EUROLOGIC EMERGENCIES - Henry Ford Health System · BOTULISM (FOOD-BORNE) Clinical Features...
44
NEUROLOGIC EMERGENCIES Nick Busch Henry Ford EM Grand Rounds August 14 th , 2014
Transcript of EUROLOGIC EMERGENCIES - Henry Ford Health System · BOTULISM (FOOD-BORNE) Clinical Features...
NEUROLOGIC EMERGENCIES
Nick Busch
Henry Ford EM Grand Rounds
August 14th, 2014
GOALS
Basic pathophysiology of each disease
Clinical Features (for ER diagnosis)
Board Exam Points
Practical ER Management

OUTLINE
Review of nerve and neuromuscular junction
Transverse Myelitis
Guillain-Barré Syndrome
Botulism
Myasthenia Gravis
Conclusion

TM
GBS
MG
Botulism

MYELIN SHEATH


CASE: PROGRESSIVE WEAKNESS
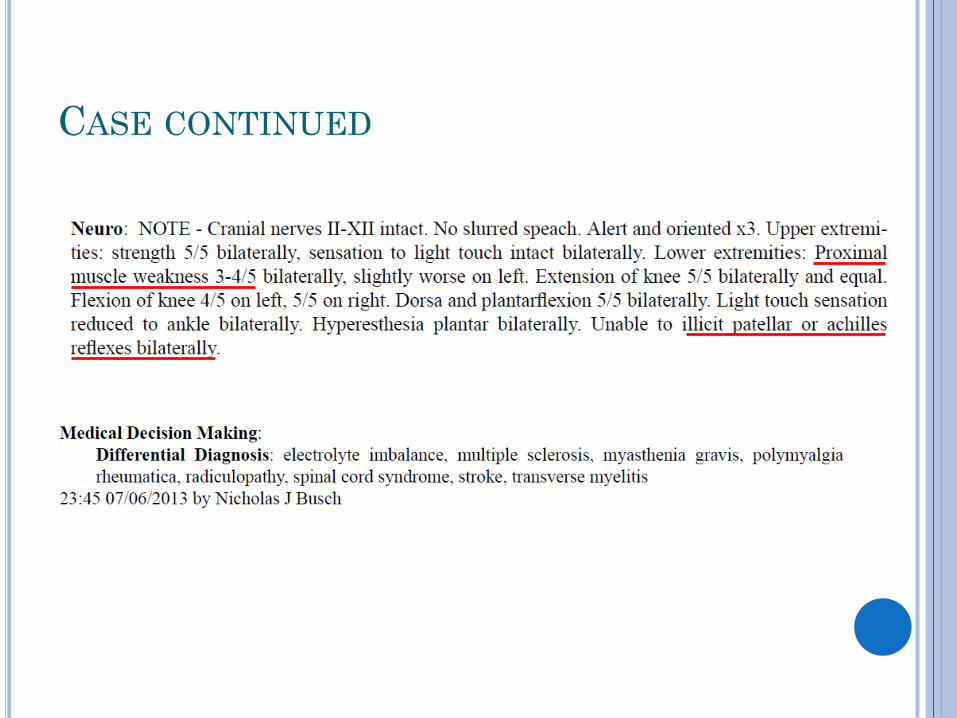
CASE CONTINUED

MYELITIS
“Acute transverse myelitis”
Pathogenesis: infectious, autoimmune, idiopathic
30% post viral infection
Clinical features
Paraplegia, sensory impairment, sphincter
disturbance
Fever, back pain, paresis, hypertonia, hyperreflexia,
clonus, +Babinski

MYELITIS
Diagnosis: CSF not useful, r/o other disease
Differential: MS, spinal epidural abscess, spinal
neoplasm, or hematoma
Management
Steroids (?)
MRI to exclude compressive lesions
Neuro consult and hospitalization
Common Theme

MYELITIS
Clinical Course:
24 hours: two thirds reach maximal deficit
3-6 months: maximal improvement
5 years:
55% good or fair recovery
30 % poor outcome
15 % dead

GUILLAIN-BARRÉ SYNDROME
„ghee-yan bah-ray‟

GUILLAIN-BARRÉ SYNDROME
Autoimmune, demyelinating
Clinical features
Progressive, symmetrical distal weakness
“ASCENDING WEEKNESS”
Usually lower extremities, 32% all, 10% upper
Decrease in deep tendon reflexes
Sphincter and ocular muscles spared (usually)
Half have autonomic dysfunction

GUILLAIN-BARRÉ SYNDROME
Diagnosis:
CSF: high protein, slight pleocytosis
MRI
Differential: MS, spinal epidural abscess, spinal
neoplasm, or hematoma

GUILLAIN-BARRÉ SYNDROME
Subtypes
Acute inflammatory demyelinating polyneuropathy
(90%) - AIDP
Acute motor axonal neuropathy - AMAN
Acute motor and sensory neuropathy - AMSAN

GUILLAIN-BARRÉ SYNDROME
Causes
AIDP – myelin invasion of the myelin sheath
Common organisms
Campylobacter jejuni ***
CMV, EBV and mycoplasma

GUILLAIN-BARRÉ SYNDROME
Management
Respiratory Function
IVIG
Plasma exchange
Neuro consult ICU
Do not treat high blood pressure
Usually transient, followed by unpredictable hypotension
No Difference in outcomes

GUILLAIN-BARRÉ SYNDROME
Respiratory Function

GUILLAIN-BARRÉ SYNDROME
Clinical Course:
Highly variable
Predominately sensory = better outcome
½ peak in 1 week, ½ long term sequelae
1/3 need vent support
3% mortality
3% recurrence
CASE CONCLUSION
• Follow up– Rehab
– 5 months walker, foley out
– 1 year: at home, no walker, continued paresthesias
BOTULISM
“Toxin mediated illness causing acute weakness”
Toxin targets peripheral NMJ and autonomic
synapses
Clostridium Botulinum
Strictly anaerobic, gram positive, rod-shaped
BOTULISM
Justinus Kerner (1786-1862)
Latin word for sausage = "botulus"
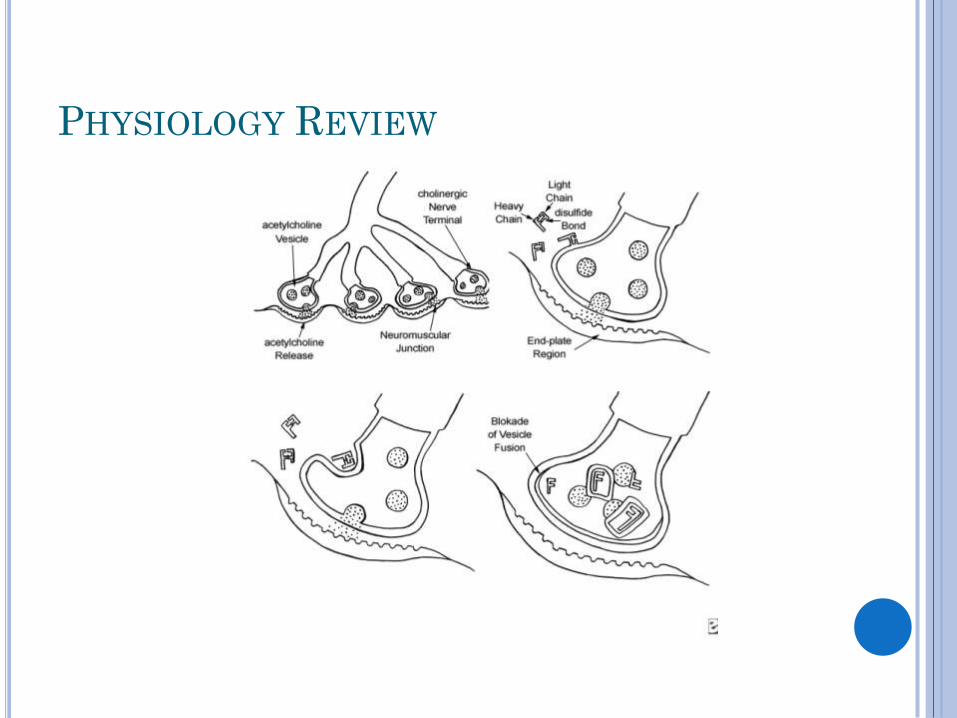
PHYSIOLOGY REVIEW

BOTULISM
7 toxin types (A,B,E and F cause disease in
humans)
110 cases confirmed per year by CDC

BOTULISM
Food-Borne
Infant
Wound
Unclassified (adult infectious)
Inadvertent (Botox)
Bioterrorism
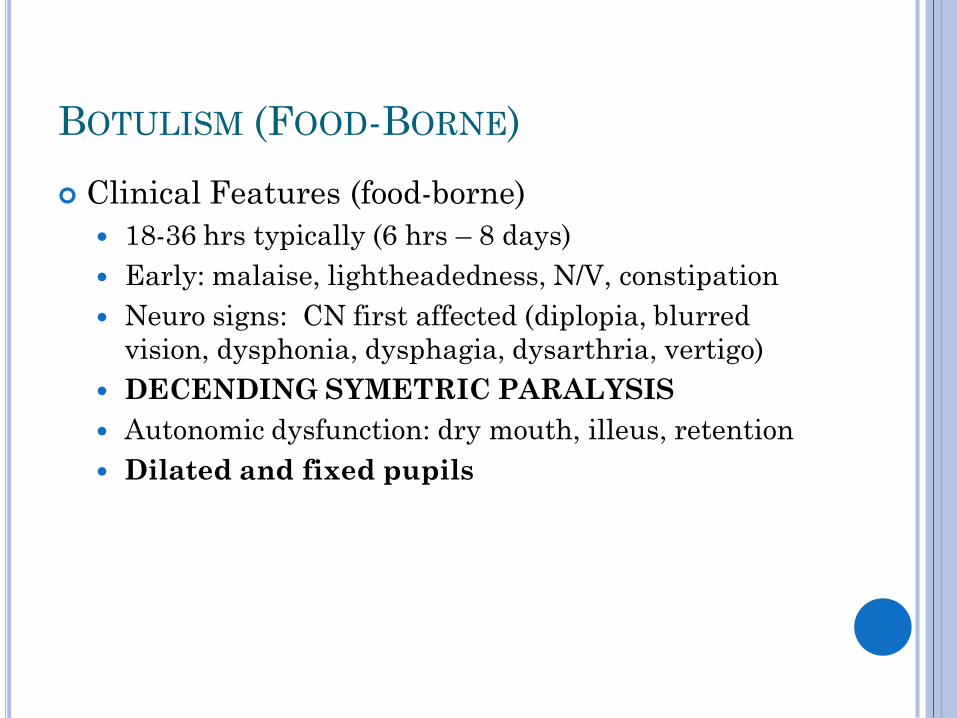
BOTULISM (FOOD-BORNE)
Clinical Features (food-borne)
18-36 hrs typically (6 hrs – 8 days)
Early: malaise, lightheadedness, N/V, constipation
Neuro signs: CN first affected (diplopia, blurred
vision, dysphonia, dysphagia, dysarthria, vertigo)
DECENDING SYMETRIC PARALYSIS
Autonomic dysfunction: dry mouth, illeus, retention
Dilated and fixed pupils
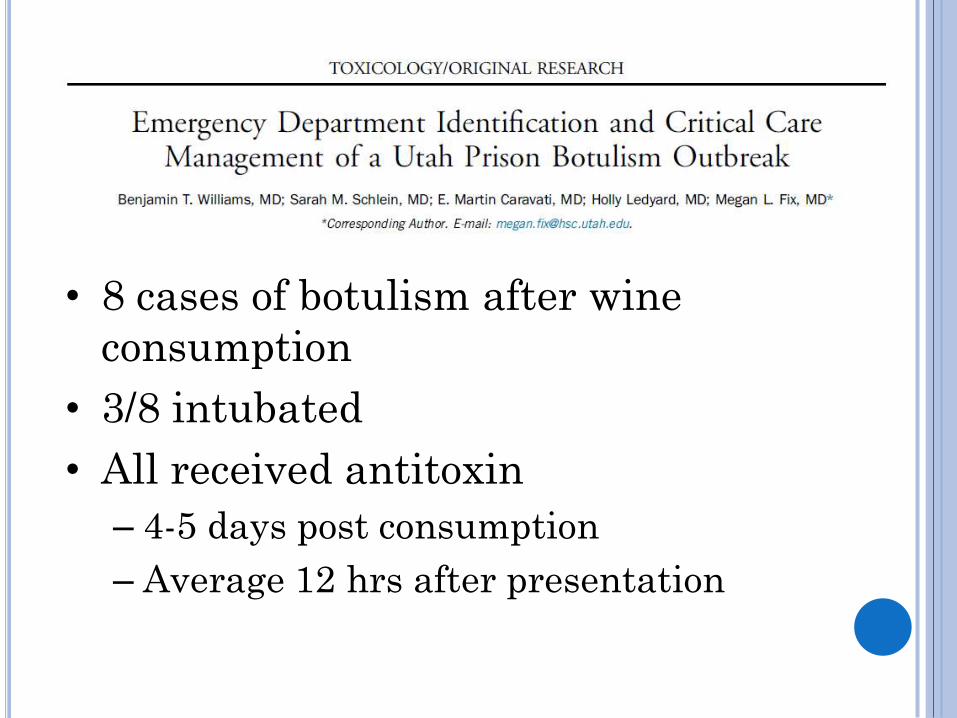
• 8 cases of botulism after wine
consumption
• 3/8 intubated
• All received antitoxin
– 4-5 days post consumption
– Average 12 hrs after presentation


BOTULISM MANAGEMENT
Respiratory Management
Vital capacity <12 mL/kg criteria for intubation
NG tube
Foley
Anti-toxin

BOTULISM ANTI-TOXIN
Anti-toxin
Equine trivalent: antibodies to A, B, and E
Circulating toxin only (will not unbind)
Prevents progression, decrease hospital stay,
decreased respiratory failure
CDC or state health department
One 10 mL vial (no repeated doses)
INFANT BOTULISM
Ingestion of spores
Classic: Honey <1 yr
Hypotonia, poor feeding, constipation
Longer incubation period
Large Differential: Sepsis, IEM, ect.
• BabyBIG: human immunoglobulin
Adult anti-toxin = high risk anaphylaxis

MYASTHENIA GRAVIS
Βαρύςgravis severe
Μῦς mys muscle
ἀσθένεια astheneiaweakness

MYASTHENIA GRAVIS
Auto-antibodies against nicotinic acetylcholine
receptor at NMJ
Complement mediated destruction
Compete with Ach for receptors

MYASTHENIA GRAVIS
Epidemiology
Bimodal
Clinical Features
Ocular symptoms: ptosis, diplopia, blurred vision
Respiratory failure (rarely first symptom, 17% will
have in first 2 years)
Fatigability (worse at end of the day)

MYASTHENIA GRAVIS
Diagnosis
Edrophonium Test
Ice bag Test
MYASTHENIA GRAVIS
Myasthenic Crisis
Respiratory failure leading to mechanical ventilation
Causes: infection, aspiration, med changes, surgery,
pregnancy
Monitor, NIPPV, mechanical ventilation

DRUGS EXACERBATING MG
Betablockers
Ca-Channel Blockers
Quinidine
Lidocaine
Procainamide
Aminoglycosides
Tetracyclines
Clindamycin
Polymyxin B
Phenytoin
Neuromuscular Blockers
Corticosteroids
Thyroxine

MYASTHENIA GRAVIS
Treatment
Cholinesterase Inhibitors
Immunosuppressants
Thymectomy
Immunoglobulin Therapy
Plasmapheresis

THE PLASTIC CIGAR
Vital Capacity
Negative Inspiratory Force

PULMONARY FUNCTION TESTING

CONCLUSION
Transverse Myelitis
Guillain-Barré Syndrome
Botulism
Myasthenia Gravis
REFERENCES
Available Upon Request