
Evaluation of bilateral minimum thickness of normal corneas based on Fourier-domain optical...
8
Evaluation of bilateral minimum thickness of normal corneas based on Fourier-domain optical coherence tomography Gaurav Prakash, MD, Dhivya Ashok Kumar, MD, Amar Agarwal, MS, FRCS, RCOphth, Yoga Sarvanan, ME, Soosan Jacob, MS, DNB, FRCS, Athiya Agarwal, MD, DO PURPOSE: To determine the normative ranges and various aspects of the relationship between the minimum corneal thicknesses (MCT) in fellow eyes and the location of the MCT in relation to the central cornea using Fourier-domain optical coherence tomography (OCT). SETTING: Tertiary care ophthalmic hospital, Chennai, India. METHODS: In this cross-sectional observational trial, both eyes of consecutive healthy young subjects with a low refractive error and no clinical or topographic evidence of corneal disorders had bilateral pachymetric assessment with a Fourier-domain OCT platform (RTVue). The MCT, central corneal thickness (CCT), and x–y coordinates of the MCT location were noted. RESULTS: The CCT and MCT followed a normal distribution with a good correlation. The difference between CCT and MCT was approximately 5 mm in right eyes and left eyes (P<.05 for both). The difference in CCT was the best predictor of the difference in MCT. The mean distance from the center (0.63 mm G 0.13 [SD], right eyes; 0.66 G 0.17 mm, left eyes) was well correlated. The MCT points in fellow eyes tended to be symmetrical along the vertical midline. The mean angular distance be- tween mirror-superimposed MCT points was 20.54 G 17.6 degrees and the mean linear distance, 0.25 G 0.17 mm. CONCLUSIONS: The findings establish normative MCT pachymetry data and location using Fourier- domain OCT. The MCT and CCT points, although symmetrical, differed significantly in location and magnitude and should be evaluated separately in normal eyes and eyes with disease. Financial Disclosure: No author has a financial or proprietary interest in any material or method mentioned. Additional financial disclosures are found in the footnotes. J Cataract Refract Surg 2010; 36:1365–1372 Q 2010 ASCRS and ESCRS A tendency toward structural symmetry has been ob- served in fellow eyes of humans. The retinal nerve fi- ber layer, retinal capillary perfusion, astigmatic axis, higher-order aberrations (HOAs), and overall corneal thickness, as well as the epithelial thickness, have sim- ilar patterns, mirror-symmetric patterns, or both. 1–11 Minimum corneal thickness (MCT) is an important parameter in surgical planning and in the detection of pathology in certain corneal and refractive surgery procedures, in which accurate assessment of MCT and its location is crucial. 12–16 Errors in pachymetric measurement are factors in poor surgical outcomes, in- cluding ectasia after laser in situ keratomileusis. 17–19 Corneal topographic assessment can be inaccurate in the presence of motion artifacts. Fourier-domain optical coherence tomography (OCT), also known as frequency-domain tomography, overcomes this prob- lem to a large extent because of its high acquisition speed. 21,22,A In Fourier-domain OCT, the light from the reference arm interferes with the reflected light, generating spectral interference fringes that are even- tually analyzed using Fourier transformation. 20–22 Therefore, information in an entire A-scan area can be acquired by a charge-coupled device camera simul- taneously. This increases the acquisition rate many times without physical movement. 20–22 Recently, we found that Fourier-domain OCT has better repeatability than time-domain OCT (Visante, Carl Zeiss) for minimum, central, and paracentral cor- neal thickness measurements. 23 A previous study 24 Q 2010 ASCRS and ESCRS Published by Elsevier Inc. 0886-3350/$dsee front matter 1365 doi:10.1016/j.jcrs.2010.02.023 ARTICLE
-
Upload
gaurav-prakash -
Category
Documents
-
view
215 -
download
0
Transcript of Evaluation of bilateral minimum thickness of normal corneas based on Fourier-domain optical...
ARTICLE
Evaluation of bilater
al minimum thicknessof normal corneas based on Fourier-domainoptical coherence tomographyGaurav Prakash, MD, Dhivya Ashok Kumar, MD, Amar Agarwal, MS, FRCS, RCOphth,
Yoga Sarvanan, ME, Soosan Jacob, MS, DNB, FRCS, Athiya Agarwal, MD, DO
Q 2010 A
Published
SCRS an
by Elsev
PURPOSE: To determine the normative ranges and various aspects of the relationship between theminimum corneal thicknesses (MCT) in fellow eyes and the location of the MCT in relation to thecentral cornea using Fourier-domain optical coherence tomography (OCT).
SETTING: Tertiary care ophthalmic hospital, Chennai, India.
METHODS: In this cross-sectional observational trial, both eyes of consecutive healthy youngsubjects with a low refractive error and no clinical or topographic evidence of corneal disordershad bilateral pachymetric assessment with a Fourier-domain OCT platform (RTVue). The MCT,central corneal thickness (CCT), and x–y coordinates of the MCT location were noted.
RESULTS: The CCT and MCT followed a normal distribution with a good correlation. The differencebetween CCT and MCT was approximately 5 mm in right eyes and left eyes (P<.05 for both). Thedifference in CCT was the best predictor of the difference in MCT. The mean distance from the center(0.63 mm G 0.13 [SD], right eyes; 0.66 G 0.17 mm, left eyes) was well correlated. The MCT pointsin fellow eyes tended to be symmetrical along the vertical midline. The mean angular distance be-tween mirror-superimposed MCT points was 20.54 G 17.6 degrees and the mean linear distance,0.25 G 0.17 mm.
CONCLUSIONS: The findings establish normative MCT pachymetry data and location using Fourier-domain OCT. The MCT and CCT points, although symmetrical, differed significantly in location andmagnitude and should be evaluated separately in normal eyes and eyes with disease.
Financial Disclosure: No author has a financial or proprietary interest in any material or methodmentioned. Additional financial disclosures are found in the footnotes.
J Cataract Refract Surg 2010; 36:1365–1372 Q 2010 ASCRS and ESCRS
A tendency toward structural symmetry has been ob-served in fellow eyes of humans. The retinal nerve fi-ber layer, retinal capillary perfusion, astigmatic axis,higher-order aberrations (HOAs), and overall cornealthickness, as well as the epithelial thickness, have sim-ilar patterns, mirror-symmetric patterns, or both.1–11
Minimum corneal thickness (MCT) is an importantparameter in surgical planning and in the detectionof pathology in certain corneal and refractive surgeryprocedures, in which accurate assessment of MCTand its location is crucial.12–16 Errors in pachymetricmeasurement are factors in poor surgical outcomes, in-cluding ectasia after laser in situ keratomileusis.17–19
Corneal topographic assessment can be inaccuratein the presence of motion artifacts. Fourier-domain
d ESCRS
ier Inc.
optical coherence tomography (OCT), also known asfrequency-domain tomography, overcomes this prob-lem to a large extent because of its high acquisitionspeed.21,22,A In Fourier-domain OCT, the light fromthe reference arm interferes with the reflected light,generating spectral interference fringes that are even-tually analyzed using Fourier transformation.20–22
Therefore, information in an entire A-scan area canbe acquired by a charge-coupled device camera simul-taneously. This increases the acquisition rate manytimes without physical movement.20–22
Recently, we found that Fourier-domain OCT hasbetter repeatability than time-domain OCT (Visante,Carl Zeiss) for minimum, central, and paracentral cor-neal thickness measurements.23 A previous study24
0886-3350/$dsee front matter 1365doi:10.1016/j.jcrs.2010.02.023

1366 MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
found that time-domain OCT pachymetry correlatesbetter with the gold standard (ultrasound pachyme-try) than with Orbscan pachymetry (Bausch & Lomb).
The aim of the current study was to determine thenormative ranges and various aspects of the relation-ship between the minimum corneal thicknesses(MCT) in fellow eyes and the location of theMCT in re-lation to the central cornea using Fourier-domain opti-cal coherence tomography (OCT). To our knowledge,no similar study using the Fourier-domain OCT plat-form has been published.
SUBJECTS AND METHODS
This trial was performed at a tertiary care ophthalmic hospi-tal and approved by the institutional review board. The re-search followed the tenets of the Declaration of Helsinki.After receiving an explanation of the nature of the study,all subjects provided informed consent.
The participants in the study were normal young volun-teers with no previously documented ocular morbidity otherthan a myopic error less than or equal to �3.00 diopters (D).Slitlamp evaluation was performed to rule out corneal disor-ders, including ectatic disorders, scarring, or thinning. Orbs-can IIz topographic evaluation was also performed in allcases. The KISA% index25 and the Melki and Azar Massa-chusetts Eye and Ear Infirmary index26 were used to ruleout cases of keratoconus and cases suspected of keratoconus.Fellow eyes with unilateral forme fruste or more severe ker-atoconus were excluded from the study. No subject worecontact lenses.
To minimize the effect of diurnal variation in cornealthickness,27,28 all tests were performed between 2 PM and5 PM by the same experienced examiner. The sequence of ex-amination (right, left–left, right) was randomized by a com-puter-generated sequence of 100 randomly selected optionsusing the numbers 1 and 2 (1 Z right eye examined first;2 Z left eye examined first).
Corneal assessment was performed using the RTVue OCTsystemA (Optovue, Inc.), which takes 26 000 A-scans per sec-ond, a much higher acquisition speed than with most otheravailable anterior segment assessment devices. The optionalcornea anterior module was used for anterior segment imag-ing. The scan beam wavelength is 840 nm G 10 (SD) and theexposure power at the pupil, 750 mW.A The L lens of themodule can acquire 6.0 mm � 6.0 mm scans of the corneafor pachymetric analysis. The frame rate is 256 to 4096 Ascans/frame. The resolution depth is 5.0 mm and the
Submitted: August 20, 2009.Final revision submitted: January 15, 2010.Accepted: February 13, 2010.
From Dr. Agarwal’s Group of Eye Hospitals, Chennai, India.
Additional financial disclosures: Dr. Amar Agarwal is a consultant toAbbott Medical Optics Inc., Staar Surgical Co., and Bausch & Lomb.
Corresponding author: Amar Agarwal, MS, FRCS, FRCOphth, Dr.Agarwal’s Eye Hospital and Eye Research Centre, 19, CathedralRoad, Chennai-600 086, India. E-mail: [email protected].
J CATARACT REFRACT SURG -
transverse resolution, 15.0 mm. The scan beam wavelengthis 840 G 10 nm and the exposure power at the pupil, 750 W.
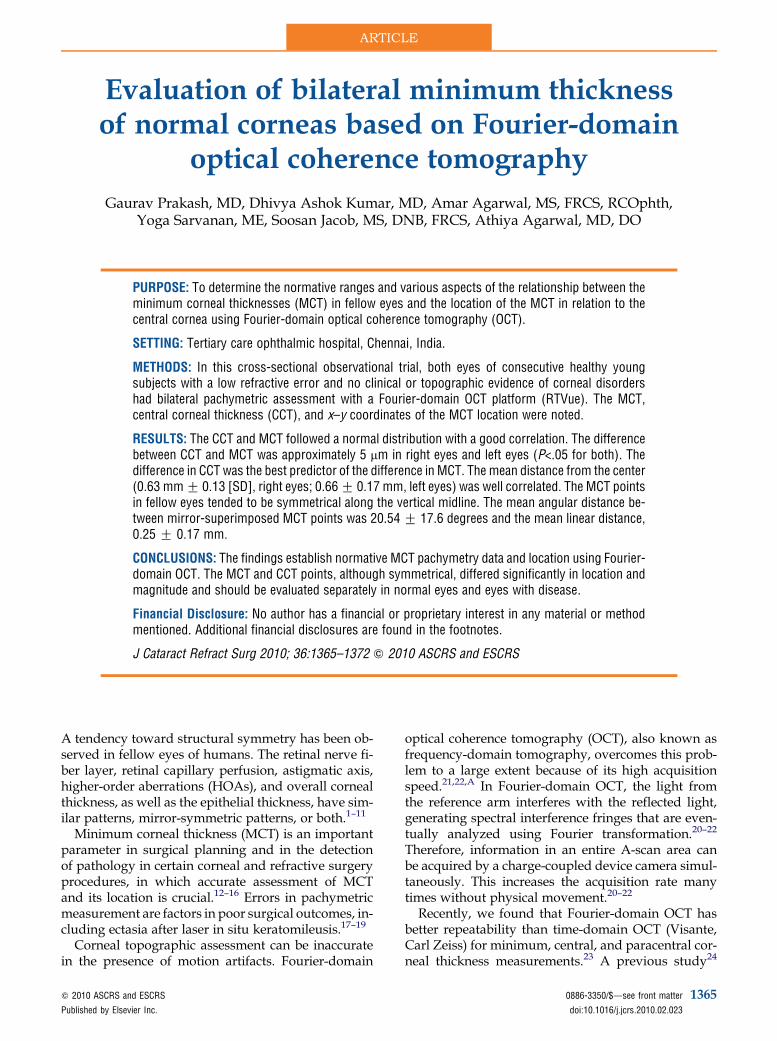
The subject’s head was positioned on the headrest. Theexaminer observed the infrared (IR) image of the corneaon the examination screen. All scans were performed withthe subject’s eye wide open by his or her own effort. Scan-ning was performed on visualization of a centered bright IRimage of the central cornea. No topical anesthesia or lubri-cating drops were used. The scan was repeated if the firstwas decentered or had a poor corneal apex reflection. Theoutput screen of the OCT system shows an IR image ofthe cornea in the upper right followed by, in clockwisedirection, keratoconus analysis data, an axial scan ofthe cornea, a color-coded corneal pachymetry map, anda numerical data map divided into zones (Figure 1). The2.0 mm central zone is surrounded by a 2.0 to 5.0 mmzone and a 5.0 to 6.0 mm zone divided into 45-degree sub-tending angles. The mean pachymetry in the respectivezones is included in the output. The MCT and its relationto the center of the cornea are shown in the keratoconusanalysis box. The location is also marked on the color-coded pachymetric map.
Mathematical Calculations and Transformations
The distance of the MCT from the center of the cornea wascalculated as
D Z�x2 þ y2
�0:5
To assess symmetry, the left-eye coordinates were trans-formed along possible axes to match the right eye data andevaluated for patterns and symmetry. A direct symmetrymodel was evaluated with the original values of R(x, y)and L(x, y). Then, reflections were performed along the y-axis (vertical midline, x Z 0), along the x-axis (horizontalmidline, y Z 0), and across the equivalence diagonal (y Z x).
The distance between the right-eye coordinates R(x, y) andthe transformed left-eye coordinates (x0, y0) was calculated as
S ZhðRx � Lx0Þ2 þ ðRy � Ry0Þ2
i0:5
To determine the angular distance, the angle q between Rand L0 was calculated as
q Z cos�1fðR � L0Þ=ðjRj� jL0jÞgwhere
R�L0Z ðRx� Lx0 þ Ry�LyÞand the cross product of R is L0
jRj � jL0j Zh�Rx2 þ Ry2
�0:5i �h�Lx2 þ Ly2
�0:5i
The angle was then converted from radians to degrees.
Statistical Analysis
The data were analyzed using SPSS software (version16.0, SPSS, Inc.). Paired t tests were used to analyze the dif-ferences in mean values, which are reported with the stan-dard deviation. Correlation coefficients and best-fit linearequations were computed to assess the correlation betweenmeasurements in right eyes and measurements in left eyes.Bland-Altman plots were drawn to show the effect of cornealthickness on the difference in measurements between the 2
VOL 36, AUGUST 2010
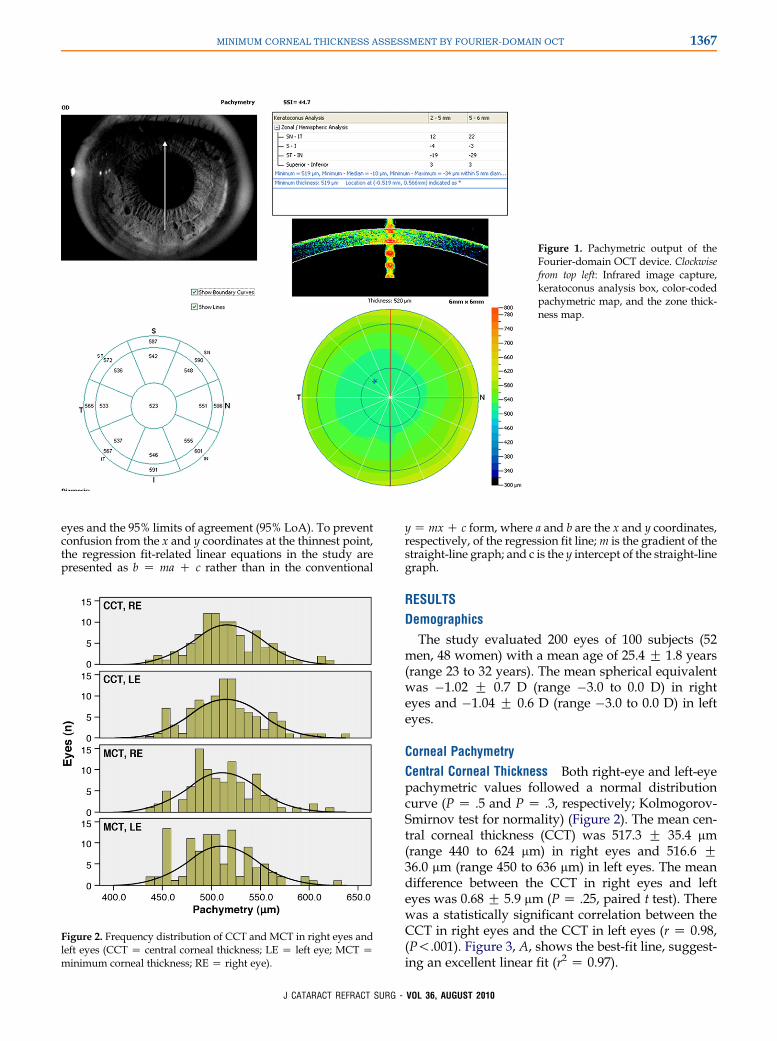
Figure 1. Pachymetric output of theFourier-domain OCT device. Clockwisefrom top left: Infrared image capture,keratoconus analysis box, color-codedpachymetric map, and the zone thick-ness map.
1367MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
eyes and the 95% limits of agreement (95% LoA). To preventconfusion from the x and y coordinates at the thinnest point,the regression fit-related linear equations in the study arepresented as b Z ma C c rather than in the conventional
Figure 2. Frequency distribution of CCT and MCT in right eyes andleft eyes (CCT Z central corneal thickness; LE Z left eye; MCT Zminimum corneal thickness; RE Z right eye).
J CATARACT REFRACT SURG -
y Z mx C c form, where a and b are the x and y coordinates,respectively, of the regression fit line;m is the gradient of thestraight-line graph; and c is the y intercept of the straight-linegraph.
RESULTS
Demographics
The study evaluated 200 eyes of 100 subjects (52men, 48 women) with a mean age of 25.4 G 1.8 years(range 23 to 32 years). The mean spherical equivalentwas �1.02 G 0.7 D (range �3.0 to 0.0 D) in righteyes and �1.04 G 0.6 D (range �3.0 to 0.0 D) in lefteyes.
Corneal Pachymetry
Central Corneal Thickness Both right-eye and left-eyepachymetric values followed a normal distributioncurve (P Z .5 and P Z .3, respectively; Kolmogorov-Smirnov test for normality) (Figure 2). The mean cen-tral corneal thickness (CCT) was 517.3 G 35.4 mm(range 440 to 624 mm) in right eyes and 516.6 G36.0 mm (range 450 to 636 mm) in left eyes. The meandifference between the CCT in right eyes and lefteyes was 0.68 G 5.9 mm (P Z .25, paired t test). Therewas a statistically significant correlation between theCCT in right eyes and the CCT in left eyes (r Z 0.98,(P!.001). Figure 3, A, shows the best-fit line, suggest-ing an excellent linear fit (r2 Z 0.97).
VOL 36, AUGUST 2010

Figure 3. Linear best-fit plots between pachymetric values. A: Cen-tral corneal thickness in right eye (CCTR) and left eye (CCTL). B:Minimum corneal thickness in right eye (MCTR) and left eye(MCTL).
Figure 4. Overlay Bland-Altman plot showing the difference infellow-eye pachymetry as a function of the mean pachymetry inright eyes and in left eyes.
1368 MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
Minimum Corneal Thickness Both right-eye and left-eye values followed a normal distribution curve(P Z .5 and P Z .7, respectively; Kolmogorov-Smirnov Z test) (Figure 2).The mean MCT was 511.9G 35.2 mm (range 435 to 624 mm) in right eyes and
Table 1. Symmetry analysis of the right and left eye coordinates.
Original Coordinates (M
Right Eye
Transform Group Rx Ry
I �0.51 G 0.20 �0.28 G 0.43 �II �0.51 G 0.20 �0.28 G 0.43 �III �0.51 G 0.20 �0.28 G 0.43 �IV �0.51 G 0.20 �0.28 G 0.43 �
Transform Z transformation*Analysis of variance, Tukey HSD
J CATARACT REFRACT SURG -
511.7 G 35.7 mm (range 440 to 633 mm) in left eyes.The mean difference in the MCT between right eyesand left eyes was 0.29 G 5.86 mm (P Z .6, pairedt test).There was a statistically significant correlationbetween the 2 MCT values (r Z 0.98, P!.001).Figure 3, B, shows the best-fit line, suggesting an excel-lent linear fit (r2 Z 0.97).
Difference Between Central and MinimumPachymetry
The mean pachymetric difference between the CCTand theMCTwas 5.34G 4.48 mm in right eyes and 4.95G 3.6 mm in left eyes (both P!.001, paired t test).
Relationship Between Thicknesses in Thinnerand Thicker Corneas
An overlay Bland-Altman plot to determinewhether the difference in fellow-eye MCT or CCT
ean G SD)
Left Eye
Lx Ly Transform Along Line
0.51 G 0.28 �0.21 G 0.33 None0.51 G 0.28 �0.21 G 0.33 x Z 00.51 G 0.28 �0.21 G 0.33 y Z 00.51 G 0.28 �0.21 G 0.33 x Z y
VOL 36, AUGUST 2010

1369MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
was more or less in thinner or thicker corneas (differ-ence in pachymetry as a function of mean pachymetryfor MCT and CCT separately) showed a 95% LoArange of 23.5 mm and 25.8 mm for MCT and CCT, re-spectively. Both measures showed a poor statisticallynonsignificant linear fit (Figure 4).
Location of Minimum Corneal Thickness
The Cartesian location of the point of MCT wasgiven in the output screen as x and y coordinates (inmillimeters), with the center of the cornea being 0.0.Therefore, the right-eye and left-eye coordinateswere denoted as R(x,y) and L(x,y). The mean value ofthe x coordinate was �0.51 G 0.21 mm (range �0.91to �0.06 mm) in right eyes (Rx) and 0.46 G 0.32 mm(range �0.30 to 1.09 mm) in left eyes (Lx). The meanvalue of the y coordinate was �0.24 G 0.23 mm(range �0.82 to 0.40 mm) in right eyes (Ry) and�0.30 G 0.28 mm (�1.06 to 0.74 mm) in left eyes(Ly). Therefore, the position of the thinnest point(r2 Z 0.68 and r2 Z 0.47 for x coordinate and y coordi-nate, respectively) was not as highly correlated be-tween eyes as the pachymetric value (r2 Z 0.97).
The location (x and y coordinates) of the thinnestpoints in right eyes and in left eyeswas statistically sig-nificantly different from the location of the center ofthe cornea (0, 0) (P!.001; 1-sample t test with testvalue of zero).
Distance of Minimum Corneal Thicknessfrom Center
The mean distance between the MCT and the centerof the cornea was 0.63 G 0.13 mm (range 0.46 to0.98 mm) in right eyes and 0.66 G 0.17 mm (range0.38 to 1.11 mm) in left eyes. The mean difference inthe distance between right eyes and left eyes was�0.03 G 0.08 mm (P!.001, paired t test). There wasa good linear correlation between the 2 eyes(r Z 0.87, P!.001).
Change inCoordinates of L Mean Lx0 G (SD) Mean Ly0 G (SD)
MeaBetwee
L(x,y) / L(x, y) 0.51 G 0.28 �0.21 G 0.33L(x,y) / L(�x, y) �0.51 G 0.28 �0.21 G 0.33L(x,y) / L(x, �y) 0.51 G 0.28 0.21 G 0.33L(x,y) /L(�x, �y) �0.51 G 0.28 0.21 G 0.33
Table 1. (continued)
J CATARACT REFRACT SURG -
Symmetry
Table 1 shows the transformations along the directsymmetry model (Figure 5, A), the vertical midline(Figure 5, B), the horizontal midline (Figure 5, C),and the across-the-equivalence diagonal (y Z x)(Figure 5, D).
The distance between the right-eye coordinates andthe transformed left-eye coordinates was significantlylower for the reflection along the y-axis (vertical mirrorsymmetry) than the original position (direct symme-try) and the other 2 transformations along the x-axisand along the y Z x (analysis of variance with TukeyHSD, Table 1). Therefore, the location of the thinnestpoints in right eyes and in left eyes tended to havesymmetry along the vertical midline.
Normal Range of Symmetry of Linear and AngularDistances
The finding that there was symmetry along x Z0 helped establish the normal range of the minimumlinear and angular distances between the locations’ 2corresponding MCT points. This analysis used theoriginal right-eye coordinates (Rx, Ry) and trans-formed left-eye coordinates (Lx0, Ly), where Lx0 ZLx � (�1). The mean scalar (linear) distance was 0.25G 0.17 mm (range 0.1 to 0.79 mm) (Figure 6). Themean angular distance between the points of MCTwas 20.54 G 17.6 degrees (range 0.06 to 74.2 degrees).
DISCUSSION
Accurate noncontact analysis of corneal structure hasbeen difficult. Previous studies have evaluatedscanning-slit, rotating Scheimpflug imaging, andtime-domain OCT platforms for such analysis. In a re-cent study,23 we found that repeated Fourier-domainOCT corneal pachymetry measurements were highlyconsistent and, in contrast to time-domain OCT, didnot seem to underestimate normal corneal thickness.
The variability in MCT and CCT measurements hasbeen a recent area of interest. Rufer et al.29 used
n Distance (mm)n R(x,y) and L(x0,y0)
Difference fromSmallest Distance (II) (mm) P Value*
1.07 G 0.44 0.81 .0010.25 G 0.17 0.00 d
1.32 G 0.30 1.06 .0010.65 G 0.39 0.40 .001
VOL 36, AUGUST 2010
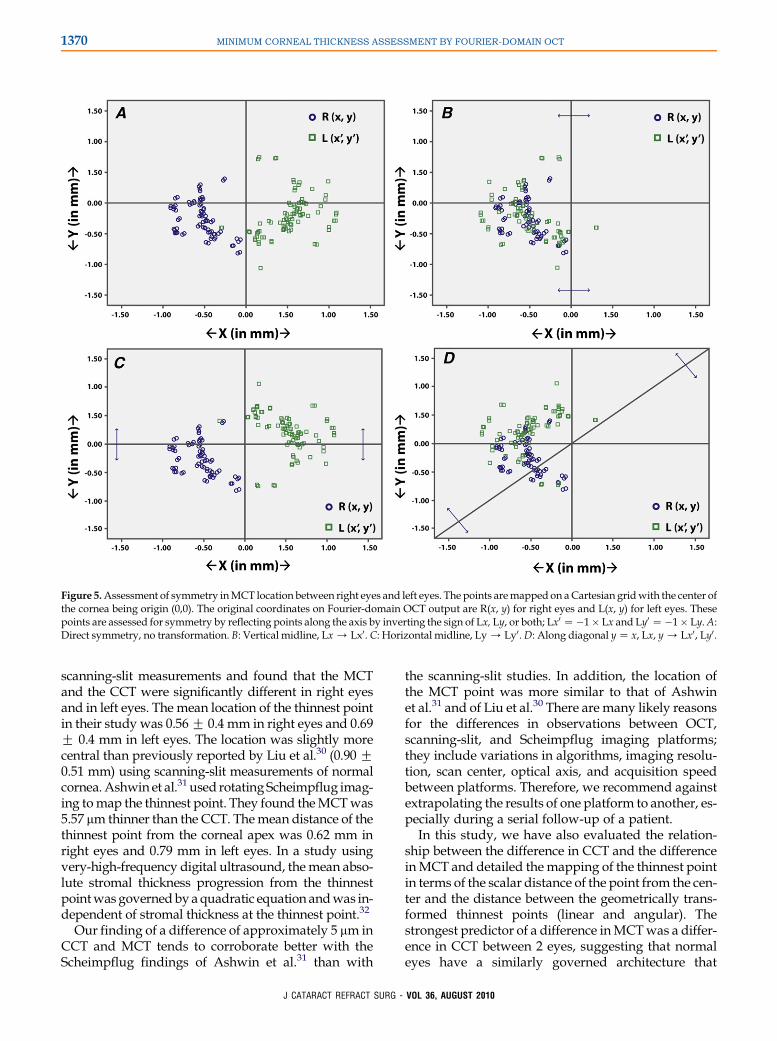
Figure 5.Assessment of symmetry inMCT location between right eyes and left eyes. The points aremapped on aCartesian gridwith the center ofthe cornea being origin (0,0). The original coordinates on Fourier-domain OCT output are R(x, y) for right eyes and L(x, y) for left eyes. Thesepoints are assessed for symmetry by reflecting points along the axis by inverting the sign of Lx, Ly, or both; Lx0 Z�1� Lx and Ly0 Z�1� Ly.A:Direct symmetry, no transformation. B: Vertical midline, Lx / Lx0. C: Horizontal midline, Ly / Ly0.D: Along diagonal y Z x, Lx, y / Lx0, Ly0.
1370 MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
scanning-slit measurements and found that the MCTand the CCT were significantly different in right eyesand in left eyes. The mean location of the thinnest pointin their study was 0.56 G 0.4 mm in right eyes and 0.69G 0.4 mm in left eyes. The location was slightly morecentral than previously reported by Liu et al.30 (0.90 G0.51 mm) using scanning-slit measurements of normalcornea.Ashwin et al.31 used rotating Scheimpflug imag-ing tomap the thinnest point. They found theMCTwas5.57 mm thinner than the CCT. Themean distance of thethinnest point from the corneal apex was 0.62 mm inright eyes and 0.79 mm in left eyes. In a study usingvery-high-frequency digital ultrasound, themean abso-lute stromal thickness progression from the thinnestpointwas governedbyaquadratic equation andwas in-dependent of stromal thickness at the thinnest point.32
Our finding of a difference of approximately 5 mm inCCT and MCT tends to corroborate better with theScheimpflug findings of Ashwin et al.31 than with
J CATARACT REFRACT SURG -
the scanning-slit studies. In addition, the location ofthe MCT point was more similar to that of Ashwinet al.31 and of Liu et al.30 There are many likely reasonsfor the differences in observations between OCT,scanning-slit, and Scheimpflug imaging platforms;they include variations in algorithms, imaging resolu-tion, scan center, optical axis, and acquisition speedbetween platforms. Therefore, we recommend againstextrapolating the results of one platform to another, es-pecially during a serial follow-up of a patient.
In this study, we have also evaluated the relation-ship between the difference in CCT and the differenceinMCT and detailed themapping of the thinnest pointin terms of the scalar distance of the point from the cen-ter and the distance between the geometrically trans-formed thinnest points (linear and angular). Thestrongest predictor of a difference inMCTwas a differ-ence in CCT between 2 eyes, suggesting that normaleyes have a similarly governed architecture that
VOL 36, AUGUST 2010

Figure 6.Diagramof a superimposed image of fellow-eye pachymet-ric output showing different entities used to map the thinnest point.Terms: R(x, y) and L(x, y) Z original locations; L(x0,y) Z reflection ofL along vertical midline; q Z angle between the 2 points with thecenter of the cornea as the vertex; S Z scalar distance between the2 points; DR and DL Z the distance of the locations of the points ofMCT from the central cornea for right eyes and left eyes. The differ-ence is seen as an annular zone denoted by the circles drawn withdashed lines.
1371MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
determines CCT and MCT. It will be interesting to de-termine whether such a relationship is disturbed incorneas with pathology. Using time-domain OCT, Liet al.14 found that a pachymetry-based diagnostic cri-teria of keratoconus may be as sensitive and specificas the topography-based KISA% index.
Mirror symmetry that is not superimposable hasbeen reported in refractive entities such as astigmatismaxis and HOAs.1–5 We found that the location of thin-nest cornea had best symmetry along the vertical mid-line. The relationship between the angle k, HOAs, thethinnest point, and the center of the corneal domeshould be studied further. As of now, OCT platformsdo not measure the angle k, and a similar study shouldbe performed with a single, fast instrument operatingat high acquisition speeds to compensate for move-ment errors.
The current study provides normative data forMCTas well as its location in relation to the central cornealarea with Fourier-domain OCT, a high-speed acquisi-tion system. The use of Fourier-domain OCT ensuredthat the motion artifact was reduced to a minimum.The study confirmed that the CCT andMCT are not in-terchangeable and that both should be considered sep-arately when evaluating eyes for corneal disease andsurgical planning. The ranges in the normal variationsin the thinnest point of the cornea in normal eyes canserve as useful parameters for ruling out pathology.
J CATARACT REFRACT SURG -
A study with a population that includes eyes with ker-atoconus, forme fruste keratoconus, high myopia, andhyperopia is underway and should provide further in-formation in this area.
REFERENCES1. Harris WF. Technical note: accounting for anatomical symmetry
in the first-order optical character of left and right eyes. Ophthal-
mic Physiol Opt 2007; 27:412–415
2. McKendrick AM, Brennan NA. The axis of astigmatism in right
and left eye pairs. Optom Vis Sci 1997; 74:668–675
3. Marcos S, Burns SA. On the symmetry between eyes of wave-
front aberration and cone directionality. Vision Res 2000;
40:2437–2447
4. Guggenheim JA, Zayats T, Prashar A, To CH. Axes of astigma-
tism in fellow eyes show mirror rather than direct symmetry. Oph-
thalmic Physiol Opt 2008; 28:327–333
5. Smolek MK, Klyce SD, Sarver EJ. Inattention to nonsuperimpos-
able midline symmetry causes wavefront analysis error. Arch
Ophthalmol 2002; 120:439–447
6. Gatinel D, Delair E, Abi-Farah H, Hoang-Xuan T. Etude de la dis-
tribution et de l’enantiomorphisme des aberrations optiques ocu-
laires de haut degre [Distribution and enantiomorphism of
higher-order ocular optical aberrations]. J Fr Ophtalmol 2005;
28:1041–1050. Available at: http://www.em-consulte.com/
showarticlefile/112940/index.pdf. Accessed April 7, 2010
7. Sugimoto M, Ito K, Goto R, Uji Y. Symmetry analysis for detect-
ing early glaucomatous changes in ocular hypertension using
optical coherence tomography. Jpn J Ophthalmol 2004; 48:
281–286
8. Rawji MH, Flanagan JG. Intraocular and interocular symmetry in
normal retinal capillary perfusion. J Glaucoma 2001; 10:4–12
9. Essock EA, Sinai MJ, Fechtner RD. Interocular symmetry in
nerve fiber layer thickness of normal eyes as determined by po-
larimetry. J Glaucoma 1999; 8:90–98
10. Myrowitz EH, Kouzis AC, O’Brien TP. High interocular corneal
symmetry in average simulated keratometry, central corneal
thickness, and posterior elevation. Optom Vis Sci 2005; 82:
428–431
11. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ.
Epithelial thickness in the normal cornea: three-dimensional dis-
play with Artemis very high-frequency digital ultrasound.
J Refract Surg 2008; 24:571–581
12. Randleman JB, Trattler WB, Stulting RD. Validation of the Ecta-
sia Risk Score System for preoperative laser in situ keratomileu-
sis screening. Am J Ophthalmol 2008; 145:813–818
13. Das S, Sullivan LJ. Comparison of residual stromal bed and flap
thickness in primary and repeat laser in situ keratomileusis in
myopic patients. J Cataract Refract Surg 2006; 32:2080–2084
14. Li Y, Meisler DM, Tang M, Lu ATH, Thakrar V, Reiser BJ,
Huang D. Keratoconus diagnosis with optical coherence tomog-
raphy pachymetry mapping. Ophthalmology 2008; 115:
2159–2166
15. Michieletto P, Balestrazzi A, Balestrazzi A, Mazzotta C,
Occhipinti I, Rossi T. Factors predicting unsuccessful big bubble
deep lamellar anterior keratoplasty. Ophthalmologica 2006;
220:379–382
16. Spoerl E, Mrochen M, Sliney D, Trokel S, Seiler T. Safety of UVA–
riboflavin cross-linking of the cornea. Cornea 2007; 26:385–389
17. Reinstein DZ, Srivannaboon S, Archer TJ, Silverman RH,
Sutton H, Coleman DJ. Probability model of the inaccuracy of re-
sidual stromal thickness prediction to reduce the risk of ectasia
after LASIK. Part I: quantifying individual risk. J Refract Surg
2006; 22:851–860
VOL 36, AUGUST 2010

1372 MINIMUM CORNEAL THICKNESS ASSESSMENT BY FOURIER-DOMAIN OCT
18. Cheng H-C, Chen Y-T, Yeh S-I, Yau C-W. Errors of residual stro-
mal thickness estimation in LASIK. Ophthalmic Surg Lasers Im-
aging 2008; 39:107–113
19. Li EYM, Mohamed S, Leung CKS, Rao SK, Cheng ACK,
Cheung CYL, Lam DSC. Agreement among 3 methods to
measure corneal thickness: ultrasound pachymetry, Orbscan
II, and Visante anterior segment optical coherence tomography.
Ophthalmology 2007; 114:1842–1847
20. Chen TC, Cense B, Pierce MC, Nassif N, Park BH, Yun SH,
White BR, Bouma BE, Tearney GJ, de Boer JF. Spectral domain
optical coherence tomography; ultra-high speed, ultra-high
resolution ophthalmic imaging. Arch Ophthalmol 2005;
123:1715–1720
21. de Boer JF, Cense B, Park BH, Pierce MC, Tearney GJ,
Bouma BE. Improved signal-to-noise ratio in spectral-domain
compared with time-domain optical coherence tomography.
Opt Lett 2003; 28:2067–2069
22. Yi K, Mujat M, Park BH, Sun W, Miller JW, Seddon JM,
Young LH, de Boer JF, Chen TC. Spectral domain optical coher-
ence tomography for quantitative evaluation of drusen and asso-
ciated structural changes in non-neovascular age-related
macular degeneration. Br J Ophthalmol 2009; 93:176–181
23. Prakash G, Agarwal A, Jacob S, Kumar DA, Agarwal A,
Banerjee R. Comparison of Fourier-domain and time-domain
optical coherence tomography for assessment of corneal thick-
ness and intersession repeatability. Am J Ophthalmol 2009; 148:
282–290
24. Ho T, Cheng ACK, Rao SK, Lau S, Leung CKS, Lam DSC. Central
corneal thickness measurements using Orbscan II, Visante, ultra-
sound, and Pentacam pachymetry after laser in situ keratomileu-
sis for myopia. J Cataract Refract Surg 2007; 33:1177–1182
25. Rabinowitz YS, Rasheed K. KISA% index: a quantitative video-
keratography algorithm embodying minimal topographic criteria
for diagnosing keratoconus. J Cataract Refract Surg 1999; 25:
1327–1335; errata 2000; 26:480
26. Melki SA, Azar DT. LASIK complications: etiology, manage-
ment, and prevention. Surv Ophthalmol 2001; 46:95–116
J CATARACT REFRACT SURG -
27. Read SA, Collins MJ. Diurnal variation of corneal shape and
thickness. Optom Vis Sci 2009; 86:170–180
28. Lattimore MR Jr, Kaupp S, Schallhorn S, Lewis R IV. Orbscan
pachymetry; implications of a repeated measures and diurnal
variation analysis. Ophthalmology 1999; 106:977–981
29. Rufer F, Sander S, Klettner A, Frimpong-Boateng A, Erb C.
Characterization of the thinnest point of the cornea compared
with the central corneal thickness in normal subjects. Cornea
2009; 28:177–180
30. Liu Z, Huang AJ, Pflugfelder SC. Evaluation of corneal thickness
and topography in normal eyes using the Orbscan corneal to-
pography system. Br J Ophthalmol 1999; 83:774–778. Available
at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1723104/pdf/
v083p00774.pdf. Accessed April 7, 2010
31. Ashwin PT, Shah S, Pushpoth S, Wehbeh L, Ilango B. The rela-
tionship of central corneal thickness (CCT) to thinnest central
cornea (TCC) in healthy adults. Contact Lens Anterior Eye
2009; 32:64–67
32. Reinstein DZ, Archer TJ, Gobbe M, Silverman RH, Coleman DJ.
Stromal thickness in the normal cornea: three-dimensional dis-
play with Artemis very high-frequency digital ultrasound.
J Refract Surg 2009; 25:776–786
OTHER CITED MATERIALA. Optovue, Inc. RTVue Overview. Available at: http://www.
optovue.com/products/rtvue. Accessed April 7, 2010
VOL
36, AUGUST 2010First author:Gaurav Prakash, MD
Tertiary care ophthalmic hospital,Chennai, India


















