cures?Real or Functional Cures?
Berlin patient: stem cell transplant; Berlin patient: stem cell transplant; donor was CCR5 mutation donor was CCR5 mutation homozygous—off ARV x 5yrshomozygous—off ARV x 5yrs
Activate resting memory cells with Activate resting memory cells with latent infection and Rx? Use of latent infection and Rx? Use of vorinostat (Nature 2012; 487: 482)vorinostat (Nature 2012; 487: 482)

ResourcesResources
Primary Care Guidelines (IDSA-2009)Primary Care Guidelines (IDSA-2009)
CID 2009; 49: 651-681.CID 2009; 49: 651-681. Pregnancy: Pregnancy:
http://aidsinfo.nih.gov/guidelines Opportunistic Infections:Opportunistic Infections:
http://aidsinfo.nih.gov/guidelines Occupational ExposureOccupational Exposure
http://www.cdc.gov/mmwr
PEPline: 1-888-448-4911PEPline: 1-888-448-4911



How to Treat HIVHow to Treat HIV
Preferred Regimens—Treatment Preferred Regimens—Treatment Naïve (DHHS 01/10/2011)Naïve (DHHS 01/10/2011)
Efavirenz plus tenofovir/emtricitabineEfavirenz plus tenofovir/emtricitabine
Atazanavir/r plus sameAtazanavir/r plus same
Darunavir/r plus sameDarunavir/r plus same
Raltegravir plus sameRaltegravir plus same

HIV in Refugee PopulationsHIV in Refugee Populations Less likely to start ARV therapyLess likely to start ARV therapy Similar CD4 at time of presentationSimilar CD4 at time of presentation Higher likelihood co-infection with latent TB, Higher likelihood co-infection with latent TB,
Hepatitis BHepatitis B Higher prevalence of a mental health disorder Higher prevalence of a mental health disorder
(especially PTSD)(especially PTSD) Acquisition by heterosexual exposure rather than Acquisition by heterosexual exposure rather than
IVDU or MSMIVDU or MSM
Beckwith et al; 2009;13:186. Internat J Inf Dis.Beckwith et al; 2009;13:186. Internat J Inf Dis.



Science Vol. 332 May 13, 2011

Science Vol. 333 July 1, 2011

Prevention of HIV InfectionPrevention of HIV Infection
Reduce high risk behaviors: Reduce high risk behaviors: education re: safer sex, clean education re: safer sex, clean needles (needle exchange programs)needles (needle exchange programs)
Pre and post-exposure chemo-Pre and post-exposure chemo-prophylaxisprophylaxis
““Test and treat”—lower the Test and treat”—lower the “community viral load”“community viral load”

“ “It has also become clear that It has also become clear that finding the cause of an infectious finding the cause of an infectious disease is the alpha but not the disease is the alpha but not the omega of its eradication.”omega of its eradication.”
R.C. Gallo MD and Luc Montagnier MDR.C. Gallo MD and Luc Montagnier MD
(“The Discovery of HIV as the Cause of (“The Discovery of HIV as the Cause of AIDS”, NEJM 2003; 349: 24)AIDS”, NEJM 2003; 349: 24)

““Test and Treat”?Test and Treat”?
More effective identification of HIV More effective identification of HIV positives—can be targeted to higher positives—can be targeted to higher risk groupsrisk groups
Lower “community viral load” leads Lower “community viral load” leads to lower high transmissionto lower high transmission
Models: San Fran--MSM (CID 2011); Models: San Fran--MSM (CID 2011); DC--community (“modest impact on DC--community (“modest impact on HIV transmission”-CID 2010)HIV transmission”-CID 2010)

Rapid HIV Testing in the ERRapid HIV Testing in the ER
N=849 adults –oral test –OraquickN=849 adults –oral test –Oraquick Brigham and Women’s Hospital ERBrigham and Women’s Hospital ER 39 with positive results: 5 positive on 39 with positive results: 5 positive on
confirmation…26 non-infected (8 declined)confirmation…26 non-infected (8 declined) 8-30 fold increased odds of HIV with 8-30 fold increased odds of HIV with
positive test, but specificity less than positive test, but specificity less than predicted (Ann Int Med 2008; 149: predicted (Ann Int Med 2008; 149: 153-160)153-160)
Increased false positives as kits near Increased false positives as kits near expiration date (PLOS ONE; 2009)expiration date (PLOS ONE; 2009)

NEJM Mar. 18, 2010

NEJM April 10, 2008

Timing of HIV Rx in Pts with Timing of HIV Rx in Pts with Opportunistic InfectionsOpportunistic Infections
Medication reactions and interactionsMedication reactions and interactions
(ie 2/3 pts with PCP may develop (ie 2/3 pts with PCP may develop rash with TM/SZ)rash with TM/SZ)
““IRIS” reactions:IRIS” reactions:
In general, start within 2 wks in pts In general, start within 2 wks in pts with AIDS…exceptions include TB in with AIDS…exceptions include TB in patients with CD4>200; cryptococcal patients with CD4>200; cryptococcal or TB meningitisor TB meningitis


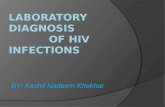
Interpreting HIV SerologyInterpreting HIV Serology
O b ta invira l load
S erocon vers ionsu sp ec ted
O b ta inH IV -2 W B
H IV -2su sp ec ted
R etes t in3 -4 m on th s
L ow riskp a tien t
H IV In d e te rm in a te

New Responses to Old QuestionsNew Responses to Old Questions
How is HIV diagnosed in 2012 (ie How is HIV diagnosed in 2012 (ie there is a new algorithm)there is a new algorithm)
Who should be treated? Who should be treated? What medications should be used and What medications should be used and
what adverse effects might we what adverse effects might we expect? expect?
How is timing of treatment affected by How is timing of treatment affected by presence of opportunistic infections?presence of opportunistic infections?