Eventi Formativi...
82
Michele Maio Medical Oncology and Immunotherapy, Department of Oncology University Hospital of Siena, Istituto Toscano Tumori SIENA, ITALY Eventi Formativi AIOM-SIAPEC-IAP “VI Corso Nazionale” Roma, 15 Giugno 2016 Strategie di immunoterapia nel melanoma
Transcript of Eventi Formativi...

Michele Maio Medical Oncology and Immunotherapy, Department of Oncology
University Hospital of Siena, Istituto Toscano Tumori
SIENA, ITALY
Eventi Formativi AIOM-SIAPEC-IAP
“VI Corso Nazionale”
Roma, 15 Giugno 2016
Strategie di immunoterapia nel melanoma
Surgery
Radiotherapy
Chemotherapy
Evolving Therapeutic Options for Cancer Treatment

Surgery
Radiotherapy
Chemotherapy
Immunotherapy
Evolving Therapeutic Options for Cancer Treatment

Tissue
samples
readily
accessible
Adaptable to
tissue culture
Amenable to
testing of
novel
therapies
Melanoma as a tool for cancer research

1970s 1980s 1990s 2000s 2010s
Spontaneous regressions in
melanoma: immune component?
1st tumour associated
antigen cloned
IL-2 approved in the US for melanoma
(1992)
IFN adjuvant
melanoma US (1995)
2011 Ipilimumab approved
for advanced melanoma
2014–2015: Nivolumab,
pembrolizumab Approved in advanced melanoma and NSCLC.
Nivolumab + ipilimumab in
melanoma (US)
2010 Provenge US
Coley in 1891: observation of a
tumour regression in a pt who developed a
post-op infection
A historical view of immunotherapy…

6
Adapted from Pardoll DM 2012.
APC/
Tumor T cell
CD40 CD40L
CD137
OX40
CD137L
OX40L
Activation
Activation
Activation
PD-1
B7-1 (CD80)
PD-L1
PD-L2
LAG-3
MHC
CD28 Activation B7-2 (CD86)
B7-1 (CD80) CTLA-4 Inhibition
TCR
Inhibition
Inhibition
Inhibition
These pathways can be
blocked via I-O agents to
counteract tumor-
mediated inhibition
These pathways can be
activated via I-O agents to
counteract tumor-mediated
inhibition
APC=antigen-presenting cell; CTLA-4=cytotoxic T-lymphocyte antigen-4; LAG-3=lymphocyte activation gene-3; MHC=major
histocompatibility complex;
PD-1=programmed death-1; PD-L1=PD ligand-1; PD-L2=PD ligand-2; TCR=T-cell receptor.
Pardoll DM. Nat Rev Cancer. 2012;12:252-264.
T-cell Checkpoint and Co-stimulatory Pathways

Immune Checkpoint Pathways
CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4 ; MHC = major histocompatibility complex; PD-1 = programmed death-1;
PD-L1 = programmed death ligand 1; TCR = T-cell receptor.
CTLA-4 Blockade (ipilimumab) PD-1 Blockade (nivolumab)

0 1 2 3 4 5 6 7 8 9 10
100
90
80
70
60
0
50
40
30
20
10
Overa
ll S
urv
ival (%
)
Years
IPI (Pooled analysis)1
NIVO Monotherapy (Phase 3 Checkmate 066)3
N=210
NIVO Monotherapy (Phase 1 CA209-003)2
N=107
N=1,861
8
Immune Checkpoint Inhibitors Provide Durable Long-
term Survival for Patients with Advanced Melanoma
1. Schadendorf et al. J Clin Oncol 2015;33:1889-1894; 2. Current analysis; 3. Poster presentation by Dr. Victoria Atkinson at SMR 2015 International Congress.

KEYNOTE-006

Topalian S, et al., NEJM 2012
PD-L1 tumor expression
PREDICTIVE MARKERS OF RESPONSE TO PD1/PD-L1 BLOCKADE

Robert C, NEJM, 2015
BMS CA209-066: Overall survival by treatment group
and PDL-1 status subgroup

[TITLE]
Presented By Padmanee Sharma, MD, PhD at 2013 ASCO Annual Meeting

Unresectable or
Metatastic Melanoma
• Previously untreated
• 945 patients
CA209-067: Study Design CA209-067: Study Design
Treat until
progression**
or
unacceptable
toxicity
NIVO 3 mg/kg Q2W + IPI-matched placebo
NIVO 1 mg/kg +
IPI 3 mg/kg Q3W for 4
doses
IPI 3 mg/kg Q3W for 4 doses +
NIVO-matched placebo
Randomize
1:1:1
Stratify by:
• Tumor PD-L1 expression*
• BRAF mutation status
• AJCC M stage
*Verified PD-L1 assay with 5% expression level was used for the stratification
of patients; validated PD-L1 assay was used for efficacy analyses.
**Patients could have been treated beyond progression under protocol-defined circumstances.
N=314
N=316
N=315
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION
NIVO 3 mg/kg Q2W
Randomized, double-blind, phase III study
to compare NIVO+IPI or NIVO alone to IPI
alone
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION 13

Progression-Free Survival (Intent-to-Treat Population)
49%
42%
18%
46%
39%
14%
Pe
rce
nta
ge
of
PF
S
PFS per Investigator (months)
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 27 24 21
314
316
315
174
148
78
133
114
46
103
94
25
8
8
3
219
177
137
156
127
58
126
104
40
48
46
15
0
0
0
Number of patients at risk:
Nivolumab + Ipilimumab
Nivolumab
Ipilimumab
NIVO+IPI
NIVO
IPI
NIVO + IPI (N=314) NIVO (N=316) IPI (N=315)
Median PFS, months (95% CI)
11.5 (8.9–16.7)
6.9 (4.3–9.5) 2.9 (2.8–3.4)
HR (99.5% CI) vs. IPI 0.42 (0.31–
0.57)* 0.55 (0.43–
0.76)* --
HR (95% CI) vs. NIVO 0.76 (0.60–
0.92)** -- --
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION
*Stratified log-rank P<0.00001 vs. IPI
**Exploratory endpoint
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION
Database lock Sept 2015
14
Pro
gre
ssio
n-f
ree S
urv
ival (%
)

Progression-free Survival by Tumor PD-L1 Expression
Tumor PD-L1 Expression Level ≥5% Tumor PD-L1 Expression Level <5%
• Similar results were seen using 1% as the PD-L1 expression cut-off
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION
NIVO + IPI
(N=68)
NIVO
(N=80)
IPI
(N=75)
Median PFS,
months (95%
CI)
NR
(9.7─NR)
22.0
(8.9─NR)
3.9
(2.8–4.2)
HR (95% CI) vs
NIVO
0.87
(0.54–
1.41)*
─ ─
NIVO + IPI
(N=210)
NIVO
(N=208)
IPI
(N=202)
Median PFS,
months (95%
CI)
11.1
(8.0–
22.2)
5.3
(2.8–7.1)
2.8
(2.8–3.1)
HR (95% CI) vs
NIVO
0.74
(0.58–
0.96)*
─ ─ *Exploratory endpoint *Exploratory endpoint
CONFIDENTIAL – NOT FOR FURTHER DISTRIBUTION
Database lock Sept 2015
15
Pro
gre
ssio
n-f
ree S
urv
ival (%
)
Pro
gre
ssio
n-f
ree S
urv
ival (%
)

Response
Time (months)
Chemotherapy/Targeted Agents and
Immuno-therapy Differ in Action and Outcome
0 6 24
CT/target
CTLA-4
CTLA-4+PD-1
PD-1
Maio M. et al, unpublished

New Clinical Settings
Mechanism(s) of resistance
New Targets
New combos/sequences

Effect in the CNS?

26-30 September 2014, Madrid, Spain
esmo.org
IPILIMUMAB Margolin K, Lancet Oncol 2012
N
DCR
OS (m)
PSF (m)
Asymptomatic 51 24% 7.0 1.5
Symptomatic 21 10% 4.0 1.2
IPILIMUMAB + FTM
NIBIT M1
Di Giacomo AM, ESMO 2013
N
DCR
OS (m)
PSF (m)
Asymptomatic 20 50% 12.7 3.4
CTLA-4 blockade in MBM
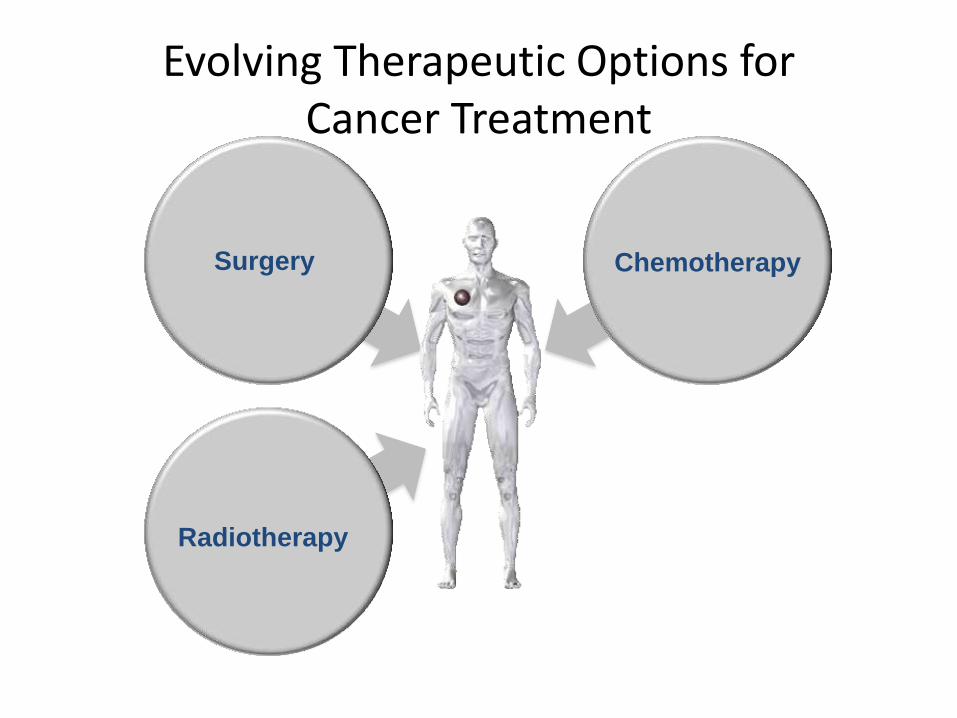
NIBIT - M1
3-years survival update
Di Giacomo AM et al., Annals Oncol 2015
Secondary Endpoints Study population
(N=86)
Patients with
MBM (N=20)
Median OS, months (95% CI)
12.9 (7.1-18.7) 12.7 (2.7-22.7)
3-year survival rate, % (95% CI)
28.5 (20.1-41.3) 27.8 (17.2-60.6)
Median ir-PFS, months (95% CI)
4.5 (3.1-5.9) 3.4 (2.3-4.5)

Screening/ Baseline Randomization
Arm A Induction Phase
Fotemustine: 100mg/m2 iv q1 week for 3 doses
Manteinance Phase Fotemustine: 100mg/m2 q3 weeks
from week 9 for 6 doses
Arm B Induction Phase
Fotemustine: 100mg/m2 iv q1 week for 3 doses and then from week 9 for 6 doses
Ipilimumab: 10 mg/kg iv q3 weeks for 4 doses
Manteinance Phase Ipilimumab: 10 mg/kg iv q12 weeks from week 24
Arm C Induction Phase
Nivolumab 1mg/kg iv + ipilimumab 3mg/kg iv q3 for 4 doses
Manteinance Phase Nivolumab 3mg/kg iv q2 weeks
Follow-up phase Treatment until PD or excessive to toxicity or patient’s refusal
The NIBIT-M2 study design

Siena - Azienda Ospedaliera Universitaria Senese
PI - Coordinatore nazionale Dr. ssa Anna Maria Di Giacomo
Milano - I.E.O. Istituto Europeo di Oncologia
PI Dr. Pier Francesco Ferrucci
Milano - Fondazione I.R.C.C.S. Istituto Nazionale dei Tumori
PI Dr. Michele Del Vecchio
Torino –AOU Città della salute e della Scienza
PI Dr. Pietro Quaglino
Padova- Istituto Oncologico Veneto
PI Dr. ssa Vanna Chiarion-Sileni
Genova - Istituto Nazionale per la Ricerca sul Cancro
PI Dr. ssa Paola Queirolo
Bergamo - Azienda Ospedaliera Papa Giovanni XXIII
PI Dr. Mario Mandalà
Bari - IRCCS Giovanni Paolo II
PI Dr. Michele Guida
Roma - Istituto Dermatopatico dell’Immacolata -IDI
PI Prof. Paolo Marchetti
Candiolo –Istituto Candiolo I.R.C.C.S.
PI Prof. Massimo Aglietta
NIBIT – M2

New Clinical Settings
Mechanism(s) of resistance
New Targets
New combos/sequences

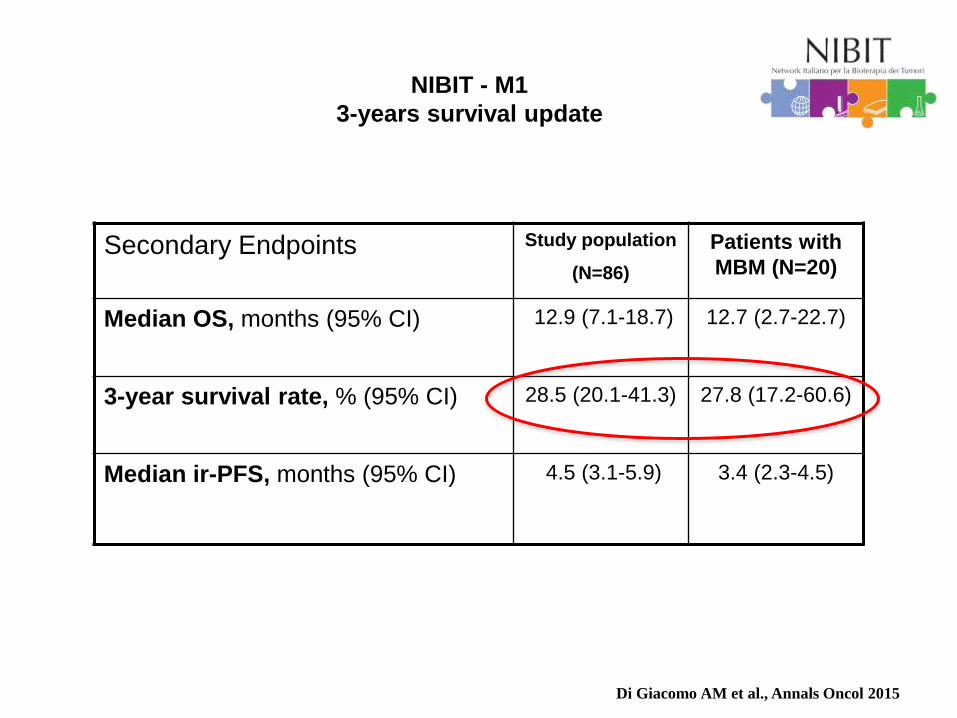
Tumors develop multiple mechanisms
to evade the immune system
HLA class I downregulation in different tumor lesions
Courtesy of S. Ferrone


It takes two to tango

New Clinical Settings
Mechanism(s) of resistance
New Targets
New combos/sequences

Multiple immune inhibitory and co-stimulatory pathways in the tumor microenvironment are
targets of therapeutic manipulation by antibodies or drugs.
Drew Pardoll, and Charles Drake J Exp Med 2012;209:201-
209
© 2012 Pardoll and Drake

IDO-mediated immunesuppression

(MK-3475-022) - Studio di Fase I/II per valutare la sicurezza e l’efficacia di MK-3475 in combinazione con trametinib e dabrafenib in soggetti con melanoma avanzato
(MK-3475 Protocol 252) - A Phase 3 Randomized, Double-Blind, Placebo-Controlled Study of Pembrolizumab (MK-3475) in Combination With Epacadostat or Placebo in Subjects with Unresectable or Metastatic Melanoma (Keynote-252/INCB 24360-
301)
SNDX-275-0601 NSCLC and Melanoma, immuno-oncology study (pembro+entinostat)
Ongoing combos
New Clinical Settings
Mechanism(s) of resistance
New Targets
New combos/sequences

Immune check-point(s) blockade-based
combinations/sequences holding the most promise
for future development
• Vaccines
• Cytokines
• Tumor microenvironment modulating agents
• Selected chemotherapeutic agents
• Targeted therapies
• Epigenetic therapies

Heritable changes in gene expression
not based
on modifications of the DNA sequence
EPIGENETICS

EPIGENETICS AND CANCER D
NA
me
thyla
tio
n
Cancer development and progression
GLOBAL genomic DNA
HYPOMETHYLATION
GENE-SPECIFIC promoter
HYPERMETHYLATION
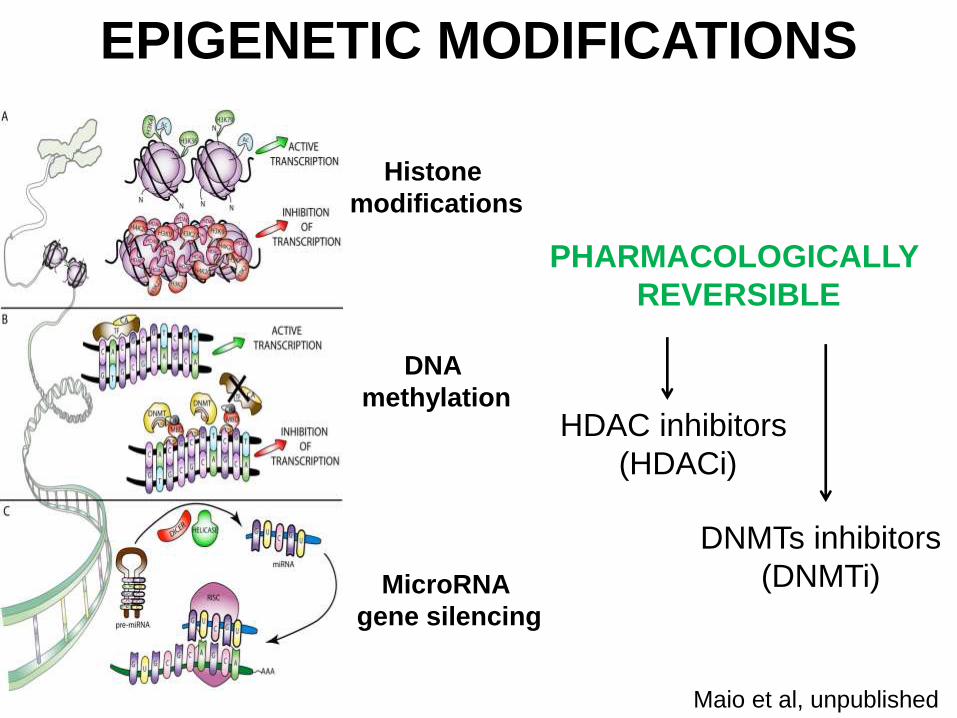
DNA
methylation
Histone
modifications
MicroRNA
gene silencing
EPIGENETIC MODIFICATIONS
PHARMACOLOGICALLY
REVERSIBLE
DNMTs inhibitors
(DNMTi)
HDAC inhibitors
(HDACi)
Maio et al, unpublished

Immunomodulatory activities of DNMTi and HDACi
Effect target DNMTi HDACi ref
CTA expression X Sigalotti L, Blood, CCR, CR, 2003-2005
MHC class I expression X X Sigalotti L Pharmacology & Therapeutics 2014
MHC class II expression X X Gialitakis M, Nucleic Acids Res. 2006
co-stimulatory molecules expression X X Magner WJ, J Immunology 2000
NKG2D ligands expression X Armeanu S, Cancer Res. 2005
FOXP3 expression X X Licciardi PV, ISRN Hematology 2012
function of DC X Licciardi PV, ISRN Hematology 2012
TRAIL and FAS expression X Sigalotti L Pharmacology & Therapeutics 2014
pro-apoptotic genes expression X Sigalotti L Pharmacology & Therapeutics 2014
CD4 proliferation X Kroesen M, Oncotarget 2014
function of CD8 X X Kroesen M, Oncotarget 2014

Can epigenetic modulation of
neoplastic cells be used to design
novel immunotherapeutic
approaches in cancer?

Maio M. et al., CCR 2015
Epigenetic Immunomodulation of Cancer cell

COMBOS
TUMOR
Epigenetic drugs
Modulate
tumor immunogenicity
and immune recognition HOST
Check-point mAb
Improve host’s immune
system activity
Epigenetic immuno-sequencing

Antitumor activity of SGI-110 + α-CTLA-4 mAb in TS/A (breast) tumors
A. Covre et al., Semin Oncol 2015
84%
63%

Epigenetic immuno-sequencing: the NIBIT-M4 Study
(NCT02608437)
W1 W4 W7 W10 Ipilimumab 4 x q21
W0 W3 W6 W9
SGI-110
5 days q21
WK
TA W 12
A.M. Di Giacomo et al. Semin Oncol, 2015
FPFV October 12, 2015

NEWS FEATURES Nature Medicine 2016

CTLA-4 PD1-PDL1 CTLA-4/PD1
Combos
Melanoma Lung cancer
Other tumors
Mesothelioma Urothelial
Colorectal
Glioblastoma
Head-Neck
Ovarian
Breast
Renal
Novel targets
4-1BB
OX-40 ICOS KIR
TIM-3
LAG-3 CD40
IDO



Cancer Bio- Immunotherapy in Siena XIV NIBIT Meeting

• Maresa Altomonte • Erika Bertocci • Luana Calabrò • Ornella Cutaia • Riccardo Danielli • Anna Maria Di Giacomo • Carolina Fazio • Ester Fonsatti • Cristina Maccalli • Lorenzo Pilla
MEDICAL ONCOLOGY AND IMMUNOTHERAPY DEPT. OF MEDICAL ONCOLOGY UNIVERSITY HOSPITAL OF SIENA
• Francesca Colizzi • Sandra Coral • Alessia Covre • Elisabetta Fratta • Hugues Nicolay • Giulia Parisi • Aurora Rizzo • Luca Sigalotti
Michele Maio and

Medical Oncology and Immunotherapy, University Hospital of Siena

© 2015 Amgen Inc. All rights reserved
1
T-VEC – an HSV-1-derived oncolytic
immunotherapy designed to produce local
and systemic effects
Proposed mechanism of action for T-VEC.
Local effect:
virus-induced tumour-cell lysis
Systemic effect:
tumour-specific immune response
Selective viral
replication in
tumour tissue1,2
Tumour cells rupture for
an oncolytic effect1–3
Systemic
tumour-specific
immune response4,5
Death of distant
cancer cells4–6
Oncology

© 2015 Amgen Inc. All rights reserved
Response to T-VEC + ipilimumab
The waterfall plot shows best reductions in tumour burden at a single time point. For the immune-related response criteria (irRC)
response table, CR, PR and PD needed to be confirmed by consecutive assessments no less than 4 weeks apart to be considered
confirmed with the following exception: if PD was the last evaluable tumour assessment, it was considered as confirmed.
*The actual number of overall responders by irRC at time of data analysis was 10, but subsequently one was found to be incorrectly
reported as a confirmed PR instead of the correct assessment of SD. The table has been updated to reflect the corrected data; †Last response was PD followed by unevaluable response. ‡This subject was incorrectly reported to have best overall response
(BOR) of −100% at time of data analysis, but the corrected BOR is −46%; §Unconfirmed CR.
Best irRC confirmed
response
Per irRC
n (%)
ORR* 9 (50)
CR 4 (22.2)
PR 5 (27.8)
SD 4 (22.2)
PD 4 (22.2)
Unevaluable† 1 (5.6)
Disease control rate
(CR + PR + SD) 13 (72.2)
d
N = 18
d
Stage IIIC (n = 3)
Stage IV M1c (n = 4)
Stage IV M1b (n = 5)
Stage IV M1a (n = 4)
Stage IIIB (n = 1)
-100
-50
0 25 50
100
200
300
400
500
600
Ch
an
ge
fro
m b
ase
line
(%
)
‡ §
Puzanov I, et al. ASCO 2015: Abstract 9063.

Phase 1b: Study design
Treatment until whichever occurs first: • Progressive disease (PD) per irRC • Intolerance • 2 Years • All injectable tumors disappeared (T-VEC only)
S
A
F
E
T
Y
F
O
L
L
O
W
-
U
P
30 (+7)
days after
end of
treatment
• Unresectable stage
III or IV melanoma
• Treatment naive
• Injectable lesions
• No clinically active
brain mets
• No active herpetic
skin lesions or prior
complications from
herpetic infection
N=21
Wk 6 DLT
Window
Pembrolizumab 200mg IV Q2W
Wk 0
T-VEC intralesional
Up to 4 mL per treatment
1st dose 106 PFU/mL
Then 108 PFU/mL Q2W
T-VEC Intralesional
Wk -5 Wk -2

Next steps
Phase 2
Monotherapy T-VEC to evaluate correlation between
ORR and baseline intratumoral CD8+ cell density
Phase 3 (MASTERKEY-265)
T-VEC + pembrolizumab vs pembrolizumab
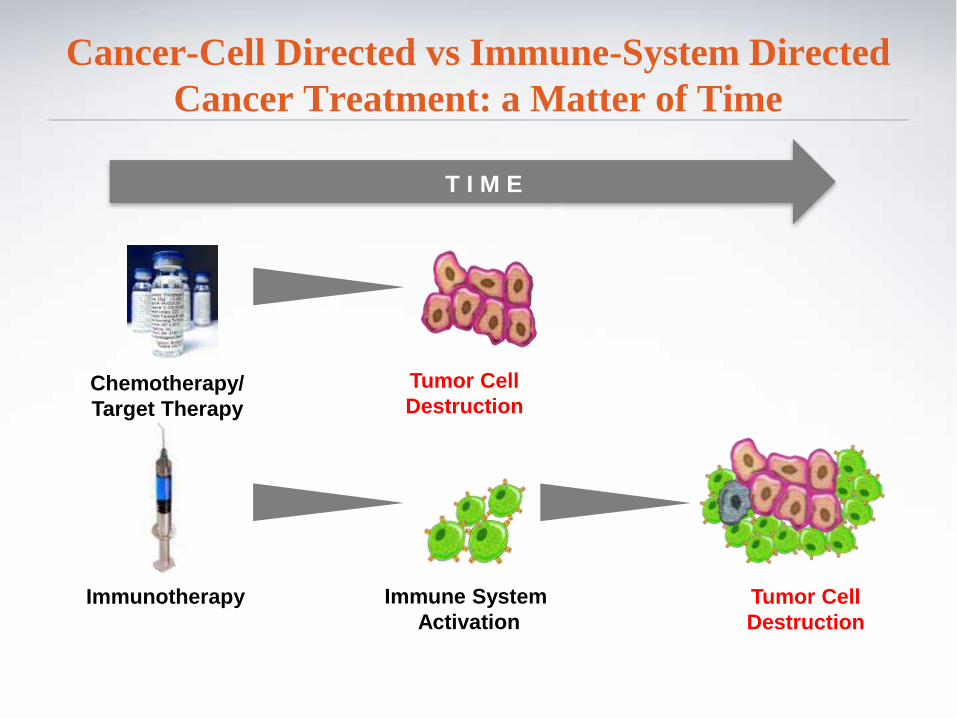
T I M E
Cancer-Cell Directed vs Immune-System Directed
Cancer Treatment: a Matter of Time
Chemotherapy/
Target Therapy
Tumor Cell
Destruction
Immunotherapy Tumor Cell
Destruction
Immune System
Activation

“Unconventional” clinical responses with I-O agents
Vaccines
(i.e., PD followed by OR)

08-1999 03-2000 06-2000
11-2000 02-2001 08-2008
Maio M. et al, unpublished
Metastatic melanoma

“Unconventional” clinical responses with I-O agents
(i.e., PD followed by OR)
Vaccines
CTLA-4

Survival 52 months, received 8 cycles (last one in Aug 2012)
Baseline PD after 2nd dose PR after 4th dose PR after 7th dose
Calabrò et al, OncoImmunology 2014
Pleural mesotelioma

“Unconventional” clinical responses with I-O agents
PD1/PDL1
(i.e., PD followed by OR)
Vaccines
CTLA-4

Early responses

“Unconventional” clinical responses with I-O agents
(i.e., PD followed by OR)
PD1/PDL1
Vaccines
CTLA-4
PD1/PDL1 +
CTLA-4

On treatment
Off treatment
First response
Ongoing response
0 8 16 24 32 40 48 64 72 80 56
Time (weeks)
NIV
O+
IPI
Timing of OR induced by anti-CTLA4 + anti-PD1
Earlier
responses

True tumor progressions
Pseudoprogressions
Tumor flares

IPILIMUMAB PATTERN OF RESPONSE
W 24 Baseline
Baseline
W 12 PD
W 12
Induction Phase IPI 10mg/Kg ev d1, Q3ws x 4 Maintenance Phase IPI 10mg/Kg ev d1, Q12ws
Di Giacomo AM., Cancer Immunol Immunother., 2011
W 24
SD

Histopathology of cutaneous biopsy at week 56
Haematoxylin and eosin staining depicting strong regressive changes both in
flat and nodular areas of the tumor biopsy; neoplastic melanocytes were
virtually absent throughout the whole lesion.
Di Giacomo AM., Cancer Immunol Immunother., 2011

Histopathology of liver biopsy at week 102
Histological examination of a liver melanoma mts showed massive necrosis of melanocytes.
On left, well-preserved fibroblats with rare lymphocytes inside a fibrotic septum, and
melanophages are recognizable (original magnification 200x)
Di Giacomo AM., Cancer Immunol Immunother., 2011

IPILIMUMAB PATTERN OF RESPONSE
Baseline W 12 PD W 120 SD W 24 SD
Baseline W 12 W 120 W 24
Induction Phase Maintenance Phase IPI 10mg/Kg ev d1, Q3ws x 4 IPI 10mg/Kg ev d1, Q12ws
Di Giacomo AM., Cancer Immunol Immunother., 2011

IPILIMUMAB PATTERN OF RESPONSE
W1R (W152)
Follow-up Reinduction Phase IPI 3mg/Kg iv d1, Q3 ws x4
PD
CR
W60 R
CR
CR
W12 R
CR
PR

w24 Baseline

CD8+ Granzyme+
Pre-therapy

W12
W20 CLINICAL CASE 60-year-old Female Affected by Stage III Melanoma
“Inflammatory flares -Pseudo-progression”
W24 W36 W48 W60 W72 W80
W18
MAINTENANCE
TA
INDUCTION
W24 W18
“Inflammatory flares -Pseudo-progression”
•Early appearance following adjuvant ipi treatment (Protocol. BMS CA 184029)
–early induction phase, up to week 12
–enlarged lymph nodes
*FNA left palatine tonsil: normal
Adjuvant melanoma trial BMS029/EORTC 18071

W60
W66
W60
At W60 evidence of a Single pulmonary lesion (37x34mm), with the morphologic feature of an inflammatory lesion.
According with the current recommendations we have skipped the scheduled dose (W60)
and we have obtained a F/U scan after 6 weeks.
CLINICAL CASE 60-year-old Female Affected by Stage III Melanoma
“Inflammatory flares -Pseudo-progression”
W60
W66

CLINICAL CASE 60-year-old Female Affected by Stage III Melanoma
“Inflammatory flares -Pseudo-progression”
INDUCTION MAINTENANCE
W24 W36 W48 W60 TA W72 W80
W72 Current Recommendations
•If F/U scan stable or resolved or biopsy negative for tumor:
–scan as scheduled at next time point
–maintain treatment per
protocol schedule
irAE management
What patients don’t say!

03 Feb 2015 diagnosis of epithelioid pleural mesothelioma, stage IV
19 Feb 2015 start 1st line CT w Cisplatin/Pemetrexed x 4 cyclesPR
--> CT w Carboplatin/Pemetrexed x 4 cycle (until 07 July 2015)-->SD
Jan 2016 PD-->enrollement in NIBIT-MESO-1 study
Clinical Case 3
M, 48-year-old, PS=0

NIBIT-Meso-1: Study Design
Cycle
Week
Re-treatment in case of PD after induction phase or follow-up
13 12 11 10 9 8 7 6 5 4 3 2 1
48 44 40 36 32 28 24 20 16 12 8 4 0
Treatment FU Screening
MEDI4736 Dose Q4W (9 doses)
Tremelimumab +
MEDI4736 Dose
Q4W (4 doses)
TA TA TA TA TA
FU= follow-up; TA= tumor assessment

08 Mar 2016 lab tests showed increase levels of Bilirubin total and direct,
transaminases (G3 CTC)
• No deterioration of clinical condition (PS=0)
• No significant abnormalities showed at liver ultrasound and liver MRI
• Viral test negatives
• Autoimmunity test negatives
21 Mar 2016 Liver biopsy
23 Feb 2016 1st dose with treme+MEDI4736


25 Mar 2016 we knew that the patient had taken homeopathy compound
(Ganoderma/Coriulus, chinese mushroom) -->hospitalization for
worsening of lab tests
Bilirubin
0
5
10
15
20
25
8 9 11 14 15 16 17 25 28 30 1 3
mg
/dl
Low doses of steroids
High doses of steroids*
Beware of “non-conventional” concurrent medications
Take home message (Case 1)

Case study liver toxicity
0
200
400
600
800
1000
1200
1400
1600
1800
W1 W12 W24 W48 W70 W71 W72 W73 W84
ALT
AST
Clincalbenefit
SD
PR
* Dexamethasone 8 mg i.v. BID x 7 daysslow tapering
*

Take home message (Case 2)
Don’t drink and drive
Don’t drink and get treated with I-O