Evidence-Based Decisions and FA (Clinical) Q’s: Community Acquired Pneumonia John H. Burton, MD...
52
Evidence-Based Evidence-Based Decisions and FA Decisions and FA (Clinical) Q’s: (Clinical) Q’s: Community Acquired Community Acquired Pneumonia Pneumonia John H. Burton, MD John H. Burton, MD Dept. Emergency Medicine Dept. Emergency Medicine Albany Medical Center Albany Medical Center
-
Upload
nigel-milton-richardson -
Category
Documents
-
view
216 -
download
0
Transcript of Evidence-Based Decisions and FA (Clinical) Q’s: Community Acquired Pneumonia John H. Burton, MD...
Evidence-Based Evidence-Based Decisions and FA Decisions and FA
(Clinical) Q’s:(Clinical) Q’s:Community Acquired Community Acquired
PneumoniaPneumoniaJohn H. Burton, MDJohn H. Burton, MD
Dept. Emergency MedicineDept. Emergency Medicine
Albany Medical CenterAlbany Medical Center
Lecturing Lecturing on CAPon CAP
Research Grants:Binax, Medtronic, SciosEMF, NIH
Lecture Sponsorship:20+ Hospitals, Roche,Bristol-Myers Squibb,Pfizer, Bayer, Scios,Aventis

Bronchitis vs CAP?Bronchitis vs CAP?

Bronchitis:Bronchitis:1. URI symptoms: cough, fever, 1. URI symptoms: cough, fever, congestion, +/- sputum production congestion, +/- sputum production (color change…) (color change…) 2. Vast majority are viral..2. Vast majority are viral..3. Don’t treat with antibiotics3. Don’t treat with antibiotics4. Consider beta-agonists (2 studies, 4. Consider beta-agonists (2 studies, weak data) weak data)
CAP: Class I:CAP: Class I:1. URI symptoms: cough, fever, 1. URI symptoms: cough, fever, congestion, +/- sputum production, congestion, +/- sputum production, +CXR+CXR (Class I exception) (Class I exception)2. Treat with antibiotics2. Treat with antibiotics
How should the How should the disposition be disposition be determined in determined in patients with patients with
community acquired community acquired pneumonia?pneumonia?
A Prediction Rule to A Prediction Rule to Identify Low-Risk Identify Low-Risk Patients with CAPPatients with CAPNEJM 1997; 336:243-250.NEJM 1997; 336:243-250.
Develop a prediction rule for Develop a prediction rule for prognosis to identify pts at low risk prognosis to identify pts at low risk of dying within 30 days.of dying within 30 days.
Analysis of data on 14,199 adults Analysis of data on 14,199 adults in a with CAP treated as inpatients. in a with CAP treated as inpatients.
Prediction rule then validated on Prediction rule then validated on database of 38,000 CAP pts.database of 38,000 CAP pts.
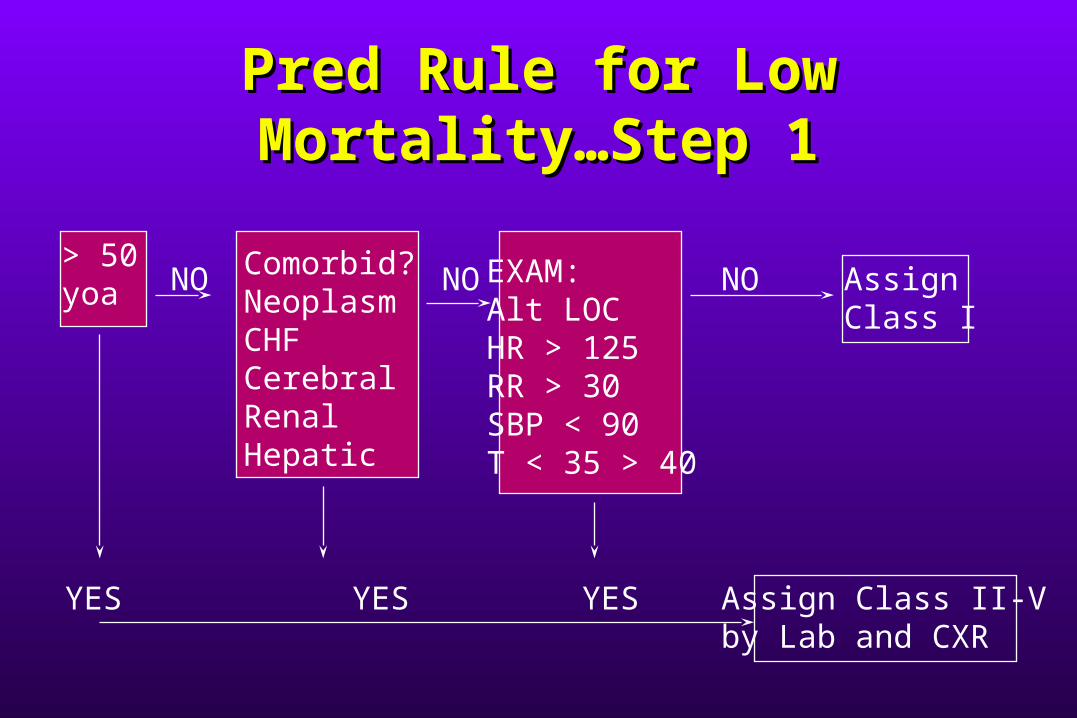
Pred Rule for Low Pred Rule for Low Mortality…Step 1Mortality…Step 1
> 50 yoa
Comorbid?NeoplasmCHFCerebralRenalHepatic
EXAM:Alt LOCHR > 125RR > 30SBP < 90T < 35 > 40
NO NO NO Assign Class I
YES YES YES Assign Class II-Vby Lab and CXR
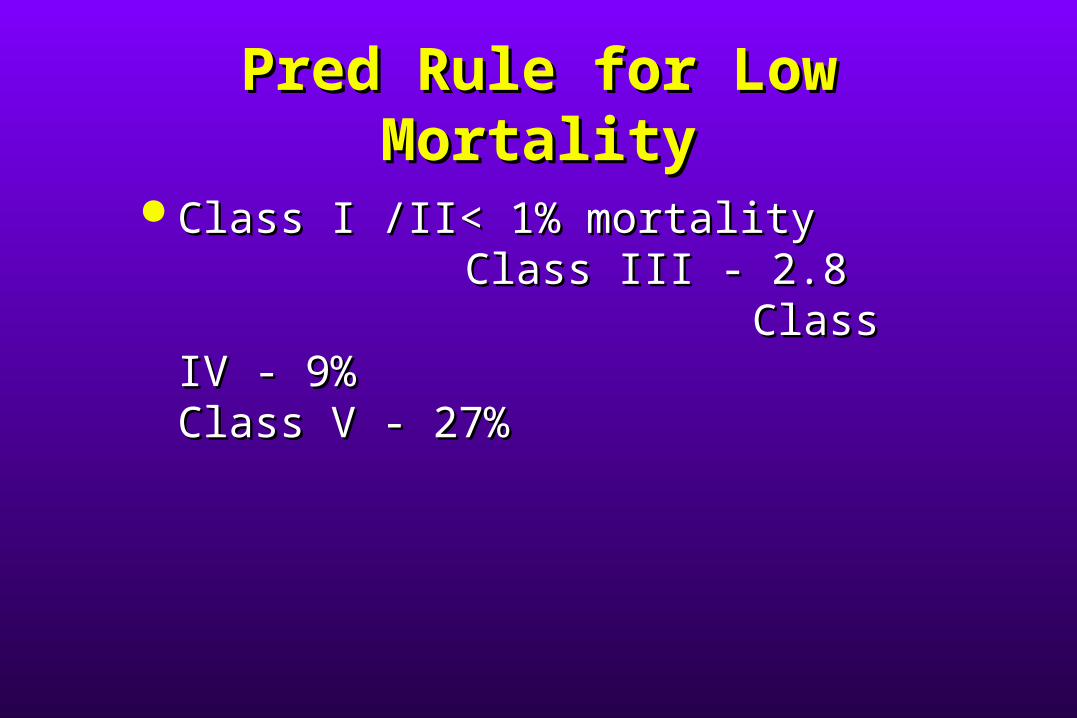
Pred Rule for Low Pred Rule for Low MortalityMortality
Class I /II< 1% mortalityClass I /II< 1% mortalityClass III - 2.8Class III - 2.8
Class IV - 9%Class IV - 9%Class V - 27%Class V - 27%
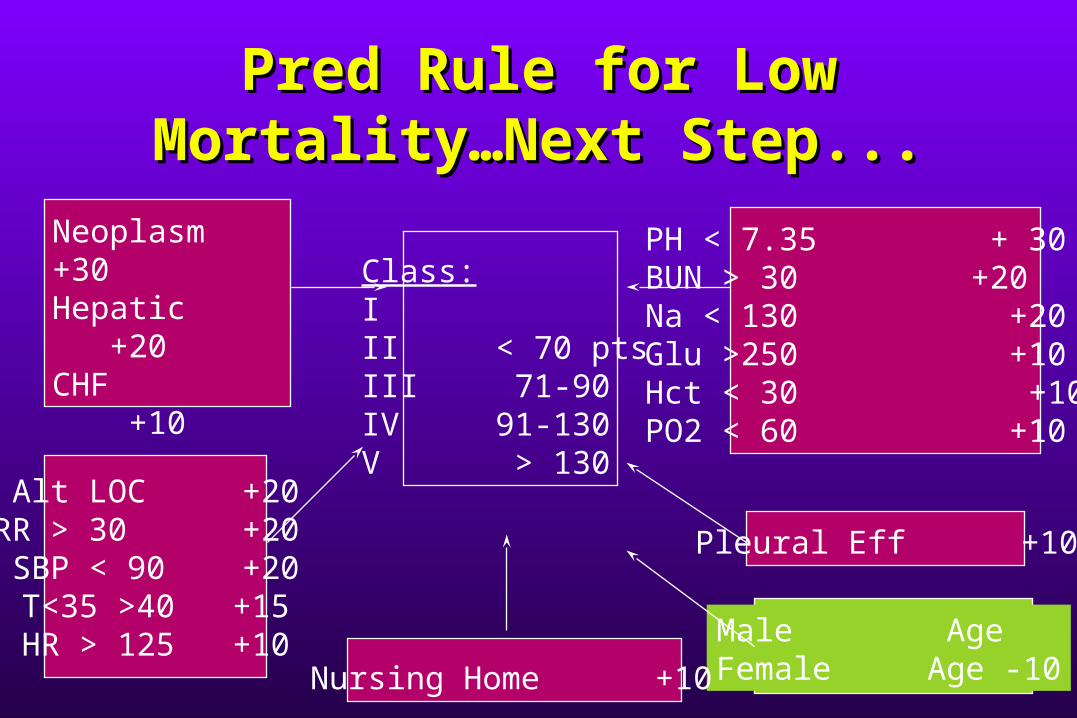
Pred Rule for Low Pred Rule for Low Mortality…Next Step...Mortality…Next Step...
Neoplasm +30 Hepatic +20CHF +10 Cerebral +10 Renal +10
Alt LOC +20RR > 30 +20 SBP < 90 +20T<35 >40 +15 HR > 125 +10
PH < 7.35 + 30BUN > 30 +20Na < 130 +20Glu >250 +10Hct < 30 +10 PO2 < 60 +10
Pleural Eff +10
Male AgeFemale Age -10Nursing Home +10
Class:III < 70 ptsIII 71-90IV 91-130V > 130
What Should I What Should I Prescribe for Prescribe for Outpatients Outpatients
with CAP?with CAP?

How common are How common are “atypicals” in the “atypicals” in the ambulatory CAP ambulatory CAP
population?population?

Community-Acquired Community-Acquired PneumoniaPneumonia
34%
15%
6%
8%
8%
7%
10% 5%7%
S Pneumo
Hflu and MCat
S Aur
Aerobic GNR
Asp/Aner
Legionella
Mycoplasma
Chlamydia
other
Bacterial CausesBacterial Causes
Hosp Form 1994; 29: 122-136
Ambulatory Patients with Ambulatory Patients with CAP: the Freq of Atypical CAP: the Freq of Atypical Agents and Clin CourseAgents and Clin Course
Am J Med 1996; 101:508-515Am J Med 1996; 101:508-515
Prospective cohort from PORTProspective cohort from PORT 149 pts. with respiratory symptoms149 pts. with respiratory symptoms Etiology determined by serum abs Etiology determined by serum abs
for legionella, mycoplasma, for legionella, mycoplasma, chlamydia, viruseschlamydia, viruses

Ambulatory CAP: Ambulatory CAP: atypicalsatypicals
23
14
1 1
8
0
5
10
15
20
25
%
Chlamydia
Mycoplasm
S Pneumo
H Flu
Viruses
74/149 patients = 50% yield
pathogen

Mycoplasma Pneumo and Mycoplasma Pneumo and Chlamydia Pneumo in Chlamydia Pneumo in PedPed CAP: CAP:
efficacy and safety of efficacy and safety of clarithromycin vs. EESclarithromycin vs. EES
Ped Inf Dis 1995; 14:471-477Ped Inf Dis 1995; 14:471-47728 27
1 1
0
5
10
15
20
25
30
%
Chlamydia
Mycoplasm
S Pneumo
H Flu
Multicenter trial with 122 of 260 pts with pos cx or serology

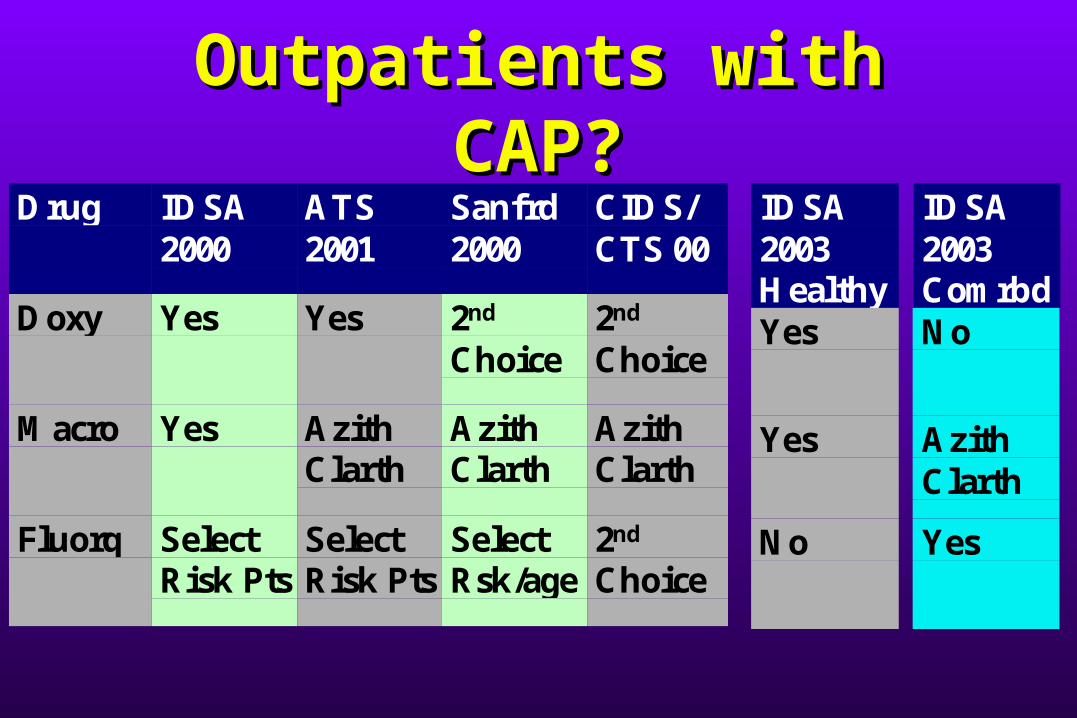
Outpatients with Outpatients with CAP?CAP?
Drug IDSA2000
ATS2001
Sanfrd2000
CIDS/CTS 00
Doxy Yes Yes 2nd
Choice2nd
Choice
Macro Yes AzithClarth
AzithClarth
AzithClarth
Fluorq SelectRisk Pts
SelectRisk Pts
SelectRsk/age
2nd
Choice
IDSA2003HealthyYes
Yes
No
IDSA2003ComrbdNo
AzithClarth
Yes
*Comrbd = copd, ca, chf, dm, renal

Should I Cover Should I Cover Atypical Pathogens in Atypical Pathogens in
Hospitalized Hospitalized Patients?Patients?

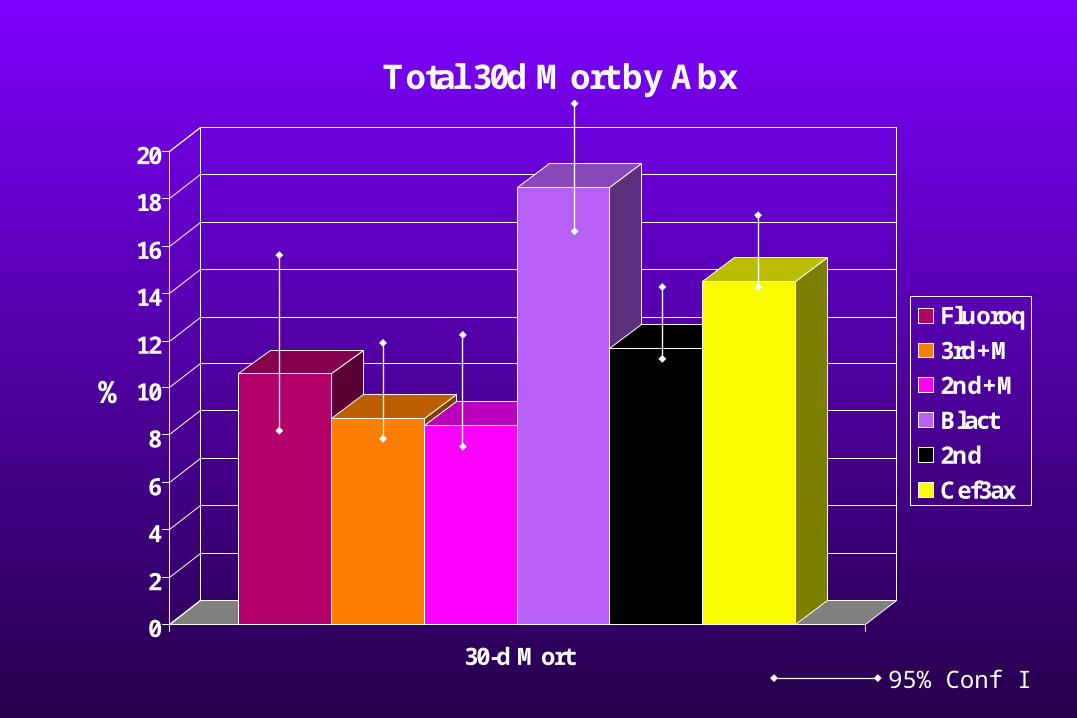
Assoc. Between Initial Assoc. Between Initial Antimicrobial Tx & Med Antimicrobial Tx & Med
Outcomes for Hospitalized Outcomes for Hospitalized Elderly Pts with PneumoniaElderly Pts with Pneumonia
Arch Intern Med 99;159:2562-2572Arch Intern Med 99;159:2562-2572
12,945 eligible pts: 12,945 eligible pts: 9751 from 9751 from
communitycommunity 3194 3194 from long-term facilityfrom long-term facility
Mean age 79 yearsMean age 79 years
0
2
4
6
8
10
12
14
16
18
20
%
30-d Mort
Total 30d Mort by Abx
Fluoroq
3rd+M
2nd+M
Blact
2nd
Cef3ax
95% Conf I

Atypical Pathogens in Atypical Pathogens in Hospitalized Hospitalized
Patients?Patients?YesYes NoNo
IDSA 2000IDSA 2000Sanford 2000 Sanford 2000 ATS 2001ATS 2001CIDS/CTS 2000CIDS/CTS 2000IDSA 2003IDSA 2003
What’s the Deal with What’s the Deal with Macrolide Macrolide
Resistance?Resistance?
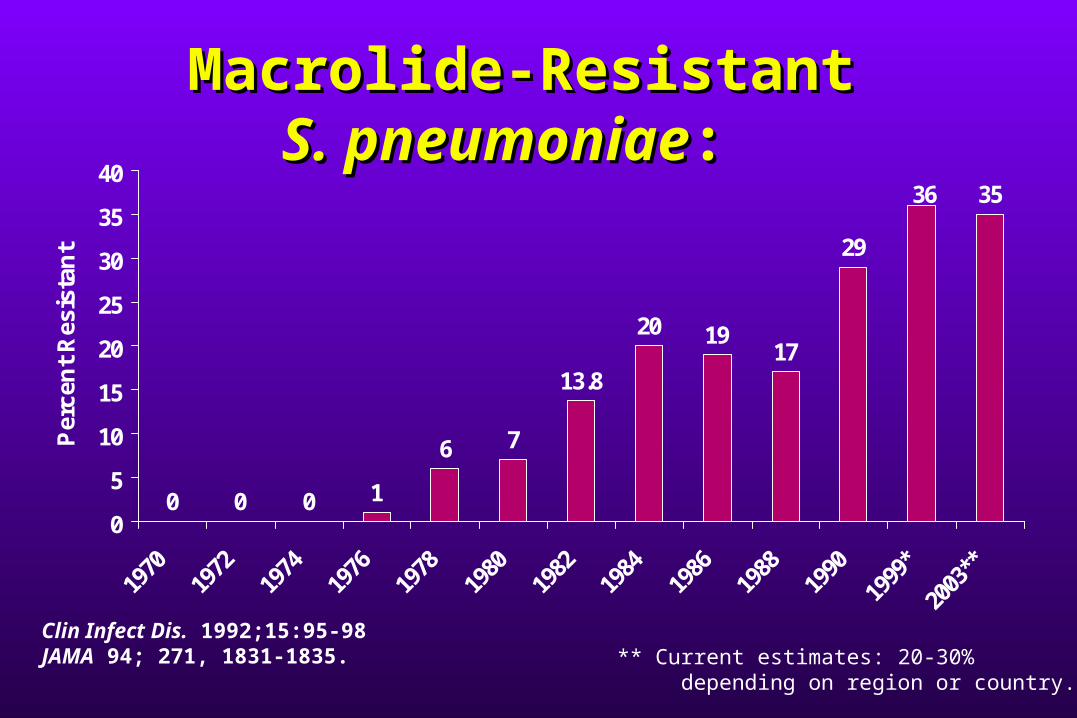
0 0 0 1
6 7
13.8
20 1917
29
3536
0
5
10
15
20
25
30
35
40
Per
cen
t R
esis
tan
t
Clin Infect Dis. 1992;15:95-98JAMA 94; 271, 1831-1835.
Macrolide-Resistant Macrolide-Resistant S. pneumoniaeS. pneumoniae: :
** Current estimates: 20-30% depending on region or country.

Pneumococcal macrolide Pneumococcal macrolide resistance - myth or realityresistance - myth or reality
Jour Antimicrob Chem 1999; 44:1-6Jour Antimicrob Chem 1999; 44:1-6
““Despite the in-vitro resistance trends ….there is Despite the in-vitro resistance trends ….there is a paucity of data indicating resistance trends a paucity of data indicating resistance trends are translating into in vivo clinical failures..it are translating into in vivo clinical failures..it appears the opposite is true.”appears the opposite is true.”Significance of Serum vs Tissue Significance of Serum vs Tissue Levels of Abx in Treatment of Levels of Abx in Treatment of
PRSP & CAPPRSP & CAPChest 1999; 116:535-538Chest 1999; 116:535-538““Clinical results in pneumonia may depend more Clinical results in pneumonia may depend more
on tissue penetration and accumulation in the on tissue penetration and accumulation in the infected lung than on serum levels.”infected lung than on serum levels.”
No correlation of increasing in vitro resistance No correlation of increasing in vitro resistance has been made with mortality outcomes.has been made with mortality outcomes.

Practice Guidelines for the Practice Guidelines for the Management of CAP: IDSA Management of CAP: IDSA
2000 2000 Clin Inf Dis 2000; 31:347-82Clin Inf Dis 2000; 31:347-82
““Cases of macrolide failure have been Cases of macrolide failure have been described anecdotally but have been described anecdotally but have been infrequent so far.”infrequent so far.”
Canadian Guidelines: Canadian Guidelines: CIDS/CTS CIDS/CTS
Clin Inf Dis 2000; 31:383-421Clin Inf Dis 2000; 31:383-421““Very few cases have been reported in Very few cases have been reported in
which ..macrolide resistance has led to which ..macrolide resistance has led to clinical failure or breakthrough bacteremia.”clinical failure or breakthrough bacteremia.”

Update of Practice Guidelines Update of Practice Guidelines for Management of CAP in for Management of CAP in Immunocompetent AdultsImmunocompetent Adults
Clin Inf Disease 2003;37:1405-Clin Inf Disease 2003;37:1405-3333
““S Pneumo resistance in vitro may be deceptive, because S Pneumo resistance in vitro may be deceptive, because the M phenotype may not be clinically relevant, and the M phenotype may not be clinically relevant, and alveolar lining fluid or intracellular levels may be more alveolar lining fluid or intracellular levels may be more important than serum levels used to determine in vitro important than serum levels used to determine in vitro activity.”activity.”

Does the Does the fluoroquinolone fluoroquinolone choice make a choice make a
difference?difference?
Generations of Generations of
FluoroquinolonesFluoroquinolones
1st: Nalidixic Acid1st: Nalidixic Acid 2nd: Cipro/Ofloxacin2nd: Cipro/Ofloxacin 3rd: Levofloxacin3rd: Levofloxacin 4th: Gatifloxacin, Moxiflox4th: Gatifloxacin, Moxiflox
(improved Gram Pos and (improved Gram Pos and Anaerobe)Anaerobe)

CNSseizures & dizziness(sparfloxacin, trovafloxacinofloxacin)
Taste perversion(grepafloxacin)
GInausea/vomiting(all quinolones)
Liver toxicity(trovafloxacin)
Prolonged QTc interval(grepafloxacin, gatifloxacin, levofloxacin, sparfloxacin, moxifloxacin) Phototoxicity(sparfloxacin, lomefloxacin, clinafloxacin) Arthritis/Tendonitis(all quinolones)
Adverse Events: Adverse Events: QuinolonesQuinolones
Adapted from Fish. Clin Pharmacokinet. 1997;32:101-119. Haria. Drugs. 1997;54:435-446. Goa. Drugs. 1997;53:700-725. Wagstaff. Drugs. 1997;53:817-824. Avelox (moxifloxacin) package insert.

AECBAECB ++ ++ ++
5 day5 day ++ -- ++
CAPCAP ++ ++ + +
Acute SinusitisAcute Sinusitis ++ ++ ++
UTIUTI ++ ++ --
Comp. UTI/PyeloComp. UTI/Pyelo ++ ++ --
Uncomp. Gonorr.Uncomp. Gonorr. ++ -- --
Current Indications and Current Indications and Uses for the Uses for the
FluoroquinolonesFluoroquinolonesGatifloxacinGatifloxacin LevofloxacinLevofloxacinLevofloxacinLevofloxacin MoxifloxacinMoxifloxacinMoxifloxacinMoxifloxacin

What’s the Deal with What’s the Deal with Fluoroquinolone Fluoroquinolone
Resistance?Resistance?
Fluoroquinolone Fluoroquinolone ResistanceResistance
THE BAD NEWSTHE BAD NEWS Resistances to Levoflox have been Resistances to Levoflox have been
reported recently.reported recently. Increasing number of centers are Increasing number of centers are
reserving fluoroquinolones for the reserving fluoroquinolones for the sickest patients and oldest: Umass, sickest patients and oldest: Umass, Brigham, etc...Brigham, etc...

What’s the Deal with What’s the Deal with Fluoroquinolone Fluoroquinolone
Resistance?Resistance?(CDC:Drug-Resistant Strep Pneumo Working Group)(CDC:Drug-Resistant Strep Pneumo Working Group)
Fluoroquinolones Limited to:-Adults who have failed Macrolide,
BLactam-Macrolide combo, or Doxy-Allergy to alternative agents-Documented PRSP infection
Arch Int Med 2000;160:1399-1408.

What’s the Deal with What’s the Deal with Fluoroquinolone Fluoroquinolone
Resistance?Resistance?(JB’s Rules)(JB’s Rules)
You may choose to reserve Fluoroquinolone use:-Increased Age (>70)
-Highest Severity-Risk of PRSP (Nursing home patients)
-Increased Risk: Cardiopulmonary Disease
Give the Best Drugs to the Give the Best Drugs to the Oldest (and Sickest) Folks...Oldest (and Sickest) Folks...
IDSA 2003For Nursing Home Pts
1. Resp Flouroquinln2. Amx/Clv + Az/Clrth

What are cost-What are cost-effective treatment effective treatment
strategies?strategies?

Prestigious Burton Prestigious Burton SurveySurvey2004200410d10d 14d14d
Zmax Zmax 47 (5d)47 (5d)
BiaxinBiaxin8282 114114
DoxyDoxy 1111 1313
LvquinLvquin 9292 128128
GatifloxGatiflox 8585 118118
MoxifloxMoxiflox 91 91 126126
AugmtnAugmtn 113113 155155
Walmart Pharmacy: Falmouth, MEWalmart Pharmacy: Falmouth, ME
Ver Imp Med Jour, 2004

Why Can’t I use Why Can’t I use Doxycycline on Doxycycline on
everyone?everyone?IDSA 2003:IDSA 2003:
“Very limited recent “Very limited recent published clinical data on published clinical data on
CAP, and few clinicians CAP, and few clinicians use it.”use it.”

Why not use Why not use Erythromycin on Erythromycin on
Everyone?Everyone?IDSA 2003:IDSA 2003:
“Erythromycin is poorly “Erythromycin is poorly tolerated and is less tolerated and is less effective against H effective against H
Influenzae.”Influenzae.”

IV CostsIV Costsqdqd
Cefrxime Cefrxime 17.4917.49
Cef3axCef3ax 23.1023.10
Zmax Zmax 18.3618.3628.1728.17 Cef3ax + Azith Cef3ax + Azith (po)(po)
EmycinEmycin 7.807.80
LvquinLvquin 24.83 (Deleted: 2000)24.83 (Deleted: 2000)
GatifloxGatiflox 12.8012.80
MoxifloxMoxiflox 12.8012.80

How long a course of How long a course of therapy?therapy?
1. Until Afebrile for 72 1. Until Afebrile for 72 hours.hours.2. Numerous trials: 7-14 2. Numerous trials: 7-14 days.days.3. No controlled, outcome 3. No controlled, outcome trials. trials. 4. It’s a wash - 10 days.4. It’s a wash - 10 days.

16-Membered Ring16-Membered Ring• SpiramycinSpiramycin
12-Membered Ring12-Membered Ring• MethymycinMethymycin
14-Membered Ring14-Membered Ring 15-Membered Ring15-Membered Ring• AzithromycinAzithromycin
Natural ErythromycinNatural Erythromycin• A, B, C, etcA, B, C, etc
SemisyntheticSemisynthetic• ClarithromycinClarithromycin• DirithromycinDirithromycin• FlurithromycinFlurithromycin• RoxithromycinRoxithromycin
Ketolides (telithromycin)Ketolides (telithromycin)
Bryskier A. Bryskier A. Macrolides: Chemistry, Pharmacology and Clinical Uses. Macrolides: Chemistry, Pharmacology and Clinical Uses. Oxford, England: Blackwell Oxford, England: Blackwell Scientific Publications; 1993.Scientific Publications; 1993.
Are there any new drugs Are there any new drugs in the pipeline or in the pipeline or
pharmacy?pharmacy?
TelithromycinTelithromycin
800 mg once/day800 mg once/day $114.00 for 10-day course of $114.00 for 10-day course of
therapytherapy GI effects about the same as GI effects about the same as
Azithromycin - slightly elevated Azithromycin - slightly elevated over placebo in the trialsover placebo in the trials
Blurred vision - 1%; group at risk: Blurred vision - 1%; group at risk: women < 40 years of age - 2%women < 40 years of age - 2%
The Medical Letter 2004;46:66-68The Medical Letter 2004;46:66-68
Outpatients with Outpatients with CAP?CAP?
Drug IDSA2000
ATS2001
Sanfrd2000
CIDS/CTS 00
Doxy Yes Yes 2nd
Choice2nd
Choice
Macro Yes AzithClarth
AzithClarth
AzithClarth
Fluorq SelectRisk Pts
SelectRisk Pts
SelectRsk/age
2nd
Choice
IDSA2003HealthyYes
Yes
No
IDSA2003ComrbdNo
AzithClarth
Yes

What’s the deal with What’s the deal with all this 4 hour all this 4 hour
business for time to business for time to antibiotics?antibiotics?

JCAHO CAP IndicatorsJCAHO CAP Indicators
Smoking cessation programSmoking cessation program Pneumovax program and documentationPneumovax program and documentation Time to Antibiotics (less than 8h) - Time to Antibiotics (less than 8h) - less than 4hless than 4h Blood Cultures for admitted patientsBlood Cultures for admitted patients
Quality of Care, Process, Quality of Care, Process, Outcomes in Elderly with Outcomes in Elderly with
PneumoniaPneumoniaJAMA 1997; 278:2080-2084JAMA 1997; 278:2080-2084

0.4
0.6
0.8
1
1.2
1.4
1.6
0 1 2 3 4 5 6 7 8 9 10
OR
Odds of Survival at 30days vs Time to Antibiotic
JAMA 1997; 278:2080-2084

What’s the deal with What’s the deal with cultures?cultures?Don’t Get Em:Don’t Get Em:
1. Positive approx 8%1. Positive approx 8%2. When Positive, no change in RX2. When Positive, no change in RX3. Cost: Patient discomfort, false 3. Cost: Patient discomfort, false positive, contaminants, etc..positive, contaminants, etc..
Get Em:Get Em:1. JCAHO interest1. JCAHO interest2. Association with decreased 2. Association with decreased mortality.mortality.3. Microbiologic/Resistance 3. Microbiologic/Resistance monitoringmonitoring

Clinical Utility of Blood Cultures Clinical Utility of Blood Cultures in Adult Pts with Comm-Acqd in Adult Pts with Comm-Acqd
Pneumonia Pneumonia Chest 1995; 108:932-936Chest 1995; 108:932-936
7%
5%
88%
Positive
Contaminant
Negative
Culture Result
517 Community Acquired Pnemonia Pts
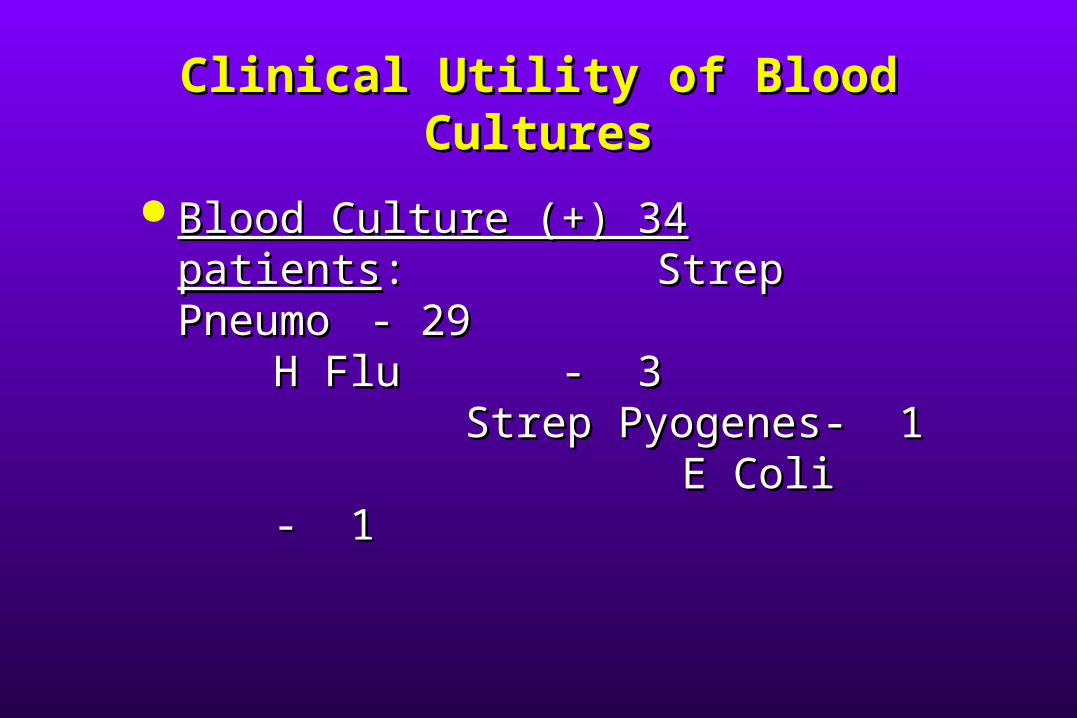
Clinical Utility of Blood Clinical Utility of Blood CulturesCultures
Blood Culture (+) 34 patientsBlood Culture (+) 34 patients::Strep Pneumo Strep Pneumo - 29- 29
H FluH Flu - 3- 3Strep Strep
Pyogenes- 1Pyogenes- 1 E E ColiColi - 1- 1
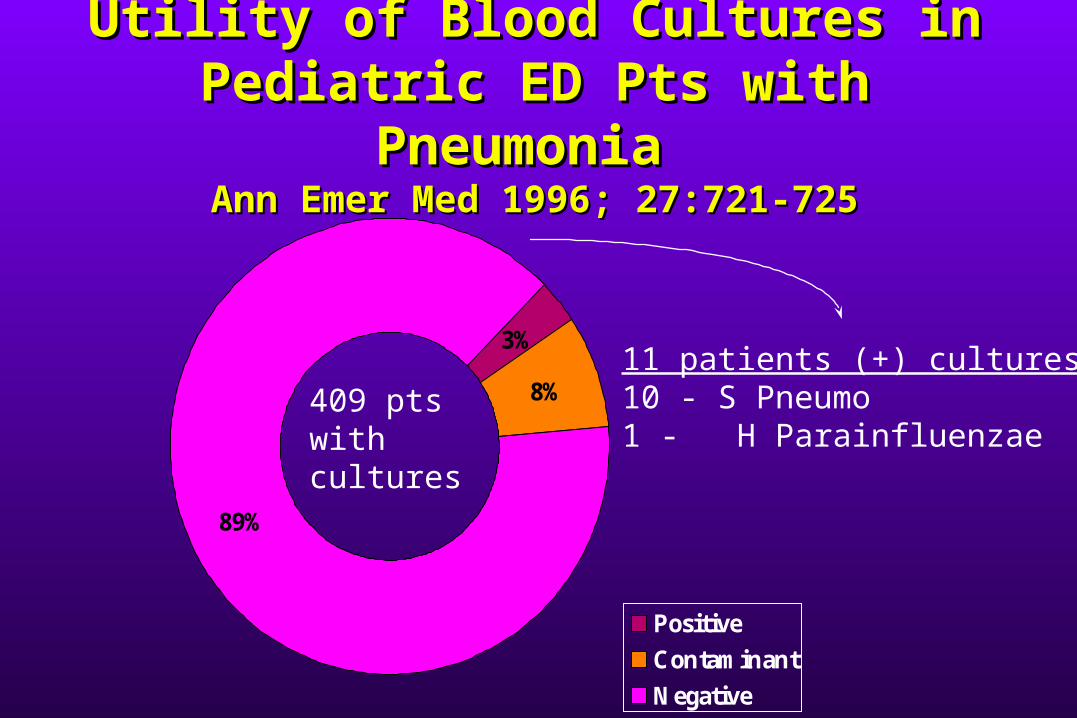
Utility of Blood Cultures in Utility of Blood Cultures in Pediatric ED Pts with Pediatric ED Pts with
Pneumonia Pneumonia Ann Emer Med 1996; 27:721-725Ann Emer Med 1996; 27:721-725
3%
8%
89%
Positive
Contaminant
Negative
409 ptswithcultures
11 patients (+) cultures10 - S Pneumo1 - H Parainfluenzae
What’s the deal with What’s the deal with cultures?cultures?Don’t Get Em:Don’t Get Em:
1. Positive approx 8%1. Positive approx 8%2. When Positive, no change in RX2. When Positive, no change in RX3. Cost: Patient discomfort, false 3. Cost: Patient discomfort, false positive, contaminants, etc..positive, contaminants, etc..
Get Em:Get Em:1. JCAHO interest1. JCAHO interest2. Association with decreased 2. Association with decreased mortality.mortality.3. Microbiologic/Resistance 3. Microbiologic/Resistance monitoringmonitoring