
Etiology of Spine-Related Disability: Overview Heidi Prather, DO Professor Vice Chair, Department of...
29
Etiology of Spine- Related Disability: Overview Heidi Prather, DO Professor Vice Chair, Department of Orthopaedic Surgery Division Chief, Physical Medicine and Rehabilitation Departments of Orthopaedic Surgery and Neurology Washington University School of Medicine St. Louis, Missouri
-
Upload
phillip-summers -
Category
Documents
-
view
214 -
download
0
Transcript of Etiology of Spine-Related Disability: Overview Heidi Prather, DO Professor Vice Chair, Department of...

Etiology of Spine-Related Disability:
OverviewHeidi Prather, DO
ProfessorVice Chair, Department of Orthopaedic Surgery
Division Chief, Physical Medicine and RehabilitationDepartments of Orthopaedic Surgery and Neurology
Washington University School of MedicineSt. Louis, Missouri

Chronic Spine Pain
• Acute spine pain has a favorable prognosis • Chronic spine pain serves no biological purpose
• a complex milieu influenced by endogenous and exogenous factors that alter the individual's productivity more than the initiating pathological dysfunction would have

Statistics and Chronic Pain
• 15-20% develop protracted pain• 2-8% have chronic pain• 25-30%of patients in a primary care setting may still have problems
after 1 year.[3, 4]

What is Disability?
• Webster• a condition (such as an illness or an injury) that damages or limits a person's physical or
mental abilities
• ADA legal definintion• a person with a disability is a person who has a physical or mental impairment that
substantially limits one or more major life activity
• SSI definition• An individual with a severe impairment that has lasted or is expected to last one year• How SSI decides one is unable to work?
• Evaluates medical evidence, limitation rating and compare the rating to the type of work done in the past
• WHO• “a multidimensional experience for the person involved”

There is no diagnostic test for disability.
LBP and disability
• Spine-related impairment is the most common cause of disability in the United States .[5, 6]
• $357 billion US public funds are spent annually to support disabled [5,
6, 16)
• • $253 billion in costs associated with spine-related impairment in US 91% increase in just over a decade.[17]
• 1% of the working-age population is totally and permanently disabled.[7, 3, 8]

Source: Social Security AdministrationCredit: Lam Thuy Vo / NPR
Spine Pain and Lost Work Time
• Back pain results in approximately 40% absenteeism • 20% of those with spine pain report they cannot continue work.
• In 2008, back pain was the cause of 671 million bed days and 385 million lost work days
• 66% of the total costs associated with spine-related impairment due to productivity loss and absenteeism
• employer annual losses of $28 billion
• $40/144 billion paid annually by SSDI goes to people with spine impairment
• Total number of SSDI beneficiaries increased by 43% between 2003 – 2013

Is society & the work place less accommodating to people with chronic pain?
• In Hale County, Alabama, nearly 1 in 4 working-age adults is on disability
• http://apps.npr.org/unfit-for-work/
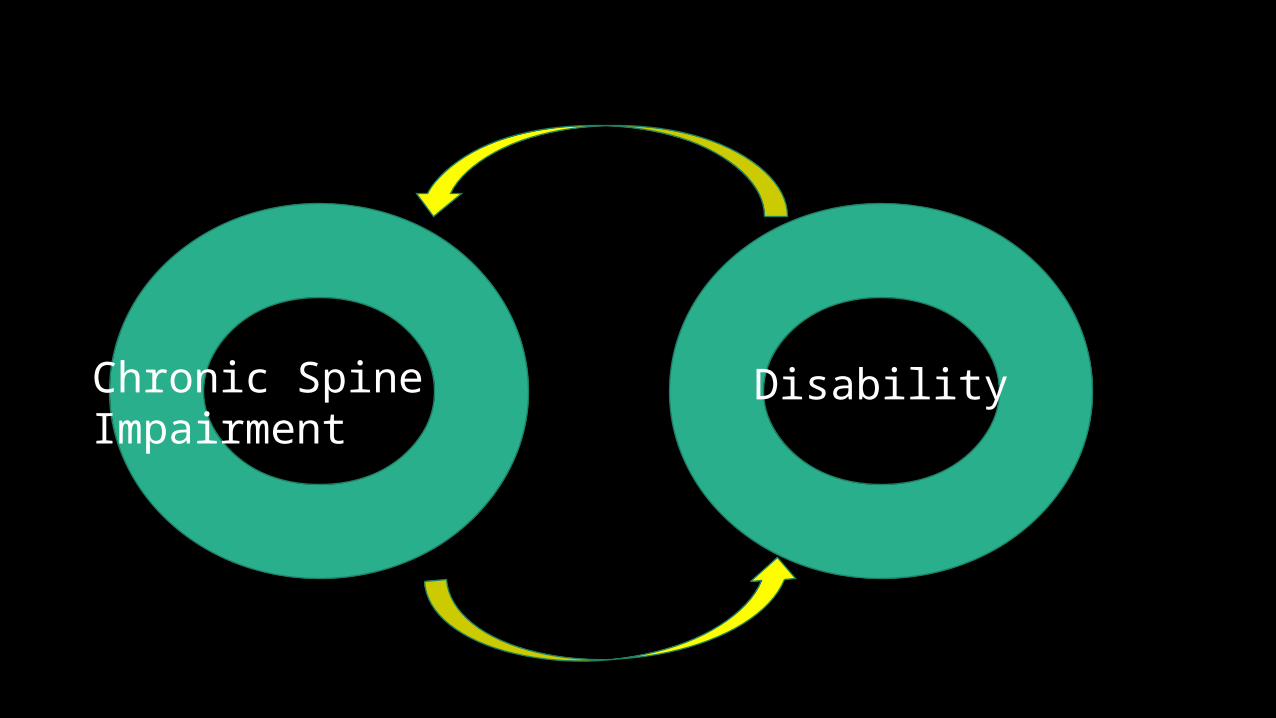
Chronic Spine Impairment Disability
Reduced Chronicity of Spine Impairment Reduced disability

Why Does Spine Pain Become Chronic?• Pain continues beyond the usual time frame of 8 -12 weeks required
for tissue repair• Chronic LBP serves no biological purpose
• a complex milieu influenced by endogenous and exogenous factors that alter the individual's productivity more than the initiating pathological dysfunction would have

Road to Chronic Pain
• An event or series of events ( living life) occurs• Tissue injury• The brain receives the message of pain• A reaction occurs• Tissue repairs• Pain remains

The Pursuit For the Pain Generator!
• Structural• Physiological• Biopsychosocial

Differential Diagnosis For Low Back Pain
Mechanical syndromesDiskal and facet motion segment degeneration Muscular pain disorders (eg,myofascial pain syndrome) Diskogenic pain with or without radicular symptoms Radiculopathy due to structural impingement Axial or radicular pain due to a biochemical or inflammatory reaction to spinal injury Motion segment or vertebral osseous fractures Spondylosis with or without central or lateral canal stenosis Macroinstability or microinstability of the spine with or without radiographic hypermobility or evidence of subluxation
Nonmechanical syndromesNeurologic syndromes Myelopathy or myelitis from intrinsic/extrinsic structural or vascular processesLumbosacral plexopathy (eg, diabetes, vasculitis, malignancy)Acute, subacute, or chronic polyneuropathy (eg, chronic inflammatory demyelinating polyneuropathy, Guillain-Barre syndrome, diabetes) Mononeuropathy, including causalgia (eg, trauma, diabetes)Myopathy, including myositis and various metabolic conditionsSpinal segmental, lumbopelvic, or generalized dystoniaSystemic disorders Primary or metastatic neoplasmsOsseous, diskal, or epidural infectionsInflammatory spondyloarthropathyMetabolic bone diseases, including osteoporosisVascular disorders (eg, atherosclerosis, vasculitis)Referred pain Gastrointestinal disorders (eg, pancreatitis, pancreatic cancer, cholecystitis)Cardiorespiratory disorders (eg, pericarditis, pleuritis, pneumonia)Disorders of the ribs or sternumGenitourinary disorders (eg, nephrolithiasis, prostatitis, pyelonephritis)Thoracic or abdominal aortic aneurysmsHip disorders (eg, injury, inflammation, or end-stage degeneration of the joint and associated soft tissues [tendons, bursae, ligaments])

If diagnostic studies do not reveal a structural cause, physicians and patients alike question whether the pain has a psychological, rather than physical, cause.

Not on the usual list of suspects
• Movement• Physiological response• Movement impairments adaptive to the chronic input of pain• Biopsychosocial factors that influence pain processing
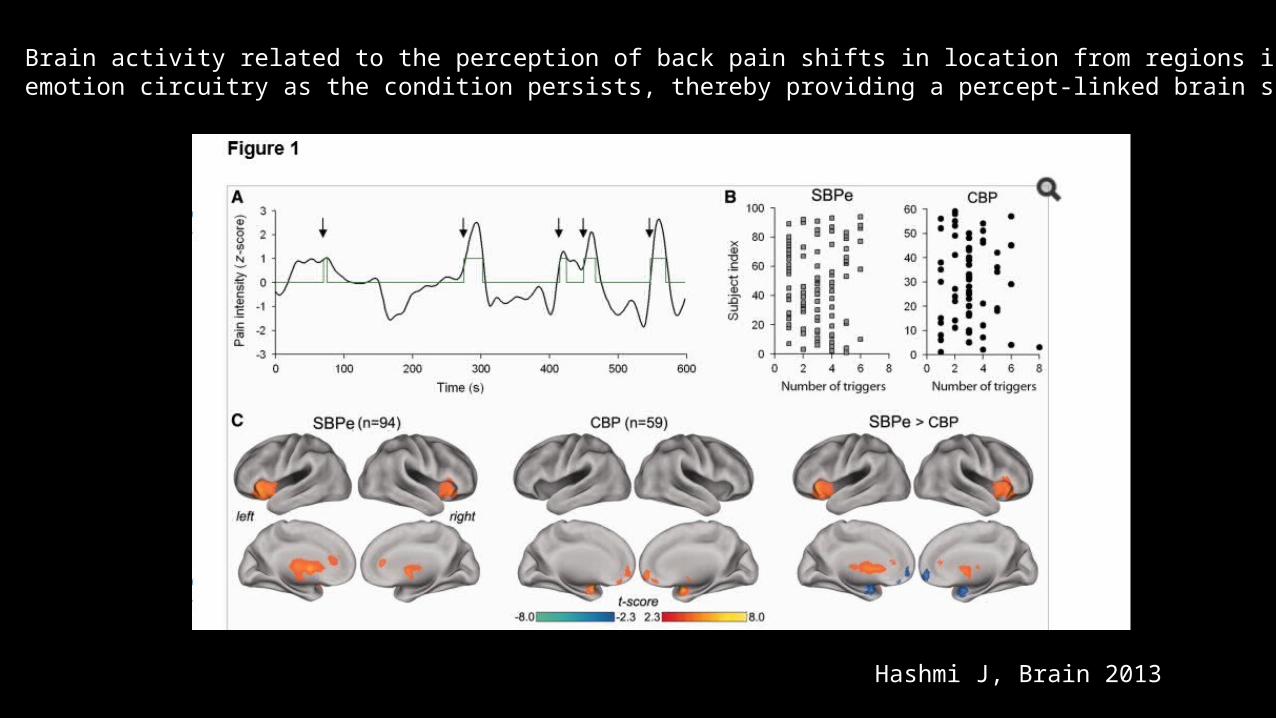
Brain activity related to the perception of back pain shifts in location from regions involved in acute pain to engageemotion circuitry as the condition persists, thereby providing a percept-linked brain signature for the transition to chronic pain.
Hashmi J, Brain 2013

Arthritis Research Campaign National Primary Care CentreKeele University
Stratified care approach for LBP Use epidemiology about back pain predictorsDetermine ‘risk status’ using an index of independent predictorsUse ‘risk status’ to help referral decision making regarding treatment
Confidence to self-manage
Lack of personal control
Fears & worries about diagnosis
Stigma & symptom legitimisation
Loss of role and identity
Catastrophizing Somatizing
Job satisfaction Stress
Loneliness
Expectations
Mood
Co-morbid pain & illnesses
SciaticaLoss of function & impact on work
Pain intensity
Courtesy Jonathan Hill PhD


Lessons from the advances in cancer treatment
MOLECULARLY TARGETED THERAPIES AND THE FUTURE OF MANAGING SCLC, PRESENTED BY PAUL A. BUNN, JR., MD

Person withSpine
Impairment
Pain modifiers
Correction movement
impairments
Modify Structural Disorder
Modify aberrant pain
processing

Person withSpine
Impairment
Pain modifiers
Correction movement
impairments
Modify Structural Disorder
Modify aberrant pain
processing
MechanismStrucutral changes
Physiological changesMovement patterns
Pain processingModifiable biopsychosocial risk
factors

Not allowing an acute event to evolve to a chronic problem
Reduction in Disability
=

Reasons for disability
• Common disorder• Variable reasons for developing spine pain• Variable reasons for continued pain• Pain is an emotional response unique to the individual• Tremendous amount of investigation has focused primarily on structural
disorders as the cause of pain• Brain-mind relationships have yet to be fully explored• As a result, our evaluation, understanding and treatment of pain is limited• Social systems do not always accommodate people with chronic pain• Hence…. Disability

“Most cases of back pain resolve regardless of the course of therapy, and some do not get better no matter what is done.
Therein lies the problem for practitioners, patients and policy makers.”
Lancet 2005
Thank You
References• 1. Wheeler A. Low Back Pain and Sciatica http://emedicine.medscape.com/article/1144130-overview accessed July 4 2015• 2. Anderssen GBJ. Epidemiologic features of chronic low back pain. Lancet. 1999. 354:581-5. • 3. Anderssen GBJ. Frymoyer JW (ed.). The epidemiology of spinal disorders, in The Adult Spine: Principles and Practice. New York: Raven
Press; 1997. 93-141. • 4. Nachemson Al, Waddell G, Norland AL. Nachemson AL, Jonsson E (eds.). Epidemiology of Neck and Low Back Pain, in. Neck and Back
Pain: The scientific evidence of causes, diagnoses, and treatment. Philadelphia: Lippincott Williams & Wilkins; 2000. 165-187. • 5. Kelsey JL, White AA. Epidemiology of low back pain. Spine. 1980. 6:133-42. • 6. Waddell G. 1987 Volvo award in clinical sciences. A new clinical model for the treatment of low-back pain. Spine (Phila Pa 1976).
1987 Sep. 12(7):632-44.• 7. Mayer TG, Gatchel RJ. Functional restoration for spinal disorders: The sports medicine approach. Philadelphia: Lea & Febiger; 1988. • 8. Cunningham LS, Kelsey JL. Epidemiology of musculoskeletal impairments and associated disability. Am J Public Health. 1984 Jun.
74(6):• 9. National Center for Health Statistics (1977):. Limitations of activity due to chronic conditions, United States. 1974. Series 10, No.111. • 10. National Center for Health Statistics (1975):. Physician visits, volume and interval since last visit, United States. 1971. Series 10,
No.97. • 11. In National Center for Health Statistics (1982):. Surgical operations in short stay hospitals by diagnosis, United States. 1978. Series
13, No.61.• 12. National Center for Health Statistics (1976):. Inpatient utilization of short stay hospitals by diagnosis, United States. 1973. Series 13,
No.25. • 13. National Center for Health Statistics (1976):. Surgical operations in short stay hospitals by diagnosis, United States. 1973. Series 13,
No.24. • 14. Spengler DM, Bigos SJ, Martin NA, Zeh J, Fisher L, Nachemson A. Back injuries in industry: a retrospective study. I. Overview and
cost analysis. Spine (Phila Pa 1976). 1986 Apr. 11(3):241-5.• 15. Hashmi JA1, Baliki MN, Huang L, Baria AT, Torbey S, Hermann KM, Schnitzer TJ, Apkarian AVShape shifting pain: chronification of
back pain shifts brain representation from nociceptive to emotional circuits. Brain.2013 Sep;136(Pt 9):2751-68. doi: 10.1093/brain/awt211.
references
• 16. Rizzo, J.A., Abbott, T.A. III, Berger, M.L.(2011). The labor productivity effects of chronic backache in the United States, 2nd Ed., 22.
• 17. United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), Third Edition, 2014. Rosemont, IL. Available at http://www.boneandjointburden.org.


















