227Day diagnostic radiology (PDF) | Diagnostic radiology ...

Mr
EVa
b
1
a
ARRA
KBEMMSR
1
btgdie
p
svr
0h
European Journal of Radiology 83 (2014) 261– 267
Contents lists available at ScienceDirect
European Journal of Radiology
jo ur nal ho me page: www.elsev ier .com/ locate /e j rad
ultidetector computerized tomography enema versus magneticesonance enema in the diagnosis of rectosigmoid endometriosis
nnio Biscaldia,∗, Simone Ferrerob,1, Umberto Leone Roberti Maggioreb,2,alentino Remorgidab,3, Pier Luigi Venturinib,4, Gian Andrea Rollandia,5
Department of Radiology, Galliera Hospital, via Mura delle Capuccine 14, 16128 Genoa, ItalyDepartment of Obstetrics and Gynecology, San Martino Hospital and National Institute for Cancer Research, University of Genoa, Largo Rosanna Benzi, 1,6132 Genoa, Italy
r t i c l e i n f o
rticle history:eceived 27 May 2013eceived in revised form 6 October 2013ccepted 15 October 2013
eywords:owel endometriosisnemaagnetic resonance imagingultidetector computerized tomography
a b s t r a c t
Purpose: To compare the accuracy of multidetector computerized tomography enema (MDCT-e) andmagnetic resonance enema (MRI-e) in determining the presence of sigmoid and rectal endometrioticnodules.Materials and methods: 260 women (32.6 ± 4.3 years) with symptoms suggestive of rectosigmoid endo-metriosis underwent MDCT-e and MRI-e prior to laparoscopy. After retrograde colonic distention andinjection of intravenous contrast medium, patients were scanned on a 64-row MDCT scanner. MRI-e wasperformed on a 1.5 T magnet using an 8 channels phased array coil; intestinal distention was achieved byintroducing in the rectum 250–300 ml of ultrasonographic gel diluted with saline solution. Radiologicalfindings were compared with surgical and histological results.
igmoidectum
Results: 176 women had rectosigmoid endometriosis at surgery. There was no significant difference inthe accuracy of MDCT-e (98.5%) and MRI-e (96.9%) in the diagnosis of sigmoid and rectal endometriosis(p = 0.248). The sensitivity, specificity, positive predictive value, negative predictive value, positive like-lihood ratio and negative likelihood ratio of MDCT-e and MRI-e were respectively 98.3%, 98.8%, 99.4%,96.5%, 81.59, 0.02 and 97.2%, 96.4%, 98.3%, 94.1%, 26.89, 0.03.Conclusions: Both MDCT-e and MRI-e are accurate in the diagnosis of rectal and sigmoid endometriosis.
. Introduction
Over the last ten years several radiological techniques haveeen proposed for the diagnosis of bowel endometriosis includingransvaginal ultrasonography [1], rectal water contrast transva-inal ultrasonography [2], rectal endoscopic ultrasonography [3],ouble-contrast barium enema [4], and magnetic resonance (MR)
maging [3–5]; the latter is the preferred method to evaluate deep
ndometriosis.Multidetector computerized tomography enteroclysis wasreviously shown to be effective in the diagnosis of bowel
∗ Corresponding author. Tel.: +39 3334361121; fax: +39 010511525.E-mail addresses: [email protected] (E. Biscaldi),
[email protected] (S. Ferrero), [email protected] (U. Leone Roberti Maggiore),[email protected] (V. Remorgida), [email protected] (P.L. Venturini),[email protected] (G.A. Rollandi).
1 Tel.: +39 3485345973.2 Tel.: +39 3289461340.3 Tel.: +39 3356083031.4 Tel.: +39 3356229988.5 Tel.: +39 0105634806.
720-048X/$ – see front matter © 2013 Elsevier Ireland Ltd. All rights reserved.ttp://dx.doi.org/10.1016/j.ejrad.2013.10.010
© 2013 Elsevier Ireland Ltd. All rights reserved.
endometriosis [6–8]. A prospective study including 98 womendemonstrated that multidetector computerized tomography ente-roclysis has a sensitivity of 98.7%, a specificity of 100%, a positivepredictive value (PPV) of 100% and a negative predictive value(NPV) of 95.7% in identifying patients with bowel endometriosis[6]. Multidetector computerized tomography enteroclysis allows toaccurately estimate the presence of infiltration of endometriosis inthe muscularis propria of the whole colon [6,7]. In addition, multi-detector computerized tomography enteroclysis urography allowsthe radiologists to assess whether ureteral compression is presentwithout increasing the radiation dose imparted to the patients [8].When compared with other techniques, in particular transvaginalultrasonography or MR, multidetector computerized tomographyenteroclysis has some limitations including the administration ofa radiation dose to young women in the childbearing age and theuse of the iodinated contrast medium, which is required to wellrecognize endometriotic lesions during volumetric acquisition.
Intestinal distention during multidetector computerized
tomography enteroclysis highlights the endometriotic nodulesinfiltrating the bowel wall because it overcomes the limits of theempty loops that hamper the detection of wall lesions. In fact, dur-ing intestinal distention, bowel lesions are detectable, the tissue
2 rnal of Radiology 83 (2014) 261– 267
atlcbc
cns
2
2
twotbwrbtfp
myo(soav
edostordisso
wuaetfietw
iFhilt
Table 1Characteristic of symptoms of the study population (n = 260).
Symptoms (number of patients, %, mean intensity ± SD)
- Dysmenorrhea a 185 (88.5%)7.3 ± 1.4
- Deep dyspareunia b 157 (67.7%)6.4 ± 2.0
- Chronic pelvic pain 142 (54.6%)5.5 ± 1.4
- Dyschezia 130 (50.0%)5.2 ± 1.1
- Infertility 54 (20.8%)- Persistent constipation 85 (32.7%)
7.7 ± 1.1- Constipation during the menstrual cycle a 45 (21.5%)
8.0 ± 0.7- Persistent diarrhea 57 (21.9%)
7.8 ± 0.9- Diarrhea during the menstrual cycle a 69 (33.0%)
7.6 ± 1.2- Intestinal cramping 127 (48.8%)
7.0 ± 1.3- Abdominal bloating 122 (46.9%)
6.8 ± 1.5- Cyclical rectal bleeding 20 (7.7%)
4.5 ± 0.9- Mucus in the stools 44 (16.9%)
6.1 ± 1.8- Incomplete evacuation 40 (15.4%)
5.3 ± 0.8
a
62 E. Biscaldi et al. / European Jou
round the intestine is visible, the density difference betweenhe lumen (hypodense) and the parietal nodule (hyperdense solidesion) improves nodule detectability. In the current study, theoncept of retrograde intestinal distention was applied to MRecause deep endometriotic lesions may have signal intensity verylose to that of the surrounding fibromuscular structures [9].
This prospective study compared the accuracy of multidetectoromputerized tomography enema (MDCT-e) and magnetic reso-ance enema (MRI-e) in determining the presence of rectal andigmoid endometriotic nodules.
. Materials and methods
.1. Study population
Subjects of the study were recruited among patients referredo our endometriosis center. Inclusion criteria for the studyere: reproductive age, suspicion of deep pelvic endometriosis
n the basis of gynecological symptoms and vaginal examina-ion, presence of gastrointestinal symptoms that might be causedy rectosigmoid endometriosis. The following exclusion criteriaere used in the study: previous bilateral ovariectomy, previous
adiological exams of the bowel requiring contrast media, previousowel surgery (except appendectomy), previous episodes sugges-ive of intolerance to iodinated contrast media, renal or hepaticailure, presence of absolute contraindications to MR examination,sychiatric disorders.
Two hundred and sixty women were included in the study. Theean (±SD) age of the patients included in the study was 32.6 ± 4.3
ears. One hundred and thirteen patients (43.5%) underwent previ-us surgery for endometriosis. At the time of the study, 162 women62.3%) did not use any hormonal therapy, 53 women (20.4%) usedequential oral contraceptive, 12 women (4.6%) used continuousral contraceptive, 19 women (7.3%) used norethisterone acetatend 14 women (5.4%) were treated with sequential contraceptiveaginal ring.
Symptoms were systematically investigated (Table 1). The pres-nce of dysmenorrhea, deep dyspareunia, chronic pelvic pain, andyschezia was assessed; the intensity of these symptoms was ratedn a 10 cm visual analogue scale (VAS), the left extreme of thecale representing the absence of pain and the right extreme ofhe scale indicating the maximal intensity of pain. The presencef the following gastrointestinal symptoms was assessed: diar-hea (more than three bowel movements per day), constipationuring the menstrual cycle, abdominal bloating, intestinal cramp-
ng, feeling of incomplete evacuation after bowel movements. Aymptom analogue scale questionnaire was used to estimate theeverity of each gastrointestinal symptom (1 indicated the absencef the symptom; 10 indicated the highest severity of the symptom).
MDCT-e and MRI-e were performed within two days. MDCT-eas performed on the first day after the bowel preparation typicallysed for this technique. MRI-e was carried out on the following daysking the patients to have a prevalent liquid diet between the twoxams. All patients underwent laparoscopy within one month fromhe radiological investigations independently from the radiologicalndings. The surgeon was aware of presence/absence of intestinalndometriosis in the radiological examinations; this was requiredo manage the informed consent and to plan the surgical procedureith the general surgeon.
Bowel endometriosis was defined as endometriotic lesionsnfiltrating at least the muscularis propria of the intestinal wall.indings of MDCT-e and MRI-e were compared with surgical and
istological results. The presence of right colon endometrioticnvolvement, if present and detected at MDCT-e, was recorded. Theocal ethics committee approved the study. All patients acceptingo participate to the study signed a written consent form.
Determined for the 209 menstruating women who were not using continuoushormonal therapies.
b Determined for the 232 sexually active women included in the study.
2.2. Multidetector computerized tomography enema technique
Bowel preparation was obtained asking the patients to use alow-residue diet for three days before the exam. In addition, a lax-ative isosmolar nonabsorbable solution (Isocolan, Bracco, Milan,Italy) was administered orally (variable doses proportionally tothe patients’ weight) on the day before the exam. Retrogradecolonic distention was performed on the CT bed introducing about2000–2200 ml of water (37 ◦C). During the enema, pharmacologicalinhibition of peristaltic waves was obtained by intravenous injec-tion of hyoscine butylbromide (Buscopan; Boehringer Ingelheim,Florence, Italy). Patients were scanned on a 64 row MDCT scanner(LightSpeed VCT, GE Medical Systems, Waukesha, WI, USA). Thescan parameters were: 64 × 0.625 mm collimation, rotation time0.5 s, tube voltage 120 kV, effective mA 340. The patients werescanned in supine position, with a volumetric acquisition from thedome of the diaphragm to the pubic symphysis, performed in portalphase (40 s after the arterial peak) after the injection of the intra-venous contrast medium (iopamidol 370 mg I/ml; Iopamiro, Bracco,Milan, Italy). The injection of the contrast medium was performedaccordingly to the ‘double split’ bolus technique [8]: a pre-bolus ofiodinated contrast medium (20% of the total dose evaluated pro-portionally to the body weight) was injected simultaneously to thecolon distention; the remaining dose was injected and the CT scanperformed in the portal phase. The rate of the injection was setat 3.0 ml/s with an automatic power injector. Bolus-tracking soft-ware (Smart-Prep, GE Medical Systems, Waukesha, WI, USA) wasused to maximize the quality of MDCT images. The estimated radi-ation exposure during this scan protocol was evaluated by the CTDindex, automatically calculated by the scanner, and it was between12 and 14 mGy in all cases. Images were evaluated with multiplanarreconstructions, performed in all cases.
The MDCT-e criterion to diagnose bowel endometriosis was thepresence of solid nodules, contiguous or penetrating the thickenedcolonic wall. Infiltration of the muscularis propria was diagnosedwhen the fat plane between the nodule and the bowel disappears

E. Biscaldi et al. / European Journal of Radiology 83 (2014) 261– 267 263
F le wht al, it is
aim
2
GpAsTin3tfsii(sTTi(1weG
wprP(bnlwpg
st
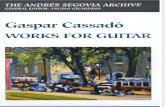
ig. 1. (a) MDCT-e, coronal reconstruction: the arrow shows an endometriotic noduhe mucosal layer. (b) T2W FrFSE fat sat sequence: the nodule has hysointense sign
nd the nodule penetrates the intestinal wall from outside, licks thenner surface and bulges toward the mucosa [6,7]. A pathological
ultilayered aspect of the wall may be detectable.
.3. Magnetic resonance enema technique
MRI-e was performed on a 1.5 T magnet (Signa Excite HDx,E Medical Systems, Waukesha, WI, USA) using an 8 channelshased array coil. In all cases, the pelvic volume was evaluated.ll studies followed an established examination protocol, con-isting of: T2W FrFSE axial images (FOV = 30–36 cm; TE = 150 ms;R = 5500 ms; matrix, 320 × 224; slice thickness = 3 mm; spac-ng = 1; acceleration factor = 1; 4 NEX); T2W FrFSE fat sat coro-al images (FOV = 31–33 cm; TE = 150 ms; TR = 4250 ms; matrix,84 × 254; slice thickness = 4 mm; spacing = 1; acceleration fac-or = 1; 4 NEX), T1W FSE coronal images (FOV = 31–33 cm; TE = minull; TR = 550 ms; matrix, 320 × 224; slice thickness = 4 mm;pacing = 1; acceleration factor = 1; 2 NEX), FIESTA sequencen coronal plane (FOV = 37 cm; slice thickness = 3 mm; spac-ng = 1; matrix, 256 × 256; 2 NEX), T2W FrSE sagittal imagesFOV = 31–33 cm; TE = 150 ms; TR = 4250 ms; matrix, 384 × 256;lice thickness = 3 mm; spacing = 1; acceleration factor = 1; 6 NEX),2W FrFSE fat sat sagittal images (FOV = 31–33 cm; TE = 120 ms;R = 4600 ms; matrix, 384 × 256; slice thickness = 4 mm; spac-ng = 1; acceleration factor = 1.5; 4 NEX), diffusion weighted EPIb = 800) axial images (FOV = 30–36 cm; TR = 3000 ms; matrix,28 × 128; slice thickness = 4 mm; spacing = 1; 8 NEX). T1 W imagesere acquired, employing fat-suppression even after contrast
nhancement (gadobutrol at a dosage of 0.2 mmol/kg body-weight;adovist 1.0, Schering, Berlin, Germany).
After the patient lied on the MR bed, the retrograde distentionas performed initially on the left lateral decubitus, then on therone position to reduce abdominal wall movements and respi-atory artifacts. 300–400 ml of ultrasonographic gel (Aquasonic,arker Laboratories, Fairfield, NJ, USA) diluted with saline solution1:8) were introduced to distend the rectum and the sigmoid colony using a syringe connected to a 20-Fr Foley catheter. Intesti-al hypotonization was not used in MR imaging because of the
imited quantity of intraluminal contrast medium (in comparisonith MDCT-e colonic distention). The examination position of theatient was preferably prone and the MR entry position in the
antry was feet first.Endometriotic nodules are detectable as solid mass outside theigmoid or rectal wall, frequently with a hypointense signal dueo their fibrous nature [9,10]. Visible penetration of the nodule
ich bulges toward the sigmoid (S) lumen, infiltrating (at the histologic verification) hysointense to the muscle in this sequence. S = sigmoid colon; U = uterus.
in the intestinal wall was the main parameter to hypothesize theinfiltration of the muscularis propria.
2.4. Tolerability of the radiological exams
Immediately after MDCT-e and MRI-e, patients were asked torate the pain encountered during each exam by using a 10 cm visualanalogue scale (VAS); the left extreme represented the absence ofpain, and the right extreme represented the worst possible pain.Mild pain was defined as VAS score <2, moderate pain as VAS score≥2 and ≤5, and severe pain as VAS score >5.
2.5. Evaluation of MDCT-e and MRI-e images
Two radiologists blindly reviewed the images at a PACS (PictureArchiving and Communication System) workstation. They were notaware of clinical findings and patients’ history, knowing only thatthe presence of bowel endometriosis was clinically suspected. Ifthere was a disagreement in the judgment of one exam, the twoobservers evaluated the exam in a joined session. In each exam,the following data were assessed: presence and location of rec-tosigmoid endometriotic nodules, size of the larger endometrioticnodule (Fig. 1).
2.6. Surgical technique
Before laparoscopy, the surgeons examined the reports and theimages of both MDCT-e and MRI-e. All the surgical procedureswere performed laparoscopically by a team of gynecological andcolorectal surgeons with extensive experience in the treatmentof pelvic and rectosigmoid endometriosis. After adequate adhe-siolysis, the sigmoid colon and the rectum were systematicallyexamined to verify the presence of endometriotic lesions. All vis-ible endometriotic lesions (except those on the diaphragm) wereexcised. Rectosigmoid endometriotic lesions infiltrating at least themuscularis propria were removed by segmental bowel resection.The specimens excised at surgery were histologically evaluated;the depth of infiltration of the endometriotic nodules in the bowelwall was determined [2,11].
2.7. Statistical analysis
Sensitivity, specificity, PPV and NPV were determined forboth MDCT-e and MRI-e. The diagnostic value of each test was

264 E. Biscaldi et al. / European Journal of Radiology 83 (2014) 261– 267
Fig. 2. A 38-year-old-woman with intestinal symptoms mimicking constipation predominant irritable bowel syndrome. The bowel preparation was incomplete. (a) MR-e,T e plann , in T1l
atceanmmwpceaaCc
3
3
6e9ate
TD
M
2W FrFSE sequence in a parasagittal plane; (b) MR-e, T1W FSE sequence in the samodule which infiltrates the rectal wall. In T2W sequence the nodule is hypo-intense
eaving stools in the rectum. B = bladder; R = rectum.
lso evaluated using positive likelihood ratio (LR+) and nega-ive likelihood ratio (LR−). The McNemar’s test with the Yatesontinuity correction was used to compare the accuracy of MDCT-
and MRI-e in the diagnosis of intestinal endometriosis. Theccuracy of the measurement of nodule size by imaging tech-iques was estimated by subtracting the size of the nodule aseasured by the techniques from the size of the nodule aseasured at histology. The nonparametric Mann–Whitney testas used to compare the intensity of pain experienced by theatients during MDCT-e and MRI-e. The �2 test was used toompare the type of pain (mild, moderate and severe) experi-nced by the patients undergoing the two exams. Data wererchived using Excel 2007 (Microsoft, Redmond, WA, USA) andnalyzed using Sigma Stat software version 3.5 (SPSS Science,hicago, IL, USA). P < 0.05 was considered statistically signifi-ant.
. Results
.1. Study population
Surgery demonstrated that 176 women (67.7%; 95% C.I.,1.6–73.3%) had rectosigmoid endometriotic nodules. Thendometriotic nodules were located on the sigmoid colon in
6 cases (54.5%), on the rectosigmoid junction in 28 cases (15.9%)nd on the rectum in 52 cases (29.6%). The mean (±SD) length ofhe resected bowel segment was 11.8 cm (±2.5 cm). Histologicalxamination of the specimens excised at surgery confirmed theable 2ifference between size of the largest nodule estimated by imaging techniques and that m
Histology MDCT-e
Largest diameter(mm,mean ± SD)
Mean difference (mm,95% CI)a
All nodules 28.2 ± 6.4 1.167 (0.843–1.491)
Nodules with diameter<30 mm
23.2 ± 3.1 0.374 (−0.044 to 0.792)
Nodules with diameter≥30 mm
34.8 ± 2.5 2.213 (1.803–2.623)
DCT-e, multidetector computerized tomography enteroclysis; MR-e, magnetic resonana Mean difference calculated by subtracting size of nodule measured by imaging technb Limits of agreement calculated as mean difference ± 2 SDs of the difference.
e; (c) MR-e, T1W FSE post-Gd sequence. In these two images the arrows indicate theW post-Gd, the enhancement is very poor. The bowel preparation was inadequate,
diagnosis of endometriosis in all the excised nodules; in addition,it demonstrated that the deeper endometriotic nodule infiltratedthe intestinal muscularis propria in 116 patients (65.9%), thesubmucosa in 40 women (22.7%) and the mucosa in 20 patients(11.4%).
3.2. Accuracy of MDCT-e and MRI-e in diagnosing rectosigmoidendometriotic nodules
Out of 176 patients with histological diagnosis of rectosig-moid endometriosis, MDCT-e yielded a diagnosis of rectosigmoidendometriosis in 175 patients, while MRI-e yielded a diagnosisof rectosigmoid endometriosis in 174 patients. In MDCT-e, a rec-tosigmoid nodule of endometriosis was not detected in one case: anodule reaching the muscularis propria of the rectosigmoid junc-tion (Fig. 2). MRI-e did not identify two rectosigmoid endometrioticnodules: one nodule was the same unidentified by MDCT-e infil-trating the muscularis propria of the rectosigmoid junction andthe other was deeply infiltrating the muscularis propria of the sig-moid. The accuracy, sensitivity, specificity, PPV, NPV, LR+ and LR− ofMDCT-e and MRI-e in the diagnosis of recto-sigmoid endometriosiswere 98.5%, 98.3%, 98.8%, 99.4%, 96.5%, 81.59, 0.02 and 96.9%, 97.2%,96.4%, 98.3%, 94.1%, 26.89, 0.03, respectively. The two techniqueshad similar accuracy in the diagnosis of recto-sigmoid endometri-
osis (p = 0.248) (Figs. 3–5). MDCT-e showed that three patients hadisolated intestinal nodules on the cecum that infiltrated the mus-cularis; these nodules could not be identified by MRI-e and theywere not considered in the statistical analysis.easured on histopathology.
MDCT-e MR-e MR-eLimits ofagreement (mm)b
Mean difference (mm, 95%CI)a
Limits ofagreement (mm)b
−3.161 to 5.495 0.994 (0.628–1.360) −3.894 to 5.882−3.822 to 4.570 −0.131 (−0.534 to 0.272) −4.169 to 3.907
−1.347 to 5.773 2.480 (1.985–2.975) −1.824 to 6.784
ce imaging enteroclysis.ique from size of nodule measured on histology.

E. Biscaldi et al. / European Journal of Radiology 83 (2014) 261– 267 265
Fig. 3. 31-year-old-woman with dysmenorrhea, chronic pelvic pain, persistent constipation and. painful bowel movements suggestive of bowel endometriosis. (a) MDCT-es triotici R-e im
et
2
3
ttenitTs(
Fa
agittal reconstruction. (b) MR-e FrFSE sequence T2W in sagittal image. The endomemages (arrow). The colon distension in MDCT-e overcomes the sigmoid colon; in M
uscular layer of the rectum; this was confirmed at surgery.
Both MDCT-e and MRI-e underestimated the size of thendometriotic nodules; in both imaging techniques the underes-imation was greater for nodules with diameter ≥30 mm (Table 2).
The mean (±SD) overall scanner room occupation time was7.3 ± 4.1 min for MDCT-e and 45.0 ± 3.6 min for MRI-e (p < 0.001).
.3. Tolerability and adverse effects of MDCT-e and MRI-e
During MDCT-e, no patient had intolerance to iodinated con-rast medium or adverse reactions to it. The colonic distention wasolerated in all the cases and no patient required interrupting thexam. The MRI-e was safely performed in all the patients; there waso adverse reaction to paramagnetic contrast medium. During the
njection of the ultrasonography jelly in the recto-sigmoid, none of
he patients showed signs of severe discomfort or allergic reactions.he mean (±SD) intensity of pain experienced by the patients wasignificantly lower during MRI-e (2.5 ± 0.7) than during MDCT-e5.8 ± 1.2; p < 0.001). Severe pain was experienced by 156 womenig. 4. 29-year-old-woman suffering dysmenorrhea, chronic pelvic pain, diarrhea during txial reconstruction. (b) MR-e T2W axial image. The intestinal nodule infiltrating the mus
nodule, which infiltrates the anterior wall of the rectum, is well detectable in botht is limited to the rectum. In both images the endometriotic nodules infiltrates the
(60.0%) undergoing MDCT-e and by 26 women (10.0%) undergo-ing MRI-e, moderate pain was experienced by 100 women (38.4%)undergoing MDCT-e and by 139 women (53.4%) undergoing MRI-e, mild pain was experienced by four women (1.5%) undergoingMDCT-e and by 95 women (36.5%) undergoing MRI-e (p < 0.001).
4. Discussion
To the best of our knowledge, this is the first prospectivestudy comparing the effectiveness of MDCT-e and MRI-e in thediagnosis of recto-sigmoid endometriosis. This study demon-strates that both techniques have similar accuracy in diagnosingrecto-sigmoid endometriosis. The non-invasive diagnosis of
endometriotic nodules infiltrating the intestinal muscularis pro-pria is relevant to identify patients requiring treatment. Intestinalnodules can be excised by segmental resection or nodulec-tomy accordingly to the preference of the surgeon and to thehe menstrual cycle, abdominal bloating and painful bowel movements. (a) MDCT-ecularis propria is shown by the white arrow.

266 E. Biscaldi et al. / European Journal of Radiology 83 (2014) 261– 267
Fig. 5. 36-year-old-woman under oral contraceptive pill which suffered severe dysmenorrhea, deep dyspareunia and persistent constipation. (a) MDCT-e sagittal recon-struction. (b) MR-e FrFSE sequence T2W in sagittal image. (c) Magnification of the MR-e image showed in Fig. 4b. The extended infiltration of the sigmoid (S) colon reducest ltratim ion ofi terisk
cit5ca
msN[duMe
aticigdptsttioowwfiFrIaiifep
he intestinal lumen and obstacles the evaluation of the depth of endometriotic infiucosa but histological examination of the excised specimen showed only infiltrat
t emphasizes the infiltration of the muscularis propria, showing the submucosa (as
haracteristics of the lesions (size and depth of infiltration in thentestinal wall) [11]. Alternatively, medical therapies (norethis-erone acetate, gonadotropin releasing hormone analogues and-HT4 receptor agonists) may be used to treat intestinal symptomsaused by rectosigmoid endometriotic nodules that do not cause
stenosis of the bowel lumen [12,13].Several authors proposed MR for the diagnosis of bowel endo-
etriosis. In fact, MR has sensitivity between 77% and 95%,pecificity between 89% and 100%, PPV between 94% and 100% andPV between 77% and 99% for the diagnosis of bowel endometriosis
9,14,3,15,16]. This is not the first study combining MR with jellyistention to facilitate the diagnosis of endometriosis. Injection ofltrasonographic jelly in the vagina and the rectum combined withR has previously been described for the diagnosis of rectovaginal
ndometriosis and obliteration of the cul-de-sac [17].MDCT-e with the retrograde enema of the entire colon provides
complete overview of the whole colon. A potential weakness ofhe current study consists in the fact that MRI-e does not exam-ne the whole colon but only the rectosigmoid wall. Therefore, theurrent study examined the accuracy of MDCT-e and MRI-e onlyn the detection of recto-sigmoid nodules. The use of water retro-rade distention (as in MDCT-e) may allow full colonic distentionuring MR. It has previously been shown that MR targeted to theelvis may be combined with contrast-enhanced MR-colonographyo evaluate the whole colon [18]. However, the whole colon MRI-etudy requires more time than MDCT-e, a complete colonic dis-ention is sometimes difficult to be tolerated for the time requiredo complete all MRI-e sequences, and, last but not least, a min-mal intestinal cleansing is required. In our experience, the usef diluted gel decreases the quantity of the injected fluid becausef its high density. Furthermore, the ultrasonographic gel dilutedith saline solution remains in the rectum during the examination,hile saline solution may leave the rectum and the sigmoid colon,
ollowing the gravity toward the transverse colon; in addition,n the mixed solution, the absorption of the water is minimized.urthermore, the low incidence of right colon endometriosis [19]educes the need of routinely evaluate the entire large bowel.ntestinal hypotonization is routinely performed during MDCT-end contrast-enhanced MR-colonography but it is not required dur-ng MRI-e, in fact, in all performed MR studies, no artifact reduced
mages quality. During the distension of the whole colon requiredor MDCT-e, the hypotonization increased the tolerability of thexam and it may also reduce the risk of artifacts caused by intenseeristalsis [6,7].on in the bowel wall at MDCT-e. The infiltration was judged to reach the intestinal the muscularis propria. At MR-e, the layered aspect of the sigmoid wall is evident:s) and mucosa (arrows). S = sigmoid colon; U = uterus; R = rectum.
A potential limitation of the current study consists in the factthat a distension of the whole colon was performed during MDCT-e while only the rectosigmoid was distended during the MRI-e.Methodologically, during MDTC, we could have performed anenema only of the rectum and sigmoid; this could have made moresimilar the two radiological techniques. However, a distension ofthe whole colon was performed during the MDTC because this wasthe technique previously described [6–8] and it allows to providemore clinical information.
Another limitation of the study is that the two techniques werenot used to diagnose pelvic endometriosis but only rectal andsigmoid nodules. However, this comparison could have not beenfeasible, in fact, while it is well known that MR is the gold standardfor the evaluation of all pelvic endometriotic lesions [20], CT isnot used to diagnose pelvic endometriosis. However, in clinicalpractice the most important preoperative diagnosis is to identifythe involvement of the bowel. In fact, intestinal surgery requiresan extensive preoperative consent and the gynecologist, who usu-ally operates patients with endometriosis, need the assistance ofthe colorectal surgeon to perform this type of procedures. Anotherstrength of MR consists in the fact that radiations are not requiredand this is particularly relevant in a population of women of repro-ductive age.
A strength of the current study is that it included a large sam-ple of patients with suspicion of rectosigmoid endometriosis andover 60% of the patients had intestinal nodules. It was possibleto recruit this population of patients because the study was per-formed in a referral center for the diagnosis and treatment ofendometriosis.
Obviously the experience of the radiologist in CT and MRcolon study may influence the accuracy of these techniques indiagnosing bowel endometriosis. In the current study, the exten-sive experience and technical familiarity of the authors with CTenema performance may have improved the accuracy of diagnosis,which may be more challenging for other radiologists. In con-trast, the MR pattern of endometriosis, the availability of differentsequences, the complementary pattern in T1W and T2W sequencesmay facilitate all radiologists in diagnosing of bowel endometri-osis.
5. Conclusions
In conclusion, this prospective study demonstrates that bothMDCT-e and MRI-e are accurate in the diagnosis of rectosigmoid

rnal of
erweidiiiemc
R
[
[
[
[
[
[
[
[
[
[19] Remorgida V, Ferrero S, Fulcheri E, Ragni N, Martin DC. Bowel endo-
E. Biscaldi et al. / European Jou
ndometriosis. MDCT-e has the disadvantage of the use of ionizingadiation and iodinated contrast medium in a population ofomen of reproductive age. The request of the clinician to ideally
valuate the whole colon should be balanced with the fact that thencidence of intestinal endometriosis in the right, transverse andescending colon is low. MRI-e is more tolerable than MDCT-e; it
s a study focused on the pelvis and on the sigmoid and rectum,s has satisfying sensitivity and specificity in identifying nodulesn the distal colon. Future studies should aim to improve thevaluation of the patients to better understand when MDCT-eay be advisable in order to perform a whole evaluation of the
olon.
eferences
[1] Hudelist G, English J, Thomas AE, Tinelli A, Singer CF, Keckstein J. Diagnosticaccuracy of transvaginal ultrasound for non-invasive diagnosis of bowel endo-metriosis: systematic review and meta-analysis. Ultrasound Obstet Gynecol2011;37(3):257–63.
[2] Valenzano Menada M, Remorgida V, Abbamonte LH, Nicoletti A, Ragni N, Fer-rero S. Does transvaginal ultrasonography combined with water-contrast inthe rectum aid in the diagnosis of rectovaginal endometriosis infiltrating thebowel? Hum Reprod 2008;23(5):1069–75.
[3] Bazot M, Lafont C, Rouzier R, Roseau G, Thomassin-Naggara I, Daraï E. Diagnosticaccuracy of physical examination, transvaginal sonography, rectal endoscopicsonography, and magnetic resonance imaging to diagnose deep infiltratingendometriosis. Fertil Steril 2009;92(6):1825–33.
[4] Faccioli N, Foti G, Manfredi R, et al. Evaluation of colonic involvement in endo-metriosis: double-contrast barium enema vs. magnetic resonance imaging.Abdom Imaging 2010;35(4):414–21.
[5] Busard MP, van der Houwen LE, Bleeker MC, et al. Deep infiltrating endome-triosis of the bowel: MR imaging as a method to predict muscular invasion.Abdom Imaging 2012;37(4):549–57.
[6] Biscaldi E, Ferrero S, Fulcheri E, Ragni N, Remorgida V, Rollandi GA. Mul-tislice CT enteroclysis in the diagnosis of bowel endometriosis. Eur Radiol2007;17(1):211–9.
[7] Biscaldi E, Ferrero S, Remorgida V, Rollandi GA. Bowel endometriosis: CT-enteroclysis. Abdom Imaging 2007;32(4):441–50.
[
Radiology 83 (2014) 261– 267 267
[8] Biscaldi E, Ferrero S, Remorgida V, Rollandi GA. MDCT enteroclysis urogra-phy with split-bolus technique provides information on ureteral involvementin patients with suspected bowel endometriosis. AJR Am J Roentgenol2011;196(5):W635–40.
[9] Bazot M, Darai E, Hourani R, et al. Deep pelvic endometriosis: MRimaging for diagnosis and prediction of extension of disease. Radiology2004;232(2):379–89.
10] Chassang M, Novellas S, Bloch-Marcotte C, et al. Utility of vaginal and rectalcontrast medium in MRI for the detection of deep pelvic endometriosis. EurRadiol 2010;20(4):1003–10.
11] Remorgida V, Ragni N, Ferrero S, Anserini P, Torelli P, Fulcheri E. The involve-ment of the interstitial Cajal cells and the enteric nervous system in bowelendometriosis. Hum Reprod 2005;20(1):264–71.
12] Ferrero S, Camerini G, Ragni N, Venturini PL, Biscaldi E, Remorgida V. Norethis-terone acetate in the treatment of colorectal endometriosis: a pilot study. HumReprod 2010;25(1):94–100.
13] Ferrero S, Camerini G, Ragni N, Valenzano Menada M, Venturini PL, RemorgidaV. Triptorelin improves intestinal symptoms among patients with colorectalendometriosis. Int J Gynaecol Obstet 2010;108(3):250–1.
14] Abrao MS, Gonc alves MO, Dias Jr JA, Podgaec S, Chamie LP, Blasbalg R. Com-parison between clinical examination, transvaginal sonography and magneticresonance imaging for the diagnosis of deep endometriosis. Hum Reprod2007;22(12):3092–7.
15] Chapron C, Vieira M, Chopin N, et al. Accuracy of rectal endoscopic ultrasono-graphy and magnetic resonance imaging in the diagnosis of rectal involvementfor patients presenting with deeply infiltrating endometriosis. UltrasoundObstet Gynecol 2004;24(2):175–9.
16] Bazot M, Malzy P, Cortez A, Roseau G, Amouyal P, Daraï E. Accuracy ofmagnetic resonance imaging and rectal endoscopic sonography for the pre-diction of location of deep pelvic endometriosis. Hum Reprod 2007;22(5):1457–63.
17] Kikuchi I, Takeuchi H, Kuwatsuru R, et al. Diagnosis of complete cul-de-sac obliteration (CCDSO) by the MRI jelly method. J Magn Reson Imaging2009;29(2):365–70.
18] Scardapane A, Bettocchi S, Lorusso F, et al. Diagnosis of colorectal endo-metriosis: contribution of contrast enhanced MR-colonography. Eur Radiol2011;21(7):1553–63.
metriosis: presentation, diagnosis, and treatment. Obstet Gynecol Surv2007;62(7):461–70.
20] Coutinho Jr A, Bittencourt LK, Pires CE, et al. MR imaging in deep pelvic endo-metriosis: a pictorial essay. Radiographics 2011;31(2):549–67.