Ethiopia: Focusing our Program for Impact & Efficiency Jocelyn Felter Brown Acting Coordinator,...

If you can't read please download the document
-
Upload
albert-nichols -
Category
Documents
-
view
213 -
download
0
Transcript of Ethiopia: Focusing our Program for Impact & Efficiency Jocelyn Felter Brown Acting Coordinator,...
- Slide 1
- Ethiopia: Focusing our Program for Impact & Efficiency Jocelyn Felter Brown Acting Coordinator, PEPFAR Ethiopia AIDS 2014 Stepping Up The Pace
- Slide 2
- Ethiopia Important Features Population 90 million Predominantly rural agrarian country Growing economy with large infrastructure development projects Low/decreasing national HIV/AIDS prevalence: 1.4% Has reached the Tipping Point Significant Urban to Rural HIV/AIDS disparity: mixed epidemic Government is the primary service provider Strong political commitment to health & equity of services Significant Global Fund investment, but expected to decline with New Funding Model
- Slide 3
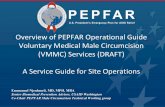
- Ethiopia: Three Ways of Looking at HIV Distribution: Prevalence, No. Infected, and Density, 2011
- Slide 4
- PEPFAR Expenditures by Geographic Location & HIV Burden with Adult Prevalence 4 Source: HIV Related Estimates and Projections for Ethiopia 2012. Excludes National and Above National Spending
- Slide 5
- Focusing the Program: Start with Clinical Care & Treatment 201320142015 Number of Adults in need of ART * 431,761530,835542,632 National Coverage Rate & Goals @69% = 298,33680% 434,106 Adoption of 2013 WHO Guidelines *Source: Spectrum HIV Related Estimates and Projections for Ethiopia, 2014
- Slide 6
- Focus on Clinical Care & Treatment HistoricallyUS University treatment partners led clinical care & treatment efforts Partners accomplished what they were brought to Ethiopia to do; time to move more responsibility to Government of Ethiopia Promising results from transition of University partners to Regional Health Bureaus in 3 regions demonstrated success and ability to manage funding Assumption is that we can achieve same treatment goals, at same level of quality, but more efficiently across all regions
- Slide 7
- Achieving Efficiency in Clinical Care & Treatment * 2014 reflects the COP14 submission, new funds only USD, in millions PEPFAR/HHS-Ethiopia Funding, by Partner Type
- Slide 8
- Defining Our Core Understand: 1.Current state of epidemicand how its expected to change 2.National Response: What is USGs current role -- how might or should it change? 3.What are roles of other HIV Donors, Global Fund, Government, private sector -- how might they change? Design: 1.What are the core program elements/critical enablers required to Save Lives and Prevent New Infections? 2.What are the core program elements /critical enablers USG is uniquely qualified to deliver? 3.How and when and to whom should non-core programs/non- critical enablers transition or end? 4.What is the cost of the core program? 8 We adapted the UNAIDS Investment Case Framework to further focus and rationalize our PEPFAR program in Ethiopia
- Slide 9
- Prioritizing Activities Activities critical to saving lives, preventing new infections - and/or which USG is uniquely qualified Core Activities that directly support our goals and cannot yet be done well by other partners or host govt. Near Core Activities that do not directly serve our HIV/AIDS goals and/or can be taken on by other partners or host govt or civil society. Non Core Must Do Should Do Nice to Do 9
- Slide 10
- Treatment Prevention (High & Med Risk) Targeted Testing Supply Chain TA HIV/AIDS Commodities Evidence Base (SI, SS, M&E) HC Financing/Insurance Training HMIS OVC (incl. ES) Non- Core Blood Safety TA to Private Sector Health Svcs VMMC In-School Youth funding to MOE Leadership and Governance (w/ transition plan) Community/Peer Support Ongoing Construction Commitments Economic Strengthening ( non-OVC) TA In-school Youth prevention Low-risk prevention (GPY) PPP TA Infection Prevention Cross-border Cervical cancer screening Near- Core Core Defining the Core: Results
- Slide 11
- Using Data to Maximize Program Investment Evidence Base Analysis Utilized most current ANC surveillance data to ensure sufficient support in regions and refugee sites with increasing prevalence Tracked those emerging regions transected by major transport corridors and targeted funding toward hottest Hot Spots Assessed areas where HRH capacity is most limited and targeted ToT support Economic Analysis We utilized national PEPFAR expenditure data to calculate unit expenditures, which allowed us to cost our programs core interventions Expenditure data at regional and partner level prompted refinement to certain activities and regional interventions Site-Level Analysis Directed spend toward highest-volume and highest-yield facilities; reduced spend to facilities with low-volume/low-yield
- Slide 12
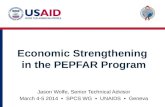
- Geographic Analysis: HIV+ yield distribution across PMTCT sites 80% (14,260) of patients in 22% (371) of 1,668 sites Key: High Yield = >1 patient/month Low Yield =
- Slide 13
- Stakeholder Coordination Government Years of successful TA and strong Govt support ensure readiness to take over Cervical Cancer, Infection Prevention, VMMC, Blood Safety Extensive Govt led Health Extension Worker program is able to take on more Community-focused activities Global Fund Revolving fund for ES allows PEPFAR to focus on OVC House Holds On-going HSS funding can support health infrastructure needs Commitment to significant funding of ARVs, RTKs Civil Society & Private Sector Years of USG and Global Fund support have capacitated CSOs to take on more Community and Peer Support activities Years of TA to Private Sector providers have strengthened their ability to serve clients and support business With a more focused PEPFAR program, on-going stakeholder alignment is key to sustain gains and prevent service gaps
- Slide 14
- ETHIOPIA HAS A REAL CHANCE AT AN AIDS FREE GENERATION Thank You