EUnetHTA WP7: Deliverable 7.2 - Final Report
76
EUnetHTA WP7 Deliverable 7.2 – Final report 1 EUnetHTA WP7: Deliverable 7.2 - Final Report Disclaimer: EUnetHTA is supported by a grant from the European Commission. The sole responsibility for the content of this document lies with the authors and neither the European Commission nor EUnetHTA are responsible for any use that may be made of the information contained therein.
Transcript of EUnetHTA WP7: Deliverable 7.2 - Final Report
EUnetHTA WP7 Deliverable 7.2 – Final report
1
EUnetHTA WP7: Deliverable 7.2 - Final Report
Disclaimer: EUnetHTA is supported by a grant from the European Commission. The sole responsibility for the content of this document lies with the authors and neither the European Commission nor EUnetHTA are responsible for any use that may be made of the information contained therein.
EUnetHTA WP7 Deliverable 7.2 – Final report
2
Contents
Abbreviations ........................................................................................................... 4 1. Executive Summary .......................................................................................... 5 4. Introduction and Objectives ........................................................................... 11
Introduction ........................................................................................................... 11 Objectives ............................................................................................................. 11
5. Methods ........................................................................................................... 12 Data collection ...................................................................................................... 12 Methods of Analysis .............................................................................................. 13
6. Report structure .............................................................................................. 14 7. Results: Overview of the JA3 use of JA/CA.................................................. 16
Response Rate ..................................................................................................... 16 Topic relevance .................................................................................................... 16
Use of JA/CA ........................................................................................................ 18 Countries reporting use of JA/CA ......................................................................... 20 Type of use of JA/CA ............................................................................................ 20 Benefits of use ...................................................................................................... 22
Non-use of JA/CA ................................................................................................. 23 Summary of limiting and preventing factors .......................................................... 25
8. Results: Comparison of use in JA2 and JA3 ................................................ 28
Pharmaceutical Assessments ............................................................................... 28 Other Technology Assessments ........................................................................... 29
Conclusions .......................................................................................................... 32 9. Relationship between participation and implementation ............................ 34
Other technologies ................................................................................................ 34
Pharmaceuticals ................................................................................................... 36 Conclusions .......................................................................................................... 38
10. Results: Awareness .................................................................................... 39 Fitness for purpose of procedures ........................................................................ 39
Agency perceptions of changes introduced in JA3 ............................................... 39 Agency recommendations for the future ............................................................... 40
Conclusions .......................................................................................................... 41 11. Results: Timing ............................................................................................ 43
Fitness for purpose of procedures ........................................................................ 43
Agency perceptions of changes introduced in JA3 ............................................... 44 Agency recommendations for the future ............................................................... 45
Conclusions .......................................................................................................... 45 12. Results: Relevance and transferability ...................................................... 46
Fitness for purpose of procedures ........................................................................ 46
Agency perceptions of changes introduced in JA3 ............................................... 47 Agency recommendations for the future ............................................................... 48
Conclusions .......................................................................................................... 49 13. Results: Reliability and scientific rigour ................................................... 50
Fitness for purpose of procedures ........................................................................ 50 Agency perceptions of changes introduced in JA3 ............................................... 51 Agency recommendations for the future ............................................................... 52 Conclusions .......................................................................................................... 52
14. Results: Evidence and Methodology ......................................................... 53 Fitness for purpose of procedures ........................................................................ 53
EUnetHTA WP7 Deliverable 7.2 – Final report
3
Agency perceptions of changes introduced in JA3 ............................................... 54
Agency recommendations for the future ............................................................... 55 Conclusions .......................................................................................................... 56
15. Results: Usability and Reporting Structure .............................................. 57 Fitness for purpose of procedures ........................................................................ 57 Agency perceptions of changes introduced in JA3 ............................................... 57 Agency recommendations for the future ............................................................... 58 Conclusions .......................................................................................................... 59
16. Results: Language ...................................................................................... 60 Fitness for purpose of procedures ........................................................................ 60 Agency perceptions of changes introduced in JA3 ............................................... 61 Agency recommendations for the future ............................................................... 61 Conclusions .......................................................................................................... 61
17. Results: Transparency and Independence................................................ 62 Fitness for purpose of procedures ........................................................................ 62
Agency perceptions of changes introduced in JA3 ............................................... 63
Agency recommendations for the future ............................................................... 63 Conclusions .......................................................................................................... 64
18. Recommendations for implementation support in a future model of HTA cooperation ............................................................................................................. 65
Conclusions .......................................................................................................... 67 Appendix 1: Implementation feedback survey .................................................... 68
Appendix 2: Response rate ................................................................................... 75
EUnetHTA WP7 Deliverable 7.2 – Final report
4
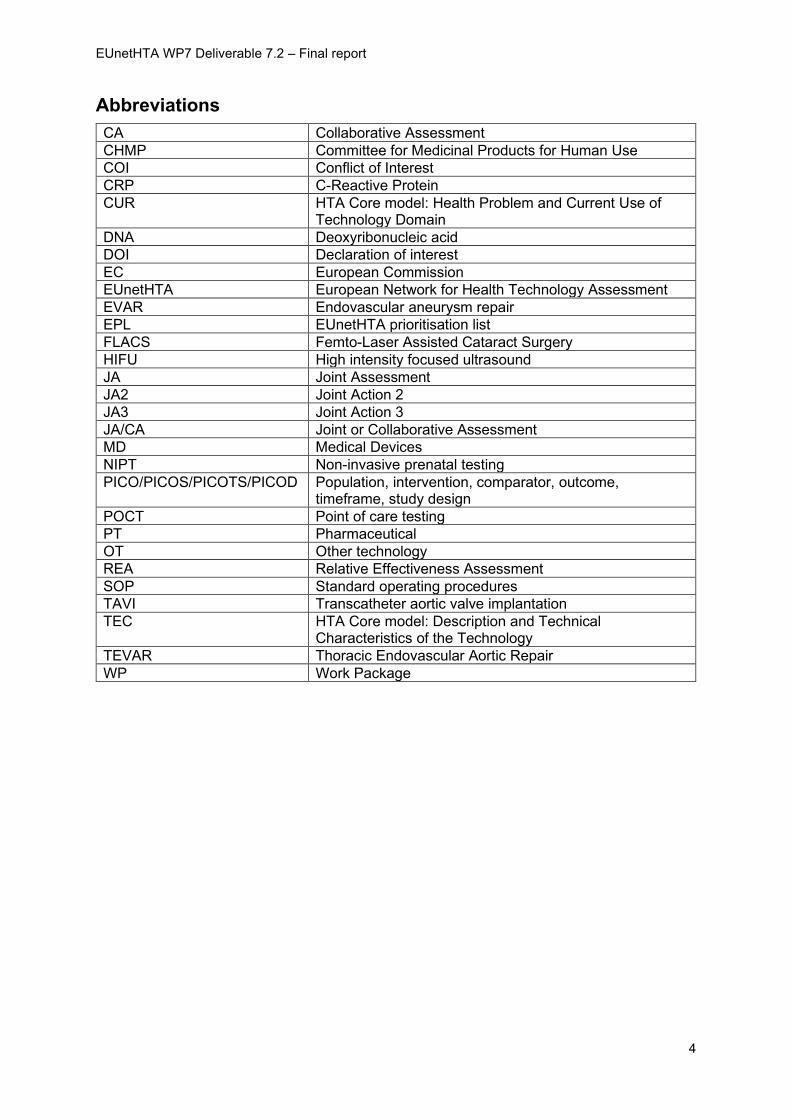
Abbreviations
CA Collaborative Assessment
CHMP Committee for Medicinal Products for Human Use
COI Conflict of Interest
CRP C-Reactive Protein
CUR HTA Core model: Health Problem and Current Use of Technology Domain
DNA Deoxyribonucleic acid
DOI Declaration of interest
EC European Commission
EUnetHTA European Network for Health Technology Assessment
EVAR Endovascular aneurysm repair
EPL EUnetHTA prioritisation list
FLACS Femto-Laser Assisted Cataract Surgery
HIFU High intensity focused ultrasound
JA Joint Assessment
JA2 Joint Action 2
JA3 Joint Action 3
JA/CA Joint or Collaborative Assessment
MD Medical Devices
NIPT Non-invasive prenatal testing
PICO/PICOS/PICOTS/PICOD Population, intervention, comparator, outcome, timeframe, study design
POCT Point of care testing
PT Pharmaceutical
OT Other technology
REA Relative Effectiveness Assessment
SOP Standard operating procedures
TAVI Transcatheter aortic valve implantation
TEC HTA Core model: Description and Technical Characteristics of the Technology
TEVAR Thoracic Endovascular Aortic Repair
WP Work Package
EUnetHTA WP7 Deliverable 7.2 – Final report
5
1. Executive Summary
In this report we describe:
• Use in Joint Action 3 (JA3) of joint assessments (JA) and collaborative
assessments (CA) and compare this with use in Joint Action 2 (JA2).
• How changes in JA and CA processes have affected implementation.
• The extent to which structures, methods and processes being implemented are
“fit for purpose” in terms of awareness, timeliness, relevance, scientific rigour,
evidence and methodology, usability, transparency and independence.
• Recommendations for structures to support implementation in a future model of
Health Technology Assessment (HTA) cooperation based on the JA3 experience.
We do this using survey data about JA2 use collected in JA2 and followed up in JA3,
and survey data about JA3 use collected in JA3. The survey data are complemented
with interview data, responses to email questions and records about agency
involvement in JA2 and in JA3.
Implementation data are available for 27 JA/CA published under JA3. 298 examples
of use have been reported. In total there have been 89 uses of the 7 pharmaceutical
(PT) assessments and 209 uses of the 20 other technology (OT) assessments. Most
uses of the PT assessments (n= 60) are in assessment procedures, with only 29
examples of sharing via dissemination. In contrast, for OT there have been 209
examples of use, with 85 of those in assessment procedures and 124 examples of
sharing via dissemination. Use of PT assessments is usually as part of a
reimbursement and/or pricing procedure, while use of OT assessments is varied
including assessment procedures but also decisions to assess, decisions to review
and targeted and non-targeted dissemination to support local decision making.
For PT there has been increased production and use of JA/CA in JA3 compared to
JA2. For OT there has been increased production of JA/CA, but there is currently
less use of JA/CA in JA3 compared to JA2. For both PT and OT there is an
increased number of countries that have used JA/CA in JA3 compared to JA2.
Changes in JA3 processes are seen to have improved implementation. Changes
made to awareness, timeliness and relevance have allowed greater use. Changes in
scientific rigour, evidence and methodology, usability, transparency and
independence have improved the confidence with which agencies use JA/CA.
Most agencies still report factors that can prevent or limit the extent to which JA/CA
are used. The most frequent factors identified are timeliness and relevance. In
addition, for PT assessments requirements to use a specified report structure and
national language can limit use.
EUnetHTA WP7 Deliverable 7.2 – Final report
6
The tables overleaf make recommendations for key scientific and procedural
features that if put in place would help maximise implementation of JA/CA in a future
model of HTA cooperation. It makes recommendations for 3 groups:
1. the entity responsible for JA/CA in a future model of HTA cooperation (table 1),
2. agencies and countries participating in future HTA cooperation (table 2), and
3. the PT industry (table 3).
This latter group is included in the recommendations because of the role that
industry plays in initiating PT assessments in many countries and providing the
evidence submission for these assessments. Different groups have the primary
responsibility for resolving different issues. Agencies and countries participating have
primary responsibility for addressing language barriers to uptake, while the entity
producing JA/CA in a future model of HTA cooperation has primary responsibility for
creating timely, rigorous, usable and transparent reports. For areas such as
awareness, relevance and evidence and methodology groups have a shared
responsibility for overcoming barriers.
Support for implementation is needed in a future model of HTA cooperation. The
level of implementation support required will differ by agency and country and will
depend on how developed HTA systems are in individual countries and the levels of
HTA experience and expertise within these countries. Once the details of a future
model of HTA cooperation are known, agencies still establishing HTA systems
should be prioritised and offered early, individualised, facilitative support at a country
level (that is, encompassing HTA agencies, and also commissioners and decision
makers) to put in place the capacity, expertise and processes to implement future
ways of working. Modalities of support proposed included online resources and
implementation advisers. The use of audit and monitoring provoked mixed opinions
as to whether these tools were appropriate.
EUnetHTA WP7 Deliverable 7.2 – Final report
7
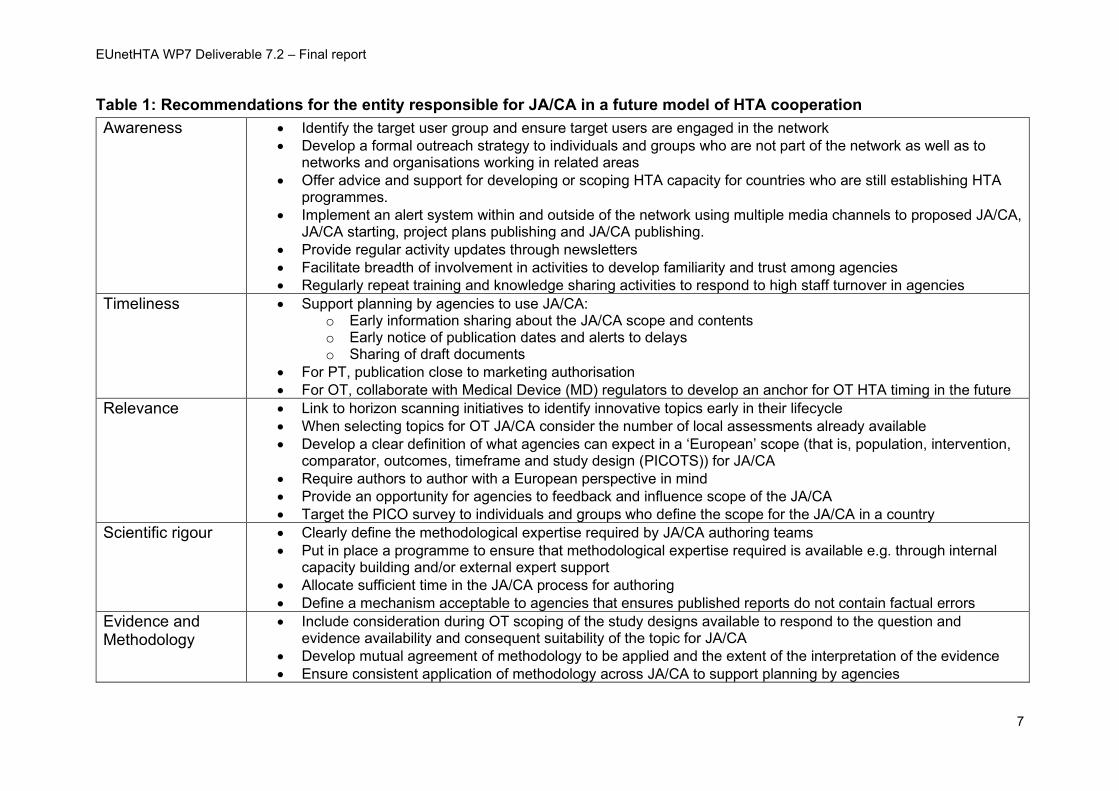
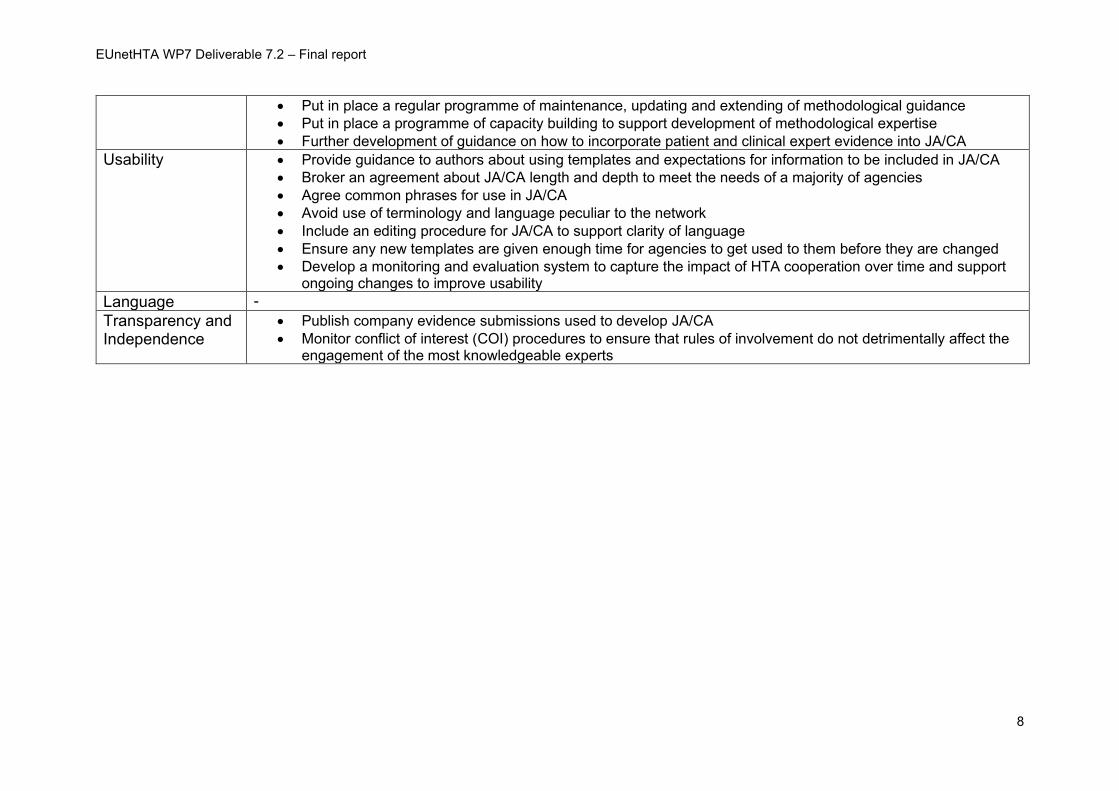
Table 1: Recommendations for the entity responsible for JA/CA in a future model of HTA cooperation
Awareness • Identify the target user group and ensure target users are engaged in the network
• Develop a formal outreach strategy to individuals and groups who are not part of the network as well as to networks and organisations working in related areas
• Offer advice and support for developing or scoping HTA capacity for countries who are still establishing HTA programmes.
• Implement an alert system within and outside of the network using multiple media channels to proposed JA/CA, JA/CA starting, project plans publishing and JA/CA publishing.
• Provide regular activity updates through newsletters
• Facilitate breadth of involvement in activities to develop familiarity and trust among agencies
• Regularly repeat training and knowledge sharing activities to respond to high staff turnover in agencies
Timeliness • Support planning by agencies to use JA/CA: o Early information sharing about the JA/CA scope and contents o Early notice of publication dates and alerts to delays o Sharing of draft documents
• For PT, publication close to marketing authorisation
• For OT, collaborate with Medical Device (MD) regulators to develop an anchor for OT HTA timing in the future
Relevance • Link to horizon scanning initiatives to identify innovative topics early in their lifecycle
• When selecting topics for OT JA/CA consider the number of local assessments already available
• Develop a clear definition of what agencies can expect in a ‘European’ scope (that is, population, intervention, comparator, outcomes, timeframe and study design (PICOTS)) for JA/CA
• Require authors to author with a European perspective in mind
• Provide an opportunity for agencies to feedback and influence scope of the JA/CA
• Target the PICO survey to individuals and groups who define the scope for the JA/CA in a country
Scientific rigour • Clearly define the methodological expertise required by JA/CA authoring teams
• Put in place a programme to ensure that methodological expertise required is available e.g. through internal capacity building and/or external expert support
• Allocate sufficient time in the JA/CA process for authoring
• Define a mechanism acceptable to agencies that ensures published reports do not contain factual errors
Evidence and Methodology
• Include consideration during OT scoping of the study designs available to respond to the question and evidence availability and consequent suitability of the topic for JA/CA
• Develop mutual agreement of methodology to be applied and the extent of the interpretation of the evidence
• Ensure consistent application of methodology across JA/CA to support planning by agencies
EUnetHTA WP7 Deliverable 7.2 – Final report
8
• Put in place a regular programme of maintenance, updating and extending of methodological guidance
• Put in place a programme of capacity building to support development of methodological expertise
• Further development of guidance on how to incorporate patient and clinical expert evidence into JA/CA
Usability • Provide guidance to authors about using templates and expectations for information to be included in JA/CA
• Broker an agreement about JA/CA length and depth to meet the needs of a majority of agencies
• Agree common phrases for use in JA/CA
• Avoid use of terminology and language peculiar to the network
• Include an editing procedure for JA/CA to support clarity of language
• Ensure any new templates are given enough time for agencies to get used to them before they are changed
• Develop a monitoring and evaluation system to capture the impact of HTA cooperation over time and support ongoing changes to improve usability
Language -
Transparency and Independence
• Publish company evidence submissions used to develop JA/CA
• Monitor conflict of interest (COI) procedures to ensure that rules of involvement do not detrimentally affect the engagement of the most knowledgeable experts
EUnetHTA WP7 Deliverable 7.2 – Final report
9
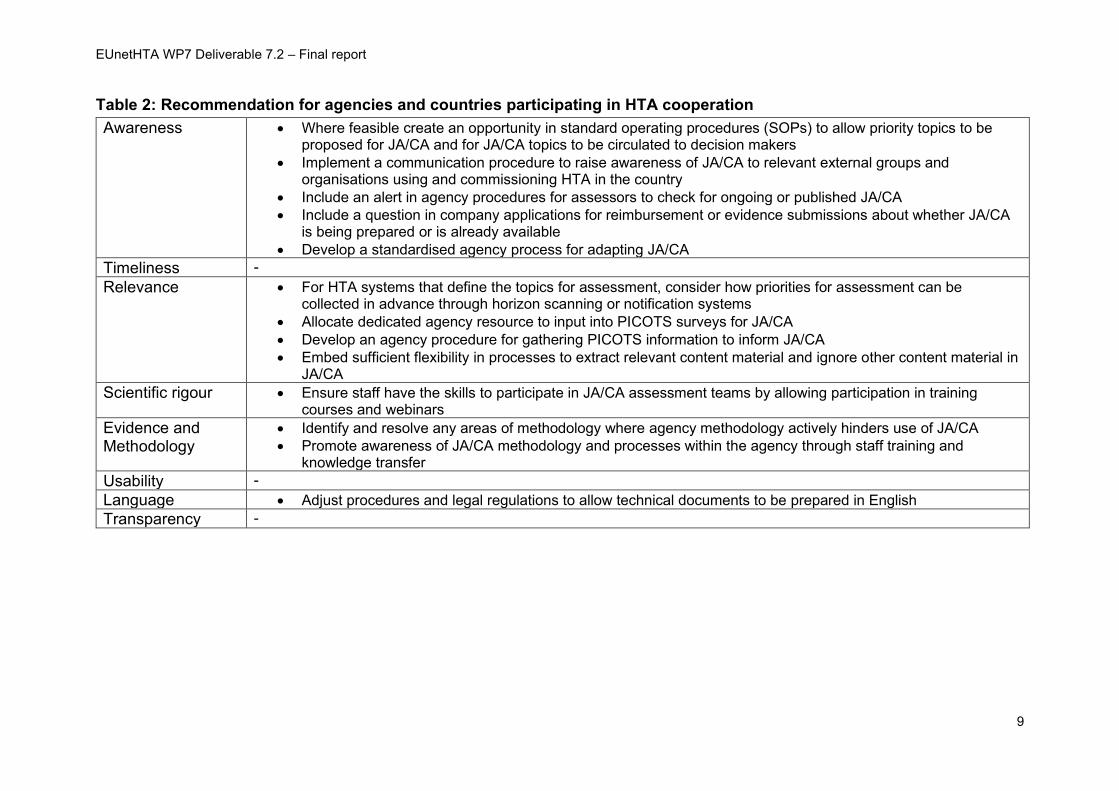
Table 2: Recommendation for agencies and countries participating in HTA cooperation
Awareness • Where feasible create an opportunity in standard operating procedures (SOPs) to allow priority topics to be proposed for JA/CA and for JA/CA topics to be circulated to decision makers
• Implement a communication procedure to raise awareness of JA/CA to relevant external groups and organisations using and commissioning HTA in the country
• Include an alert in agency procedures for assessors to check for ongoing or published JA/CA
• Include a question in company applications for reimbursement or evidence submissions about whether JA/CA is being prepared or is already available
• Develop a standardised agency process for adapting JA/CA
Timeliness -
Relevance • For HTA systems that define the topics for assessment, consider how priorities for assessment can be collected in advance through horizon scanning or notification systems
• Allocate dedicated agency resource to input into PICOTS surveys for JA/CA
• Develop an agency procedure for gathering PICOTS information to inform JA/CA
• Embed sufficient flexibility in processes to extract relevant content material and ignore other content material in JA/CA
Scientific rigour • Ensure staff have the skills to participate in JA/CA assessment teams by allowing participation in training courses and webinars
Evidence and Methodology
• Identify and resolve any areas of methodology where agency methodology actively hinders use of JA/CA
• Promote awareness of JA/CA methodology and processes within the agency through staff training and knowledge transfer
Usability -
Language • Adjust procedures and legal regulations to allow technical documents to be prepared in English
Transparency -
EUnetHTA WP7 Deliverable 7.2 – Final report
10
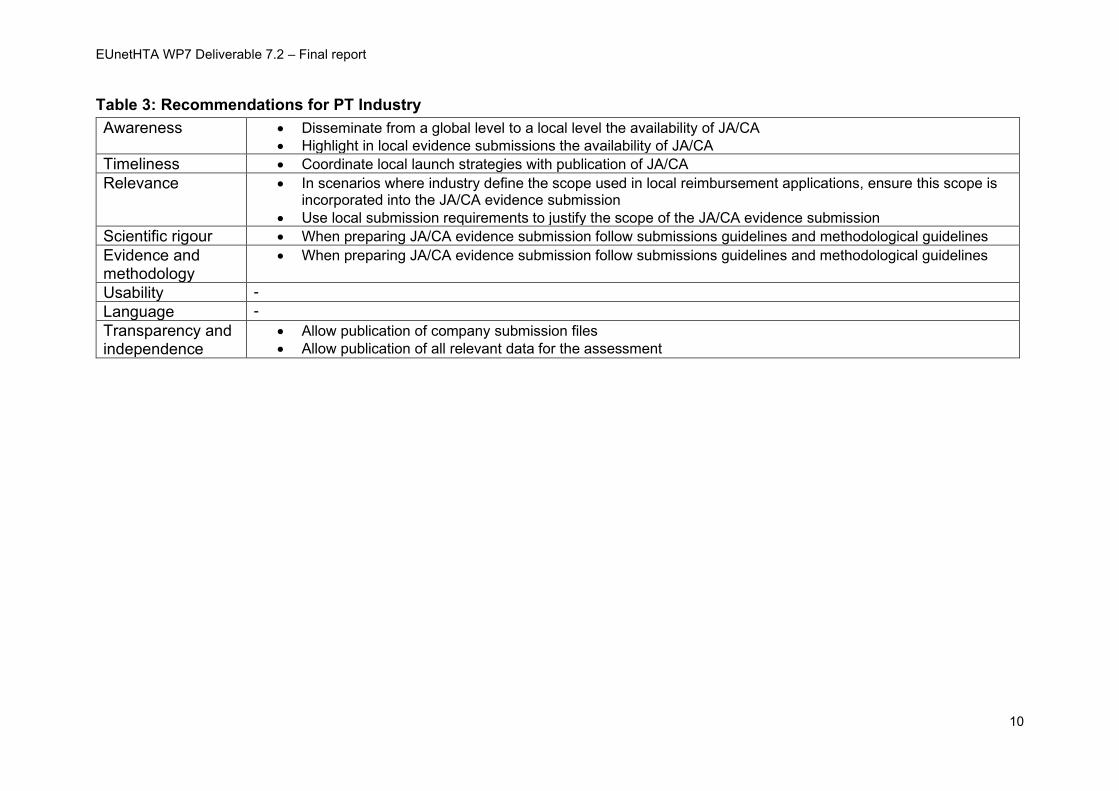
Table 3: Recommendations for PT Industry
Awareness • Disseminate from a global level to a local level the availability of JA/CA
• Highlight in local evidence submissions the availability of JA/CA
Timeliness • Coordinate local launch strategies with publication of JA/CA
Relevance • In scenarios where industry define the scope used in local reimbursement applications, ensure this scope is incorporated into the JA/CA evidence submission
• Use local submission requirements to justify the scope of the JA/CA evidence submission
Scientific rigour • When preparing JA/CA evidence submission follow submissions guidelines and methodological guidelines
Evidence and methodology
• When preparing JA/CA evidence submission follow submissions guidelines and methodological guidelines
Usability -
Language -
Transparency and independence
• Allow publication of company submission files
• Allow publication of all relevant data for the assessment
EUnetHTA WP7 Deliverable 7.2 – Final report
11
4. Introduction and Objectives
Introduction
There are two main objectives of the European Network for Health Technology
Assessment (EUnetHTA) JA3:
1.1 To increase the use, quality and efficiency of joint HTA work at
European level to support evidence-based, sustainable and equitable
choices in healthcare and health technologies and ensure re-use in
regional and national HTA reports and activities.
1.2 To support voluntary cooperation at scientific and technical level
between HTA agencies by providing a sustainable model for the scientific
and technical mechanism of a permanent European cooperation on HTA
This report supports these objectives. The report describes use of JA3 JA/CA and
compare this with use in JA2 and makes recommendations for structures to support
implementation in a future model of HTA cooperation based on the JA3 experience.
Objectives
This report answers the following research questions:
1. Compared with JA2, has there been an increase in JA3 in the number and
uptake of JA/CA?
2. What is the relationship between changes in uptake and changes in JA/CA
processes, including:
a. changes that were implemented between JA2 and JA3, and
b. changes that were implemented in JA3?
3. To what extent are the structures, methods and processes being used fit for
purpose meeting the individual needs of agencies?
4. What are the key scientific and procedural features that need to be put in
place by the individuals, groups, and agencies coordinating and participating
in future HTA cooperation to maximise implementation of JA/CA?
5. What support for implementation (e.g. implementation advisers, mechanisms
for shared learning, measurement and evaluation of implementation) should
be built into a future model of HTA cooperation?
EUnetHTA WP7 Deliverable 7.2 – Final report
12
5. Methods
Data collection
At the start of JA3, EUnetHTA developed a feedback tool to capture use of JA/CA
(see appendix 1). The tool was developed collaboratively by Work Package (WP) 1,
WP3 and WP7 to support monitoring and evaluation by WP3 and WP7. The draft
tool was subject to consultation with EUnetHTA WP7 partners.
The final tool is available on the EUnetHTA intranet and EUnetHTA partners are
asked to complete the feedback survey after publication of each JA/CA and update
their survey entry if their work status changes. A password protected version is
available on the EUnetHTA internet so that non-EUnetHTA agencies can also
provide feedback on their use of JA/CA.
The data used in this analysis were downloaded June 29th, 2020.
The data from the WP7 implementation survey is supplemented in this report by the
findings from an e-mail survey sent to selected agencies (N=38) to identify reasons for
patterns of use and changes in use between JA2 and JA3. We received 22 responses
to the email survey.
Additionally, semi-structured qualitative interviews were undertaken with 12 selected
agencies to collect more detailed information, specifically on:
• their perceptions of the changes made to the production processes and the
impact of these on implementation
• their ability to participate in process stages requiring user engagement (for
example topic identification, selection and prioritisation pilots, scoping and
authoring)
• the extent to which the structures, methods and processes being implemented
are considered "fit for purpose" in meeting their needs. Areas of discussion
focussed on awareness, timeliness, relevance, scientific rigour, evidence and
methodology, usability, transparency and independence.
WP7 also updated the JA2 evaluation results to capture examples of use of JA2
assessments that had occurred after the end of JA2. The JA2 implementation data in
this report includes follow up to April 2018. Further details of the JA2 data used in
this report are available in the implementation report published in May 20181.
1 https://eunethta.eu/wp-content/uploads/2018/06/May-2018-Implementation-report_website_FINAL.pdf
EUnetHTA WP7 Deliverable 7.2 – Final report
13
Methods of Analysis
Stage 1: Identification of procedural changes
In stage 1 of the work WP7, WP4 and WP6 lead and co-lead partners developed a
list of changes in JA3 assessment processes to be evaluated. Changes evaluated
were those perceived to have an effect on implementation either in terms of the
absolute level of implementation (e.g. number of agencies using JA/CA) or on the
implementation experience (e.g. trust in the JA/CA or ease of JA/CA adaptation).
The changes were grouped into key themes for analysis, for example: changes
aimed to improve timeliness, relevance, scientific rigour and awareness.
Differences in production processes for PT and OT assessments means that this
report evaluates a different set of changes for PT compared with OT assessments.
Stage 2: Relationship between existing procedures, procedural changes and uptake
In stage 2 of the work the relationship between changes in JA3 procedures and
uptake of JA/CA was explored. In this stage of the work the quantitative and
qualitative data from the implementation feedback survey, records of partner
involvement, email survey and interviews were thematically analysed. The themes
for analysis were the effect of changes on (1) awareness of reports, (2) report
timeliness, (3) scope and content relevance, (4) reliability and scientific rigour, (5)
appropriateness of evidence and methodology applied, (6) usability in terms of report
structure and language, (7) transparency and independence.
Stage 3: Definition of uptake processes
The final stage of the work sought to make recommendations for the scientific and
procedural features that need to be in place to maximise uptake of JA/CA in a future
model of HTA cooperation. These recommendations were developed from the
outcomes of the stage 2 work and additionally areas where agencies identified that
further improvements were needed.
EUnetHTA WP7 Deliverable 7.2 – Final report
14
6. Report structure
The results and recommendations are presented in the following order:
Section 5 presents a summary of the implementation data reported in JA3
Section 6 addresses the first research question:
1. Compared with JA2, has there been an increase in JA3 in the number and
uptake of JA/CA?
Section 7 explores the relationship between reported use in JA2, participation in
production processes in JA3 and reported use in JA3.
Sections 8-14 address the second, third and fourth research questions:
2. What is the relationship between changes in uptake and changes in
JA/CA processes, including:
a. changes that were implemented between JA2 and JA3 and
b. changes that were implemented in JA3?
3. To what extent are the structures, methods and processes being
implemented “fit for purpose” meeting the individual needs of
agencies?
4. What are the key scientific and procedural features that need to be
put in place by the individuals, groups, and agencies coordinating
and participating in future HTA cooperation to maximise
implementation of JA/CA?
These sections are structured around the following key themes
• Awareness
• Timing
• Relevance and transferability
• Reliability and scientific rigour
• Evidence and methodology
• Usability and reporting structure
• Language

EUnetHTA WP7 Deliverable 7.2 – Final report
15
• Transparency and independence
Section 16 addresses the final research question:
What support for implementation should be built into a future model of HTA
cooperation?
EUnetHTA WP7 Deliverable 7.2 – Final report
16
7. Results: Overview of the JA3 use of JA/CA
This report includes 27 JA/CA that have been published under JA3 up to the end of
April 2020 for which implementation data are available, 20 OT assessments and 7
PT assessments. An 8th PT assessment sotagliflozin (PTJA04), has been published
but as yet no implementation data are reported because it is not launched in Europe.
To accurately capture the implementation of JA/CA a follow up period of
approximately 18 months to 2 years is needed for PT and of approximately 3 years
for OT. At the time of writing this report, 4 OT assessments (OTCA17, OTCA18,
OTCA20 and OTCA22) and 3 PT assessments (PTJA06, PTJA08 and PTJA09)
have been published for under 6 months. An additional 3 OT assessments
(OTCA10, OTCA14 and OTCA19) and 1 PT assessment (PTJA07) have been
published for less than 1 year. Data reported for these JA/CA will be affected by an
inadequate follow-up period.
Response Rate
The agency response rate to the survey is high with similar levels for OT and PT. For
JA/CA published over 6 months ago the response rate ranges from 43-86% (see
appendix 2 for a breakdown). As expected, response rates increase over time as
companies submit applications for reimbursement and/or agencies make decisions
to complete or not to complete work on a topic. The highest response rates are for
assessments with the longest follow-up period.
Shortly after publication of JA/CA responses to the implementation feedback survey
are usually from agencies who know they will not or are unlikely to work on a topic
e.g. it is out of remit or work has already been carried out. In addition, earlier
responders to the survey tend to be (1) agencies in countries where companies
launch their PT products earliest, (2) from authors of OT JA/CA where the topic is
already in their work programme and from (3) agencies who are able to choose their
own work areas and have identified the topic as relevant to their context. Agencies
responding early on to the implementation feedback survey are not a representative
sample of all JA/CA users and this should be considered when interpreting the
implementation feedback survey data from recently published assessments.
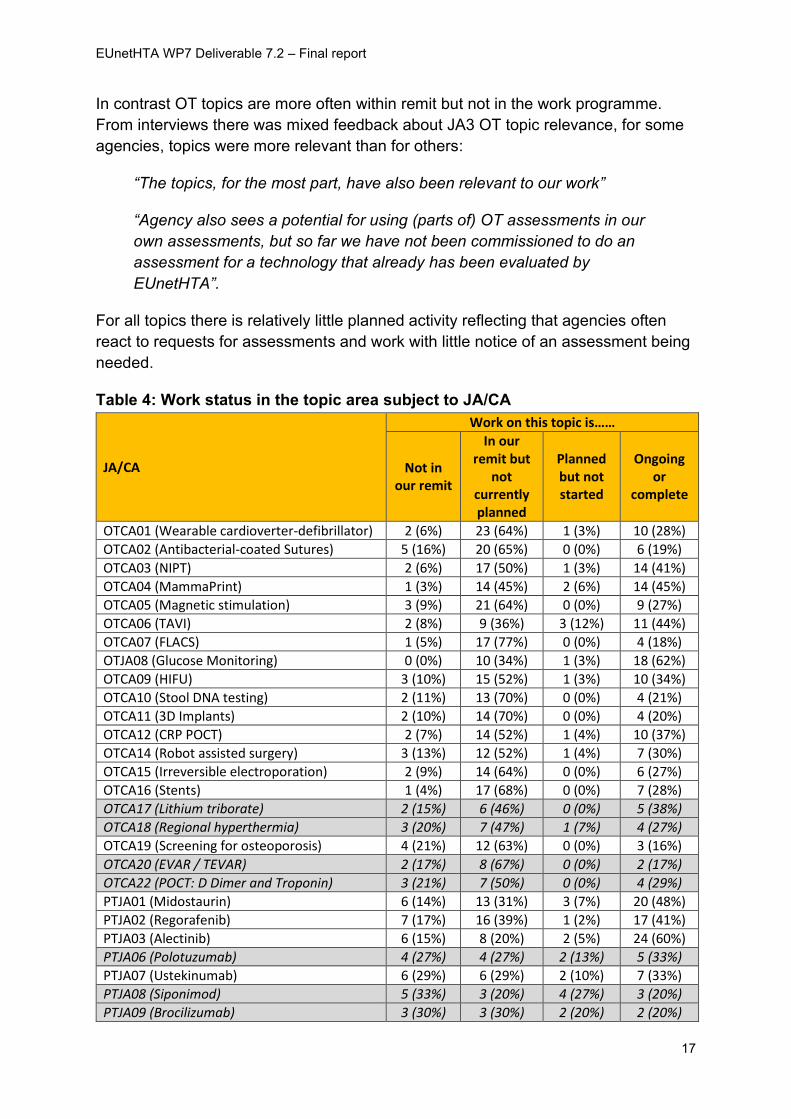
Topic relevance
As shown in table 4, EUnetHTA is usually selecting topics that are within an
agency’s remit. There are slightly higher levels of PT topics being out of remit than
OT topics. In their responses agencies indicated that they may (1) only do certain PT
products e.g. inpatient or outpatient products, (2) have additional criteria to select PT
topics for HTA such as likely budget impact or (3) only do specific types of PT HTA
e.g. multiple technology assessments.
EUnetHTA WP7 Deliverable 7.2 – Final report
17
In contrast OT topics are more often within remit but not in the work programme.
From interviews there was mixed feedback about JA3 OT topic relevance, for some
agencies, topics were more relevant than for others:
“The topics, for the most part, have also been relevant to our work”
“Agency also sees a potential for using (parts of) OT assessments in our
own assessments, but so far we have not been commissioned to do an
assessment for a technology that already has been evaluated by
EUnetHTA”.
For all topics there is relatively little planned activity reflecting that agencies often
react to requests for assessments and work with little notice of an assessment being
needed.
Table 4: Work status in the topic area subject to JA/CA
JA/CA
Work on this topic is……
Not in our remit
In our remit but
not currently planned
Planned but not started
Ongoing or
complete
OTCA01 (Wearable cardioverter-defibrillator) 2 (6%) 23 (64%) 1 (3%) 10 (28%)
OTCA02 (Antibacterial-coated Sutures) 5 (16%) 20 (65%) 0 (0%) 6 (19%)
OTCA03 (NIPT) 2 (6%) 17 (50%) 1 (3%) 14 (41%)
OTCA04 (MammaPrint) 1 (3%) 14 (45%) 2 (6%) 14 (45%)
OTCA05 (Magnetic stimulation) 3 (9%) 21 (64%) 0 (0%) 9 (27%)
OTCA06 (TAVI) 2 (8%) 9 (36%) 3 (12%) 11 (44%)
OTCA07 (FLACS) 1 (5%) 17 (77%) 0 (0%) 4 (18%)
OTJA08 (Glucose Monitoring) 0 (0%) 10 (34%) 1 (3%) 18 (62%)
OTCA09 (HIFU) 3 (10%) 15 (52%) 1 (3%) 10 (34%)
OTCA10 (Stool DNA testing) 2 (11%) 13 (70%) 0 (0%) 4 (21%)
OTCA11 (3D Implants) 2 (10%) 14 (70%) 0 (0%) 4 (20%)
OTCA12 (CRP POCT) 2 (7%) 14 (52%) 1 (4%) 10 (37%)
OTCA14 (Robot assisted surgery) 3 (13%) 12 (52%) 1 (4%) 7 (30%)
OTCA15 (Irreversible electroporation) 2 (9%) 14 (64%) 0 (0%) 6 (27%)
OTCA16 (Stents) 1 (4%) 17 (68%) 0 (0%) 7 (28%)
OTCA17 (Lithium triborate) 2 (15%) 6 (46%) 0 (0%) 5 (38%)
OTCA18 (Regional hyperthermia) 3 (20%) 7 (47%) 1 (7%) 4 (27%)
OTCA19 (Screening for osteoporosis) 4 (21%) 12 (63%) 0 (0%) 3 (16%)
OTCA20 (EVAR / TEVAR) 2 (17%) 8 (67%) 0 (0%) 2 (17%)
OTCA22 (POCT: D Dimer and Troponin) 3 (21%) 7 (50%) 0 (0%) 4 (29%)
PTJA01 (Midostaurin) 6 (14%) 13 (31%) 3 (7%) 20 (48%)
PTJA02 (Regorafenib) 7 (17%) 16 (39%) 1 (2%) 17 (41%)
PTJA03 (Alectinib) 6 (15%) 8 (20%) 2 (5%) 24 (60%)
PTJA06 (Polotuzumab) 4 (27%) 4 (27%) 2 (13%) 5 (33%)
PTJA07 (Ustekinumab) 6 (29%) 6 (29%) 2 (10%) 7 (33%)
PTJA08 (Siponimod) 5 (33%) 3 (20%) 4 (27%) 3 (20%)
PTJA09 (Brocilizumab) 3 (30%) 3 (30%) 2 (20%) 2 (20%)
EUnetHTA WP7 Deliverable 7.2 – Final report
18
Gray shaded cells are the most recently published JA/CA <6 months
Use of JA/CA
Under JA3 implementation data are collected on two principal types of use:
1. Support for or as an alternative to the agency’s existing HTA procedures
2. Dissemination of JA/CA to support awareness of the availability of JA/CA and/or
evidence informed decision making
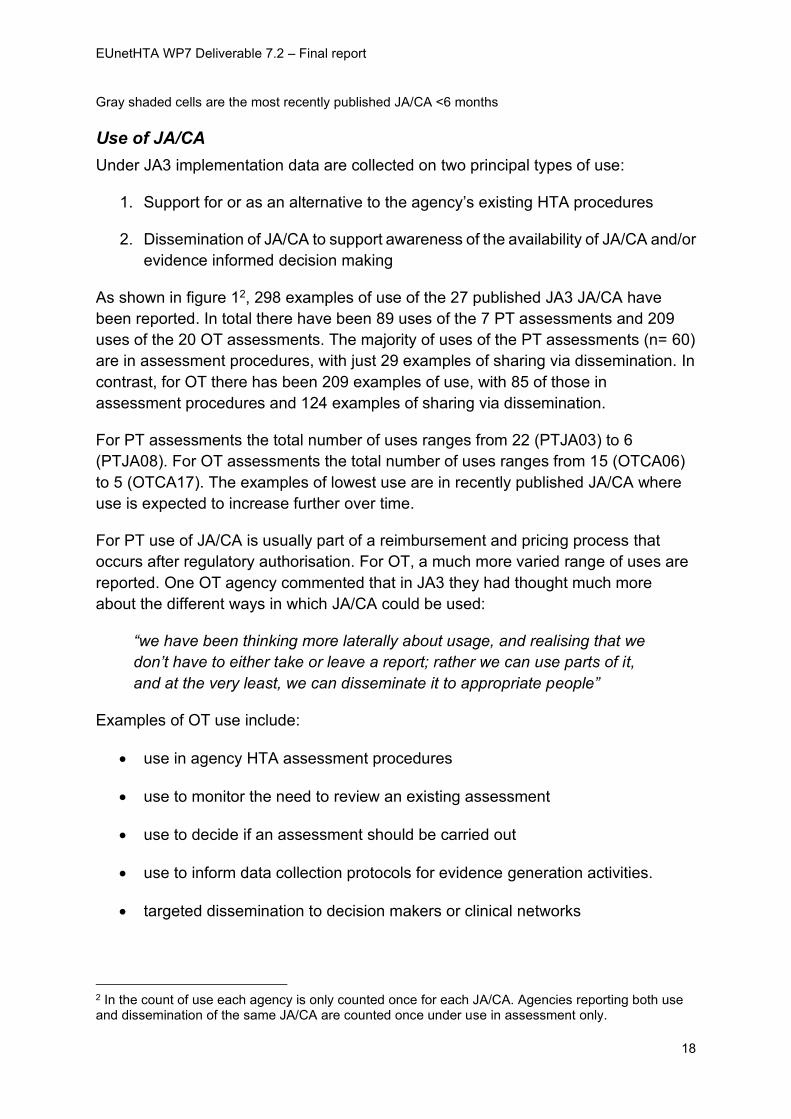
As shown in figure 12, 298 examples of use of the 27 published JA3 JA/CA have
been reported. In total there have been 89 uses of the 7 PT assessments and 209
uses of the 20 OT assessments. The majority of uses of the PT assessments (n= 60)
are in assessment procedures, with just 29 examples of sharing via dissemination. In
contrast, for OT there has been 209 examples of use, with 85 of those in
assessment procedures and 124 examples of sharing via dissemination.
For PT assessments the total number of uses ranges from 22 (PTJA03) to 6
(PTJA08). For OT assessments the total number of uses ranges from 15 (OTCA06)
to 5 (OTCA17). The examples of lowest use are in recently published JA/CA where
use is expected to increase further over time.
For PT use of JA/CA is usually part of a reimbursement and pricing process that
occurs after regulatory authorisation. For OT, a much more varied range of uses are
reported. One OT agency commented that in JA3 they had thought much more
about the different ways in which JA/CA could be used:
“we have been thinking more laterally about usage, and realising that we
don’t have to either take or leave a report; rather we can use parts of it,
and at the very least, we can disseminate it to appropriate people”
Examples of OT use include:
• use in agency HTA assessment procedures
• use to monitor the need to review an existing assessment
• use to decide if an assessment should be carried out
• use to inform data collection protocols for evidence generation activities.
• targeted dissemination to decision makers or clinical networks
2 In the count of use each agency is only counted once for each JA/CA. Agencies reporting both use and dissemination of the same JA/CA are counted once under use in assessment only.
EUnetHTA WP7 Deliverable 7.2 – Final report
19
• non-targeted dissemination in newsletters and on websites
Targeted dissemination to decision makers and clinical networks sometimes
included an explicit decision about whether a topic should proceed for agency
assessment, or if an existing agency assessment should be reviewed. In other
cases, the JA/CA was shared for information only.
Figure 1: Use of the JA3 JA/CA
EUnetHTA WP7 Deliverable 7.2 – Final report
20
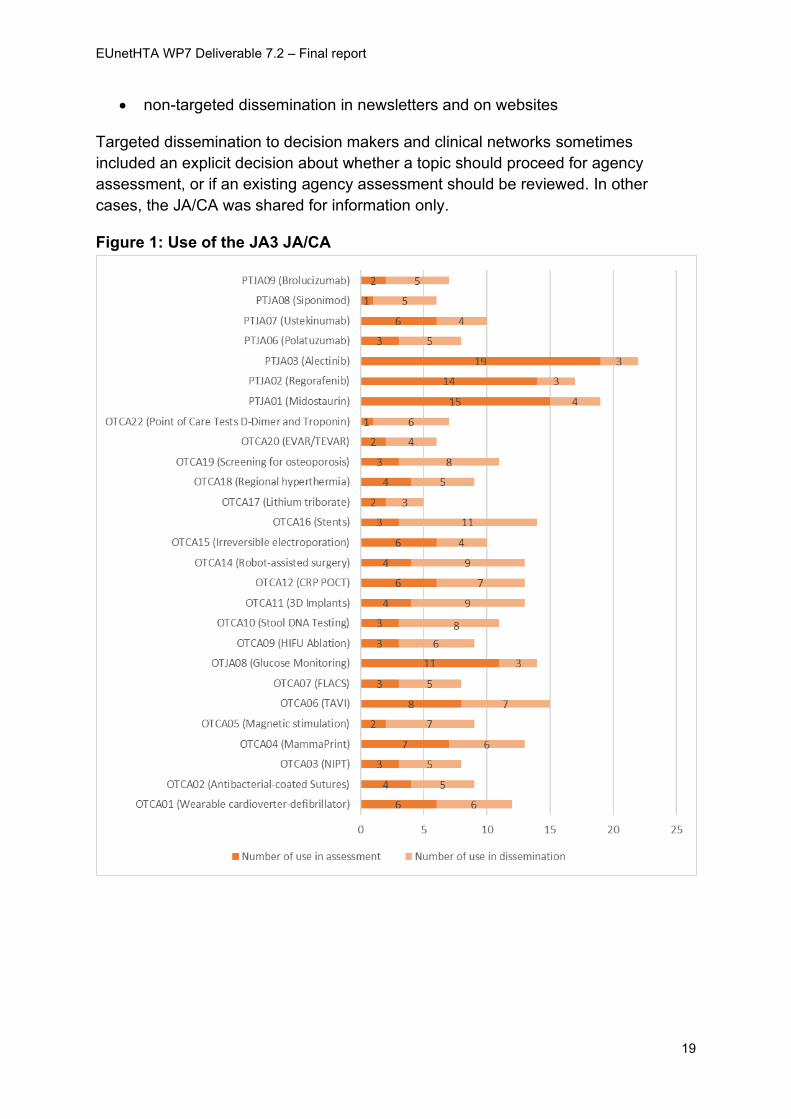
Countries reporting use of JA/CA
For PT assessments 19 countries report using a JA3 JA/CA. All 19 countries report
use in assessment activities. Countries using PT assessments in their assessment
activities report using between 1-7 JA/CA. Six countries report using 1-2 JA/CA, 11
countries report using 3-4 JA/CA and 2 countries report using 5 or more.
For OT assessments 20 countries report using a JA3 JA/CA. Of those, 17 report use
in assessment activities and 3 countries report dissemination of reports only
(Germany, Romania and Sweden). Six countries report using 1-2 JA/CA in their
assessment activities, 5 countries report using 3-4 JA/CA, 3 countries report using 5-
6 JA/CA and 3 countries report using 7 or more JA/CA. The highest use is reported
by Austria.
Figure 2 below provides colour coded maps illustrating the number of uses of JA/CA
in assessment activities. The darker the shading indicates the more reported uses.
Figure 2: Number of uses of JA/CA – analysis by country
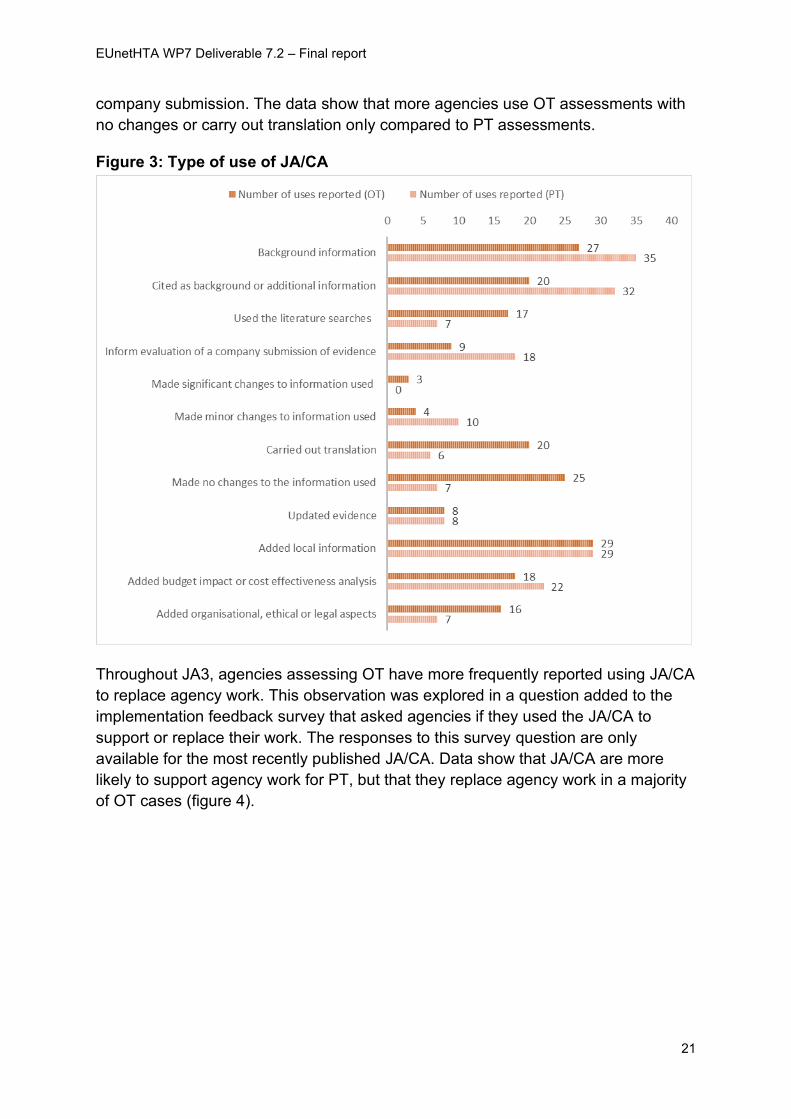
Type of use of JA/CA
Figure 3 below details the type of use of JA/CA published under JA3. Most frequently
the JA/CA is read for background information or cited in the agency assessment as
background or additional information. Agencies also frequently reported using the
JA/CA and adding local information and budget impact or cost-effectiveness
analysis. PT assessments are also frequently used to inform the evaluation of a
EUnetHTA WP7 Deliverable 7.2 – Final report
21
company submission. The data show that more agencies use OT assessments with
no changes or carry out translation only compared to PT assessments.
Figure 3: Type of use of JA/CA
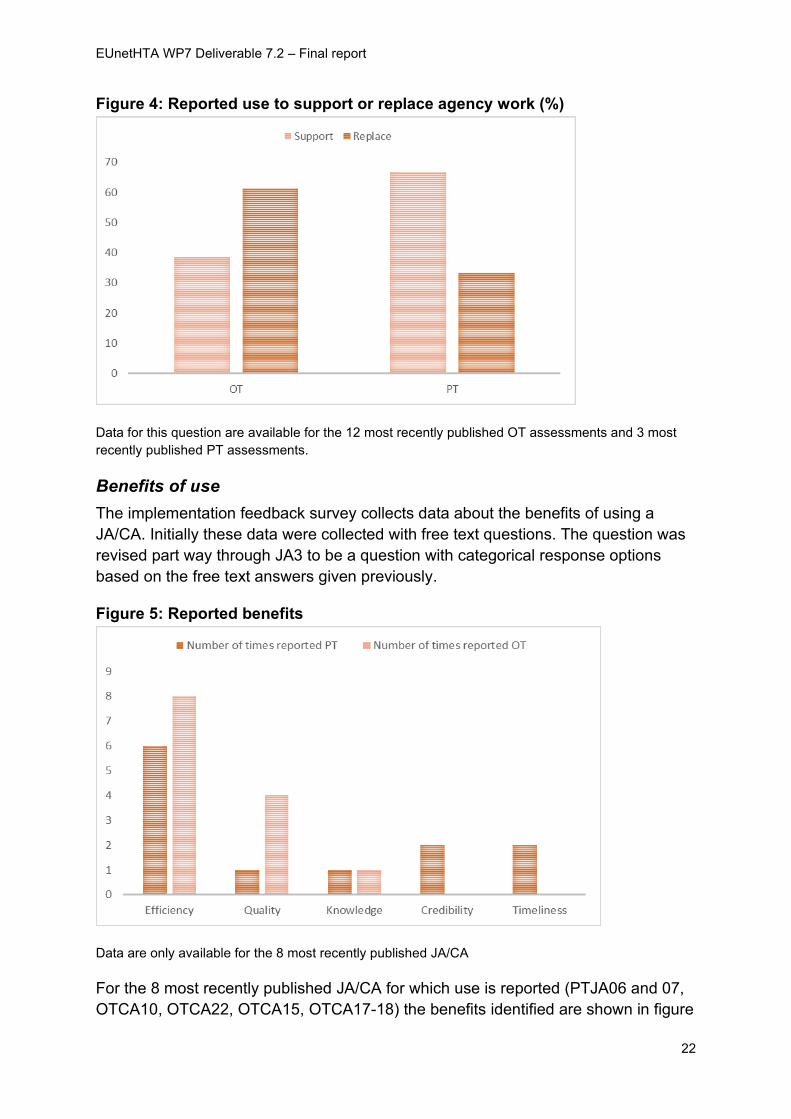
Throughout JA3, agencies assessing OT have more frequently reported using JA/CA
to replace agency work. This observation was explored in a question added to the
implementation feedback survey that asked agencies if they used the JA/CA to
support or replace their work. The responses to this survey question are only
available for the most recently published JA/CA. Data show that JA/CA are more
likely to support agency work for PT, but that they replace agency work in a majority
of OT cases (figure 4).
EUnetHTA WP7 Deliverable 7.2 – Final report
22
Figure 4: Reported use to support or replace agency work (%)
Data for this question are available for the 12 most recently published OT assessments and 3 most
recently published PT assessments.
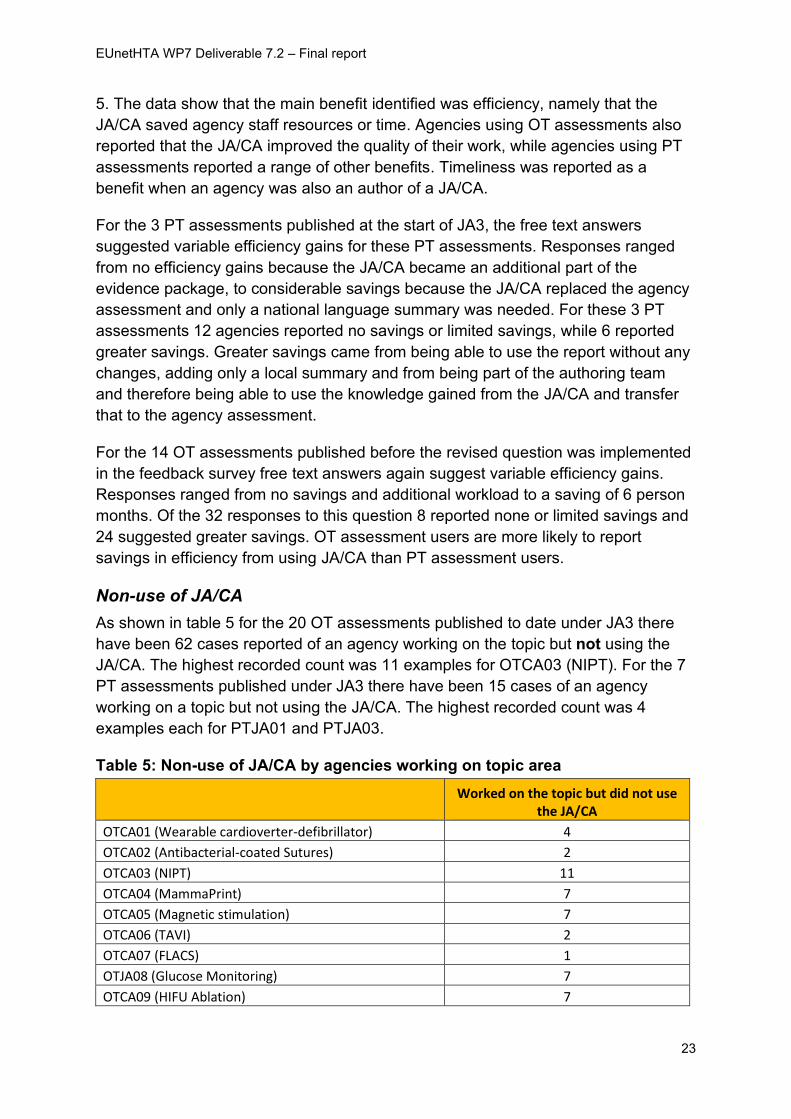
Benefits of use
The implementation feedback survey collects data about the benefits of using a
JA/CA. Initially these data were collected with free text questions. The question was
revised part way through JA3 to be a question with categorical response options
based on the free text answers given previously.
Figure 5: Reported benefits
Data are only available for the 8 most recently published JA/CA
For the 8 most recently published JA/CA for which use is reported (PTJA06 and 07,
OTCA10, OTCA22, OTCA15, OTCA17-18) the benefits identified are shown in figure
EUnetHTA WP7 Deliverable 7.2 – Final report
23
5. The data show that the main benefit identified was efficiency, namely that the
JA/CA saved agency staff resources or time. Agencies using OT assessments also
reported that the JA/CA improved the quality of their work, while agencies using PT
assessments reported a range of other benefits. Timeliness was reported as a
benefit when an agency was also an author of a JA/CA.
For the 3 PT assessments published at the start of JA3, the free text answers
suggested variable efficiency gains for these PT assessments. Responses ranged
from no efficiency gains because the JA/CA became an additional part of the
evidence package, to considerable savings because the JA/CA replaced the agency
assessment and only a national language summary was needed. For these 3 PT
assessments 12 agencies reported no savings or limited savings, while 6 reported
greater savings. Greater savings came from being able to use the report without any
changes, adding only a local summary and from being part of the authoring team
and therefore being able to use the knowledge gained from the JA/CA and transfer
that to the agency assessment.
For the 14 OT assessments published before the revised question was implemented
in the feedback survey free text answers again suggest variable efficiency gains.
Responses ranged from no savings and additional workload to a saving of 6 person
months. Of the 32 responses to this question 8 reported none or limited savings and
24 suggested greater savings. OT assessment users are more likely to report
savings in efficiency from using JA/CA than PT assessment users.
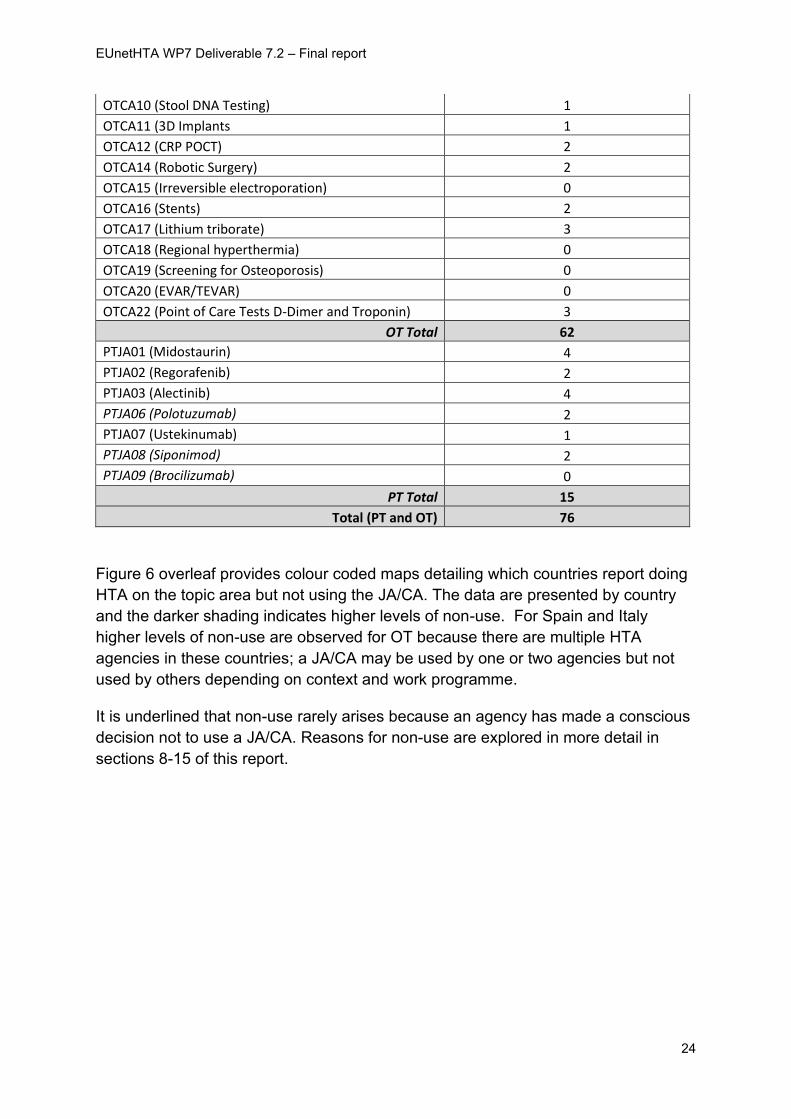
Non-use of JA/CA
As shown in table 5 for the 20 OT assessments published to date under JA3 there
have been 62 cases reported of an agency working on the topic but not using the
JA/CA. The highest recorded count was 11 examples for OTCA03 (NIPT). For the 7
PT assessments published under JA3 there have been 15 cases of an agency
working on a topic but not using the JA/CA. The highest recorded count was 4
examples each for PTJA01 and PTJA03.
Table 5: Non-use of JA/CA by agencies working on topic area
Worked on the topic but did not use
the JA/CA
OTCA01 (Wearable cardioverter-defibrillator) 4
OTCA02 (Antibacterial-coated Sutures) 2
OTCA03 (NIPT) 11
OTCA04 (MammaPrint) 7
OTCA05 (Magnetic stimulation) 7
OTCA06 (TAVI) 2
OTCA07 (FLACS) 1
OTJA08 (Glucose Monitoring) 7
OTCA09 (HIFU Ablation) 7
EUnetHTA WP7 Deliverable 7.2 – Final report
24
OTCA10 (Stool DNA Testing) 1
OTCA11 (3D Implants 1
OTCA12 (CRP POCT) 2
OTCA14 (Robotic Surgery) 2
OTCA15 (Irreversible electroporation) 0
OTCA16 (Stents) 2
OTCA17 (Lithium triborate) 3
OTCA18 (Regional hyperthermia) 0
OTCA19 (Screening for Osteoporosis) 0
OTCA20 (EVAR/TEVAR) 0
OTCA22 (Point of Care Tests D-Dimer and Troponin) 3
OT Total 62
PTJA01 (Midostaurin) 4
PTJA02 (Regorafenib) 2
PTJA03 (Alectinib) 4
PTJA06 (Polotuzumab) 2
PTJA07 (Ustekinumab) 1
PTJA08 (Siponimod) 2
PTJA09 (Brocilizumab) 0
PT Total 15
Total (PT and OT) 76
Figure 6 overleaf provides colour coded maps detailing which countries report doing
HTA on the topic area but not using the JA/CA. The data are presented by country
and the darker shading indicates higher levels of non-use. For Spain and Italy
higher levels of non-use are observed for OT because there are multiple HTA
agencies in these countries; a JA/CA may be used by one or two agencies but not
used by others depending on context and work programme.
It is underlined that non-use rarely arises because an agency has made a conscious
decision not to use a JA/CA. Reasons for non-use are explored in more detail in
sections 8-15 of this report.
EUnetHTA WP7 Deliverable 7.2 – Final report
25
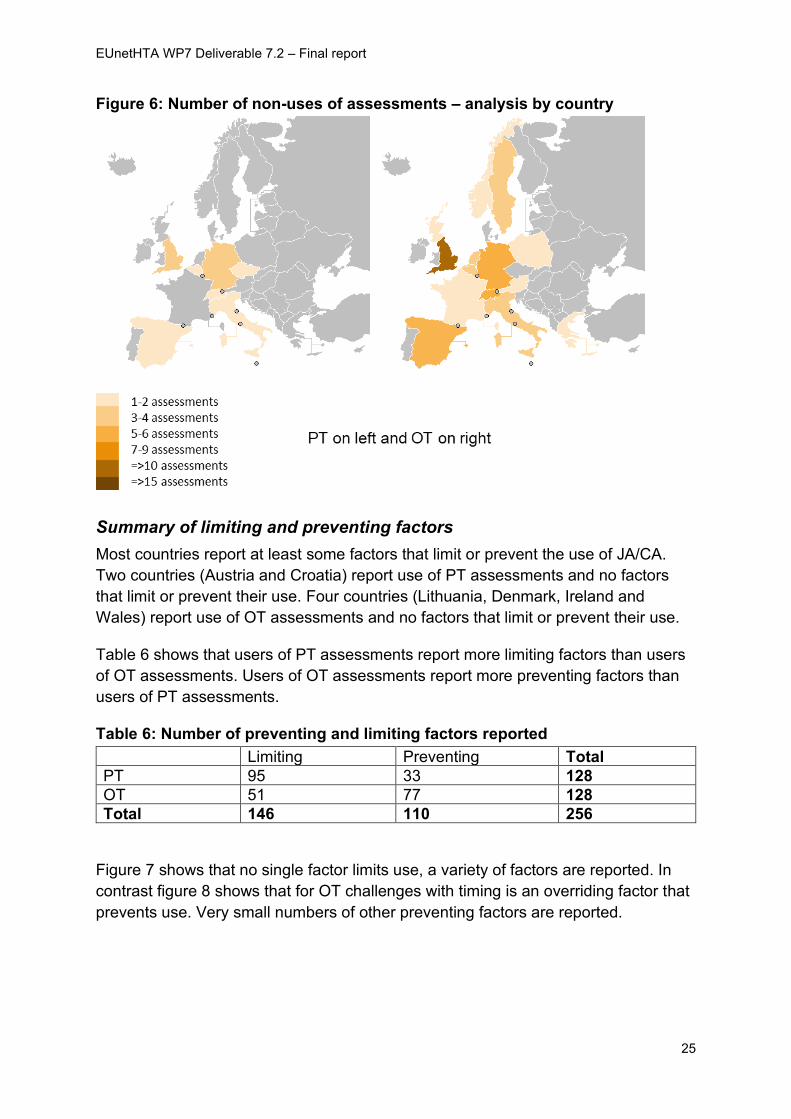
Figure 6: Number of non-uses of assessments – analysis by country
Summary of limiting and preventing factors
Most countries report at least some factors that limit or prevent the use of JA/CA.
Two countries (Austria and Croatia) report use of PT assessments and no factors
that limit or prevent their use. Four countries (Lithuania, Denmark, Ireland and
Wales) report use of OT assessments and no factors that limit or prevent their use.
Table 6 shows that users of PT assessments report more limiting factors than users
of OT assessments. Users of OT assessments report more preventing factors than
users of PT assessments.
Table 6: Number of preventing and limiting factors reported
Limiting Preventing Total
PT 95 33 128
OT 51 77 128
Total 146 110 256
Figure 7 shows that no single factor limits use, a variety of factors are reported. In
contrast figure 8 shows that for OT challenges with timing is an overriding factor that
prevents use. Very small numbers of other preventing factors are reported.

EUnetHTA WP7 Deliverable 7.2 – Final report
26
Figure 7: Number of limiting factors reported by category
Figure 8: Preventing factors reported by category
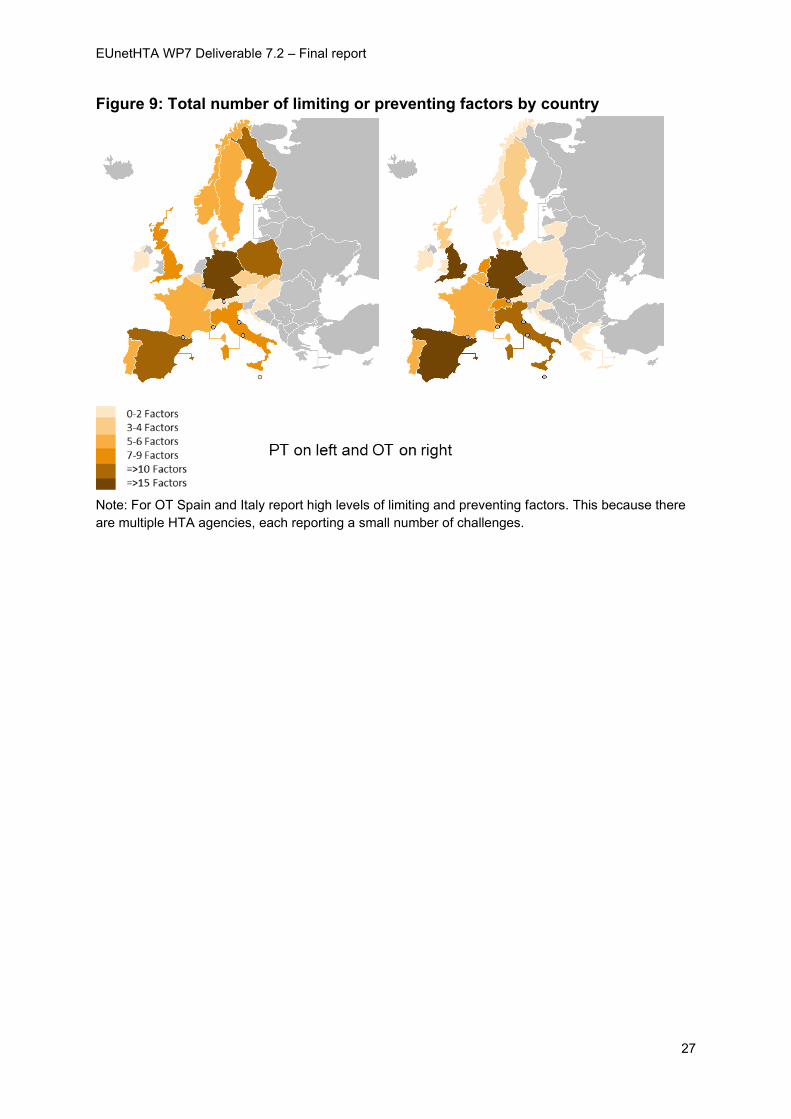
The maps (figure 9) below show the number of factors reported to limit or prevent
use of JA/CA by country. In each map the darker the shading indicates that a country
reports more limiting and preventing factors. When interpreting these data, the data
will in part be related to the number of assessments that were used or not used e.g.
a country reporting more use or non-use of JA/CA also has more opportunities to
report factors that either prevent or limit the use of the JA/CA. However, the maps
show that not all countries have the same level of challenges.
EUnetHTA WP7 Deliverable 7.2 – Final report
27
Figure 9: Total number of limiting or preventing factors by country
Note: For OT Spain and Italy report high levels of limiting and preventing factors. This because there
are multiple HTA agencies, each reporting a small number of challenges.
EUnetHTA WP7 Deliverable 7.2 – Final report
28
8. Results: Comparison of use in JA2 and JA3
The results of the analysis presented in this section of the report draw primarily on
findings from the JA3 implementation feedback survey and data on use of JA2
relative effectiveness assessments3. In JA2, both full Core HTA and rapid relative
effectiveness assessments were produced, but for this analysis only JA2 rapid
relative effectiveness assessments are used as this is similar to the JA3 output.
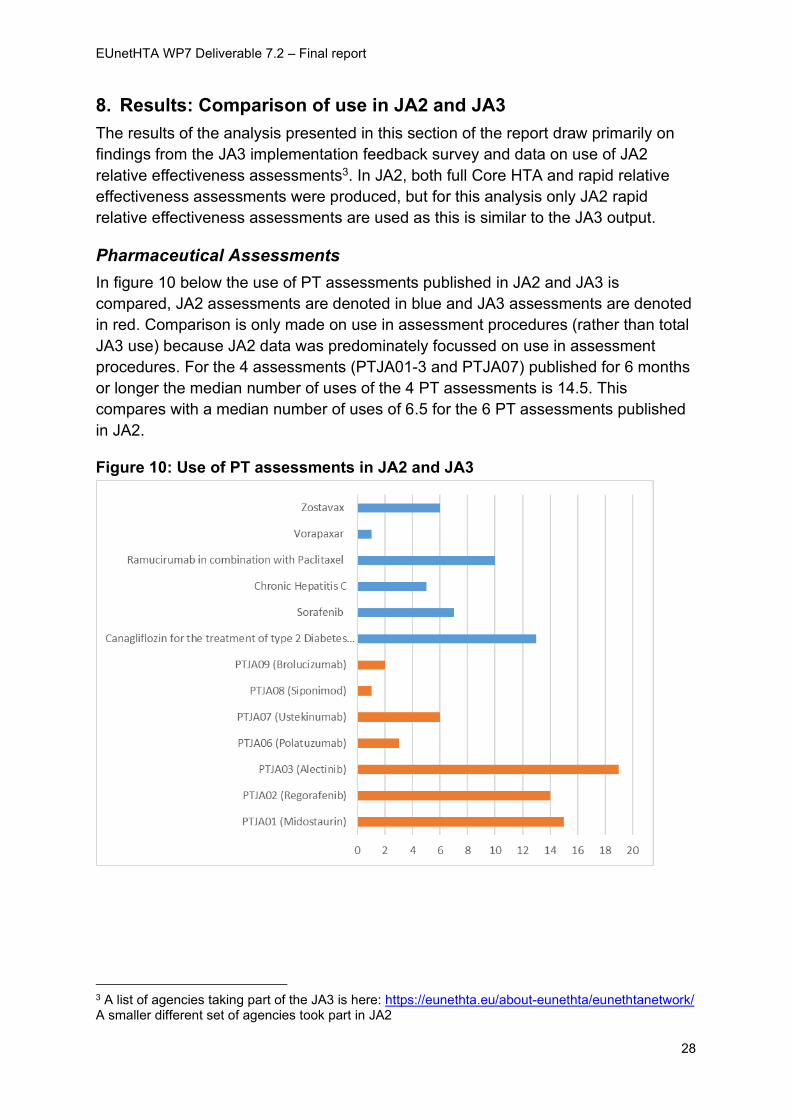
Pharmaceutical Assessments
In figure 10 below the use of PT assessments published in JA2 and JA3 is
compared, JA2 assessments are denoted in blue and JA3 assessments are denoted
in red. Comparison is only made on use in assessment procedures (rather than total
JA3 use) because JA2 data was predominately focussed on use in assessment
procedures. For the 4 assessments (PTJA01-3 and PTJA07) published for 6 months
or longer the median number of uses of the 4 PT assessments is 14.5. This
compares with a median number of uses of 6.5 for the 6 PT assessments published
in JA2.
Figure 10: Use of PT assessments in JA2 and JA3
3 A list of agencies taking part of the JA3 is here: https://eunethta.eu/about-eunethta/eunethtanetwork/ A smaller different set of agencies took part in JA2
EUnetHTA WP7 Deliverable 7.2 – Final report
29
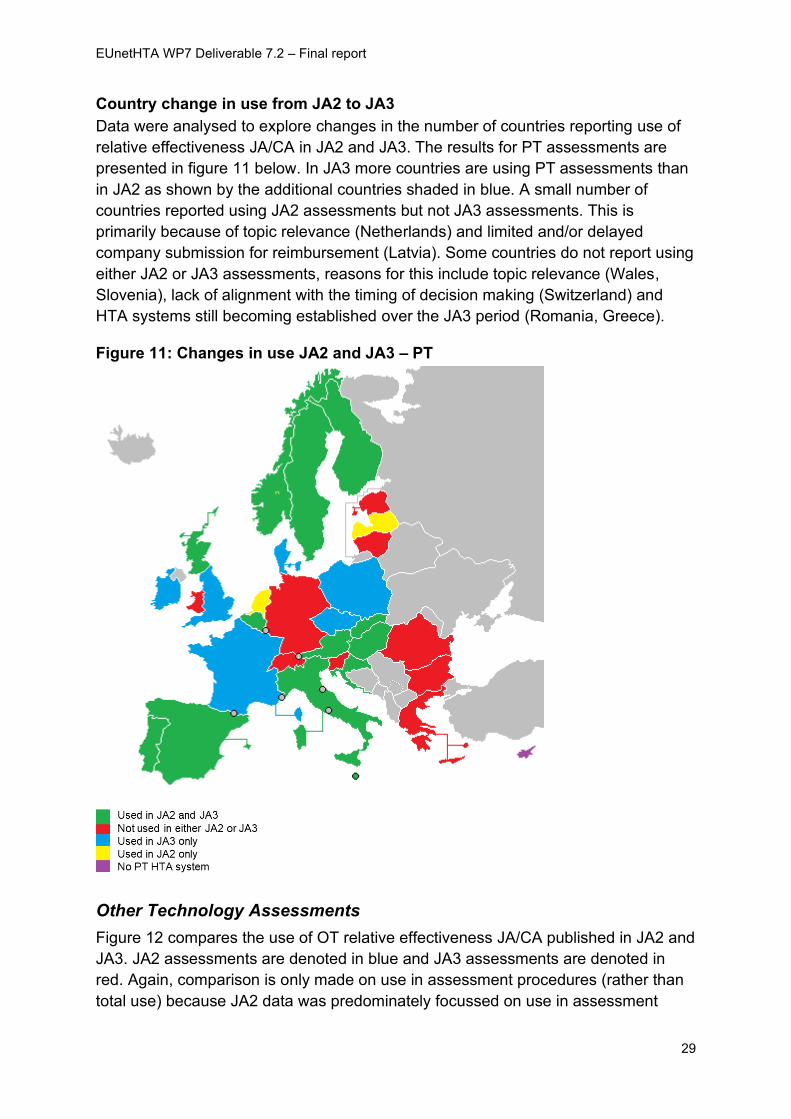
Country change in use from JA2 to JA3
Data were analysed to explore changes in the number of countries reporting use of
relative effectiveness JA/CA in JA2 and JA3. The results for PT assessments are
presented in figure 11 below. In JA3 more countries are using PT assessments than
in JA2 as shown by the additional countries shaded in blue. A small number of
countries reported using JA2 assessments but not JA3 assessments. This is
primarily because of topic relevance (Netherlands) and limited and/or delayed
company submission for reimbursement (Latvia). Some countries do not report using
either JA2 or JA3 assessments, reasons for this include topic relevance (Wales,
Slovenia), lack of alignment with the timing of decision making (Switzerland) and
HTA systems still becoming established over the JA3 period (Romania, Greece).
Figure 11: Changes in use JA2 and JA3 – PT
Other Technology Assessments
Figure 12 compares the use of OT relative effectiveness JA/CA published in JA2 and
JA3. JA2 assessments are denoted in blue and JA3 assessments are denoted in
red. Again, comparison is only made on use in assessment procedures (rather than
total use) because JA2 data was predominately focussed on use in assessment
EUnetHTA WP7 Deliverable 7.2 – Final report
30
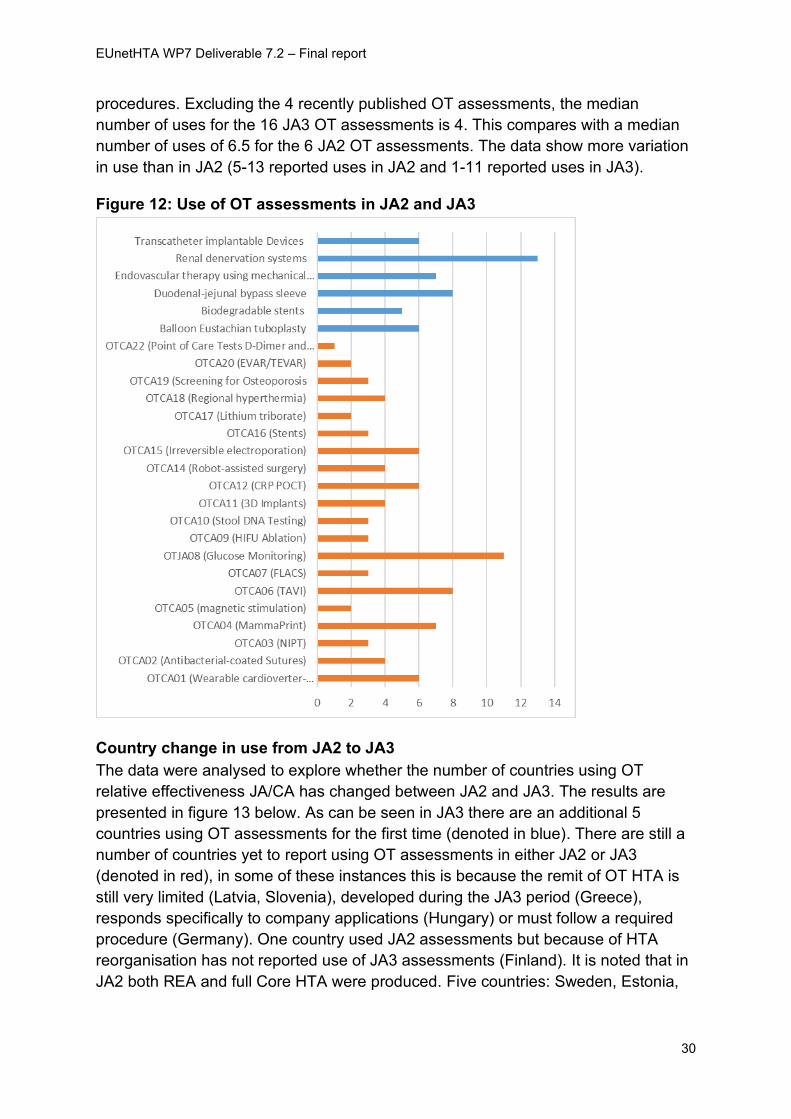
procedures. Excluding the 4 recently published OT assessments, the median
number of uses for the 16 JA3 OT assessments is 4. This compares with a median
number of uses of 6.5 for the 6 JA2 OT assessments. The data show more variation
in use than in JA2 (5-13 reported uses in JA2 and 1-11 reported uses in JA3).
Figure 12: Use of OT assessments in JA2 and JA3
Country change in use from JA2 to JA3
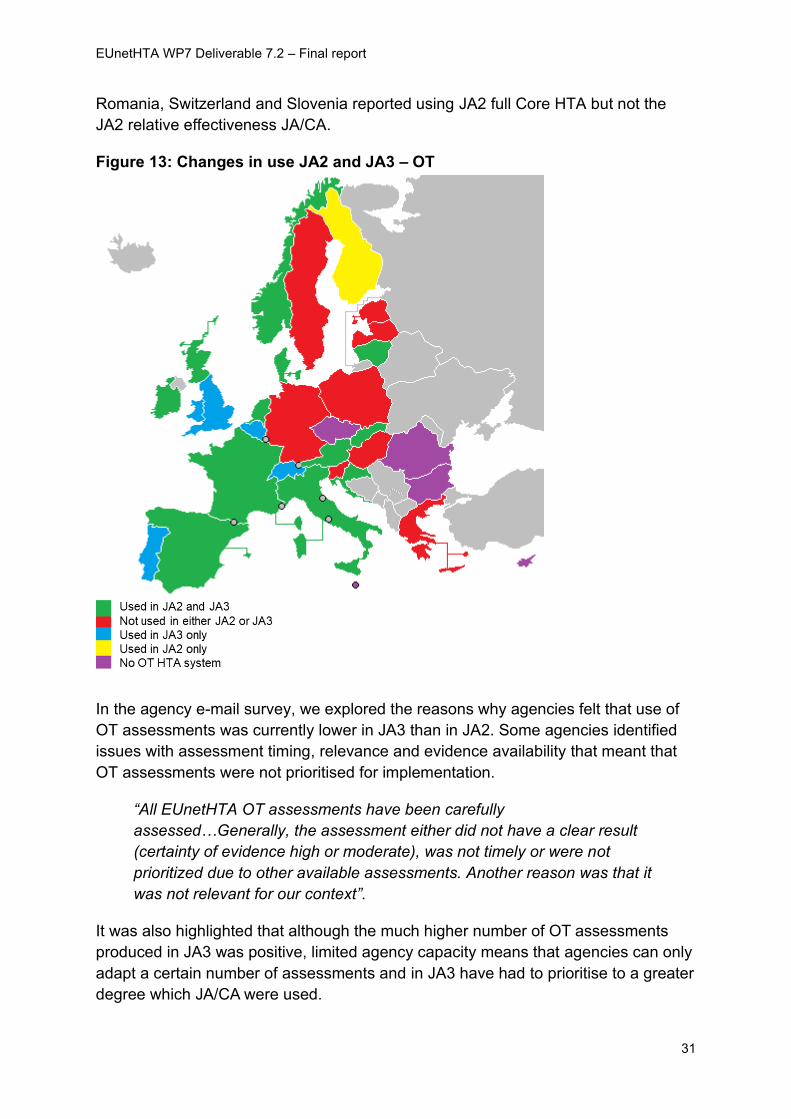
The data were analysed to explore whether the number of countries using OT
relative effectiveness JA/CA has changed between JA2 and JA3. The results are
presented in figure 13 below. As can be seen in JA3 there are an additional 5
countries using OT assessments for the first time (denoted in blue). There are still a
number of countries yet to report using OT assessments in either JA2 or JA3
(denoted in red), in some of these instances this is because the remit of OT HTA is
still very limited (Latvia, Slovenia), developed during the JA3 period (Greece),
responds specifically to company applications (Hungary) or must follow a required
procedure (Germany). One country used JA2 assessments but because of HTA
reorganisation has not reported use of JA3 assessments (Finland). It is noted that in
JA2 both REA and full Core HTA were produced. Five countries: Sweden, Estonia,
EUnetHTA WP7 Deliverable 7.2 – Final report
31
Romania, Switzerland and Slovenia reported using JA2 full Core HTA but not the
JA2 relative effectiveness JA/CA.
Figure 13: Changes in use JA2 and JA3 – OT
In the agency e-mail survey, we explored the reasons why agencies felt that use of
OT assessments was currently lower in JA3 than in JA2. Some agencies identified
issues with assessment timing, relevance and evidence availability that meant that
OT assessments were not prioritised for implementation.
“All EUnetHTA OT assessments have been carefully
assessed…Generally, the assessment either did not have a clear result
(certainty of evidence high or moderate), was not timely or were not
prioritized due to other available assessments. Another reason was that it
was not relevant for our context”.
It was also highlighted that although the much higher number of OT assessments
produced in JA3 was positive, limited agency capacity means that agencies can only
adapt a certain number of assessments and in JA3 have had to prioritise to a greater
degree which JA/CA were used.
EUnetHTA WP7 Deliverable 7.2 – Final report
32
“We do not have the resources to make use of all the produced EUnetHTA
assessments, which means that we have to prioritise in relation to the
relevance to our context”
Other agencies reflected that their low use of OT assessments arose from the fact
that their own OT HTA processes were still developing:
“The OT assessment process is under improvement in our Agency”.
In addition, it was noted that for some countries the recipient of an OT assessment
was not always very clear which affected the ability to use:
“The processes in the pharmaceutical field are more established. For
example, there has been a clear recipient of PT assessments, as opposed
to OT assessments”.
Other agencies noted environmental factors and the challenges that arise because
there is no regulatory timetable for other technologies:
“PT assessments are linked to the regulatory timetable and are on
products that are expected to be evaluated by all or most agencies….
Other technologies have their own unpredictable way and timing of
coming to the attention of decision makers”
And other agencies noted there may simply have not yet been sufficient follow-up:
“this could be due to several reasons: 1) Assessments from JA2 are done
a long time ago, so HTA agencies have an opportunity to use them longer;
2). It takes a while for a technology to come into some small countries and
into their reimbursement systems, so maybe older technologies currently
became more relevant for some parts of Europe”.
Conclusions
• For PT there has been increased production and use of JA/CA in JA3
compared to JA2
• For OT there has been increased production of JA/CA, but there is currently
less use of JA/CA in JA3 compared to JA2, reasons for low uptake of OT
assessments include:
o Limited agency capacity and increased output in JA3 means agencies
have had to prioritise which JA/CA they use
o The characteristics of access to OT across Europe means that OT can
be introduced and come to the attention of decision makers in different
countries at very different time points
EUnetHTA WP7 Deliverable 7.2 – Final report
33
o OT HTA processes are not fully established in some countries and the
process of linking OT HTA to decision making often less clear than for
pharmaceuticals
o Short follow up time for some JA/CA
• For both PT and OT there is an increased number of countries that have used
JA/CA in JA3 compared to JA2
EUnetHTA WP7 Deliverable 7.2 – Final report
34
9. Relationship between participation and implementation
In this section we explore the influence that participation in previous joint actions and
in JA3 assessment procedures has had on implementation.
A much larger number of agencies have been involved in EUnetHTA JA3 than were
involved in JA2. Summarising the possible reasons for increased uptake of PT
assessments in JA3, one agency commented that they felt that the increase in the
number of PT agencies participating in JA3 positively contributes to PT
implementation.
“Timeliness, increased awareness of the product and EUnetHTA
collaboration, relevance of the topics, higher number of published JAs,
easy access, publicity, involvement of many HTA [agencies] as partners in
EUnetHTA”.
In addition, several agencies highlighted the positive role that participation in JA/CA
processes and activities have on uptake:
“[the agency] became an active member in the Assessments (as a DR,
co-author and author) and more involved in the different EUnetHTA
working parties”
Other technologies
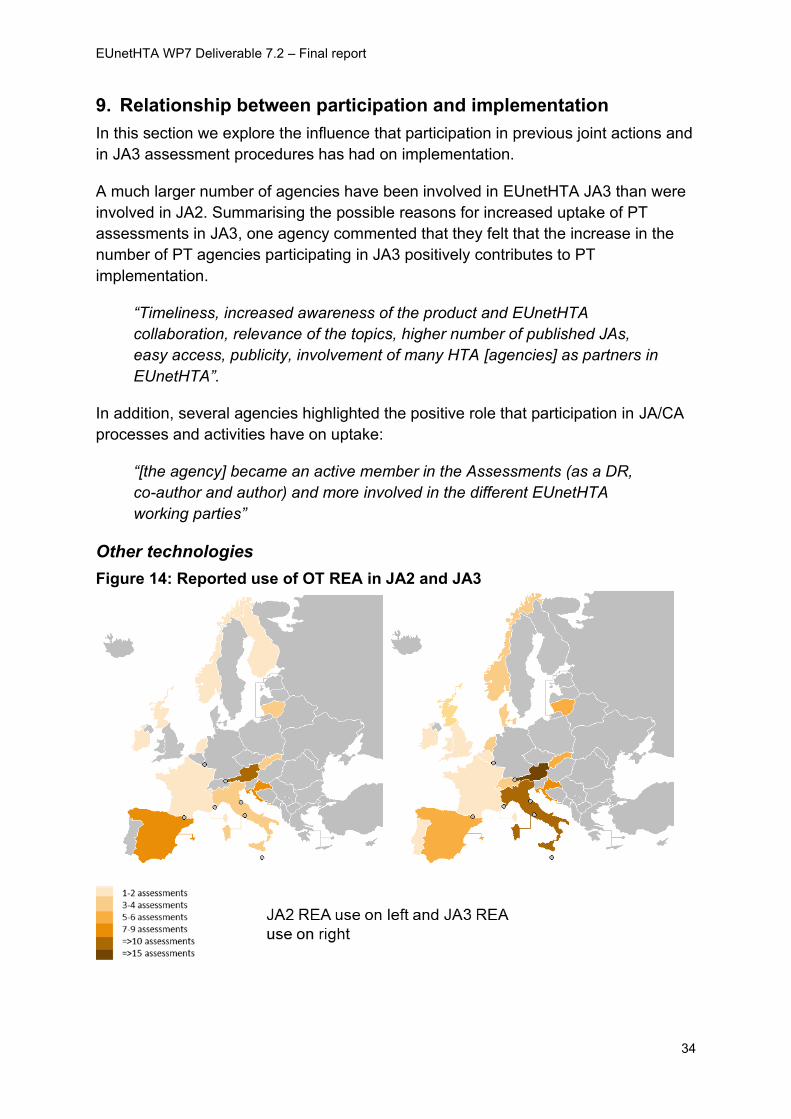
Figure 14: Reported use of OT REA in JA2 and JA3
EUnetHTA WP7 Deliverable 7.2 – Final report
35
Figure 14 above shows the reported use of JA2 OT REA and JA3 OT REA. Darker
shades indicate more reported use. The figures are in broad alignment. Countries
who reported using more JA2 REA assessments also report using most JA3 REA
assessments.
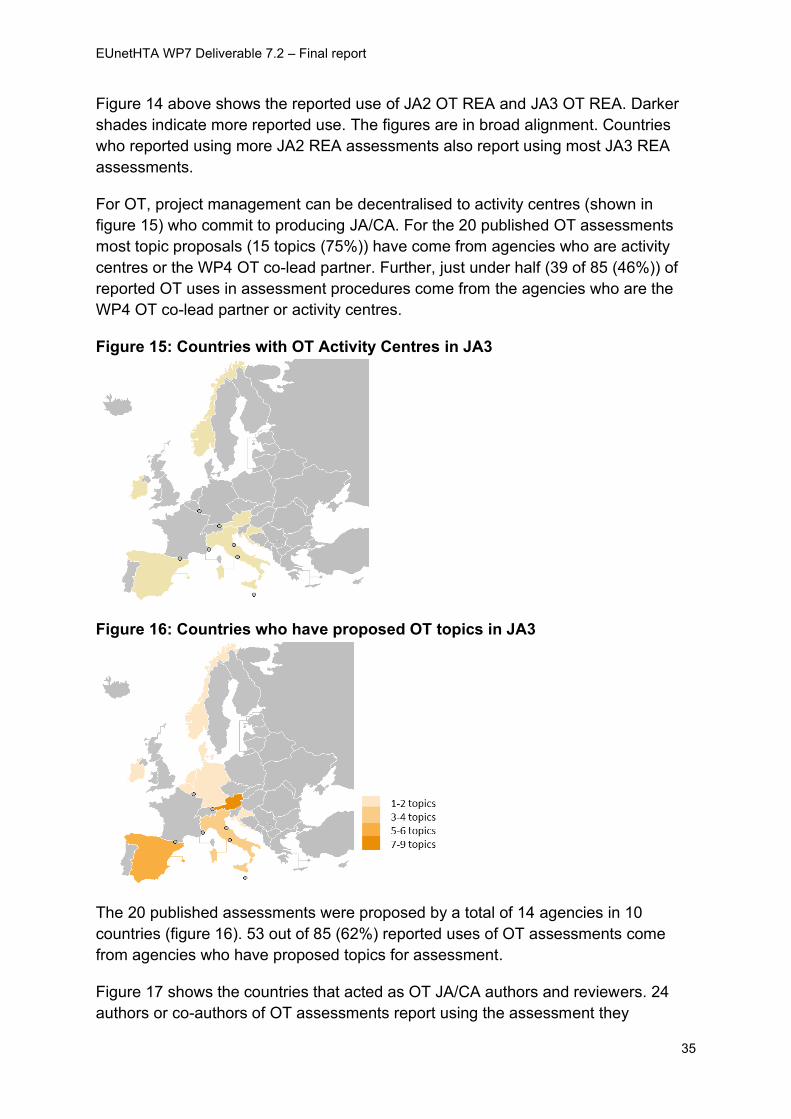
For OT, project management can be decentralised to activity centres (shown in
figure 15) who commit to producing JA/CA. For the 20 published OT assessments
most topic proposals (15 topics (75%)) have come from agencies who are activity
centres or the WP4 OT co-lead partner. Further, just under half (39 of 85 (46%)) of
reported OT uses in assessment procedures come from the agencies who are the
WP4 OT co-lead partner or activity centres.
Figure 15: Countries with OT Activity Centres in JA3
Figure 16: Countries who have proposed OT topics in JA3
The 20 published assessments were proposed by a total of 14 agencies in 10
countries (figure 16). 53 out of 85 (62%) reported uses of OT assessments come
from agencies who have proposed topics for assessment.
Figure 17 shows the countries that acted as OT JA/CA authors and reviewers. 24
authors or co-authors of OT assessments report using the assessment they
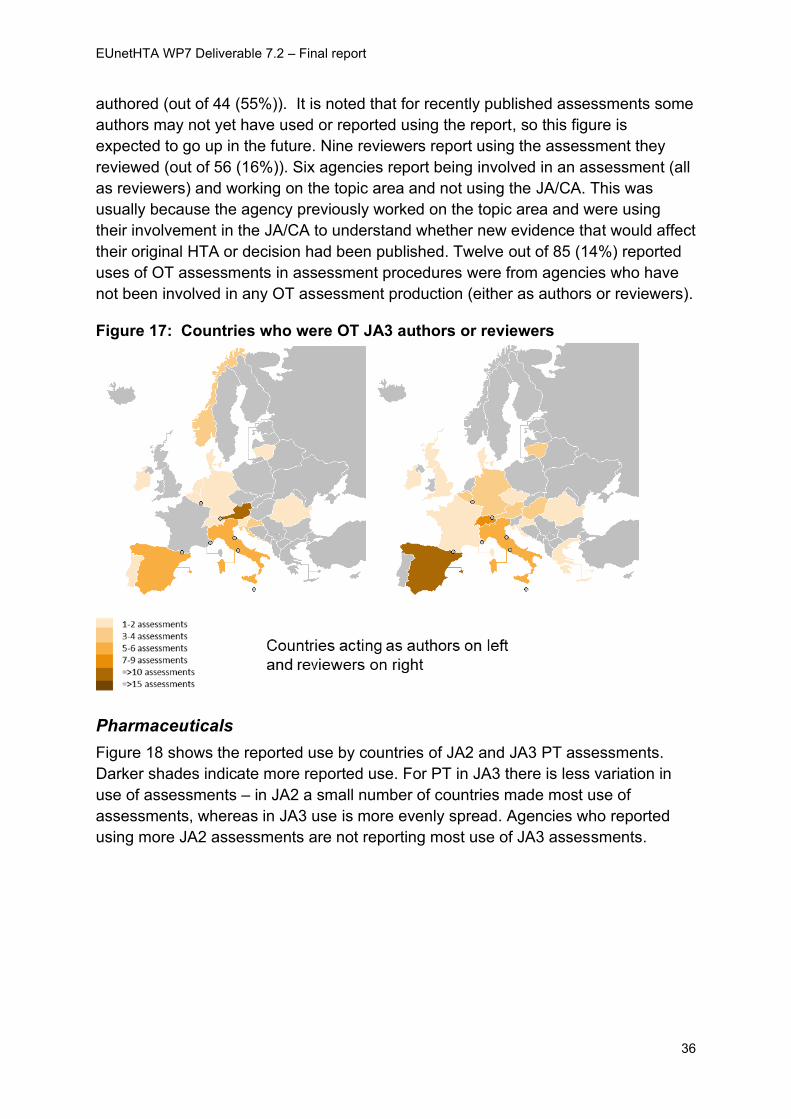
EUnetHTA WP7 Deliverable 7.2 – Final report
36
authored (out of 44 (55%)). It is noted that for recently published assessments some
authors may not yet have used or reported using the report, so this figure is
expected to go up in the future. Nine reviewers report using the assessment they
reviewed (out of 56 (16%)). Six agencies report being involved in an assessment (all
as reviewers) and working on the topic area and not using the JA/CA. This was
usually because the agency previously worked on the topic area and were using
their involvement in the JA/CA to understand whether new evidence that would affect
their original HTA or decision had been published. Twelve out of 85 (14%) reported
uses of OT assessments in assessment procedures were from agencies who have
not been involved in any OT assessment production (either as authors or reviewers).
Figure 17: Countries who were OT JA3 authors or reviewers
Pharmaceuticals
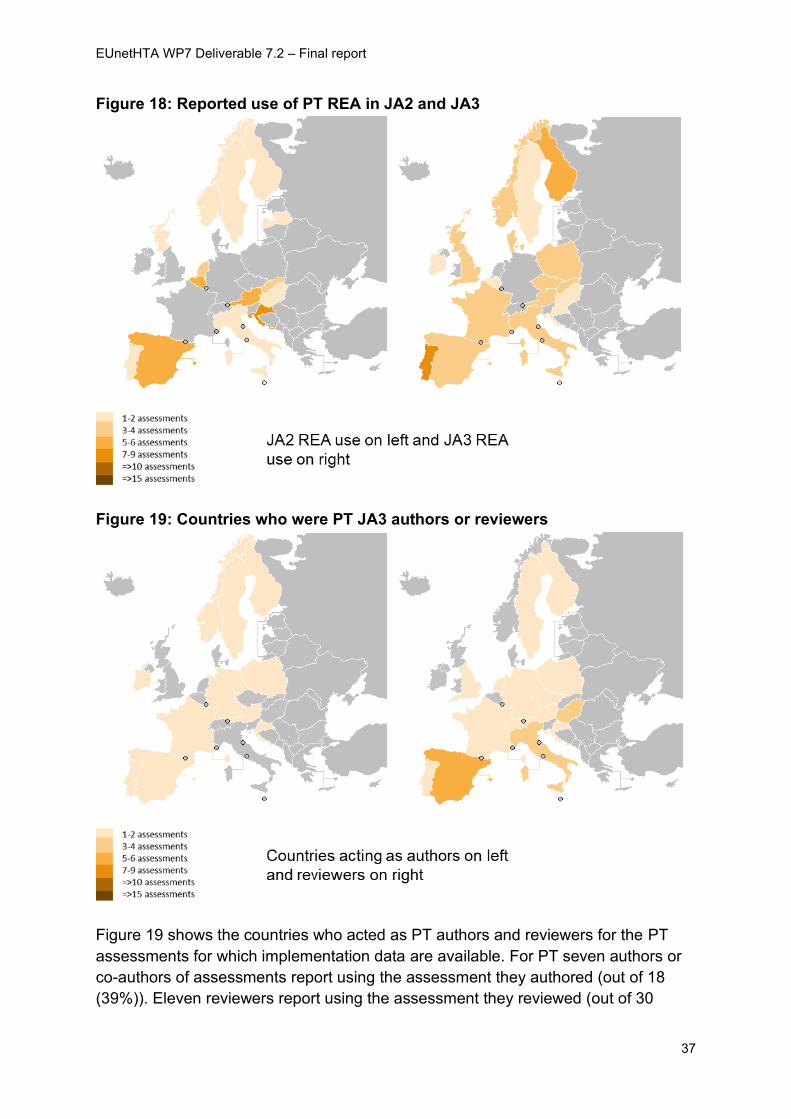
Figure 18 shows the reported use by countries of JA2 and JA3 PT assessments.
Darker shades indicate more reported use. For PT in JA3 there is less variation in
use of assessments – in JA2 a small number of countries made most use of
assessments, whereas in JA3 use is more evenly spread. Agencies who reported
using more JA2 assessments are not reporting most use of JA3 assessments.
EUnetHTA WP7 Deliverable 7.2 – Final report
37
Figure 18: Reported use of PT REA in JA2 and JA3
Figure 19: Countries who were PT JA3 authors or reviewers
Figure 19 shows the countries who acted as PT authors and reviewers for the PT
assessments for which implementation data are available. For PT seven authors or
co-authors of assessments report using the assessment they authored (out of 18
(39%)). Eleven reviewers report using the assessment they reviewed (out of 30
EUnetHTA WP7 Deliverable 7.2 – Final report
38
(37%)). It is noted that for recently published assessments some authors and
reviewers may not yet have received company applications for reimbursement, so
this figure is expected to go up in the future. Only 1 agency reports being involved in
an assessment (as a reviewer) and working on the topic area and not using the
JA/CA (reason given timing – JA/CA was not available at the time of agency
assessment). Where authors or reviewers have not used the JA/CA reasons for this
include:
• the topic was not subsequently prioritised for HTA
• the topic was found to be in the remit of an alternative agency in the country
• the company has not (yet) asked the agency to assess the product at the time
of the cut-off date for this analysis.
Eleven out of 60 (18%) reported uses of PT assessments in assessment procedures
come from agencies (n=4) who have not been involved in any PT assessment
production (either as authors or reviewers).
Conclusions
• Engagement of a larger number of agencies in JA3 compared with JA2 is seen to
have positively influenced awareness and uptake
• Participation in production processes is seen to support subsequent uptake.
• OT agencies who reported more use of JA2 REA assessments are also more
likely to report higher use of JA3 REA assessments. For PT reported use in JA2
appears to be less related to reported use in JA3.
• The model of topic identification and selection used in OT supports use of
assessments by activity centres, authors and co-authors, but appears less
successful at consistently identifying topics that also gather significant use from
agencies acting as reviewers and agencies outside of the assessment team.
• Involvement in PT assessments is less related to uptake than OT involvement,
this is because the PT assessment team is identified before an agency knows
whether a company will apply for reimbursement in their country and therefore
whether they will need to carry out HTA.
EUnetHTA WP7 Deliverable 7.2 – Final report
39
10. Results: Awareness
Fitness for purpose of procedures
Figure 20: Countries reporting awareness as a limiting or preventing factor
Table 7: Limiting and Preventing factors reported about awareness
Prevented use Limited use Total
PT OT PT OT
Not aware of the assessment being produced
1 0 2 0 3
Number of agencies reporting
The data in figure 20 and table 7 do not show issues reported about JA/CA
awareness in JA3. The challenges reported are for PT assessments and in two
cases are reported by an agency who is not a EUnetHTA partner and so has access
to fewer communication channels and alert systems than other agencies.
Agency perceptions of changes introduced in JA3
During JA3 EUnetHTA has made the following changes to its procedures to improve
partner awareness of JA/CA:
• Publication of the project plan at CHMP opinion (PT)
• Publication of the project plan as soon as it is final (OT)
EUnetHTA WP7 Deliverable 7.2 – Final report
40
• Alerts for JA/CA starting and publication of project plans and assessments (PT
and OT)
Most agencies interviewed were aware of these procedural changes to improve
awareness of JA/CA.
The earlier publication of the project plan was felt to be helpful for PT and OT
assessments and expected to improve use in the future. The notification systems
and publicity of assessments in JA3 was considered to have improved compared
with JA2 and generally felt to have improved awareness of JA/CA and uptake in JA3.
The recent introduction of a monthly newsletter by WP4 for PT assessments was
identified as being particularly helpful.
“Better information about the timelines for planned and ongoing
assessments”.
Agency recommendations for the future
A need for further improvements to internal communication with partners was
highlighted. An extension of the PT newsletter to OT would be welcomed. In
addition, the following areas were mentioned:
• Regular and routine updates of distribution lists (as staff turnover is high in many
agencies)
• Enhanced use of e-mails and social media (felt to be particularly important given
varying levels of use of the intranet in different agencies)
• The list of assessments on the intranet and internet should list the phase
and timescales of each assessment stage e.g. scoping, assessment.
Agencies reporting higher use of JA/CA were able to add JA/CA topics into agency
topic selection processes and were able to take topics from their agency topic
selection processes and put them into JA/CA topic selection processes.
“The basic reason [for our increased use] is that EUnetHTA topics have
been included as part of the list of topics to be prioritized by the Ministry of
Health. If they are selected, they are included as part of the Work Plan for
translation/adaption”.
“Now we are better in coordinating proposals of topics relevant to our
Commissioning Forum with selection/suggestions of topics in JA3”
This level of awareness of JA/CA with commissioners and decision makers outside
of partner organisations is still being put in place in some countries.
EUnetHTA WP7 Deliverable 7.2 – Final report
41
“in the future, [agency] aims to notify health insurance companies about
the EUnetHTA reports if we do not have the topic on our internal agenda”
“OT assessments could also be relevant for the regions. We are in contact
with the regions in order to increase awareness of the EUnetHTA reports”.
While some awareness raising activities must be undertaken at an agency or country
level, it was also suggested that EUnetHTA could do more to raise awareness in
other organisations and networks, for example support for JA/CA could be improved
by engaging more with Cochrane Groups and the Guidelines International Network
to develop strategic relations and build relationships:
“what I am missing in this discussion is the possibility to strengthen the
support for EUnetHTA products and processes by reaching out to two
particular communities: Cochrane and Guidelines International Network,
both doing assessments often on the very same topic”.
There was agreement that at an agency level inclusion of the reuse of JA/CA in
agency SOPs and procedures is imperative if joint work is to be properly embedded.
“Key first area is to have procedures in place to support
inclusion…important to embed this infrastructure”.
“It is important that this is noted down in national procedures, so that it is
not only dependent on EUnetHTA “ambassadors”
“We have developed a standardised way of using the assessments as
well, which has also made it easier to use the assessments”.
Conclusions
• A lack of awareness of JA/CA among HTA users is not a key factor preventing or
limiting use of JA/CA.
• The following changes to notification systems have been positively received:
o More alerts for planned, ongoing and published assessments
o Earlier publication of OT and PT project plans
• Agencies recommend:
o The implementation of a robust information and communication system
o Internal communication mechanisms that use a wide variety of channels
without relying on any single channel
o Contacts lists require regular updating because of staff turnover

EUnetHTA WP7 Deliverable 7.2 – Final report
42
o Extension of the PT newsletter to OT
o Greater dissemination to and collaboration with people, groups and
organisations who are not part of the network or not directly involved in the
production work
o Formal inclusion in agency procedures of an alert to check for ongoing or
published relevant joint work to support improved awareness of JA/CA
across agency staff not directly connected to EUnetHTA
o Agency communication strategies to ensure relevant HTA users and
commissioners in a country are aware of JA/CA
EUnetHTA WP7 Deliverable 7.2 – Final report
43
11. Results: Timing
Fitness for purpose of procedures
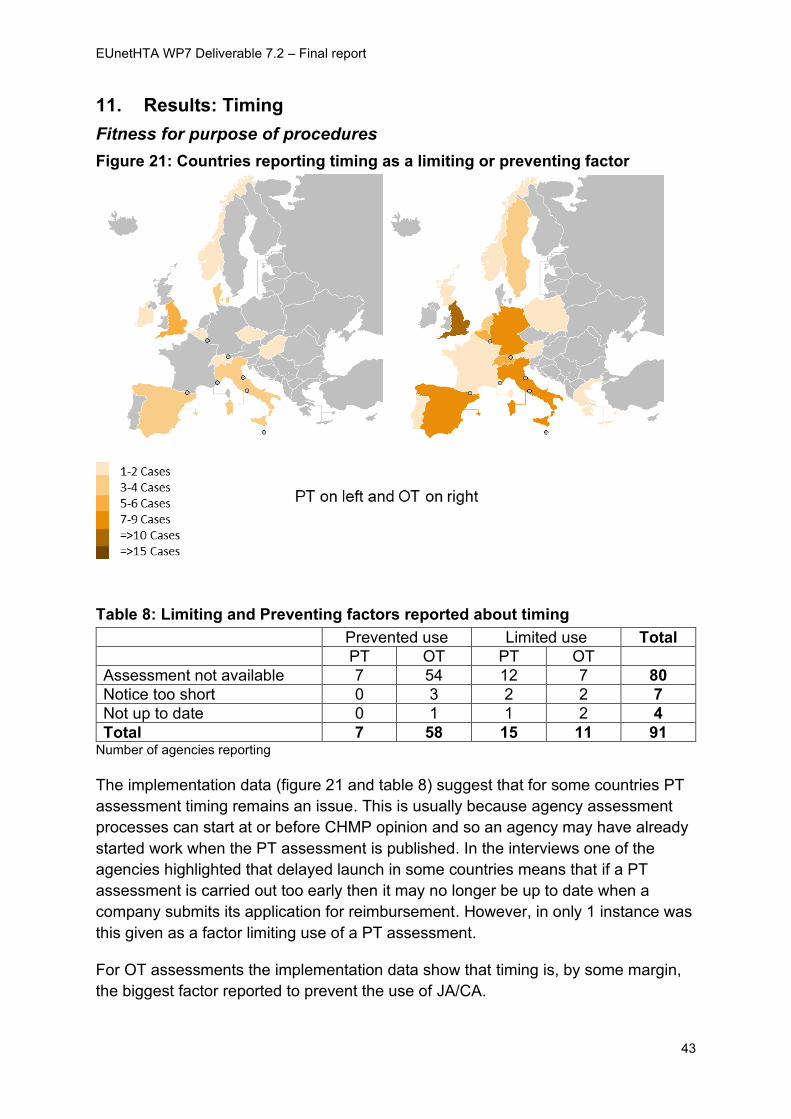
Figure 21: Countries reporting timing as a limiting or preventing factor
Table 8: Limiting and Preventing factors reported about timing
Prevented use Limited use Total
PT OT PT OT
Assessment not available 7 54 12 7 80
Notice too short 0 3 2 2 7
Not up to date 0 1 1 2 4
Total 7 58 15 11 91 Number of agencies reporting
The implementation data (figure 21 and table 8) suggest that for some countries PT
assessment timing remains an issue. This is usually because agency assessment
processes can start at or before CHMP opinion and so an agency may have already
started work when the PT assessment is published. In the interviews one of the
agencies highlighted that delayed launch in some countries means that if a PT
assessment is carried out too early then it may no longer be up to date when a
company submits its application for reimbursement. However, in only 1 instance was
this given as a factor limiting use of a PT assessment.
For OT assessments the implementation data show that timing is, by some margin,
the biggest factor reported to prevent the use of JA/CA.
EUnetHTA WP7 Deliverable 7.2 – Final report
44
It was noted that in countries with later adoption of an OT having a JA/CA is of value
and can be used even if it needs updating, although opposite views were expressed
as to how resource intensive updating is:
“when the topic actually crops up at the national level, a OT assessment is
extremely useful, even though it has become out of date, because update
is generally quite quick and a lot of background work has already been
done, saving time and resources”
“if use EUnetHTA assessment and it is 6 months old you then have to
update on searches etc.so whilst you cut down work you won’t eliminate it
or replace work.”
However, the key barrier for OT timing was when agency work had already taken
place before the JA/CA became available, in some cases some years before
EUnetHTA produced their assessment.
“Some reports were in principle useable but too late”.
Agency perceptions of changes introduced in JA3
The main procedural change made by EUnetHTA in respect of timeliness for PT
assessments were changes made at the start of JA3 allowing the publication of PT
assessments closer to marketing authorisation.
All agencies interviewed viewed changes to PT timing as either positive or neutral in
supporting them to use PT assessments. Among respondents the main reason for
increased use of JA3 assessments compared to JA2 assessments was identified to
be improved timing, assessments often came too late in JA2.
“Timing – all reports are published close to EPAR which is in line with our
national procedure”.
“The key reason for the change [in use of assessments] is timing. PT
EUnetHTA assessments in JA3 have been available at the time [agency]
receive a submission”.
The main procedural change made by EUnetHTA in respect of timelines for OT
assessments was the sharing of draft assessments. In September 2019 it was
approved that draft assessments would be shared with partners outside of the
assessment teams, with this to become operational from OTCA23 onwards.
A number of agencies interviewed were not aware of this change and because the
change has yet to be implemented agencies were unable to comment definitively on
the impact of the change, but many felt that it will be positive and will help agencies
to plan to use OT assessments.
EUnetHTA WP7 Deliverable 7.2 – Final report
45
“It will be really helpful to support early adaptation work and plan at an
earlier point to plan and determine whether they will use the assessment
nationally”.
Agency recommendations for the future
To further improve the timeliness of PT assessments it was suggested that agencies
could benefit by having the PICO made available to them earlier, rather than an at
CHMP opinion as currently. It was suggested that it may be possible to achieve this
through making the PICO available internally to partners on the intranet and not
publicly on the internet.
Whilst the findings from the interviews confirmed OT timing as a key barrier to use,
partners identified no obvious solutions to solve the challenge of timing. It is,
however, hoped and anticipated that going forward the new medical devices
regulations in Europe will help to provide an anchor to ensure less spread out and
variable uptake across Europe for OT.
Conclusions
• Earlier publication of PT assessments close to marketing authorisation has
supported increased use of these assessments. However, for agencies who can
start work at CHMP opinion, timing of the joint PT assessment remains a limiting
factor in the ability to use EUnetHTA assessments.
• There are ongoing challenges to identify the best possible timing to carry out OT
assessments so they are of value to the largest number of agencies. It is hoped
that EU MD regulations will help create an anchor that will allow for greater
alignment of timing of OT HTA across Europe.
• Early sharing of information about PICO and draft assessments supports better
planning and use of JA/CA. The improvements in JA3 are welcomed, but
partners suggest it would be helpful if more PICO information can be shared
earlier.
EUnetHTA WP7 Deliverable 7.2 – Final report
46
12. Results: Relevance and transferability
Fitness for purpose of procedures
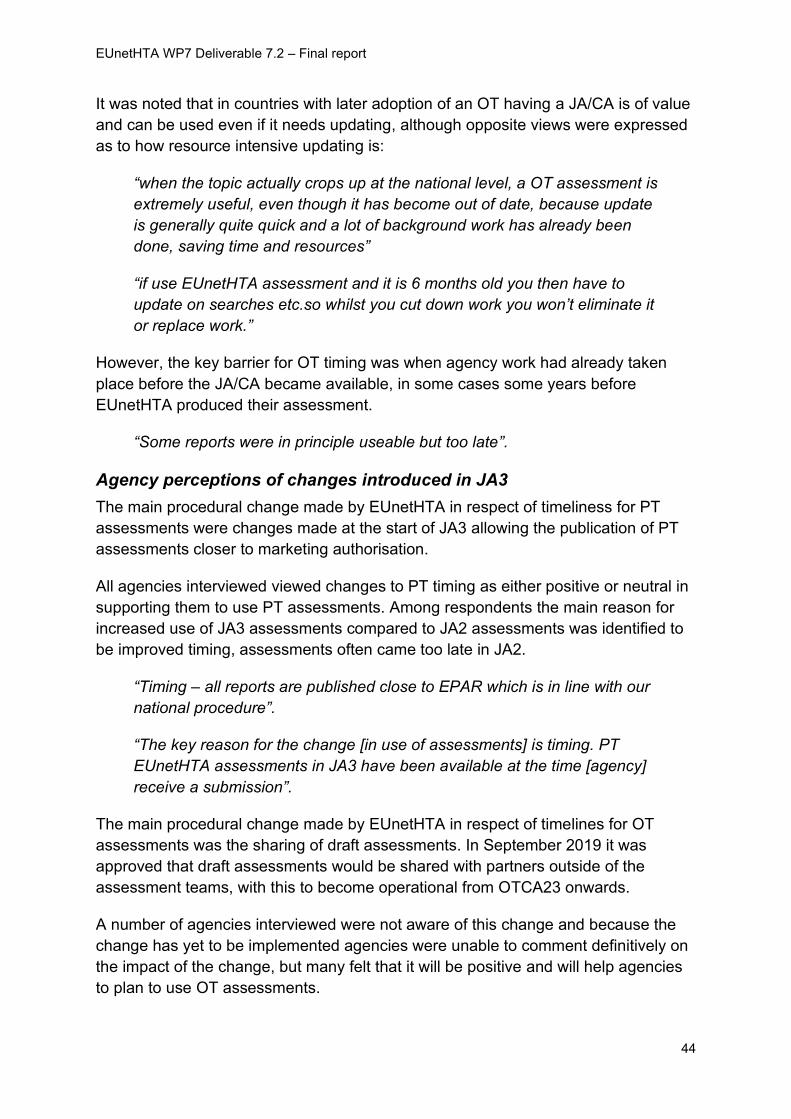
Figure 22: Countries reporting relevance as a limiting or preventing factor
Table 9: Limiting and Preventing factors reported about relevance
Prevented use Limited use Total
PT OT PT OT
Scope Relevance 4 7 7 11 29
Content Relevance 0 1 14 7 22
Transferability 0 0 1 2 3
Total 4 8 22 20 54 Number of agencies reporting
Respondents to the implementation feedback survey are asked if the following factors
either prevented or limited use of JA/CA.
• Differences in the scope of the JA/CA and agency assessment (“scope
relevance”)
• Differences in the content of the JA/CA and agency assessment (“content
relevance”)
Implementation data (figure 22 and table 9) show that relevance remains a key issue
limiting and preventing use of both PT and OT assessments.
The data show that a lack of alignment of the scope more often prevents use, but a
lack of alignment of content does not. For PT assessments fewer agencies report
EUnetHTA WP7 Deliverable 7.2 – Final report
47
issues with alignment of scope and more report issues with requiring different
content information. For OT assessments more users report issues with scope
relevance and fewer report issues with content alignment.
Issues of content alignment in PT arise in part from the use of economic information
in agency assessments and need to analyse clinical data to inform and interpret
economic analyses. In contrast, OT assessments have more heterogenous
objectives and PICOs which create more challenges with creating a European
scope. Giving reasons for non-use of OT assessments one agency commented:
“In some other cases the PICO was not in line according to ours (different
place of OT in the therapy, which we scope at the professional societies)”
The challenge of adaptation when there was a lack of alignment of scope was
illustrated by one agency:
“for those reports that were chosen to be adapted (which means not only
translated in their summaries and published on our websites) we usually
found that the PICOD did not fit our context (relevance) and in some
cases we needed to basically re-run literature searches, re-make
systematic reviews and rewrite CUR and TEC chapters”.
Agency perceptions of changes introduced in JA3
Several procedural changes have been implemented by EUnetHTA to improve the
relevance of PT assessments, including:
• Formal request to partners for interest in topic
• EUnetHTA prioritisation list (EPL) for topic selection
• PICO Survey
• Early access to confidential information in the draft regulatory assessment
report allowing citation of the CHMP assessment report in PT assessments
Most agencies were aware of these changes. Agencies identified PICO surveys as
being important in improving relevance and supporting engagement of agencies
early in the assessment process.
“PICO survey is very useful, and we always participate in this”.
“The PICO surveys were able to involve our Agency from the beginning of
the process”
However, not all agencies found taking part in the PICO survey easy:
EUnetHTA WP7 Deliverable 7.2 – Final report
48
“PICO surveys are difficult to answer as often the populations are more
limited / focussed to limit budget impact”.
“But difficult to input to the PICO at the stage it is undertaken – but have
tried to do so to ensure that the report is of relevance when it comes
through”.
The EUnetHTA prioritisation list (EPL) was also identified by PT users as being
helpful in improving relevance for some agencies. However, several agencies
commented that the prioritisation had little impact nationally either because they
assess all new medicines in that country or because the identification and selection
of topics is industry led.
For OT, the key procedural change implemented to improve the relevance of JA/CA
was the EUnetHTA Prioritisation List (EPL) for topic selection. This was published on
2nd July 2019 for OT.
Reactions to the OT EPL were mixed, some agencies considered that it had been
helpful for their own topic selection processes, but for the most part it was not
considered to have been very useful for OT assessments.
“Would be good to have a shorter more focussed prioritisation list that
gives more detail such as the PICO”.
“An administrative burden but of limited use for OT. As in most instances -
authors will only act as authors if they have been asked to review the topic
at a national level”.
“Helpful document and we shared it very widely but feedback now is that a
topic is prioritised but then it does not start, and we get questions as to
why”
Some agencies considered that a greater use of horizon scanning would help
better alignment of topics for JA/CA with agency priorities, while other agencies
proposed sharing lists of agency priorities before work had been started.
Agency recommendations for the future
For PT it was identified that the PICO survey has been particularly helpful in
improving relevance.
“Keep emphasis on PICO development (PICO survey and adherence to
PICO in report) to support relevance”
It was suggested that further work on the PICO would be helpful to establish who
defines the PICO in different partner countries and that the PICO survey should be
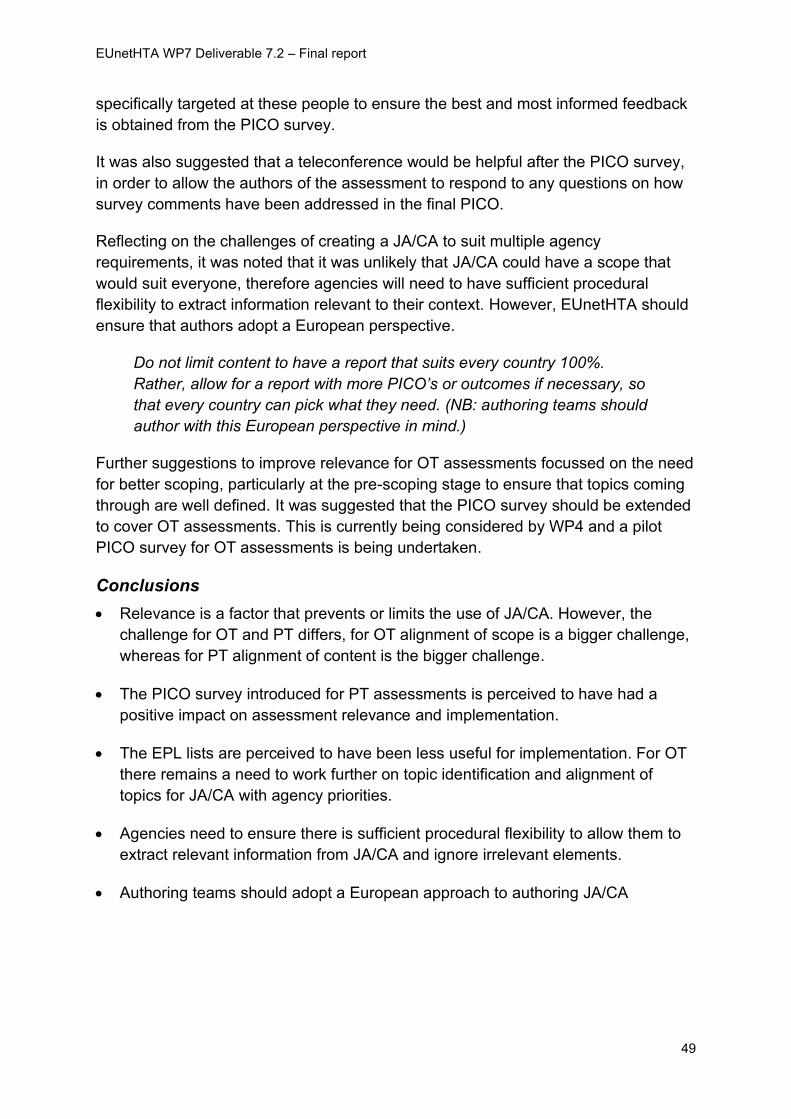
EUnetHTA WP7 Deliverable 7.2 – Final report
49
specifically targeted at these people to ensure the best and most informed feedback
is obtained from the PICO survey.
It was also suggested that a teleconference would be helpful after the PICO survey,
in order to allow the authors of the assessment to respond to any questions on how
survey comments have been addressed in the final PICO.
Reflecting on the challenges of creating a JA/CA to suit multiple agency
requirements, it was noted that it was unlikely that JA/CA could have a scope that
would suit everyone, therefore agencies will need to have sufficient procedural
flexibility to extract information relevant to their context. However, EUnetHTA should
ensure that authors adopt a European perspective.
Do not limit content to have a report that suits every country 100%.
Rather, allow for a report with more PICO’s or outcomes if necessary, so
that every country can pick what they need. (NB: authoring teams should
author with this European perspective in mind.)
Further suggestions to improve relevance for OT assessments focussed on the need
for better scoping, particularly at the pre-scoping stage to ensure that topics coming
through are well defined. It was suggested that the PICO survey should be extended
to cover OT assessments. This is currently being considered by WP4 and a pilot
PICO survey for OT assessments is being undertaken.
Conclusions
• Relevance is a factor that prevents or limits the use of JA/CA. However, the
challenge for OT and PT differs, for OT alignment of scope is a bigger challenge,
whereas for PT alignment of content is the bigger challenge.
• The PICO survey introduced for PT assessments is perceived to have had a
positive impact on assessment relevance and implementation.
• The EPL lists are perceived to have been less useful for implementation. For OT
there remains a need to work further on topic identification and alignment of
topics for JA/CA with agency priorities.
• Agencies need to ensure there is sufficient procedural flexibility to allow them to
extract relevant information from JA/CA and ignore irrelevant elements.
• Authoring teams should adopt a European approach to authoring JA/CA
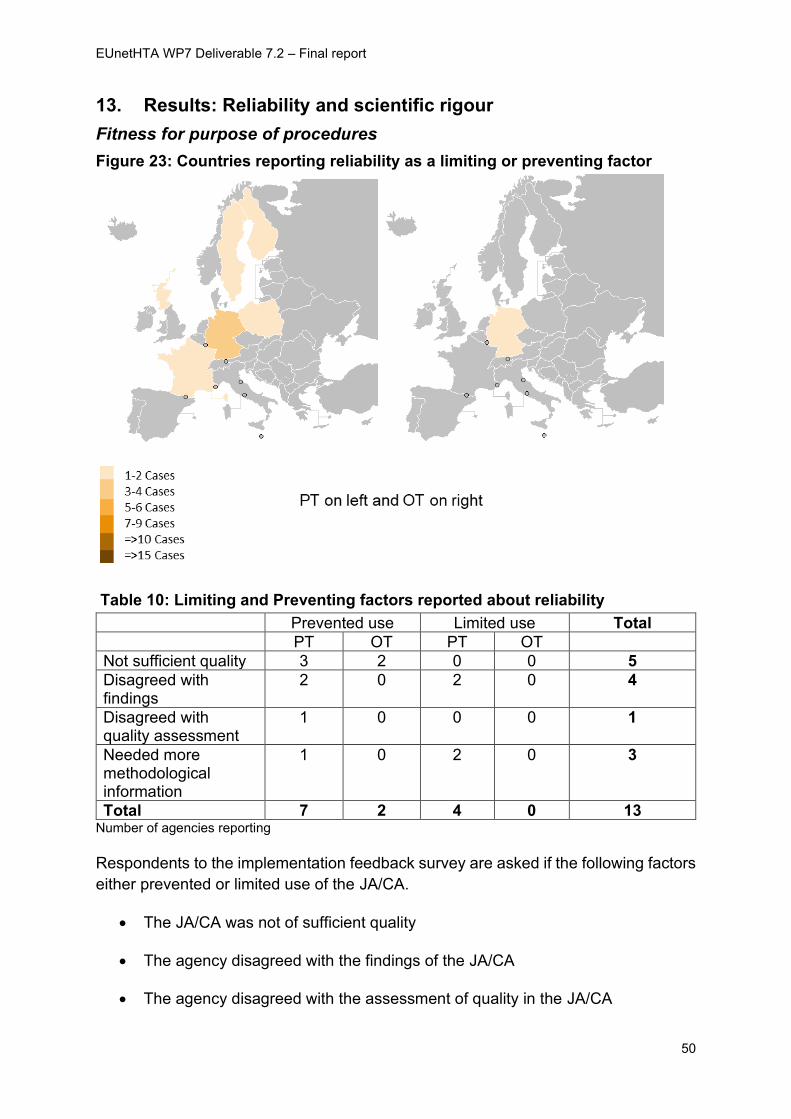
EUnetHTA WP7 Deliverable 7.2 – Final report
50
13. Results: Reliability and scientific rigour
Fitness for purpose of procedures
Figure 23: Countries reporting reliability as a limiting or preventing factor
Table 10: Limiting and Preventing factors reported about reliability
Prevented use Limited use Total
PT OT PT OT
Not sufficient quality 3 2 0 0 5
Disagreed with findings
2 0 2 0 4
Disagreed with quality assessment
1 0 0 0 1
Needed more methodological information
1 0 2 0 3
Total 7 2 4 0 13 Number of agencies reporting
Respondents to the implementation feedback survey are asked if the following factors
either prevented or limited use of the JA/CA.
• The JA/CA was not of sufficient quality
• The agency disagreed with the findings of the JA/CA
• The agency disagreed with the assessment of quality in the JA/CA
EUnetHTA WP7 Deliverable 7.2 – Final report
51
• The agency needed more methodological information to make a judgement
about quality
The data (figure 23 and table 10) show that factors relating to reliability are more
apparent for PT assessments than for OT assessments, and most often prevent use.
No single reliability factor is identified as a bigger issue than the others.
In general, the data show that the scientific rigour of JA/CA was felt to be fit for
purpose, though one agency commented that quality of OT assessments was
variable. In addition, quality remains an important factor limiting use of assessments
in a small number of locations:
“agency has not used the EUnetHTA PT assessment reports….as they
did not meet the requirements of transparency, standardization,
completeness, independence and methodological quality which are
prerequisites for the use in our country”.
Agency perceptions of changes introduced in JA3
The procedural changes made to improve scientific rigour were common across PT
and OT assessments and were:
• Implementation of the Companion Guide
• Submission requirements documents
• Optional factual accuracy checks
In JA3 EUnetHTA has implemented a quality management system through the
Companion Guide to support production of JA/CA. The Companion Guide was
largely viewed positively for both PT and OT, but agencies were equivocal about
whether it has or will improve implementation of assessments. One agency viewed
the benefits mainly to be in providing more confidence in assessments while another
commented that the decision makers did not have that level of knowledge and so
would not really consider it in detail when choosing to use an assessment
“Absence of quality management system was not stopping the agency
using EUnetHTA assessments previously…although the presence may
give users more confidence”.
“Not sure if changes will improve uptake as our commissioner is not at that
level of knowledge of procedures when undertaking HTA and considering
use of EUnetHTA assessments”.
The introduction of a submission requirements document was again viewed
positively by the agencies that were aware of it, although not all were aware that it
has been introduced. For OT it was recognised that some companies, particularly
EUnetHTA WP7 Deliverable 7.2 – Final report
52
smaller companies, do not always fill in the submission file. There was, therefore,
uncertainty about how beneficial it would be in this context.
The optional factual accuracy check by manufacturers on draft documents was
welcomed by some, with this being an important additional step to allow companies
to check and if necessary, get corrected assessment errors. Some agencies were,
however, not in favour of company involvement in this stage.
“Factual accuracy check by manufacturers is of great interest and should
be mandatory, to increase scientific rigour and transparency”.
“Addition of factual accuracy checks is particularly helpful for complex
devices or where there are issues around the CE mark”.
Agency recommendations for the future
Several agencies underlined that there was a need to ensure that authoring teams
had sufficient methodological expertise to undertake JA/CA through internal training
and internal or external expert support.
In addition, it was noted that authoring teams need to have sufficient time allocated
to undertake JA/CA using the procedures that have been defined.
Finally, it was noted that while the implementation of the quality management system
was useful, it has focussed a lot on procedures and there was still a need to focus on
methods.
Conclusions
• Reliability of JA/CA is not reported as a major factor preventing or limiting use
• The implementation of the Companion Guide and submissions requirements
documents give greater confidence in the JA/CA, but mostly have not
impacted on whether agencies use them
• Agencies recommend:
o There is a need to ensure that there is sufficient methodological
expertise within authoring teams through internal capacity building
and/or external methodological expertise
o There needs to be alignment of the procedure followed and time
allowed for authoring. Robustness of JA/CA is reduced if authors are
not given sufficient time to follow the defined procedure
o A factual accuracy process to correct errors in JA/CA before
publication can help to give confidence in the findings.
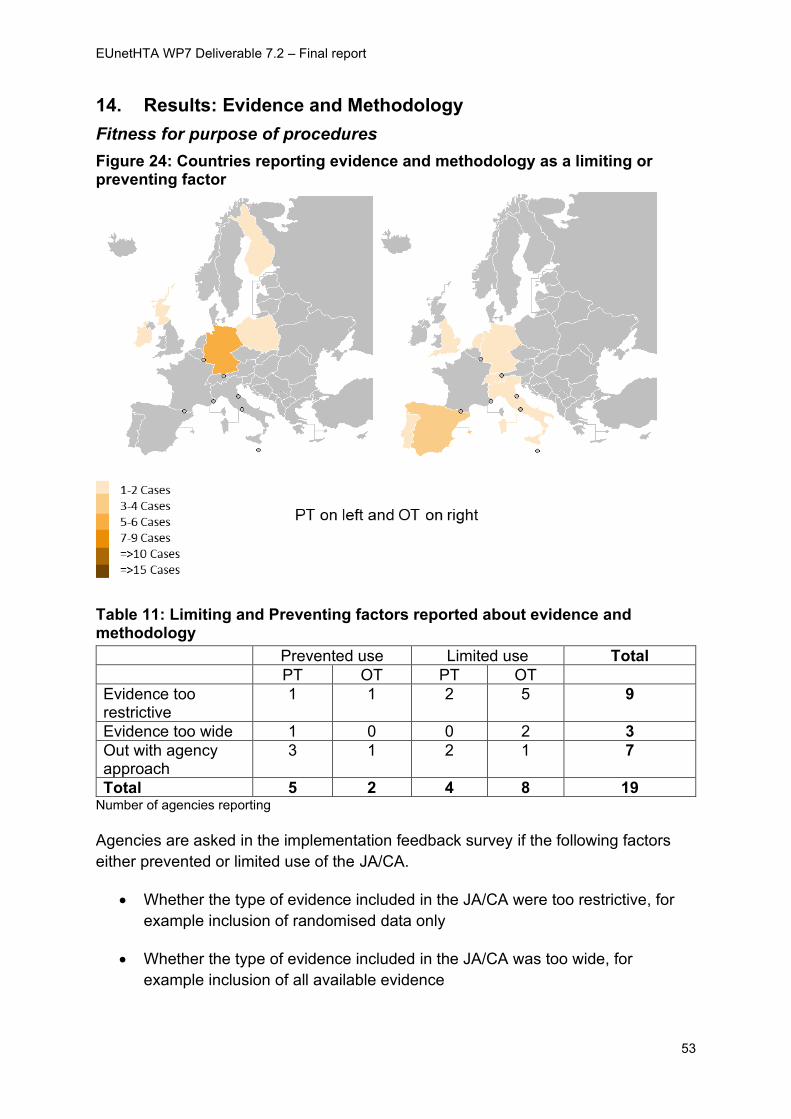
EUnetHTA WP7 Deliverable 7.2 – Final report
53
14. Results: Evidence and Methodology
Fitness for purpose of procedures
Figure 24: Countries reporting evidence and methodology as a limiting or preventing factor
Table 11: Limiting and Preventing factors reported about evidence and methodology
Prevented use Limited use Total
PT OT PT OT
Evidence too restrictive
1 1 2 5 9
Evidence too wide 1 0 0 2 3
Out with agency approach
3 1 2 1 7
Total 5 2 4 8 19 Number of agencies reporting
Agencies are asked in the implementation feedback survey if the following factors
either prevented or limited use of the JA/CA.
• Whether the type of evidence included in the JA/CA were too restrictive, for
example inclusion of randomised data only
• Whether the type of evidence included in the JA/CA was too wide, for
example inclusion of all available evidence
EUnetHTA WP7 Deliverable 7.2 – Final report
54
• Extent to which the evidence and methodology used aligned with that used by
the agency.
The data (figure 24 and table 11) show that for OT in the majority of cases issues
arose from the choice of evidence included in the assessment rather than that the
approach to methodology was out with that adopted by the agency. For PT, more
agencies comment on evidence and methodology being out with the agency
approach than the choice of evidence inclusion. However, the numbers in all
categories are small.
In regard to evidence inclusion, among OT users a number of interviewees noted
that they or their decision makers had reviewed the JA/CA and decided that an
agency assessment was not timely based on the evidence availability in the report.
“We shared the report with the relevant managed clinical network. They
scanned it and considered that insufficient evidence to indicate action at
this time”.
It is positive that agencies are using JA/CA to support topic identification and
decisions about agency assessments. However, it may not be the best possible use
of joint HTA resources if outputs of the process primarily inform a decision that an
agency assessment is not timely because of evidence availability. At the stage of
determining topics for joint assessment and scoping these, it may be appropriate to
include consideration of evidence availability and the types of evidence to be
included in the JA/CA. This might help target joint HTA resources on topics most
likely to result in agency assessments.
Survey data shows that the methodology used for JA/CA is not a key limiting factor.
This is consistent with the findings from the WP7 case study4 that identified that the
EUnetHTA guidelines do not hinder uptake.
Agency perceptions of changes introduced in JA3
In JA3 EUnetHTA developed recommendations and guidance for involving European
patient organisations.
Most agencies were aware of the procedural changes and viewed this change as
positive. The involvement of patients in JA/CA was seen most positively by agencies
who engaged patients less in their agency process compared with agencies who
already had methods of patient engagement. Several agencies are currently
developing their own procedures for involving patients and learning from EUnetHTA
on improving patient involvement was felt to be helpful. A number of agencies
reported that whilst the improved patient involvement in JA/CA would not specifically
4 https://eunethta.eu/wp-content/uploads/2019/06/Implementation-Report-May-2019-FINAL.pdf
EUnetHTA WP7 Deliverable 7.2 – Final report
55
impact on their ability to use the JA/CA, the involvement of patients does improve
their confidence in the findings of the JA/CA.
“It doesn’t impact the ability to use it but the ability to understand and trust
its conclusions”.
One agency also felt that the evidence and methodology focus in JA3 had
become more pragmatic with less focus on specific terminology which helped
them engage better in the process.
“JA2 seemed to very focussed on the core model and all the terminology
around this, and we struggled to get our heads round a lot of what was
being discussed and proposed. We have felt much more engaged in JA3,
and this has made it much easier to get a handle on what is going on and
get involved”
Agency recommendations for the future
Some agencies indicated that the role of patients in scoping needs to be extended.
In addition, having developed the procedures for involvement, there is a need to
ensure that there is follow through from the procedures to engagement.
“Development of procedures for patient involvement is a good step but
often patient organisations do not engage and hence often it does not
improve the assessment”.
In addition, patients are only one group of experts and there is a need for
engagement of clinical experts and potentially also payers.
“Patient participation has improved a lot through changes. Contribution of
clinical experts has not improved much in PT and needs to be improved”.
“Would be good to have more involvement from a payer perspective –
particularly in terms of their input into the [OT] project plan”.
Considering other aspects of evidence and methodology, it was felt that there should
be an increased focus on methodology, particularly in respect of updating existing
EUnetHTA methodological guidelines and developing new methodological guidelines
in emerging areas such as personalised health and precision medicine.
Partners underlined the ongoing need to develop mutual acceptance of certain
methodologies (use of GRADE was highlighted by several agencies).
“It is important that EUnetHTA supported methods are accepted by the
partner agencies and there is mutual agreement in the use of certain
methodologies. The piece of work done by the Common phrases and
EUnetHTA WP7 Deliverable 7.2 – Final report
56
GRADE task group, as well as the PICO subgroup, is very important in
this matter”.
Several agencies identified that once these methods and processes have been agreed
by EUnetHTA, these then needed to be fed back to staff involved in agency
assessment through training and knowledge transfer. One agency stated:
“It is very important that all agency staff involved in the national HTA is
well trained in utilising the joint HTA tools and assessments. Also, it is
essential that there is good communication and knowledge transfer
between staff experienced in the European joint work and national HTA”
Conclusions
• The methodological approach adopted by EUnetHTA is not a key factor limiting
or preventing use of JA/CA
• The decisions made about the study types to be included in an OT assessment is
more frequently reported as a limiting factor than methodological approach.
Consideration of evidence availability and evidence inclusion in OT assessments
should be considered as part of topic identification and scoping.
• The recommendations and guidance for involving patients developed during JA3
has been positively welcomed.
• Agencies recommend:
o Methodological guidance is regularly maintained and extended to cover
new and complex issues arising in HTA
o The methodological approach adopted by EUnetHTA needs to be
consistently applied across all JA/CA
o Agencies need to identify and resolve any methodological areas where
agency adopted approaches actively hinders the use of JA/CA
o Agencies need to ensure that methodologies and processes agreed
through EUnetHTA are communicated to agency assessors through
training and knowledge transfer
o Principles of patient engagement need to be followed up and turned into
actual engagement
o Principles of engagement need to be developed for other expert groups
e.g. clinical experts and payers
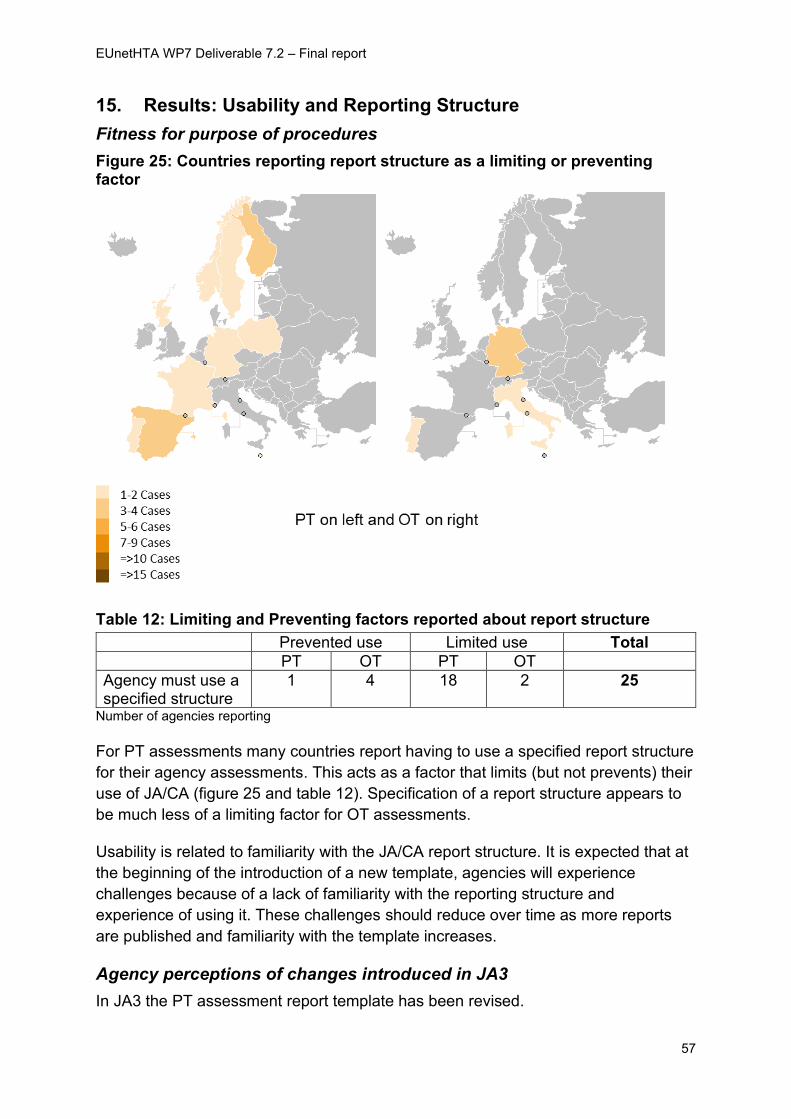
EUnetHTA WP7 Deliverable 7.2 – Final report
57
15. Results: Usability and Reporting Structure
Fitness for purpose of procedures
Figure 25: Countries reporting report structure as a limiting or preventing factor
Table 12: Limiting and Preventing factors reported about report structure
Prevented use Limited use Total
PT OT PT OT
Agency must use a specified structure
1 4 18 2 25
Number of agencies reporting
For PT assessments many countries report having to use a specified report structure
for their agency assessments. This acts as a factor that limits (but not prevents) their
use of JA/CA (figure 25 and table 12). Specification of a report structure appears to
be much less of a limiting factor for OT assessments.
Usability is related to familiarity with the JA/CA report structure. It is expected that at
the beginning of the introduction of a new template, agencies will experience
challenges because of a lack of familiarity with the reporting structure and
experience of using it. These challenges should reduce over time as more reports
are published and familiarity with the template increases.
Agency perceptions of changes introduced in JA3
In JA3 the PT assessment report template has been revised.
EUnetHTA WP7 Deliverable 7.2 – Final report
58
There was limited feedback available on changes to the PT template given the
relatively small number of PT assessments published in the last 12 months. Those
that have used the new template were largely positive reporting that it is easier to
use, simpler and less repetitive. There were also favourable comments on the
availability and use of medical editors.
“The new template is now more simplified and less repetitive”.
“Input of medical editor was very useful….and we suggest keeping this for
future assessments”.
In JA3 the OT template has not yet been revised (a pilot for the revised
template started after the implementation data cut-off), but improved
standardisation of the process and a small number of changes to the
presentation, summary and discussion have positively influenced the readability
of the JA/CA.
“The assessments have become more standardised and the format more
familiar and therefore it is easier for us to use the assessments in JA3”.
“More standardised structure of the assessments”
Agency recommendations for the future
Some agencies felt that further instruction is still required for authors on how to use
the new template
“We are currently an author of an assessment and would be helpful to have
more information on the requirements / expectations of authors in each
section”.
An outstanding issue for PT assessments is about the length of the assessments.
From interviews, there is, however, no clear sense of the best way forward. Some
agencies require detailed JA/CA and others want shorter more concise documents.
Some agencies want specific headings included and covered in the JA/CA and
others do not.
“The structure of the reports has improved, but they are still too
excessive”
For OT assessments one agency commented that there is still a need for
further improvements in clarity and readability.
“In order to make OT assessments more useful, it is important that they
have a clear conclusion on the value of the product in relation to the
relevant comparator/s. Several conclusions of EUnetHTA reports do not
EUnetHTA WP7 Deliverable 7.2 – Final report
59
help the reader to know the answer to the relative effectiveness question
due to unclear language”
Conclusions
• The requirements for agencies to use a specific report structure acts as a limiting
factor in use of JA/CA but rarely prevents use
• The new template for PT assessments has been positively received from those
who have used it
• Changes to the OT process and influence of these on the report structure have
also been positively received
• The heterogenous needs of agencies in their assessments means that defining a
report structure that meets all agencies’ needs completely is unlikely to ever be
fully realised. A balance will be required between different agency needs and
time and resources available for authors.
• To accurately capture usability issues, the introduction of new templates needs to
allow sufficient follow-up time for agencies to become familiar with it, before it is
further revised
• Agencies recommend:
o Further guidance is provided for authors about using the template and
information expectations
o Active brokering of an agreement about the length of JA/CA to meet most
needs of most agencies
o Agreement on the conclusions that can be made in JA/CA
o Editing of JA/CA to ensure language is clear
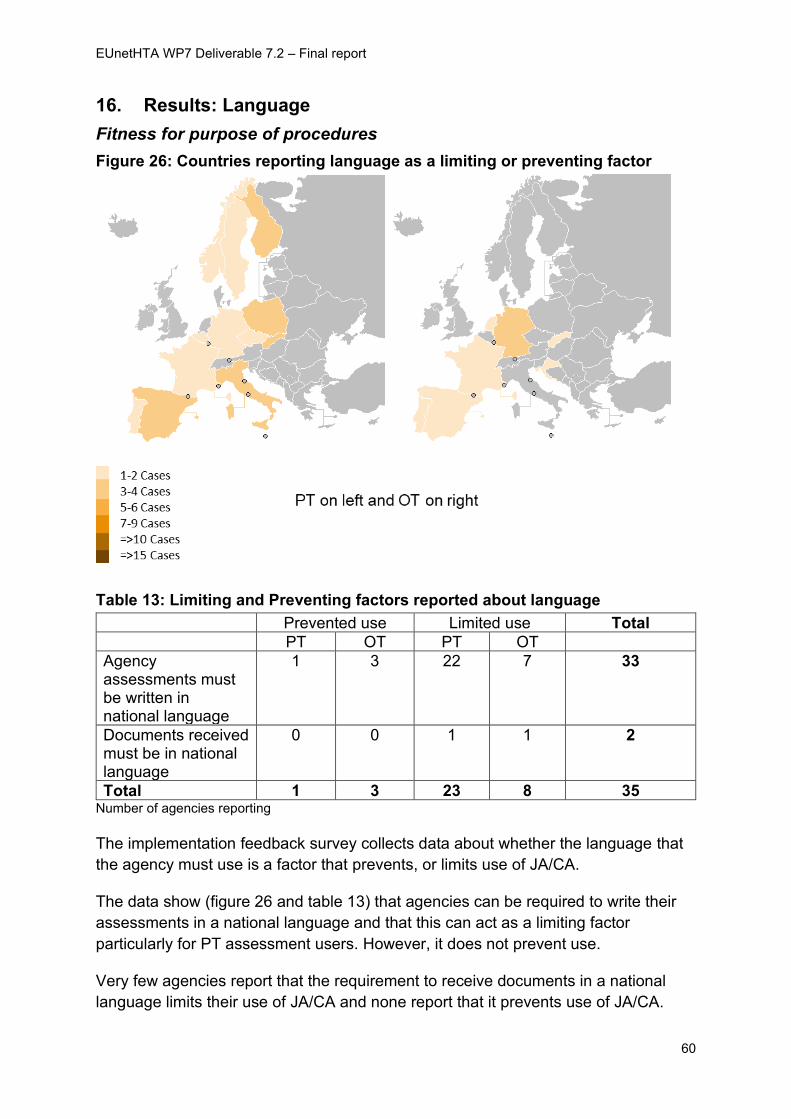
EUnetHTA WP7 Deliverable 7.2 – Final report
60
16. Results: Language
Fitness for purpose of procedures
Figure 26: Countries reporting language as a limiting or preventing factor
Table 13: Limiting and Preventing factors reported about language
Prevented use Limited use Total
PT OT PT OT
Agency assessments must be written in national language
1 3 22 7 33
Documents received must be in national language
0 0 1 1 2
Total 1 3 23 8 35 Number of agencies reporting
The implementation feedback survey collects data about whether the language that
the agency must use is a factor that prevents, or limits use of JA/CA.
The data show (figure 26 and table 13) that agencies can be required to write their
assessments in a national language and that this can act as a limiting factor
particularly for PT assessment users. However, it does not prevent use.
Very few agencies report that the requirement to receive documents in a national
language limits their use of JA/CA and none report that it prevents use of JA/CA.
EUnetHTA WP7 Deliverable 7.2 – Final report
61
Agency perceptions of changes introduced in JA3
Not applicable
Agency recommendations for the future
There was quite a strong view that language and specifically the use of English in
agency assessments could be a tool to improve use of JA/CA. This was suggested
as one of the few areas where potential legal changes could be made.
Agencies with the freedom to prepare reports in English commented on how this
made use easier.
“Agency can publish reports in English or even partially in English which
makes it more convenient to re-use the EUnetHTA report without the need
to translate the information”
Conclusions
• Many agencies must prepare their assessments in their national language. This
acts as a factor that limits use, because text needs to be translated and cannot
be directly used. However, it does not prevent use of JA/CA.
• There is a perception that a change to allow technical documents to be written in
English is required to support implementation, this change is seen as possible by
agencies but to make this change requires legal changes for some countries
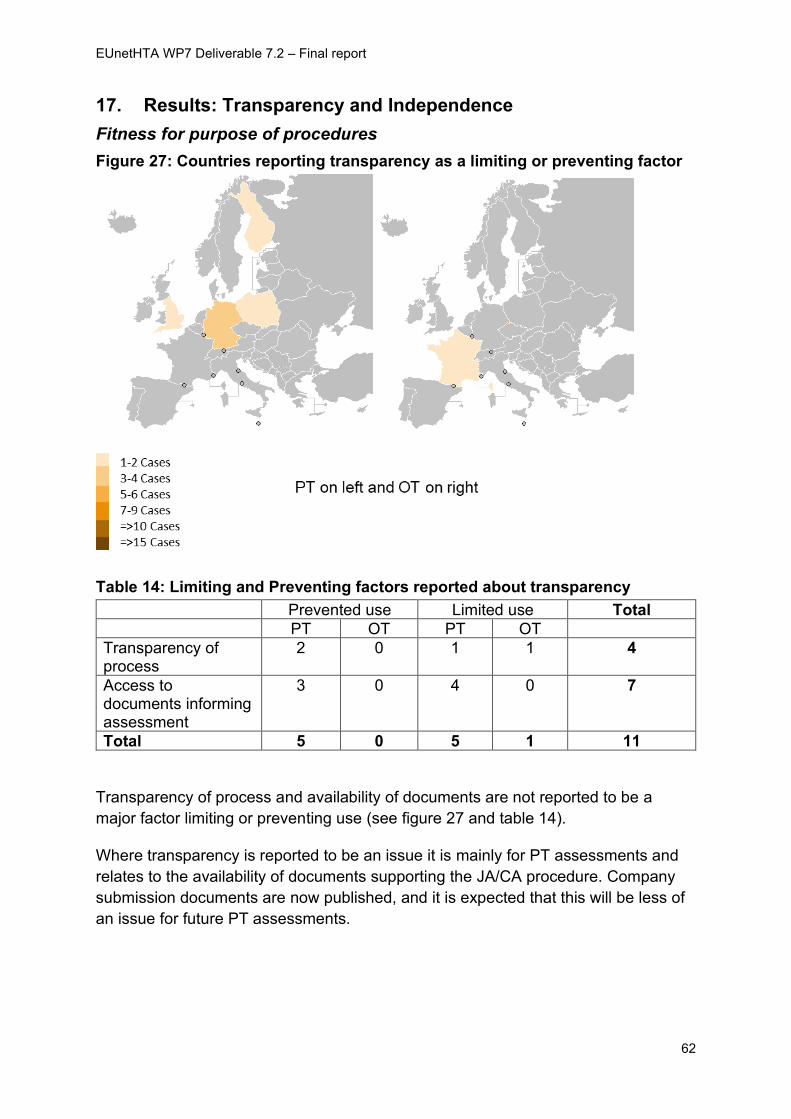
EUnetHTA WP7 Deliverable 7.2 – Final report
62
17. Results: Transparency and Independence
Fitness for purpose of procedures
Figure 27: Countries reporting transparency as a limiting or preventing factor
Table 14: Limiting and Preventing factors reported about transparency
Prevented use Limited use Total
PT OT PT OT
Transparency of process
2 0 1 1 4
Access to documents informing assessment
3 0 4 0 7
Total 5 0 5 1 11
Transparency of process and availability of documents are not reported to be a
major factor limiting or preventing use (see figure 27 and table 14).
Where transparency is reported to be an issue it is mainly for PT assessments and
relates to the availability of documents supporting the JA/CA procedure. Company
submission documents are now published, and it is expected that this will be less of
an issue for future PT assessments.
EUnetHTA WP7 Deliverable 7.2 – Final report
63
Agency perceptions of changes introduced in JA3
The main key change made to improve transparency has been the publication of
submission dossiers for PT assessments. This change has also been implemented
for OT submission dossiers but was not implemented at the time of data cut off.
The key procedural changes made to improve independence were common across
PT and OT assessments and were:
• Publication and communication of DOI form and guidance
• Establishment of the EUnetHTA COI committee
Agencies either felt that publication of PT submission dossiers was a helpful change,
or they viewed this as a neutral change. Some agencies did not need to see the
submission dossier and others did not consider there was enough time in their
agency process to review both the JA/CA and the submission dossier.
“A positive change and good that the REA actually cross-refers to the
submission dossier. Really pleased as lack of submission dossier was a
big issue in JA2”.
Not sure it is a big or particularly helpful change as would probably just
use the EUnetHTA report rather than also check the submission dossier.
All the agencies interviewed were aware of the changes made to declaring COI.
There was a clear consensus from the interviewees that having these procedures in
place give users more confidence and trust in JA/CA, though not necessarily
changing how they will use the JA/CA.
“It increases trust in the assessment”. “They are again positive changes. They create a more transparent process...but there are bigger issues that impact on our ability to use EUnetHTA REAs at a national level, in particular relevance”
Agency recommendations for the future
Regarding publication of the data behind the assessments one agency commented
that publication of company submission dossiers could be extended to also included
clinical study reports.
In regard to COI, Some felt that the COI policy may need to be more flexible in some
instances to ensure appropriate access to clinical expertise and that the length of the
document put people off from participating in assessments.
“The COI procedure was actually too restrictive. Compared to the
[national] COI procedure, an expert can declare an interest but normally
EUnetHTA WP7 Deliverable 7.2 – Final report
64
this expert wouldn’t be excluded as reviewer but flagged or skipped on
those matters at which his interest might affect his judgement”.
“we are told that the DOICU form can be quite long and some people drop
out rather than complete it. So, a recommendation would be to simplify
the DOICU”.
Conclusions
• The principles of transparency and independence adopted by EUnetHTA are
not key factors limiting or preventing use of JA/CA
• The publication of company submission files is viewed as having a positive
impact on PT implementation
• Changes made to the COI policy adds confidence to use of JA/CA
• Agencies recommend:
o Ongoing monitoring of the COI policy to ensure that the stringent
measures in place are not acting as a barrier to getting the best
possible expert involvement
EUnetHTA WP7 Deliverable 7.2 – Final report
65
18. Recommendations for implementation support in a future model of HTA cooperation
The fifth and final key question that we answer in this report is:
“What support for implementation should be built into a future model of HTA
cooperation?”
In JA3 implementation support has mainly focused on raising awareness of JA/CA,
encouraging use, sharing implementation experiences, putting in place a reporting
system to monitor use, feedback to EUnetHTA to support improvements in
processes and reaching out to agencies who are not part of the network but are
potential users of reports. Because the details and requirements of a future model of
HTA cooperation are not yet known JA3 implementation has not worked towards a
set of specific implementation requirements for using JA/CA.
Most agencies agreed that support for implementation should be built into a future
model of HTA cooperation. However, there was a range of different views and
opinions on what types of implementation support should be available.
Agencies considered that the level of implementation support required will differ by
agency and country, and will be dependent on:
• how developed HTA systems are in individual countries
• the levels of HTA experience and expertise within these countries
• whether HTA cooperation has a legislative basis in the future.
Agencies with less developed systems or limited HTA experience will require more
implementation support. Likewise, if there is a legislative basis more implementation
support will be required to support the changes needed.
One respondent felt that to really strengthen HTA in Europe capacity building is
required, specifically to support HTA in smaller and less developed countries. This
was echoed by a respondent from a country where HTA is still establishing who felt
that the HTA regulation would serve as a lever for capacity building and that capacity
development should be built into the future model.
“The needs of member states for implementation support will give a broad
spectrum of responses, depending on how developed their HTA systems
are and how recently HTA activities have started….a key priority is
capacity building and organisational development particularly for smaller
countries…the potential that is not yet tapped for smaller agencies could
be bigger if we do some capacity building to take these agencies forward”.
EUnetHTA WP7 Deliverable 7.2 – Final report
66
Another respondent felt that implementation support could best be provided
centrally:
“A central support office would be helpful, providing a central contract
point for different support…. for example, training, background information
on assessments and procedures and translation support if needed by
some partners”.
In terms of specific types of implementation support that could be offered in the
future a range of options were discussed and proposed.
Monitoring, audit and indicators
Audit tools and indicators can help agencies measure whether they are
implementing outputs appropriately. Some agencies considered the use of audit and
indicators as important as they provide guidance on what is acceptable use.
However, others noted that these can be intrusive and unpopular.
“For PT audit and implementation and workshops indicators most
important”.
“monitoring and audit may be seen as intrusive”.
Training and workshops
It was noted that some training on how to update, adapt and adopt JA/CA might be
needed.
“Some training and update on how to adapt/adopt HTA assessments
might prove useful for implementation purposes”
However, it was also noted that face-to-face approaches do not always work well
because agencies use reports over different time periods. Having online resources
enables agencies to use them when they need them and for more staff to take part.
Online resources and repositories
Sharing implementation experiences through webinars and case studies was viewed
as being helpful because agencies can see the challenges other agencies face and
how they overcame them.
“The sharing of implementation experiences and webinars and case studies are
helpful as enables you to see the difficulties agencies went through and how they
worked through them”
It was also noted that assessment specific webinars where authors shared the key
results and issues in assessments could be helpful for agencies to understand an
assessment and its importance.
EUnetHTA WP7 Deliverable 7.2 – Final report
67
“Webinars are useful. Important that we are aware what is out there and
available for use – so good mechanisms for sharing information on
assessments”
Outreach and field teams
In certain situations (such as where HTA systems were still establishing) dedicated
advisers to support implementation, to engage agencies to discuss and to resolve
issues and to promote outputs might be needed.
“For OT as still in early stages of development nationally workshops and
implementation advisers would be most helpful”
Conclusions
• Implementation support is required in the future model of HTA cooperation
• Support should be centralised and provided in a range of different formats to
fully meet the needs of a range of different HTA agencies across Europe with
different levels of HTA infrastructure, expertise and experience.
• A clear framework needs to be developed and agreed upon, so users of
JA/CA understand the expectations of use.
• Acting alongside the framework there needs to be appropriate organisational
development for agencies to ensure a sustainable model of HTA cooperation.
• In the first instance those agencies still establishing HTA systems require
early facilitative support to put in place the capacity, expertise and processes
to implement the framework.
• Suggested modalities for support:
o Audit and indicators to support agencies to monitor acceptable
implementation
o Online webinars, case studies and training about JA/CA and
implementation experiences
o Outreach and field teams to support developing HTA systems
EUnetHTA WP7 Deliverable 7.2 – Final report
68
Appendix 1: Implementation feedback survey
The same set of questions are used for all JA/CA.
The Intranet survey function automatically records the person who completed the
entry, the date of completion and if the survey was fully completed
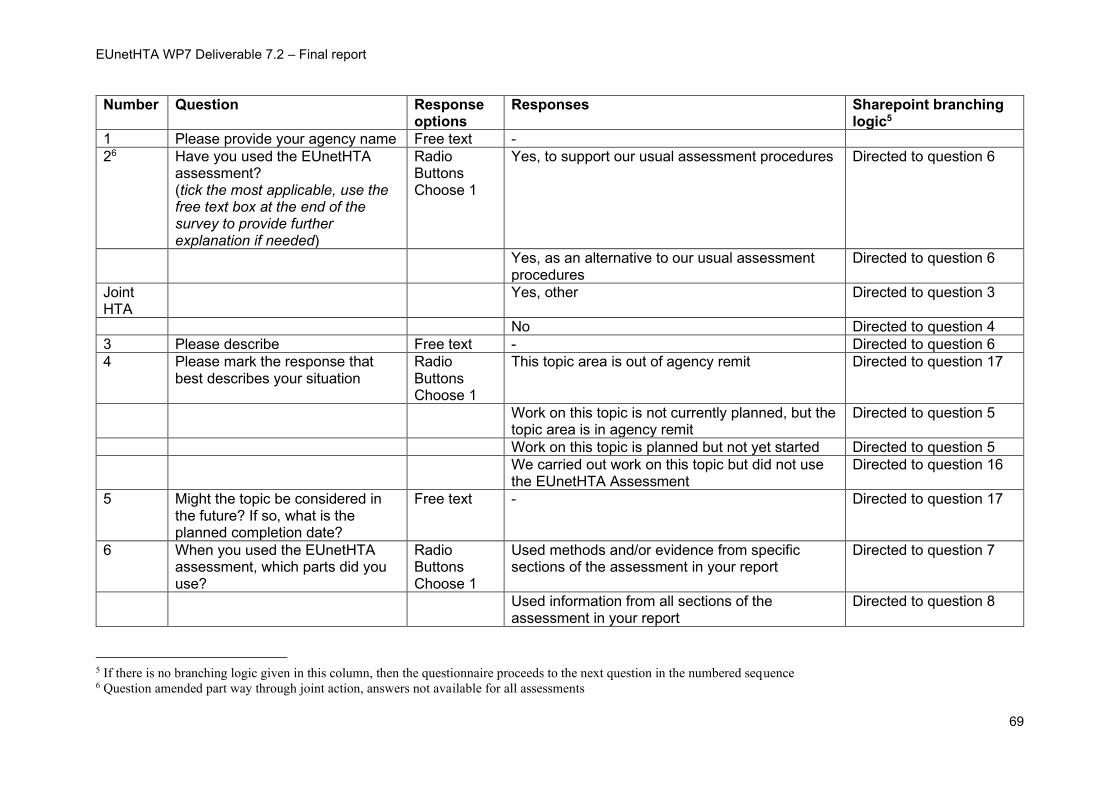
EUnetHTA WP7 Deliverable 7.2 – Final report
69
Number Question Response options
Responses Sharepoint branching logic5
1 Please provide your agency name Free text -
26 Have you used the EUnetHTA assessment? (tick the most applicable, use the free text box at the end of the survey to provide further explanation if needed)
Radio Buttons Choose 1
Yes, to support our usual assessment procedures Directed to question 6
Yes, as an alternative to our usual assessment procedures
Directed to question 6
Joint HTA
Yes, other Directed to question 3
No Directed to question 4
3 Please describe Free text - Directed to question 6
4 Please mark the response that best describes your situation
Radio Buttons Choose 1
This topic area is out of agency remit Directed to question 17
Work on this topic is not currently planned, but the topic area is in agency remit
Directed to question 5
Work on this topic is planned but not yet started Directed to question 5
We carried out work on this topic but did not use the EUnetHTA Assessment
Directed to question 16
5 Might the topic be considered in the future? If so, what is the planned completion date?
Free text - Directed to question 17
6 When you used the EUnetHTA assessment, which parts did you use?
Radio Buttons Choose 1
Used methods and/or evidence from specific sections of the assessment in your report
Directed to question 7
Used information from all sections of the assessment in your report
Directed to question 8
5 If there is no branching logic given in this column, then the questionnaire proceeds to the next question in the numbered sequence 6 Question amended part way through joint action, answers not available for all assessments
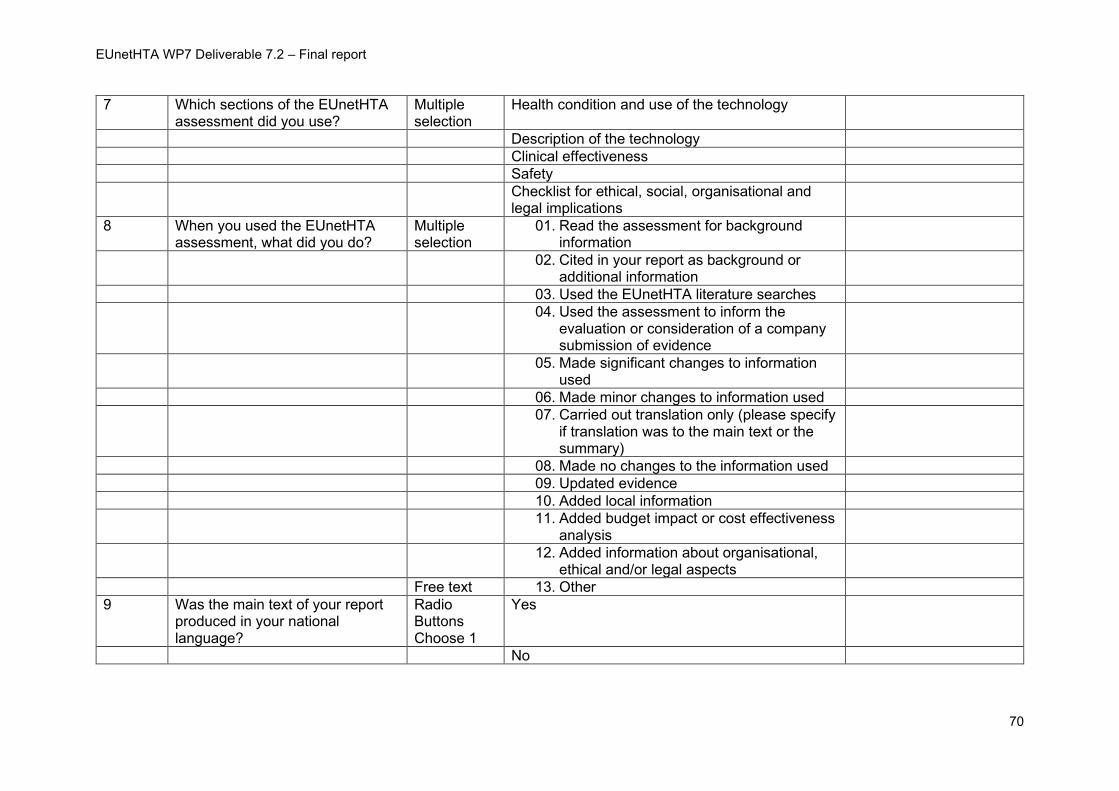
EUnetHTA WP7 Deliverable 7.2 – Final report
70
7 Which sections of the EUnetHTA assessment did you use?
Multiple selection
Health condition and use of the technology
Description of the technology
Clinical effectiveness
Safety
Checklist for ethical, social, organisational and legal implications
8 When you used the EUnetHTA assessment, what did you do?
Multiple selection
01. Read the assessment for background information
02. Cited in your report as background or additional information
03. Used the EUnetHTA literature searches
04. Used the assessment to inform the evaluation or consideration of a company submission of evidence
05. Made significant changes to information used
06. Made minor changes to information used
07. Carried out translation only (please specify if translation was to the main text or the summary)
08. Made no changes to the information used
09. Updated evidence
10. Added local information
11. Added budget impact or cost effectiveness analysis
12. Added information about organisational, ethical and/or legal aspects
Free text 13. Other
9 Was the main text of your report produced in your national language?
Radio Buttons Choose 1
Yes
No
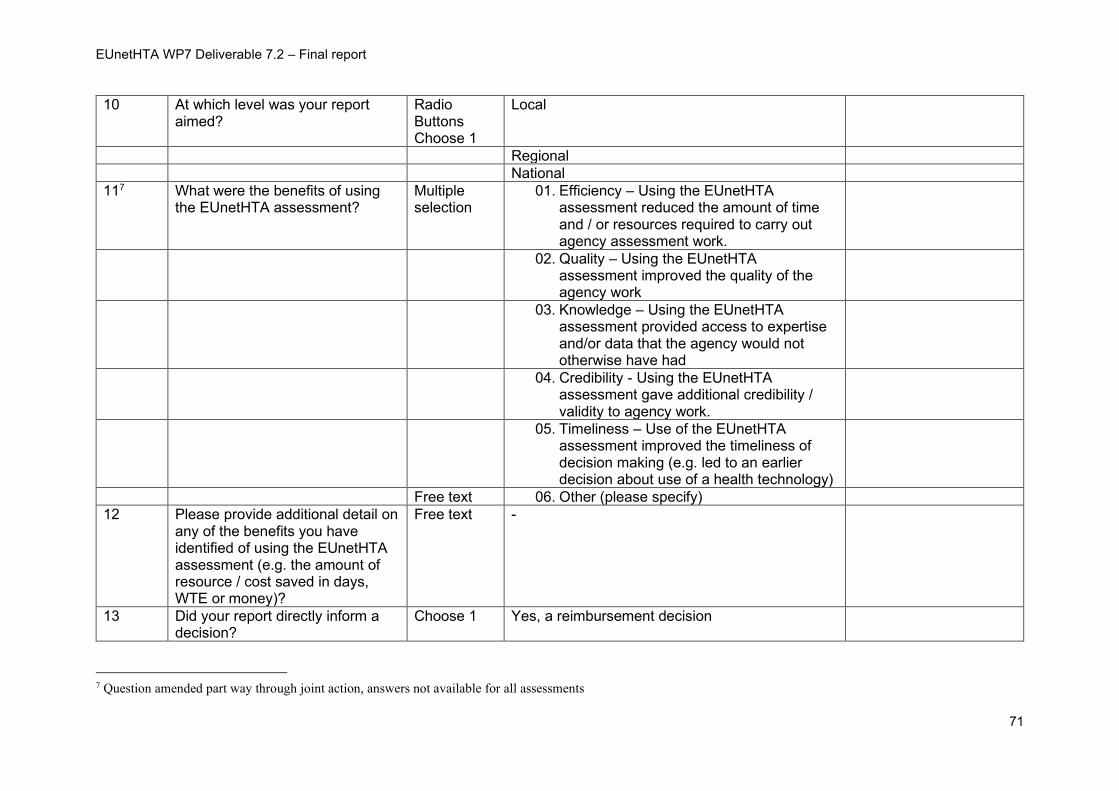
EUnetHTA WP7 Deliverable 7.2 – Final report
71
10 At which level was your report aimed?
Radio Buttons Choose 1
Local
Regional
National
117 What were the benefits of using the EUnetHTA assessment?
Multiple selection
01. Efficiency – Using the EUnetHTA assessment reduced the amount of time and / or resources required to carry out agency assessment work.
02. Quality – Using the EUnetHTA assessment improved the quality of the agency work
03. Knowledge – Using the EUnetHTA assessment provided access to expertise and/or data that the agency would not otherwise have had
04. Credibility - Using the EUnetHTA assessment gave additional credibility / validity to agency work.
05. Timeliness – Use of the EUnetHTA assessment improved the timeliness of decision making (e.g. led to an earlier decision about use of a health technology)
Free text 06. Other (please specify)
12 Please provide additional detail on any of the benefits you have identified of using the EUnetHTA assessment (e.g. the amount of resource / cost saved in days, WTE or money)?
Free text -
13 Did your report directly inform a decision?
Choose 1 Yes, a reimbursement decision
7 Question amended part way through joint action, answers not available for all assessments
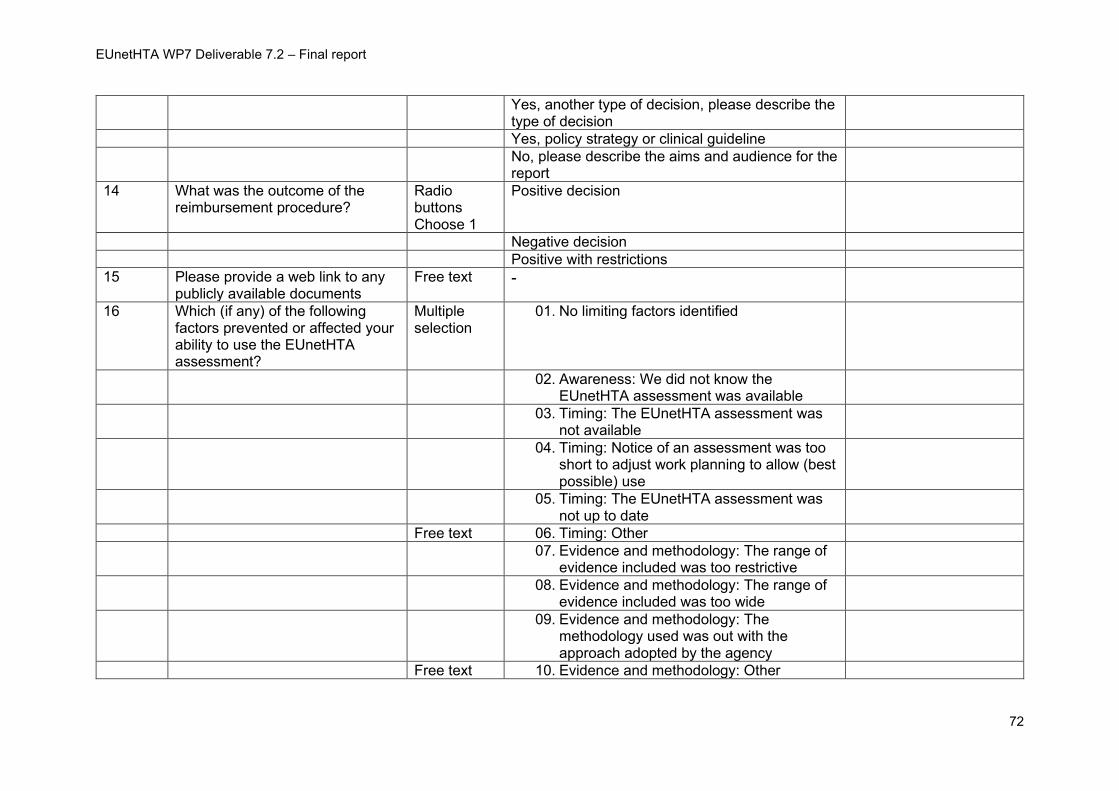
EUnetHTA WP7 Deliverable 7.2 – Final report
72
Yes, another type of decision, please describe the type of decision
Yes, policy strategy or clinical guideline
No, please describe the aims and audience for the report
14 What was the outcome of the reimbursement procedure?
Radio buttons Choose 1
Positive decision
Negative decision
Positive with restrictions
15 Please provide a web link to any publicly available documents
Free text -
16 Which (if any) of the following factors prevented or affected your ability to use the EUnetHTA assessment?
Multiple selection
01. No limiting factors identified
02. Awareness: We did not know the EUnetHTA assessment was available
03. Timing: The EUnetHTA assessment was not available
04. Timing: Notice of an assessment was too short to adjust work planning to allow (best possible) use
05. Timing: The EUnetHTA assessment was not up to date
Free text 06. Timing: Other
07. Evidence and methodology: The range of evidence included was too restrictive
08. Evidence and methodology: The range of evidence included was too wide
09. Evidence and methodology: The methodology used was out with the approach adopted by the agency
Free text 10. Evidence and methodology: Other
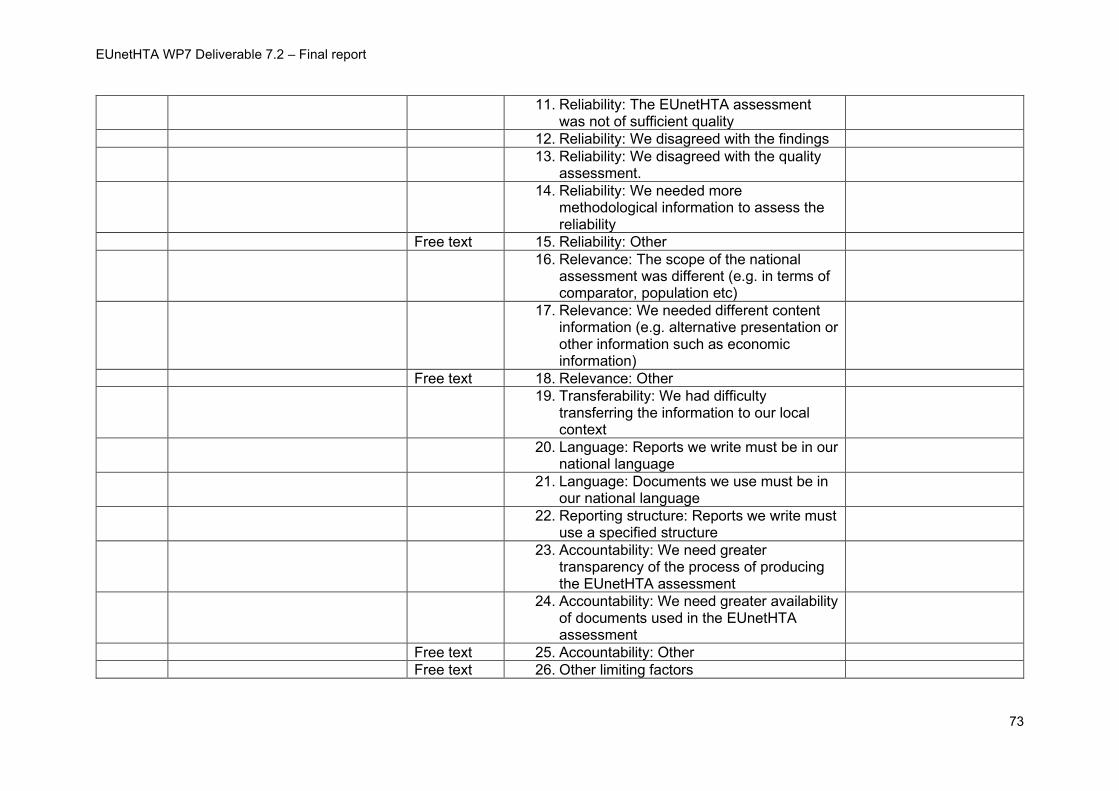
EUnetHTA WP7 Deliverable 7.2 – Final report
73
11. Reliability: The EUnetHTA assessment was not of sufficient quality
12. Reliability: We disagreed with the findings
13. Reliability: We disagreed with the quality assessment.
14. Reliability: We needed more methodological information to assess the reliability
Free text 15. Reliability: Other
16. Relevance: The scope of the national assessment was different (e.g. in terms of comparator, population etc)
17. Relevance: We needed different content information (e.g. alternative presentation or other information such as economic information)
Free text 18. Relevance: Other
19. Transferability: We had difficulty transferring the information to our local context
20. Language: Reports we write must be in our national language
21. Language: Documents we use must be in our national language
22. Reporting structure: Reports we write must use a specified structure
23. Accountability: We need greater transparency of the process of producing the EUnetHTA assessment
24. Accountability: We need greater availability of documents used in the EUnetHTA assessment
Free text 25. Accountability: Other
Free text 26. Other limiting factors
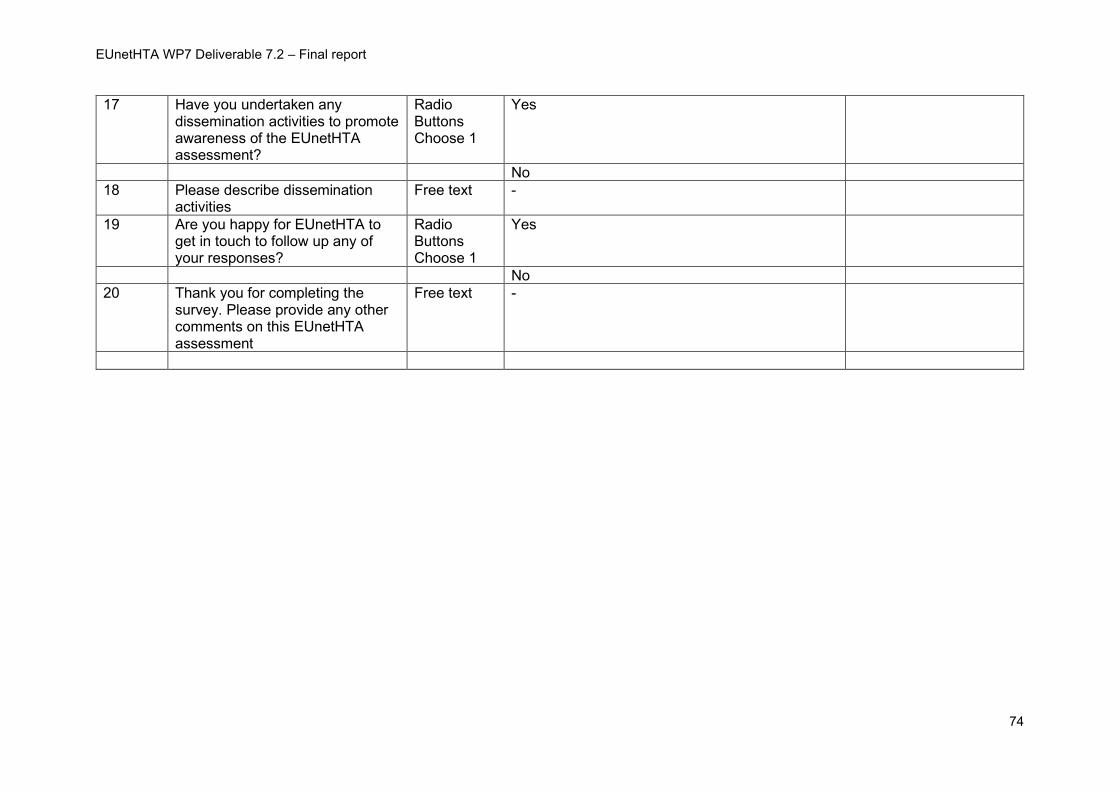
EUnetHTA WP7 Deliverable 7.2 – Final report
74
17 Have you undertaken any dissemination activities to promote awareness of the EUnetHTA assessment?
Radio Buttons Choose 1
Yes
No
18 Please describe dissemination activities
Free text -
19 Are you happy for EUnetHTA to get in touch to follow up any of your responses?
Radio Buttons Choose 1
Yes
No
20 Thank you for completing the survey. Please provide any other comments on this EUnetHTA assessment
Free text -
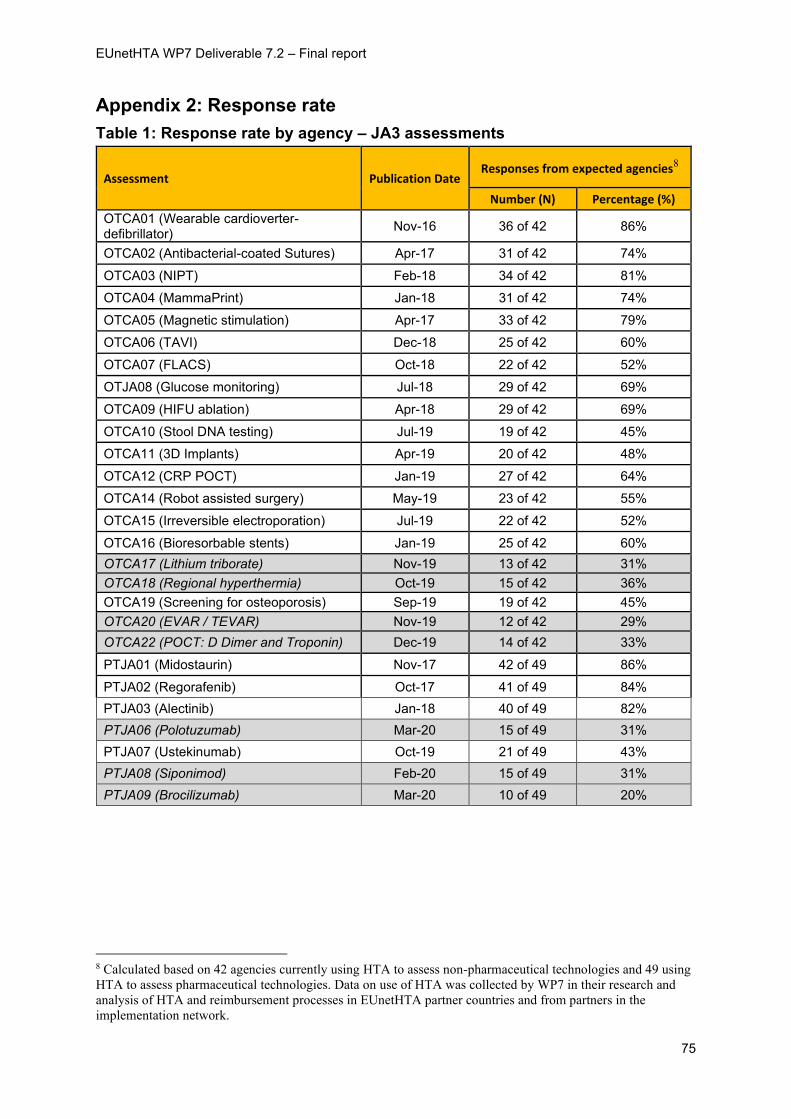
EUnetHTA WP7 Deliverable 7.2 – Final report
75
Appendix 2: Response rate
Table 1: Response rate by agency – JA3 assessments
Assessment Publication Date Responses from expected agencies8
Number (N) Percentage (%)
OTCA01 (Wearable cardioverter-defibrillator)
Nov-16 36 of 42 86%
OTCA02 (Antibacterial-coated Sutures) Apr-17 31 of 42 74%
OTCA03 (NIPT) Feb-18 34 of 42 81%
OTCA04 (MammaPrint) Jan-18 31 of 42 74%
OTCA05 (Magnetic stimulation) Apr-17 33 of 42 79%
OTCA06 (TAVI) Dec-18 25 of 42 60%
OTCA07 (FLACS) Oct-18 22 of 42 52%
OTJA08 (Glucose monitoring) Jul-18 29 of 42 69%
OTCA09 (HIFU ablation) Apr-18 29 of 42 69%
OTCA10 (Stool DNA testing) Jul-19 19 of 42 45%
OTCA11 (3D Implants) Apr-19 20 of 42 48%
OTCA12 (CRP POCT) Jan-19 27 of 42 64%
OTCA14 (Robot assisted surgery) May-19 23 of 42 55%
OTCA15 (Irreversible electroporation) Jul-19 22 of 42 52%
OTCA16 (Bioresorbable stents) Jan-19 25 of 42 60%
OTCA17 (Lithium triborate) Nov-19 13 of 42 31%
OTCA18 (Regional hyperthermia) Oct-19 15 of 42 36%
OTCA19 (Screening for osteoporosis) Sep-19 19 of 42 45%
OTCA20 (EVAR / TEVAR) Nov-19 12 of 42 29%
OTCA22 (POCT: D Dimer and Troponin) Dec-19 14 of 42 33%
PTJA01 (Midostaurin) Nov-17 42 of 49 86%
PTJA02 (Regorafenib) Oct-17 41 of 49 84%
PTJA03 (Alectinib) Jan-18 40 of 49 82%
PTJA06 (Polotuzumab) Mar-20 15 of 49 31%
PTJA07 (Ustekinumab) Oct-19 21 of 49 43%
PTJA08 (Siponimod) Feb-20 15 of 49 31%
PTJA09 (Brocilizumab) Mar-20 10 of 49 20%
8 Calculated based on 42 agencies currently using HTA to assess non-pharmaceutical technologies and 49 using
HTA to assess pharmaceutical technologies. Data on use of HTA was collected by WP7 in their research and
analysis of HTA and reimbursement processes in EUnetHTA partner countries and from partners in the
implementation network.
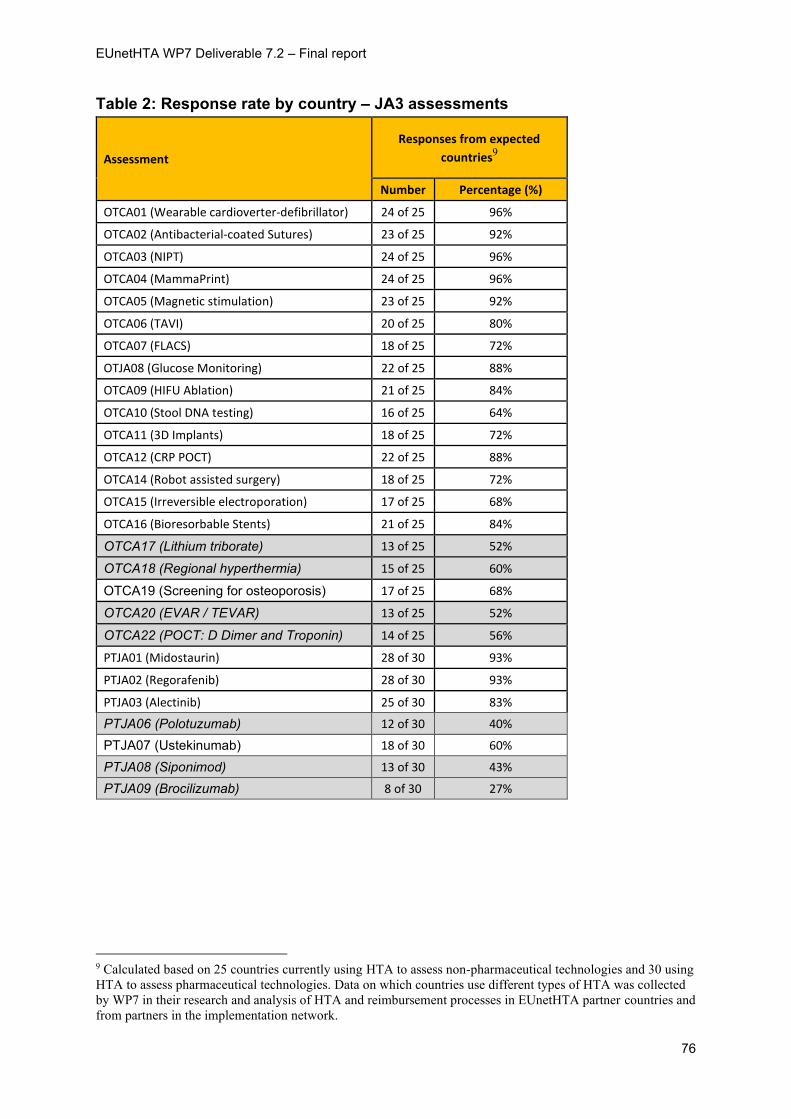
EUnetHTA WP7 Deliverable 7.2 – Final report
76
Table 2: Response rate by country – JA3 assessments
Assessment
Responses from expected
countries9
Number Percentage (%)
OTCA01 (Wearable cardioverter-defibrillator) 24 of 25 96%
OTCA02 (Antibacterial-coated Sutures) 23 of 25 92%
OTCA03 (NIPT) 24 of 25 96%
OTCA04 (MammaPrint) 24 of 25 96%
OTCA05 (Magnetic stimulation) 23 of 25 92%
OTCA06 (TAVI) 20 of 25 80%
OTCA07 (FLACS) 18 of 25 72%
OTJA08 (Glucose Monitoring) 22 of 25 88%
OTCA09 (HIFU Ablation) 21 of 25 84%
OTCA10 (Stool DNA testing) 16 of 25 64%
OTCA11 (3D Implants) 18 of 25 72%
OTCA12 (CRP POCT) 22 of 25 88%
OTCA14 (Robot assisted surgery) 18 of 25 72%
OTCA15 (Irreversible electroporation) 17 of 25 68%
OTCA16 (Bioresorbable Stents) 21 of 25 84%
OTCA17 (Lithium triborate) 13 of 25 52%
OTCA18 (Regional hyperthermia) 15 of 25 60%
OTCA19 (Screening for osteoporosis) 17 of 25 68%
OTCA20 (EVAR / TEVAR) 13 of 25 52%
OTCA22 (POCT: D Dimer and Troponin) 14 of 25 56%
PTJA01 (Midostaurin) 28 of 30 93%
PTJA02 (Regorafenib) 28 of 30 93%
PTJA03 (Alectinib) 25 of 30 83%
PTJA06 (Polotuzumab) 12 of 30 40%
PTJA07 (Ustekinumab) 18 of 30 60%
PTJA08 (Siponimod) 13 of 30 43%
PTJA09 (Brocilizumab) 8 of 30 27%
9 Calculated based on 25 countries currently using HTA to assess non-pharmaceutical technologies and 30 using
HTA to assess pharmaceutical technologies. Data on which countries use different types of HTA was collected
by WP7 in their research and analysis of HTA and reimbursement processes in EUnetHTA partner countries and
from partners in the implementation network.