Evaluation of the qualitative and quantitative ... · Evaluation of the qualitative and...
12
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu - 8 - © 2014 Prague Development Center Peer-reviewed and Open access journal e-ISSN: 1804-4999 | www.academicpublishingplatforms.com ATI - Applied Technologies & Innovations Volume 10 | Issue 1 | 2014 |pp.11-19 The primary version of the journal is the on-line version DOI: http://dx.doi.org/10.15208/ati.2014.03 Evaluation of the qualitative and quantitative characteristics of dual diagnosis (Pilot Study) 1 Maria Prodromou 1 , Savoula Ghobrial 2 , Koukia Eumorfia 3 1 Cyprus Mental Health Services, Department of Addiction Psychiatry 2 University of Nicosia Cyprus 3 Ethniko Kapodistriako Panepistimio Athinon corresponding e-mail: [email protected] postal address: Athalassa Psychiatric Hospital, Cyprus Mental Health Services, Leoforos 199/2, 1452 Nicosia, Cyprus Objective: Dual diagnosis can be defined as a combination of a substance use disorder and a coexistent psychiatric disorder in one patient. It constitutes a challenge for Therapeutic Rehabilitation Programme, because of its multifaceted nature. This pilot study was conducted using a naturalistic approach to study for eighteen months. Clients were admitted as inpatients in Residential Therapeutic Rehabilitation Program offered by the Mental Health Services in Cyprus. Methods: Forty-five consecutive patients admitted to the Residential Therapeutic Rehabilitation Program (RTRP) under the Mental Health Services in Cyprus during the period of January 2009 to June 2010. Primary outcomes were the coexistence of psychiatric disorder and substance use disorder, the client profile with dual diagnosis and treatment retention. The EuropASI questionnaire and examination of personal records were used, which included the psychiatric diagnosis of the patients according to the DSM-IV. Results: A total of forty five patients were used, 30 were males (80%) with mean age 27.5 ± 6.7, and 15 were females, (20%) with mean age 26.4 ± 4.1. The study revealed that 33.3% of patients suffered with psychiatric disorder with coexistence of drug dependency, thus, showing that only a minority of patients admitted to the (RTRP) in Mental Health Services have double diagnosis. Additionally the most commonly appeared psychiatric disorder is mood disorder. The psychiatric disorder is often associated with the main drug use (heroin, cocaine, THC e.t.c), further more patients diagnosed with double diagnosis often abandoned the Residential Rehabilitation Program early. Results support that the group of dually diagnosed and the group with drug-dependence are showing differences in relation to their treatment retention. Conclusion: Despite the fact that the minority of the patients admitted in (RTRP) have double diagnosis, this study reports that patients with dual diagnosis live treatment earlier than patients with drug addiction only. Dual diagnosis negatively affect prognosis in patients with drug dependence. Concluding this pilot study is supporting those clients that are diagnosed with co morbid disorder should be assessed and evaluated at the beginning of their treatment in order to offer them care that is meeting their needs and encourage them to adhere with their treatment. Keywords: Psychiatric disorder, dual diagnosis, drug addiction, substance use disorder, treatment retention Introduction Various studies have examined the prevalence of dual diagnosis amongst the general population and patients of mental health services and substance use rehabilitation 1 Originally published in: Prodromou, M., Ghobrial, S., Eumorfia, K., 2014. "Evaluation of the qualitative and quantitative characteristics of dual diagnosis (Pilot Study)", Medical and Health Science Journal, Vo.15(1), pp.8-19, DOI: http://dx.doi.org/10.15208/mhsj.2014.02
Transcript of Evaluation of the qualitative and quantitative ... · Evaluation of the qualitative and...
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 8 - © 2014 Prague Development Center
Peer-reviewed and Open access journal
e-ISSN: 1804-4999 | www.academicpublishingplatforms.com
ATI - Applied Technologies & Innovations
Volume 10 | Issue 1 | 2014 |pp.11-19
The primary version of the journal is the on-line version DOI: http://dx.doi.org/10.15208/ati.2014.03
Evaluation of the qualitative and quantitative characteristics of dual diagnosis (Pilot Study)1
Maria Prodromou1, Savoula Ghobrial2 , Koukia Eumorfia3
1Cyprus Mental Health Services, Department of Addiction Psychiatry 2 University of Nicosia Cyprus
3 Ethniko Kapodistriako Panepistimio Athinon
corresponding e-mail: [email protected]
postal address: Athalassa Psychiatric Hospital, Cyprus Mental Health Services,
Leoforos 199/2, 1452 Nicosia, Cyprus
Objective: Dual diagnosis can be defined as a combination of a substance use disorder and a coexistent psychiatric disorder in one patient. It constitutes a challenge for Therapeutic Rehabilitation Programme, because of its multifaceted nature. This pilot study was conducted using a naturalistic approach to study for eighteen months. Clients were admitted as inpatients in Residential Therapeutic Rehabilitation Program offered by the Mental Health Services in Cyprus.
Methods: Forty-five consecutive patients admitted to the Residential Therapeutic Rehabilitation Program (RTRP) under the Mental Health Services in Cyprus during the period of January 2009 to June 2010. Primary outcomes were the coexistence of psychiatric disorder and substance use disorder, the client profile with dual diagnosis and treatment retention. The EuropASI questionnaire and examination of personal records were used, which included the psychiatric diagnosis of the patients according to the DSM-IV.
Results: A total of forty five patients were used, 30 were males (80%) with mean age 27.5 ± 6.7, and 15 were females, (20%) with mean age 26.4 ± 4.1. The study revealed that 33.3% of patients suffered with psychiatric disorder with coexistence of drug dependency, thus, showing that only a minority of patients admitted to the (RTRP) in Mental Health Services have double diagnosis. Additionally the most commonly appeared psychiatric disorder is mood disorder. The psychiatric disorder is often associated with the main drug use (heroin, cocaine, THC e.t.c), further more patients diagnosed with double diagnosis often abandoned the Residential Rehabilitation Program early. Results support that the group of dually diagnosed and the group with drug-dependence are showing differences in relation to their treatment retention.
Conclusion: Despite the fact that the minority of the patients admitted in (RTRP) have double diagnosis, this study reports that patients with dual diagnosis live treatment earlier than patients with drug addiction only. Dual diagnosis negatively affect prognosis in patients with drug dependence. Concluding this pilot study is supporting those clients that are diagnosed with co morbid disorder should be assessed and evaluated at the beginning of their treatment in order to offer them care that is meeting their needs and encourage them to adhere with their treatment.
Keywords: Psychiatric disorder, dual diagnosis, drug addiction, substance use disorder,
treatment retention
Introduction
Various studies have examined the prevalence of dual diagnosis amongst the general population and patients of mental health services and substance use rehabilitation
1 Originally published in: Prodromou, M., Ghobrial, S., Eumorfia, K., 2014. "Evaluation of the qualitative and
quantitative characteristics of dual diagnosis (Pilot Study)", Medical and Health Science Journal, Vo.15(1), pp.8-19, DOI: http://dx.doi.org/10.15208/mhsj.2014.02
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 9 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
programme. According to Rady, Salama, Elkholy & Shawky (2013) 22% of mental health hospital patients met the criteria for dual diagnosis. Regarding to outpatient of rehabilitation programme Watkins et al. (2004) found that 50% of this patients may have dual diagnosis. Mueser, Bennett & Kushner (1995), Menezes, Johnson & Thornicroft (1996) found that the prevalence of dual diagnosis amongst patients with psychiatric problems is estimated to be around 35-60%. A research that was conducted in USA public hospitals, using the medical records of alcohol and substanse use disorder patients during 2003-2007, showed that 43.6% of these patients met the criteria for dual diagnosis, while this percentage showed increase through the years (Ding, Yang, Cheng, Schiltz, Summers & Skinstad, 2011). Dual diagnosis percentage was higher in women (54.6%) than men (38.4%). Vergara-Moragues et al. (2012) examined dual diagnosis in 227 cocaine-addicted patients receiving treatment in therapeutic programmes in Spain during 2008-2010 they reported that more than 65% of the participants could be identified as having a lifetime dual diagnosis. 55.5% of these patients had a coexisting Axis I disorder, while 30.4% of them had a coexisting Axis II disorder.
The high prevalence of this co morbidity has been documented in multiple national population surveys since the 1980s. Data show that persons diagnosed with mood or anxiety disorders are about twice as likely to suffer from a drug use disorder (abuse or dependence) compared with respondents in general. The same is true for those diagnosed with an antisocial syndrome, such as antisocial personality or conduct disorder. Similarly, persons diagnosed with drug disorders are roughly twice as likely to suffer from mood and anxiety disorders as well. Gender is also identified as a factor in the specific patterns of observed co morbidities. For example, the overall rates of abuse and dependence for most drugs tend to be higher among males than females. Furthermore, males are more likely to suffer from antisocial personality disorder, while women have higher rates of mood and anxiety disorders, all of which are risk factors for substance abuse (Negrete, 2003; Nestler & Carlezon 2006; Quello, Brady & Sonne, 2005; Kessler, 2004).
Research of literature shows that the number of drug users in the group of the psychotic disorder has significant differences (p<0.001) in comparison with the patient group with mood and personality disorder. Additionally it was found that the drug users group with mood disorder had a higher percentage of psychiatric disorder in comparison with psychotic patients (Alexandrakou, Velentza, Aivalioti, Kiovreki, Manousis, Frankos, 2004).
A study by Cheryl, Swofford, Kasckow, Scheller, Gilkey & Lawrence (1995) examines substance use among a group of 37 schizophrenia patients. It showes that the substance use group appeares with worsen overall symptomatology, although some patients use substances in an effort to self-medicate. Additionally at the onset of the study, the substance used group has a significantly higher severity of illness score; however, the non-use group lives more independently. The substance use group had nearly twice as many hospitalizations in the 2 years prior to the study, a greater rate of missed appointments in the year before and during the study, and 4 times as many relapses during the year of the study than the non- use group. Among 9 of the 37 patients who relapsed in the year of the study, 7 had a history of substance use. Thus, substance use among the schizophrenia patients is a major complicating factor (Baker, Lewin, Reichler, Clancy, Carr & Garrett, 2002).
Regarding the causal relationship between coexisting disorders, there are three main hypotheses in contemporary literature: a) Substance dependence may cause one or more symptoms of psychiatric disorder; b) Psychiatric disorder may lead to substance dependence since a patient may use substances for self therapy and symptom relief; c) the coexisting disorders are caused by overlapping factors, such as brain anomalies, genetic predisposition, early exposure to stressful and traumatic events (McKeown, Philips & Sandford, 2010).
Research has shown that psychiatric disorder may constitute a risk factor for the onset of drug use (Najt, Fusar-Poli & Brambilla, 2011; Swendsen et al., 2010). More specifically, major depressive disorder, bipolar disorder and anxiety disorders (except from generalized
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 10 - © 2014 Prague Development Center
anxiety disorder, PTSD and agoraphobia) are related with an increased risk of drug use (Swendsen et al., 2010). Moreover, Liang & Chikritzhs (2011) found that patients with mood and anxiety disorders were in higher risk for developing alcohol use disorders in comparison to individuals without any psychiatric disorder. Psychiatric disorder patients may use alcohol and other substances for self medication, i.e. to reduce symptoms, which further increases risk for developing substance use disorders (e.g. Bolton, Cox, Robinson & Sareen, 2011). In the case of PTSD, marihuana is commonly used for self medication due to its stress relieving nature (Villagonzalo, Dodd, Ng, Mihaly, Langbein, Berk, 2011). On the other hand, there is evidence that cannabis use may act as a risk factor for the development of psychotic symptoms (Moore et al., 2007; Mastrigt, Addington, & Addington, 2004).
The aim of this study was to examine and identify the percentage of patients, admitted to the Residential Therapeutic Rehabilitation Program in Mental Health Services in Cyprus, with dual diagnosis, explore their special characteristics and the way this affects their treatment.
Methods
Design
This is a new approach to research in Cyprus, and one could argue that is a pioneering type of research since it has never been attempted before. Basically it is a naturalistic quantitative approach research that examines a number of patients for a period of one year and six months in realistic situations against predetermined factors that determine their therapeutic course. The study was conducted in an Inpatients Therapeutic Rehabilitation Program from Psychoactive Substances in Cyprus.
Participants
In this study, the deliberate sampling method was used. Subjects were sampled from an Inpatient Specialized Therapeutic Rehabilitation Program for Drug Addiction which is located in Nicosia and is free of charge as is funded by the Cyprus Ministry of Health. The Therapeutic Rehabilitation Program for Drug Addiction started since the December 2003.
In order to be eligible for the baseline assessment, participants had to be part of the man power of the Program from 01/01/2009-01/06/2010 and count for the whole number of attendees to the program at the time of the study. This actually means that the sample covered those patients who were admitted in the Program before 01/01/2009 but were continuing to be members of the Therapeutic Program at the time of the study.
The study sample consisted of 45 consecutive drug-dependent adult patients (Table 1). Participants a) had to be at least 18 years to 69; b) were actively enrolled in the program, met the criteria for any substance use disorder except alcohol addiction; c) were abstain from illegal and legal drug use for at least the last 15 days, d) were highly motivated for treatment as confirmed in 3 initial appointments with a special nurse before entering the program; e) had a mental state examination by a Psychiatrist and a Clinical Psychologist in order to exclude or confirm mental health comorbidity, and to exclude mental disability and/pathological brain damage. Persons under the age of eighteen and over the age of seventy and persons with brain injury or with somatic or pathological disease were excluded from the study. Upon completion of the baseline assessment participants, who met the initial inclusion criteria, were eligible potentially to participate in the study. The EuropASI questionnaire, review of personal records, which included the psychiatric diagnosis of the patients according to the DSM-IV and was confirmed by the psychiatrist, were attached to the Program. Another outcome considered was retention in treatment, measured in months for the purposes of the analysis. All patients entered voluntarily the treatment program, and no patient had been involuntarily treated under section. However,
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 11 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
any participant was free to leave the programme without any consequences to their treatments.
The patients entered into the Therapeutic Program when they were free from any substance use and they were continuing their therapeutic effort if they were remained drug free. If at any stage of the program the patients were suspected and proven by positive urine testing that they went back to drug taking, had any sexual relationship with any other participant or they committed any violent acts against the other participants, they were expelled from the program.
The validity of the sample was determined by the fact that the sample included all of the participants that constituted the totality of patients participating in the therapeutic program from 01/01/2009-01/06/2010 and met the specific criteria. For this population the sample is representative since it consists of all the people who asked for help in a period of one year and six months in the treatment program.
The ethics committee of the affiliated institutions approved the study, as well as the Cyprus Bioethics Committee. All participants were asked to sign a informed consent to participate in the study. No allocation into groups took place, and all patients received the standard care provided.
Measures
Addiction Severity Index (ASI) or EuropASI
The Addiction Severity Index (ASI) is a multi-dimensional interview used to measure the substance use, health and social problems of those with alcohol and other drug problems; both at admission to treatment and subsequently at follow-up contacts. The Addiction Severity Index (ASI) was developed 25 years ago (Cacciola, Alterman, McLellan, Lin and Lynch, 2007; McLellan, Cacciola, Alterman, Rikoon and Carise, 2006) by a team of investigators as a semi-structured clinical-research interview designed to measure patient status in seven functional domains: alcohol and drug use, medical and psychiatric health, employment/self support, family relations, and illegal activity.
DSM-IV Diagnostic Criteria of Mental Disorders (Maser and Patterson, 2002)
The Diagnostic and Statistical Manual of Mental Disorders is practically the bible for psychologists and psychiatrists when diagnosing if an individual has a mental disorder. The DSM-IV is a categorical classification system (Maser and Patterson, 2002)
Multi-axial system
1.1.1 The DSM-IV organizes each psychiatric diagnosis into five dimensions (axes) relating to different aspects of disorder or disability:
Axis I: All diagnostic categories except mental retardation and personality disorder
Axis II: Personality Disorder and mental retardation
Axis III: General medical condition; acute medical conditions and physical disorders
Axis IV: Psychosocial and environmental factors contributing to the disorder
The above tool was used by the psychiatrist to assess the participants.
Procedure
All subjects were approached by the researcher who also was working on the programme to determine their interest to the study. If a subject was interested to participate, the researcher individually interviewed the patient to give the necessary information and gain his/her acceptance, informed consent was signed and anonymity was also assured; they were also informed that they could leave the study anytime without interference with their
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 12 - © 2014 Prague Development Center
therapeutic treatment. The study was conducted in strict accordance with all human subject protection and good clinical practices (Helsinki Declaration, Belmont Principles and the Nuremberg Code, 1964).
If a subject was eligible to participate in the study, the researcher met with the participant individually to complete the research questionnaire (EuropASI), assessed by the psychiatrist attached to the programme according to the DSM-IV. Additionally information from the patients files were collected according to the time retention in the therapy. All interventions were delivered over 18 months.
Background to therapeutic programme
The therapeutic programme was based on a modified therapeutic community (TC) model Bunt, Muehlbach and Moed (2008) for drug dependent populations, that reside in one treatment community, including the drug dependent patients (Sacks, McKendrick, Sacks and Cleland, 2010). The therapeutic model was also inspired from milieu therapy (Moline, 1977) and contingency management approach (Prendergast, Podus, Finney, Greenwell and Roll, 2006)
In the examine facility no methadone or buprenorphine users were accepted.
Data analysis
Data were analyzed using SPSS Statistics version 17.0 (SPSS Inc, Chicago Ill.). Baseline participants characteristics were analysed using t-test. After descriptive statistics methods and correlation analysis, time-to-event as well as univariate and multivariate Cox regression analysis was conducted to investigate the effect of the participants characteristics and multiple-drug dependence, on retention time.
Results
The average age of male participants was 27.5 ± 6.7, and the one for female - 26.4 ± 4.1. The majority of participants (71.11%) were Greek Cypriots, 17.77% were Greeks (from mainland Greece), 4.44% were from British nationality, 2.22% were Australian nationals and 4.44% were Russian and Georgian nationals.
28 participants (62.22%) were living at home with their parents, 5 participants (11.1%) were living with their marital partner and with their children, 4 participants (8.9%) were living with their partners, 3 participants (6.66%) were living alone and 1 (2.22%) participant was living with friends, while 4 participants (8.9%) were living with another person in non stable conditions. Also the majority (41 person or 91.1%) lived in family accommodation while 4 persons (8.88%) lived in temporary accommodation or they were homeless. Most of the participants (18 participant or 40%) were working full-time, 11 (24.4%) were unemployed, 4 (8.9%) were students and 6 participants (13.3%) were working part-time. The majority of them (28.88%) completed at least secondary school, 11 participants (24.44%) completed college, 5 participants (11.11%) attended technical college, 8 participants (17.77%) only attended primary school and 1 participant (2.22%) had no education at all.
The results has shown that the earliest age of main substance use was 11 years and the older one - 43 years with average age made the 27 years. The Table 1 shows information about the frequency and the type of drug use.
Additionally, 19 participants (42.22%) were found with multiple drug addiction, 10 participants (22.22%) were heroine users, the substance use for 7 participants (15.55%) was cannabis and for 4 participant (8.88%) the main substances use were alcohol and drugs. One participant (2.22%) failed to answer this particular question “what was the main substance used”. Moreover in the persons attended the Rehabilitation Therapeutic Program had heroine as the main substance use, when we excluded those participants who
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 13 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
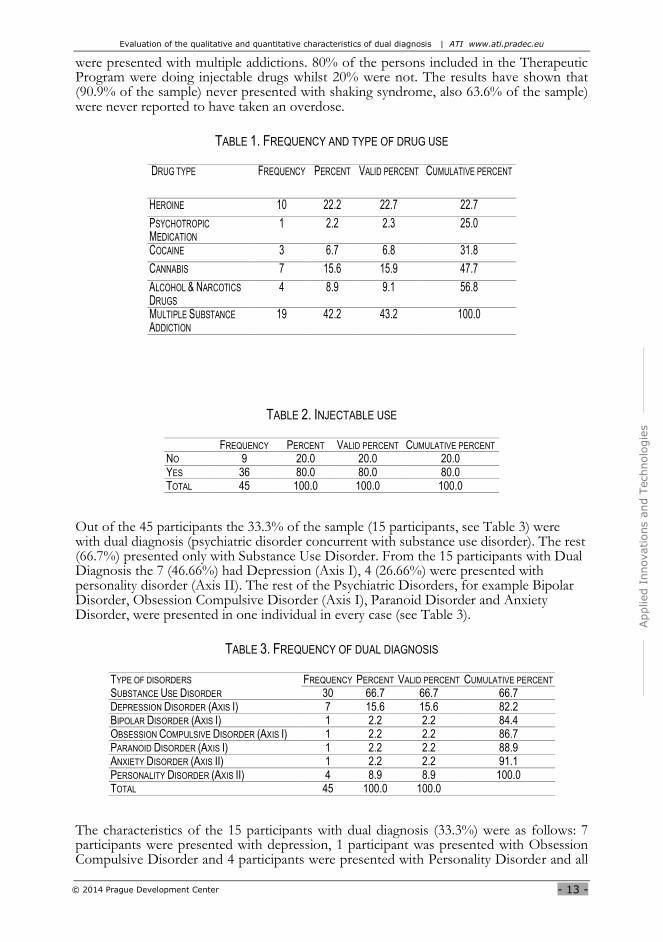
were presented with multiple addictions. 80% of the persons included in the Therapeutic Program were doing injectable drugs whilst 20% were not. The results have shown that (90.9% of the sample) never presented with shaking syndrome, also 63.6% of the sample) were never reported to have taken an overdose.
TABLE 1. FREQUENCY AND TYPE OF DRUG USE
DRUG TYPE FREQUENCY PERCENT VALID PERCENT CUMULATIVE PERCENT
HEROINE 10 22.2 22.7 22.7
PSYCHOTROPIC
MEDICATION 1 2.2 2.3 25.0
COCAINE 3 6.7 6.8 31.8
CANNABIS 7 15.6 15.9 47.7
ALCOHOL & NARCOTICS
DRUGS 4 8.9 9.1 56.8
MULTIPLE SUBSTANCE
ADDICTION 19 42.2 43.2 100.0
TABLE 2. INJECTABLE USE
FREQUENCY PERCENT VALID PERCENT CUMULATIVE PERCENT NO 9 20.0 20.0 20.0 YES 36 80.0 80.0 80.0 TOTAL 45 100.0 100.0 100.0
Out of the 45 participants the 33.3% of the sample (15 participants, see Table 3) were with dual diagnosis (psychiatric disorder concurrent with substance use disorder). The rest (66.7%) presented only with Substance Use Disorder. From the 15 participants with Dual Diagnosis the 7 (46.66%) had Depression (Axis I), 4 (26.66%) were presented with personality disorder (Axis II). The rest of the Psychiatric Disorders, for example Bipolar Disorder, Obsession Compulsive Disorder (Axis I), Paranoid Disorder and Anxiety Disorder, were presented in one individual in every case (see Table 3).
TABLE 3. FREQUENCY OF DUAL DIAGNOSIS
TYPE OF DISORDERS FREQUENCY PERCENT VALID PERCENT CUMULATIVE PERCENT SUBSTANCE USE DISORDER 30 66.7 66.7 66.7 DEPRESSION DISORDER (AXIS I) 7 15.6 15.6 82.2 BIPOLAR DISORDER (AXIS I) 1 2.2 2.2 84.4 OBSESSION COMPULSIVE DISORDER (AXIS I) 1 2.2 2.2 86.7 PARANOID DISORDER (AXIS I) 1 2.2 2.2 88.9 ANXIETY DISORDER (AXIS II) 1 2.2 2.2 91.1 PERSONALITY DISORDER (AXIS II) 4 8.9 8.9 100.0 TOTAL 45 100.0 100.0
The characteristics of the 15 participants with dual diagnosis (33.3%) were as follows: 7 participants were presented with depression, 1 participant was presented with Obsession Compulsive Disorder and 4 participants were presented with Personality Disorder and all
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 14 - © 2014 Prague Development Center
were Cypriots (71.1% of the sample). The other 2 participants diagnosed with Bipolar Disorder (1) and with Anxiety Disorder (1) were British (4.4% of the sample).
In those patients with dual diagnosis their working circumstances over the last three years were as follows:
The three participants out of seven that were diagnosed with depression had a full time job (42% of the sample), one participant had a part time job (14.3%), and two participants were unemployed (28.6%). Among those with bipolar disorder the only one person was unemployed. One participant with Obsession Compulsive Disorder was a student, one participant with Paranoid Disorder was unemployed and one participant with Anxiety Disorder was in full employment. Among those participants with Personality Disorder, 1 (25% of the sample) was in full employment, 1 (25%) was in part time employment, and 2 (50%) were unemployed.
The above results demonstrate that the majority of the participants with dual diagnosis were unemployed.
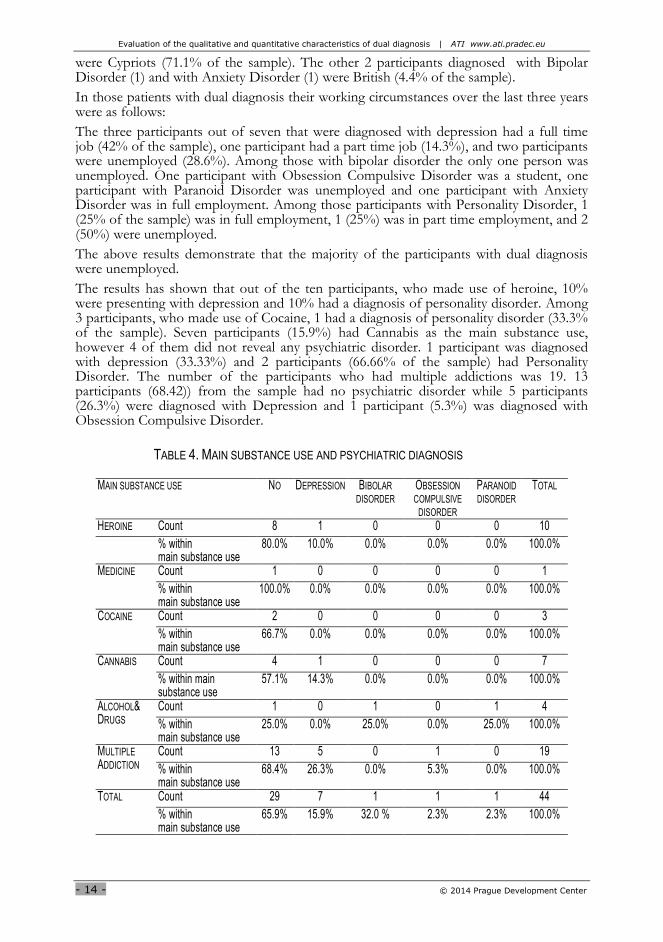
The results has shown that out of the ten participants, who made use of heroine, 10% were presenting with depression and 10% had a diagnosis of personality disorder. Among 3 participants, who made use of Cocaine, 1 had a diagnosis of personality disorder (33.3% of the sample). Seven participants (15.9%) had Cannabis as the main substance use, however 4 of them did not reveal any psychiatric disorder. 1 participant was diagnosed with depression (33.33%) and 2 participants (66.66% of the sample) had Personality Disorder. The number of the participants who had multiple addictions was 19. 13 participants (68.42)) from the sample had no psychiatric disorder while 5 participants (26.3%) were diagnosed with Depression and 1 participant (5.3%) was diagnosed with Obsession Compulsive Disorder.
TABLE 4. MAIN SUBSTANCE USE AND PSYCHIATRIC DIAGNOSIS
MAIN SUBSTANCE USE NO DEPRESSION BIBOLAR
DISORDER OBSESSION
COMPULSIVE
DISORDER
PARANOID
DISORDER TOTAL
HEROINE Count 8 1 0 0 0 10
% within main substance use
80.0% 10.0% 0.0% 0.0% 0.0% 100.0%
MEDICINE
Count 1 0 0 0 0 1
% within main substance use
100.0% 0.0% 0.0% 0.0% 0.0% 100.0%
COCAINE
Count 2 0 0 0 0 3
% within main substance use
66.7% 0.0% 0.0% 0.0% 0.0% 100.0%
CANNABIS
Count 4 1 0 0 0 7
% within main substance use
57.1% 14.3% 0.0% 0.0% 0.0% 100.0%
ALCOHOL& DRUGS
Count 1 0 1 0 1 4
% within main substance use
25.0% 0.0% 25.0% 0.0% 25.0% 100.0%
MULTIPLE
ADDICTION
Count 13 5 0 1 0 19
% within main substance use
68.4% 26.3% 0.0% 5.3% 0.0% 100.0%
TOTAL Count 29 7 1 1 1 44
% within main substance use
65.9% 15.9% 32.0 % 2.3% 2.3% 100.0%
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 15 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
There were no significant differences in treatment retention between genders. Cox- Regression analysis did not reveal any significant correlation between treatment retention and age or gender of the patient, category of the substance, multi-drug use, prescribed psychotropic medication use.
The participants with dual diagnosis left the programme early, before the commencement of the main phase of the treatment and they presented with a significant difference from the participants who had drug addiction disorder only. 77.77% of those participants who left the programme after a month were not diagnosed with dual diagnosis. And 22.22% of those who remained with the programme up to 10 months had dual diagnosis. What is evident here, the participants with dual diagnosis did not continue the programme with the same frequency with those participants who only had drug addiction disorder (87.5% of the sample).
Discussion
The sample was chosen from a specific Therapeutic Programme. Similar studies were carried out by De Leon, Ziegenfuss, (1986); De Leon, Wexler, Jainchill, (1982); Havassy, Allvidrez and Owen (2004), also chose their sample from a specific Therapeutic Programme.
The percentage of women who participated in this study was 20% and the percentage of male participants was 80%. The percentage of participation is similar again to the percentage represented in other studies. It is evident that the number of women with Substance Use Problem is lower than the number of relevant men. The majority of the participants in the study live with their families (28 persons or 62.22%). Probably this is due to the Greek Cypriot family culture when family members are supported even when the children are in adulthood; but also it could be due to the inclination of persons with addiction to clink to their families. The majority of the sample are Greek Cypriots (71.11%); possibly this is due to the sample taken from a public Health Therapeutic Center where free therapy is given to those people who are eligible. Persons who are nationals from other countries are not eligible for free therapy which of course has negative implications to this kind of therapy. The occupational status of the majority of the participants revealed that they were in full-time employment (n= 40%) and eleven were unemployed (n=24.4%). This could be due to the fact that the programme supports the individuals to continue their work and remain in the Therapeutic Programme. Most of them had Secondary School Education (n=28.88%).
The results reveal that most of the observed people started their addiction of illegal drug by using Cannabis. These results are also confirmed by the “European Monitoring Center for Drugs and Drug Addiction - Annual Report 2007”.
The starting age of the main drug use was eleven years old. The majority of the participants (n=42.22%) are found with Multiple Drug Addiction; the main substance use was Heroine (out of 45 participants 36 were Heroine Users. 15 out of the 45 participants were diagnosed with Dual Diagnosis (Psychiatric Disorder and Substance Use Disorder).
The findings are in agreement in the number of studies. The research by De Leon and Ziegenfuss (1986) shows that the majority of the participants had dual diagnosis. The study by Kokkevi and Stephani (1995) shows that the majority (n=90.3%) has at least once the Axis I and II Psychiatric Disorder, on top of the Diagnosis of Substance Use Disorder, thus 83% has two or more Disorders.
The Alexandrakou,Velentza, Aivalioti, Kiovreki, Manousis and Frangos (2004) study reveals that the 45.84% of participants are diagnosed with psychotic disorder, ideation disorder, schizoaffective disorder, and the 42.79% has Bipolar Disorder I and II, Depression, and Mania, dysthymia.
Dually diagnosed participants in our study showed poorer prognosis compared to drug dependent only population, when retention in treatment was used as the endpoint for
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 16 - © 2014 Prague Development Center
between groups comparison. Other studies also found dual diagnosis to be a poor prognostic factor when compliance or adherence to treatment (Drake, McFadden, Mueser, McHugo, and Bond, 1998).
Our findings is also consistent with studies that used other relative endpoints such as the symptom severity (Chouljian, Shumway, Balancio, Dwyer, Surber, and Jacobs, 1995; Drake et al.,1998; Osher, Drake, Noordsy, Teague, Hurlbult, and Biesanz, 1994; Kokkevi, Stefanis, Anastasopoulou, and Kostogianni, 1998) as well as illness duration (Chouljian et al., 1995; Drake, Osher,Wallach, 1989; Kokkevi et al.,1998). Other authors also found that dual diagnosis is a poor prognostic factor for relapse, underlying that even when concomitant psychotropic medication treatment is used this is still not associated with successful participation in the treatment program (Wise, Cuffe, and Fisher, 2001). Also is in agreement with our results, even though separate analysis for each mental health disorder category and/or substance category was not possible due to the inadequate sample size.
In our sample, mood and anxiety disorder were the most frequent among participants of the study which is evident in many others studies (Brewer, Catalano, Haggerty, Gaineey and Fleming, 1998).
In our program dually diagnosed patients had a shorter retention time into treatment, there were no control group in this study to compare prognosis between dually diagnosed in abstinence and dually diagnosed in treatment with substitutes. Consequently, a question remains if substitutes could decrease or eliminate the difference in treatment retention. Recently, there is some evidence that harm reduction approaches could help dually diagnosed population. In our study abstinence from any illegal substance, as well as alcohol, was a prerequisite for patients in order to enter and remain in the treatment program. Harm reduction approaches were not incorporated in this study protocol, due to treatment design, inadequate training and consequent inability to apply this approach (Sacks et al., 2010; Strang, McCambridge, Best, Beswick, Bearn, Rees, 2003; Stitzer and Vandrey, 2008; Sorensen, Andrews, Delucchi, Greenberg, Guydish, Masson, 2009; Specka, Boning, Scherbaum, 2011).
Limitation of the study
This is the first study in Cyprus examining retention in treatment between dually diagnosed and drug dependent only patients, participating in a Therapeutic Programme by the same multidisciplinary team. Some important limitations decrease the power and generalizability of the findings, generating interesting questions for future researchers in the field. E.g., researchers did not make use of structured diagnostic interview for the diagnosis of comorbidity. Diagnosis of comorbidity was confirmed after clinical interviews by a Psychiatrist and a Clinical Psychologist. Also, the small sample size precluded the in between gender and/or between category of the substance comparisons. There was no control group of patients receiving care while they were under active use of the substance or under treatment with substitutes. Additionally, in the inclusion criteria for this study the abstinence of the participants from addictive legal or illegal substances resulted to a lower percentage of dual diagnosis. Furthermore, the low population numbers of addictive persons in Cyprus (Anti Narcotics Association of Cyprus) influenced our results.
Future research
The patients with dual diagnosis tend to be more problematic to treat and manage in view of higher rates of non-compliance, violence, homelessness and suicide. The relationship between substance misuse and mental health problems is complex. Intoxication and withdrawal from drugs and alcohol can produce psychiatric symptoms, while on the other hand some individuals with psychiatric disorders, such as antisocial personality disorders and schizophrenia are more susceptible to substance misuse. Is suggested that there is a need for further research to explore the mechanism of coexisting of the two disorders,

Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 17 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
psychiatric disorder and substance use disorder. There is a need to clarify which one of the two is preceding the other, i.e. can the psychiatric disorder lead to substance use disorder or vice versa.
References
Alexandrakou, P., Velentza, Κ., Aivalioti, C., Kiovreki, Α., Manousis, Ν., 2004. “Comorbidity study of substance users in a population of 1963 patients nursed during the last three years in the clinic,” Galini. Psychiatry, Vol.15(1), pp.144
Baker, A., Lewin, T., Reichler, H. Clancy, R., Carr, V., Garrett, R. et al., 2002. "Evaluation of a motivational interview for substance use within psychiatric in-patient services," Addiction, Vol.97(10), pp.1329-37, http://dx.doi.org/10.1046/j.1360-0443.2002.00178.x
Brewer, D.D., Catalano, R.F., Haggerty, K., Gainey, R.R., Fleming, C.B, 1998. "Research report. A meta-analysis of predictors of continued drug use during and after treatment for opiate addiction," Addiction, Vol.93(1), pp.73-92, http://dx.doi.org/10.1046/j.1360-0443.1998.931738.x
Bunt, G. C. Muehlbach, B. Moed, C. O. (2008). "The therapeutic community: an international perspective," Substance Abuse, Vol.29(3), pp.81-7, http://dx.doi.org/10.1080/08897070802218844
Cacciola, J.S., Alterman, A.I., McLellan, A.T.,Lin, Y.T., & Lynch, K.G, 2007. "Initial evidence for the reliability and validity of a lite version of the addiction severity index," Drug and Alcohol Dependence, Vol.87(2-3), pp.297-302, http://dx.doi.org/10.1016/j.drugalcdep.2006.09.002
Cheryl, D., Swofford, J., Kasckow, W., Geri Scheller-Gilkey, Lawrence, B.I., 1995. "Substance use: A powerful predictor of relapse in schizophrenia," Schizophrenia Research, Vol.20, pp.145-151
Chouljian, T.L., Shumway, M., Balancio, E., Dwyer, E.V., Surber, R., Jacobs, M., 1995. "Substance use among schizophrenic outpatients: Prevalence, course, and relation to functional status," Ann Clin Psychiatry, Vol.7(1), pp.19-24, http://dx.doi.org/10.3109/10401239509149020
De Leon, G., Ziegenfuss, Jr., 1986. "Therapeutic communities for addictions: Perspective and approach," In: De Leon, G. & Zeigenfuss (Eds.), The therapeutic community treatment for addictions theory research and practice, Springfield Illinois Charlew C Thomas
De Leon, G., Wexler, H.K., and Jainchill, N., 1982. "The therapeutic community: Success and improvement rates 5 years after treatment," The international Journal of the Addictions, Vol.17(4), pp.703-747
Ding, K., Yank, J., Cheng, G., Schiltz, T., Summers, M.K., Skinstad, A.H., 2011. "Hospitalizations and hospital charges for co-occuring substance use and mental disorders," Journal of Substance Abuse Treatment, Vol.40, pp.366-375, http://dx.doi.org/10.1016/j.jsat.2010.12.005
Drake, R.E., Osher, F.C., Wallach, M.A., 1989. "Alcohol use and abuse in schizophrenia: A prospective community study", J Nerv Ment Dis., Vol.177(7), pp.408-14, http://dx.doi.org/10.1097/00005053-198907000-00004
Drake, R.E., Mercer-McFadden, C., Mueser, K.T., McHugo, G.J., Bond, G.R., 1998. "Review of integrated mental health and substance abuse treatment for patients with dual disorders," Schizophr Bull., Vol.24(4), pp.589-608, http://dx.doi.org/10.1093/oxfordjournals.schbul.a033351
European Monitoring Center for Drugs and Drug Addiction - Annual Report 2007
Havassy, B., Allvidrez, J., Owen, K., 2004. "Comparisons of patients with comorbid psychiatric and substance use disorders: Implications for treatment and service delivery," Am J Psychiatry, January, Vol.161, pp.139-145
Kessler, R., 2004. "The epidemiology of dual diagnosis," Biol Psychiatry, Vol.56, pp.730-737, http://dx.doi.org/10.1016/j.biopsych.2004.06.034
Kokkevi, A., Stefanis, C.N., 1995. Psychiatric co morbidity in substance abuse department of psychiatry, Athens University Medical School, Eginition Hospital, Athens, Greece
Kokkevi, A., Stefanis, N., Anastasopoulou, E., Kostogianni, C., 1998. "Personality disorders in drug abusers: Prevalence and their association with AXIS I disorders as predictors of treatment retention," Addiction Behaviour, Vol.23(6), pp.841-53, http://dx.doi.org/10.1016/S0306-4603(98)00071-9
Liang, W., Chikritzhs, T., 2011. "Affective disorders, anxiety disorders and the risk of alcohol dependence and misuse," The British Journal of Psychiatry, Vol.199, pp.219-224, http://dx.doi.org/10.1192/bjp.bp.110.086116
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 18 - © 2014 Prague Development Center
Moore, T. H. M. Zammit, S. Lingford- Hughes, A. Barnes, T. R.E. Jones, B. P Burke, M. Lewis, G., 2010. "Cannabis use and risk of psychotic or affective mental health outcomes: A systematic review," Lancet, Vol.370, pp.319-28, http://dx.doi.org/10.1016/S0140-6736(07)61162-3
Moragues, E.V., Gonzalez-Saiz, F., Lozano, M.O., Espinosa, P.B., Calderon, F.F. Acebos, I.B., Garcia, M.P., Garcia, A.V., 2012. "Psychiatric comorbidity in cocaine users treated in therapeutic community: Substance-induced versus independent disorders," Elsevier Psychiatry Research, Vol.200, pp.734-741, http://dx.doi.org/10.1016/j.psychres.2012.07.043
Mastrigt, V.S. Addington, D. Addington, J., 2004. Substance misuse at presentation to an early psychosis program, Vol.39, pp.69-72
Maser, J. D. & Patterson, T., 2002. "Spectrum and nosology: Implications for DSM-5," Psychiatric clinics of North America, December, Vol.4, pp.855-885
McLellan, A.T, Cacciola, J.S., Alterman, A.I., Rikoon, S.H. & Carise, D., 2006. "The addiction severity index at 25: Origins, contributions and transitions," American Journal of Addiction, Vol.15(Issue2), pp.113-124, http://dx.doi.org/10.1080/10550490500528316
McKeown, O., 2010. "Definition, recognition and assesment of dual diagnosis," In: Philips, P., McKeown, O. and Sandford, T. (Eds.), Dual diagnosis practice in context, pp.1-13
Menezes, P.R., Johnson, S. Thornicroft, G., 1996. "Drug and alcohol problems among individuals with severe mental illness in south London," Br j Psychiatry, Vol.168, pp.612-19, http://dx.doi.org/10.1192/bjp.168.5.612
Moline, R.A., 1977. "The therapeutic community and milieu therapy: A review and current assessment," Community Ment Health Rev., Vol.2(5)1, pp. 3-13
Mueser, K.T, Bennett, M, and Kushner, M.G., 1995. "Epidemiology of substance use disorders among persons with chronic mental illnesses," In: Lehman, A.F. and Dixon, L. (Eds.), Double jeopardy: Chronic mentall illness and substance abuse, New York, NY: Harwood Academic Publishers, pp.9-25
Najt, P. Fusar-Poli, P. Brambilla, P., 2011. "Co-occuring mental and substance abuse disorders: A review on the potential predictors and clinical outcomes," Psychiatry Res, Vol.186, pp.159-164, http://dx.doi.org/10.1016/j.psychres.2010.07.042
Negrete, J.C., 2003. "Clinical aspects of substance abuse in persons with schizophrenia," Can J Psychiatry, Vol.48(1), pp.14-21
Nestler, E.J., and Carlezon, W.A., 2006. "The mesolimbic dopamine reward circuit in depression," Biol Psychiatry, Vol.59(12), pp.1151-1159, http://dx.doi.org/10.1016/j.biopsych.2005.09.018
Osher, F.C., Drake, R.E., Noordsy, D.L., Teague, G.B., Hurlbut, S.C. Biesanz, J.C. et al., 1994. "Correlates and outcomes of alcohol use disorder among rural outpatients with schizophrenia," J Clin Psychiatry, Vol.55(3), pp.109-13
Prendergast, M. Podus, D., Finney, J., Greenwell, L., Roll, J., 2006. "Contingency management for treatment of substance use disorders: A meta-analysis. Addiction," Vol.101(11), pp.1546-60, http://dx.doi.org/10.1111/j.1360-0443.2006.01581.x
Quello, S.B., Brady, K.T., and Sonne, S.C., 2005. "Mood disorders and substance abuse disorders: A complex comorbidity," Science & Practice Perspectives, Vol.3(1), pp.13-24, http://dx.doi.org/10.1151/spp053113
Rady, A., Salama, H., Elkholy, O., & Shawky, A., 2013. "845-Dual diagnosis of anxiety disorders and substance abuse: The need for awareness," European Psychiatry, Vol.28 (Supplement1)
Robinson, J. Sareen Brian, J. Cox, J. Bolton, M., 2011. "Role of self-medication in the development of comorbid anxiety and substance use disorders: A longitundinal investigation," Arch Gen Psychiatry, Vol.68(8), pp.800-807, http://dx.doi.org/10.1001/archgenpsychiatry.2011.75
Sacks, S., McKendrick, K., Sacks, J.Y., Cleland, C.M., 2010. "Modified therapeutic community for co-occurring disorders: single investigator meta analysis," Subst Abus, Vol.31(3)pp.146-61, http://dx.doi.org/10.1080/08897077.2010.495662
Specka, M., Boning, A., Scherbaum, N., 2011. "Contingency management in opioid substitution treatment," Fortschr Neurol Psychiatr, Vol.79(7), pp.395-403,
http://dx.doi.org/10.1055/s-0029-1245810
Sorensen, J.L., Andrews S, Delucchi KL, Greenberg B, Guydish J, Masson CL, et al., 2009. "Methadone patients in the therapeutic community: A test of equivalency," Drug Alcohol Depend, Vol.100(1-2), pp.100-6, http://dx.doi.org/10.1016/j.drugalcdep.2008.09.009
Evaluation of the qualitative and quantitative characteristics of dual diagnosis | ATI www.ati.pradec.eu
- 19 -
Applied I
nnovations a
nd T
echnolo
gie
s
© 2014 Prague Development Center
Stitzer, M.L., Vandrey, R., 2008. "Contingency management: Utility in the treatment of drug abuse disorders," Clin Pharmacol Ther., Vol.83(4), pp.644-7, http://dx.doi.org/10.1038/sj.clpt.6100508
Strang, J. McCambridge, J. Best, D. Beswick, T., Bearn, J., Rees, S. et al., 2003. "Loss of tolerance and overdose mortality after inpatient opiate detoxification: Follow up study," BMJ, Vol.326(7396), pp.959-60, http://dx.doi.org/10.1136/bmj.326.7396.959
Swendsen, J., Conway, K.P., Degenhardt, L., Glantz, M., Jin, R., Merikangas, K.R., Sampson, N., Kessler, R., 2010. "Mental disorders as risk factors for substance use, abuse and dependence: Results from the 10-year follow-up of the National Comorbidity Survey," Addiction Journal, Vol.105, pp.1117-1128, http://dx.doi.org/10.1111/j.1360-0443.2010.02902.x
Villagonzalo, K. A. Dodd, S. Ng, F. Mihaly, S. Langbein, A. Berk, M., 2011. "The relationship between substance use and posttraumatic stress disorder in a methadone maintenance treatment program," Comprehensive Psychiatry, Vol.52, pp.562-566, http://dx.doi.org/10.1016/j.comppsych.2010.10.001
Watkins, E.K., Hunter, S.B., Wenzel, S.L., Tu, W., Paddock, M.S., Griffin, A., Ebener, P., 2004. "Prevalence and characteristics of clients with co-occurring disorders in outpatient substance abuse treatment," American Journal of Drug and Alcohol Abuse, Vol.30, No.4, pp.749-764, http://dx.doi.org/10.1081/ADA-200037538
Wise, B.K., Cuffe, S.P., Fischer, T., 2001. "Dual diagnosis and successful participation of adolescents in substance abuse treatment," Journal of Substance Abuse Treatment, Vol21(3), pp.161-5, http://dx.doi.org/10.1016/S0740-5472(01)00193-3