
Evaluation of Florida’s...Project 4 Final Interim Report ... approaches with utilization...
49
Contract MED180 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration: Project 4 Final Interim Report Contract Deliverable No. 23, Managed Medical Assistance Final Interim Report – Project 4 DY11: Component 6 Dual Eligibles Presented to: Prepared by: Department of Health Outcomes and Biomedical Informatics College of Medicine University of Florida and Department of Behavioral Sciences and Social Medicine College of Medicine Florida State University June 24, 2019
Transcript of Evaluation of Florida’s...Project 4 Final Interim Report ... approaches with utilization...

Contract MED180
Evaluation of Florida’s
Managed Medical Assistance (MMA) Program
Demonstration:
Project 4 Final Interim Report
Contract Deliverable No. 23, Managed Medical Assistance
Final Interim Report – Project 4 DY11: Component 6 Dual Eligibles
Presented to:
Prepared by:
Department of Health Outcomes and Biomedical Informatics
College of Medicine
University of Florida
and
Department of Behavioral Sciences and Social Medicine
College of Medicine
Florida State University
June 24, 2019

Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
Table of Contents
Executive Summary ............................................................................................................... 1
Overview .................................................................................................................................... 1
Key Findings .............................................................................................................................. 2
Introduction .......................................................................................................................... 5
Background ........................................................................................................................... 5
Components, Research Questions, and Hypotheses ............................................................... 5
Data and Methods ................................................................................................................. 6
Results ................................................................................................................................ 10
Research Question 6A ..............................................................................................................10
Research Question 6B ..............................................................................................................13
Research Question 6C ..............................................................................................................27
Conclusion and Recommendations ...................................................................................... 39
Appendix 1. DY11 MMA Evaluation Components and Research Questions ........................... 41

Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
List of Tables
Table 1. Component 6 - MMA Plans Included in Health Plan Key Informant Survey ................................... 8 Table 2. Behavioral Health and Non-Emergency Transportation in Medicaid in DY11: Dual-Eligible
Encounters and Amounts Paid ................................................................................................................... 10 Table 3. Behavioral Health and Non-Emergency Transportation in Medicaid in DY11: Dual Eligible
Encounters and Amounts Paid Per User Per Encounter ............................................................................ 12 Table 4. Dual-Eligible Membership (Medicaid and Medicare) as of December 31, 2018........................... 14 Table 5. Case Management Practices ........................................................................................................ 15 Table 6. Reasons for Encounter Data Review ............................................................................................ 15 Table 7. Member Outreach Practices ......................................................................................................... 16 Table 8. Disease Management Programs .................................................................................................. 17 Table 9. Other Care Coordination Strategies .............................................................................................. 18 Table 10. Dual-Eligible Membership (Medicare and Medicaid) as of December 31, 2018 ........................ 20 Table 11. Call Center Information ............................................................................................................... 20 Table 12. Reported NET Services Complaints ........................................................................................... 21 Table 13. Number of NET Complaints Received ........................................................................................ 21 Table 14. Types of Complaints ................................................................................................................... 21 Table 15. Case Manager NET Coordination Strategies ............................................................................. 22 Table 16. Transportation Coordinator NET Coordination Strategies .......................................................... 23 Table 17. Transportation Network Sufficiency Strategies ........................................................................... 23 Table 18. Types of Applications Used to Provide NET Services ................................................................ 24 Table 19. Functions of Applications Used to Provide NET Services .......................................................... 24 Table 20. Types of Performance Measures Used to Evaluate NET Services ............................................ 25 Table 21. Dual-Eligible Telephone Survey – Respondent Demographics ................................................. 28 Table 22. Dual-Eligible Telephone Survey – Self-Reported Mental Health Status..................................... 29 Table 23. Dual-Eligible Telephone Survey – Self-Reported Functional Status .......................................... 30 Table 24. Dual-Eligible Telephone Survey – Need For and Utilization of BH Services .............................. 32 Table 25. Dual-Eligible Telephone Survey Access to and Timeliness of BH Services............................... 33 Table 26. Dual-Eligible Telephone Survey – Person-Centered BH Care ................................................... 34 Table 27. Dual-Eligible Telephone Survey – Managed BH Care................................................................ 35 Table 28. Dual-Eligible Telephone Survey – Experiences with NET Services ........................................... 37

Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
List of Figures
Figure 1. Dual-Eligible Telephone Survey – Percentage of Respondents Rating their BH Care a “9” or
“10” .............................................................................................................................................................. 35
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
List of Acronyms
AA Alcoholics Anonymous
AHCA Agency for Health Care Administration
BH Behavioral Health
CMS Centers for Medicare and Medicaid Services
CAHPS Consumer Assessment of Healthcare Providers and Systems
CATI Computer Assisted Telephone Interviewing
DY Demonstration Year
ED Emergency Department
ECHO Experience of Care & Health Outcomes
HEDIS Healthcare Effectiveness Data and Information Set
HCPCS Healthcare Common Procedure Coding System
LTC Long-term care
MBHO Managed Behavioral Health Organization
MMA Managed Medical Assistance
MPT Mental Health Utilization
NAMI National Alliance on Mental Illness
NA Narcotics Anonymous
NET Non-Emergency Transportation
P&P Policies and Procedures
RQ Research Question
SMMC Statewide Medicaid Managed Care
SFY State Fiscal Year
UFSRC University of Florida Survey Research Center

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
1
Executive Summary
Overview
This report presents the Demonstration Year 11 (DY11), SFY 2016-17, results of the impact of Florida’s Managed Medical Assistance (MMA) program on Medicare-Medicaid dual-eligible enrollees. This report covers Project 4 of the MMA evaluation, one of the four projects comprising the Florida MMA Program Evaluation conducted by the Department of Health Outcomes and Biomedical Informatics of the College of Medicine at the University of Florida, the Department of Behavioral Sciences and Social Medicine of the College of Medicine at Florida State University, and the Department of Health Services Administration of the University of Alabama-Birmingham.
Project 4 consists of one component (Component 6), “The impact of efforts to align with Medicare and improving beneficiary experiences and outcomes for dual-eligible individuals”.
Component 6 contains three research questions designed to examine access, utilization and quality of care in behavioral health (BH) and non-emergency transportation (NET) services among dual-eligible enrollees. It should be noted that dual-eligible enrollees receive most of their health care through Medicare. At the time this evaluation was designed, the Center for Medicare and Medicaid Services had not released any Medicare Advantage encounter data to researchers, so only a limited picture of total dual-eligible utilization was available. BH and NET services were chosen as the scope of this report because Medicaid pays for most (but not all) of these services; therefore, the lack of Medicare Advantage encounter data will have less of an impact on analyses of dual-eligible enrollees’ utilization of these services. Cost analyses were included to provide a more comprehensive evaluation of service utilization. Behavioral health services include individual, group or family behavioral therapy and substance abuse services provided by trained and licensed specialists to recipients diagnosed with behavioral health, substance use and co-occurring behavioral-health disorders. Project 4 uses quantitative analyses of Medicaid encounter data for dual-eligibles, telephone surveys of dual-eligibles regarding their Medicaid experiences, and qualitative analyses of dual-eligible documents and key informant interviews. Descriptive quantitative results consist of means and rates for the use and costs of BH and NET services for dual-eligible enrollees and non-dual-eligible enrollees obtained from DY11. MMA encounter data and the Florida Statewide Medicaid Enrollment Report. Additional results are based on a combination of MMA health plan surveys along with a telephone survey of MMA dual-eligible enrollees. More details on both the quantitative and qualitative methods can be found in the body of this report.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
2
Key Findings
Use and Cost of Services
The January 2017 Florida Statewide Medicaid Enrollment Report indicates that 228,440 dual- eligible individuals were enrolled in the MMA program.1 The evaluation team calculated behavioral health and non-emergency transportation encounters and amounts paid2 per user and per encounter during DY11 for both dual-eligible and non-dual-eligible users of these services.
For BH services in DY11:
• Dual-eligibles have lower dollars per user compared to non-dual-eligibles ($389.65 vs. $1563.86, respectively).
• Both dollars per encounter and encounters per user are lower for dual-eligibles compared to non-dual-eligibles ($81.80 vs. $144.51 and 4.76 vs. 10.82, respectively).
• Both dollars per encounter and encounters per user contribute to the lower dollars per user for dual-eligibles.
For NET services in DY11:
• Dual-eligibles have higher dollars per user than non-dual-eligibles ($512.35 vs. $270.93, respectively).
• Dollars per encounter are lower for dual-eligibles ($56.72 vs. $72.24) while encounters per user are higher for dual-eligibles (9.03 vs. 3.75).
• The higher number of NET encounters per user outweighed the lower NET dollars per encounter to result in higher NET dollars per user for dual users.
To summarize, the data show that:
• Dual-eligible users are using fewer BH services and those services have lower costs per service compared to non-dual-eligible users.
• Dual-eligible users are using more transportation services, but those services have lower costs per use compared to non-dual-eligible users.
Access to Services and Quality of Care
To assess access to care, quality of care, and customer satisfaction, surveys of dual-eligible enrollees and key informants that included health plan experts and their contracted BH providers and NET vendors were conducted. The results of these surveys are discussed below.
Surveys with key informants revealed several challenges to coordinating BH and NET services:
• More plans reported difficulty with coordinating BH services than NET services.
• Not having updated contact information created a challenge for coordination of care, sometimes because the member did not give accurate information to the Department
1 http://www.fdhc.state.fl.us/medicaid/Finance/data_analytics/enrollment_report/index.shtml , January 2017, Worksheet DISTRICT_TANF_SSI, MMA Duals Total column. 2 While RQ 6A focuses on utilization counts, different BH and NET encounters require different amounts of resources (e.g., longer distance NET services use more resources than shorter distance NET services). Therefore, in addition to examining utilization counts, the evaluation team also weighted each BH and NET encounter by the amounts paid for each encounter to create a resource-weighted measure of utilization.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
3
of Children and Families when enrolling or when contact information changes and is not updated in the system.
• Reviewing encounters to facilitate case management was also sometimes difficult for BH service provision by MMA plans because two separate systems are used to process encounters one for medical and the other for BH, requiring more time to compile needed information.
• The lag time between service provision and encounters submission in encounters data gives a delayed picture of services needed, making coordination challenging.
• In some situations, for members who have a Medicare plan owned by a different parent company than the MMA plan, the Medicare plan is unwilling to share any BH information (including encounters) due to HIPAA regulations.
• Some plans or behavioral health organizations (BHOs) do not know which Medicare providers are providing services to the members, or a big time lag is experienced in the response of these providers, which can result in incomplete or delayed information needed to optimize coordination of care.
• For the provision of NET services, challenges are also encountered when the Medicare provider information is unknown by the MMA plans or NET vendors, also potentially resulting in incomplete information.
The key informant surveys also revealed several possible best practices for coordinating BH and NET services for dual-eligible members:
• For improving access to and quality of BH services, MMA plans should consider a comprehensive case management strategy that interfaces traditional case management approaches with utilization management, performance measures, member education, member and family engagement, and linkage to community resources and peer supports. Efforts to integrate BH and physical health services may include working with hospital case managers for discharge planning, establishing behavioral health homes at community mental health centers, and working with Medicare plans to share information on members. Obtaining access to systems such as the Homeless Management Information System (HMIS) can facilitate member location.
• For improving access to and quality of NET services, MMA plans should consider strategies that focus on transportation vendors and providers, including regular vendor oversight and case management communication with vendors. Establishing transportation coordinators and setting up three-way calls with members, case managers, and transportation providers can help to address immediate transportation needs. Technological innovations that involve mobile applications show promise for connecting members, medical providers, and transportation providers and coordinating NET services in real-time. Encouraging members to select a preferred provider and reuse that provider with regular appointment times scheduled improves service, as does the use of ridesharing. To improve NET network adequacy, MMA plans should consider using secondary or contingency transportation providers. For dual-eligible members, efforts should ensure that specialized vehicles and equipment are adequate in number and quality.
Telephone surveys revealed that dual-eligible enrollees had generally positive experiences and satisfaction with the BH and NET services provided by MMA standard and MMA specialty plans. Enrollees are generally getting the BH care they need and reporting positively about

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
4
communication with their BH service provider. Some areas for improvement include ensuring that needed BH services are fully covered by health plans (which may involve better coordination with Medicare plans), helping specialty plan members receive BH services when health plan approval is needed, and improving the timeliness of NET services in picking up enrollees after their scheduled appointments.
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
5
Introduction
This report presents the Demonstration Year 11 (DY11), SFY 2016-17, results for Project 4, one of the four projects comprising the Florida Medicaid Managed Medical Assistance (MMA) Program Evaluation conducted by the Department of Health Outcomes and Biomedical Informatics of the College of Medicine at the University of Florida, the Department of Behavioral Sciences and Social Medicine of the College of Medicine at Florida State University, and the Department of Health Services Administration of the University of Alabama-Birmingham.
Project 4 consists of one component (Component 6), “The impact of efforts to align with Medicare and improving beneficiary experiences and outcomes for dual eligible individuals”.
Component 6 contains three research questions designed to examine access, utilization and quality of care in behavioral health (BH) services (e.g., behavioral therapy and substance use services) and non-emergency transportation (NET) services (e.g., transportation to doctors’ appointments) among dual-eligible enrollees. These two types of services were chosen because Medicaid pays for most (but not all) of these services. The research questions for Project 4, Component 6 are presented below. All the components and research questions for the DY11 MMA evaluation can be found in Appendix 1 to this report.
Background
In 2011, The Florida Legislature directed Florida’s Agency for Health Care Administration (the Agency) to create the Statewide Medicaid Managed Care (SMMC) Program designed to (1) provide integrated health care to Florida’s Medicaid enrollees through a uniform statewide program of access to providers and health services; (2) emphasize patient-centered care delivered through alternative delivery models that promote personal responsibility and active patient participation, and (3) implement innovative reimbursement methodologies that emphasize health plan accountability and quality. The two components of the SMMC program, the Long-term care (LTC) program and the Managed Medical Assistance (MMA) program, began operation under a section 1915(b) (c) combination waiver in July 2013 (LTC) and a section 1115 demonstration waiver in July 2014 (MMA), both waivers granted by the Centers for Medicare and Medicaid Services (CMS). Federal CMS approved a second extension of the MMA 1115 waiver demonstration for a period of five years beginning August 3, 2017 through June 30, 2022.
To comply with the CMS requirement for an independent contractor to evaluate the SMMC Demonstration Program, the Agency contracted with the Department of Health Outcomes and Biomedical Informatics in the College of Medicine at the University of Florida in December 2016. The University of Florida, in turn, established subcontracts with the Florida State University Department of Behavioral Sciences and Social Medicine, and the University of Alabama Birmingham Department of Health Services Administration to provide additional expertise in evaluating Florida’s MMA program.
Components, Research Questions, and Hypotheses
For DY11 (SFY 2016-17), Project 4 consists of Component 6 and its associated research questions and hypotheses as listed below.
Component 6. The impact of efforts to align with Medicare and improving beneficiary

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
6
experiences and outcomes for dual eligible individuals.
6A. How many MMA enrollees are also Medicare recipients (dual-eligibles) and to what extent do dual-eligible enrollees utilize behavioral health (BH) and non-emergency transportation services (NET)?
Research Question 6A is included to provide context (descriptive information) for this Component, so there is no hypothesis to be tested for this question.
6B. What specific care coordination strategies and practices are most effective for ensuring access to and quality of care for behavioral health services and non-emergency transportation services for dual-eligible enrollees?
6C. How do dual-eligible enrollees rate their experience and satisfaction with the delivery of
care they received related to behavioral health and non-emergency transportation services?
Research Questions 6B and 6C will be answered using survey and qualitative methods; they are exploratory and descriptive in nature so there are no hypotheses to be tested.
Data and Methods
Project 6 employed both quantitative and survey/qualitative analyses to address the research questions in Component 6. Analyses related to dual-eligible health care use were limited by the lack of availability of Medicare Advantage encounter data. Consequently, only a limited picture of total dual-eligible utilization was available. BH and NET services were chosen specifically because these services for dual-eligible enrollees are funded mostly by Medicaid.
Quantitative: Descriptive Statistics (RQ 6A)
RQ 6A examined the total number of BH and NET encounters and amounts paid for MMA users by dual-eligibility status along with encounters per users and amounts paid per user by dual-eligibility status3. In addition, the amount paid per user was broken into amount paid per encounter and the number of encounters per user for both BH and NET services across dual-eligibility status to measure the contribution of each component to the amount paid per user for these services.
Surveys and Qualitative Interviews of MMA Health Plans (RQ 6B)
Surveys of MMA Health Plans Experts in care coordination at the MMA health plans were identified to participate in a survey about NET and BH care coordination strategies and practices. The survey was predominantly structured with closed-ended questions with a limited number of open-ended questions expected to elicit a brief answer. Two instruments were developed by the study team based on previous qualitative research done under this evaluation on care coordination practices of health plans providing BH and NET services to dual-eligible enrollees. One instrument, based on care coordination of NET services, includes questions about:
1) Dual-eligible membership counts including those enrolled in Medicare fee-for-service,
3 Utilization for non-dual-eligibles was included to provide context and a frame of reference for the dual-eligible
utilization statistics.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
7
Medicare Advantage plans (both owned and not owned by the same parent company as owns the MMA plan), and those receiving NET services;
2) NET systems and structures including call center characteristics and complaint handling procedures;
3) NET service coordination including identifying the employee roles who are responsible for this coordination and the specific strategies used;
4) NET network adequacy including strategies used to ensure sufficient providers and specialized vehicles and equipment;
5) NET technological applications including the types and functions of the applications;
6) NET vendor oversight including performance measures, and mode and content of communication with vendors;
7) NET service plan opinions including the most effective care coordination strategies and ease of coordination.
The survey form instructs the health plan to include their NET vendor when answering questions in the sections about NET systems and structures, NET service coordination, NET network adequacy, and NET technological applications. The other instrument, based on care coordination of BH services, includes questions about:
1) Dual-eligible membership counts including those enrolled in Medicare fee-for-service, Medicare Advantage plans (both owned and not owned by the same parent company as owns the MMA plan), and those receiving BH services;
2) BH case management issues including criteria for case manager assignment, case management practices, use of encounters data reviews, member outreach practices, care coordination activities related to hospitalized members, and care coordination goal measures;
3) Case coordination strategies for behavioral and physical health integration including member access to a BH home, reliability of access to members’ Medicare data who use BH services, and specific coordination questions based on whether the member’s Medicare plan is owned by the same parent company as owns the MMA plan;
4) Disease management issues related to members receiving BH services including specific disease program availability and strategies used to address changes in behavioral health symptoms;
5) Additional strategies used to coordinate the care of members receiving BH services; and
6) BH service plan opinions including the most effective care coordination strategies and ease of coordination.
The survey form instructs the health plan to include their contracted behavioral health organization when answering the questions unless the health plan provides the services directly.
The Agency approved a list of 11 MMA standard plans and 4 MMA specialty plans to be included in the MMA health plan survey. Of the 6 MMA specialty plans statewide, two were excluded because they were specific to children and did not cover the dual-eligible population to be studied in this evaluation (Children’s Medical Services and Sunshine Child Welfare). In

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
8
addition, Positive Healthcare declined to participate in the MMA health plan survey, resulting in a total of 14 health plans (11 standard and 3 specialty) included in the surveys and analysis as shown in Table 1.
Table 1. Component 6 - MMA Plans Included in Health Plan Key Informant Survey
MMA Standard Plans MMA Specialty Plans
1. Aetna 1. Clear Health Alliance
2. Community Care Plan 2. Freedom Health
3. Humana Medical Plan 3. Magellan Complete Care
4. Molina Healthcare
5. Prestige Health Choice
6. Simply Healthcare
7. Staywell
8. Sunshine Health Plan
9. United Health
10. Amerigroup
11. Better Health
Each plan’s contract manager assisted the investigators in identifying and contacting the appropriate experts in BH and NET services for the surveys. Identified experts received an email that explains the purpose of the study with a form-fillable PDF containing the survey questions attached to the email. The MMA plan experts were asked to email the completed PDF form to the study team.
Follow-Up Qualitative Interviews of Health Plans (as needed). The research team reviewed the MMA plan’s responses to the closed-ended survey questions in PDF format. These reviews generated follow-up questions and points of clarification tailored to each specific health plan. Follow-up emails and/or telephone interviews were conducted with the same experts who were initially contacted and who provided the written PDF responses, and appropriate individuals who are knowledgeable in the areas of interest as designated by the plans. Interviews were conducted by trained interviewers by telephone, audio recorded, and transcribed for analysis if needed. The content of each health plan’s answers were integrated into the survey answers given by that health plan in the PDF surveys.
Component 6 Member Survey Aim: Using a structured telephone survey, the evaluation team assessed experiences and satisfaction with BH care and NET services received by dual-eligible members in MMA standard and MMA specialty plans (RQ 6C).
RQ 6C – Dual-Eligible Member Telephone Survey. The study team developed a structured telephone survey administered to dual-eligible members in MMA standard and MMA specialty plans, addressing experiences and satisfaction with coordination of behavioral health and non-emergency transportation services. The survey tool includes questions from:
1) The Consumer Assessment of Healthcare Providers and Systems (CAHPS) Experience of Care & Health Outcomes (ECHO) survey, including items addressing access, timeliness, utilization, and satisfaction with BH phone counseling, urgent BH care, general BH care, prescription BH care, and managed BH care;
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
9
2) The CAHPS Health Plan Survey for Medicaid (Version 4) Supplemental Item set, including items addressing access to health plan transportation;
3) The Florida Medicaid Non-Emergency Transportation (NET) Survey, originally developed by the University of South Florida and modified for use in this study, including items addressing timeliness, safety, and satisfaction with NET services;
4) The Medicare Current Beneficiary Survey, including items addressing comparative health, chronic medical impairments, and activities of daily living; and
5) Items developed by the University of Florida to collect sociodemographic characteristics, including race/ethnicity, marital status, housing, and language.
The sample for the survey included dual-eligible members in any of the 11 MMA standard plans or 3 MMA specialty plans listed in Table 1 above as well as those dual-eligible members in Positive Healthcare, a specialty MMA plan 4. The sample was stratified into two quotas, targeting 100 completed surveys among MMA standard plan members (the 11 MMA standard plans combined) and 100 completed surveys among MMA specialty plan members (the 4 MMA specialty plans combined). The sampling plan required members to:
1) be dual-eligible and 18 years of age or older at the time of sampling;
2) have been enrolled in the same MMA plan continuously in the 12 months between January 2018 and December 2018;
3) have received BH services during the 12-month continuous enrollment period, as defined by numerator specifications for any of three Healthcare Effectiveness Data and Information Set (HEDIS) measures:
a. Mental Health Utilization (MPT) – Outpatient/ED, Intensive Outpatient/Partial Hospitalization
b. Identification of Alcohol and Other Drug Services – Outpatient/ED, Intensive Outpatient/Partial Hospitalization
c. Initiation and Engagement of Alcohol or Other Drug Dependence Treatment (IET) – 18+ years; and
4) have received NET services during the 12-month continuous enrollment period, as identified using the following Healthcare Common Procedure Coding System (HCPCS) codes for NET services: A0080 to A0210, A0426, A0428, S0215, T2001 to T2005, and T2049.
One week prior to survey fielding, the study team mailed advance letters to all sampled members, explaining the purpose of the study and informing them that they would be receiving a telephone call to participate in a survey for a research study. The letters identified the Agency and the University of Florida as the agencies conducting the study, informed members that participation in the survey was voluntary, and provided contact information for the University of Florida Survey Research Center (UFSRC) and study director.
Telephone surveys were conducted by trained UFSRC interviewers using a computer-assisted telephone interviewing (CATI) system. During the first two weeks of fielding, the study team
4 Positive Healthcare did not participate in the health plan expert surveys or interviews, but their dual-eligible
enrollees did participate in the telephone survey of dual-eligibles. Consequently, enrollees from four specialized plans (the three listed in Table 1 and Positive Healthcare) participated in the dual-eligible telephone interviews.
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
10
conducted in-person quality monitoring of telephone surveys, and provided feedback to UFSRC managers as needed. The survey had the option to be completed by sampled members or (in cases where the member was physically or mentally unable to participate) by proxy respondents (such as family members) who were familiar with the member’s health and health care. Participants also had the option to complete the surveys in English or Spanish.
Telephone survey data were analyzed by the study teams using Statistical Package for the Social Sciences (SPSS Version 23).
Results
Component 6. The impact of efforts to align with Medicare and improving beneficiary experiences and outcomes for dual eligible individuals.
Research Question 6A
How many MMA enrollees are also Medicare recipients (dual-eligibles) and to what extent do dual-eligible enrollees utilize behavioral health and non-emergency transportation services?
For this research question, descriptive statistics were used and therefore, no hypothesis was tested.
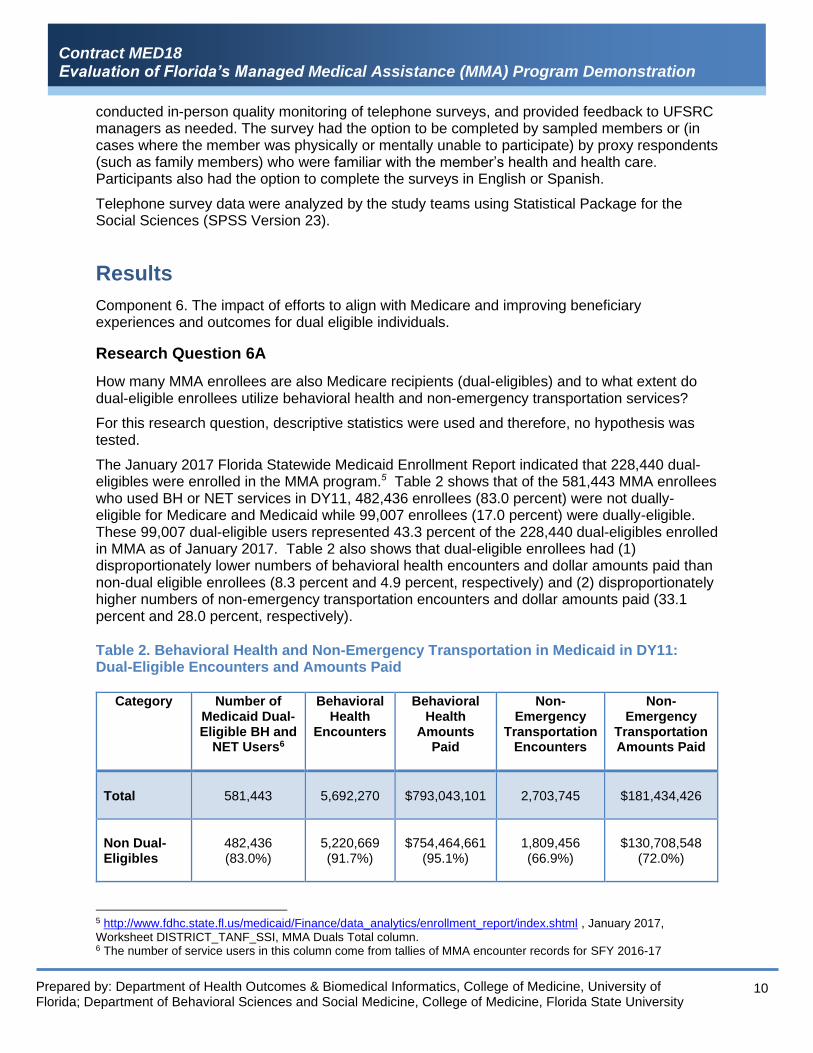
The January 2017 Florida Statewide Medicaid Enrollment Report indicated that 228,440 dual- eligibles were enrolled in the MMA program.5 Table 2 shows that of the 581,443 MMA enrollees who used BH or NET services in DY11, 482,436 enrollees (83.0 percent) were not dually-eligible for Medicare and Medicaid while 99,007 enrollees (17.0 percent) were dually-eligible. These 99,007 dual-eligible users represented 43.3 percent of the 228,440 dual-eligibles enrolled in MMA as of January 2017. Table 2 also shows that dual-eligible enrollees had (1) disproportionately lower numbers of behavioral health encounters and dollar amounts paid than non-dual eligible enrollees (8.3 percent and 4.9 percent, respectively) and (2) disproportionately higher numbers of non-emergency transportation encounters and dollar amounts paid (33.1 percent and 28.0 percent, respectively).
Table 2. Behavioral Health and Non-Emergency Transportation in Medicaid in DY11: Dual-Eligible Encounters and Amounts Paid
Category Number of Medicaid Dual-Eligible BH and
NET Users6
Behavioral Health
Encounters
Behavioral Health
Amounts Paid
Non-Emergency
Transportation Encounters
Non-Emergency
Transportation Amounts Paid
Total 581,443 5,692,270 $793,043,101 2,703,745
$181,434,426
Non Dual-Eligibles
482,436 (83.0%)
5,220,669 (91.7%)
$754,464,661 (95.1%)
1,809,456 (66.9%)
$130,708,548
(72.0%)
5 http://www.fdhc.state.fl.us/medicaid/Finance/data_analytics/enrollment_report/index.shtml , January 2017, Worksheet DISTRICT_TANF_SSI, MMA Duals Total column. 6 The number of service users in this column come from tallies of MMA encounter records for SFY 2016-17

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
11
Category Number of Medicaid Dual-Eligible BH and
NET Users6
Behavioral Health
Encounters
Behavioral Health
Amounts Paid
Non-Emergency
Transportation Encounters
Non-Emergency
Transportation Amounts Paid
Dual-Eligibles
99,007 (17.0%)
471,601 (8.3%)
$38,578,439 (4.9%)
894,289 (33.1%)
$50,725,878
(28.0%)
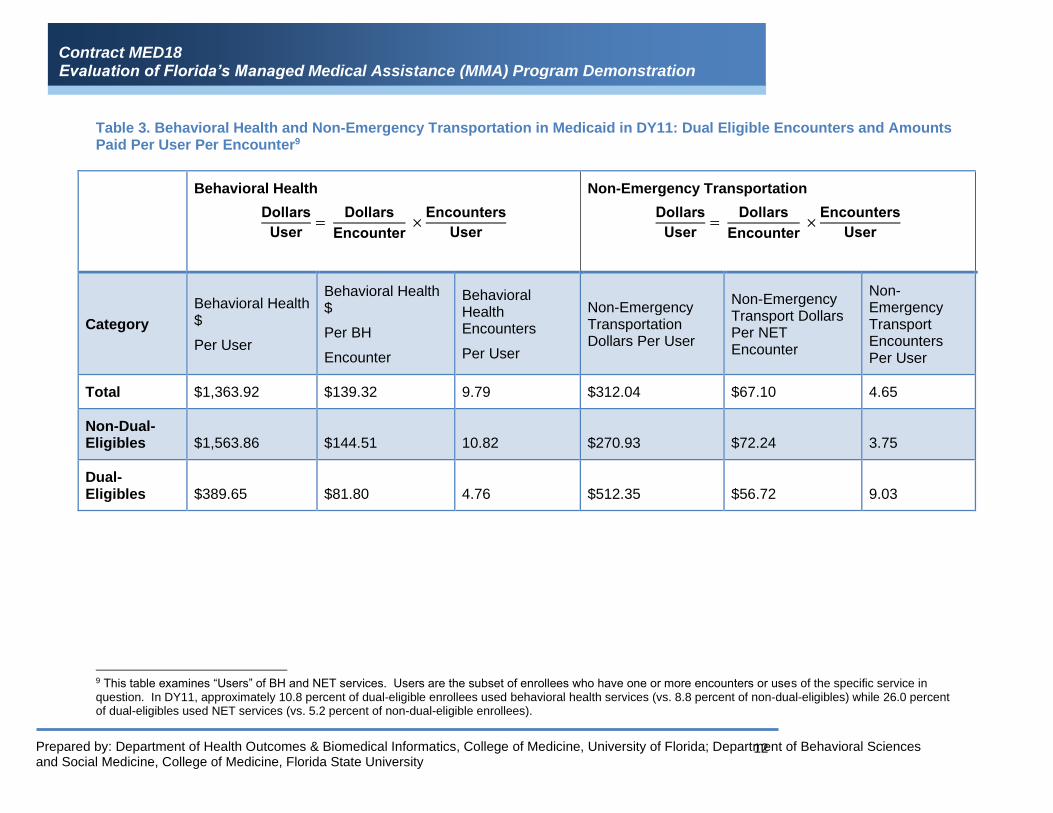
Table 3. Behavioral Health and Non-Emergency Transportation in Medicaid in DY11: Dual Eligible Encounters and Amounts Paid Per User Per EncounterTable 3 uses the data from Table 2 to calculate behavioral health and non-emergency transportation (1) dollar amounts paid per user7,8 (2) dollar amounts paid per encounter, and (3) encounters per user during DY11. The header and columns of Table 3 show how dollars per user equals the product of dollars per encounter and encounters per user; i.e.
Dollars
User=
Dollars
Encounter ×
Encounters
User
By breaking dollars per users into its two component parts and examining differences between dual-eligibles and non-dual-eligibles, the relative contributions of the two component parts to the differences in dollars per user can be assessed.
Examining the last two rows in Table 3 shows that dual-eligibles have lower behavioral health amounts paid per enrollee ($389.65 vs. $1,563.86, respectively) along with lower behavioral health amounts paid per encounter ($81.80 vs. $144.51) and lower behavioral health encounters per user (4.76 versus 10.82) compared to non-dual-eligibles. In other words, the two component parts of behavioral health dollars per user both contribute to the lower dollars per user seen for behavioral health services for dual-eligibles.
By contrast, dual-eligibles had higher NET amounts paid per user ($512.35 vs. $270.93) along with lower NET amounts paid per encounter ($56.72 vs. $72.24, respectively) and higher NET encounters per user (9.03 vs. 3.75) compared to non-dual-eligible users. For NET services provided to dual-eligibles, the higher number of NET encounters per user outweighed the lower NET dollars per encounter to result in higher NET dollars per user.
7 The term “user” here refers to the subset of enrollees who consume one or more units of the service in question. 8 The dollars per user and per encounter, along with the encounters per user, are average amounts across all
encounters and users, and therefore represent the expected or typical amounts per user and per encounter.
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
12
Table 3. Behavioral Health and Non-Emergency Transportation in Medicaid in DY11: Dual Eligible Encounters and Amounts Paid Per User Per Encounter9
Behavioral Health
Dollars
User=
Dollars
Encounter ×
Encounters
User
Non-Emergency Transportation
Dollars
User=
Dollars
Encounter ×
Encounters
User
Category
Behavioral Health $
Per User
Behavioral Health $
Per BH
Encounter
Behavioral Health Encounters
Per User
Non-Emergency Transportation Dollars Per User
Non-Emergency Transport Dollars Per NET Encounter
Non-Emergency Transport Encounters Per User
Total $1,363.92 $139.32 9.79 $312.04 $67.10 4.65
Non-Dual-Eligibles $1,563.86 $144.51 10.82 $270.93 $72.24 3.75
Dual-Eligibles $389.65 $81.80 4.76 $512.35 $56.72 9.03
9 This table examines “Users” of BH and NET services. Users are the subset of enrollees who have one or more encounters or uses of the specific service in question. In DY11, approximately 10.8 percent of dual-eligible enrollees used behavioral health services (vs. 8.8 percent of non-dual-eligibles) while 26.0 percent of dual-eligibles used NET services (vs. 5.2 percent of non-dual-eligible enrollees).

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
13
To summarize, the data show that dual-eligibles use fewer behavioral health encounters and lower-cost behavioral health encounters than non-dual-eligibles. The data also show that dual-eligibles spend more on NET services because they use more services than non-dual-eligibles. However, dual-eligibles use lower cost NET services on average compared to non-dual-eligibles.
Research Question 6B
What specific care coordination strategies and practices are most effective for ensuring access to and quality of care for behavioral health services and non-emergency transportation services for dual eligible enrollees?
Research Question 6B is a qualitative question and has no hypothesis. To answer this question, the research team sent surveys to the health plans to collect information on their BH and NET coordination strategies and practices used to ensure access and quality of BH and NET services. The surveys were developed based on previous years’ qualitative interviews conducted by this research team with the MMA plans about BH and NET service provision. The surveys were form-fillable pdfs with instructions on including their BHO (if the plan contracts with a BHO), and their NET vendor. This effort focused on the following 11 MMA plans and 3 specialty plans.
MMA Standard Plans
• Aetna
• Amerigroup
• Better Health
• Community Care Plan
• Humana
• Molina
• Prestige
• Simply Health
• Staywell
• Sunshine
• United Healthcare (UHC) MMA Specialty Plans
• Clear Health Alliance
• Freedom Health
• Magellan
Four of the plans are owned by parent company Anthem: Amerigroup, Better Health, Simply Health, and Clear Health Alliance. These plans, also known as Simply Healthcare Plans, adhere to the same policies and procedures and will be treated as one plan group for the purpose of this analysis, for a total of 11 plan groups.
After receiving the responses from the health plans, the research team reviewed the open-ended responses and developed follow-up questions. These follow-up questions were sent by email or asked through a phone interview. Answers to the follow-up questions are incorporated into the analysis.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
14
Behavioral Healthcare Coordination
To obtain a picture of the effective BH care coordination strategies and practices used by the health plans and their contracted BHOs, questions were asked about the number of dual-eligible members, case management, behavioral and physical health integration, disease management, other care coordination strategies, and the health plans’ opinions about aspects of BH care coordination.
Dual-Eligible Membership
The survey asked the health plans to report on the number of dual-eligible members enrolled as well as the number of enrollees in several subgroups of dual-eligible enrollees as of December 31, 2018, as seen in Table 4.
Table 4. Dual-Eligible Membership (Medicaid and Medicare) as of December 31, 2018
Mean Minimum Maximum
Medicare fee-for-service 11,115 0 33,046
Medicare fee-for-service who received BH services during calendar year 2018 2,329 0 19,756
Medicare Advantage Plan 4,740 88 8,036
Medicare Advantage Plan owned by same parent company as MMA plan 1,568 0 8,036
Medicare Advantage Plan owned by different company than MMA plan 3,602 0 23,871
Total dual-eligible members enrolled in MMA plan 13,397 88 40,673
The mean dual-eligible members enrolled in an MMA plan was 13,397. On average, 2,329 dual-eligible members in an MMA plan who were enrolled in Medicare fee-for-service received BH services during calendar year 2018. Eight Plans contracted with a BHO to manage behavioral health services.
Case Management
The use of case management to coordinate care for people receiving BH services was common. The survey asked respondents about case management practices, encounters review, strategies related to member hospitalization, and tracking progress on care coordination goals.
As part of care coordination, seven plans and seven BHOs assigned a case manager to at least some of their dual-eligible members who received BH services. One plan reported that all dual-eligible members were assigned a case manager. The remaining plans that assigned a case manager, or whose BHO assigned a case manager, used criteria such as members who requested a BH case manager, members who were high utilizers of BH services, or those who were high-risk (rapid re-admissions, suicide attempts, or pregnant requiring acute BH services). Additionally, any member who was identified as needing BH services was assigned a case manager, as well as those who were receiving fragmented services, or who had struggled to find a BH provider.
The health plans and their contracted BHOs employed a variety of case management practices
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
15
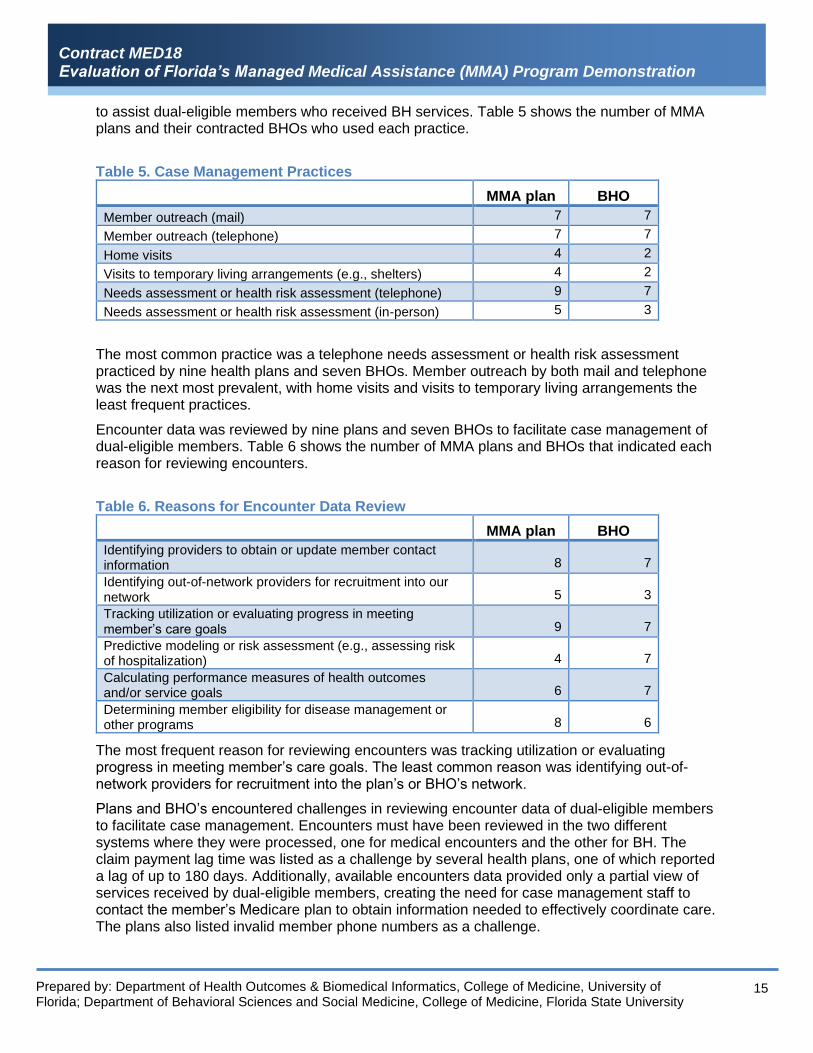
to assist dual-eligible members who received BH services. Table 5 shows the number of MMA plans and their contracted BHOs who used each practice.
Table 5. Case Management Practices
MMA plan BHO
Member outreach (mail) 7 7
Member outreach (telephone) 7 7
Home visits 4 2
Visits to temporary living arrangements (e.g., shelters) 4 2
Needs assessment or health risk assessment (telephone) 9 7
Needs assessment or health risk assessment (in-person) 5 3
The most common practice was a telephone needs assessment or health risk assessment practiced by nine health plans and seven BHOs. Member outreach by both mail and telephone was the next most prevalent, with home visits and visits to temporary living arrangements the least frequent practices.
Encounter data was reviewed by nine plans and seven BHOs to facilitate case management of dual-eligible members. Table 6 shows the number of MMA plans and BHOs that indicated each reason for reviewing encounters.
Table 6. Reasons for Encounter Data Review
MMA plan BHO
Identifying providers to obtain or update member contact information 8 7
Identifying out-of-network providers for recruitment into our network 5 3
Tracking utilization or evaluating progress in meeting member’s care goals 9 7
Predictive modeling or risk assessment (e.g., assessing risk of hospitalization) 4 7
Calculating performance measures of health outcomes and/or service goals 6 7
Determining member eligibility for disease management or other programs 8 6
The most frequent reason for reviewing encounters was tracking utilization or evaluating progress in meeting member’s care goals. The least common reason was identifying out-of-network providers for recruitment into the plan’s or BHO’s network.
Plans and BHO’s encountered challenges in reviewing encounter data of dual-eligible members to facilitate case management. Encounters must have been reviewed in the two different systems where they were processed, one for medical encounters and the other for BH. The claim payment lag time was listed as a challenge by several health plans, one of which reported a lag of up to 180 days. Additionally, available encounters data provided only a partial view of services received by dual-eligible members, creating the need for case management staff to contact the member’s Medicare plan to obtain information needed to effectively coordinate care. The plans also listed invalid member phone numbers as a challenge.
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
16
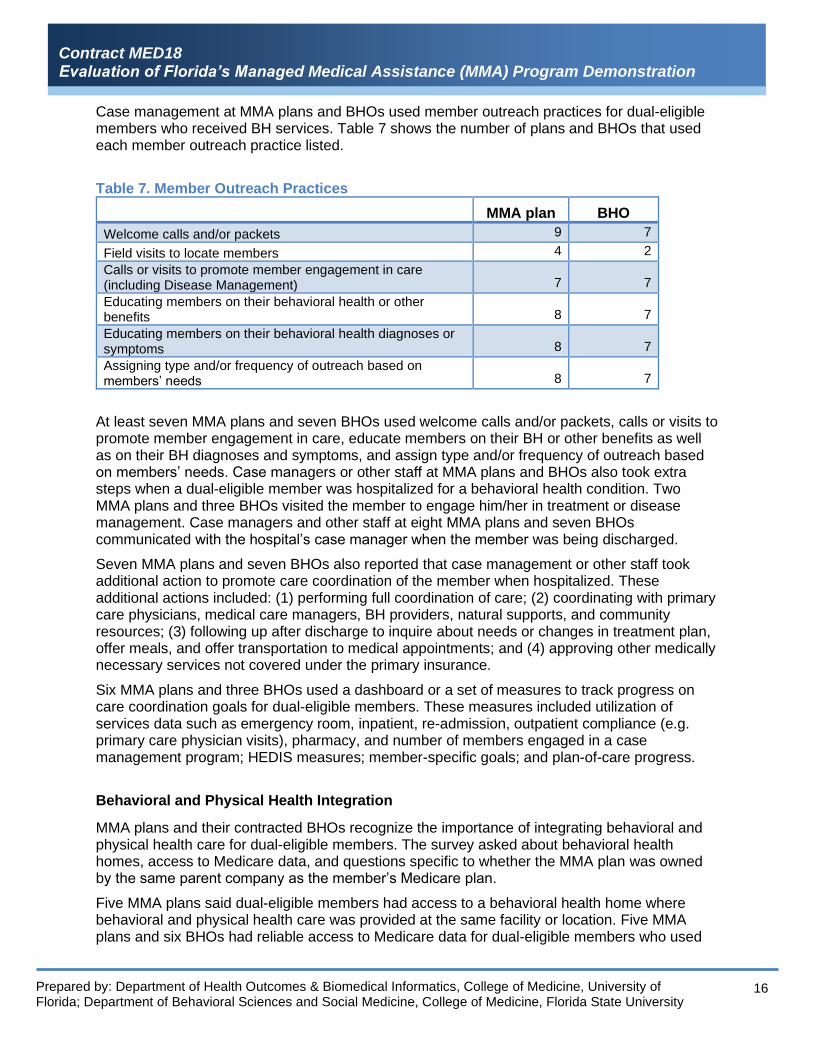
Case management at MMA plans and BHOs used member outreach practices for dual-eligible members who received BH services. Table 7 shows the number of plans and BHOs that used each member outreach practice listed.
Table 7. Member Outreach Practices
MMA plan BHO
Welcome calls and/or packets 9 7
Field visits to locate members 4 2
Calls or visits to promote member engagement in care (including Disease Management) 7 7
Educating members on their behavioral health or other benefits 8 7
Educating members on their behavioral health diagnoses or symptoms 8 7
Assigning type and/or frequency of outreach based on members’ needs 8 7
At least seven MMA plans and seven BHOs used welcome calls and/or packets, calls or visits to promote member engagement in care, educate members on their BH or other benefits as well as on their BH diagnoses and symptoms, and assign type and/or frequency of outreach based on members’ needs. Case managers or other staff at MMA plans and BHOs also took extra steps when a dual-eligible member was hospitalized for a behavioral health condition. Two MMA plans and three BHOs visited the member to engage him/her in treatment or disease management. Case managers and other staff at eight MMA plans and seven BHOs communicated with the hospital’s case manager when the member was being discharged.
Seven MMA plans and seven BHOs also reported that case management or other staff took additional action to promote care coordination of the member when hospitalized. These additional actions included: (1) performing full coordination of care; (2) coordinating with primary care physicians, medical care managers, BH providers, natural supports, and community resources; (3) following up after discharge to inquire about needs or changes in treatment plan, offer meals, and offer transportation to medical appointments; and (4) approving other medically necessary services not covered under the primary insurance.
Six MMA plans and three BHOs used a dashboard or a set of measures to track progress on care coordination goals for dual-eligible members. These measures included utilization of services data such as emergency room, inpatient, re-admission, outpatient compliance (e.g. primary care physician visits), pharmacy, and number of members engaged in a case management program; HEDIS measures; member-specific goals; and plan-of-care progress.
Behavioral and Physical Health Integration
MMA plans and their contracted BHOs recognize the importance of integrating behavioral and physical health care for dual-eligible members. The survey asked about behavioral health homes, access to Medicare data, and questions specific to whether the MMA plan was owned by the same parent company as the member’s Medicare plan.
Five MMA plans said dual-eligible members had access to a behavioral health home where behavioral and physical health care was provided at the same facility or location. Five MMA plans and six BHOs had reliable access to Medicare data for dual-eligible members who used

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
17
behavioral health services. When asked to describe this access, MMA plans/BHOs indicated information was regularly shared between case management staff in both the medical and BH areas. Additionally, they indicated that data was housed from both programs in their system when the Medicare plan was jointly owned by the same parent company as the MMA plan, giving the health plan the ability to access data. Some MMA plans and BHOs also described issues with limited or no access to data. In some situations, for members who had a Medicare plan owned by a different parent company than the MMA plan, the Medicare plan was unwilling to share any BH information (including encounters) due to HIPAA regulations. Additionally, some plans or BHOs did not know which Medicare providers offered BH services to the members, or encountered long delays in the responses from these providers.
For members who belonged to a Medicare plan owned by the same parent company as the MMA plan, the MMA plan took steps to integrate care. Five MMA plans and four BHOs reported having a shared information system that allowed the MMA plan or BHO access to both Medicare Advantage and Medicaid data. Six MMA plans and five BHOs said MMA plan/BHO and Medicare plan staff met (telephonically or in-person) to discuss the behavioral and physical health needs and status of specific members. Seven MMA plans and five BHOs reported members having a single case manager through the MMA plan or BHO who helped coordinate both behavioral and physical health services. For members who belonged to a Medicare plan owned by a different company than the MMA plan, other steps were taken to integrate care. Seven MMA plans and four BHOs identified case managers at the member’s Medicare plan. Seven MMA plans and three BHOs had staff who informed case managers at the member’s Medicare plan on Medicaid-provided benefits. Seven MMA plans and three BHOs had staff who shared member information with case managers at the member’s Medicare plan.
Disease Management
MMA plans and BHOs offered disease management programs to dual-eligible members who received behavioral health services. The survey asked respondents to indicate the disease management programs available to dual-eligible members and the strategies used to address changes in BH symptoms for members that required a rapid response.
Table 8 shows the disease management programs offered by the MMA plans and BHOs specifically asked in the survey.
Table 8. Disease Management Programs
MMA plan BHO
Attention deficit/hyperactivity disorder (ADHD) 3 4
Bipolar disorder 3 4
Depression 6 4
Schizophrenia 3 4
Severe mental illness (SMI) 3 4
Substance abuse 6 5
The most offered disease management program was substance abuse, with six MMA plans and five BHOs providing this service. A disease management program for depression also was offered by a similar number of MMA plans and BHOs. For attention deficit hyperactivity disorder, bipolar disorder, schizophrenia, and severe mental illness, three MMA plans and four BHOs offered disease management programs.
Seven MMA plans and seven BHOs said disease management staff employed strategies to

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
18
address changes in behavioral health symptoms among dual-eligible members that required a rapid response. Specifically, strategies listed included a 24-hour crisis intervention hotline, case management staff assigned to cases when there is a need to expedite care and coordination, and a formal intensive case management program that utilized more frequent case management services.
Other Care Coordination Strategies
After asking about case management, behavioral and physical health integration, and disease management, the survey asked the MMA health plans and their contracted BHOs about other strategies used to facilitate care coordination for dual-eligible members who received behavioral health services. Table 9 lists four specific strategies and the number of plans and BHOs that used each.
Table 9. Other Care Coordination Strategies
MMA plan BHO
Health navigators (who help members connect to community resources) 7 4
Partnerships with behavioral health community or advocacy organizations 7 6
Technology-focused interventions, such as smartphone apps 4 3
Telemedicine for diagnosis and treatment 6 6
Seven MMA plans and six BHOs use partnerships with behavioral health community or advocacy organizations to coordinate care, the most utilized strategy. Health navigators are used by seven MMA plans and four BHOs to help members connect to community resources. Six MMA plans and 6 BHOs use telemedicine for diagnosis and treatment. The least used strategy of the four listed is technology-focused interventions such as smartphone apps.
Plan Opinions
The final section of the survey asked MMA health plans their opinions about care coordination strategies for dual-eligible enrollees of their MMA plan who receive BH services.
MMA plans were asked which care coordination practices and strategies were most effective in providing timely and high-quality care to dual-eligible members receiving BH services. The plans’ list of practices included field and community supports through expanded use of outreach care specialists and peer educators, partnerships with community organizations, obtaining access to the Homeless Management Information System (HMIS) to identify and locate members with BH needs who were living in shelters or who were homeless, identification and outreach when members were discharged from facilities to connect the member to an outpatient BH provider, appropriate prioritization of requests for services, monthly staffing with the BH partner to discuss and evaluate progress, and ongoing follow-up and communication between all members of the care team to facilitate service provision.
Having onsite behavioral health case managers at high-utilization hospitals was also mentioned as an effective strategy. These case managers have established relationships with discharge planners and nurses to better streamline discharge planning and smooth the transition to a lower level of care. Other strategies listed as effective included (1) implementing clinical rounds to discuss specific cases and coordinate with the medical/behavioral health case managers, (2)

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
19
providing member access to a behavioral health home, (3) adopting an integrated case management model that includes BH as part of the team, and (4) providing immediate outreach to members upon admission.
Plans were also asked, “Overall, how easy or difficult is it for your plan or BHO to assist in care coordination for dual-eligible members who receive behavioral health services?” Eight plans said “very easy” or “somewhat easy,” and three MMA plans said “somewhat difficult” or very difficult.
One of the three plans that selected “somewhat or very difficult” said that for members who have another insurance or fee-for-service Medicare, their primary care providers or BH providers may not be contracted with the plan and would be reticent to share clinical information regarding a behavioral health diagnosis. This plan also had challenges with the Medicaid member population supplying current and accurate demographic information to the health plans or the Florida Department of Children and Families during the enrollment process, which can result in a delay in the coordination of their BH needs.
Another plan reported that it did not always know the Medicare providers for members or did not receive information regarding the member’s care. The plan stated that it used the coordination of benefits agreement information to obtain information on SSI dual-eligible members; however, not all providers submit this information to the health plan. Since members may see primary care providers that might not be part of the MMA plan’s network for Medicaid, there are challenges in identifying those providers as well as in receiving encounters or electronic medical records from those providers.
The final question in the survey asked MMA plans to provide any additional information relevant to understanding how their plan or contracted BHO coordinates care for dual-eligible members who received BH services. Several plans indicated they have a comprehensive or holistic approach to coordinating care that includes the strategies discussed earlier in the survey. One specific additional strategy mentioned was awareness of the social determinants of health and providing help for members with related issues such as food pantry, supportive housing, rental assistance, clothing, and support groups like the National Alliance on Mental Illness (NAMI), and Narcotics Anonymous (NA) or Alcoholics Anonymous (AA).
Another plan indicated that it works with provider partners, community organizations and public stakeholders to continuously refine an integrated health plan model that supports individuals with severe mental illness. This model of care reinforces and prioritizes recovery, stabilization, health maintenance, optimal safety, and independence through partnering with the enrollee, his or her natural supports and the enrollee's providers.
Several plans plan to increase the use of some practices such as greater community presence, use of social media, and texting. Another plan said the BHO participates in weekly operations meetings with the MMA plan as well as other clinical team meetings. In these meetings, all aspects of care coordination, including member and provider complaints, appeals, quality of care concerns, network access and availability, are addressed.
Non-Emergency Transportation Coordination
MMA plans provide non-emergency transportation services to their members. In order to understand the effectiveness of practices and strategies used by the MMA plans and their contracted NET vendors to coordinate these services, a survey was sent to the plans asking about dual-eligible membership, NET systems and structures, NET coordination, NET network adequacy, technological applications used in the course of providing NET services, NET vendor
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
20
oversight, and MMA plans’ opinions about NET service coordination.
Dual-Eligible Membership
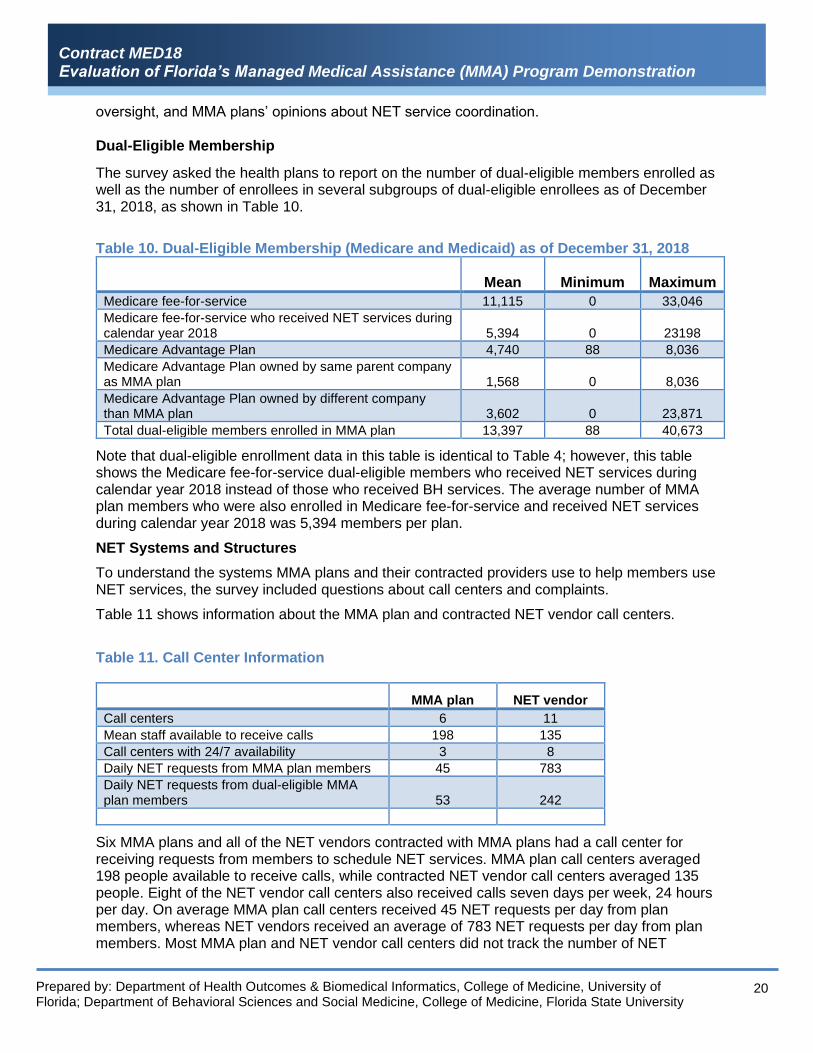
The survey asked the health plans to report on the number of dual-eligible members enrolled as well as the number of enrollees in several subgroups of dual-eligible enrollees as of December 31, 2018, as shown in Table 10.
Table 10. Dual-Eligible Membership (Medicare and Medicaid) as of December 31, 2018
Mean Minimum Maximum
Medicare fee-for-service 11,115 0 33,046
Medicare fee-for-service who received NET services during calendar year 2018 5,394 0 23198
Medicare Advantage Plan 4,740 88 8,036
Medicare Advantage Plan owned by same parent company as MMA plan 1,568 0 8,036
Medicare Advantage Plan owned by different company than MMA plan 3,602 0 23,871
Total dual-eligible members enrolled in MMA plan 13,397 88 40,673
Note that dual-eligible enrollment data in this table is identical to Table 4; however, this table shows the Medicare fee-for-service dual-eligible members who received NET services during calendar year 2018 instead of those who received BH services. The average number of MMA plan members who were also enrolled in Medicare fee-for-service and received NET services during calendar year 2018 was 5,394 members per plan.
NET Systems and Structures
To understand the systems MMA plans and their contracted providers use to help members use NET services, the survey included questions about call centers and complaints.
Table 11 shows information about the MMA plan and contracted NET vendor call centers.
Table 11. Call Center Information
MMA plan NET vendor
Call centers 6 11
Mean staff available to receive calls 198 135
Call centers with 24/7 availability 3 8
Daily NET requests from MMA plan members 45 783
Daily NET requests from dual-eligible MMA plan members 53 242
Six MMA plans and all of the NET vendors contracted with MMA plans had a call center for receiving requests from members to schedule NET services. MMA plan call centers averaged 198 people available to receive calls, while contracted NET vendor call centers averaged 135 people. Eight of the NET vendor call centers also received calls seven days per week, 24 hours per day. On average MMA plan call centers received 45 NET requests per day from plan members, whereas NET vendors received an average of 783 NET requests per day from plan members. Most MMA plan and NET vendor call centers did not track the number of NET

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
21
requests from MMA plan dual-eligible members. All MMA plans and all of the contracted NET vendors reported having a system for receiving and processing complaints from members or providers about NET services.
Table 12 summarizes the units and departments within MMA plans and their contracted NET vendors that receive complaints about NET services from members and providers.
Table 12. Reported NET Services Complaints
MMA plan NET vendor
NET call center 2 10
Member Services 11 2
Provider Relations 7 5
Case Management 7 0
Other 4 3
The department most frequently listed by the MMA plans that receives complaints about NET services was member services. Seven MMA plans indicated their provider relations and case management departments also received complaints.
Ten NET vendors used a NET call center to receive complaints about NET services from MMA plan members. Additionally, five NET vendors’ provider relations departments, and two NET vendors’ member services departments received complaints. Table 13 shows the number of complaints about NET services received by MMA plans and NET vendors.
Table 13. Number of NET Complaints Received
MMA plan NET vendor
Average NET complaints received from MMA plan members per week 15 23
Average NET complaints received from dual-eligible MMA plan members per week 10 8
Average NET complaints received by providers per week 5 0
MMA plans received an average of 15 complaints per week from MMA plan members about NET services, while NET vendors received an average of 23 complaints per week. Many of the MMA plans and NET vendors did not separately track the number of complaints received from dual-eligible MMA plan members. Of the MMA plans and vendors that track these numbers, the average weekly complaints received were 10 and 8 respectively. Table 14 shows the types of complaints received by the MMA plans and NET vendors about NET services provided to dual-eligible members.
Table 14. Types of Complaints
MMA plan NET vendor
Late pick-up before appointment 10 8
Late arrival to appointment 6 6
Late pick-up after appointment 6 5
Driver safety 1 0
Driver courtesy 0 1
Other 3 3
Ten plans and eight NET vendors said they received complaints about members who were

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
22
picked up late before an appointment. Six MMA plans and six NET vendors indicated members complained about arriving late to appointments. Six plans and five vendors said members complain about late pick-up after appointments. MMA plans and their contracted vendors should work on improving timeliness of service for NET requests. In particular, improving the timeliness of pick-up before an appointment will reduce the number of this type of complaint as well as complaints about late arrival to an appointment.
The MMA plans and NET vendors largely attended effectively to safety and courtesy of NET services. Driver safety and courtesy received almost no complaints, with only one MMA plan reporting driver safety complaints, and only one NET vendor reporting driver courtesy complaints. Three plans and three NET vendors indicated receiving other complaints; all of these complaints were described as no-shows.
NET Coordination
Coordinating NET services for dual-eligible MMA plan members helps these members receive transportation needed for non-emergency medical appointments. The survey asked about coordination provided by case managers and transportation coordinators at the MMA plans and NET vendors.
Ten MMA plans and seven NET vendors used case managers to assist in coordinating NET services for MMA plan members. Table 15 shows the strategies used by the case managers to coordinate NET services for dual-eligible members.
Table 15. Case Manager NET Coordination Strategies
MMA plan NET vendor
Handling regular trip requests 9 6
Handling special trip requests, including short-notice requests or changes 10 7
Proactive coordination of NET services for members 8 3
Direct communication with the NET vendor to resolve immediate issues 9 7
Facilitating 3-way calls with members and the NET vendor 8 6
NET service needs for high-need members 9 6
The most common strategy reported by both the MMA plans and the NET vendors in coordination of NET services by case managers was handling special trip requests, with ten MMA plans and seven NET vendors offering this service. Other frequently used strategies by case managers at both MMA plans and NET vendors were handling regular trip requests, direct communication with NET vendor to resolve immediate issues, focusing on trip requests and NET service needs for high-needs members, and facilitating three-way calls with members and the NET vendor. Respondents were also asked whether the MMA plan or NET vendor has transportation coordinators who assist in coordinating NET services for plan members. Four MMA plans and ten NET vendors said they use transportation coordinators for this purpose. Table 16 shows the number of plans and vendors that used each strategy to assist coordinating NET services for plan members using transportation coordinators.
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
23
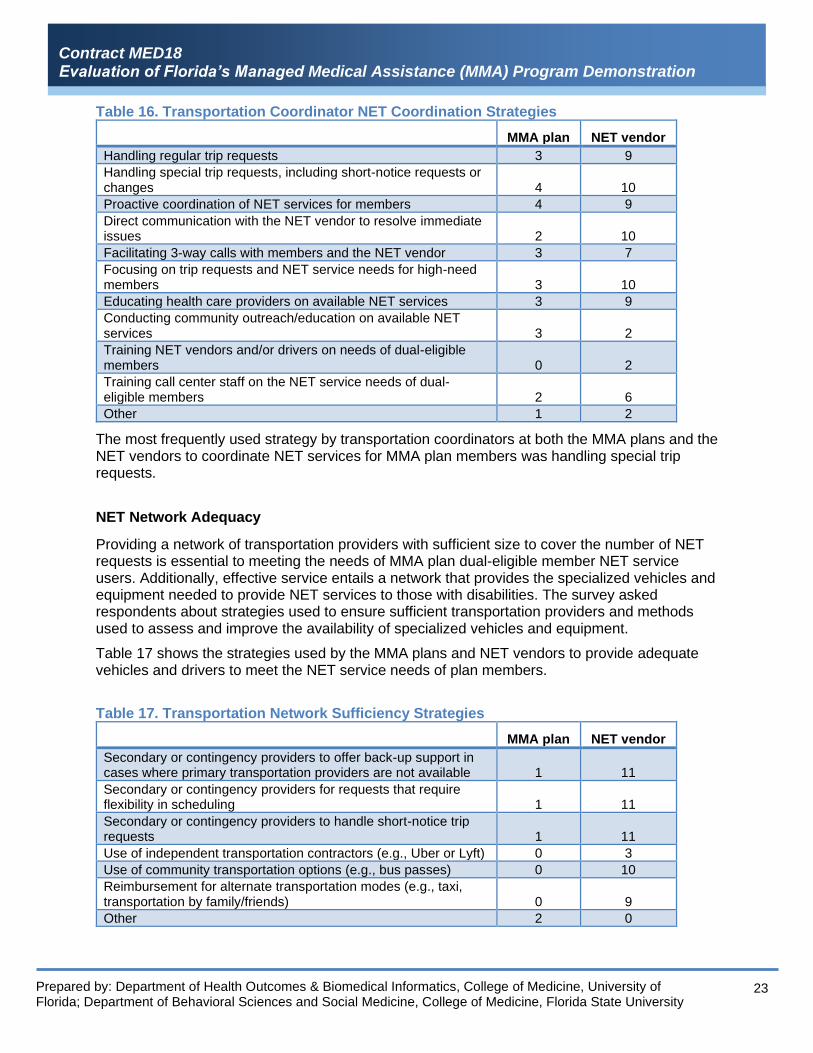
Table 16. Transportation Coordinator NET Coordination Strategies
MMA plan NET vendor
Handling regular trip requests 3 9
Handling special trip requests, including short-notice requests or changes 4 10
Proactive coordination of NET services for members 4 9
Direct communication with the NET vendor to resolve immediate issues 2 10
Facilitating 3-way calls with members and the NET vendor 3 7
Focusing on trip requests and NET service needs for high-need members 3 10
Educating health care providers on available NET services 3 9
Conducting community outreach/education on available NET services 3 2
Training NET vendors and/or drivers on needs of dual-eligible members 0 2
Training call center staff on the NET service needs of dual-eligible members 2 6
Other 1 2
The most frequently used strategy by transportation coordinators at both the MMA plans and the NET vendors to coordinate NET services for MMA plan members was handling special trip requests.
NET Network Adequacy
Providing a network of transportation providers with sufficient size to cover the number of NET requests is essential to meeting the needs of MMA plan dual-eligible member NET service users. Additionally, effective service entails a network that provides the specialized vehicles and equipment needed to provide NET services to those with disabilities. The survey asked respondents about strategies used to ensure sufficient transportation providers and methods used to assess and improve the availability of specialized vehicles and equipment.
Table 17 shows the strategies used by the MMA plans and NET vendors to provide adequate vehicles and drivers to meet the NET service needs of plan members.
Table 17. Transportation Network Sufficiency Strategies
MMA plan NET vendor
Secondary or contingency providers to offer back-up support in cases where primary transportation providers are not available 1 11
Secondary or contingency providers for requests that require flexibility in scheduling 1 11
Secondary or contingency providers to handle short-notice trip requests 1 11
Use of independent transportation contractors (e.g., Uber or Lyft) 0 3
Use of community transportation options (e.g., bus passes) 0 10
Reimbursement for alternate transportation modes (e.g., taxi, transportation by family/friends) 0 9
Other 2 0

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
24
One MMA plan used secondary providers for back-up support when primary providers were not available, for requests that required scheduling flexibility, and to handle short-notice trip requests. All 11 NET vendors also used these strategies. Additionally, ten of the NET vendors used community transportation options such as bus passes, and nine of the NET vendors used reimbursement for alternate transportation modes such as a taxi. Independent transportation providers such as Uber were used by three NET vendors. When asked about methods used to assess and improve the availability of specialized vehicles and equipment, MMA plans and their NET vendors gave a variety of responses that included an analysis of NET service utilization.
Technological Applications
The use of computer technology to help ensure the timely, safe, and high-quality delivery of NET services to dual-eligible MMA plan members was common. Respondents were asked whether the plan or NET vendor used particular kinds of applications for this purpose. Two MMA plans and all 11 NET vendors indicated they use applications to provide NET services. Table 18 shows the types of applications used.
Table 18. Types of Applications Used to Provide NET Services
MMA plan NET vendor
Computer software 1 11
Web-based application 1 11
Mobile (e.g., smartphone) application 1 6
Other 0 1
One MMA plan used computer software, web-based applications, and mobile applications. All 11 NET vendors used computer software and web-based applications. Six NET vendors used mobile applications. One NET vendor used other applications. Respondents were also asked about the functions of the applications used to provide NET services to MMA plan dual-eligible members. Table 19 shows the number of MMA plans and NET vendors that used applications with each listed function.
Table 19. Functions of Applications Used to Provide NET Services
MMA plan NET vendor
Enhance communication between transport providers and members 1 8
Enhance communication between transport and medical providers 0 4
Automate transportation scheduling and routing 1 10
Facilitate trip manifest distribution for drivers 0 10
Optimize dispatching of vehicles for trips (e.g., via real-time GPS) 0 9
Allow members to view vehicle locations (e.g., via real-time GPS) 0 6
Allow medical providers to view vehicle locations (e.g., via real-time GPS) 0 3
Provide members or medical providers with trip information 1 8
Allow members to confirm or cancel trips 1 8
Other 2 0
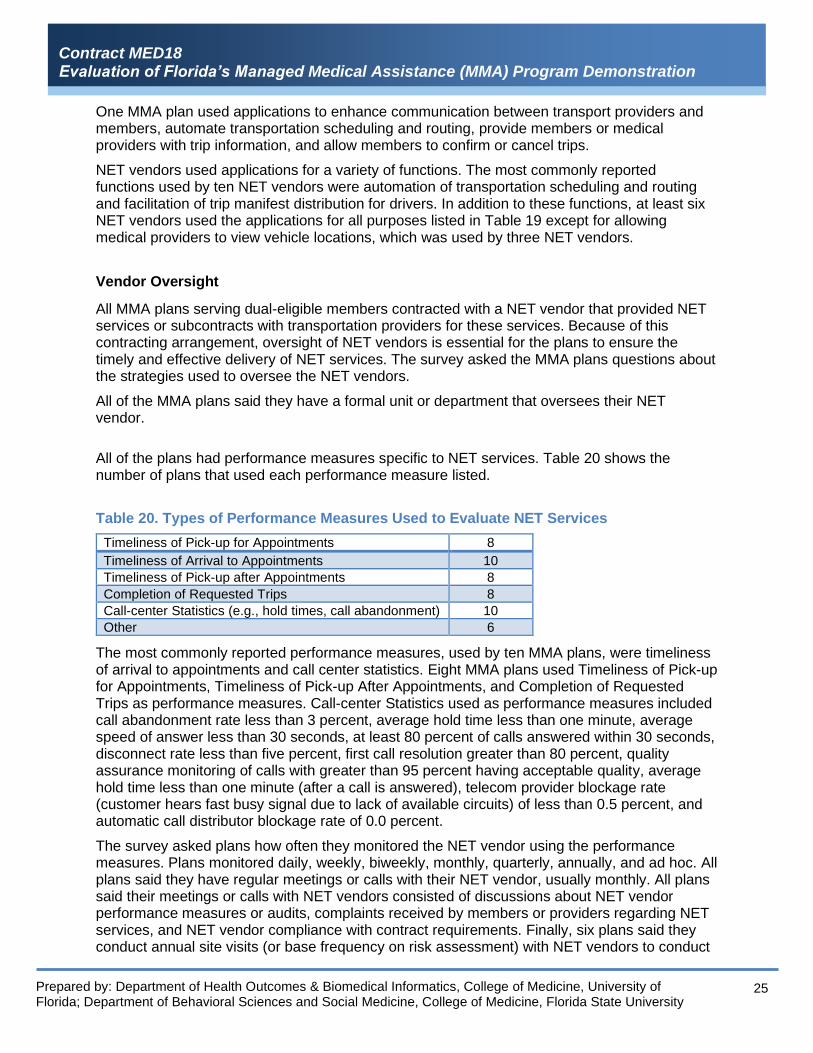
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
25
One MMA plan used applications to enhance communication between transport providers and members, automate transportation scheduling and routing, provide members or medical providers with trip information, and allow members to confirm or cancel trips.
NET vendors used applications for a variety of functions. The most commonly reported functions used by ten NET vendors were automation of transportation scheduling and routing and facilitation of trip manifest distribution for drivers. In addition to these functions, at least six NET vendors used the applications for all purposes listed in Table 19 except for allowing medical providers to view vehicle locations, which was used by three NET vendors.
Vendor Oversight
All MMA plans serving dual-eligible members contracted with a NET vendor that provided NET services or subcontracts with transportation providers for these services. Because of this contracting arrangement, oversight of NET vendors is essential for the plans to ensure the timely and effective delivery of NET services. The survey asked the MMA plans questions about the strategies used to oversee the NET vendors.
All of the MMA plans said they have a formal unit or department that oversees their NET vendor.
All of the plans had performance measures specific to NET services. Table 20 shows the number of plans that used each performance measure listed.
Table 20. Types of Performance Measures Used to Evaluate NET Services
Timeliness of Pick-up for Appointments 8
Timeliness of Arrival to Appointments 10
Timeliness of Pick-up after Appointments 8
Completion of Requested Trips 8
Call-center Statistics (e.g., hold times, call abandonment) 10
Other 6
The most commonly reported performance measures, used by ten MMA plans, were timeliness of arrival to appointments and call center statistics. Eight MMA plans used Timeliness of Pick-up for Appointments, Timeliness of Pick-up After Appointments, and Completion of Requested Trips as performance measures. Call-center Statistics used as performance measures included call abandonment rate less than 3 percent, average hold time less than one minute, average speed of answer less than 30 seconds, at least 80 percent of calls answered within 30 seconds, disconnect rate less than five percent, first call resolution greater than 80 percent, quality assurance monitoring of calls with greater than 95 percent having acceptable quality, average hold time less than one minute (after a call is answered), telecom provider blockage rate (customer hears fast busy signal due to lack of available circuits) of less than 0.5 percent, and automatic call distributor blockage rate of 0.0 percent.
The survey asked plans how often they monitored the NET vendor using the performance measures. Plans monitored daily, weekly, biweekly, monthly, quarterly, annually, and ad hoc. All plans said they have regular meetings or calls with their NET vendor, usually monthly. All plans said their meetings or calls with NET vendors consisted of discussions about NET vendor performance measures or audits, complaints received by members or providers regarding NET services, and NET vendor compliance with contract requirements. Finally, six plans said they conduct annual site visits (or base frequency on risk assessment) with NET vendors to conduct
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
26
assessments of vendor operations or inspect vehicles.
Plan Opinions
The final section of the survey asked MMA health plans their opinions about coordination strategies for dual-eligible enrollees of their MMA plan who received NET services.
MMA plans were asked which strategies and practices used to coordinate NET services for dual-eligible MMA plan members were most effective. One plan said the most effective practice was reviewing the performance metrics on a monthly basis and determining areas where the vendor was not compliant in order to create a corrective action plan. Another plan indicated the most effective strategy was real-time trip monitoring to ensure timely pick-up and drop-off for appointments. Other plans described communication as key between member and NET vendor scheduler, scheduler and driver, driver and members, and MMA plan staff and NET provider staff. Another plan described ridesharing services such as Lyft as revolutionary, with less than two trips out of 1,000 resulting in any member dissatisfaction. Other plans said effective practices are a large network with the right kinds of vehicles and equipment,
One plan used a member-centered approach and said, “Members are able to select a preferred provider, this allows the members company of choice to have first access to confirm and accept the scheduled transportation trip. Members are encouraged to schedule transportation pick-up time at least one hour prior to appointment (depending on mileage) to ensure member arrives timely to appointment. The most effective way ensuring timely and high quality NET transportation is to help the member develop standing orders for recurring trips where a company can be assigned to take the member on a routine basis to those scheduled appointments.”
Another plan used technology and said, “Our NET vendor has deployed a transportation technology platform, Reveal, which is improving scheduling, dispatching, and tracking member transports. The system allows for real-time GPS tracking of where vehicles are within a transport or prior to picking member up for a transport. This allows the NET dispatcher to direct a transport away from traffic, or reroute a vehicle where a delay to pick up a member is anticipated. Reveal will also provide members and facilities with the ability to view real-time vehicle locations, and change, cancel or reschedule trips through a smartphone app which will enhance member / provider satisfaction.”
The survey next asked, “Overall, how easy or difficult is it for your plan or NET vendor to coordinate NET services for dual-eligible members?” Ten MMA plans answered “very easy” or “somewhat easy.” One MMA plan said “somewhat difficult” because they do not usually have access to the members’ Medicare provider information.
The last question in the survey asked plans to provide any additional information relevant for understanding how the MMA plan or their NET vendor coordinates NET services for dual-eligible members. Regarding transportation networks, one plan said, “The Plan continuously works with our NET vendor to improve networks of transportation providers capable of supporting the quantity of trips anticipated for each mode of transportation (i.e. sedan, wheelchair, stretcher). A continued concern in many areas is the availability of ambulance providers, who have the ability to provide stretcher transports, which are limited due to cross county restrictions, and have the responsibility to provide transportation for 911 calls. Our NET vendor is constantly recruiting private transports within the county to facilitate these type of trips.”

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
27
Research Question 6C
How do dual-eligible enrollees rate their experience and satisfaction with delivery of care they receive related to behavioral health and non-emergency transportation services?
To answer Research Question 6C, the research team conducted a structured telephone survey with dual-eligible enrollees in MMA standard and MMA specialty plans. Ideally, two separate surveys would have been conducted with MMA plan members who received BH or NET services or both, with sample frames consisting of BH service recipients and NET service recipients. However, due to limited budget, because respondents who received both BH and NET services could complete one survey that asked questions about each service, the initial sample frame included only enrollees who had used both BH and NET services in calendar year 2018 (based on encounters data). Completed surveys were collected from 100 dual-eligible enrollees in MMA standard plans, and 41 dual-eligible enrollees in MMA specialty plans.
Because only 41 dual-eligible MMA specialty plan enrollees from the initial sample frame completed the survey, a second sample frame was developed. Eligibility for the second sample frame was the same as for the initial sample frame with one exception: the enrollee had received either BH or NET services during calendar year 2018 instead of receiving both of these services (based on encounters data). Subsequently, the target of 100 completed surveys with specialty plan members was achieved.
As this research question is descriptive, no statistical tests were required. However, it is important to note that because findings are based on samples of dual-eligible members in MMA standard plans and MMA specialty plans, inferences regarding experiences and satisfaction with care in these respective populations are made within a certain margin of error. For dual-eligible enrollees receiving BH and NET services in MMA standard plans, the margin of error (based on 100 completed surveys) is +/- 9.8 percent. Likewise, for questions asked of all specialty plan members surveyed, the margin of error (based on 100 completed surveys) is +/- 9.8 percent. For dual-eligible specialty plan enrollees receiving BH services, the margin of error associated with the questions asked of only these respondents (based on 71 completed surveys) is +/-11.7 percent. For dual-eligible enrollees in specialty plans receiving NET services, the margin of error associated with the questions asked of only these respondents (based on 70 completed surveys) is +/- 11.8 percent. In many cases, survey items were not completed by all respondents (for example, experience with access to care among those who reported receiving a specific type of BH service); margins of error were greater for items answered by a sub-set of survey respondents. To avoid misinterpretation of findings based on a small number of respondents, low denominator thresholds for reporting were established based on standards used by the National Committee for Quality Assurance (NCQA) for the Consumer Assessment of Healthcare Providers and Systems (CAHPS) survey. The NCQA standards for reporting require a 24.3 percent item response rate from all survey respondents in a reporting group. Following this standard, the research team did not report survey results for items with denominators less than 24 for MMA standard plan enrollees, less than 24 for items asked of all MMA specialty plan enrollees, or less than 17 for BH-specific or NET-specific items asked of MMA specialty plan enrollees. For these items, “LD” (low denominator) is specified in the tables below. Additionally, when all answer choices to a question are listed, the sum of the percentages may not add to exactly 100 percent due to rounding.
The racial/ethnic distribution of dual-eligible enrollees whose households were successfully contacted for the survey did not differ significantly from the racial/ethnic distribution of those who could not be contacted. As a result, weights were not needed to perform the analysis.
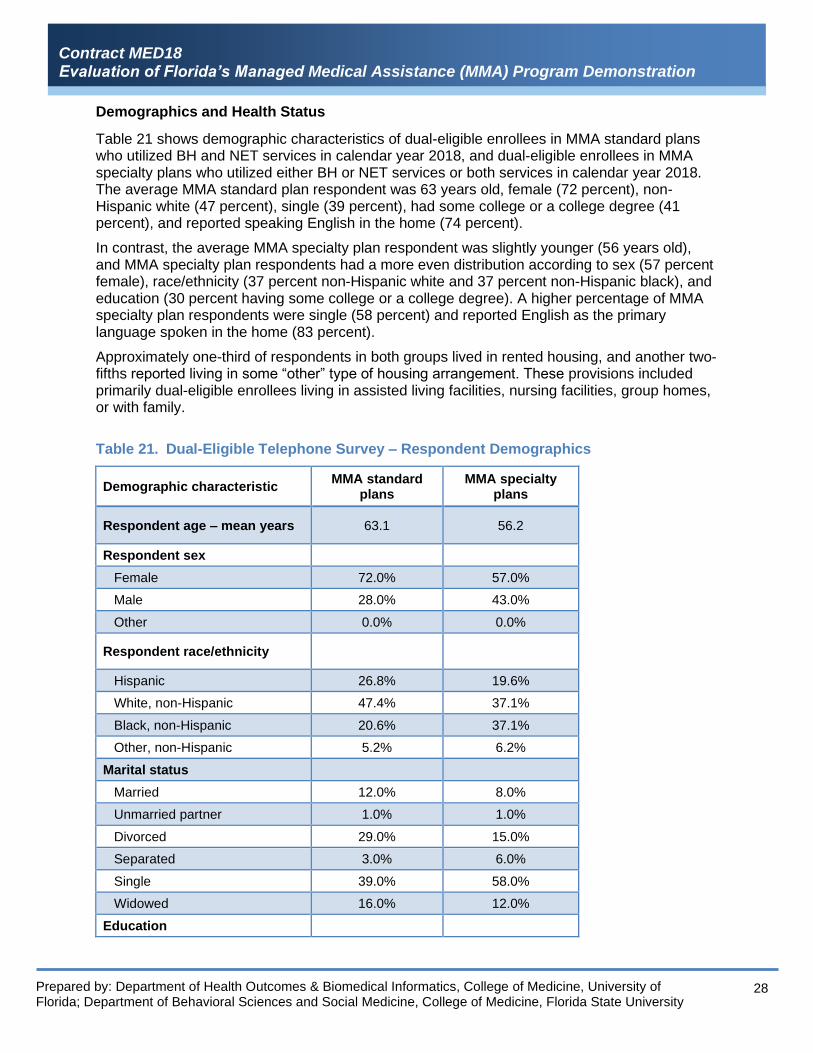
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
28
Demographics and Health Status
Table 21 shows demographic characteristics of dual-eligible enrollees in MMA standard plans who utilized BH and NET services in calendar year 2018, and dual-eligible enrollees in MMA specialty plans who utilized either BH or NET services or both services in calendar year 2018. The average MMA standard plan respondent was 63 years old, female (72 percent), non-Hispanic white (47 percent), single (39 percent), had some college or a college degree (41 percent), and reported speaking English in the home (74 percent).
In contrast, the average MMA specialty plan respondent was slightly younger (56 years old), and MMA specialty plan respondents had a more even distribution according to sex (57 percent female), race/ethnicity (37 percent non-Hispanic white and 37 percent non-Hispanic black), and education (30 percent having some college or a college degree). A higher percentage of MMA specialty plan respondents were single (58 percent) and reported English as the primary language spoken in the home (83 percent).
Approximately one-third of respondents in both groups lived in rented housing, and another two-fifths reported living in some “other” type of housing arrangement. These provisions included primarily dual-eligible enrollees living in assisted living facilities, nursing facilities, group homes, or with family.
Table 21. Dual-Eligible Telephone Survey – Respondent Demographics
Demographic characteristic MMA standard
plans MMA specialty
plans
Respondent age – mean years 63.1 56.2
Respondent sex
Female 72.0% 57.0%
Male 28.0% 43.0%
Other 0.0% 0.0%
Respondent race/ethnicity
Hispanic 26.8% 19.6%
White, non-Hispanic 47.4% 37.1%
Black, non-Hispanic 20.6% 37.1%
Other, non-Hispanic 5.2% 6.2%
Marital status
Married 12.0% 8.0%
Unmarried partner 1.0% 1.0%
Divorced 29.0% 15.0%
Separated 3.0% 6.0%
Single 39.0% 58.0%
Widowed 16.0% 12.0%
Education
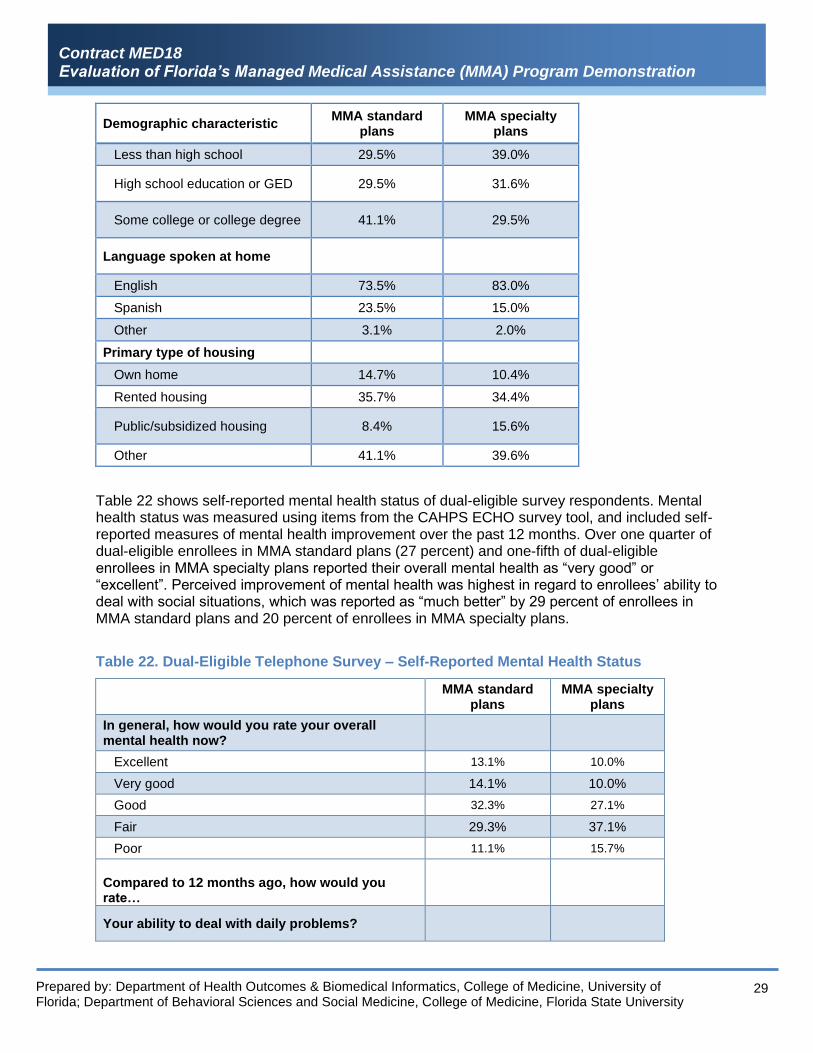
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
29
Demographic characteristic MMA standard
plans MMA specialty
plans
Less than high school 29.5% 39.0%
High school education or GED 29.5% 31.6%
Some college or college degree 41.1% 29.5%
Language spoken at home
English 73.5% 83.0%
Spanish 23.5% 15.0%
Other 3.1% 2.0%
Primary type of housing
Own home 14.7% 10.4%
Rented housing 35.7% 34.4%
Public/subsidized housing 8.4% 15.6%
Other 41.1% 39.6%
Table 22 shows self-reported mental health status of dual-eligible survey respondents. Mental health status was measured using items from the CAHPS ECHO survey tool, and included self-reported measures of mental health improvement over the past 12 months. Over one quarter of dual-eligible enrollees in MMA standard plans (27 percent) and one-fifth of dual-eligible enrollees in MMA specialty plans reported their overall mental health as “very good” or “excellent”. Perceived improvement of mental health was highest in regard to enrollees’ ability to deal with social situations, which was reported as “much better” by 29 percent of enrollees in MMA standard plans and 20 percent of enrollees in MMA specialty plans.
Table 22. Dual-Eligible Telephone Survey – Self-Reported Mental Health Status
MMA standard
plans MMA specialty
plans
In general, how would you rate your overall mental health now?
Excellent 13.1% 10.0%
Very good 14.1% 10.0%
Good 32.3% 27.1%
Fair 29.3% 37.1%
Poor 11.1% 15.7%
Compared to 12 months ago, how would you rate…
Your ability to deal with daily problems?

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
30
Much better 18.8% 20.0%
A little better or about the same 66.7% 65.7%
A little worse or much worse 14.6% 14.3%
Your ability to deal with social situations?
Much better 28.6% 20.3%
A little better or about the same 58.2% 66.7%
A little worse or much worse 13.3% 13.0%
Your ability to accomplish the things you want to do?
Much better 16.3% 11.8%
A little better or about the same 58.2% 64.7%
A little worse or much worse 25.5% 23.5%
Your problems or symptoms?
Much better 23.7% 14.3%
A little better or about the same 53.6% 68.6%
A little worse or much worse 22.7% 17.1%
Functional status was measured using selected items from the Medicare Current Beneficiary Survey (Table 23). Self-reported physical and social functioning was similar for dual-eligible enrollees in MMA standard plans and MMA specialty plans. Between one-half and three-fourths of enrollees in both groups reported having cognitive impairments, mobility impairments, and difficulty in instrumental activities of daily living, such as visiting a doctor’s office or shopping. These functional limitations, in particular, point toward the potential need of dual-eligible MMA enrollees for non-emergency medical transportation. About 54 percent of enrollees surveyed in standard plans and 43 percent of enrollees in specialty plans said their health limited their social activities “all of the time” or “most of the time.”
Table 23. Dual-Eligible Telephone Survey – Self-Reported Functional Status
MMA standard plans
MMA specialty plans
Functional impairment
Deaf or serious difficulty hearing 17.0% 14.1%
Blind or serious difficulty seeing, even wearing glasses
29.3% 32.3%
Serious difficulty concentrating, remembering, or making decisions
56.0% 61.6%
Serious difficulty walking or climbing stairs 71.0% 55.0%
Difficulty dressing or bathing 43.4% 32.7%
Difficulty doing errands alone, such as visiting a doctor's office or shopping
55.6% 53.1%
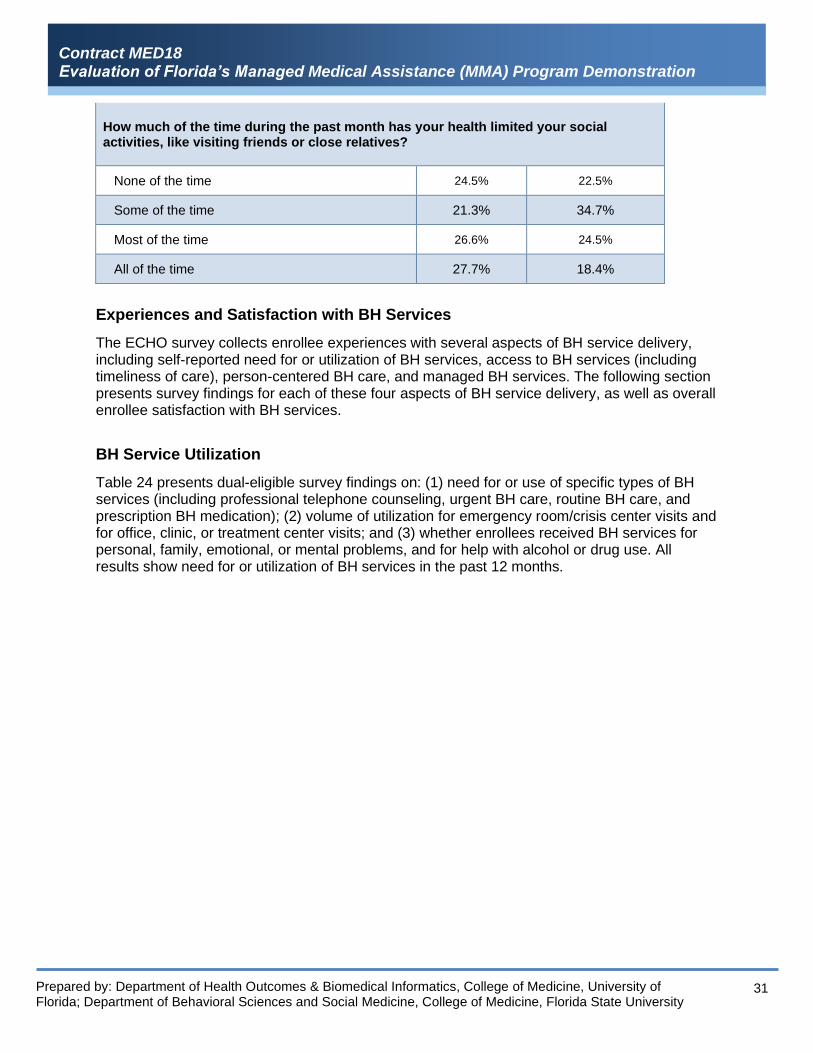
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
31
How much of the time during the past month has your health limited your social activities, like visiting friends or close relatives?
None of the time 24.5% 22.5%
Some of the time 21.3% 34.7%
Most of the time 26.6% 24.5%
All of the time 27.7% 18.4%
Experiences and Satisfaction with BH Services
The ECHO survey collects enrollee experiences with several aspects of BH service delivery, including self-reported need for or utilization of BH services, access to BH services (including timeliness of care), person-centered BH care, and managed BH services. The following section presents survey findings for each of these four aspects of BH service delivery, as well as overall enrollee satisfaction with BH services.
BH Service Utilization
Table 24 presents dual-eligible survey findings on: (1) need for or use of specific types of BH services (including professional telephone counseling, urgent BH care, routine BH care, and prescription BH medication); (2) volume of utilization for emergency room/crisis center visits and for office, clinic, or treatment center visits; and (3) whether enrollees received BH services for personal, family, emotional, or mental problems, and for help with alcohol or drug use. All results show need for or utilization of BH services in the past 12 months.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
32
Table 24. Dual-Eligible Telephone Survey – Need For and Utilization of BH Services
MMA standard plans
MMA specialty plans
Need for/use of
Professional counseling on the phone 16.0% 14.1%
Urgent BH counseling or treatment 24.2% 27.5%
Routine appointments for BH counseling or treatment
36.1% 47.9%
Prescription medicines for mental health treatment 79.0% 80.0%
Emergency room or crisis center visit for BH counseling or treatment
None 62.2% 62.3%
Once or twice 20.4% 14.5%
Three or more times 17.4% 23.2%
Office, clinic, or treatment program visit for BH counseling or treatment
None 43.3% 32.9%
One to ten times 41.2% 43.3%
Eleven or more times 15.5% 23.9%
Counseling or treatment for…
Personal, family, emotional, or mental problems 62.5% 69.6%
Help with alcohol use or drug use 6.1% 8.7%
Need for and utilization of all types of BH services were largely similar between dual-eligible enrollees in MMA standard plans and MMA specialty plans. About one-fourth of enrollees in both groups reported needing urgent BH counseling or treatment. Prescription medications represented the most frequently used type of BH service for 79 percent of MMA standard plan enrollees and 80 percent of MMA specialty plan enrollees. Routine appointments for BH services showed the largest difference between the two groups with 36 percent for standard plan members and 48 percent for specialty plan members.
About 38 percent of enrollees in both groups reported visiting an emergency room or crisis center for BH counseling or treatment in the past 12 months. About 16 percent of enrollees in MMA standard plans reported making 11 or more visits to an office, clinic, or treatment center for BH counseling or treatment in the past 12 months while about one-fourth of MMA specialty plan enrollees reported this frequency of visits.
About two-thirds of enrollees in both groups (63 percent standard plan and 70 percent specialty plan) reported they used BH services for personal, family, emotional, or mental problems, while less than one in ten said they used BH services for problems with alcohol or drug use.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
33
Access to BH Services
Table 25 presents findings on access to urgent BH care and routine BH care, and timeliness of office, clinic, or treatment center visits for BH counseling or treatment. About half (47percent) of specialty plan dual-eligible enrollees reported that they “usually” or “always” received urgent BH services as soon as they wanted while two-thirds of these enrollees and 86 percent of standard plan enrollees said they “usually” or “always” received routine BH services as soon as they wanted.
Table 25. Dual-Eligible Telephone Survey Access to and Timeliness of BH Services
MMA standard
plans MMA specialty
plans
Percent who "usually" or "always" received needed…
Professional counseling on the phone LD a LD a
Urgent BH counseling or treatment LD a 47.4%
Routine appointments for BH counseling or treatment 85.7% 66.7%
Among enrollees who had an office, clinic, or treatment center visit for BH counseling or treatment…
How often were you seen within 15 minutes of your appointment?
Never 5.8% 18.2%
Sometimes 17.3% 22.7%
Usually 25.0% 22.7%
Always 51.9% 36.4%
a LD: The denominator for the measure of access to professional phone counseling was too low to meet the threshold for reporting for both groups, as was the denominator for the measure of access to urgent BH counseling for the standard plan enrollees.
Among enrollees who reported having one or more visits to an office, clinic, or treatment center for BH counseling or treatment, the percentage who said they “usually” or “always” were seen within 15 minutes of their appointment was higher for MMA standard plan enrollees (77 percent) than MMA specialty plan enrollees (59 percent).
Person-Centered BH Care
The ECHO survey includes several questions that address aspects of person-centered BH care, including provider-patient communication, shared decision-making, and cultural competency. Table 26 shows survey findings on dual-eligible experiences with provider communication and shared decision-making. Overall, enrollees in both groups reported positive experiences with all aspects of provider communication. The percentage who said that providers “usually” or “always” spent enough time with the enrollee was higher for enrollees in MMA specialty plans (70 percent) than enrollees in MMA standard plans (62 percent).
Findings on shared decision-making – including receiving information on prescription medicine side effects and feeling involved in counseling and treatment – were also generally high for both groups. About 62 percent of standard plan members and 68 percent of specialty plan members stated they “usually” or “always” were involved as much as they wanted in their BH counseling or treatment.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
34
Table 26. Dual-Eligible Telephone Survey – Person-Centered BH Care
MMA standard
plans MMA specialty
plans
BH providers "usually" or "always"…
Listened carefully to the enrollee 69.6% 66.2% Explained things in a way that was easy to understand
61.5% 64.2%
Showed respect for what the enrollee had to say 70.8% 71.0%
Spent enough time with the enrollee 61.9% 69.6%
Among enrollees who took prescription BH medications…
BH providers told them what side effects to watch for
64.6% 69.1%
In the last 12 months, how often were you involved as much as you wanted in your counseling or treatment?
Never 26.3% 19.7%
Sometimes 11.6% 12.1%
Usually 17.9% 13.6%
Always 44.2% 54.6%
With regard to cultural competency, 18 percent of dual-eligible enrollees in MMA standard plans and 14 percent in MMA specialty plans stated that their language, race, religion, ethnic background, or culture made a difference in the kind of counseling or treatment they needed (results not shown in table). The ECHO survey includes a follow-up question to assess whether BH care received in the last 12 months was responsive to these needs; however, the denominators for this item were too low to meet the threshold for reporting.
Managed BH Care
The ECHO survey also includes questions that address several aspects of managed BH care, including the amount of counseling or treatment that was paid for by the enrollee’s health plan, how easy it was to find a network BH provider, delays in counseling or treatment due to need for health plan approval of services, and getting help from health plan customer service. Table 27 presents findings on experiences regarding health plan coverage of BH services, getting new network BH providers, and calling health plan customer service.
Approximately two-thirds of dual-eligible enrollees in both MMA standard (63 percent) and specialty plans (68 percent) said that all of the counseling or treatment they received in the last 12 months was paid for by their health plan. About two-thirds of enrollees in the standard plans and about three-fourths of enrollees in the specialty plans who got a new BH provider in the last 12 months said it was not a problem to get someone they were happy with.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
35
Table 27. Dual-Eligible Telephone Survey – Managed BH Care
MMA standard
plans MMA specialty
plans
How much of the counseling or treatment you got in the last 12 months was paid for by your health plan?
All of it was paid for 62.9% 67.7%
Most of it was paid for 16.9% 17.7%
Some of it was paid for 7.9% 11.8%
None of it was paid for 12.4% 2.9%
Among enrollees who got someone new for counseling or treatment since joining their plan… 10
It was "not a problem" to get someone they were happy with
68.8% 73.7%
Among enrollees who called their health plan's customer service to get information or help about counseling or treatment…11
It was "not a problem" to get the help they needed
73.1% LD b
Among enrollees who needed approval for counseling or treatment…12
It was "not a problem" to wait for approval 77.8% 40.0%
It was "not a problem" to get the counseling or treatment needed
70.4% 55.0%
Of the standard plan enrollees in the survey who needed approval for counseling or treatment, about three-fourths said it was not a problem to wait for approval, and about 70 percent said it was not a problem to get needed counseling or treatment. Of the specialty plan enrollees in the survey, two-fifths said it was not a problem to wait for approval, and 55 percent said it was not a problem to get the needed counseling or treatment.
Satisfaction with BH services
The ECHO survey also includes two ratings questions which ask respondents to rate, on a scale from 0 to 10: (1) all of the BH counseling or treatment they received in the last 12 months; and (2) their health plan for BH counseling or treatment (Figure 1). Overall, about half of dual-eligible enrollee survey participants in both groups (55 percent of standard plan and 49 percent of specialty plan) said they were helped “a lot” by the BH counseling or treatment they received in the last 12 months. Additionally, about half of dual-eligible enrollees in both groups rated their counseling or treatment and their health plan a “9” or “10” on a scale from 0 to 10.
Figure 1. Dual-Eligible Telephone Survey – Percentage of Respondents Rating their BH Care a “9” or “10”
10 Among MMA standard plan enrollees in the survey, 32 (33 percent) said they got someone new for counseling or
treatment. Among MMA specialty plan enrollees in the survey, 19 (28 percent) said they got someone new for counseling or treatment 11 Among MMA standard plan enrollees in the survey, 26 (27 percent) said they contacted customer service. Among MMA
specialty plan enrollees in the survey, 11 (16 percent) said they contacted customer service. The number of MMA specialty plan enrollees who contacted customer service was too low to meet the threshold for reporting on the measure of experience with customer service. 12 Among MMA standard plan enrollees in the survey, 27 (28 percent) said they needed approval for counseling or
treatment while 20 (29 Percent) of MMA specialty plan enrollees in the survey said they needed approval.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
36
Experiences and Satisfaction with NET Services
The dual-eligible telephone survey also included several items addressing experiences and satisfaction with non-emergency transportation services, which had previously been fielded as part of the Florida Medicaid Non-Emergency Transportation Survey, originally developed by the University of South Florida and modified for use in this study.
Overall, 72 percent of MMA standard plan enrollees and 76 percent of MMA specialty plan enrollees reported having phoned their health plan in the last 12 months to get help with transportation. These respondents were asked follow-up questions regarding access, timeliness, and perceived safety of the NET services they received (Table 28).
Dual-eligible enrollees in both groups generally had positive experiences with NET services. Among those who requested assistance with NET from their health plan over the phone, more than two-thirds “usually” or “always” received transportation, and the vast majority reported that transportation met their needs. About seventy percent of MMA plan enrollees in both groups reported getting to appointments on time. However, slightly more than half of enrollees in both groups reported waiting 30 minutes or longer to be picked up after their appointments.
54.7%50.8%49.0% 50.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
MMA standard plans MMA specialty plans
All BH counseling or treatment Health plan for counseling or treatment
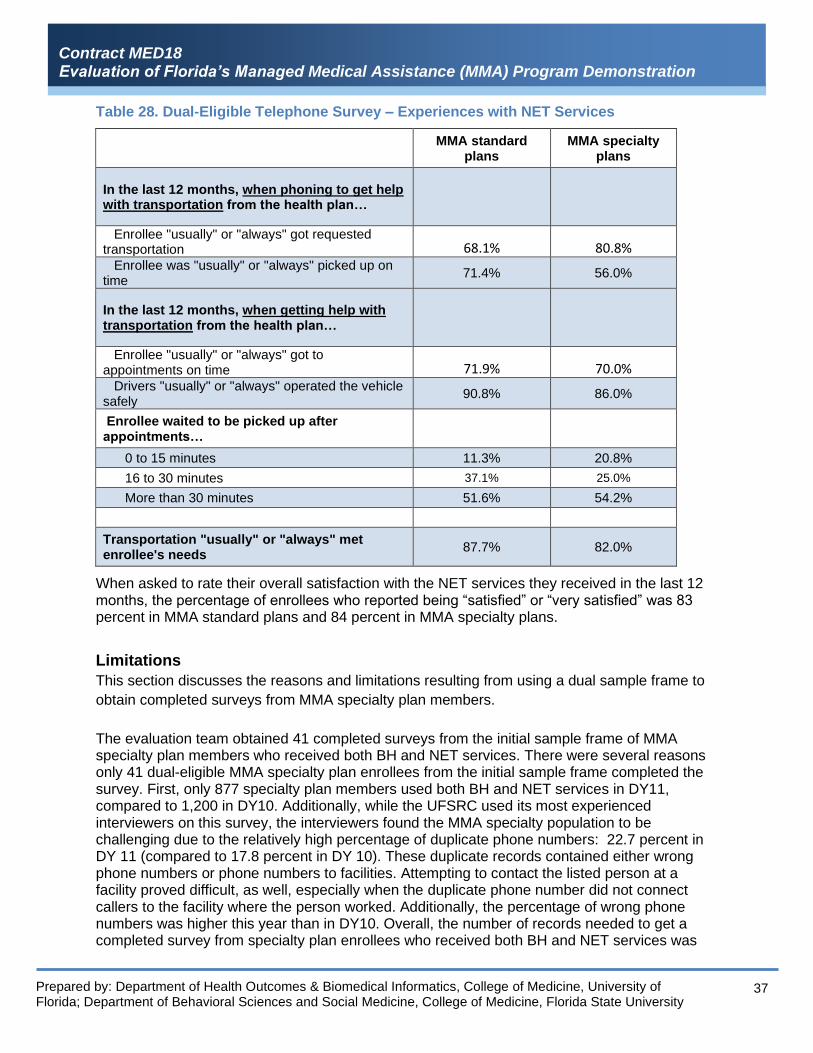
Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
37
Table 28. Dual-Eligible Telephone Survey – Experiences with NET Services
MMA standard plans
MMA specialty plans
In the last 12 months, when phoning to get help with transportation from the health plan…
Enrollee "usually" or "always" got requested transportation 68.1% 80.8% Enrollee was "usually" or "always" picked up on time
71.4% 56.0%
In the last 12 months, when getting help with transportation from the health plan…
Enrollee "usually" or "always" got to appointments on time 71.9% 70.0% Drivers "usually" or "always" operated the vehicle safely
90.8% 86.0%
Enrollee waited to be picked up after appointments…
0 to 15 minutes 11.3% 20.8%
16 to 30 minutes 37.1% 25.0%
More than 30 minutes 51.6% 54.2%
Transportation "usually" or "always" met enrollee's needs
87.7% 82.0%
When asked to rate their overall satisfaction with the NET services they received in the last 12 months, the percentage of enrollees who reported being “satisfied” or “very satisfied” was 83 percent in MMA standard plans and 84 percent in MMA specialty plans.
Limitations
This section discusses the reasons and limitations resulting from using a dual sample frame to
obtain completed surveys from MMA specialty plan members.
The evaluation team obtained 41 completed surveys from the initial sample frame of MMA specialty plan members who received both BH and NET services. There were several reasons only 41 dual-eligible MMA specialty plan enrollees from the initial sample frame completed the survey. First, only 877 specialty plan members used both BH and NET services in DY11, compared to 1,200 in DY10. Additionally, while the UFSRC used its most experienced interviewers on this survey, the interviewers found the MMA specialty population to be challenging due to the relatively high percentage of duplicate phone numbers: 22.7 percent in DY 11 (compared to 17.8 percent in DY 10). These duplicate records contained either wrong phone numbers or phone numbers to facilities. Attempting to contact the listed person at a facility proved difficult, as well, especially when the duplicate phone number did not connect callers to the facility where the person worked. Additionally, the percentage of wrong phone numbers was higher this year than in DY10. Overall, the number of records needed to get a completed survey from specialty plan enrollees who received both BH and NET services was

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
38
21, compared to 13 in DY10, representing a 68 percent increase in records required to complete a survey. From the second sample frame, 30 completed surveys were obtained from enrollees who received only BH services, and 29 completed surveys were obtained from enrollees who received only NET services. A total of 100 completed surveys with MMA specialty plan members from the initial and second sample frames were obtained comprising 71 who received BH services and 70 who received NET services. All of the specialty plan members in the survey received questions about demographics and self-reported functional status. Specialty plan members who received BH services were also asked about self-reported mental health status and experiences and satisfaction with BH services, while those who received NET services were asked about experiences and satisfaction with NET services.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
39
Conclusion and Recommendations
The DY11 results for Research Question 6A for both BH and NET services largely mirror the results found in DY10. There remain substantial and contrasting differences between MMA dual-eligibles and non-dual-eligibles in BH and NET service use and costs, but the pattern of those differences in DY11 is quite similar to the pattern found in DY10, (e.g., lower BH use and cost among dual-eligibles and higher NET use among dual-eligibles).
Work to date examining the impact of MMA on dual-eligibles has been hampered by the lack of Medicare Advantage encounter data. These Medicare data are essential to gain a complete understanding of the health utilization profile of dual-eligibles. CMS recently approved the first release of Medicare Advantage data to researchers, and the evaluation team has ordered and received these important data from CMS.
Moving forward, the evaluation team recommends that the Agency consider how these new Medicare Advantage encounter data can provide a more complete assessment of MMA’s impact on dual-eligibles. The focus on BH and NET services in DY10 and DY11 was necessary given the lack of Medicare Advantage encounter data. However, that limitation has now been removed, and the range of possible questions concerning MMA’s impact on dual-eligibles could be expanded. The evaluation team urges the Agency to consider modifying the focus of Component 6 to take advantage of these new data.
The results for Research Question 6B for DY11 are similar to DY10 revealing several challenges to coordinating BH and NET services. Poor contact information and difficulty locating members pose barriers for delivery and coordination of BH services. Coordinating BH care and NET service for dual-eligibles can be challenging when access to multiple encounter systems is needed, or when Medicare data are not available to MMA plans, and/or Medicare case managers and providers are not available or are reluctant to cooperate. Overall, dual-eligibility status has less impact on access and quality to NET services.
The results for Research Question 6B also revealed several possible best practices for coordinating BH and NET services for dual-eligible members.
For improving access to and quality of BH services, MMA plans should consider a comprehensive case management strategy that interfaces traditional case management approaches with utilization management, performance measures, member education, member and family engagement, and linkage to community resources and peer supports. Efforts to integrate BH and physical health services may include working with hospital case managers for discharge planning, establishing behavioral health homes at community mental health centers, and working with Medicare plans to share information on members. Obtaining access to systems such as the Homeless Management Information System (HMIS) can facilitate member location.
For improving access to and quality of NET services, MMA plans should consider strategies that focus on transportation vendors and providers, including regular vendor oversight and case management communication with vendors. Establishing transportation coordinators and setting up three-way calls with members, case managers, and transportation providers can help to address immediate transportation needs. Technological innovations that involve mobile applications show promise for connecting members, medical providers, and transportation providers and coordinating NET services in real-time. Encouraging members to select a preferred provider and reuse that provider, especially when regular appointment times are scheduled, improves service as does the use of ridesharing services. To improve NET network adequacy, MMA plans should consider using secondary or contingency transportation

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
40
providers. For dual-eligible members, efforts should ensure that specialized vehicles and equipment are adequate in number and quality.
The DY11 results for Research Question 6C are similar to DY10. Dual-eligible members overall had positive experiences and satisfaction with the BH and NET services through MMA standard plans and MMA specialty plans.
With regard to BH services, about one-fourth of enrollees reported needing or using urgent BH care, and approximately one-third and one-half of standard and specialty plan enrollees respectively reported needing or using routine BH care. For urgent BH care, although the denominator was too low to report on standard plan members, about half of specialty plan members “usually” or always” received needed care. For routine BH care, around 86 percent of standard plan members and two-thirds of specialty plan members “usually” or “always” received needed services. The most common type of BH service used by dual-eligible enrollees was prescription medications, around 80 percent. Enrollees also had positive experiences with person-centered BH care. In particular, about two-thirds said they were “usually” or “always” involved in their care as much as they wanted to be.
Enrollees also reported favorable experiences with their health plan regarding BH services. Although 12 percent of standard plan enrollees reported at least some portion of their BH services not paid for by their health plan, only three percent of specialty plan members said they had this experience. Between two-thirds and three-quarters of enrollees stated it was not a problem to get a new BH provider that they were happy with.
With regard to NET services, enrollee experiences were generally positive. 68 percent of standard plan members, and 81 percent of specialty plan members “usually” or “always” got requested NET services; 71 percent of standard plan members and 56 percent of specialty plan members were picked up on time; and about 70 percent of dual-eligible members in both types of plans got to their appointments on time. However, slightly more than half of enrollees reported waiting more than 30 minutes to be picked up after their scheduled appointments. Plans should work with transportation vendors to explore reasons for and improve upon these delays.
While the results between DY10 and DY11 for the MMA plan dual enrollee survey were similar, a significant area of difference between DY10 and DY11 for the telephone survey is the precipitous drop in sample productivity for the specialty plan members who received both BH and NET services. For DY10, 13 records were needed to get a completed survey from these members while in DY11, 21 records were needed, a 68 percent increase. Because the general trend with telephone surveys is a decrease in response rates over time, the number of completed surveys obtainable per year from this population will continue to decrease, thereby resulting in larger margins of error associated with the estimates calculated to answer this research question. To address this issue, the Agency may wish to consider increasing the resources allocated to the survey data collection, or using two years of resources every other year to conduct dual-eligible MMA plan enrollee surveys about BH and NET services.

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
41
Appendix 1. DY11 MMA Evaluation Components and Research
Questions Component Research Questions
1. The effect of managed care on access to care, quality and efficiency of care, and the cost of care
1A. What barriers do enrollees encounter when accessing primary care and preventive services? 1B. What changes in the accessibility of services occur with MMA implementation, comparing the accessibility in pre-MMA implementation plans (Reform plans and 1915(b) waiver plans) to MMA plans? 1C. What changes in the utilization of services for enrollees are evident post-MMA implementation, comparing: 1) utilization of services in the pre-MMA period (FFS, Reform plans and pre-MMA 1915(b) waiver plans) to utilization of services in post-MMA implementation; 2) utilization of services in specialty MMA plans versus standard MMA plans for enrollees eligible for enrollment in a specialty plan (e.g., enrollees with HIV or SMI) who are enrolled in standard MMA plans versus enrollees in the specialty plans? 1D. What changes in quality of care for enrollees are evident post MMA implementation, comparing: 1) quality of care in pre-MMA implementation plans (Reform plans and 1915(b) waiver plans) to quality of care in MMA plans in the MMA period; 2) quality of care in specialty MMA plans versus standard MMA plans for enrollees eligible for enrollment in a specialty plan (e.g. enrollees with HIV or SMI) who are enrolled in standard plans versus enrollees in the specialty plans (to the extent possible)? 1E. What strategies are standard MMA and specialty MMA plans using to improve quality of care? Which of these strategies are most effective in improving quality and why? 1F. What changes in timeliness of services occur with MMA implementation, comparing timeliness of services in pre-MMA implementation plans (Reform plans and 1915(b) waiver plans) to post-MMA implementation plans? 1G. What is the difference in per-enrollee cost by eligibility group pre-MMA implementation (FFS, Reform plans and pre-MMA 1915(b) waiver plans) compared to per-enrollee costs in the MMA period (MMA plans as a whole, standard MMA plans and specialty MMA plans)?

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
42
2. The effect of customized benefit plans on beneficiaries’ choice of plans, access to care, or quality of care
Note: Since the MMA plans do not offer customized benefit plans, the state will evaluate the effect of expanded benefits on enrollees’ utilization of services, access to care, and quality of care.
2A. What is the difference in the types of expanded benefits offered by standard MMA and specialty MMA plans? How do plans tailor the types of expanded benefits to particular populations? 2B. How many enrollees utilize expanded benefits and which ones are most commonly used? 2C. How does Emergency Department (ED) and inpatient hospital utilization differ for those enrollees who use expanded benefits (e.g. additional vaccines, physician home visits, extra outpatient services, extra primary care and prenatal/perinatal visits, and over-the-counter drugs/supplies) vs. those enrollees who do not? 2D. How do enrollees rate their experiences and satisfaction with the expanded benefits that are offered by their health plan?
3. Participation in the Healthy Behaviors programs and its effect on participant behavior or health status
3A. What Healthy Behaviors programs do MMA plans offer? What types of programs and how many are offered in addition to the three required programs (the medically approved smoking cessation program, the medically directed weight loss program, and the medically approved alcohol or substance abuse treatment program)?
3B. What incentives and rewards do MMA plans offer to their enrollees for participating in Healthy Behaviors programs?
3C. How many enrollees participate in each Healthy Behaviors program? How many enrollees complete Healthy Behaviors programs? Which types of Healthy Behaviors programs attract higher numbers of participants? 3D. How does participation in Healthy Behaviors programs vary by gender, age, race/ethnicity and health status of enrollees (DY13 and beyond)?
3E. What differences in service utilization occur over the course of the demonstration for enrollees participating in Healthy Behaviors programs versus enrollees not participating (DY13 and beyond)?
4. The impact of LIP funding on hospital charity care programs
4A. What is the impact of LIP funding on access to care for Medicaid, uninsured, and underinsured recipients served in hospitals? That is, how many Medicaid, uninsured, and underinsured recipients receive services in LIP-funded hospitals?
4B. What types of services are being provided to Medicaid, uninsured, and underinsured recipients receiving care in LIP-funded hospitals?

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
43
4C. What is the impact of LIP funding on access to care for uncompensated charity care recipients served in hospitals? That is, how many uncompensated charity care recipients receive services in LIP-funded hospitals? How does this compare among hospitals in different tiers of LIP finding? 4D. What types of services are being provided to uncompensated charity care recipients receiving care in LIP-funded hospitals? 4E. What is the difference in the type and number of services offered to uncompensated charity care patients in hospitals receiving LIP funding? 4F. What is the impact of LIP funding on the number of uncompensated charity care patients served and the types of services provided in FQHCs, RHCs, and medical school physician practices?
5. The effect of having separate managed care programs for acute care and LTC services on access to care, care coordination, quality, efficiency of care, and the cost of care13
5A. How many enrollees are enrolled in separate Medicaid managed care programs for acute (medical) care and LTC services? 5B. How many enrollees are enrolled in comprehensive plans for both acute (medical) care and LTC services? 5C. Are there differences in service utilization, as well as in the appropriateness of service utilization (to the extent this can be measured), between enrollees who are in a comprehensive plan for both MMA and LTC services versus those who are enrolled in separate MMA and LTC plans?
6. The impact of efforts to align with Medicare and improving beneficiary experiences and outcomes for dual-eligible individuals
6A. How many MMA enrollees are also Medicare recipients (dual-eligibles) and to what extent do dual-eligible enrollees utilize behavioral health and non-emergency transportation services? 6B. What specific care coordination strategies and practices are most effective for ensuring access to and quality of care for behavioral health services and non-emergency transportation services for dual-eligible enrollees? 6C. How do dual-eligible enrollees rate their experience and satisfaction with delivery of care they received related to behavioral health and non-emergency transportation services?
13 Component 5 will sunset following the evaluation of DY12 (SFY 2017-18).

Prepared by: Department of Health Outcomes & Biomedical Informatics, College of Medicine, University of Florida; Department of Behavioral Sciences and Social Medicine, College of Medicine, Florida State University
Contract MED18 Evaluation of Florida’s Managed Medical Assistance (MMA) Program Demonstration
44
7. The effectiveness of enrolling individuals into a managed care plan upon eligibility determination in connecting beneficiaries with care in a timely manner
7A. How quickly do new enrollees access services, including expanded benefits in excess of State Plan covered benefits, after becoming Medicaid eligible and enrolling in a health plan? 7B. Among new enrollees, what is the time to access services for enrollees who are enrolled under Express Enrollment compared to enrollees who were enrolled prior to the implementation of Express Enrollment?
8. The effect the Statewide Medicaid Prepaid Dental Health Program has on accessibility, quality, utilization, and cost of dental health care services
8A. How does enrollee utilization of dental health services vary by age, gender, race/ethnicity, and geographic area? 8B. What changes in dental health service utilization occur with the implementation of the Statewide Medicaid Prepaid Dental Health Program?
8C. What changes in quality of dental health services occur with the implementation of the Statewide Medicaid Prepaid Dental Health Program? 8D. What changes in the accessibility of dental services occur with the implementation of the Statewide Medicaid Prepaid Dental Health Program? 8E. What barriers do enrollees encounter when accessing dental health services? 8F. How many enrollees utilize expanded benefits provided by the dental health plans and which ones are most commonly used?
8G. How does enrollee utilization of dental health services impact dental-related hospital events (e.g., Emergency Department, Inpatient hospitalization)? How does utilization of expanded benefits offered by the dental health plans impact dental-related hospital events? 8H. What changes in per-enrollee cost for dental health services occur with the implementation of the Statewide Medicaid Prepaid Dental Health Program? 8I. How do enrollees rate their experiences and satisfaction with dental health services, including timeliness of dental health services, provided by their dental health plans? 8J. How do enrollees rate their experiences and satisfaction with the expanded benefits offered by their dental health plans?


















