
Evaluating Autism Spectrum Disorders with the ADOS
73
Including Every Learner: How schools, families, and experts can better educate children with challenges David Black, PhD Pediatric Neuropsychologist Laura Kenealy, PhD Children’s National Medical Center Dr. Black’s presentation is based on his expertise with autism and as a pediatric neuropsychologist, and is not acting in an official capacity for the National Institutes of Health.
Transcript of Evaluating Autism Spectrum Disorders with the ADOS
Including Every Learner: How schools, families,
and experts can better educate children with challenges
David Black, PhDPediatric Neuropsychologist
Laura Kenealy, PhDChildren’s National Medical Center
Dr. Black’s presentation is based on his expertise with autism and as a pediatric neuropsychologist, and is not acting in an official capacity for the National Institutes of Health.

Including Every Learner:Why it matters
Major trends in education1. Inclusion of special needs learners at
every level2. Larger population in early education
settings than ever before3. Stakes are higher than ever
Exploring barriers
Teachers may feel unprepared to cope with special needs learners…
Parents may wonder what is best for their child…
Some students are less able to benefit from inclusion…

Making it Work
Five factors associated with successful inclusion (Webber, 1997)
Making it Work
1. Sense of Community and Social Acceptance
“I am as good as others here”
“Everyone makes a valuable contribution to our group”

2. Appreciation for Diversity
“I like to learn about how we’re different.”
3. Attention to Curricular Needs“What I teach meets the needs of my learners”
4. Effective Management and Instruction
“I know what works”
“Everything about my class helps me learn”
5. Personnel Support and Collaboration
“I have the support of my team.”
Overview
Learning about our learners with special needs:
* Autism Spectrum Disorders* Language Delays* Sensory Processing Problems* Learning Difficulties* Attention and Impulsivity
Problems

Overview
What it is What it looks like in the early education
setting What the science tells us Classroom strategies that work: Tips
and Tricks for all kinds of special needs kids

Autism Spectrum Disorders
Autism Spectrum Disorders
Prevalence Rates What is Autism Recognizing Autism in the Classroom Latest Research Autism in inclusion classrooms
Prevalence of Autism
Rate of autism is ~1%› 2008: CDC Estimates 1/110 diagnosed with autism› 2007: UK Adult Psychiatric Comorbidity study estimate 1% › 2007: National Survey of Children's Health (sample size:
78,037)
Gender ratio: 4-5:1 male: female No differences across racial/ethnic groups
› Some research suggests African American children diagnosed later, however
59% (range 49-70%) have IQ > 70› CDC, 2007; 2002 surveillance data
Prevalence Rates
Rates have been steadily increasing over past 20+ years
Recent study of special education enrollment data in Wisconsin suggest the increase may be leveling off in some areas (Maenner and Durkin, 2010).

Autism Prevalence: Past 15 Years
Number (per 1,000) of children aged 6–17 who were served under the IDEA with a diagnosis of autism, from 1996 through 2007.
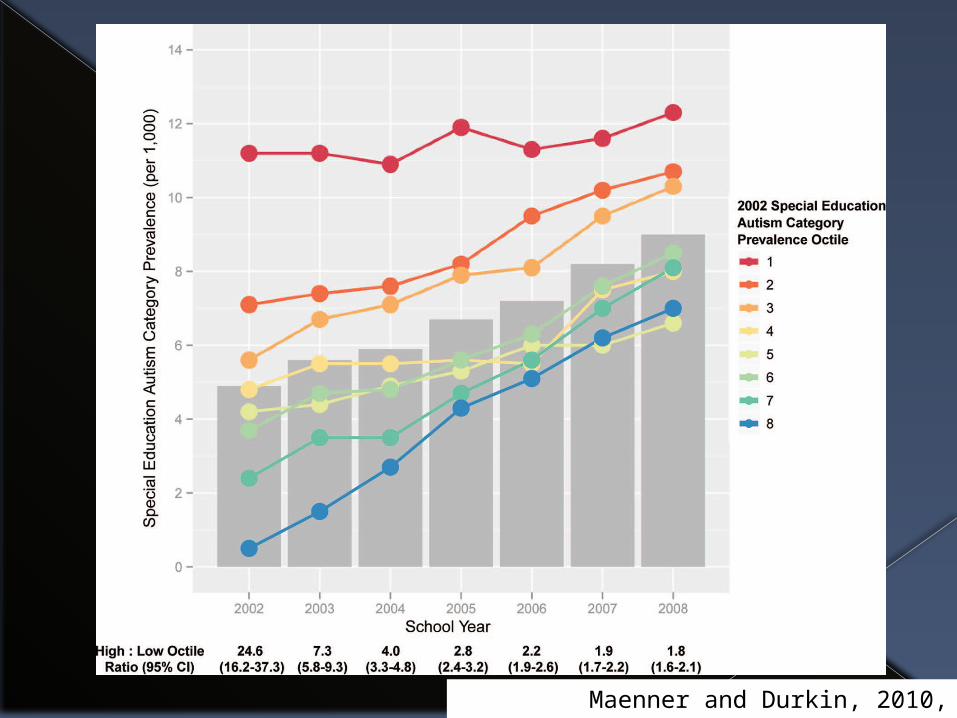
Maenner and Durkin, 2010, Pediatrics

What Causes Autism
~90% of cases, we don’t know ~10% of cases associated with known
chromosomal or genetic disorders Most heritable of all neuropsychiatric
conditions› Identical twin concordance: 60-96%› Sibling risk: 2-8%
Poor parenting practices DO NOT cause autism
Research has NO LINK between vaccines and autism
CDC.gov, 11.3.2010

Autism Spectrum Disorders Include …
Autism/Autistic Disorder Asperger’s Syndrome Pervasive Developmental Disorder, Not
Otherwise Specified (PDD-NOS) Autism Spectrum Disorder **Nonverbal Learning Disability**

Autism Spectrum Disorders: Symptoms in Three Main Areas
Social Impairment
Repetitive Behaviors & Restricted Interests
Speech/Communication
Deficits
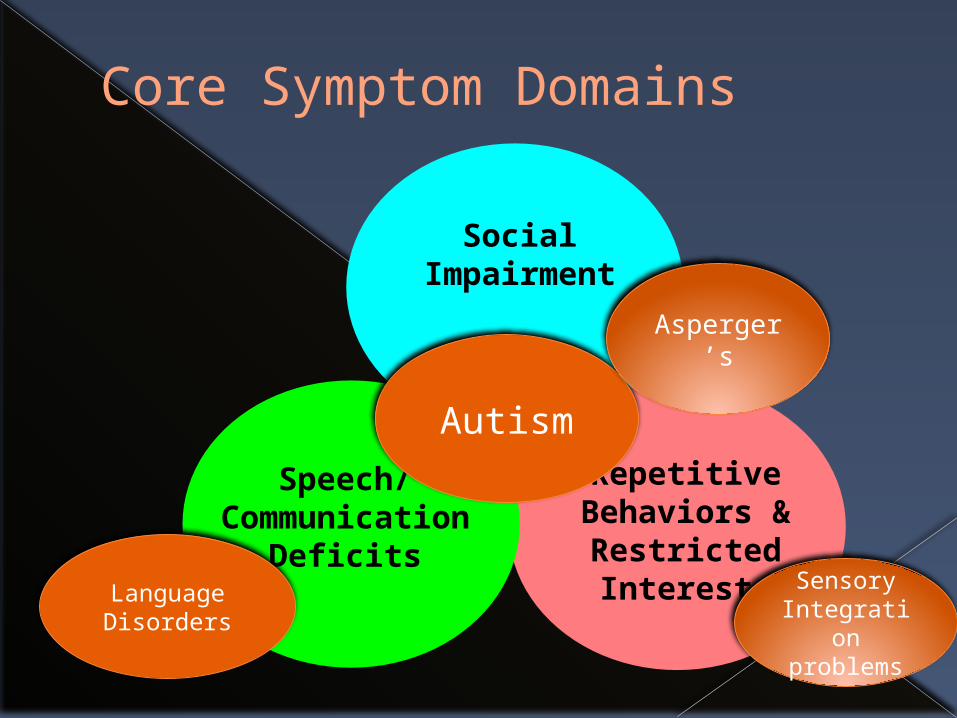
Core Symptom Domains
Social Impairment
Repetitive Behaviors & Restricted Interests
Speech/Communication
Deficits
Autism
Language Disorders
Asperger’s
Sensory Integration problems
ASD is Very Broad
Broad range of….› Intellectual functioning› Social Interest and motivation› Social competence› Language ability › Repetitive, unusual, challenging behaviors

http://www.cdc.gov/ncbddd/autism/signs.html
Impaired Social Interaction
Includes: Deficits in nonverbal communication Failure to develop peer relationships Spontaneously seeking to share
enjoyment Lack of social or emotional reciprocity Impaired social cognition

Impaired Nonverbal Communication
Eye contact Communicative use of gestures/body
language Directed facial expressions Flat or limited range of facial
expression Inappropriate facial expressions
Failure to Develop Peer Relationships
Unable to sustain reciprocal friendships Lack of interest/oblivious Lack of responsiveness when other
children approach Avoidance of peer interactions Preference to play alone Overly rule bound in social interaction Lack of sharing
Lack of Shared Enjoyment
Limited social initiation Lack of bringing or showing objects Unlikely to share interest or excitement
of activities No reaction to praise No desire to please
Social Reciprocity
Lack of social awareness Little interest in social interaction Tends to be more “object oriented”
than “socially oriented” Excessively directive or rigid in social
interactions Does not notice another’s lack of
interest

Social Cognition: Social Thinking
Impaired ability to … Make social predictions Grasp impact of actions on others Imagine thoughts and feelings of others Develop, maintain, and repair a social
interchange Recognize social mishaps Recognize/follow social convention Recognize distress in others

Impaired Communication
Language delay Inability to sustain a conversation Stereotyped, repetitive, idiosyncratic
language use Lack of varied make-believe, or social
imitative play
Language Delay
Understanding spoken language Communicating verbally Lack of compensation through other
means*› Gesture› Facial expression› Bringing of objects
*Differs in children with ASDs and language delay
Reciprocal Conversation
Conversation may be one-sided Limited in flexibility or range of topics Back and forth of interchange may be
limited Minimal “social chat”

Stereotyped Speech
Scripted, repetitive use of speech Echolalic speech Unusual use of language Neologisms Pedantic “little professor” speech Odd intonation, rhythm, or pitch to
vocal quality
Limited Imaginative Play Skills
Play tends to literal, functional, concrete Difficulty ascribing agency to figures
› E.g. Elmo feeding Buzz Light Year Impacts social play and cooperative play In young children, functional play skills
may also be limited

Repetitive Behaviors and Restricted Interests
Excessive preoccupation with stereotyped pattern of interest
Inflexible adherence to routine and rituals
Persistent preoccupation with parts of objects
Stereotyped repetitive motor mannerisms
Stereotyped Pattern of Interests
Fixated interest May be odd – doors, bumpers on cars May be a conventional interest but
extreme – obsession with dinosaurs, maps, or a favorite movie
Excessively perfectionistic Socially interfering, limiting other
activities

Difficulty with Transition & Changes in Routine
Rigid adherence to routines Transition between activities (even
preferred activities) very difficult Unusual compulsion or rituals with
routine events Catastrophic reaction to minor changes
in environment Lining up objects

Hand and Whole Body Mannerisms
Hand flapping Finger flicking Repetitively bouncing or spinning
Repetitive & Unusual Use of Objects
Non-function use of a part of an object – spinning wheels, opening/closing doors
Sensory interest in objects› Smelling people or objects› Preoccupation with texture› Close visual inspection› Seeking proprioceptive input
Cognitive Profile
Developmental delay/Intellectual deficits Splinter strengths Language deficits Poor self-regulation Weaknesses in executive functioning Poor motor planning/graphomotor control Sensory sensitivity/sensory integration
weaknesses

Sensory Processing ProblemsOversensitivityUndersensitivity

Sensory Processing Problems
Difficulty with the processing of sensory input› Sight, sound, taste, texture, proprioception
Oversensitivity or undersensitivity No formal criteria to diagnosis Usually identified by an occupational
therapist
Sensory Processing Problems
Oversensitivity: Aversion to› Texture (play dough, rice, finger paint,
grass)› Light (fluorescent light, bright sunlight)› Sound (classroom noise, lots of children
talking, loud music)› Being touched
Undersensitivity usually to pain, but also to hot and cold
What do we know…
Higher rate of oversensitivity in clinical populations› ASD – 56%› ADHD – 69%
Undersensitivity also very common in ASD

What do we know…
Oversensivity has been associated with› Anxiety/internalizing problems› Difficulty modulating response to input
If distracted by sensory input, then harder to respond in a socially appropriate, well-modulated manner
What do we know…
Birth cohort study n=925 › Developmental disorders excluded
16% of elementary children reported tactile sensitivity – 4 tactile sensations› May not be impairing, however
Oversensitivity › 4-fold increase in internalizing problems› Less social competence (empathy,
prosocial behavior)Ben-Sasson, Carter, Briggs-Gowan, 2009, Journal of Abnormal Child Psychology

Language Disorders
Comprehension of languageSpeech sound disordersPhonological disorders
Language Disorders
Impairment in comprehension and/or use of language › Speech sound disorders very common
8% of kindergarteners have a specific language impairment (SLI)
5% of 1st graders have a recognizable speech (phonological) disorder › Range from sound substitutions to
impaired communication
http://www.nidcd.nih.gov/StaticResources/about/Plans/strategic/strategic06-08.pdf
Language Disorders
Affects boys 1.5 times more than girls 20-40% have family history of SLI Associated with future learning
disorders› Especially reading› Phonological disorders associated with
math and written language weaknesses Common in autism Early intervention effective in treating
language disordershttp://www.asha.org/research/reports/children.htm
Who Can Be Included
Reasonable Classroom Fit
Consideration of: Cognitive functioning Receptive language Expressive language Self-regulation Social abilities Emotional maturity

Who can be included: Autism
Social motivation: highly aloof children may not do as well
Ability to follow basic social rules and direction
Functional speech Repetitive behaviors can be redirected
Ferraioli and Harris, 2010, Journal of Contemporary
Psychotherapy
Outcomes of Inclusion Models in Autism

Research Cautions…
Minimal research available Research is largely based on case
studies and a handful of group studies Many studies are of children “trained”
to produce a specific response› Unknown whether behavior will generalize
Not clear which children will benefit
General Observations
Inclusion better for younger than older kids (4th grade)› Older children Less tolerant of “differences”
Paradox: there is less peer acceptance of more socially competent ASD kids
Limited evidence of benefit for inclusion without additional support
With adequate support emerging research suggests inclusion models support social competence
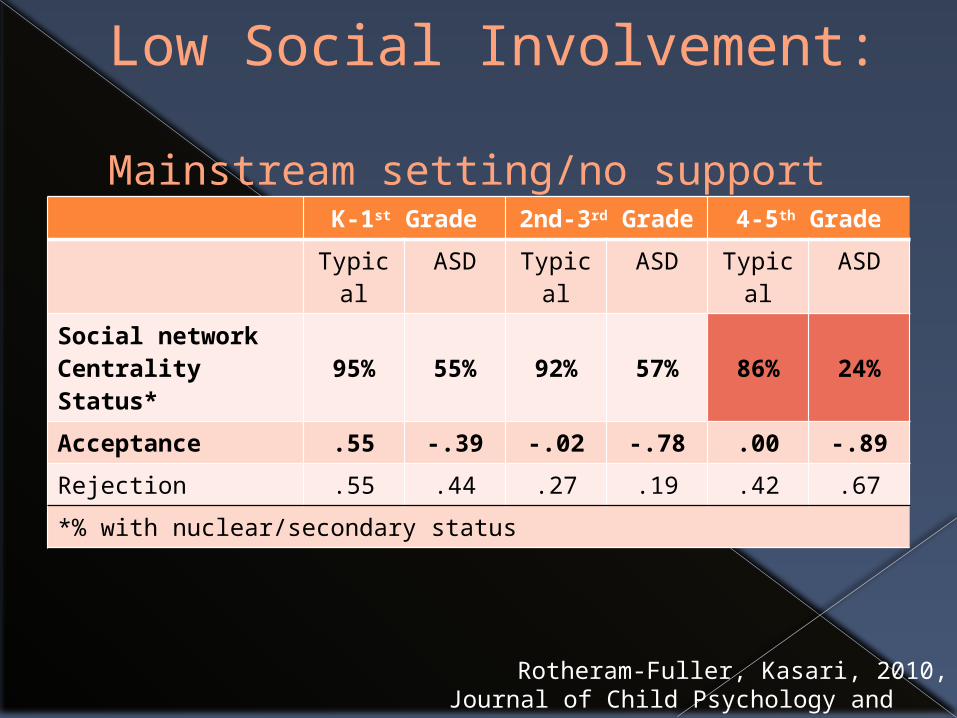
Low Social Involvement: Mainstream setting/no support
K-1st Grade 2nd-3rd Grade
4-5th Grade
Typical ASD Typical ASD Typical ASD
Social network Centrality Status*
95% 55% 92% 57% 86% 24%
Acceptance .55 -.39 -.02 -.78 .00 -.89
Rejection .55 .44 .27 .19 .42 .67
*% with nuclear/secondary status
Rotheram-Fuller, Kasari, 2010,Journal of Child Psychology and Psychiatry

Reasons for Low Social Involvement
Misperceptions of social involvement Typical peers become less tolerant of
differences and aberrant behavior Limited cooperative play skills Poor motor skills – social involvement
of boys is largely sports oriented
Rotheram-Fuller, Kasari, 2010,Journal of Child Psychology and Psychiatry
What predicts social rejection?
Low levels of cooperation Being regarded as shy More help-seeking
Jones & Frederickson, 2010, Journal of Autism and Developmental Disorders
Will Inclusion Adversely Affect Typical Children?
Concerns:› Takes away teacher time› Decreases classroom instruction› Typical children may feel uncomfortable
Research (limited):› When done appropriately, typical children
develop better social competence› No adverse impact on learning
Ongoing monitoring is important
Diary Study in ASD: General Observations
School is stressful and anxiety provoking
Social isolation & bullying are common High risk for deliberate teasing Anxiety worse in ASD than other
groups› Secondary to social deficits› Need for order, consistency, and routine
Humphrey and Lewis, 2008, Autism, 12, 23-46.

Diary Study in ASD:Take Home Points
Quiet classrooms, hand-pick teachers Time out/break from busy classrooms Try not to treat ASD kids differently,
especially as they get older› Provide ‘behind the scenes’ support closely
integrated with classroom teacher Leverage ‘special interests’ to motivate
Humphrey and Lewis, 2008, Autism, 12, 23-46.

Diary Study in ASD:Take Home Points
Peer relationships more important than teacher for inclusion success
Facilitate development of peer relationships› Stick up for kids with ASD› Support positive sense of self
Humphrey and Lewis, 2008, Autism, 12, 23-46.
Life in school, Student with ASDHumphrey & Lewis, 2008, Autism
Student with ASDHumphrey & Lewis, 2008, Autism
Diary Study in ASD:Teachers Need Support…
Training to:› Individualize instruction› Modify curriculum› Manage the social and self-regulation needs
Disorder specific education, support and problem-solving resources
Access to an ASD specialist
Humphrey and Lewis, 2008, Autism, 12, 23-46.
When Does Inclusion Work?
Explicit social instruction Education about differences Peer mediated intervention Teacher prompting, modeling, support
Peer Mediated Intervention
Case study of two kids with ASD Intervention:
› 4-5 minute training of whole classroom› Adult prompting throughout day› Explicit modeling, prompting, and
reinforcement Increased peer to peer interaction &
social skills
Banda, Hart, Liu-Gitz, 2010, Research in Autism Spectrum
Disorders
Facilitating Social Inclusion
Select tasks that require social interaction – e.g. frequent requests for more materials
Adult supported group activities

Learning Disability
“Sophia”
• A little slow to talk• Unclear articulation, mixing up syllables (“aminals”)
• Preschool: • Alphabet, nursery rhymes, memorized sequences
• Letter and color names• Counting and 1:1 correspondence
By Kindergarten› Not associating sounds with letters› Trouble with rhyming› Confusing similar-looking letters

End of first grade› Delay in reading and
writing skills
Tested and found to have a learning disability

Learning Disabilities
Definition – Controversies and Changes!
* 1960’s: “minimal brain dysfunction”
* 1970’s-2004: IQ-Achievement “discrepancy”
* 2000’s: Low achievement, assess Response to Intervention (RTI)






![Learning Visual Attention to Identify People With Autism ...openaccess.thecvf.com/content_ICCV_2017/papers/Jiang_Learning... · Convolution & ReLU Max Pooling ... ule (ADOS) [23]](https://static.fdocuments.us/doc/165x107/5abc1f977f8b9a76038d817e/learning-visual-attention-to-identify-people-with-autism-relu-max-pooling-.jpg)











