
Evaluation of Poisoning and Drug Overdose
41
Evaluation of Poisoning and Drug Overdose Kara Lynch, PhD, DABCC University of California San Francisco San Francisco, CA
Transcript of Evaluation of Poisoning and Drug Overdose

Evaluation of Poisoning and Drug Overdose
Kara Lynch, PhD, DABCC University of California San Francisco
San Francisco, CA

Learning Objectives
• Understand the laboratories role in the diagnosis and treatment of toxicology cases
• Review the pathophysiology of toxic exposures • Identify the common toxidromes • Calculate the osmolar gap and anion gap • Be able to recognize drug overdoses

Paraclesus – “father of toxicology”
• “All things are poison, and nothing is without poison; only the dose permits something not to be poisonous.”
• “The dose makes the poison.” • substances considered toxic
are harmless in small doses, and an ordinarily harmless substance can be deadly if over-consumed
Paraclesus, 1490 - 1541

• A poisoning occurs when a person’s exposure to a natural or manmade substance has an undesirable effect - CDC
• Poisonings can be classified as: – Self-harm or suicide – Assault or homicide – Unintentional or accidental, when no harm was
intended – includes overdoses resulting from drug misuse, drug abuse or taking too much of a drug for medical reasons
Definition of “Poisoning”

• AAPCC – American Association of Poison Control Centers – – National poison data system (NPDS) annual report
• DAWN – Drug Abuse Warning Network • SAMHSA World Drug Report – Substance
Abuse and Mental Health Services Administration
• CDC – Center for Disease Control – National Vital Statistics System (NVSS)
Monitoring Poisonings

Poisoning / Overdose Trends

Poisoning / Overdose Trends

AAPCC: Top 25 human exposures

AAPCC: Top 25 pediatric exposures

Increase in Exposure – Top 4

• ABCs (airway, breathing, circulation) • Supportive Care • Antidote if available and indicated • Decontamination (surface and gastrointestional)
– Wash skin and irrigate eyes, emesis or gastric lavage, activated charcoal or cathartic, whole-bowel irrigation
• Enhanced Elimination – Hemodialysis – Hemoperfusion – Repeat-dose charcoal
Poisoning: Treatment Approach

• Airway → Endotracheal intubation – Check gag/cough reflex – Position patient – Clear/suction airway
• Breathing → ventilatory failure, hypoxia, bronchospasm – Obtain arterial blood gases – Assist with bag/mask device – Give supplemental oxygen
• Circulation → bradycardia, tachycardia, prolonged QRS interval, arrhythmias, hypotension, hypertension – Measure blood pressure/pulse – Monitor electrocardiogram – Start 1-2 IV lines – Obtain routine bloodwork
Treatment: ABC’s or CAB

Antidote or Specific Treatment Toxin Antidote/Treatment Acetaminophen N-Acetylcysteine (NAC, Mucomyst)
Aluminum or Iron Deferoxamine
Anticholinergic agents Physostigmine
Arsenic and Mercury Unithiol, Dimercaprol (BAL), oral succimer (DMSA)
Benzodiazepines Flumazenil
Beta-blockers Glucagon
Calcium channel blockers Calcium
Carbon monoxide Oxygen (normobaric or hyperbaric)
Cyanide Amyl nitrite, sodium nitrite, sodium tiosulfate
Digoxin Digibind (Fab fragments)
Ethylene glycol, methanol Ethanol, fomepizole (5-methylpyrazol), hemodialysis
Isoniazid Pyridoxine (Vitamin B6)
Lead Calcium EDTA, Dimercaprol (BAL), oral succimer (DMSA)
Nitrites, nitrates Methylene blue
Opioids Naloxone
Salicylates Bicarbonate, hemodialysis, alkaline diuresis

Poisoning Evaluation: toxidromes
• Toxidrome = A collection of symptoms and signs that consistently occur after ingestion of a particular toxin or drug class
• Often identified with a basic history and physical examination
• Rapid identification of the toxidrome saves time in evaluating and managing a poisoned patient

Poisoning Evaluation: toxidromes
Kinetic Anatomy with Web Resource, 3rd Edition

Toxidrome Clinical Manifestation Agents commonly involved Anticholinergic • Hypertermia, tachycadia,
hypertension • Agitation, delirium, seizures • Mydriasis • Decreased bowel sounds
• Nonselective antihistamines • Tricyclic antidepressants • Antipsychotic drugs • Benztropine • Scopolamine, atropine • Jimsonweed, deadly nightshade,
amanita muscaria
Cholinergic – Nicotinic / Muscarinic
• Bradycardia(M), Tachycardia(N) • Hypertension (N) • Miosis • Bronchorrhea • Salivation, Lacrimation,
Urination, Diarrhea, GI upset, Emesis – “SLUDGE”
• Organophosphates, carbamates • Physostigmine • Pilocarpine • Betel nut • Mushrooms: clitocybe dealbata,
C. illudens, Inocybe lacera • Black widow spider venom (N)
Sympathomimetic • Hyperthermia, tachycardia, hypertension
• Agitation, delirium, seizures • Mydriasis • Increased bowel sounds • Dry, flushed skin
• Cocaine, amphetamines • Theophylline, caffeine • Salicylates • Monoamine oxidase (MAO)
inhibitors • Sedative/hypnotic withdrawal
Opioid • Hypopnea/bradypnea • Lethargy, obtundation • Miosis
• All opiates and phenothiazines • Hypoglycemic agents • Clonidine
Sedative-hypnotic • Hypothermia, bradypnea/ hypopenia
• Lethargy, stupor, obtundation
• Ethanol • Benzodiazepines, barbiturates • Meprobamate, methaqualone,
chloral hydrate

Blood Pressure
Heart Rate
Resp. Rate
Temp. Pupil size
Bowel sounds
Diaph-oresis
Anticholinergic ↑ ↑ ↑ ↓ ↓
Cholinergic ↓ ↑ ↑
Opioid ↓ ↓ ↓ ↓ ↓ ↓ ↓
Sympathomimetic ↑ ↑ ↑ ↑ ↑ ↑ ↑
Sedative-hypnotic ↓ ↓ ↓ ↓ ↓ ↓
Poisoning Evaluation: toxidromes

psychiatryonline.org
Illicit Drugs: Mechanism of Action

• Serum osmolality and calculation of the osmolar gap • Electrolytes for determination of sodium, potassium and
anion gap • Serum glucose • BUN and creatinine for evaluation of renal function • Liver function tests • Complete blood count • Urinalysis to check for crystalluria, hemoglobinuria or
myoglobinuria • Stat serum acetaminophen and serum ethanol level • Pregnancy test (females of childbearing age) • Electrocardiogram
Essential Laboratory Tests

Toxic Alcohols
• Ethanol • Methanol • Isopropanol • Acetone • Ethylene glycol

• First-order kinetics – rate of elimination is proportional to the amount of drug present
• Zero-order kinetics – rate of elimination is constant regardless of the amount of drug present in the system
• Capacity-limited kinetics – occurs when the rate of elimination shifts from first-order to zero-order based on the saturation of the elimination processes (overdoses)
• Serum half-life – time required for serum concentrations to decrease by one half
• First-pass effect – applies to drugs cleared by the liver before reaching systemic circulation
• Steady-state – applies to repeated dosing; reached in about 4 half-lives
Pharmacokinetics: Review

Toxic Alcohols: Ethanol
• Ethanol or ethanol combined with other drugs accounts for the highest number of toxic exposures
• Potent central nervous system depressant • Effects vary with concentration • Common cause of hyperosmolality in the ED • Metabolism follows zero-order kinetics

Ethanol
Acetate
Acetaldehyde
UGT 1A1 UGT 2B7 SULTs
Ethylsulfate (EtS) Ethylglucuronide (EtG)
ADH1B ADH1C
ALDH2
CYP2E1
Urine ~ 80 hours Urine ~ 80 hours
Serum ~ 3.5 hours
Ethanol Metabolism

Ethanol Measurement
• Enzymatic methods – alcohol dehydrogenase • CH3CH2OH CH3CHO
• ADH is selective but not specific for ethanol, although current assays have minimal reactivity with non-ethanol alcohols
• Other enzymes that involve NADH can potentially interfere (ie: lactate, LD)
• Other methods - Headspace GC-MS
NAD+
ADH
NADH 340 nm

• Toxicity if primarily related to metabolites: – Ethanol → Acetaldehyde → Acetate – Isopropanol → Acetone – Methanol → Formaldehyde → Formic Acid – Ethylene Glycol → Oxalate and Hippuric Acid
• Effects: – Isopropanol (Acetone)- 2X more potent CNS
depressant than ethanol, can cause upper GI bleeding – Methanol – can cause metabolic acidosis, blindness
and death after a latent period of 6-30 hours – Ethylene glycol – same CNS depressant effects as
ethanol but with toxic metabolites – myocardial depression and renal necrosis
Other toxic alcohols

Other toxic alcohols

• measured Osmol – calc. Osmol = osmolal gap • Osmolality = 2(Na in mmol/L) + (Glucose in mg/dL / 18) +
(BUN in mg/dL / 2.8) • Other contributors:
– [ethanol] / 4.6 – [methanol] / 3.2 – [isopropanol] / 6.0 – [ethylene glycol] / 6.2 – [acetone] / 5.8
• Causes: – Methanol – Ethylene Glycol – Diuretics – Isopropanol – Ethanol
Osmolal Gap

Anion Gap
MUDPILES:
• Methanol → formate • Uremia → chronic renal failure (impaired excretion of acids) • Diabetic Ketoacidosis – DKA (also AKA) → acetaldehyde →
acetylCoA → B-hydroxybutyrate, acetoacetate • Paraldehyde, Phenformin, Propylene glycol • Isoniazide → lactic acidosis 2° to seizure activity OR Iron →
lactic acidosis → uncoupling of oxidative phosphorylation • Lactate • Ethylene glycol → glyoxylate, glycolate, oxalate • Salicylates → ketones, lactate
(Na+ + K+) – (Cl- + HCO3-) = 16 (range 10-20)

Ingestion of Alcohols: Lab Findings
Alcohol Osmolal Gap
Metabolic Acidosis with anion gap
Serum Acetone
Urine Oxalate
Ethanol + - - -
Methanol + + - -
Isopropanol + - + -
Ethylene glycol + + - +

• Healthy 50 year-old man was found unconscious in this home, believed to be down for ~24 hours
• Emergency response – GCS 3, vitals normal, oxygen saturation 80%, patient intubated and brought to UCSF ED
• Remarkable lab findings: HCO-3 5, osmolol gap and
anion gap >35, pH 6.7, lactate above the ULOQ, creatinine 2.4
• LFTs, tox screen, APAP and salicylate normal • Normal head and abdominal CT, all cultures negative
no vasopressors required • Patient received IVFs and died before they could start
dialysis
Case Study

Case Study

• Ethanol, methanol or ethylene glycol?
• Ethanol, methanol results negative • Ethylene glycol positive 162 mg/dL, range of
toxic doses – 50 -775 mg/dL
Case Study
Alcohol Osmol Gap
Metabolic Acidosis with anion gap
Serum Acetone
Urine Oxalate
Ethanol + - - -
Methanol + + - -
Isopropanol + - + -
Ethylene glycol + + - +

• Analgesic and antipyretic • Peak concentrations – 4 hours post-ingestion • Normal half-life 2-3 hours; >4 hours hepatic
toxicity; >12 hours hepatic coma likely • Acute liver damage threshold; adults 150-250
mg/kg • Children under the age of 10 more resistant to
toxicity • Measured by enzymatic / colorimetric methods • Antidote is N-acetylcysteine
Acetaminophen (Tylenol)
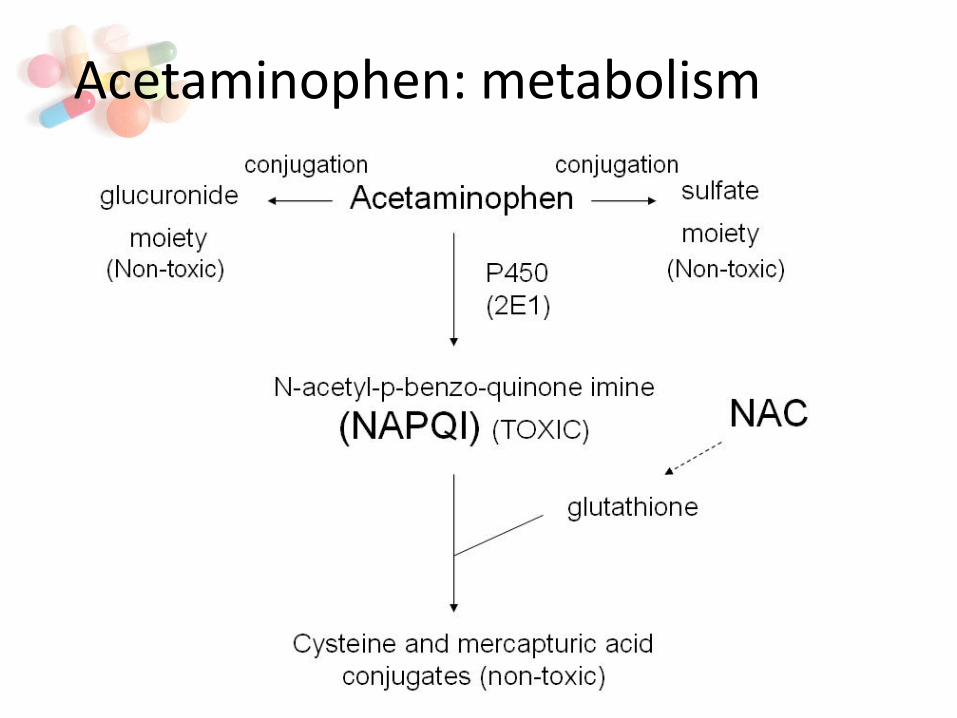
Acetaminophen: metabolism

Acetaminophen: hepatic toxicity

Salicylate (Aspirin) • Analgesic, antipyretic and anti-inflammatory • Therapeutic dose – single dose – 10 mg/kg; daily dose
– 40-60 mg/kg • Mild intoxication – 150-200 mg/kg; severe intoxication
– 300-500 mg/kg; chronic toxicity - >100 mg/kg/day • Lab results reveal mixed metabolic acidosis /
respiratory alkalosis • Tinnitus, hyperthermia, hyperventilation, CNS • Measured by enzymatic / colorimetric methods • Treatment of salicylate overdose
– Hydration, glucose, K+ supplements, bicarbonate, hemodialysis
• Most common cause of fatal poisonings – smoke inhalation
• Colorless, odorless, tasteless gas • Has 240x the affinity for hemoglobin than oxygen
→ carboxyhemoglobin (COHb) • Symptoms begin at COHb levels of 10-20% and
50% can be fatal • Nonsmokers – 1-2% COHb, smokers 5-6% COHb • Treatment: fresh air, 100% O2 or hyperbaric
oxygen may be indicated
Carbon Monoxide

Wavelength (nm)
Abso
rban
ce →
methemoglobin
oxyhemoglobin
reduced hemoglobin
carboxyhemoglobin
UV Absorption of Hb forms
Comparison of absorbencies at different wavelengths allows estimation of the relative concentrations of different forms of hemoglobin beer-lambert law – A = ɛbc or A = ɛ1bc1 + ɛ2bc2 + ɛ3bc3 ….

Lead Poisoning • Demyelinates nerve fibers • Inhibits Fe incorporation into
heme • Chronic lead poisoning
causes hypochromic anemia, with basophilic stippling
• Treatment – chelation – EDTA • Laboratory Test – whole
blood – ICP-MS, atomic absortion, anodic stripping voltammetry
• Erythrocyte protoporphyrin is not sensitive to low level Pb exposure, but is a definitive marker of acute exposure source: www.aafp.org

Iron Poisoning • Approximately 5,000 case per year – mostly children • Toxicity of related to the dose of elemental iron • Treatment:
– Serial monitoring of serum iron – Obtain creatinine, electrolytes, hemoglobin, PT, LFTs and arterial
blood gases – Calculate elemental iron dose ingestion; 20-60 mg Fe/kg
moderate risk; >60 mg/kg high risk – <350 μg/dL and no symptoms – supportive care – >300 μg/dL and symptoms – deferoxamine infusion
Compound Elemental Iron
Ferrous sulfate (hydrate) 20%
Ferrous fumarate 33%
Ferrous gluconate 12%
Ferrous chloride (hydrate) 28%
Ferric chloride (hydrate) 20%

1. Which toxidrome is characterized by Salivation, Lacrimation, Urination, Diarrhea, GI upset, Emesis – “SLUDGE”?
a) Anticholinergic b) Cholinergic c) Sympatomemetic d) Sedative-hypnotic
2. A blood ethanol concentration of 130 mg/dL will contribute how much to a serum osmolality?
a) 2.8 mOsm/kg b) 3.5 mOsm/kg c) 28 mOsm/kg d) 35 mOsm/kg e) 280 mOsm/kg
3. By what mechanism does N-acetylcystine help prevent hepatic damage in acetaminophen overdose?
a) Blocks absorption of acetaminophen b) Provides a source of glutathione c) Prevents hepatic conjugation of acetaminophen d) Blocks acetaminophen receptors on hepatocytes e) Forms an in active complex with acetaminophen
Self-Assessment Questions


















