Etiology of Obesity Over the Life Span: Ecological and Genetic Highlights from Asian Countries
22
ETIOLOGY OF OBESITY (MS WESTERTERP-PLANTENGA, SECTION EDITOR) Etiology of Obesity Over the Life Span: Ecological and Genetic Highlights from Asian Countries Pei Nee Chong & Christinal Pey Wen Teh & Bee Koon Poh & Mohd Ismail Noor Published online: 15 January 2014 # Springer Science+Business Media New York 2014 Abstract Obesity is a worldwide pandemic, and the preva- lence rate has doubled since the 1980s. Asian countries are also experiencing the global epidemic of obesity with its related health consequences. The prevalence of overweight and obesity are increasing at an alarming rate across all age groups in Asia. These increases are mainly attributed to rapid economic growth, which leads to socio-economic, nutrition and lifestyle transitions, resulting in a positive energy balance. In addition, fat mass and obesity-associated gene variants, copy number variants in chromosomes and epigenetic modifications have shown positive associations with the risk of obesity among Asians. In this review highlights of prevalence and related ecological and genetic factors that could influence the rapid rise in obesity among Asian populations are discussed. Keywords Adolescents . Adults . Asia . Children . Ecology . Elderly . Epigenetics . Etiology . Genetic variants . Nutrition transition . Overweight . Obesity . Physical activity . Prevalence . Socio-economy Introduction Obesity, a main contributor to many metabolic diseases, is a public health concern of the twenty first century. Over the last three decades, the global obesity rate has doubled. In 2008, among adults over 20 years of age, approximately 1.4 billion were affected, of whom 35 % were overweight and 11 % were obese [1]. Without exception, Asian countries that were pre- viously better recognized for their undernourished populations are now serious contenders in the global obesity epidemic race. These increases have been mainly attributed to the rapid economic growth in Asia in the last three decades, which has led to socio-economic transition, increased food production, improved transportation systems, and reduced physical activity demands in the workplace due to substitution of mechanization; and together, these changes contribute to a positive energy balance [2, 3]. The WHO reported that 65 % of the global population is now either over- weight or obese (OW/OB), with more fatal conse- quences than being underweight [1]. Obesity is a mul- tifactorial disease that results from complex interactions between environmental and genetic factors [4]. Rapid economic growth that alters the cause and effect be- tween the risks of obesity [5], together with genetic differences [6] may be responsible for the drastic rise in body weight among Asians. This review attempts to provide an insight of the etiology of obesity from the ecological and genetic perspective of Asian cohorts to better understand and help tackle the problem. P. N. Chong : B. K. Poh (*) Nutritional Sciences Programme, School of Healthcare Sciences, Faculty of Health Sciences, Universiti Kebangsaan Malaysia, Jalan Raja Abdul Aziz, 50300 Kuala Lumpur, Malaysia e-mail: [email protected] B. K. Poh e-mail: [email protected] C.P. W. Teh UKM Medical Molecular Biology Institute, Universiti Kebangsaan Malaysia, Jalan Ya’acob Latiff, Bandar Tun Razak, 56000 Cheras, Kuala Lumpur, Malaysia M. I. Noor Department of Nutrition and Dietetics, Faculty of Health Sciences, MARA University of Technology, 42300 Puncak Alam, Selangor, Malaysia Curr Obes Rep (2014) 3:16–37 DOI 10.1007/s13679-013-0088-1
-
Upload
mohd-ismail -
Category
Documents
-
view
213 -
download
1
Transcript of Etiology of Obesity Over the Life Span: Ecological and Genetic Highlights from Asian Countries

ETIOLOGY OF OBESITY (MS WESTERTERP-PLANTENGA, SECTION EDITOR)
Etiology of Obesity Over the Life Span: Ecological and GeneticHighlights from Asian Countries
Pei Nee Chong &Christinal PeyWenTeh &BeeKoonPoh &
Mohd Ismail Noor
Published online: 15 January 2014# Springer Science+Business Media New York 2014
Abstract Obesity is a worldwide pandemic, and the preva-lence rate has doubled since the 1980s. Asian countries arealso experiencing the global epidemic of obesity with itsrelated health consequences. The prevalence of overweightand obesity are increasing at an alarming rate across all agegroups in Asia. These increases are mainly attributed to rapideconomic growth, which leads to socio-economic, nutritionand lifestyle transitions, resulting in a positive energy balance.In addition, fat mass and obesity-associated gene variants,copy number variants in chromosomes and epigeneticmodifications have shown positive associations with therisk of obesity among Asians. In this review highlightsof prevalence and related ecological and genetic factorsthat could influence the rapid rise in obesity amongAsian populations are discussed.
Keywords Adolescents . Adults . Asia . Children . Ecology .
Elderly . Epigenetics . Etiology . Genetic variants .
Nutrition transition .Overweight .Obesity . Physical activity .
Prevalence . Socio-economy
Introduction
Obesity, a main contributor to many metabolic diseases, is apublic health concern of the twenty first century. Over the lastthree decades, the global obesity rate has doubled. In 2008,among adults over 20 years of age, approximately 1.4 billionwere affected, of whom 35%were overweight and 11 % wereobese [1]. Without exception, Asian countries that were pre-viously better recognized for their undernourished populationsare now serious contenders in the global obesity epidemicrace. These increases have been mainly attributed to the rapideconomic growth in Asia in the last three decades, which hasled to socio-economic transition, increased food production,improved transportation systems, and reduced physicalactivity demands in the workplace due to substitution ofmechanization; and together, these changes contribute toa positive energy balance [2, 3]. The WHO reportedthat 65 % of the global population is now either over-weight or obese (OW/OB), with more fatal conse-quences than being underweight [1]. Obesity is a mul-tifactorial disease that results from complex interactionsbetween environmental and genetic factors [4]. Rapideconomic growth that alters the cause and effect be-tween the risks of obesity [5], together with geneticdifferences [6] may be responsible for the drastic risein body weight among Asians. This review attempts toprovide an insight of the etiology of obesity from theecological and genetic perspective of Asian cohorts tobetter understand and help tackle the problem.
P. N. Chong : B. K. Poh (*)Nutritional Sciences Programme, School of Healthcare Sciences,Faculty of Health Sciences, Universiti Kebangsaan Malaysia, JalanRaja Abdul Aziz, 50300 Kuala Lumpur, Malaysiae-mail: [email protected]
B. K. Pohe-mail: [email protected]
C. P. W. TehUKM Medical Molecular Biology Institute, Universiti KebangsaanMalaysia, Jalan Ya’acob Latiff, Bandar Tun Razak, 56000 Cheras,Kuala Lumpur, Malaysia
M. I. NoorDepartment of Nutrition and Dietetics, Faculty of Health Sciences,MARA University of Technology, 42300 Puncak Alam, Selangor,Malaysia
Curr Obes Rep (2014) 3:16–37DOI 10.1007/s13679-013-0088-1

Health Complications Linked to Obesity
Having an increased bodymass index (BMI) increases the riskof non-communicable diseases, such as heart disease andstroke, which are the main cause of death, diabetes, musculo-skeletal diseases and cancers [1]. Childhood obesity is ofspecial concern because it leads to obesity in adulthood,a shorter lifespan and disability. Obese children sufferfrom difficulty in breathing; are at risk of bone fracturesand hypertension; show early symptoms of cardiovascu-lar disease and insulin insensitivity; and display adversepsychological effects [1].
The 2007 National Survey of Children’s Health in UnitedStates revealed that obese children had limited physical activ-ity, scored poorly on examinations, had problem in schoolsand had higher incidences of absenteeism compared withnormal weight children [7]. Obese children commonly reporthaving problems staying focused; being hyperactive;displaying disorderly conduct; being depressed; having diffi-culty in learning; and developing slowly. Furthermore, obesechildren may suffer from diseases of the bone, joint andmuscle; asthma; allergy; headaches; and ear infections [7].
Many Asian studies have shown similar obesity-relatedcomplications as reported in Western countries [8–12]. Find-ings from a recent study in Malaysia revealed that 5.3 % ofOW/OB children were at risk of metabolic syndrome, whileno metabolic syndrome indicators were detected in normalweight children [9]. Based on ethnicity, Indian children ex-hibit higher risk of metabolic syndrome than Malays andChinese children [9].
The Obesity Scenario in Asia
Many of the Asian countries classified as low to middle-income countries are currently experiencing the ‘double bur-den’ of disease [1, 3]. These countries not only have tocontinue tackling infectious diseases and under-nutrition, butthey also have to counter the drastic increase of non-communicable disease risk factors, including overweight andobese, especially in urban areas. It is not uncommon to findunder-nutrition and obesity coexisting in the same country,community or even household [1]. Low-income families thatreside in urban settings have higher obesity risks comparedwith higher income families due to the easy accessibility ofcheap food [3], which is high in energy, sugar, fats and salt butpoor in nutrient quality [1]. Combination of a calorie-densediet that is low in nutrients and a sedentary lifestyle leads to anincrease in childhood obesity even while under-nutrition stillprevails in many Asian countries [1]. Hence, many Asiancountries are faced with new challenges to address the ‘doubleburden’ of disease [3].
India, for example, is one the Asian countries that is facingthe double burden of underweight and obesity. Underweightin India is a problem that cuts across all social and economiccategories, whereas overweight or obesity is a problem of thewealthier, urban women [13]. Similarly, in Vietnam, bothunderweight and overweight coexist [14]. In urban Hanoi,Vietnam, the overweight and obese prevalence is 28.6 %and 2.1 %, respectively; while the underweight preva-lence is 13.3 % [15]. The coexistence of underweightand overweight is partly due to ‘Doi moi’, which is thenational reformation of social and economic policy, andthe effect of removing the embargo on Vietnam by theUnited States government [16, 17].
Prevalence of Obesity in Asian Countries
China was once the world’s slimmest nation; however, overthe past two decade there is a drastic increase in prevalence ofoverweight and obesity [18–20]. Other countries in Asia haveshown similar trends of rising prevalence of overweight andobesity. Table 1 summarizes the findings of OW/OB for Asiancountries over the lifespan.
Prevalence Among Children and Adolescents
In China, within 25 years, the obesity prevalence in childrenrose from 0.2 to 8.1 % [18]. Among 7 to 17 year old childrenand adolescents, a study demonstrated an increase in BMIfrom 17.4 to 18.3 kg/m2 from 1991 to 2006, respectively [19].When comparing the sexes, an earlier study conducted in theyear 2000 had shown that the prevalence of OW/OB washigher in girls than boys [20]. However, a more recent studydemonstrated that boys had a higher increase in prevalence;the OW/OB tripled from 4.8 % in 1991 to 15.4 % in 2006,while in girls, it only increased from 5.4 to 11.0 % duringthe same period [19]. The escalating obesity rate in boys iscontributing to the growing childhood obesity prevalencein China [18].
Likewise, in Ernakulam, a district in southern India, theprevalence of overweight children had increased from 4.9 %in 2003 to 6.6 % in 2005 [28]. When comparing the sexes,among children aged 12 to 18 years old, boys had higher bodyweights, with 14.3 and 2.9 % of boys being overweight andobese compared with only 9.2 and 1.5 % of girls, respectively[6]. According to the International Obesity Task Force(IOTF), 18.9 % of girls and 20.6 % of boys in India wereoverweight and obese [24]. In Japan, studies have also report-ed an increased prevalence of obese children. Between1976 and 1980, obesity in boys and girls was 6.1 and7.1 %, but it increased to 11.1 and 10.2 % between 1996and 2000, respectively [23]. A recent study reported thatJapanese children increased their upper body weight
Curr Obes Rep (2014) 3:16–37 17

Tab
le1
Prevalence
ofoverweightand
obesity
amongvariousagegroups
inAsian
countries
Country
Yearof
study
Prevalence
ofoverweight(OW)
Prevalence
ofobesity
(OB)
Age
inyears(y)
Samplesize
Definition
ofOW/OB
Reference
A)Childrenandadolescents
i.Eastern
Asia
China
1985-2010
NA
Total:0.2%→
8.1%
Boys:11
%Girls:5
.2%
7y-18y
Boys:17,922
Girls:1
7,964
Working
Group
onObesity
inChina
(WGOC)criteria[21]
Song
etal.2013[18]
China
1991-2006
NA
*Boys:4.8%→
15.4
%*G
irls:5
.4%→
11.0
%7y–17y
NA
InternationalO
besity
Task
Force
(IOTF)
BMIcut-offs[22]
Cui
etal.2010[19]
China
2000
Bothsexes:6.4%
Bothsexes:1%
3.5y–
6.4y
262,738
NA
Liu
etal.2007[20]
India
2010
Boys:14.3
%Girls:9
.2%
Boys:2.9%
Girls:1
.5%
12y-18y
5,664
NA
Goyaletal.2010[6]
Japan
1976-2000
NA
Boys:6.1%→
11.1
%Girls:7
.1%→
10.2
%6y-14y
Boys:29,052
Girls:2
7,552
NA
Matsushita
etal.2004[23]
SouthKorea
2003
NA
*Boys:16.2
%*G
irls:9
.9%
NA
NA
NA
IOTF2003
[24]
Taiwan
2001-2002
Boys:15.5
%Girls:1
4.4%
Boys:14.7
%Girls:9
.1%
6y-12y
2,405
The
Departm
ento
fHealth
(DOH)childhood
obesity
expertpanelg
ender-and
age-specificcriteria[25]
Chu
&Pan2007
[10]
Taiwan
1980-1996
NA
*Boys:25.4
%→
28.0
%*G
irls:2
1.4%→
21.3
%12y-15y
3,346
NA
Chu
2001
[26]
ii.So
uth-CentralAsia
Ernakulam
,India
2003-2005
Boys:5.4%→
7.3%
Girls:4
.6%→
5.9%
Boys:1.7%→
2.5%
Girls:0
.9%→
1.3%
5y-16y
24,842
CentersforDisease
Control
andPreventio
n2000
for
BMIcut-offs[27]
Rajetal.2007[28]
India
2007-2008
NA
*Boys:20.6
%*G
irls:1
8.3%
NA
NA
NA
IOTF2008
[24]
Iran
2011
Boys:16.7
%Girls:1
3.3%
Boys:9.0%
Girls:5
.6%
2y-5y
1,035
WHOBMI-for-age[29]
Nouhjah
etal.2011[30]
Pakistan
2008-2009
Boys:8.0%
Girls:1
8.0%
Boys:15.0
%Girls:8
.0%
9y-18y
501
WHOBMI-for-age[29]
Ahm
edetal.2013[31]
iii.S
outh-EastA
sia
Indonesia
2011
Urban
Bothsexes:5.6%
Rural
Bothsexes:3.2%
Urban
Bothsexes:5.1%
Rural
Bothsexes:1.8%
0.5y-12y
7,211
Forage0–5yearsold,WHO
grow
thstandards[32],for
age5–19
years
old,WHOBMI-for-age[29]
Sandjajaetal.2013[33]
Peninsular
Malaysia
2001-2002
Bothsexes:11.0
%Bothsexes:9.7%
6y-12y
11,242
WHOBMI-for-age[29]
Ismailetal.2006
[34]
Peninsular
Malaysia
2007-2008
Bothsexes:12.5
%Bothsexes:13.6
%6y-12y
10,009
WHOBMI-for-age[29]
Ismailetal.2009
[35]
Malaysia
2011
NA
Bothsexes:6.0%
5y-17y
NA
NA
Khoretal.2012[36]
Malaysia
2010-2011
Urban
Bothsexes:9.7%
Rural
Bothsexes:9.9%
Urban
Bothsexes:12.7
%Rural
Bothsexes:8.2%
0.5y-12y
3,542
Forage0–5yearsold,WHO
grow
thstandards[32],for
age5–19
yearsold,WHO
BMI-for-age[29]
Pohetal.2013[37]
KualaLum
pur,Malaysia
2011
Boys:34.4
%Girls:2
7.2%
Boys:4.3%
Girls:2
.3%
9y-12y
402
WHOBMI-for-age[29]
Wee
etal.2011[9]
Singapore
1975-1993
Boys:1.6%→
15.2
%Girls:1
.1%→
12.9
%NA
6y-16y
NA
Cheah
1997
[38]
18 Curr Obes Rep (2014) 3:16–37

Tab
le1
(contin
ued)
Country
Yearof
study
Prevalence
ofoverweight(OW)
Prevalence
ofobesity
(OB)
Age
inyears(y)
Samplesize
Definition
ofOW/OB
Reference
Thailand
1991-2004
NA
Bothsexes:5.8%→
6.7%
6y-12y
NA
NA
Aekplakorn&
Suwan
2009
[39]
Thailand
2004
NA
Bothsexes:8.3%
2y-10y
4,610
NA
Firestoneetal.2011[40]
Thailand
2010
Bothsexes:9.5%
Bothsexes:4.9%
7y-12y
7,096
WHOBMI-for-age[29]
Sengmeuanga
etal.2010
[41]
Thailand
2011
Urban
Bothsexes:6.9%
Rural
Bothsexes:8.0%
Urban
Bothsexes:11.8
%Rural
Bothsexes:5.9%
0.5y-12.9y
3,119
Forage0–5yearsold,WHO
grow
thstandards[32],for
age5–19
yearsold,WHO
BMI-for-age[29]
Rojroongw
asinkuletal.
2013
[42]
Vietnam
1992–1993;
2002
NA
*Boys:1.4%→
2.0%
*Girls:1
.4%→
1.6%
2y-17y
Year1992:
24,068
Year2002:1
58,019
CentersforDisease
Control
andPreventio
n2000
for
BMIcut-offs[27]
Tuanetal.2008[14]
HoChi
MinhCity,V
ietnam
2004-2009
Bothsexes:12.5
%→
16.7
%Bothsexes:1.7→
5.1%
12y-17y
759
InternationalO
besity
Task
Force
(IOTF)
BMIcut-offs[22]
Hongetal.2013[43]
HoChi
MinhCity,V
ietnam
2010
Boys:22.0
%Girls:1
3.3%
Boys:5.4%
Girls:1
.3%
11y–14y
1,989
InternationalO
besity
Task
Force
(IOTF)
BMIcut-offs[22]
Nguyenetal.2013[44]
Vietnam
2013
Bothsexes:6.7%
Bothsexes:2.0%
11y-14y
1,528
NA
Leetal.2013[45]
Vietnam
2011-2012
Urban
Bothsexes:15.7
%Rural
Bothsexes:4.5%
Urban
Bothsexes:18.0
%Rural
Bothsexes:2.0%
0.5y-11.9y
2,872
Forage0–5yearsold,WHO
grow
thstandards[32],
forage5–19
yearsold,WHO
BMI-for-age[29]
Nguyenetal.2013[46]
B)Adults
i.Eastern
Asia
China
1992
to2002
NA
*Bothsexes:14.6→
21.8
%18y-59y
288,553
World
Health
Organization
classifications
[47]
Wangetal.2006[11]
China
2000
to2001
Men:24.8%
Wom
en:2
9.7%
Men:1
2.7%
Wom
en:11.5%
35y-74y
15,540
World
Health
Organization
classifications
[47]
Reynoldsetal.2007[48]
ii.So
uth-CentralAsia
Chattisgarhstate,India
2011
Bothsexes:19.9
%Bothsexes:8.6%
18y-50y
688
World
Health
Organization
classifications
[47]
Singhetal.2012[49]
Rasht,Iran
2010
Men:4
3.4%
Wom
en:4
2.8%
Men:1
2.2%
Wom
en:2
5.1%
>18y
12,251
NA
Maddahetal.2010[50]
Northern,Iran
2013
NA
Bothsexes:24
%15y-65y
2,452
NA
Veghariaetal.2013[12]
iii.S
outh-EastA
sia
Selangor,M
alaysia
2009
NA
Wom
en:1
6.7%
20y-59y
972
World
Health
Organization
classifications
[47]
Sidik&
Ram
pal2
009[51]
Malaysia
2004
NA
Men:9
.6%
Wom
en:1
3.8%
15y-93y
16,127
World
Health
Organization
classifications
[47]
Ram
paletal.2007
[52]
Malaysia
2011
Bothsexes:33.6
%Bothsexes:19.5
%≥1
8y4,428
World
Health
Organization
classifications
[47]
Moham
udetal.2011[53]
Malaysia
2002-2003
Bothsexes:26.7
%Bothsexes:12.2
%18y-59y
10,216
World
Health
Organization
classifications
[47]
Azm
ietal.2009
[54]
TanjongPagar,Singapore
2007
NA
*Men:3
3.0%
*Wom
en:3
4.0%
40y-81y
942
NA
Sabanayagam
etal.2007
[55]
Thailand
2004
NA
Men:2
2.4%
Wom
en:3
4.3%
18y-59y
NA
NA
Aekplakorn&
Suwan
2009
[39]
Curr Obes Rep (2014) 3:16–37 19

Tab
le1
(contin
ued)
Country
Yearof
study
Prevalence
ofoverweight(OW)
Prevalence
ofobesity
(OB)
Age
inyears(y)
Samplesize
Definition
ofOW/OB
Reference
Thailand
2004-2005
NA
*Men:3
5.0%
*Wom
en:4
4.9%
18y-70y
6,445
World
Health
Organization’s
Asian
cut-offs[56]
Jitnarin
etal.2010[57]
Vietnam
1992–1993;
1997–1998;
2001–2002
Bothsexes:
2.0%→
5.7%
Bothsexes:0%
>18y
Year1992:
11,982
Year1997:
15,975
Year2001:
94,656
World
Health
Organization
classifications
[47]
Nguyenetal.2007[58]
Vietnam
1992;
2002
NA
Bothsexes:
*2.0
%→
5.2%
18y-65y
Year1992:
24,068
Year2002:1
58,019
World
Health
Organization
classifications
[47]
Tuanetal.2008[14]
HoChi
MinhCity,V
ietnam
2004
Bothsexes:26.2
%Bothsexes:6.4%
20y-60y
1,488
World
Health
Organization’s
Asian
cut-offs[56]
Cuong
etal.2007[16]
C)Elderly
i.Eastern
Asia
Shangdong,China
2010-2011
NA
Bothsexes:13.1
%>60y
1,538
NA
Song
etal.2013[59]
China
1992
-2002
Bothsexes:
20.2
%-24.3%
Bothsexes:6.7-
8.9%
>60y
NA
Chinese
BMIcut-offs[60]
Wangetal.2006[11]
HongKong
1998
-2000
Men:8
.0%
Wom
en:1
4.4%
Men:1
2.3%
Wom
en:2
8.1%
>65y
56,167
World
Health
Organization’s
Asian
cut-offs[56]
Schoolingetal.2006[61]
Taiwan
1998
Men:2
4.8%
Wom
en:2
9.7%
Men:1
2.7%
Wom
en:11.5%
>65y
1,093
Chinese
adultsBMI
criterion
[62]
Lin
etal.1999[63]
ii.So
uth-CentralAsia
SouthIndia
1994
NA
Urban
men:7
.7%
Ruralmen:1
.7%
Urban
wom
en:
24.2
%Ruralwom
en:
4.9%
>60y
Urban:8
73Rural:5
88NA
Ram
achandranetal.1994
[64]
Iran
2009
Bothsexes:28.9
%Bothsexes:11.7
%>60y
Men:9
17Wom
en:1
,045
NA
Nem
atyetal.2009[65]
Iran
1999-2000
NA
Men:6
.9%
Wom
en:1
5.5%
>60y
4,380
NA
Bakhshi
etal.2011[66]
iii.S
outh-EastA
sia
Malaysia
2006
Men:2
9.2%
Wom
en:3
0.3%
Men:7
.4%
Wom
en:1
3.8%
>60y
4,746
World
Health
Organization
classifications
[47]
Suzana
etal.2012[67]
Singapore
NA
Bothsexes:18.6
%Bothsexes:7.4%
>60y
4,371
NA
Otsbyeetal.2011[68]
Thailand
2004-2007
Men:1
9.6%
Wom
en:2
6.6%
Men:2
.9%
Wom
en:8
.3%
>60y
Men:7
,742
Wom
en:8
,255
World
Health
Organization’s
Asian
cut-offs[56]
Vapattanawongetal.2010
[69]
Hanoi,V
ietnam
2004
Men:2
6.9%
Wom
en:3
1.2%
Men:0
%Wom
en:2
.6%
>65y
Men:1
40Wom
en:1
22World
Health
Organization’s
Asian
cut-offs[56]
Wallsetal.2009[15]
*Com
bine
prevalence
foroverweightand
obese.NA=Not
available
20 Curr Obes Rep (2014) 3:16–37

between 0.7 to 1.3 kg/decade and 0.2 to 1.0 kg/decade inboys and girls, respectively [70].
In Vietnam, a small increase in prevalence of overweightfrom 1.4 to 1.8 % from 1992 to 2002 had been reported [14].In Ho Chi Minh City, a 5-year prospective cohort studyreported a rising prevalence of OW/OB among adolescents.From the first year to the fifth year of the study, the prevalenceof overweight increased from 12.5 to 16.7 %, and the preva-lence of obesity increased from 1.7 to 5.1 % [43]. In Ho ChiMinh City, the overweight prevalence in children and adoles-cent was 17.8 %, while the obesity prevalence was 3.2 % [44].In Bac Giang city, the northern city of Vietnam, the prevalenceof overweight and obesity among adolescents was 6.7 and2.0 %, respectively [45].
In Malaysia, Ismail et al. [35] using WHO (2007) criteriareported a rising trend of overweight and obesity among chil-dren aged 6 to 12 years old in Peninsular Malaysia from 11.0and 9.7 % in 2002 to 12.5 and 13.6 % in 2008, respectively. Inanother study, the prevalence of obesity was 6.7 % for childrenaged 5.0 to 9.9 years old, 6.3 % for children aged 10.0 to14.9 years old and 4.9 % for children aged 15.0 to 17.9 yearsold [36]. A study in Peninsular Malaysia using IOTF criteriareported a prevalence of overweight of 10.5 % and obese of5.9 % among children aged 7 to 12 years old [34].
According to the IOTF, 9.9% of girls and 16.2% of boys inSouth Korea were OW/OB [24]. In Thailand, from 1997 to2001, the prevalence of obesity for children aged 2 to 5 yearsold rose from 5.8 to 7.9 %. For children aged 6 to 12 years old,the obesity prevalence increased from 5.8 to 6.7 % [39].Recent data indicate an obesity prevalence in children of8.3 % [40]. In Northeast Thailand, the prevalence of OWand OB children are 4.9 % and 9.5 %, respectively [41]. InTaiwan, the overweight and obesity prevalence in children are15.5 and 14.7 % in boys and 14.4 and 9.1 % in girls, respec-tively. The obesity prevalence is highest in the southern regionfor boys and the central region for girls. The obesity preva-lence is lowest in mountain areas for boy and southern areasfor girls [10]. Among children aged 2 to 5 years old in Ahwaz(Iran), the prevalence of overweight and obesity are 15 and7.3 %, respectively [30]. In Pakistani school children, theprevalence of overweight and obesity are 8 and 12 %, respec-tively [31].
More recently, the South East Asian Nutrition Surveys(SEANUTS) were conducted in four countries, Indonesia,Malaysia, Thailand and Vietnam, involving some 16,744children between the ages of 0.5 to 12 years old [71••]. Whencomparing data from urban areas, Vietnam had the highestobesity rate of 18.0% [46], followed byMalaysia 12.7% [37],Thailand 11.8% [42], and Indonesia 5.1 % [33]. In contrast, inthe rural settings, Malaysia had the highest obesity rate,followed by Thailand, Vietnam and Indonesia; with preva-lence of 8.2 % [37], 5.9 % [42], 2.0 % [46], and 1.8 % [33],respectively.
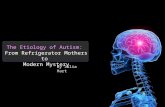
Figure 1 presents the obesity prevalence among childrenand adolescents in Asian countries. In Eastern Asia, Taiwanchildren aged 6 to 12 years [25] had the highest obesity rate(12.1 %) compared to Japan at 10.7% [23] and China at 8.1 %[18]. Among the South-Central Asian countries, Pakistan hadthe highest obesity rate in children aged 9 to 18 years at 11.6%[31] compared to India at 2.3 % [28] and Iran at 7.3 % [30].Between Eastern and South-Central Asia, direct comparisonsbetween countries cannot be done due to the different agegroups and BMI classification criteria used by each country.However, the South-East Asian countries were comparable,andMalaysia [37] had the highest obesity rate (11.8%) amongchildren 0.5 years to 12 years, followed by Thailand (7.8 %)[42], Vietnam (5.0 %) [46], and Indonesia (3.5 %) [33].
Prevalence Among the Adult Population
In China, the OW/OB prevalence increased from 20.0 to29.9 % between 1992 and 2002. Men aged 18 to 44 yearsold and women aged 45 to 59 years old had the highestincreases in obesity rates, which were 1.6 and 1.0 %, respec-tively [11]. The OW/OB prevalence in northern region was41.6 % compare to 16.5 % in southern region [48]. Similarly,India while facing malnutrition throughout the nation, nowhas to address OW/OB and their consequences [72]. In Chhat-tisgarh state, India, the prevalence of overweight and obesityamong adults were 19.9 and 8.6 %, respectively [49].
Likewise, the OW/OB prevalence in Vietnam amongadults aged 18 to 65 years old [14] more than doubled from1992 to 2002, increasing from 2.0 to 5.7 % [14, 58]. Theprevalence of OW/OB was higher Ho Chi Minh City, at 26.2and 6.4 %, respectively; however, among Vietnamese adults,females have a higher prevalence of OW/OB (33.6 %) com-pared with males (31.6 %) [16].
In Malaysia, a population-based cross-sectional study byRampal et al. [52] reported that 11.7 % of Malaysians aged15 years and older were obese. The Malaysian Adults Nutri-tion Survey (MANS) also reported that 26.7 and 12.2 % ofadults aged 18 to 59 years old were overweight and obese,respectively [54]. Like most other Asian countries, theprevalence of obesity in Malaysian females (22.5 %), ishigher compared with males (14.1 %). Of note, amongadults younger than 30 years old, more than 43 % areeither OW/OB, with prevalence of 20 % and 13.9 %,respectively [53]. In contrast, in Singapore, the preva-lence of OW/OB among people aged 40 to 81 years oldwas quite similar between genders, 33 and 34 % in malesand females, respectively [55].
In northern Iran, the prevalence of obesity is relativelyhigh, at 12.2 % in males and 25.1 % in females [50]. Subse-quently, a more recent study reported that the obesity preva-lence in Iran is 24 % [12]. Like other Asian countries, Thai-land is also facing an increased prevalence of obesity in adults.
Curr Obes Rep (2014) 3:16–37 21

Among males, the prevalence of obesity increased from13.0 to 18.6 % and then to 22.4 % from 1991 to 1997and then to 2004, respectively. Similar to other studies,the prevalence in adult females is higher than in malesand increases from 23.2 to 29.5 % and then to 34.3 %,respectively [39]. A more recent study of Thailand re-ported that the OW/OB prevalence for adults aged be-tween 18 to 70 years old is 35.0 % for males and evenhigher at 44.9 % in females [57].
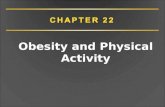
In 2008, based on a WHO report of adults aged20 years and above, Fig. 2 was generated, and showsthat the United Arab Emirates had the highest obesityrate (33.7 %), followed by Iran (21.6 %). Among theSouth-East Asian countries, Malaysia had the highestrate of obesity (14.1 %), followed by Thailand (8.5 %).India and Vietnam have the lowest obesity prevalence inAsia, at 1.9 and 1.6 %, respectively [73].
Prevalence Among the Elderly
Taiwan, Hong Kong, Iran, and Malaysia have a relativelyhigher prevalence of obesity among the elderly in Asia. Theprevalence of obesity in elderly Taiwanese males and femalesis 12.7 % and 11.5 %, respectively [63]. In Hong Kong, theprevalence of obesity in elderly males and females is12.3 and 28.1 %, respectively [61]. The prevalence ofobesity in elderly Iranians is 6.9 and 15.5 % for malesand females, respectively [66]. Likewise, the prevalenceof obesity in elderly Malaysians is 7.4 and 13.8 % formales and females, respectively [67].
In contrast, countries such as China, Vietnam, Thailand andSingapore have relatively lower prevalence of obesity amongthe elderly. In China, although the prevalence of obesity iscomparatively low, there is a steady rise from 6.7 to 8.9 %from year 1992 to 2002 [11]. In Singapore, the prevalence of
Fig. 1 Prevalence of obesity among children and adolescents in Asia.1Working Group on Obesity in China (WGOC) criteria [21]. 2The De-partment of Health (DOH) childhood obesity expert panel gender- and
age-specific criteria [25]. 3WHO BMI-for-age [29]. 4WHO growth stan-dards for age 0–5 years old [32], WHO BMI-for-age for age 5–19 yearsold [29]. 5Information not available for criteria of obesity classification
Fig. 2 Prevalence of obesity among Asian adults aged 20 years plus. Source: WHO 2013 [1]
22 Curr Obes Rep (2014) 3:16–37

obesity in the elderly is 7.4% [68]. In Thailand, the prevalenceof obesity among elderly men and women is 2.9 and 8.3 %,respectively [69]. In Hanoi, Vietnam, the prevalence of obe-sity among the elderly is quite low, at approximately 2.6 % forfemales and 0 % for males [15].
Figure 3 demonstrated a comparison of the prevalence ofobesity among the elderly populations of some Asian coun-tries. Direct comparisons between countries are not possibledue to the different BMI classification criteria used. Nonethe-less, Hong Kong had the highest obesity rate (21.9 %) [61]compared to other Asian countries. On the other hand, bothThailand [69] and Hanoi [15] had the lowest obesity rateamong the elderly.
Ecological Factors Influencing Obesity in Asia
With escalating prevalence of overweight and obesity all overAsia, it is of utmost importance to understand the etiology ofobesity, as an in-depth understanding of its related factors maylead to better strategies to fight the increase in prevalence andprevent the impending health consequences of obesity.
Figure 4 shows a conceptual framework linking the ecologicaland genetic factors that influences the development of obesity.
Socio-economic Transition
Table 2 shows the GDP per capita and literacy rate for Asiancountries. From 1985 to 2011, all Asian countries experiencedrapid economic development, China in particular, recordedthe highest increase in the GDP per capita, which rose fromUSD290 to USD5445 followed by Korea with a USD847growth in GDP per capita over 26 years. Among other Asiancountries, Singapore and Japan had the highest incomes, withGDP per capita of USD46,241 and USD45,903, respectively[74]. In tandem with rising household income, most Asiancountries show an increment in literacy rate from 10 to 60 %within two to three decades among population aged 15 yearsabove. Among Asian countries, both Iran and India have thegreatest increment of literacy rate at 64 and 53%, respectivelywithin 30 years [75]. The massive increase in householdincome, education level, and literacy rate in Asia has broughtabout changes in the traditional eating habits, and coupled
Fig. 3 Prevalence of obesity among the elderly in Asia. 1Chinese BMI cut-offs [60]. 2World Health Organization’s Asian cut-offs [56]. 3Chinese adultsBMI criterion [62]. 4World Health Organization classifications [47]. 5Information not available for criteria of obesity classification
Curr Obes Rep (2014) 3:16–37 23

with reduced physical activity due to heavy mechanization,has been partly implicated for the current obesity dilemma.
In China, the 1766 % increase in GDP per capita [74]within 25 years has led to changes in dietary intake andphysical activity of its population [79]. A recent study froma northern city of Vietnam demonstrated OW/OB is moreprevalent among adolescents who come from families withhigher incomes and higher food expenditures [45].
Chinese parents are also able to provide energy-densefoods in excess of the requirements due to high availabilityof low-cost food that is energy dense yet nutritional insuffi-cient [3], and luxury entertainments lead to a sedentary life-style. Thus, children and adolescents from higher incomefamilies have a higher prevalence of OW/OB [19].
In contrast to popular belief, Chinese adults from low-income and rural areas had the fastest increase in the
Fig. 4 Conceptual framework describing the etiology of obesity
24 Curr Obes Rep (2014) 3:16–37

overweight rate, suggesting that the problem is not confined tothe urban setting alone [80]. Similarly, there was a greaterincrease in the prevalence of OW/OB in children from the lowsocioeconomic status group compared with the moderate andhigh socioeconomic status groups [81]. Unlike other coun-tries, the prevalence of obesity in Pakistani school childrenwho came from the upper tertile of socioeconomic status waslower compared with children from the lower socioeconomicstatus. This discrepancy is likely because children from highsocioeconomic status were more health conscious and thusconsume healthier diets and probably lead more active life-styles than the children from low socioeconomic status [31].
In northern Iran, BMI is positively correlated to educationallevel in men. In women, however, a U-shaped association wasfound between education level and BMI. The risk of obesitywas 2.044 (P=0.001) in the uneducated compared to highschool or college-educated subjects [12]. Among Thai fe-males, education status, marital status and occupation arehighly related to weight status. OW/OB risk was highamongst single females (OR=1.6; 95 % CI=1.2, 2.1) andsemi-professional females (OR=3.3; 95 % CI=1.0, 11.4)
and the prevalence of obesity was lower in educated women(OR=0.5; 95 % CI=0.3, 0.9) [57].
The prevalence of OW/OB is higher for women who live inhigh-income districts than in low-income districts, 70.7 and65.3 %, respectively. For men, however, the area of living isnot associated with OW/OB [50]. In Thailand, men who earnan annual income more than USD3875 were 1.8 times morelikely to be OW/OB compared with the lowest incomeearners, of less than USD508. Non-routine manual jobworkers were 1.6 times more at risk to be OW/OB thanmanual job workers [57]. In Malaysia, the prevalence ofobesity was highest in the income group of USD454 toUSD1061 compared with those whose income was less thanUSD454 or more than USD1061. The prevalence of over-weight was also highest among those who had a primaryeducation level compared with their counterparts with second-ary and tertiary education level [54].
In contrast, socioeconomic status indicators had no associ-ation with OW/OB in Singaporean man; meanwhile socioeco-nomic status indicator had negative association with OW/OBin women. Among Singaporean women, the odds ratio of
Table 2 GDP per capita (current USD), literacy rate, fixed broadband internet subscribers, motor vehicle per 1000 people, and percentage of total urbanpopulation in Asian countries
GDP per capita1
(current USD)Literacy rate2
(% of people ages 15and above)
Fixed broadband internetsubscribers3
Motor vehicle per1000 people4
Percentage of totalurban population5
Country Year1995
Year2011
Change%
Year1 9 7 9 -1985
Year2 0 0 5 -2010
Change%
Year2001
Year2011
Change%
Year2003
Year2010
Change%
Year1961
Year2011
Change%
Eastern Asia
China 293 5,445 1,766 66 94 44 336,280 156,487,000 46,435 15 56 285 16.6 50.5 205
Japan 11,466 45,903 300 - - 3,835,000 34,917,822 811 581 591 2 64.2 91.1 42
Korea 2,368 22,424 847 - - 7,806,000 17,859,003 129 303 363 20 28.6 83.2 191
South-Central Asia
India 302 1,509 400 41 63 54 50,000 13,350,000 26,600 12 18 53 18.1 31.3 73
Iran 3,671 4,526 23 53 85 63 661 1,772,867 268,110 - 128 - 34.4 69.1 101
South-East Asia
Indonesia 520 3,495 573 67 93 38 15,000 2,736,379 18,143 36 60 66 14.8 50.7 242
Malaysia 2,016 9,977 395 70 93 34 4,000 2,147,800 53,595 272 361 33 27.3 72.7 167
Philippines 569 2,370 317 83 95 15 10,000 1,791,000 17,810 34 30 −11 30.6 48.9 60
Singapore 6,960 46,241 564 83 96 16 151,000 1,329,900 781 133 149 12 100.0 100.0 0
Thailand 743 4,972 569 88 94 6 1,613 3,496,000 216,639 146 157 8 19.8 34.1 72
Vietnam 239 1,407 488 84 93 11 - 3,838,206 - - - - 15.0 31.0 106
Western Asia
United ArabEmirates
20099 45653 52 71 90 26 8,374 866,968 10,253 - - - 73.9 84.3 14
Source:1World Bank 2013 [74]2World Bank 2013 [75]3World Bank 2013 [76]4World Bank 2013 [77]5World Bank 2013 [78]
Curr Obes Rep (2014) 3:16–37 25

OW/OB for those with a lower education level was 2.5 com-pared with women who had a higher education level. Singa-porean women earning less than USD784 per month were 2.5times more likely to become OW/OB compared with womenwho earn more than USD784 per month. Women who residein small and medium size apartments were 1.8 times morelikely to be OW/OB compared with women who reside inlarger apartments or private houses [55].
In Taiwan, the likelihood of becoming obese varies amongthe sexes, education levels, ethnic groups, and areas they livein. Women with low socioeconomic status who reside in themost affluent areas have an increased risk of obesity comparedwith women with high socioeconomic status. This is becausewomen with low socioeconomic status residing in affluentareas have a reduced ability to cope with their living environ-ment where fresh foods and whole grains are usually expen-sive. They live on cheap processed foods high in calories, thusincreasing the risk of obesity. In rural areas, men with 13 yearsor more of education had lower risk of obesity, implying thatthey were more successful at managing a disadvantaged en-vironment compared to those who had less than six years ofeducation [82].
Rapid Urbanization
In Asia, the obesity pandemic is more prevalent in the urbansetting due to the availability of different kinds of foods withan enormous variety of refined carbohydrates and processedfoods that are high in saturated fat and low in fiber content [2].Moreover, aggressive marketing strategies and mass mediahave introduced a greater range of foods and make it moreaccessible and cheaper, such as fast food [3].
According to the World Bank [78], from 1961 until2011, all the Asian countries experienced a rapid incre-ment in the percentage of urban population (Table 2). Incomparison to other Asian countries, Indonesia and Chi-na were both top of the list, at 241 and 204 %, respec-tively. They were followed by, Korea, Malaysia, Vietnamand Iran, which had at least more than 100 % incrementof urban population. In the year 2011, many countries inAsia had more than half of their population residing inurban areas. In Singapore 100 % of its population residesin urban areas, whereas Japan have 91 % of the popula-tion living in urban areas. In countries like the UnitedArab Emirates, Korea, Malaysia, Iran, China and Philip-pines, between 50 to 80 % of their populations reside inurban areas [78].
Highly urbanized provinces in China, such as Beijing,are facing the challenges of increased body weightamong its residents. Adolescents residing in urban andsuburban areas are at higher risk of being OW/OB.Highly convenient public transportation system and easyaccessibility to commercial food products and restaurants
are affecting the lifestyle of adolescents. Moreover, theirparents are usually busy at work; hence, adolescents mayeat out, especially at fast food restaurants, and consumefoods that are high in fat. In addition, urban adolescentsspend more time doing homework [83].
The rate of increase in BMI of the urban population isfaster than the rural population [14]. In Vietnam, urbanpopulations were 1.79 times more likely to be over-weight than the rural populations [58]. Between 2 to65 years old, the prevalence of OW/OB in urban areaswas 8.2 % compared to 2.5 % in rural areas. AmongVietnamese children aged 6 to 15 years old, the risk ofurban children being OW/OB were fivefold higher thanrural children, 6.2 and 1.2 %, respectively. The increasedOW/OB risk among urban Vietnamese children occurredfaster than in rural children. This difference may bebecause the urban areas had faster socioeconomic growththan the rural areas [17]. Despite this, Vietnamese urbanadults had a lower prevalence of OW/OB than other eastand Southeast Asian countries [16]. In the Ernakulamdistrict of India, the prevalence of overweight childrenin urban schools was higher than in rural schools(8.66 % and 3.75 %, respectively). This same trend isseen among adults in Northern Iran, where obesity riskwas 1.668-fold greater (P=0.001) in urban areas com-pared with rural areas [12]. This trend was mainly due toimproper urban planning and the rapid growth of auto-mated transport [28].
In Thailand, urban children have a 2.66-fold higher likeli-hood of becoming obese compared with rural children. Snacksare highly promoted in Thailand, thus children in urban areashave greater exposure to media that advertise snacks andfoods that have low nutritional quality [40].
Among Thai adults, urban males were at 1.3 timeshigher risk for OW/OB compared with their rural coun-terpart. This may be ascribed to the more sedentary life-style and the changes of dietary habits and food choicesof the urban residents [57].
In contrast with other Asian countries, a recent survey inJapan to investigate the determinants that lead to the child-hood OW/OB differences in rural and urban areas reporteddifferent results compared with the other Asian countries.The study demonstrated that rural children were signifi-cantly more OW/OB than urban children. This findingmay be attributed to lower physical activity, particularlythe reduced time spent walking to school compared withtheir urban counterparts [84].
Thus, to address the obesity challenge in urban areas, oneimportant measure is to have scientific urban planning, in-cluding streets that are well connected to every part of the areawith specific places for pedestrians and cyclists; well-maintained parks; mixed land use; compact and modularorganization; and a healthy food environment [85].
26 Curr Obes Rep (2014) 3:16–37

Lifestyle Transition
Technological advancements have minimized the need forvigorous physical activity in the workplace, during householdchores, and during traveling, and these advances are largelyresponsible for the increase in sedentary pastimes such aswatching television, playing online games, and surfing theInternet [86]. The combination of increased energy consump-tion and reduced energy expenditure accounts for the primarydetrimental risk factor for Asian populations [2] in developingeconomies. Physical inactivity leads to a low metabolic rateand poor physical fitness, which is attributed to increasedbody weight and an elevated risk of non-communicablechronic diseases [87].
The increasing percentage of households with televisions,fixed broadband Internet subscription, and motor vehicles aregood indicators of the lifestyle transition among Asian popu-lations and lead toward an increasingly sedentary lifestyle.Table 2 also shows the number of Internet subscribers andmotor vehicle owners in Asian countries, while Fig. 5 indi-cates the percentage of Asian households with television.
The reduction in physical activities in urban areas [72] iscaused by a better transportation system, and a shift of thelabor market has drastically reduced the physical activityamong urban residents [3]. From the World Bank report,approximately 90 % of Asian households owned a televisionin the year 2011. In countries such as Japan, Korea, Thailand,Iran, and United Arab Emirates, 99, 99, 98, 97, and 96 % ofhouseholds have a television at home, respectively [76]. Inother countries, such as India, Indonesia, and the Philippines,at least 60 to 74 % of households own televisions [76].
In addition, Asian countries showed a dramatic increase of128 % in Internet users from 2001 to 2011. Iran and Thailandhad the greatest increases, 268,111 and 216,639 %, respec-tively, in Internet subscribers compared with other Asiancountries. In contrast, Korea had the smallest increase of128 %, followed by Singapore (780 %) and Japan (810 %).
Within the same period, Asian countries such as China, India,Indonesia and Malaysia recorded moderate increases in inter-net subscribers, ranging from 17,810 to 46,434 % [76].
Between the years 2003 and 2010, all Asian countriesexcept the Philippines reported increased motor vehicle own-ership. In particular, China topped the list with a 285 %increase in motor vehicle ownership, corresponding to anincrease from 15 motor vehicles per 1000 people in 2003 to77 motor vehicles per 1000 people in 2010. Other countries,such as Indonesia and India, also had at least 52 to 66 %increases in motor vehicle ownership. Countries such as Ma-laysia, Korea, Singapore, and Thailand had relatively lowerincreases inmotor vehicle ownership, with 33, 20, 12, and 7%increases, respectively, over a 7-year period. Among Asiancountries, Japan had the lowest motor vehicle ownershipincrease of only 2 % [77] (Table 2).
The World Bank report for the year 2011, clearly demon-strated a high ownership of household televisions, a dramaticincrease in Internet subscribers and an increase in motorvehicle ownership in Asia over a 7 to 10 year period. Thisphenomenon signifies a drastic lifestyle transition in Asiancountries that had shifted from a largely outdoor lifestyle withphysically demanding activities to a more sedentary lifestylethat requires very low energy expenditure; this transition isconsidered to be a contributing factor toward the obesityepidemic in Asia. This can be evidenced in the richer Viet-namese families, who can provide a more comfortable life-style, such as having numerous household electronic appli-ances that replace physical work and electronics such ascomputer games, internet and television, which induce seden-tary lifestyle and lead to the high occurrence of OW/OB [89].
The Lancet Physical Activity Series Working Group in2012 reported that globally, 31.1 % of adult were not physi-cally active; the physical activity rate ranged from 17.0 % inSoutheast Asia to approximately 43 % in America and easternMediterranean countries [90]. Figure 6 presents the preva-lence of physical activity insufficiency in Asian populations
Fig. 5 Percentage of Asian households with television. Source: WDI 2013 [88]
Curr Obes Rep (2014) 3:16–37 27

aged 15 years and above based on the global status report onnon-communicable diseases in the year 2008 [91]. Japan(65.3 %) had the highest physical activity insufficiency ratein Asian countries. Among the South-East Asian countries,Malaysia had the highest rate of physical activity insufficiency(60.5 %). Physical inactivity increases with older age, is morecommon in females and is increasing in high-income popula-tions. As many as 80% of adolescents aged 13 to 15 years oldwere involved in moderate to vigorous physical activity forless than one hour per day [90].
In Hong Kong, a study of year 1 and year 3 Chineseundergraduate students reported that 31 % of the participantswere not physically active [92]. Factors such as being female,not a university resident, studying in the Faculty of Arts, andthose in poor or very poor health (self-reported) were reasonsfor being physically inactive. The most frequent answers fornot doing physical activity were ‘no time’ and ‘not interested’.Ng et al. [93] reported a low level of physical activity, partic-ularly among urban females in the United Arab Emirates.In Taiwan, among adolescents aged 13 to 16 years old,those who watched television for at least 2 hours perweekday and slept less than 7.75 hours per day were atgreater risk of obesity [94].
In Malaysia, Ismail et al. [95] reported that Indian men andwomen recorded physical activity levels that were higher thantheir Malay and Chinese counterparts, and that rural popula-tion was relatively more active than urban population. TheMalaysian Adults Nutrition Survey (MANS) conducted in2002 and 2003 reported that most of the subjects spent 74 %of their day engaged in sedentary activities, for instancesleeping or lying down [96]. Approximately 15 % of theirtime, they were doing light intensity activities, and thosesubjects were engaged in moderate to vigorous intensity ac-tivities for only 10 % of the day. As little as 14 % of subjects
had a sufficient amount of exercise. In addition, an earlierstudy also indicated that within two decades, the motor vehi-cle ownership had risen threefold, and TV ownership hadincreased at least twofold [97]. The drastic increase of thesetwo indicators signified the sedentary lifestyle among Malay-sian adults and children.
Global guidelines recommend 500–1000 MET minutes/week energy expenditure on physical activity for body fitness[98]. In contrast to the earlier reported study, a more recentstudy demonstrated that urban South Asian women wererelatively active, with 94.3 % of Indian women spendinggreater than 1000 MET-minutes/week on walking andperforming moderate and vigorous physical activities andachieving the recommendation [99]. Because physical inac-tivity and sedentary lifestyle are risk factors for increased bodyweight for both children and adults, a new policy of one-hour physical activity every day was released by theChinese government. The one-hour physical activity ev-ery day has had a beneficial effect in preventing obesityin adolescents in Shandong, China [100].
Nutrition Transition
Since 1970, dietary habits have changed, and people are moredependent on processed foods, eat out more frequently, andhave higher intake of oil and sugar-sweetened beverages[101•]. Moreover, increasing mechanization and improvedeconomic status have led to changes of dietary preferencesfrom the traditional low fat, high fiber foods to highly proc-essed, sweetened, and high fat, energy-dense foods. Animalprotein is becomingmore favorable than vegetarian food. Thisphenomenon is particularly common in low and middle-income Asian countries [2].
Fig. 6 The prevalence of insufficient physical activity among Asianpopulation aged 15 years and above for Asian countries. Note: Definitionof insufficient physical activity is less than 5 times 30 minutes of moderate
activity per week, or less than 3 times 20 minutes of vigorous activity perweek, or equivalent. Source: World Health Organization 2010 [91]
28 Curr Obes Rep (2014) 3:16–37

Table 3 shows available calories (per capita per day) andpercentage of changes in calories from selected foods in Asiancountries. Based on the Food Balance Sheets from 1969–2009, most Asian countries are getting an increasing numberof calories from animal products. Overall, Asia has seen anincrease of 198 % of the calories coming from animal prod-ucts over these 40 years. In term of the calories from animalproducts (per capita per day), China had the greatest increase,from 117 kcal/day in 1969 to 694 kcal/day in 2009 [102],which is approximately a 493 % increase; China is followedby Korea, Vietnam and Indonesia, which had increases ofmore than 200 % within this period. The increase in caloriesfrom animal products implies that the Asian population hasadopted processed food as part of their daily diet.
Concurrently with the increasing number of calories fromanimal products, Asian populations had an average 285 %increase in calories per day per capita from meat. Korea hadthe highest increase from 1969 to 2009 (952 %) comparedwith other Asian countries; this increase suggests thatKorea underwent a major nutrition transition to an an-imal protein-dense diet. However, China is still thegreatest meat consumer at 462 kcal/day/capita, followedby Vietnam at 403 kcal/day/capita [102].
On a related note, Asian populations have had an averageincrease of 147% of their calories from animal fat within a 40-year period. Vietnam, China, and India had the highest in-creases of more than 200 %, while Iran and Korea consumedthe most calories from animal fat (66 kcal/day/capita and63 kcal/day/capita, respectively) [102].
Asians are typically rice eaters, but this traditional staplecarbohydrate food is slowly being replaced by potatoes. From1969 to 2009, Asia had an increase of 178 % of calories percapita from potato, which far exceeded rice, which only had a4 % increase. Seven of 12 Asian countries consumed fewercalories per capita from rice over the last 40 years. Japan,Malaysia, and the United Arab Emirates had the greatestdecreases in calories per capita from rice at −39, -37, and−27 %, respectively. In contrast, the calories per capita frompotatoes increased over this 40-year period, especially inIndonesia, Philippines and Iran, which respectively had 800,400, and 361 % increases in the calories per capita frompotatoes [102]. This scenario, together with the increasedcalories per capita from animal products, meat, andanimal fat in Asian countries implies that the Western-ized diet has already become part of an Asian diet.However, rice still remains a staple food, providing anaverage 777 kcal/day/capita, while potatoes only con-tribute 50 kcal/day/capita [102].
In the last 30 to 40 years, sugar intake has increased rapidlyworldwide due to the high consumption of sugar-sweetenedbeverages. This may lead to unconsciously excessive calorieintake because of the low satiety that follows the consumptionof sugar-sweetened beverages; thus, the caloric intake at
subsequent meals is not reduced [3]. In addition, Asia has alsoseen a 33 % increase in calories per capita from sugar andsweeteners in the last three decades. Among the Asian coun-tries, Korea, Thailand, and China had the highest increase incalories per capita from sugar and sweeteners, with increasesof approximately 370, 226, and 117%, respectively. However,Brunei, the United Arab Emirates, and Malaysia consumedthe most calories per capita from sugar and sweeteners, withan average of 385 kcal/day/capita from sugar [102].
During the ‘Better Health for a Better Hong Kong’ cam-paign, women who consume more than two units of sugar-sweetened beverages were found to have an 8% higher rate ofcentral obesity and a 1.5 cm greater waist circumference thanwomen who consumed fewer sugar-sweetened beverages.Compared with women, men tend to consume sugar-sweetened beverages more frequently and consumed moremeat but were less sedentary. In addition, the campaign alsoreported that younger people are more likely to consume moresugar-sweetened beverages [103].
According to the American Heart Association, sugar intakeis recommended to be less than 100 kcal per day for womenand less than 150 kcal per day for men [104], yet most Asiancountries had sugar and sweetener intakes that were greaterthan the American Heart Association recommendations, apoint policy makers in every Asian country should take noteof. Overall, based on the current Food Balance Sheets of1969–2009, there has been a shift in the dietary patternsamong Asian countries from the conventional traditionaldiet toward a diet with elevated levels of meat, animalproducts, and sugar.
Changes in dietary habits and food choices are majorcontributing factors to obesity in Asia; for example, a house-hold study in the United Arab Emirates found that almost halfof the children had a caloric intake that exceeded their energyrequirement. Snacking contributed to more than 20 % of thetotal calories, followed by sugar-sweetened beverages, whichcontributed 8 to 14 % [93]. In Pakistan, a study reported thatschool children who frequently ate at fast food outlets asopposed to at home were more prone to be obese [31]. Inaddition, a study from Thailand revealed that children fromhigher socioeconomic status families differed in their foodchoices and consumed a higher percentage of calories fromfats and protein compared with children from lower socioeco-nomic status families [41].
Similarly, in Malaysia, the gradual improvement of socio-economic status among theMalaysian population attributed tothe increasing consumption of calories from fat and sugars;these increases have led to additional food importation bills,and the drastic proliferation of the fast food industry is also animportation factor that has led to this nutrition transitionamongMalaysians [97]. Thus, for the last 40 years, a nutritiontransition had led to an increased availability of calories fromanimal products, sugar, and sweeteners [36]. In addition to
Curr Obes Rep (2014) 3:16–37 29

Tab
le3
Changes
inavailablecalories
(per
capitaperday)
from
selected
foodsin
Asian
countries1
Availabilityof
food
Animalproducts
Meat
Animalfat
Rice
Potatoes
Sugarandsw
eetener
Year
1969
kcal
per
day
2009
kcal
per
day
Change
%1969
kcal
per
day
2009
kcal
per
day
Change
%1969
kcal
per
day
2009
kcal
per
day
Change
%1969
kcal
per
day
2009
kcal
per
day
Change
%1969
kcal
per
day
2009
kcal
per
day
Change
%1969
kcal
per
day
2009
kcal
per
day
Change
%
Eastern
Asia
China
117
694
493
81462
470
1141
273
637
794
24.6
2372
213
2963
117
Japan
408
566
3961
176
189
5133
−35
959
581
−39.4
4838
−21
300
263
−12
Korea
107
504
371
23242
952
3163
103
1,195
883
−26.1
2920
−31
67315
370
South-CentralAsia
India
106
209
9715
1713
1962
226
679
676
−0.4
1139
255
178
210
18
Iran
210
393
8776
158
108
3366
100
218
221
1.4
2197
362
235
261
11
South-EastA
sia
Brunei
251
573
128
107
263
146
2126
24827
749
−9.4
718
157
405
388
−4Indonesia
52162
212
2162
195
49
125
991
1,259
27.0
19
800
114
138
21
Malaysia
280
510
82103
245
138
4120
−51
1,167
731
−37.4
415
275
324
383
18
Philippines
275
395
44133
232
7425
54116
780
1,213
55.5
15
400
197
224
14
Thailand
207
315
5294
170
8116
11−3
11,501
1,323
−11.9
08
-86
281
227
Vietnam
136
545
301
78403
417
1142
282
1,318
1,390
5.5
39
200
84113
35
Western
Asia
UnitedArabEmirates
965
690
−28
277
289
4405
52−8
7637
466
−26.8
518
260
408
386
−5Asia
144
429
198
55212
285
1947
147
745
777
4.3
1850
178
118
158
34
Source:1
FAOFoodBalance
Sheet2013
[102]
30 Curr Obes Rep (2014) 3:16–37

unhealthy diets, decreased physical activity accounts for themajor risk factor for obesity and non-communicable disease inMalaysia [97]. In Malaysia, refined carbohydrates remain themain source of calories in low-income families because theyare cheaper than protein-rich foods [36].
Genetic Factors Influencing Obesity in Asian Population
As discussed earlier, environment factors play an importantrole in the alarmingly increasing prevalence of obesity. How-ever, everyone within a sedentary, food-abundant society doesnot become OW/OB, indicating that genetic variation may bean influential factor. Recent genome-wide association studies(GWAS) have discovered multiple loci on chromosomes thatalter the obesity-related phenotypes [105]. The familial prev-alence of obesity reported in different populations contributes40-70 % to the variation in common obesity [106, 107]. Thisindicates that a potent genetic constitution can contribute tothe risk of obesity.
The genetic factors that influence the development of obe-sity can be categorized into single mutations that contribute tomonogenic obesity and multiple genetic variants that interactwith the environment to cause polygenic obesity [108]. Thediscovery of genetic variation effects typically involves theidentification of single nucleotide polymorphisms (SNPs) orcopy number variants (CNVs), followed by an analysis of thesevariations in different populations. In addition to identifyinggenetic variation, epigenetics studies on the regulation of bio-logical processes such as gene expression and growth factorshave also intensified because abnormal changes in the epige-netics will consequently increase the risk of obesity [109, 110].
Single Nucleotide Polymorphisms (SNPs) in the Fat Massand Obesity-Associated (FTO) Gene
Many SNPs have been associated with overweight or obesity.The fat mass and obesity associated (FTO) gene [111],melanocortin-4 receptor (MC4R) gene [112], transmem-brane protein 18 (TMEM18) gene, potassium channeltetramerization domain containing 15 (KCTD15) gene,glucosamine-6-phosphate deaminase 2 (GNPDA2) geneand mitochondrial carrier 2 (MTCH2) gene [113] are asso-ciated with increased BMI. The SH2B adaptor protein 1(SH2B1) gene, neuronal growth regulator 1 (NEGR1) gene[113] and brain-derived neurotrophic factor (BDNF) gene[114] influence energy balance and appetite through thecentral nervous system (CNS). The transcription factorAP-2 beta (TFAP2B) gene, methionine sulfoxide reductaseA (MSRA) gene and lysophospholipase-like 1 (LYPLAL1)gene affect the adiposity and fat distribution [115].
Of these many candidate genes, FTO is currently the moststudied gene in Asia and shows contradictory results. Hence,
FTO will be discussed because it has been reported in thepopulations of China, India, Japan, Korea, Singapore, Malay-sia, Hong Kong, and the Philippines. Recently, several inde-pendent studies described strong associations of the fat massand obesity-associated (FTO) gene variants with obesity, es-pecially in European populations [116, 117]. A GWAS re-vealed that genetic variants near FTO (rs9930506, rs8050136,rs7193144, rs1121980 and rs9939973) are associated withobesity and obesity-related traits in Europeans and Hispanicpopulations [111, 118]. Furthermore, FTO gene polymor-phisms (rs9939609, rs1421085, and rs17817449) arestrongly associated with obesity in European childrenand adults [116, 117].
However, the association of FTO with obesity is contro-versial among Asian populations. A study from Shanghai andBeijing of the Chinese Han population showed no associationof FTO gene polymorphisms with obesity or obesity-relatedtraits, even though the analysis was sex- and geographic-stratified with adequate power to replicate the associationstudies [119]. In contrast, polymorphisms of the FTO genein a Chinese population of China [120], Taiwan [121], HongKong [122], and Singapore [123] were significantly associat-ed with BMI. Similarly, among studies in Japanese and Indianpopulations, some studies showed significant association ofthe FTO gene variants with obesity [124, 125], but othersfailed to replicate the results [126, 127].
The replication failure may be due to substantially lowerrisk allele frequency and linkage disequilibrium (LD) strengthfor genetic variants in certain populations. For example, thepeople of northern and western Europe (CEU) have a higherminor allele frequency (MAF) for rs8050136 and rs9939609compared with the Chinese or Japanese populations (MAFs ofCEU vs. Chinese populations vs. Japanese population forrs8050136 and rs9939609: 0.45 vs. 0.12 vs. 0.22 and 0.48vs. 0.12 vs. 0.20, respectively) [119, 126–128]. Moreover,distinct ethnic backgrounds and different geographic regionsmay have different genetic architecture, leading to differentgene-gene interactions [129]. The patterns of association mayalso vary among different populations due to a historicalnegative selection on the FTO risk alleles in Asia populationscompared with European populations, when the evolutionarydivergence of chimpanzee and human occurred [130].
The development of obesity is not only influenced bystrong genetic variants [131], and an influential obesogenicenvironment is commonly essential for the obesity phenotype[132]. The interplay of genes and environmental factors, forexample eating habits and physical activity level, may con-tribute to common obesity. A recent study has shown theimportance of environment modifications in LIPC, APO45,and PPARG gene variants, which associated with metabolictraits [133]. Therefore, the differences of association resultswithin the same population could be explained by differentenvironments or lifestyles. Physically active adults can
Curr Obes Rep (2014) 3:16–37 31

attenuate the effect of a FTO risk allele and reduce the obesityrisk by 27 % [134]. This phenomenon can be observed inChinese populations that stayed in Singapore (where the FTOgene is significantly associatedwith obesity) [123] and Shang-hai China (where the FTO gene is not associated with obesity)[119], where an average of 35 % of subjects are regularexercisers [135, 136] compared with only 14.7 % of theSingapore Chinese [123].
In addition, studies in Japanese and Indian populationsdemonstrated that in different geographic areas, the same riskallele frequency can result in a different FTO gene associationwith BMI. The study in Takahata, an agricultural and subur-ban area in Japan, successfully replicated the results with thesame FTO rs9939609 risk allele frequency (0.20) as the studyin Tokyo, which failed to replicate these results [124, 126].Similarly, studies conducted in North and South/West Indiashowed a discrepancy in the relationship of the FTO gene withBMI [125, 127]. The stronger association of FTO gene vari-ants with weight observed among urban dwellers may bebecause the prevalence of obesogenic environment risk fac-tors is much higher than in rural areas (p for interaction=0.03).
Therefore, further studies should investigate the factors thatmodify the obesity genetic risk in urban environments [137].Interestingly, a recent study on the association of ROBO1variants with obesity highlighted the possibility of age-geneinteractions [138]. The distinctive differences in the averageage between the two Chinese populations studied in Beijing,China (12.4±3.1 years old in Xi et al. [139] and 58.6±0.6 yearsold in Li et al. [119]) demonstrated a discrepancy in the FTOgene association with obesity. However, studies across Euro-pean populations that include greatly varying average agesshowed no heterogeneity in the association of FTO with BMI[116]. In addition, a study from Singapore also confirmed thatFTO locus showed consistent associationwith obesity in adultsas well as children [140]. Nevertheless, there are also similarityand contradictory results reported for the association of FTOpolymorphisms with adult obesity from different Asia coun-tries. Thus, investigations on the interactions between genesand gene-environment are warranted to further clarify theinfluence of genetic architecture on common obesity.
Copy Number Variants (CNVs)
Recently, loci that potentially have strong contributions toobesity susceptibility variation have been examined throughthe identification of rare variants, copy number variants(CNVs), and epigenetic variation [141]. CNV is a commonvariation for genes with sizes ranging from 1 kb to several Mb.CNV is associated with different complex diseases, such asmental retardation, autism [142, 143], schizophrenia and os-teoporosis [144]. Thus, intensive studies on CNVs are impor-tant to investigate the effects of genetic variation on biologicalfunctions and phenotypes.
Few CNV regions have been associated with obesity andBMI; these regions include 16p11.2 [145, 146], 10q11.22[147], and 11q11 [148], suggesting that CNVs may influencethe obesity risk. Recently, two CNVs, 1p31.1 [113] and16p12.3 [149], were associated with obesity by two large-scale GWAS. Another group of researchers also successfullyconfirmed that CNV 1p31.1 is related to obesity, but contra-dictory results were found for CNV 16p12.3 [148]. In China,the CNVassociation with BMI was examined in 597 ChineseHan subjects. The authors reported that BMI was associatedwith the CNV at 10q11.22 (raw P=0.011), which accountedfor 1.6 % of the BMI variation among the Chinese population[147]. A GWAS also showed a similar effect in a case-controlled European sample (adjusted p=0.0004) [148].
However, the study from Yang et al. [150••] indicated nosignificant association of CNV 16p12.3 with obesity amongthe Chinese population but showed significant association inEuropeans (p=0.993 and p=0.0138 for BMI, respectively, p=0.613 and p=0.00213 for body fat mass, respectively). Thismay be due to differences in the CNV frequency between theEuropean and Chinese populations (P=0.001). The Europeanpopulation has manymore common copy number deletions of16p12.3 when compared with the Chinese (deletion frequen-cy=27.26 % and 0.8 %, respectively); this higher copy num-ber deletion frequency may increase the obesity risk in Euro-peans. These findings suggest that greater genomic variationcan be observed when making comparisons across ethnicities.Hence, it is crucial to evaluate different ancestries of popula-tions when assessing CNVassociation with obesity [150••].
Epigenetics
More than 40 genetic variants have been associated withobesity, but these polymorphisms are not sufficient to eluci-date the heritability of obesity. Hence, epigenetics must betaken into consideration [151]. Epigenetics is defined as geneexpression changes without DNA sequence modification [152,153]. Epigenetics not only predisposes some people to extremeobesity but also increases the susceptibility of some people tocommon obesity, especially in the presence of an obesogenicenvironment [151]. Therefore, DNA methylation profiles andmodifications of histone or other processes that change theepigenetics may predict an individual’s susceptibility to obesi-ty. Thus, exploring the mechanisms of epigenetics variationswould allow new therapeutic implementations [154].
Environmental factors induce modification of epigeneticsand lead to metabolic and chronic diseases, such as obesity.Studies have shown that the mother’s weight is associated withher offspring, and the obesity risk is reduced in children whosemothers had undergone clinical interventions for weight loss[155, 156]. This indicates that the intrauterine environmentinfluences the epigenome during fetal development [157]. Fur-ther, in vitro studies have demonstrated that epigenetic
32 Curr Obes Rep (2014) 3:16–37

modifications are affected by diet, which predisposes a personto obesity [154]. Abnormal methylation due to insufficientmethyl donors is a possible mechanism [158–160].
Hence, increased BMI and adiposity due to a disturbance ingene expression is most likely mediated by epigenetic-environment interactions. This hypothesis is possible becauseevidence suggests that the FTO gene is a DNA-demethylaseenzyme [161], and the MC4R gene has a reduction in meth-ylation after prolonged exposure to a high fat diet [162].Additionally, the peroxisome proliferator-activated receptorγ (PPARγ) protein reacts with histone acetyltransferases[163] during fat cell generation, and diet-induced methylationcauses epigenetics changes on proopiomelanocortin (POMC)[164] and leptin [165]. However, evidence in humans is lim-ited due to the difficulties in conducting the confirmation testson the epigenetic changes [166].
Conclusion
Asia, once known as the continent with ‘lean nations,’ is nowhaving to combat an obesity epidemic as a ‘side effect’ ofchanges in the socio-economy, rapid urbanization, nutrition,and lifestyle transition. Thus, proper measures, such as nationalprograms that target public awareness, should be undertaken,and improved structural facilities are necessary to promotehigher physical activity and reduce overweight and obesity.Despite on-going interventions to decrease the prevalence ofobesity through diet, increased physical activity, and education,we are still unable to slow down the drastic growth of obesity.
Hence, screening for obesity susceptibility variants in obeseindividuals may help predict the underlying mechanism ofobesity, so more effective and specific obesity prevention strat-egies can be designed. However, due to the different geneticbackground and environmental exposure of Asian populations,further investigation on gene-environmental interaction in dif-ferent populations of Asians is warranted before further con-clusions can be made. Therefore, efforts to prevent obesityshould occur at multiple levels, including societal actions andnewmedical discoveries, to eliminate the root causes of obesity.
Compliance with Ethics Guidelines
Conflict of Interest Pei Nee Chong declares that she has no conflict ofinterest.
Christinal Pey Wen Teh declares that she has no conflict of interest.Bee Koon Poh is Honorary Secretary, Malaysian Association for the
Study of Obesity.Life Member, Nutrition Society of Malaysia.Mohd Ismail Noor is the President of Malaysian Association for the
Study of Obesity.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. World Health Organization. Obesity and overweight. Fact sheets.Available at: http://www.who.int/mediacentre/factsheets/fs311/en/. Accessed July 2013.
2. Ramachandran A, Chamukuttan S, Shetty SA, et al. Obesity inAsia – is it different from rest of the world. Diabetes Metab ResRev. 2012;28 Suppl 2:47–51.
3. Malik VS,Willett WC, Hu FB. Global obesity: trends, risk factorsand policy implications. Nat Rev Endocrinol. 2013;9:13–27.
4. Ang YN, Wee BS, Poh BK, Ismail MN. Multifactorial influencesof childhood obesity. Curr Obes Rep. 2013;2:10–22.
5. Shimokawa S, Chang H-H, Pinstrup-Andersen P. Understandingthe differences in obesity among working adults between Taiwanand China. Asia Pac J Clin Nutr. 2008;18(1):88–95.
6. Goyal RK, Shah VN, Saboo BD, et al. Prevalence of overweightand obesity in Indian Adolescent School Going Children: itsrelationship with socioeconomic status and associated lifestylefactors. J Assoc Physicians India. 2010;58:151–8.
7. Halfon N, Larson K, Slusser W. Associations between obesity andcomorbid mental health, developmental, and physical health con-ditions in a nationally representative sample of US children aged10 to 17. Acad Pediatr. 2013;13:6–13.
8. Gothankar JS. Prevalence of obesity and its associated comorbid-ities amongst adults. Natl J Community Med. 2011;2(2):211–24.
9. Wee BS, Poh BK, Bulgiba A, et al. Risk of metabolic syndromeamong children living in metropolitan Kuala Lumpur: a casecontrol study. BMC Public Health. 2011;11:333.
10. Chu N-F, Pan W-H. Prevalence of obesity and its comorbiditiesamong schoolchildren in Taiwan. Asia Pac J Clin Nutr.2007;16(S2):601–7.
11. WangY,Mi J, Shan X-Y, et al. Is China facing an obesity epidemicand the consequences? The trends in obesity and chronic diseasein China. Int J Obes. 2006;31(1):177–88.
12. Vegharia G, Sedaghatb M, Maghsodlob S, et al. Influence ofeducation in the prevalence of obesity in Iranian northern adults.J Cardiovasc Dis Res. 2013;4(1):30–3.
13. Sengupta A. The changing face of malnutrition in India. J HealthManag. 2012;14(4):451–65.
14. Tuan NT, Tuong PD, Popkin BM. Body mass index (BMI) dy-namics in Vietnam. Eur J Clin Nutr. 2008;62:78–86.
15. Walls HL, Peeters A, Son PT, et al. Prevalence of underweight,overweight and obesity in urban Hanoi, Vietnam. Asia Pac J ClinNutr. 2009;18(2):234–9.
16. Cuong TQ, Dibley MJ, Bowe S, et al. Obesity in adults: anemerging problem in urban areas of Ho Chi Minh City,Vietnam. Eur J Clin Nutr. 2007;61:673–81.
17. Dang CV, Day RS, Selwyn B, et al. Initiating BMI prevalencestudies in Vietnamese children: changes in a transitional economy.Asia Pac J Clin Nutr. 2010;19(2):209–16.
18. Song Y, Wang H-J, Ma J, et al. Secular trends of obesity preva-lence in Urban Chinese Children from 1985 to 2010: genderdisparity. PLoS ONE. 2013;8(1):e53069.
19. Cui ZH, Huxley R, Wu YF, et al. Temporal trends in overweightand obesity of children and adolescents from nine Provinces inChina from 1991–2006. Int J Pediatr Obes. 2010;5(5):365–74.
20. Liu J-M, Ye R, Li S, et al. Prevalence of overweight/obesity inChinese children. Arch Med Res. 2007;38(8):882–6.
Curr Obes Rep (2014) 3:16–37 33

21. Ji CY, WGOC. Body mass index reference for screening over-weight and obesity in Chinese school-age children. BiomedEnviron Sci. 2005;18:390–400.
22. Cole TJ, Bellizzi MC, Flegal KM, et al. Establishing a standarddefinition for child overweight and obesity worldwide: interna-tional survey. BMJ. 2000;320(7244):1240–3.
23. Matsushita Y, Yoshiike N, Kaneda F, et al. Trends in childhoodobesity in Japan over the last 25 years from the national nutritionsurvey. Obes Res. 2004;12(2):205–14.
24. International Obesity Task force. Available at: http://www.iaso.org/iotf/obesity/?map=children. Accessed July 2013.
25. Department of Health (DOH) of Executive Yuan, Taiwan, ROC.Available at http://www.doh.gov.tw. Accessed July 2013.
26. Chu NF. Prevalence and trends of obesity among school childrenin Taiwan/the Taipei Children Heart Study. Int J Obes Relat MetabDisord. 2001;25:170–6.
27. Centers for Disease Control and Prevention. 2000. Department ofHealth and Human Services. Centers for Disease Control andPrevention, USA. CDC growth charts for the United States [data-base on the internet]. Available at http://www.cdc.gov/nchs/data/nhanes/growthcharts/zscore/bmiagerev.xls. Accessed July 2013.
28. Raj M, Sundaram KR, Paul M, et al. Obesity in Indian children:time trends and relationship with hypertension. Natl Med J India.2007;20(6):288–93.
29. World Health Organization. 2007. Growth Chart for Children 5–19 years. Geneva: WHO. Available at http://www.who.int/growthref/en/. Accessed July 2013.
30. Nouhjah S, Karandish M, Malihi R, et al. Prevalence of over-weight and obesity in 2–5 years children based on New WhoGrowth Standards in Ahwaz, Iran. Pediatr Res. 2011;70:392.
31. Ahmed J, Laghari A, Naseer M, et al. Prevalence of and factorsassociated with obesity among Pakistani schoolchildren: a school-based, cross-sectional study. East Mediterr Health J. 2013;19(3):242–7.
32. World Health Organization. 2006.WHOChild Growth Standards.Geneva: WHO. Available at http://www.who.int/childgrowth.Accessed July 2013.
33. Sandjaja S, Budiman B, Harahap H, et al. Food consumption andnutritional and biochemical status of 0·5–12-year-old Indonesianchildren: the SEANUTS study. Br J Nutr. 2013. doi:10.1017/S0007114513002109.
34. Ismail MN, Norimah AK, Poh BK. Nutritional status and dietaryhabits of primary school children in peninsular Malaysia. Finalreport for UKM-Nestle Research Project. Kuala Lumpur:Department of Nutrition & Dietetics, Faculty of Allied HealthSciences, Universiti Kebangsaan Malaysia; 2006.
35. Ismail MN, Ruzita AT, Norimah AK, et al. Prevalence and trendsof overweight and obesity in two cross-sectional studies ofMalaysian children, 2002–2008. Presented at the MASOScientific Conference on Obesity. Kuala Lumpur, Malaysia;August 12–13, 2009.
36. Khor GL. Food availability and the rising obesity prevalence inMalaysia. IeJSME. 2012;6 Suppl 1:S61–8.
37. Poh BK, Ng BK, Haslinda MDS, et al. Nutritional status anddietary intakes of children aged 6 months to 12 years: findingsof the Nutrition Survey of Malaysian Children (SEANUTSMalaysia). Br J Nutr. 2013. doi:10.1017/S0007114513002092.
38. Cheah JS. Obesity in Singapore. Ann Acad Med Singapore.1997;26:145–6.
39. Aekplakorn W, Mo-Suwan L. Prevalence of obesity in Thailand.Obes Rev. 2009;10(6):589–92.
40. Firestone R, Punpuing S, Peterson KE, et al. Child overweight andundernutrition in Thailand: is there an urban effect? Soc Sci Med.2011;72:1420–8.
41. Sengmeuanga P, Kukongviriyapana U, Pasurivonga O, et al.Prevalence of obesity among Thai schoolchildren: a survey in
Khon Kaen, Northeast Thailand. Asian Biomed. 2010;4(6):965–70.
42. Rojroongwasinku N, Kijboonchoo K, Wimonpeerapattana W,et al. SEANUTS: the nutritional status and dietary intakes of0.5–12-year-old Thai children. Br J Nutr. 2013. doi:10.1017/S0007114513002110.
43. Hong TK, Trang NHHD, Dibley MJ. Changes in adiposity indi-cators of Ho Chi Minh City adolescents in a 5-year prospectivecohort study. Int J Obes. 2013. doi:10.1038/ijo.2012.217.
44. Nguyen PVN, Hong TK, Hoang T, et al. High prevalence ofoverweight among adolescents in Ho Chi Minh City, Vietnam.BMC Public Health. 2013;13:141.
45. Le HT, Vu NTT, Huyen DTT, et al. Overweight, obesity andassociated factors among secondary school students in a northerncity of Vietnam in 2011. Health. 2013;5:24–9.
46. Nguyen BKL, Thi HL, Do VAN, et al. Double burden of under-nutrition and overnutrition in Vietnam in 2011: results of theVietnamese SEANUTS study in 0·5–11-year-old children. Br JNutr. 2013. doi:10.1017/S0007114513002080.
47. World Health Organization. Obesity: preventing andmanaging theglobal epidemic—report of a WHO consultation. World HealthOrgan Tech Rep Ser. 2000;894:1–253.
48. Reynolds K, Gu DF, Whelton PK, et al. Prevalence and riskfactors of overweight and obesity in China. Obesity. 2007;15(1):10–8.
49. Singh V, Sahu M, Yadav S, et al. Body mass index (BMI), waistcircumference (WC) and obesity in the resident adults of RaipurDistrict (Chhattisgarh state: India). J Phytology. 2012;4(3):33–9.
50. MaddahM, Solhpour A. Obesity in relation to gender, educationallevels and living area in adult population in Rasht, northern Iran.Int J Cardiol. 2010;145(2):310–1.
51. Sidik SM, Rampal L. The prevalence and factors associated withobesity among adult women in Selangor, Malaysia. Asia PacificFamily Medicine. 2009;8(1):2.
52. Rampal L, Rampal S, Khor GL, et al. A national study on theprevalence of obesity among 16,127 Malaysians. Asia Pac J ClinNutr. 2007;16(3):561–6.
53. Mohamud WN, Musa KI, Khir AS, et al. Prevalence of over-weight and obesity among adult Malaysians: an update. Asia Pac JClin Nutr. 2011;20(1):35–41.
54. Azmi MY, Junidah R, Mariam SA, et al. Body Mass Index (BMI)of adults: findings of the Malaysian Adult Nutrition Survey(MANS). Mal J Nutr. 2009;15(2):97–119.
55. Sabanayagam C, Shankar A, Wong TY, et al. Socioeconomicstatus and overweight/obesity in an adult chinese population inSingapore. J Epidemiol. 2007;17(5):161–8.
56. World Health Organization. Expert consultation. Appropriatebody-mass index for Asian populations and its implications forpolicy and intervention strategies. Lancet. 2004;363:157–63.
57. Jitnarin N, Kosulwat V, Rojroongwasinkul N, et al. Riskfactors for overweight and obesity among Thai adults:results of the national Thai food consumption survey.Nutrients. 2010;2:60–74.
58. Nguyen MD, Beresford ASS, Drewnowski A. Trends in over-weight by socio-economic status in Vietnam: 1992 to 2002. PublicHealth Nutr. 2007;10(2):115–21.
59. Song A, Liang Y, Yan Z, et al. Highly prevalent and poorlycontrolled cardiovascular risk factors among Chinese elderly peo-ple living in the rural community. Eur J Prev Cardiol. 2013. doi:10.1177/2047487313487621.
60. Zhou BF, CooperativeMeta-Analysis Group of the WorkingGroup on Obesity in China. Predictive values of body mass indexand waist circumference for risk factors of certain related diseasesin Chinese adults – study on optimal cut-off points of body massindex and waist circumference in Chinese adults. Biomed EnvironSci. 2002;15:83–96.
34 Curr Obes Rep (2014) 3:16–37

61. Schooling CM, Lam TH, Li ZB, et al. Obesity, physical activity,andmortality in a prospective Chinese Elderly Cohort. Arch InternMed. 2006;166:1498–504.
62. Huang PC, Yu SL, Lin YM. Body weight of Chinese adults bysex, age and body height and criterion of obesity based on bodymass index. J Chin Nutr Soc. 1992;17:157–72.
63. Lin CC, Li TC, Lai SW, et al. Epidemiology of obesity in elderlypeople. Epidemiology of obesity in elderly people. Yale J BiolMed. 1999;72:385–91.
64. Ramachandran A, Snehalatha C, Shyamala P, et al. High preva-lence of NIDDM and IGT in an Elderly South Indian Populationwith low rates of obesity. Diabetes Care. 1994;17(10):1190–2.
65. Nematy M, Sakhdari A, Ahmadi-Moghaddam P, et al. Prevalenceof obesity and its association with socioeconomic factors inElderly Iranians from Razavi-Khorasan Province. ScientificWorld Journal. 2009;9:1286–93.
66. Bakhshi E, Seifi B, Biglarian A, et al. Factors associated withobesity in Iranian elderly people: results from the National HealthSurvey. BMC Res Notes. 2011;4:538.
67. Suzana S, Kee CC, Jamaludin AR, et al. The Third NationalHealth and Morbidity Survey: prevalence of obesity, and abdom-inal obesity among the Malaysian Elderly Population. Asia Pac JPublic Health. 2012;24(2):218–29.
68. Ostbye T, Malhotra R, Chan A. Variation in and correlates of bodymass status of older Singaporean men and women: results from aNational Survey. Asia Pac J Public Health. 2013;25(1):48–62.
69. Vapattanawong P, Aekplakorn W, Rakchanyaban U, et al. Obesityand mortality among older Thais: a four year follow up study.BMC Public Health. 2010;10:604.
70. Kagawa M, Hills AP. Secular changes in BMI and obesity risk inJapanese Children: considerations from a MorphologicPerspective. Open Obes J. 2011;3:9–16.
71. •• SchaafsmaA,Deurenberg P, CalameW, et al. Design of the SouthEast Asian Nutrition Survey (SEANUTS): a four-country multi-stage cluster design study. British Journal of Nutrition. 2013;1–9.This is a combination of surveys carried out in Indonesia, Malaysia,Thailand and Vietnam that clearly demonstrated the differences ofobesity prevalence and imbalances of energy intake and energyexpenditure. These data is important for formulating nutritionalhealth policies, as well as for designing innovative food and nutri-tion research and development programmes.
72. Kalra S, Unnikrishnan AG. Obesity in India: the weight of thenation. J Med Nutr Nutraceuticals. 2012;1(1):37–41.
73. World Health Organization. Global health and observatory.Overweight and obesity. Available at http://www.who.int/gho/ncd/risk_factors/overweight/en/. Accessed July 2013.
74. World Bank 2013. World Bank national accounts data, and OECDNational Accounts data files. Available at http://api.worldbank.org/datafiles/NY.GDP.MKTP.CD_Indicator_MetaData_en_EXCEL.xls. Accessed July 2013.
75. World Bank 2013. Literacy rate, adult total (Percentage of peopleages 15 and above). Available at http://data.worldbank.org/indicator/SE.ADT.LITR.ZS. Accessed August 2013.
76. World Bank 2013. International Telecommunication Union,World Telecommunication/ICT Development Report and data-base. Available at http://search.worldbank.org/data?qterm=IT.NET.BBND&language=EN. Accessed July 2013.
77. World Bank 2013. International Road Federation, World RoadStatistics and data files Available at http://data.worldbank.org/indicator/IS.VEH.NVEH.P3. Accessed July 2013.
78. World Bank 2013. United Nations, World Urbanization Prospects.Available at http://search.worldbank.org/data?qterm=SP.URB.TOTL.IN.ZS&language=EN. Accessed July 2013.
79. Shen J, Goyal A, Sperling L. The emerging epidemic of obesity,diabetes, and the metabolic syndrome in China. Cardiol Res Pract.2012;2012:1–5.
80. Dearth-Wesley T, Wang H, Popkin BM. Under- and overnutritiondynamics in Chinese children and adults (1991–2004). Eur J ClinNutr. 2008;62:1302–7.
81. Zhang YX, Wang SR. Prevalence and regional distribution ofchildhood overweight and obesity in Shandong Province, China.World J Pediatr. 2013;9(2):135–9.
82. Chen D-R, Wen T-Z. Socio-spatial patterns of neighborhood ef-fects on adult obesity in Taiwan: a multi-level model. Soc SciMed. 2010;70:823–33.
83. Li M, Dibley MJ, Sibbritt D, et al. Factors associated with ado-lescents’ overweight and obesity at community, school and house-hold levels in Xi’an City, China: results of hierarchical analysis.Eur J Clin Nutr. 2008;62:635–43.
84. Itoi A, Yamada Y, Watanabe Y, et al. Physical activity, energy intake,and obesity prevalence among urban and rural schoolchildren aged11–12 years in Japan.Appl Physiol NutrMetab. 2012;37(6):1189–99.
85. Lebel L, Krittasudthacheewa C, Salamanca A, et al. Lifestyles andconsumption in cities and the links with health and well-being: thecase of obesity. Curr Opin Environ Sustain. 2012;4:405–13.
86. Ng SW, Popkin BM. Time use and physical activity: a shift awayfrom movement across the globe. Obes Rev. 2012;13:659–80.
87. Lau XC, Chong KH, Poh BK, et al. Physical activity, fitness andthe energy cost of activities: implications for obesity in childrenand adolescents in the tropics. In: Jeyakumar H, editor. Advancesin food and nutrition research, vol. 70. Burlington: AcademicPress; 2013. p. 49–101.
88. World Development Indicator 2013. 5.12 The information society.Available at http://wdi.worldbank.org/table/5.12. Accessed July2013.
89. Trang NH, Hong TK, Dibley MJ, et al. Factors associated withphysical inactivity in adolescents in Ho Chi Minh City, Vietnam.Med Sci Sports Exerc. 2009;41(7):1374–83.
90. Hallal PC, Andersen LB, Bull FC, et al. Global physical activitylevels: surveillance progress, pitfalls, and prospects. Lancet.2012;380:247–57.
91. World Health Organization. Global status report on non commu-nicable diseases 2010. Available at http://www.who.int/nmh/publications/ncd_report2010/en/. Accessed August 2013.
92. Abdullah ASM,Wong CM, YamHK, et al. Factors related to non-participation in physical activity among the students in HongKong. Int J Sports Med. 2005;26(7):611–5.
93. Ng SW, Zaghloul S, Ali H, et al. Nutrition transition in the UnitedArab Emirates. Eur J Clin Nutr. 2011;65:1328–37.
94. Liou YM, Liou T-H, Chang L-C. Obesity among adolescents:sedentary leisure time and sleeping as determinants. J Adv Nurs.2010;66(6):1246–56.
95. Ismail MN, Chee SS, Nawawi H, et al. Obesity in Malaysia. ObesRev. 2002;3:203–8.
96. Poh BK, Safiah MY, Tahir A, et al. Physical activity pattern andenergy expenditure of Malaysian adults: findings from theMalaysian Adult Nutrition Survey (MANS). Mal J Nutr.2010;16(1):13–37.
97. Ismail MN. The nutrition and health transition in Malaysia. PublicHealth Nutr. 2002;5(1A):191–5.
98. U.S. Department of Health & Human Services. Physical ActivityGuidelines for Americans. Washington, DC: U.S. Department ofHealth & Human Services. Available at: http://health.gov/paguidelines/guidelines/appendix1.aspx. Accessed July 2013.
99. Waidyatilaka I, Lanerolle P, Wickremasinghe R, et al. Sedentarybehaviour and physical activity in South Asian Women: time toreview current recommendations? PLoS ONE. 2013;8(3):e58328.
100. Zhang Y-X, Zhou J-Y, Zhao J-S, et al. The role of 1-h physicalactivity every day in preventing obesity in adolescents inShandong, China. Eur J Pediatr. 2013;172(3):325–30.
101. • Popkin BM, Adair LS, Ng SW. Now and then: the globalnutrition transition: the pandemic of obesity in developing
Curr Obes Rep (2014) 3:16–37 35

countries. Nutr Rev. 2012;70(1):3–21. This paper addressed thepractical consideration for future programs and policy in tacklingthe rising prevalence of obesity. It did specifically pay attention tolow- to middle- income countries for its nutritional shift, foodsystem changes and dual burden of over- and under-nutrition.
102. FAO 2013. Food and Agricultural Organization of the UnitedNations. Food balance sheets. Available at http://faostat3.fao.org/home/index.html#DOWNLOAD. Accessed July 2013.
103. Ko GT, So W-Y, Chow C-C, et al. Risk associations of obesitywith sugar-sweetened beverages and lifestyle factors in Chinese:the ‘Better Health for Better Hong Kong’ health promotion cam-paign. Eur J Clin Nutr. 2010;64:1386–92.
104. Johnson RK, Appel JL, Brands M, et al. Dietary sugars intake andcardiovascular health: a scientific statement from the AmericanHeart Association. Circulation. 2009;120:1011–20.
105. Loos RJF, Bouchard C. FTO: the first gene contributing to com-mon forms of human obesity. Obes Rev. 2008;9(3):246–50.
106. Davey G, Ramachandran A, Snehalatha C, et al. Familial aggre-gation of central obesity in Southern Indians. Int J Obes.2000;24(11):1523–7.
107. Clément K, Sorensen TIA. Obesity: genomics and Post-genomic.New York: Informa Healthcare; 2008. p. 1–576.
108. Clément K. Genetics of human obesity. C R Biol. 2006;329:608–22.109. Herrera BM, Lindgren CM. The genetics of obesity. Curr Diab
Rep. 2010;10:498–505.110. Rhee KE, Phelan S, McCaffery J. Review article: early determi-
nants of obesity: genetic, epigenetic, and in utero influences. Int JPediatr. 2012;2012:1–9.
111. Scuteri A, Sanna S, Chen WM, et al. Genome-wide associationscan shows genetic variants in the FTO gene are associated withobesity-related traits. PLoS Genet. 2007;3:e115.
112. Loos RJF, Lindgren CM, Li S, et al. Common variants nearMC4Rare associated with fat mass, weight and risk of obesity. Nat Genet.2008;40:768–75.
113. Willer CJ, Speliotes EK, Loos RJF, et al. Six new loci associatedwith body mass index highlight a neuronal influence on bodyweight regulation. Nat Genet. 2009;41(1):25–34.
114. Li S, Zhaom H, Luan J, et al. Cumulative effects and predictivevalue of common obesity-susceptibility variants identified bygenome-wide association studies. Am J Clin Nutr. 2010;91:184–90.
115. Lindgren CM, Heid IM, Randall JC, et al. Genome-wide associ-ation scan meta-analysis identifies three loci influencing adiposityand fat distribution. PLoS Genet. 2009;5(6):e1000508.
116. Frayling TM, Timpson NJ, Weedon MN, et al. A common variantin the FTO gene is associated with body mass index and predis-poses to childhood and adult obesity. Science. 2007;316:889–94.
117. Dina C, Meyre D, Gallina S, et al. Variation in FTO contributes tochildhood obesity and severe adult. Obes Nat Genet. 2007;39:724–6.
118. Hinney A, Nguyen TT, Scherag A, et al. Genome wide association(GWA) study for early onset extreme obesity supports the role offat mass and obesity associated gene (FTO) variants. PLoS ONE.2007;2:e1361.
119. Li H, Wu Y, Loos RJF, et al. Variants in the fat-mass and obesity-associated (FTO) gene are not associated with obesity in ChineseHan population. Diabetes. 2008;57:264–8.
120. Liu Y, Liu Z, Song Y, et al. Meta-analysis added power toidentify variants in FTO associated with type 2 diabetes andobesity in the Asian population. Obesity (Silver Spring).2010;18(8):1619–24.
121. Chang Y-C, Liu P-H, Lee W-J, et al. Common variation in the fatmass and obesity-associated (FTO) gene confers risk of obesityand modulates BMI in the Chinese population. Diabetes. 2008;57:2245–52.
122. Cheung CYY, Tso AWK, Cheung BMY, et al. Obesity suscepti-bility genetic variants identified from recent genome-wide
association studies: implications in a Chinese population. J ClinEndocrinol Metab. 2010;95:1395–403.
123. Tan JT, Dorajoo R, Seielstad M, et al. FTO variants are associatedwith obesity in the Chinese and Malay populations in Singapore.Diabetes. 2008;57:2851–7.
124. Karasawa S, Daimon M, Sasaki S, et al. Association of thecommon fat mass and obesity associated (FTO) gene polymor-phism with obesity in a Japanese population. Endocr J.2010;57(4):293–301.
125. Chauhan G, Tabassum R, Mahajan A, et al. Commonn variants ofFTO and the risk of obesity and type 2 diabetes in Indians. J HumGenet. 2011;56:720–6.
126. Horikoshi M, Hara K, Ito C, et al. Variantions in HHEX gene areassociated with increased risk of type 2 diabetes in Japanesepopulation. Diabetologia. 2007;50:2461–6.
127. Yajnik CS, Janipalli CS, Bhaskar S, et al. FTO gene variantsstrongly associated with type 2 diabetes but only weakly withobesity in South Asian Indians. Diabetologia. 2009;52(2):247–52.
128. International HapMap Project. Available at http://hapmap.ncbi.nlm.nih.gov/cgi-perl/gbrowse/hapmap27_B36/#search. AccessedJuly 2013.
129. Greene CS, Penrod NM, Williams SM, et al. Failure to replicate agenetic association may provide important clues about geneticarchitecture. PLoS ONE. 2009;4(6):e5639.
130. Ohashi J, Naka I, Kimura R, et al. FTO polymorphisms in oceanicpopulations. J Hum Genet. 2007;52(12):1031–5.
131. Parizkova J, ChinM-K, ChiaM, et al. An international perspectiveon obesity, health and physical activity: current trends and chal-lenges in China and Asia. J Exerc Sci Fit. 2007;5(1):7–23.
132. Loos RJF, Bouchard C. Obesity—is it a genetic disorder? J InternMed. 2003;254(5):401–25.
133. Grarup N, Andersen G. Gene-environment interactions in thepathogenesis of type 2 diabetes and metabolism. Curr Opin ClinNutr Metab Care. 2007;10:420–6.
134. Kilpeläinen TO, Qi L, Brage S, et al. Physical activity attenuated theinfluence of FTO variants on obesity risk: ameta-analysis of 218166adults and 19268 children. PLoS Med. 2011;8(11):e1001116.
135. Lee SA, Xu WH, Zheng W, et al. Physical activity patterns andtheir correlates among Chinese men in Shanghai. Med Sci SportsExerc. 2007;39:1700–7.
136. Jurj AL, WenW, Gao YT, et al. Patterns and correlates of physicalactivity: a cross-sectional study in urban Chinese women. BMCPublic Health. 2007;7:213.
137. Taylor AE, Sandeep MN, Janipalli CS, et al. Associations of FTOand MC4R variants with obesity traits in Indians and the role ofrural/urban environment as a possible effect modifier. J Obes.2011;2011:1–7.
138. Lasky-Su J, Lyon HN, Emilsson V, et al. On the replication ofgenetic associations: timing can be everything! Am J Hum Genet.2008;82:849–58.
139. Xi B, Shen Y, Zhang M, et al. The common rs9939609 variant ofthe fat mass and obesity-associated gene is associated with obesityrisk in children and adolescents of Beijing, China. BMC MedGenet. 2010;11:107.
140. Dorajoo R, Blakemore AIF, Sim X, et al. Replication of 13 obesityloci among Singaporean Chinese, Malay and Asian-Indian popu-lations. Int J Obes. 2012;36:159–63.
141. Li S, Zhao JH, Luan J, et al. Cumulative effects and pre-dictive value of common obesity-susceptibility variants iden-tified by genome-wide association studies. Am J Clin Nutr.2010;91:184–90.
142. Sebat J, Lakshmi B,Malhotra D, et al. Strong association of de novocopy number mutations with autism. Science. 2007;316:445–9.
143. Marshall C, Noor A, Vincent J, et al. Structural variation ofchromosomes in autism spectrum disorder. Am J Hum Genet.2008;82:477–88.
36 Curr Obes Rep (2014) 3:16–37

144. Yang TL, Chen XD, Guo Y, et al. Genome-wide copy-number-variation study identified a susceptibility gene, UGT2B17, forosteoporosis. Am J Hum Genet. 2008;83:663–74.
145. Bochukova EG, Huang N, Keogh J, et al. Large, rare chromosom-al deletions associated with severe early-onset obesity. Nature.2010;463:666–70.
146. Walters RG, Jacquemont S, Valsesia A, et al. A novel highly-penetrant form of obesity due to microdeletions on chromosome16p11.2. Nature. 2010;463(7281):671–5.
147. Sha B-Y, Yang T-L, Zhao L-J, et al. Genome-wide associationstudy suggested copy number variation may be associated withbody mass index in the Chinese population. J Hum Genet.2009;54(4):199–202.
148. Jarick I, Vogel CIG, Scherag S, et al. Novel common copy numbervariation for early onset extreme obesity on chromosome 11q11identified by a genome-wide analysis. Hum Mol Genet.2011;20(4):840–52.
149. Speliotes EK, Willer CJ, Berndt SI, et al. Association analyses of294796 individuals reveal eighteen new loci associated with bodymass index. Nat Genet. 2010;42(11):937–48.
150. •• Yang T-L, Guo Y, Li SM, et al. Ethnic differentiation of copynumber variation on chromosome 16p12.3 for association withobesity phenotypes in European and Chinese populations. Int JObes. 2013;37:188–90. This paper suggested that copy numbervariants (CNV) 16p12.3 might be ethnic specific and cause phe-notypic diversity, which may provide some new clues into theunderstanding of the genetic architecture of obesity.
151. Herrera BM, Keildson S, Lindgren CM. Genetics and epigeneticsof obesity. Maturitas. 2011;69(1):41–9.
152. Bird A. Perceptions of epigenetics. Nature. 2007;447:396–8.153. Wolffe AP, Guschin D. Review: chromatin structural features and
targets that regulate transcription. J Struct Biol. 2000;129:102–22.154. Campión J, Milagro F, Martínez JA. Epigenetics and obesity. Prog
Mol Biol Transl Sci. 2010;94:291–347.155. Dabelea D, Mayer-Davis EJ, Lamichhane AP. Association of
intrauterine exposure to maternal diabetes and obesity with type
2 diabetes in youth: the SEARCH case–control study. DiabetesCare. 2008;31(7):1422–6.
156. Smith J, Cianflone K, Biron S. Effects of maternal surgical weightloss in mothers on intergenerational transmission of obesity. J ClinEndocrinol Metab. 2009;94(11):4275–83.
157. Waterland RA, Jirtle RL. Early nutrition, epigenetic changes attransposons and imprinted genes, and enhanced susceptibility toadult chronic disease. Nutrition. 2004;20(1):63–8.
158. Waterland RA, Michels KB. Epigenetic epidemiology of thedevelopmental origins hypothesis. Annu Rev Nutr. 2007;27:363–88.
159. Poirier LA. The effects of diet, genetics and chemicals on toxicityand aberrant DNA methylation: an introduction. J Nutr.2002;132(8 Suppl):S2336–9.
160. Biniszkiewicz D, Gribnau J, Ramsahoye B. Dnmt1 overexpres-sion causes genomic hypermethylation, loss of imprinting, andembryonic lethality. Mol Cell Biol. 2002;22(7):2124–35.
161. Gerken T, Girard CA, Tung YC. The obesity-associated FTO geneencodes a 2-oxoglutarate-dependent nucleic acid demethylase.Science. 2007;318(5855):1469–72.
162. Widiker S, Karst S, Wagener A, et al. High-fat diet leadsto a decreased methylation of the MC4R gene in the obeseBFMI and the lean B6 mouse lines. J Appl Genet.2010;51(2):193–7.
163. Choy JS, Wei S, Lee JY, et al. DNA methylation increases nucle-osome compaction and rigidity. J Am Chem Soc. 2010;132(6):1782–3.
164. Plagemann A, Harder T, Brunn M. Hypothalamicproopiomelanocortin promoter methylation becomes alteredby early overfeeding: an epigenetic model of obesity andthe metabolic syndrome. J Physiol. 2009;587(20):4963–76.
165. Milagro FI, Campión J, Garcia-Diaz DF, et al. High fat diet-induced obesity modifies the methylation pattern of leptin pro-moter in rats. J Physiol Biochem. 2009;65(1):1–9.
166. Han JC, Lawlor DA, Kimm SYS. Childhood obesity. Lancet.2010;375:1737–48.
Curr Obes Rep (2014) 3:16–37 37