ESVNU Pre Congress Day 2017esvnu.eu/Media/ESVNU/resources/ESVNU Pre Congress day 2017... · ESVNU...
33
ESVNU Pre-Congress Day 2017 PROCEEDINGS sponsored by
Transcript of ESVNU Pre Congress Day 2017esvnu.eu/Media/ESVNU/resources/ESVNU Pre Congress day 2017... · ESVNU...
ESVNU Pre-Congress Day 2017
PROCEEDINGS
sponsored by
ESVNU Pre-Congress Day - PROCEEDINGS Page 2
Lecture Title Speaker Page
Advanced diagnostic imaging of the urinary tract
Randi Drees, UK Dr. med. vet., PhD, DipACVR,
DipECVDI, MRCVS
3
Decision making in canine urolithiasis
Larry Adams, USA DVM, PhD, DipACVIM
7
Challenges associated with management of canine ureterolithiasis and nephrolithiasis
Larry Adams, USA DVM, PhD, DipACVIM
11
Management of feline ureterolithiaisis: Is there room for improvement?
Zoe Halfacree, UK MA, VetMB, CertVDI, CertSAS,
FHEA, DipECVS
15
SDMA and feline urolithiasis Jane Robertson, USA DVM, DipACVIM-SAIM
IDEXX
Hereditary urolithiasis in dogs and cats
Urs Giger, USA Dr. med. vet., MS, FVH,
DipACVIM&ECVIM, DipECVCP
20
What’s new in the nutritional management of canine and feline urolithiasis
Iveta Becvarova, CH DVM, MS, DipACVN Hill’s Pet Nutrition
24
Acquired and inherited Fanconi Syndrome Urs Giger, USA Dr. med. vet., MS, FVH,
DipACVIM&ECVIM, DipECVCP
30

ESVNU Pre-Congress Day - PROCEEDINGS Page 3
Advanced diagnostic imaging of the urinary tract Randi Drees, Dr. med. vet., PhD, DipACVR, DipECVDI, MRCVS
Royal Veterinary College, Hawkshead Lane, North Mymms, Hatfield, Hertsfortshire,
AL9 7TA, UK
Conventional radiography
Using standard radiography, five opacities can be differentiated in radiographs, namely metal, mineral, soft
tissue, fat and gas. The kidneys are located in the retroperitoneum and outlined surrounded by fat and the
urinary bladder is surrounded by peritoneal fat, which enables to see these soft tissue organs. The normal
ureters are small and are thus usually not visible on conventional radiographs, though in obese cats using a
high quality digital radiography system these are visible occasionally.
Radiography allows to evaluate shape, size, margination, number and opacity of the organ. This can be
limited by superimposition of the three-dimensional structures of the patient in the two-dimensional
images created, in addition the cranial pole of the right kidney is often poorly visible, as it abuts the
caudate lobe of the liver, that is also soft tissue opaque. Conventional radiography remains a valuable tool
for surveying the urinary tract for evidence of presence of mineralized uroliths, rupture of the urinary tract
or altered anatomy.
Contrast radiography
To supplement the information gained from conventional radiographs, iodine based contrast media are
used to highlight the urinary tract. Studies can be performed in an antegrade fashion either by i.v. injection
of a contrast medium into the venous system or by direct injection of the contrast into the dilated renal
pelvis. The iodine based contrast media are excreted via glomerular filtration and after i.v. injection, a
vascular (approximately 5-10s post injection), nephrogram (i.e. parenchymal, approximately 10s to 2min
post injection) and pyelogram (i.e. excretory, starting approximately 2-3min post injection) phase can be
observed. Excretory urograms allow for a good depiction of the renal architecture. Since the iodinated
contrast medium is delivered through the glomerular vessels and filtrated into the nephron only, duration
and degree of kidney opacification in the excretory urogram is an indication, although not a very precise
one, for renal function. Duration and intensity of the renal opacification during the study depends on the
dose of contrast medium administered, renal perfusion, glomerular filtration, tubular reabsorption of
water, hydration status of the patient as well as patency of the renal outflow tract. The ureters are to be
followed to their termination at the dorsal aspect of the bladder neck, where they enter the urinary
bladder wall to terminate in the lumen at the ureterovesical junction. Antegrade pyelography is performed
ultrasound guided, and preferred in azotemic patients without loss of image quality due to reduced renal
function. It only highlights the collecting system, and is not depending on renal function. Evaluation of
ureteral location and patency can be made. Retrograde studies remain useful to determine the anatomy
and patency of the male urethra and the female vestibulovaginal and urethral structures. Studies may be
performed using conventional radiography or fluoroscopy.

ESVNU Pre-Congress Day - PROCEEDINGS Page 4
Computed tomography (CT)
The x-ray technology used in CT is comparable to that of the conventional radiography system in that it
uses ionizing radiation, though cross-sectional images are acquired. Using CT, superimposition is eliminated
and over 4000 grey shades can be resolved, which allows for example differentiation of fluid from soft
tissue; smaller mineral foci can be resolved especially by using lower kV settings. Anatomical resolution
depends on the imaging parameters used and especially the elimination of superimposition allows exact
depiction of the urinary structures. Multiplanar and 3D reconstructions can add valuable anatomical
information about the urinary structures. Post contrast CT exams are helpful to highlight the renal and
excretory system, and depending on the timing(s) of the study, an excretory urogram can be performed in
the CT exam. Vascular phase images are acquired ideally with bolus tracking software or test bolus
technique to depict the arterial and venous structures in the first 10s after contrast injection. Nephrogram
images are usually acquired 1min after injection of contrast medium, adequate ureteral opacification is
seen approximately 3minutes post injection, though multiple scans may be necessary to depict the entire
ureter filled with contrast, due to the peristalsis present. Computed tomography methods for
determination of the glomerular filtration rate (GFR) have been published, allowing for exaction of global
and split renal function, though the results vary between authors; commonly CT GFR underestimates GFR
established with conventional methods. To ideally depict the ureterovesical junction, the patient is to be
placed in ventral recumbency, so that the urine can ‘drizzle’ into the urine filled urinary bladder from
dorsally. For optimal depiction of the ureters, multiple techniques have been described, aiming to optimize
ureteral opacification and minimize repeat scanning. Additional furosemide injection or multiphase
injection protocols have been proposed as well as bolus tracking over the distal ureter to optimize scan
timing. Determining extramural from intraumural ectopic ureter location can remain challenging, especially
if the ureter runs in close proximity to the urinary bladder neck or urethra. Retrograde studies can
theoretically be performed CT guided, yet the technique has not been well established; diluted contrast is
used and administration of contrast during the scan through a catheter placed may require personnel in the
CT exam suite using shielding.
Ultrasonography
The ultrasound exam uses soundwaves to evaluate renal architecture and vascularity, different tissue
parameters are evaluated compared to exams using ionizing radiation. The renal cortex can be
differentiated from the medulla and the cortex should be hyperechoic to the medulla. Organ comparisons
have been described, and the left renal cortex should be hypoechoic to the spleen and the right iso- or
mildly hyperechoic to the liver. Cats may have fat deposition in their renal cortex, leading to
hyperechogenicity. The interlobar vessels and pelvic diverticula may give the medulla a lobulated
appearance; the arcuate vessels can be seen as hyperechoic striations at the corticomedullary border. The
renal pelvis can be seen as a small anechoic line in the normal kidney. The normal ureters are usually only
visible using high resolution ultrasound probes and best when they are mildly dilated, uroliths can be
detected. Since conventional radiography cannot differentiate soft tissue from fluid, nor resolve the
internal architecture of the kidneys, ultrasound has found a prominent role in anatomical evaluation of the
urinary tract. A quantitative study evaluating the correlation of cortical echogenicity with renal
histopathology found limited relevance for detecting chronic renal disease in dogs whereas ehogenecity
was correlated with severe renal damage in cats; overall sensitivity and specificity for correlating cortical
disease was low.

ESVNU Pre-Congress Day - PROCEEDINGS Page 5
Doppler ultrasound allows for assessment of the renal vessels, the resistive index has been established
normal as less than 0.72 in dogs and 0.7 in cats, and the pulsatility index as no greater than 1.52 in dogs and
1.29 in cats.
Elastography is introduced into veterinary practice and helps to evaluate the stiffness or elasticity of a
tissue in conjunction with conventional B-mode ultrasonography; shear wave elastography or strain
elastography are the two main techniques employed. Reliable clinical applications of this technique are to
be developed.
Contrast enhanced ultrasound uses microbubbles that are injected intravenously and aids to determine
tissue perfusion. Several studies have established normal perfusion pattern in dogs and cats; the sedation
protocol used has shown impact on the perfusion curves. Evaluation of renal transplants, focal space
occupying lesions and renal hemorrhage have been described.
Magnetic resonance imaging (MRI)
MRI has found very limited application in veterinary patients for evaluation of the urinary tract, likely due
to the availability of the other modalities as well as the limitations of the modality with need for general
anesthesia and cost involved. In people, structural renal disease, perfusion and function are analyzed using
MRI. Magnetic resonance angiography has been employed for evaluation of the arterial and venous phase
in dogs, that may serve for vascular evaluation in cases of transplant or surgical planning. MRI
nephrography has allowed to extract time-intensity curves in addition to excellent anatomical detail.
Scintigraphy
Inherently, scintigraphy images have low spatial or anatomical resolution and are mainly used for functional
evaluation. Technetium-99m diethylenetriamine pentaacetic acid is usually injected as a radioactive tracer
and can resolve combined and split renal function. Availability is often limited to specialty centers, though
the techniques for evaluation of renal function as well as diuretic renal scintigraphy have been well
established.
Excretory urography using computed tomography in a dog: Nephrogram and pyelogram phase 30s, 3min
and 6min post contrast injection.

ESVNU Pre-Congress Day - PROCEEDINGS Page 6
Ectopic ureters in a dog depicted using computed tomography excretory urography; pyelogram phase.
Transverse plane image at the level of the urethra (center, bottom arrow), showing the ectopic ureter to
the left and right (top arrows) and 3D volume rendering.
Selected references
Alexander K, Authier S, del Castillo JR, Arora V, Qi S, Guillot M, Beauchamp G, Troncy E. Contrast Media Mol
Imaging. 2010 May-Jun;5(3):133-9
Banzato T, Bonsembiante F, Aresu L, Zotti A. BMC Vet Res. 2017 Jan 17;13(1):24.
Cavrenne R, Mai W. Vet Radiol Ultrasound. 2009 Jan-Feb;50(1):58-64.
Feeney DA, Sharkey LC, Steward SM, Bahr KL, Henson MS, Ito D, O'Brien TD, Jessen CR, Husbands
BD, Borgatti A, Modiano JF. Comp Med. 2013 Apr;63(2):174-82.
Fonseca-Matheus JM1, Pérez-García CC, Ginja MM, Altónaga JR, Orden MA, Gonzalo-Orden JM. Vet J. 2011
Sep;189(3):341-5.
Granger LA, Armbrust LJ, Rankin DC, Ghering R, Bello NM, Alexander K. Vet Radiol Ultrasound. 2012 Mar-
Apr;53(2):181-8
Haers H, Vignoli M, Paes G, Rossi F, Taeymans O, Daminet S, Saunders JH. Veterinary Radiology &
Ultrasound, Vol. 51, No. 5, 2010, pp 516–522.
Holdsworth A, Bradley K, Birch S, Browne WJ, Barberet V. Vet Radiol Ultrasound. 2014 Nov-Dec;55(6):620-7
Jeon S, Lee G, Lee SK, Kim H, Yu D, Choi J. Vet Radiol Ultrasound. 2015 Jul-Aug;56(4):425-31
Leinonen MR1, Raekallio MR, Vainio OM, Ruohoniemi MO, Biller DS, O'Brien RT. Am J Vet Res. 2010
Nov;71(11):1305-11
O'Dell-Anderson KJ, Twardock R, Grimm JB, Grimm KA, Constable PD. Vet Radiol Ultrasound. 2006 Mar-
Apr;47(2):127-35
Schweiger S, Ohlerth S, Gerber B. Acta Vet Scand (2015) 57:80
https://www.ncbi.nlm.nih.gov/pubmed/?term=Cavrenne%20R%5BAuthor%5D&cauthor=true&cauthor_uid=19241755
https://www.ncbi.nlm.nih.gov/pubmed/?term=Sharkey%20LC%5BAuthor%5D&cauthor=true&cauthor_uid=23582424
https://www.ncbi.nlm.nih.gov/pubmed/?term=Steward%20SM%5BAuthor%5D&cauthor=true&cauthor_uid=23582424
https://www.ncbi.nlm.nih.gov/pubmed/?term=Borgatti%20A%5BAuthor%5D&cauthor=true&cauthor_uid=23582424
https://www.ncbi.nlm.nih.gov/pubmed/?term=Modiano%20JF%5BAuthor%5D&cauthor=true&cauthor_uid=23582424
https://www.ncbi.nlm.nih.gov/pubmed/?term=Taeymans%20O%5BAuthor%5D&cauthor=true&cauthor_uid=20973385

ESVNU Pre-Congress Day - PROCEEDINGS Page 7
Decision making in canine urolithiasis Larry Adams, DVM, PhD, DipACVIM-SAIM
Purdue University College of Veterinary Medicine, West Lafayette, Indiana, USA
Introduction
Effective management of urolithiasis involves both removal of the uroliths and prevention of recurrence.
Removal of bladder and urethral stones has traditionally been by open cystotomy and urethrotomy.
Surgical removal is usually effective for uroliths in the bladder and urethra, although post-operative
radiographs should be performed to confirm complete removal. Uroliths may be inadvertently left in the
urinary tract in 10-20% of dogs following open cystotomy, with the majority of the uroliths remaining in the
urethra. These remaining urethroliths may be removed by laser lithotripsy or basket extraction to avoid an
additional surgery. Minimally invasive management techniques often can be used to replace open surgical
removal of uroliths. Minimally invasive techniques include medical dissolution, voiding urohydropropulsion,
cystoscopic basket extraction, laser lithotripsy and laparoscopic-assisted cystotomy. Prevention of
recurrence should be based on quantitative analysis from a veterinary urolith center.
The decision about which approach to pursue for urolith removal is influenced by multiple factors including
the potential for medical dissolution of the suspected urolith type, number and location of uroliths,
clinician experience with minimally invasive options, owner preferences and availability of specialized
equipment.
Medical dissolution
Medical dissolution is effective for some uroliths locations and types. Urocystoliths and nephroliths are
amenable to dissolution whereas ureteroliths and urethroliths are not without additional procedures.
Struvite, urate, and cystine uroliths may be medically dissolved whereas calcium oxalate, calcium
phosphate, silica and compound uroliths cannot be medically dissolved. For dissolution to occur, uroliths
must be surrounded by under-saturated urine to allow the crystals to go back into solution. Medical
dissolution of urocystoliths in male dogs is associated with risk of urethral obstruction once the uroliths are
small enough to pass into the urethra; however, dissolution is often successful without urethral
obstruction. The risk of leaving uroliths in the urinary tract after cystotomy is likely higher than the risk of
urethral obstruction during dissolution of uroliths.1
Struvite uroliths in dogs are usually infection-induced from infection to urease producing bacteria. Over
90% of struvite stones in dogs are caused by UTI with Staphylococcus and Proteus. Other urease-producing
organisms that infrequently cause struvite uroliths include Pseudomonas spp, Klebsiella spp,
Corynebacterium urealyticum and mycoplasmas such as Ureaplasma urealyticum.2 Medical dissolution of
infection-induced struvite urocystoliths requires a combination of appropriate antimicrobial and calculolytic
dietary therapy. Antimicrobial selection should be based on urine culture obtained by cystocentesis prior to
antimicrobial therapy. Antimicrobial therapy must be given throughout the entire dissolution period
because viable bacteria are contained within the layers of struvite uroliths. Commercial diets that aid in
dissolution of struvite uroliths in dogs include Hill’s Prescription diet s/d, Hill’s Prescription diet c/d,
Purina UR, and Royal Canin S/O Lower Urinary Tract Support Diet. Antimicrobial and dietary therapy
should continue approximately 1 month beyond radiographic resolution of struvite urolithiasis or until

ESVNU Pre-Congress Day - PROCEEDINGS Page 8
resolution of uroliths on ultrasonography. One week after initiation of antimicrobial therapy, urine should
be obtained by cystocentesis for urinalysis and culture. Urinalysis should reveal decrease of the urine pH to
<6.5 and the urine culture should be negative for bacterial growth. If the UTI is persistent, antimicrobial
therapy should be changed on the basis of urine culture and sensitivity testing. Monitoring of dissolution
therapy should consist of abdominal radiographs and urinalyses every 3-4 weeks. If bacteriuria, pyuria or
inappropriate alkaline urine pH are present, the urine should be re-cultured. Prevention and treatment of
recurrent UTI is critical for prevention of infection-induced struvite uroliths in dogs.
If the owner is motivated to avoid surgery, then retrograde urohydropropulsion of urethroliths followed by
medical dissolution of struvite urocytoliths should be considered. Once the active UTI is controlled by
appropriate antibiotic therapy, the clinical signs of pollakiuria and dysuria often resolve thereby lowering
the risk of recurrent urethral obstruction. Similarly, ureteroliths may be bypassed using ureteral stent
placement for medical dissolution of suspected infection-induced struvite ureteroliths in dogs.
Voiding urohydropropulsion
Voiding urohydropropulsion is the removal of smaller urocystoliths by inducing voiding while the dog is
positioned vertically so that urocystoliths pass during voiding.3 General anesthesia is required for complete
urethral relaxation, preventing development of high intravesicular pressures that could cause iatrogenic
trauma to the bladder wall. If the bladder is not distended with urine, it is distended with sterile saline via
cystoscopy or urethral catheterization. The dog is positioned so that the spine is roughly 25 degrees caudal
to a line perpendicular to the effects of gravity, such that a line drawn through the urethra into the bladder
is approximately vertical. The bladder is agitated side to side to cause the urocystoliths to settle in the
trigone by gravity. The bladder is palpated and the intravesicular pressure is gradually increased by manual
compression of the bladder to initiate a detrusor contraction. Once voiding begins, the bladder is
compressed more firmly to attempt to maintain maximum urine flow to flush out the cystoliths. The
bladder is refilled with sterile saline through the cystoscope or a urinary catheter and the process is
repeated until no urocystoliths are passed with the expelled fluid. Then post-procedural radiographs or
cystoscopy are performed to confirm complete removal of the urocystoliths. Digital flexible ureteroscopes
and high definition cameras for rigid cystoscopes permit visualization of smaller uroliths than digital
radiographs and may eliminate the need for post-procedural radiographs.
Laser lithotripsy
If available, laser lithotripsy using the holmium: YAG laser is an option for fragmentation of cystoliths that
are too large for voiding urohydropropulsion.4 The holmium laser energy is absorbed in <0.5 mm of fluid,
allowing it to safely fragment uroliths within the urethra or bladder without damage to adjacent mucosa.
Success rates for complete urolith removal with laser lithotripsy using the holmium laser are similar to open
cystotomy for female dogs and larger male dogs with relatively small “stone burdens”.4-6 Laser lithotripsy is
preferred over urethrotomy for removal of urethroliths assuming the dog is large enough to allow passage
of the cystoscope.4 For 1-4 urethral calculi, laser lithotripsy and basket extraction of the urolith fragments is
successful in almost 100% of dog provided the urethral diameter allows for passage of the flexible
ureteroscope.1 Unfortunately, urethral strictures are present in up to 20% of dogs with recurrent
urethroliths due to current or prior urethral injury. Urethral strictures may preclude passage of the
ureteroscope, thereby requiring retrograde urohydropropulsion and removal of the uroliths from the
urinary bladder.

ESVNU Pre-Congress Day - PROCEEDINGS Page 9
Male dogs with large stone burdens are not good candidates for removal of cystoliths by laser lithotripsy. In
general, laser lithotripsy should be limited to no more than 4 urethral or 2 bladder uroliths.7 Likewise male
dogs smaller than 5-7 kg may be too small for this transurethral cystoscopic technique. Alternatively,
laparoscopic-assisted cystolithotomy or percutaneous cystoscopic cystolithotomy may be utilized for male
dogs.1,8 If these minimally invasive options are available, the owner should be advised that non-invasive
urolith removal may be preferable to open surgical cystotomy.1 Percutaneous cystoscopic cystolithotomy
may achieve complete urolith removal more often than open cystotomy.
Table 1. Guidelines for selection of minimally invasive options (modified from reference 7)
Management of urolith recurrence
Calcium oxalate uroliths tend to recur in most dogs with recurrence rates of up to 50% within 3 years of
initial diagnosis.1 Avoiding cystotomy and closure of the bladder with sutures eliminate the risk of suture-
induced urolith recurrence, which may be responsible for up to 9% of recurrent urolith cases. Therefore
preventative measures such as diet and medications should be utilized to reduce the risk of recurrence.
Dietary changes should be attempted; additional medications are recommended if there is persistent
calcium oxalate crystalluria or recurrence of calcium oxalate urolithiasis. Increased water intake though
feeding a canned diet or by adding water to the diet may be the most important recommendation to help
prevent recurrence of calcium oxalate urolithiasis in dogs.
The commercial diets recommended to reduce the risk of calcium oxalate urolith recurrence in dogs include
Royal Canin Canine Urinary S/O Diet, Purina UR, and Hill’s Prescription diet c/d MultiCare. Dietary therapy
alone will not always prevent calcium oxalate urolith recurrence. Hydrochlorothiazide (2 mg/kg PO q12h)
should be considered in dogs that have persistence of calcium oxalate crystalluria or recurrence of calcium
Procedure Urolith size limit Patient size limit Equipment required Comments and limitations
Voiding urohydropropulsion
Male dog: 2 mm Female dog: 3-4 mm
Any size patient -Urinary catheter for male dogs -Rigid cystoscope or urinary catheter for female dogs
Often easier to fill the urinary bladder using a rigid cystoscope in female dogs rather than repeat urethral catheterization.
Basket extraction via cystoscopy
Male dog: 2-3 mm Female dog: 4-5 mm
Large enough to accept an appropriately sized cystoscope
Cystoscope and various sized stone baskets
The operator should be prepared for laser lithotripsy.
Laser Lithotripsy
Male dog: 5 mm Female dog: 10 mm
Must be able to pass cystoscope comfortably. Urethral strictures may prevent passage of cystoscope.
Various cystoscopes Ho: YAG laser with laser fibers
1) <4 urethral stones in males 2) <4 cystoliths that require fragmentation in female dogs 3) <2 cystoliths that require fragmentation in male dogs.

ESVNU Pre-Congress Day - PROCEEDINGS Page 10
oxalate urolithiasis despite diet therapy. Thiazide diuretics cause subclinical volume depletion resulting in
increased proximal tubular reabsorption of sodium and calcium. Once dietary and hydrochlorothiazide
therapy have been implemented, if calcium oxalate crystalluria is persistent or calcium oxalate uroliths
recur, potassium citrate should also given to adjust the urine pH to 6.5—7.0 using a starting dose of 50—75
mg/kg PO q12h. The serum potassium should be initially monitored initially with potassium citrate
supplementation and the dose reduced if hyperkalemia occurs.
Because calcium oxalate uroliths commonly recur, appropriate surveillance using radiographs should be
utilized to document recurrences before the uroliths become too large to void. If small recurrent
urocystoliths are diagnosed, many recurrences may be managed by voiding urohydropropulsion. Avoiding
cystotomy and closure of the bladder with sutures eliminates the risk of suture-associated urolith
recurrence, which may be responsible for up to 9% of recurrent urolith cases.9 Suture-associated uroliths
are usually S or C shaped and may be attached to the bladder wall in some cases.
When the appropriate option is “watchful waiting”
Asymptomatic dogs and cats with non-dissolvable uroliths too large to pass into the urethra or too irregular
to cause a urethral obstruction may need only periodic monitoring and appropriate client education.1
Likewise, non-dissolvable uroliths smaller than 1 mm don’t require removal by voiding urohydropropulsion
until the uroliths enlarge enough to justify an intervention at a later date. For these situations, periodic
monitoring with abdominal radiographs every 3-6 months may be the most appropriate plan.
References
1. Lulich JP, Berent AC, Adams LG, et al. ACVIM Small Animal Consensus Recommendations on the
Treatment and Prevention of Uroliths in Dogs and Cats. J Vet Intern Med 2016;30:1564-1574.
2. Adams LG, Syme HM. Canine ureteral and lower urinary tract diseases In: Ettinger SJ,Feldman BF,
eds. Textbook of Veterinary Internal Medicine. St. Louis: Saunders Elsevier, 2010;2086-2115.
3. Lulich JP, Osborne CA, Sanderson SL, et al. Voiding urohydropropulsion. Lessons from 5 years of
experience. Vet Clinics of N Am Small Anim Practice 1999;29:283-291.
4. Adams LG, Berent AC, Moore GE, et al. Use of laser lithotripsy for fragmentation of uroliths in dogs:
73 cases (2005-2006). J Am Vet Med Assoc 2008;232:1680-1687.
5. Bevan JM, Lulich JP. Comparison of laser lithotripsy and cystotomy for the management of dogs with
urolithiasis. J Am Vet Med Assoc 2009;234:1286-1294.
6. Lulich JP, Osborne CA, Albasan H, et al. Efficacy and safety of laser lithotripsy in fragmentation of
urocystoliths and urethroliths for removal in dogs. J Am Vet Med Assoc 2009;234:1279-1285.
7. Berent AC, Adams LG . Minimally-invasive treatment of bladder and urethral stones in dogs and cats
In: Weiss CW, Berent A.C., ed. Veterinary Imaging-Guided Interventions. Ames, Iowa: Wiley-Blackwell
Publishing, 2015;360-372.
8. Runge J, Berent A, Weisse C, Mayhew P. Transvesicular percutaneous cystolithotomy for the retrieval
of cystic and urethral calculi in dogs and cats: 27 cases (2006-2008). J Am Vet Med Assoc 2011;
239:344-349.
9. Appel SL, Lefebvre SL, Houston DM, et al. Evaluation of risk factors associated with suture-nidus
cystoliths in dogs and cats: 176 cases (1999–2006). J Am Vet Med Assoc 2008;233:1889–1895.

ESVNU Pre-Congress Day - PROCEEDINGS Page 11
Challenges associated with management of canine
ureterolithiasis and nephrolithiasis Larry Adams, DVM, PhD, DipACVIM-SAIM
Purdue University College of Veterinary Medicine, West Lafayette, Indiana, USA
Introduction
Nephroliths and ureteroliths pose unique challenges to the clinician compared to lower tract uroliths. Nephroliths may obstruct the renal pelvis or ureter, may predispose to pyelonephritis, and may result in compressive injury of the renal parenchyma leading to renal failure. Nephroliths may be considered incidental or "inactive" if they are not causing any of these complications. Inactive nephroliths do not require removal, but they should be monitored periodically by urinalysis, urine culture, and radiography. Indications for intervention for nephroliths and ureteroliths in dogs include obstruction of the ureteral pelvic junction (UPJ) or ureter, relapsing UTI from infected uroliths, progressive nephrolith enlargement, and nephroliths located near the UPJ of a solitary functional kidney.1-3 The major indication for removal of upper tract uroliths in cats is obstructive ureteroliths.3,4,5
Unlike humans with ureteroliths that tend to move in an antegrade fashion due to the effects of gravity, spontaneous retrograde movement of ureteroliths in dogs and cats may result in relieve of ureteral obstruction.6 Furthermore, we have also documented uroliths moving from the renal pelvis into the proximal ureter, and back into the renal pelvis in some animals.6
Calcium oxalate was the most common composition of nephroliths in dogs and cats. The second most common composition of upper tract uroliths in dogs is struvite associated with urease-producing bacterial UTI. The second most common nephrolith composition in cats is dried solidified blood calculi.7,8 Calcium oxalate and dried solidified blood calculi are not amendable to medical dissolution thereby limiting the treatment options for these uroliths.
Clinical signs
Many dogs with nephroliths are asymptomatic and the nephroliths are diagnosed during work up of other problems. Potential clinical signs associated with upper tract uroliths include hematuria, recurrent UTI, fever, vomiting, abdominal or lumbar pain, and uremia from bilateral ureteral obstruction or progressive renal injury resulting in renal damage.1,9 Ureteroliths may be bilateral, or one kidney may be non-functional from prior ureteral obstruction when a subsequent ureterolith obstructs the contralateral kidney resulting in an acute uremic crisis. Diagnosis
Radiodense nephroliths and ureteroliths are usually diagnosed by abdominal radiography. Ultrasonography or excretory urography may be used to confirm the presence, size, and number of nephroliths and ureteroliths; however, ultrasonographic confirmation of ureteroliths is not always possible. Documentation of upper tract uroliths accompanied by progressive renal pelvic dilation is highly suggestive of obstructive ureteroliths even if the ureterolith is not documented directly by ultrasonography.5 Animals with ureteral obstruction may have poor excretion of dye during excretory urography and identification of the cause of ureteral obstruction may be facilitated by antegrade pyelography via nephropyelocentesis. The author prefers to perform contrast ureterogram via nephropyelocentesis as part of an interventional procedure rather than as an isolated diagnostic procedure. Another excellent imaging modality to confirm upper tract uroliths is CT scan performed before and after contrast administration.

ESVNU Pre-Congress Day - PROCEEDINGS Page 12
Urinalysis results from animals with nephroliths or ureteroliths may reveal hematuria and crystalluria. Crystal identification and urine pH may be helpful in predicting urolith composition. Likewise, collection of small uroliths from the urinary bladder may be used to determine likely composition of concurrent upper tract uroliths. Pyuria and bacteriuria may be noted in patients with concomitant UTI and infection-induced uroliths. Urine culture should be performed on urine obtained by cystocentesis because concurrent UTI is relatively common.5 Serum chemistry profile and CBC may indicate systemic abnormalities that have resulted from or contributed to formation of nephrolithiasis. Dogs with pyelonephritis or pyonephrosis and concurrent ureteral obstruction may have an inflammatory leukogram and thrombocytopenia.9 Anemia is also common in animals with CKD from obstructive ureteroliths. Azotemia may be present with bilateral renal disease or bilateral obstruction. Dogs that have alkaline urine pH, UTI, struvite crystalluria and staghorn-shaped radiodense nephroliths most likely have struvite nephroliths.
Treatment of nephroliths and ureteroliths
Treatment options for nephroliths include monitoring of inactive nephroliths, surgery, medical dissolution, and extracorporeal shock wave lithotripsy. Calcium oxalate, calcium phosphate and matrix nephroliths are not amenable to dissolution. Ureteroliths are also not amenable to medical dissolution because they are not bathed in under-saturated urine unless the obstruction is bypassed with a ureteral stent. Medical dissolution of ureteroliths may be facilitated by placement of a ureteral stent to induce passive ureteral dilation. In most dogs, the nephroliths are surrounded by renal tissue such that pyelolithotomy is not possible, so nephrotomy is the only open surgical option.10,11 In one study, neither intersegmental nor bisection nephrotomy adversely affected GFR; however complete nephrolith removal via nephrotomy is challenging.11 Percutaneous nephrolithomy (PCNL) is used to remove large staghorn nephroliths in humans, and PCNL and surgically-assisted endoscopic nephrolithomy (SENL) have been performed in dogs for removal of larger nephroliths.3 For obstructive ureteroliths, ureterotomy may be performed in dogs but is associated with a number of potential complications. Ureterotomy requires microsurgical experience and post-operative complications are common compared to ureteral stents.4
Ureteral stent placement for ureteroliths
Ureteral stents are useful for management of ureteral obstruction from ureteroliths in dogs.4 Ureteral stents can be placed retrograde via cystoscopy in female dogs and induce passive ureteral dilation within 2-4 weeks.12 In male dogs, ureteral stent placement may require open cystotomy, laparoscopic-assisted cystostomy or temporary perineal access.13 Placement of a ureteral stent bypasses the ureteral obstruction created by the stone and the stent causes passive dilation of the ureter.12 Once the ureter has dilated, the ureteral stone may pass around the ureteral stent. Alternatively, ureteral stents may be left in place long-term; however there is a risk of stent mineralization (encrustation) that may occlude the stent. If this occurs and the obstruction is detected early, then the stent can be exchanged for a new stent either by cystoscopy or surgery. Once the ureter passively dilates from the ureteral stent, ureterorenoscopy using flexible digital ureteroscope is possible in medium sized or larger dogs.12 Ureterorenoscopy for removal of nephroliths is possible with use of appropriate sized urologic guidewires, ureteral access sheath placement, flexible stone baskets, and concurrent fluoroscopy.
Extracorporeal shock wave lithotripsy in dogs
Extracorporeal shock wave lithotripsy (ESWL) is fragmentation of uroliths using shock waves are generated outside the body.1 ESWL uses repeated shock-waves to fragment the nephrolith into many small fragments that can pass spontaneously through the excretory system. We originally reported the safety and efficacy of ESWL for the treatment of canine nephroliths and ureteroliths from our first 5 cases.2 The author has treated 200 dogs with ESWL for fragmentation and removal of nephroliths and ureteroliths. ESWL treatment was successful in approximately 85% of the dogs with calcium containing nephroliths.1 Overall approximately 30% of dogs required more than one ESWL treatment for complete fragmentation of their nephroliths. For dogs with obstructed ureteroliths, success rates were slightly lower (76%), with over 50%

ESVNU Pre-Congress Day - PROCEEDINGS Page 13
requiring more than 1 ESWL treatment to achieve adequate fragmentation of ureteroliths.1 Considering our experience, ESWL is a safe and effective method of treating nephroliths and ureteroliths in dogs. Unlike dogs, ESWL is not effective in most cats. Uroliths from cats are more resistant to fragmentation than uroliths from dogs.14
We have seen several complications from ESWL treatment. The most common complication has been the developed transient ureteroliths that partially obstructed the ureter in approximately 10% of dogs treated for nephroliths, although only about 10% of these dogs require additional treatment to facilitate removal of these fragments.1 Pre-placement of a ureteral stent before ESWL may be useful to prevent ureteral obstruction in dogs with nephroliths larger than 1-1.5 cm. Lithotripsy treatment of the right kidney in small dogs often results in mild asymptomatic increases in amylase, lipase and TLI suggestive of pancreatic injury. Approximately 2% of dogs develop clinical acute pancreatitis following ESWL treatment of the right kidney.1
Large nephroliths (> 1.5-2 cm) are not good candidates for ESWL treatment because of the risk of ureteral obstruction by nephrolith fragments. PCNL or SENL are preferred over ESWL for larger nephroliths.3,5 Cystoscopic-assisted placement of a ureteral stent with periodic stent exchange is an alternative to ESWL treatment of obstructive ureteroliths.12 Ureteroliths cause increased risk of development of ureteral strictures which may complicate placement of ureteral stents.
Nephrolith recurrence is a frequent problem in dogs. Because nephrotomy results in reduced renal function, repeated surgery for may result in progressive loss of renal function and renal failure. Therefore, ESWL may be preferable to nephrotomy for treatment of nephroliths. Repeated ESWL treatments have been successfully performed in dogs with highly recurrent nephroliths.
Medical management of ureteral obstruction
Conservative medical management by serial monitoring of ureteroliths along with administration of intravenous fluids and diuretics may initially be attempted provided there is minimal renal functional compromise and no infection, renal colic, or progressive ureteral dilation. Typically, dogs with evidence of complete obstruction, worsening azotemia, or evidence of pyelonephritis should be treated via surgical intervention, ureteral stent placement or shock wave lithotripsy (ESWL). The optimal time to allow for passage of ureteroliths by medical management prior to surgical intervention is unknown.
References 1. Adams LG, Goldman CK. Extracorporeal shock wave lithotripsy In: Polzin DJ,Bartges J, eds.
Nephrology and urology of small animals. 1 ed. Ames, Iowa: Blackwell Publishing, 2011;340-348.
2. Block G, Adams LG, Widmer WR, et al. Use of extracorporeal shock wave lithotripsy for treatment of
spontaneous nephrolithiasis and ureterolithiasis in dogs. J Am Vet Med Assoc 1996;208:531-536.
3. Berent AC, Adams LG. Interventional management of complicated nephrolithiasis. In: Weisse CW,
Berent AC, eds. Veterinary Imaging-Guided Interventions. Ames, IA. Wiley-Blackwell Publishing:
2015:289-300.
4. Berent AC. Ureteral obstructions in dogs and cats: a review of traditional and new interventional
diagnostic and therapeutic options. J Vet Emerg Critical Care 2011;21:86-103.
5. Lulich JP, Berent AC, Adams LG, et al. ACVIM Small Animal Consensus Recommendations on the
Treatment and Prevention of Uroliths in Dogs and Cats. J Vet Intern Med 2016;30:1564-1574.
6. Dalby AM, Adams LG, Salisbury SK, et al. Spontaneous retrograde movement of ureteroliths in three
dogs and five cats. J Am Vet Med Assoc 2006;229:1118-1121.
ESVNU Pre-Congress Day - PROCEEDINGS Page 14
7. Westropp JL, Ruby AL, Bailiff NL, et al. Dried solidified blood calculi in the urinary tract of cats. J Vet
Intern Med 2006;20:828-834.
8. Cannon AB, Ruby AL, Westropp JL, et al. Evaluation of trends in urolith composition in cats: 5,230
cases (1985-2004). J Am Vet Med Assoc 2007;231:570-576.
9. Kuntz JA, Berent AC, Weisse CW, et al. Double pigtail ureteral stenting and renal pelvic lavage for
renal-sparing treatment of obstructive pyonephrosis in dogs: 13 cases (2008-2012). J Am Vet Med
Assoc 2015;246:216-225.
10. Greenwood KM, Rawlings CA. Removal of canine renal calculi by pyelolithotomy. Vet Surg
1981;10:12-21.
11. Stone EA, Robertson JL, Metcalf MR. The effect of nephrotomy on renal function and morphology in
dogs. Vet Surg 2002;31:391-397.
12. Vachon C, Defarges A, Brisson B, et al. Passive ureteral dilation and ureteroscopy after ureteral stent
placement in five healthy Beagles. Am J Vet Res 2017;78:381-392.
13. Tong K, Weisse C, Berent AC. Rigid urethrocystoscopy via a percutaneous fluoroscopic-assisted
perineal approach in male dogs: 19 cases (2005-2014). J Am Vet Med Assoc 2016;249:918-925.
14. Adams LG, Williams JC, Jr., McAteer JA, et al. In vitro evaluation of canine and feline urolith fragility
by shock wave lithotripsy. Am J Vet Res 2005;66:1651-1654.

ESVNU Pre-Congress Day - PROCEEDINGS Page 15
Management of feline ureterolithiaisis: Is there room for
improvement? Zoe Halfacree, MA, VetMB, CertVDI, CertSAS, FHEA, DipECVS
Royal Veterinary College, Hawkshead Lane, North Mymms, Hatfield, Hertfortshire, AL9
7TA, UK
Optimal management of cats with ureterolithiasis presents many challenges to the clinician and is an area
in which management options are evolving with much on-going debate.
A) Surgical versus medical management
Kyles et al provided the earliest description of surgical management of this condition in 11 cats (Kyles et al
1998 JAVMA) and subsequently produced two larger studies (153 cats, Kyles et al., JAVMA 2005a, 2005b)
which compared medical and surgical management outcomes. They concluded that although there was still
significant morbidity and mortality, surgical outcomes were superior to those of medical management.
Survival rates for patients managed surgically were greater for surgically than medically managed patients
(91% versus 66% at 12 months post-diagnosis). They concluded that renal function may improve or
stabilise after removal of the ureteral obstruction, but that microsurgical techniques and intensive post-
operative care is necessary to minimise morbidity in these cats. These publications were fundamental to
the subsequent management of these patients as it documented that outcome is better if there is an
intervention to relieve the obstruction.
Later studies from the University of Pennsylvania (Roberts et al Vet Surg 2011; Wormser et al, JAVMA 2016)
provided similar results (this centre also has a renal transplantation program indicating advanced
microsurgical experience).
B) Interventional techniques
Drs Berent & Weisse, formerly of the University of Pennsylvania, Philadelphia, now Animal Medical Centre,
New York, recognised that the outcome was much better when intervention was performed to relieve the
obstruction, but considered that the complications (stricture, leakage and recurrence) were still
unacceptably high. They used a translation of techniques from human interventional radiology and
pioneered its use in the veterinary field. There has been an ongoing evolution of these techniques over the
past 5 years. The techniques described by this group and others have included:
Use of percutaneous nephrostomy tubes.
Use of intraluminal double pigtail ureteral stents
Use of a subcutaneous ureteral bypass system
C) Percutaneous nephrostomy tubes
This technique allows stabilisation of the patient by decompression of the renal pelvis prior to a definitive
procedure for management of ureteric obstruction. The paper states that tubes could effectively be placed
and achieve renal pelvic decompression therefore improving patient stability. An important point to note
ESVNU Pre-Congress Day - PROCEEDINGS Page 16
however is that in 15/18 cats that had this technique performed a ventral midline laparotomy was
necessary due to the mobile nature of the kidneys. This technique is therefore not as useful as a rapid
stabilisation step and techniques have subsequently evolved replacing this option.
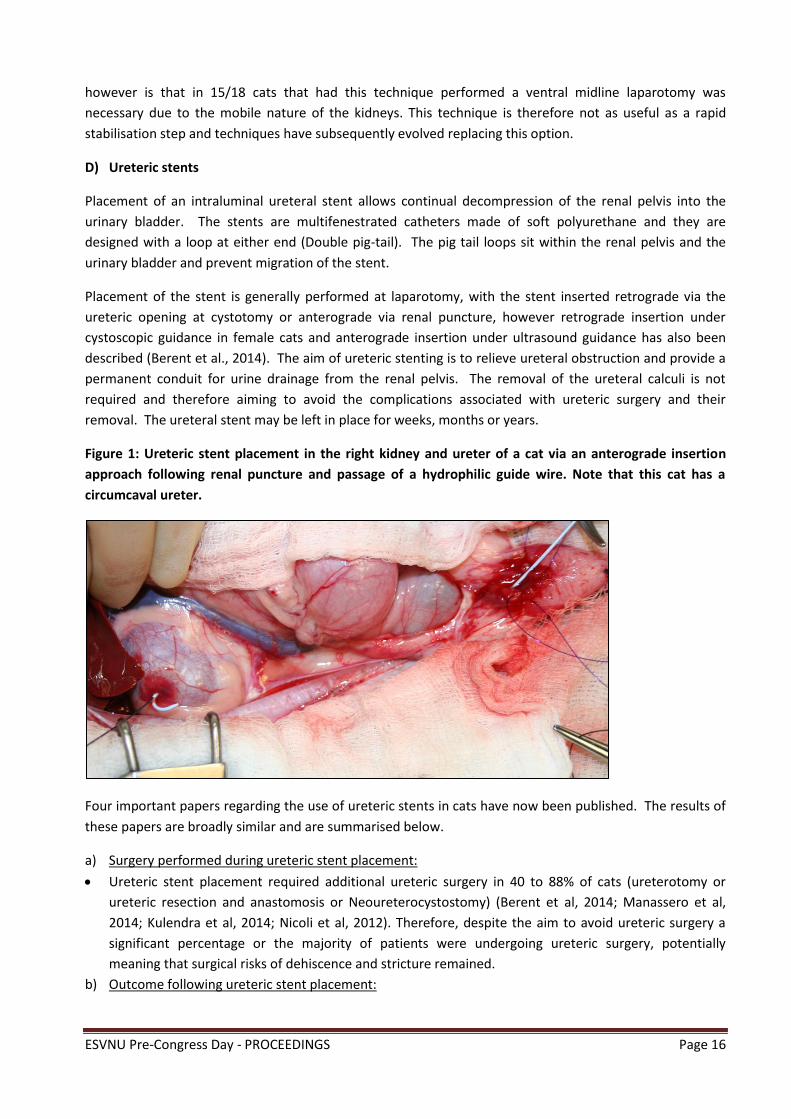
D) Ureteric stents
Placement of an intraluminal ureteral stent allows continual decompression of the renal pelvis into the
urinary bladder. The stents are multifenestrated catheters made of soft polyurethane and they are
designed with a loop at either end (Double pig-tail). The pig tail loops sit within the renal pelvis and the
urinary bladder and prevent migration of the stent.
Placement of the stent is generally performed at laparotomy, with the stent inserted retrograde via the
ureteric opening at cystotomy or anterograde via renal puncture, however retrograde insertion under
cystoscopic guidance in female cats and anterograde insertion under ultrasound guidance has also been
described (Berent et al., 2014). The aim of ureteric stenting is to relieve ureteral obstruction and provide a
permanent conduit for urine drainage from the renal pelvis. The removal of the ureteral calculi is not
required and therefore aiming to avoid the complications associated with ureteric surgery and their
removal. The ureteral stent may be left in place for weeks, months or years.
Figure 1: Ureteric stent placement in the right kidney and ureter of a cat via an anterograde insertion
approach following renal puncture and passage of a hydrophilic guide wire. Note that this cat has a
circumcaval ureter.
Four important papers regarding the use of ureteric stents in cats have now been published. The results of
these papers are broadly similar and are summarised below.
a) Surgery performed during ureteric stent placement:
Ureteric stent placement required additional ureteric surgery in 40 to 88% of cats (ureterotomy or
ureteric resection and anastomosis or Neoureterocystostomy) (Berent et al, 2014; Manassero et al,
2014; Kulendra et al, 2014; Nicoli et al, 2012). Therefore, despite the aim to avoid ureteric surgery a
significant percentage or the majority of patients were undergoing ureteric surgery, potentially
meaning that surgical risks of dehiscence and stricture remained.
b) Outcome following ureteric stent placement:

ESVNU Pre-Congress Day - PROCEEDINGS Page 17
Post-operative uroabdomen was 0 to 15% (Nicoli et al, 2012; Manassero et al; Kulendra et al, 2014;
Berent et al, 2014).
Survival to discharge was 85 to 100 % (Kulendra et al, 2014; Berent et al, 2014; Manassero et al, 2014;
Nicoli et al, 2012).
c) Long term follow up:
Median survival time: 415 days to 498 days (Kulendra et al, 2014; Manassero et al, 2014; Berent et al,
2014)
Intermittent dysuria was seen in around 33 -37% of cats (Kulendra et al, 2014; Berent et al, 2014).
Subsequent stent exchange was necessary in 15-30% of cats (Kulendra et al, 2014; Berent et al, 2014;
Manassero et al, 2014) due to stent migration, stent fracture or stent encrustation.
d) General conclusions:
Ureteric stenting can be an effective means of achieving renal pelvic decompression in the acute phase
of obstruction, however ureteric surgery is often required for insertion.
Ureteric stenting is also able to provide long term prophylaxis for management of recurrent
ureterolithiasis, however ongoing monitoring is required as stent migration, obstruction or fracture
may affect function requiring revision.
A significant percentage of cats (around 30% in two studies) had evidence of lower urinary tract signs
associated with sterile cystitis presumed to be related to the presence of the stents.
E) Subcutaneous ureteric bypass system (SUB™ NorfolK Medical)
The subcutaneous ureteric bypass system is another technique that was develop through the pioneering
work by Drs Berent and Weisse, in collaboration with Norfolk Medical. The system is based upon a
nephrovesicular subcutaneous ureteral bypass that has been described for use in human patients. The
extra-anatomic location means that the device can be placed quickly and simply, with appropriate
experience, and seems to have lower short and long term complications when compared to other
techniques. In addition the larger bore tubing and the capacity to flush the system via the subcutaneous
port, potentially reduce the risk of subsequent obstruction. Publications related to use of SUB™ devices
have recently become available in the literature and some early information about long term follow up is
being obtained.
Experience at The Royal Veterinary College
One hundred cats have had SUB™ devices placed (April 2012 to July 2017). 96 cats had the device placed
for management of benign ureteral obstruction (80 ureterolithiasis, 13 exact cause of obstruction not
identified (stricture/ureteritis?), 3 blood clots). Age range was 2-12 years. 98 % of cats were azotaemic at
presentation. Median creatinine at presentation was 713 µmol/L (range 127 to 2070 µmol/L), 54 % of cats
were hyperkalaemic on presentation (median serum potassium 4.6 mmol.L (2.3 -8.5 mmol/L), 38% of cats
were anaemic (24%, range: 16% to 47%). Unilateral SUBs were placed in 60 cats (left 33, right 27), bilateral
in 39 cats). Survival to discharge was 94 % (90/96); reasons for death in the immediate post-operative
period included: persistent anuria (2), recurrent obstruction of the nephrostomy tube with blood clots (2),
severe chronic renal failure (1), marked electrolyte derangements resulting in cardiopulmonary arrest (1).
Median survival time was 529 days (range 1 to 1382d). Percentage survival at 1 month, 6 months, 1 year
and 2 years respectively was 77%, 72%, 60% and 44% respectively.

ESVNU Pre-Congress Day - PROCEEDINGS Page 18
Thirteen percent (12/96) of cats had urinary tract infection diagnosed perioperatively (E Coli, Enterococcus
and Staphylococcus). 75% (9/12) of cats had resolution of their urinary tract infection following extended
antibiotics, although 2 of these required removal of the SUB device. One cat died within 24 hours of
surgery (with some clinical signs consistent with sepsis) and one cat died at 266 days, following extended
treatment of urinary tract infection, which was refractory to antibiotic treatment.
Figure 2: A labelled radiograph of the lateral abdomen in a cat 3 months following placement of a SUB™
device in the left kidney for management of ureteral obstruction with a proximal ureterolith. Note that
ureteral patency has been restored and the device is also confirmed to be patent.
A further thirteen percent (12/96) developed urinary tract infection post-operatively (E Coli (5),
Pseudomonas (5) and mixed (2) with Enterococcus and E Coli). E Coli urinary tract infection was resolved in
all 5 cats, but 2 cats required removal of the SUB device. One of the cats with the mixed Enterococcus and E
Coli infection had developed an enterovesicular fistula associated with the cystostomy tube and the urinary
tract infection resolved following removal of the SUB device; the other cat is currently receiving antibiotic
treatment. Three cats with Pseudomonas urinary tract infection died related to the infection, 1 due to
sepsis and 2 due to refractory urinary tract infection and additional comorbidities leading to euthanasia.
One cat had resolution of the Pseudomonas urinary tract infection following removal of the SUB device and
one cat is currently undergoing treatment. In the 5 cases where the SUB device(s) were removed
fluoroscopic imaging had demonstrated restored ureteric patency in 4 cases; in 1 case in which restored
ureteric patency was not documented the SUB device was removed and replaced after a 48 hour course of
appropriate antibiotic therapy and until an inactive urine sediment was documented.
Tube failure and uroabdomen was seen as a complication following discharge in 4 cats at 7 days, 41 days,
450 days and 1070 days. Exploratory surgery was performed in all cases and all cats made a good recovery
from revision surgery. The sites of leakage were identified as: small defect in nephrostomy tube at passage
through body wall, separation of the cystostomy catheter from the Dacron cuff at the apex of the bladder,
ESVNU Pre-Congress Day - PROCEEDINGS Page 19
complete fracture of the cystostomy tube and leakage from a nephrostomy tube at a site previously noted
to be kinked but not obstructed.
Client questionnaires were completed in 31 cats and a median score of 9/10 was given when asked about
their perception of their cat’s quality of life. Lower urinary tract signs, in the absence of the diagnosis of a
urinary tract infection, were seen rarely and were only minor when reported. This contrasts with more
frequent signs of dysuria associated with sterile cystitis in cats treated with ureteric stents for ureteral
obstruction. This is presumed to be due to the location of the cystostomy catheter away from the trigone
of the bladder and the proximal urethra.
References
1. Kyles AE, Stone EA, Gookin J et al (1998) Diagnosis and surgical management of obstructive ureteral
calculi in cats: 11 cases (1993-1996) JAVMA 213:1150-6.
2. Hardie EM & Kyles AE (2004) Management of ureteral obstruction. VCNA 34: 989-1010.
3. Kyles AE, Hardie EM, Wooden BG (2005) Management and outcome of cats with ureteral calculi: 153
cases (1984-2002) JAVMA 226: 937-44.
4. Kyles AE et al (2005) Clinical, clinicopathological, radiographic, and ultrasonographic abnormalities in
cats with ureteral calculi: 163 cases (1984-2002) JAVMA 226: 932-6.
5. Roberts SF, Aronson LR & Brown DC (2011) Post-operative mortality in cats after ureterolithotomy. Vet
Surg 40: 438-43.
6. Berent AC (2011) Ureteral obstructions in dogs and cats: a review of traditional and new interventional
diagnostic and therapeutic options. J Vet Emerg Crit Care 21: 86-103.
7. Berent AC, Weisse CW, Todd KL et al (2012) Use of a locking-loop pigtail nephrostomy catheters in dogs
and cats: 20 cases (2004-2009) JAVMA 241: 348-57.
8. Berent AC, Weisse CW, Todd K et al (2014) Technical and clinical outcomes of ureteral stenting in cats
with benign ureteral obstruction: 69 cases (2006-2010). JAVMA 244:559-76.
9. Kulendra NJ et al (2014) Feline double pigtail ureteric stents for management of ureteric obstruction:
short- and long-term follow-up of 26 cats. JFMS 16: 985-91.
10. Manassero M et al (2014) Indwelling double pigtail ureteral stent combined or not with surgery for
feline ureterolithiasis: complications and outcome in 15 cases. JFMS 16: 623-30
11. Nicoli S, Morello E, Martano M (2012) Double J ureteral stenting in nine cats with ureteral obstruction.
Vet J 194: 60-5.
12. Horowitz C, Berent A, Weisse C et al (2013) Predictors of outcome for cats with ureteral obstructions
after interventional management using ureteral stents of a subcutaneous ureteral bypass device. JFMS
15: 1052-62.
13. Berent A, Weisse C, Bagley D et al (2016) Subcutaneous ureteral bypass device placement for benign
ureteral obstruction(s) in cats: one hundred and thirty-seven cats (one hundred and seventy-four
obstructed ureters) (2009-2015) Vet Surg 45: E23-E51VC
14. Wormser C et al (2016) Outcomes of ureteral surgery and ureteral stenting in cats: 117 cases (2006-
2014). JAVMA 248: 518-25
15. http://www.norfolkvetproducts.com/subs

ESVNU Pre-Congress Day - PROCEEDINGS Page 20
Hereditary urolithiasis in dogs and cats – Focus on cystine Urs Giger, Dr. med. vet., MS, FVH, DipACVIM-SAM & ECVIM-CA, DipECVCP
University of Pennsylvania, Philadelphia, PA
Disorders of the renal proximal tubules can cause selective or generalized aminoaciduria and may be
associated with urinary losses of other solutes such as glucose, lactate, electrolytes and bicarbonate. Two
renal tubular defects involving amino acids have long been recognized in dogs, namely cystinuria, a
selective amino aciduria leading to cystine calculi and urinary obstruction, and Fanconi syndrome, a
generalized tubular defect, and both can progress to renal failure if untreated. Both hereditary disorders
have been investigated at the molecular level and are more complex than originally anticipated.
Furthermore, the ingestion of Chinese jerky treats has recently been found to be associated with Fanconi
syndrome in many dogs and rarely cats. The current understanding of pathophysiology, clinicopathological
findings, diagnosis, and (briefly) therapeutic options will be presented.
Cystinuria
In contrast to the rather broad transmembrane transport defect causing hereditary and acquired
forms of Fanconi syndrome, cystinuria is a limited hereditary renal transport disorder involving cystine and
the dibasic amino acids ornithine, lysine, and arginine, collectively known as COLA. Instead of the normal
>99% reabsorption in the proximal renal tubules, these four amino acids are lost in the urine, but only
cystine causes a problem. The low solubility of cystine in acidic urine predisposes the formation of cystine
crystals and uroliths in the urinary tract, resulting in the typical clinical signs of cystinuria. While the
transport of these amino acids also occurs in the gut and thus cystinuria also affects intestinal COLA
absorption, the impaired intestinal absorption of the COLA amino acids is not associated with any clinical
deficiencies in animals, with the exception of hyperammonemia due to arginine deficiency in cats.
Cystinuria is one of the first reported “inborn errors of metabolism” described in humans more
than 200 years ago, and has been described in several other species including dogs, cats, ferrets, maned
wolves, and servals. Two genes, SLC3A1 and SLC7A9 encode the polypeptide subunits of the bo,+ basic
amino acid transporter system and its dysfunction results in cystinuria. SLC3A1 encodes a protein referred
to as rBAT and SLC7A9 encodes a protein called bo,+AT. bo,+AT heterodimerizes with rBAT exclusively to
form the COLA amino acid transporter. Cystinuria in humans has been classified phenotypically into two
types differing by mode of inheritance (autosomal recessive or incomplete autosomal dominant) are
caused by mutations in the SLC3A1 and SLC7A9 genes which encode the bo,+AT basic amino acid transporter
system; mutations have not been identified for approximately 10% of cystinuric human patients.
Since 1823, when cystinuria was first described in dogs, dogs of many breeds have been diagnosed,
but only recently have studies revealed the genetic heterogeneity. We have proposed a new classification
system for canine cystinuria based upon that in humans. A severe cystinuria showing autosomal recessive
inheritance was first characterized in Newfoundlands and Landseers, and has more recently been identified

ESVNU Pre-Congress Day - PROCEEDINGS Page 21
in additional breeds. Although both males and females are affected, males more frequently show clinical
signs of urinary obstruction. Different mutations in SLC3A1 resulting in an early stop codon and loss of
bo,+AT function have been identified in Newfoundlands and Labrador Retrievers (Type I-A). A 6 bp deletion
removing 2 threonine residues in SLC3A1 was found in autosomal-dominant cystinuria with a more severe
phenotype in homozygous than in heterozygous Australian Cattle dogs and a mixed breed dog (Type II-A).
A missense mutation in SLC7A9 was identified in autosomal dominant cystinuria in miniature Pinschers
from Europe, with only heterozygous affected dogs observed to date (Type II-B).
Cystinuria has also been described in an additional 70 canine breeds. In several of these breeds
from which more data is available, such as the Mastiff, French Bulldog, Scottish deerhounds, Basset hound,
Kromfohrlaender, and Irish terrier, the disease predominantly occurs later in life, is less severe, more
variable, and only involves mature intact males. We refer to this as canine androgen-dependent or type III
cystinuria, but still do not know the specific genetic defects. Interestingly, Irish Terriers in Europe and
Australia seem to be more commonly affected than in the US, where cystinuria in Irish Terriers is rarely
diagnosed (possibly because they are frequently early castrated and may represent an different gene pool).
Type III cystinuric dogs (with or without cystine calculi) also seem to have variable degrees of cystine and
COLA in their urine. These variations could be due to cystine precipitation, diet, age-related variability, the
castration effects, and genetic heterogeneity. Molecular studies in Irish Terriers, Mastiffs and several other
breeds have failed to detect disease-causing mutations in the exons of either SLC3A1 or SLC7A9 genes,
however an SLC3A1 missense mutation appears to be associated with cystinuria in Mastiffs and related
breeds but not Irish Terriers or Scottish Deerhounds. Only mature males are cystinuric and surgical (and
even medical) castration resolves excessive cystine and COLA excretion, but the mode of inheritance is still
unclear. On average, dogs with type I and II cystinuria have a several fold higher urinary COLA excretion
than type III cystinuric male dogs.
Cystine uroliths can form in the kidney (rarely), ureters, bladder or urethra and can lead to urinary
blockage, renal failure and associated life-threatening clinical manifestations. A clinical diagnosis of cystine
uroliths can be suspected based upon the canine breed and yellow-brown color of the uroliths, and can be
confirmed by crystallographic or chemical analysis of calculi in specialized stone laboratories such as those
at the Universities of Minnesota and California, as well as commercial laboratories worldwide. While in the
US approximately 1% of analyzed urinary calculi are cystine stones, in Europe the proportion appears to be
as high as 3%. Cystine calculi are usually radiolucent and thus may be missed by radiography, but are
readily visualized by ultrasound. Furthermore, urinalysis often reveals the presence of characteristic
hexagonal cystine crystals.
A simple urinary screening test, to determine if a dog is cystinuric, is available through the
Metabolic Genetic Laboratory at the University of Pennsylvania
(http://research.vet.upenn.edu/penngen/PennGenHome/tabid/91/Default.aspx; PennGen). This test can detect
any type I and II cystinuric animal, but not necessarily all dogs with type III cystinuria. Amino acid analyzers
can be used to determine the amount of cystine and the other amino acids in urine, however this
quantitative amino acid analysis is currently restricted to a few laboratories and is relatively expensive.
Inclusion of the dibasic amino acids (ornithine, lysine, and arginine) in the quantitation of cystine is
preferred due to the possibility that urinary cystine may have precipitated, causing lower concentrations
than were originally present in the urine, and therefore leading to false negative interpretations. Based
upon our studies, dogs with either cystine levels of >200 µmol/g creatinine or COLA values of >700 µmol/g
creatinine are considered cystinuric. Moreover, for several breeds with type I and II cystinuria, a breed-

ESVNU Pre-Congress Day - PROCEEDINGS Page 22
specific mutation test is available that not only detects cystinuric dogs, but also the asymptomatic carriers
(for recessive traits). While in the 1990s as many as 5% and 30% of Newfoundlands were cystinuric
(homozygous affected) and carriers, respectively, very few Newfoundlands are cystinuric or carriers in
2015, thanks to the implementation of this DNA screening test, which is available through our and many
commercial laboratories. In contrast, the mutant alleles in Labrador Retrievers, Australian Cattle Dogs,
Miniature Pinscher and Scottish Terrier dogs appear to be limited to a small subset of the breed population.
Finally, in Mastiffs and closely related breeds, a DNA marker test to identify dogs that are at risk for early
stone formation is being offered on a limited basis at the University of Pennsylvania
(http://research.vet.upenn.edu/WSAVA-LabSearch).
Cystinuria is also seen in domestic non-purpose bred and purebred cats and several mutations in
SLC3A1 and SLC7A9 have been reported recently by PennGen lab (Mizukami et al 2015 and 2016).
Interestingly one missense SLC7A9 mutation has been observed in a Maine coon, Sphinx and Siamese-
crossbred and non-purpose bred cat in different geographic locations in North America and even in
Germany.
Urinary tract obstructions due to cystine calculi can present as life-threatening emergency
situations. If the calculi are in the urethra, catheterization and endoscopy may allow their passage, permit
them to be moved back into the bladder (retrograde hydropulsion). Laser therapy as well as lithotripsy
may break them up, and endoscopy and surgery can be used to remove them entirely. In contrast,
attempts to dissolve cystine stones medically by drugs and diet have generally failed. Dogs with type I and
II cystinuria are persistently strongly cystinuric from puppyhood and remain at high risk of developing
cystine calculi throughout life, independent of gender. Alpha-mercaptopropionylglycine (Thiopronin,
Thiola), a chelating agent that has fewer side-effects and is more potent than D-penicillamin, may lower the
risk of calculi formation in cystinuria but is expensive and not always commercially available. Forced
diuresis, urine alkalinization (pH>7.5), and reduced protein diets (no chicken) may lower the recurrence
risk, while high protein diets and protein supplements tend to increase the risk for calculi formation. Male
dogs with type III cystinuria have more variable and usually lower cystine excretion. Thus, they may or may
not develop calculi and their recurrence rate is lower. Moreover, castration of Mastiffs and related breeds,
Scottish Deerhounds, and Irish Terriers and some other breeds with type III cystinuria diminishes the
excretion of cystine and dibasic amino acids to the normal female range, indicating a testosterone-
mediated modulating effect on the renal tubular amino acid reabsorption. Surgical and medical castration
are curative in these breeds, but we recommend castration to reduce the formation and risk of blockage by
cystine calculi in all breeds, which will also contribute to reducing the incidence of this genetic
predisposition.
Supported in part by grants from the NIH (OD 010939) and the AKC Canine Health Foundation. Biocontrol
Laboklin and Minnesota’s Urolith Laboratory assisted in sample collection. Dr. Tosso Leeb at Vetsuisse Bern
and Dr. Adrian Sewell at Biocontrol are acknowledged for their collaborative studies.
Conflict of Interest: The author’s laboratory (PennGen) offers DNA testing and metabolic screening for cystinuria and Fanconi Syndrome.
ESVNU Pre-Congress Day - PROCEEDINGS Page 23
Selected references
Brons AK, Henthorn PS, Raj K, Fitzgerald CA, Liu J, Sewell AC, Giger U (2013): SLC3A1 and SLC7A9 mutations
in autosomal recessive or dominant canine cystinuria: A new classification system. J Vet Intern Med 27:
1400–1408
Casal ML, Giger U, Bovee KC, Patterson DF (1995): Inheritance of cystinuria and renal defect in
Newfoundlands. Journal of the Am Vet Med Assoc 207: 1585-1589.
Harvenik L, Hoppe A, Söderkvist P (2006): SLC7A9 cDNA cloning and mutational analysis of SLC3A1 and
SLC7A9 in canine cystinuria. Mamm Genome 17: 769-776.
Henthorn PS, Liu J, Gidalevich T, Fang J, Casal ML, Patterson DF, and Giger U (2000): Canine cystinuria:
Polymorphism in the canine SLC3A1 gene and identification of a nonsense mutation in cystinuric
Newfoundland dogs. Human Genetics 200; 107: 295-303.
Henthorn PS, Giger, U (2006): Cystinuria, in The Dog and Its Genome, eds. Ostrander, Giger, and Lindblad-
Toh (Cold Spring Harbor Laboratory Press), 349-364.
Henthorn PS, Raducha M, Brons AK, Raj K, Fitzgerald C, Liu J, Sewell A, Giger U (2013): Unraveling the
phenotypic and genetic complexity of canine cystinuria. Proceedings of the Advances in Canine and
Feline Genomics and Inherited Diseases Conference, Boston, MA.
Hilton S, Mizukami K, Giger U (2017): Cystinuria caused by an SLC7A9 missense mutation in Siamese-
crossbred littermates. Tieraerztliche Praxis, Epub.
Mizukami K, Raj K, Giger U (2015): Feline cystinuria caused by a missense mutation in the SLC3A1 gene. J
Vet Intern Med 29: 120-125.
Mizukami K, Raj K, Osborne C, Giger U (2016): Cystinuria associated with different SLC7A9 gene variants in
the cat. Plos One 11(7): e0159247.
Moresco A, Van Hoeven M, Giger U (2004). Cystine urolithiasis and cystinuria in captive Servals (Leptailurus
serval) 163.
Nwaokorie EE, Osborne CA, Lulich JP, Albasan H (2013): Epidemiological evaluation of cystine urolithiasis in
domestic ferrets (Mustela putorius furo): 70 cases (1992-2009). J Am Vet Med. Assoc 242: 1099-1103.
Osborne CA, Sanderson SL, Lulich JP, Bartges JW, Ulrich LK, Koehler LA, Bird KA, Swanson LL (1999): Canine
cystine urolithiasis: cause, detection, treatment, and prevention. Vet Clin N Am, Small Animal Practice
29: 193-211.
Osborne CA, Lulich JP, Sanderson S, Ggier U (1999): Feline cystine urolithiasis – 18 cases. Fel Pract 27: 31–
32.
Palacin M, Nunes V, Font-Llitjos M, Jimenez-Vidal M, Fort J, Gasol E, Pineda M, Feliubadalo L, Chillaron J,
Zorzano A (2005): The genetics of heteromeric amino acid transporters. Physiol 20: 112-124.
Slutsky J, Raj K, Yunke S, Bell J, Fretwell N, Hedhammar A, Wade C, Giger U (2013) A web resource on DNA
tests for canine and feline hereditary diseases. Vet J 197: 182-187.
Tordiffe ASW, Watt GF, Reyers F (2012): Cystine urolithiasis in a caracal (Caracal caracal). J Zoo Wildlife Med
43: 649-651.
ESVNU Pre-Congress Day - PROCEEDINGS Page 24
What’s new in the nutritional management of canine and
feline urolithiasis
Iveta Becvarova, DVM, MS, DipACVN
Hill’s Pet Nutrition Europe
The recently published ACVIM consensus statement on urolith management is a great resource that
supports nutritional modification as the standard of care for common calculi.1 This information can be used
to encourage the veterinary healthcare teams to recommend nutritional strategies to manage and prevent
most common uroliths found in dogs and cats. Moreover, new research findings emerge in the area of
nutritional modification for pets with urolithiasis.
Link between obesity and urolithiasis
Excess weight is considered a risk factor for several conditions that cause lower urinary tract signs in
humans, dogs and cats. In humans, several studies indicate a positive association between obesity and risk
of nephrolithiasis, with CaOx nephroliths being most common.2 While studies linking obesity and
urolithiasis in cats have not been reported, there are reports finding associations of these two conditions in
dogs. In one study, overweight dogs had more than twice the risk (odds ratio = 2.2) for developing calcium
oxalate (CaOx) uroliths compared with dogs of ideal body weight (P<0.05).3 A more recent study indicated
that dogs with CaOx uroliths had higher Body Condition Score (BCS) than control dogs and this association
was independent of urine pH.4
The mechanism by which obesity increases risk for CaOx uroliths is not fully understood. In humans,
overweight and obesity was strongly associated with increased risk of stone formation due to increased
urinary excretion of promoters but not inhibitors of calcium oxalate stone formation.2 In dogs, it is possible
that obesity-related food patterns and nonadjusted drinking habits which relate to increased risk of
urolithiasis play a role.
The link between urolithiasis and obesity in cats is not straight forward. The consistently reported increased
risk of uroliths in neutered cats provides indirect evidence for this association.5,6 Neutering is a well-
recognized risk factor for obesity in cats.7,8 Indoor housed cats are also at increased risk for lower urinary
tract signs. Again, obesity is more common in cats housed indoors due to a more sedentary lifestyle.9
The relationship of excess adiposity and LUTS was demonstrated in a National Companion Animal Study
population of adult cats where LUTS increased in rate with increasing Body Condition Score (BCS) (Figure
1).10

ESVNU Pre-Congress Day - PROCEEDINGS Page 25
0
1
2
3
4
5
6
7
8
Normal weight &underweight
Overweight Obese
4.8
7.4 7.1
Figure 1. Urinary disease prevalence increases with increasing Body Condition Score (BCS). A total of
9,865 adult cats with a reported condition were included in this analysis of a National Companion Animal
Study population of 11,102 adult cats.
The link between obesity and urolithiasis is significant enough that human health care providers are
encouraged to recommend both dietary modification and weight loss to obese patients to reduce the risk
of kidney stone formation. Therefore, it is warranted to consider nutritional modification for any dog or cat
that demonstrates the combination of being obese and having uroliths.
Link between obesity and urinary tract infection
Obesity may increase risk of urinary tract infection (UTI) through several possible mechanisms, including
reluctance to move and void the urine or through ascension of bacteria from skin folds surrounding the tail
base and perineal areas. The link between morbid obesity and asymptomatic bacteriuria has been
evaluated in a recent retrospective study in dogs.11 Morbid obesity was defined as ≥ 45% body fat
determined by the dual energy absorptiometry (DEXA) scan and urinary tract infection was confirmed by
bacterial urine culture. Among morbidly obese dogs, 25% (6 of 24 dogs) had asymptomatic UTI whereas no
dogs that were lean, overweight, or obese (% body fat < 45) had bacterial UTI. Prevalence of UTI in the dogs
in this study had a strong statistical relationship to % body fat (P=0.007). These findings support the need
for screening obese dogs for bacteriuria but they are not a proof of cause and effect between obesity and
UTI. Further studies are needed to evaluate whether the asymptomatic bacteriuria represents a risk for
infectious struvite formation in the population of obese dogs and whether weight loss would reduce the
risk of infection.
The issue of calcium oxalate urolith recurrence
The etiology of CaOx calculi in dogs and cats has not been elucidated and the reported recurrence rate of is
of clinical importance. A significant number of cats with CaOx uroliths will have recurrence within 2 years of
removal.12 The rate of recurrence of CaOx cystic calculi in dogs has been reported to be as high as 90%
1.0 < BCS < 3.5
n = 6,434
3.5 < BCS ≤ 4.5
n = 2,792
4.5 <BCS ≤ 5.0
n = 639
Pre
vale
nce
uri
nar
y d
isea
se (
%)

ESVNU Pre-Congress Day - PROCEEDINGS Page 26
within 3 years 13 and 100% within 4 years.14 There is a number of commercially available dietetic foods with
variable nutrient profiles that use different strategies to reduce calcium (Ca) and oxalic acid concentrations
in the urine, promote high urinary concentration of CaOx crystal growth inhibitors, and maintain dilute
urine.
One prospective, 2- year-long, randomized, double-masked and controlled study evaluated 2 foods
for management of CaOx urolithiasis in cats with a history of CaOx calculi.30 The test food (n=17; target
urine pH of 6.2-6.4) had higher concentration of antioxidants, n-3 PUFAs, and lower concentration of Ca
and magnesium when compared to the control food (n=16; target urine pH 6.6-6.8). Recurrence of calculi
was observed in 29.4% test food and in 37.5% control food fed cats. RSS CaOx and urine[Ca] were
significantly higher in cats with stone recurrence and in cats fed the control food. Authors concluded that
recurrence of CaOx uroliths may be lower in cats fed the test food.
A retrospective study evaluated the long-term risk of recurrence of uroliths in 135 dogs with a history of
CaOx calculi fed one of two commercial dietetic foods that are designed for CaOx prevention using different
nutritional strategies.15 In this study, prevalence of recurrence was not different between these two CaOx
preventative foods.
Since the number of clinical trials with the end point of urolith recurrence is still limited, more studies are
needed to evaluate the long-term effect of specially formulated foods on the recurrence of CaOx calculi.
Calcium and calcium oxalate urolithiasis
Intestinal absorption of dietary Ca is dependent on number of factors, including the concentration of
dietary oxalate, because dietary Ca forms unabsorbable complexes with oxalate.16 Calcium is excreted in
the urine and hypercalciuria is thought to be a risk factor for CaOx urolithiasis. Nutritional factors
responsible for hypercalciuria include hypercalcemia, feeding an acidifying food or food low in phosphorus
(P).17 One feline study demonstrated that dietary potassium (K) supplementation may decrease urinary Ca
excretion. The mechanism of this effect is unclear but is possibly related to the natriuretic effect of K or
alkalinizing effect of K salts.18 A recent canine study revealed that dogs with a history of CaOx urolithiasis
had decreased conversion of 25(OH) vitamin D3 to the inactive 24,25(OH)2 vitamin D3, which could possibly
contribute to the risk of stone formation.19 There is a need for long-term prospective controlled nutritional
trials with the recurrence of CaOx stone as the hard end point to evaluate the effect of modification of
dietary Ca in the prevention of CaOx calculi.
Oxalic acid and calcium oxalate urolithiasis
Many plants, animals and fungi produce oxalic acid, and share the same common pathways of oxalic acid
synthesis. In mammals, oxalate is a terminal metabolite that is primarily derived from dietary sources, with
some portion produced through endogenous metabolism of glycine, glyoxylate, and vitamin C, and
hydroxyproline. Although oxalic acid is wide-spread in the nature, it is considered as an undesirable
component of food because it raises the risk of urolithiasis and also results in sequestration of calcium into
insoluble calcium oxalate in the gut lumen, rendering calcium from being utilized by the animal. Oxalate is
absorbed in both the small and large intestine by a non-energy dependent diffuse mechanism, and it
appears that the colon may be the predominant absorption site.20 Besides the dietary oxalate and calcium
content, the absorption of oxalate from the intestine is also influenced by conditions leading to fat
malabsorption and by the presence of gut microbes that degrade oxalate. Undigested fatty acids within the

ESVNU Pre-Congress Day - PROCEEDINGS Page 27
colon can increase colonic absorption of oxalate and contribute to hyperoxaluria, suggesting that
steatorrhea can contribute to hyperoxaluria and that feeding low fat foods can by of hypothetical benefit in
certain population of patients.20 Oxalate elimination is through the feces and kidney but also through the
degradation by oxalate-metabolizing gut microbes.
A number of studies in humans, rats and dogs have focused on selected intestinal oxalate-degrading
bacteria, such as Oxalobacter formigenes, Bifidobacterium spp and Lactobacillus spp 21-24, and their
effectiveness in minimizing freely available oxalate for colonic absorption. Oxalobacter formigenes has
been shown to increase the risk of CaOx urolithiasis in dogs that have low enteric colonization with the
bacterial species.25 Most recently published studies revealed promising results of oxalate-degrading
capacity of selected bacteria in vitro, suggesting that they may be a future target for lowering intestinal
oxalate concentration in the gut of dogs and cats. More research is needed to assess dietary interventions
that can modify gut microbes towards higher abundance of oxalate-degrading bacteria and whether this
can lead to decreased urine oxalate concentration and reduced risk of urolith recurrence.
Source of dietary protein and calcium oxalate
Total body oxalate originates from dietary oxalate and from the endogenous metabolism of vitamin C,
glycine and hydroxyproline.26 Hydroxyproline can be metabolized to glyoxyalte, and then to oxalate in the
hepatocyte. Absorbed or endogenously synthesized oxalate is excreted in the urine and not stored in the
body. Studies in humans, mice and cats demonstrated that metabolism of hydroxyproline results in
endogenous synthesis of glyoxylate and oxalate, thereby contributing to urinary oxalate excretion.27 One
randomized controlled study showed that cats fed foods containing collagen (rich in hydroxyproline) had 2-
to 3-fold greater urinary oxalate excretion when compared to cats fed food containing soy isolate or horse
meat as the protein source.28 Since the foods fed in this study differed in nutrient profile, it was not
possible to distinguish whether this effect was solely due to the difference in hydroxyproline content.
However, a more recent randomized and controlled study did show that dietary hydroxyproline and not
dietary oxalate increased endogenous urinary oxalate excretion in healthy adult cats.27 In the same study,
some dietary oxalate appeared to be metabolized in the intestine by oxalate-degrading bacteria, however,
the study was not designed to isolate the gut microbial species. Furthermore, dietary oxalate did not
appear to be important factor affecting urinary oxalate excretion in cats. This observation differs from
findings in humans, where oxalate plays the primary role in CaOx urolith formation.29 It has been postulated
that relatively high Ca concentrations in feline foods, when compared to human diet, result in increased
oxalate binding within the intestines, making oxalate less available for gut absorption.
These findings indicate that the protein source might be an important factor to consider in CaOx
preventative foods and these special foods should be formulated with the respect to hydroxyproline
content. Whether such foods would result in decreased clinical recurrence of CaOx uroliths in stone
forming cats is still unknown.
Conclusion
New research is emerging to elucidate relationships between urolithiasis, obesity, precursors of
endogenous oxalate production, and oxalate-degrading gut microbes. Expanding in-depth knowledge on
the role of nutrients and food on urolith formation is the important research target, especially for the CaOx,
a type of stone not amenable to dissolution with calculolytic foods.
ESVNU Pre-Congress Day - PROCEEDINGS Page 28
References
1. Lulich JP, Berent AC, Adams LG, et al. ACVIM Small Animal Consensus Recommendations on the
Treatment and Prevention of Uroliths in Dogs and Cats. J Vet Intern Med 2016;30:1564-1574.
2. Siener R, Glatz S, Nicolay C, et al. The role of overweight and obesity in calcium oxalate stone
formation. Obes Res 2004;12:106-113.
3. Lekcharoensuk C, Lulich JP, Osborne CA, et al. Patient and environmental factors associated with
calcium oxalate urolithiasis in dogs. J Am Vet Med Assoc 2000;217:515-519.
4. Kennedy SM, Lulich JP, Ritt MG, et al. Comparison of body condition score and urinalysis variables
between dogs with and without calcium oxalate uroliths. J Am Vet Med Assoc 2016;249:1274-1280.
5. Appel SL, Houston DM, Moore AE, et al. Feline urate urolithiasis. Can Vet J 2010;51:493-496.
6. Lekcharoensuk C, Lulich JP, Osborne CA, et al. Association between patient-related factors and risk of
calcium oxalate and magnesium ammonium phosphate urolithiasis in cats. J Am Vet Med Assoc
2000;217:520-525.
7. Alexander LG, Salt C, Thomas G, et al. Effects of neutering on food intake, body weight and body
composition in growing female kittens. Br J Nutr 2011;106 Suppl 1:S19-23.
8. Backus RC, Cave NJ, Keisler DH. Gonadectomy and high dietary fat but not high dietary carbohydrate
induce gains in body weight and fat of domestic cats. Br J Nutr 2007;98:641-650.
9. Kienzle E, Bergler R. Human-animal relationship of owners of normal and overweight cats. J Nutr
2006;136:1947S-1950S.
10. Lund EM, Armstrong PJ, Kirk CA, et al. Prevalence and risk factors for obesity in adult cats from
private US veterinary practices. Intern J Appl Res Vet Med 2005;3:88-96.
11. Wynn SG, Witzel AL, Bartges JW, et al. Prevalence of asymptomatic urinary tract infections in
morbidly obese dogs. PeerJ 2016;4:e1711.
12. Lulich JP, Osborne CA, Lekcharoensuk C, et al. Effects of diet on urine composition of cats with
calcium oxalate urolithiasis. J Am Anim Hosp Assoc 2004;40:185-191.
13. Lulich JP, Perrine L, Osborne CA. Postsurgical recurrence of calcium oxalate uroliths in dogs J Vet
Intern Med 1992;6:119.
14. Lulich JP, Osborne CA, Daubs TH. Biologic behavior of calcium oxalate uroliths in Bichon Frise dogs. J
Vet Intern Med 2004;18:440–441.
15. Allen HS, Swecker WS, Becvarova I, et al. Associations of diet and breed with recurrence of calcium
oxalate cystic calculi in dogs. J Am Vet Med Assoc 2015;246:1098-1103.
16. Holmes RP, Goodman HO, Assimos DG. Contribution of dietary oxalate to urinary oxalate excretion.
Kidney Int 2001;59:270-276.
17. Pastoor FJ, Van 't Klooster AT, Mathot JN, et al. Increasing phosphorus intake reduces urinary
concentrations of magnesium and calcium in adult ovariectomized cats fed purified diets. J Nutr
1995;125:1334-1341.
18. Lekcharoensuk C, Osborne CA, Lulich JP, et al. Association between dietary factors and calcium
oxalate and magnesium ammonium phosphate urolithiasis in cats. J Am Vet Med Assoc
2001;219:1228-1237.
19. Groth E, Lulich J, Chew D, et al. Vitamin D metabolism in dogs with calcium oxalate urolithiasis J Vet
Intern Med 2017;31:1318.
20. Dobbins JW, Binder HJ. Effect of bile salts and fatty acids on the colonic absorption of oxalate.
Gastroenterology 1976;70:1096-1100.
ESVNU Pre-Congress Day - PROCEEDINGS Page 29
21. Weese JS, Weese HE, Yuricek L, et al. Oxalate degradation by intestinal lactic acid bacteria in dogs
and cats. Vet Microbiol 2004;101:161-166.
22. Weese JS, Palmer A. Presence of Oxalobacter formigenes in the stool of healthy dogs. Vet Microbiol
2009;137:412-413.
23. Murphy C, Murphy S, O'Brien F, et al. Metabolic activity of probiotics-oxalate degradation. Vet
Microbiol 2009;136:100-107.
24. Cho JG, Gebhart CJ, Furrow E, et al. Assessment of in vitro oxalate degradation by Lactobacillus
species cultured from veterinary probiotics. Am J Vet Res 2015;76:801-806.
25. Gnanandarajah JS, Abrahante JE, Lulich JP, et al. Presence of Oxalobacter formigenes in the intestinal
tract is associated with the absence of calcium oxalate urolith formation in dogs. Urol Res
2012;40:467-473.
26. Osborne CA, Polzin DJ, Lulich JP, et al. Relationship of nutritional factors to the cause, dissolution,
and prevention of canine uroliths. Vet Clin North Am Small Anim Pract 1989;19:583-619.
27. Dijcker JC, Hagen-Plantinga EA, Thomas DG, et al. The effect of dietary hydroxyproline and dietary
oxalate on urinary oxalate excretion in cats. J Anim Sci 2014;92:577-584.
28. Zentek J, Schulz A. Urinary composition of cats is affected by the source of dietary protein. J Nutr
2004;134:2162S-2165S.
29. Holmes RP, Ambrosius WT, Assimos DG. Dietary oxalate loads and renal oxalate handling. J Urol
2005;174:943-947; discussion 947.
30. Lulich J, Kruger JM, MacLeay J, et al. A two year long prospective, randomized, double-masked study
of nutrition on the recurrence of calcium oxalate urolithiasis in stone forming cats. J Vet Intern Med
2014; 28:1366.

ESVNU Pre-Congress Day - PROCEEDINGS Page 30
Acquired and inherited Fanconi Syndrome Urs Giger, Dr. med. vet., MS, FVH, DipACVIM-SAM & ECVIM-CA, DipECVCP
University of Pennsylvania, Philadelphia, PA
Disorders of the renal proximal tubules can cause selective or generalized aminoaciduria and may be associated with urinary losses of other solutes such as glucose, lactate, electrolytes and bicarbonate. Two renal tubular defects involving amino acids have long been recognized in dogs, namely cystinuria, a selective amino aciduria leading to cystine calculi and urinary obstruction, and Fanconi syndrome, a generalized tubular defect, and both can progress to renal failure if untreated. Both hereditary disorders have been investigated at the molecular level and are more complex than originally anticipated. Furthermore, the ingestion of Chinese jerky treats has recently been found to be associated with Fanconi syndrome in many dogs and rarely cats. The current understanding of pathophysiology, clinicopathological findings, diagnosis, and (briefly) therapeutic options will be presented. Fanconi Syndrome Fanconi syndrome, named after the Swiss pediatrician Guido Fanconi and also known as Fanconi’s syndrome or Fanconi disease, should not be confused with Fanconi anemia, a hereditary bone marrow disorder in humans. Fanconi syndrome represents a major proximal renal tubular defect, which hampers the adequate reabsorption of glucose, amino acids, bicarbonate, sodium, calcium, phosphate, lactate, ketones, and carnitine. This rather general loss of multiple functions of the proximal renal tubules can be associated with renal tubular acidosis and lead to progressive renal failure if left untreated. In the renal tubules there are multiple co-transporters for sodium and glucose, amino acids, calcium, and inorganic phosphorus and a sodium/hydrogen ion antiporter, which, depending upon the concentration gradient established by the sodium-potassium pump, move hydrogen ions into the urine.
The molecular defect associated with Fanconi syndrome in Basenjis has been elucidated. Basenjis are genetically predisposed to Fanconi syndrome, which is inherited as an autosomal recessive trait in the breed. As many as 10% of Basenjis are affected, and they typically develop signs in middle-age (4-7 years). A mutation in the Fan1 gene on CFA3 has been discovered. Norwegian Elkhounds also often develop glucosuria early in life, which may progress to Fanconi syndrome, but no molecular studies have been reported. Other breeds that may also be potentially genetically predisposed to develop Fanconi syndrome include Labrador Retrievers, and Cocker spaniels, West Highland White Terriers, Shetland Sheepdogs, and Schnauzers in which Fanconi syndrome has been secondary and possibly related to a copper-associated hepatopathy in these breeds.
There are several acquired causes of Fanconi syndrome such as exposure to heavy metals (e.g. lead, mercury, and cadmium), drugs (gentomycin, tetracycline, and azathioprine, chlorambucil in cats) and infections (leptospirosis). Fanconi syndrome has also been reported in cancer and hepatic copper disease in several dogs. Particularly, case reports and recent studies indicate that Labrador Retrievers with copper-associated hepatopathy develop Fanconi syndrome.
More recently Fanconi syndrome has been associated with the ingestion of chicken and duck and even veggie jerky treats of different brands that contain Chinese products. It should be noted the source of the ingredients may not be specified, if not entirely made in China as much as as jerky may be part of other treats like pet biscuits and sausages. Currently no specific ingredient or contaminant responsible for the intoxication has been identified but the FDA and state governments are actively investigating the jerky treats. Six antibiotics (trimethoprim, tilmicosin, enrofloxacin, sulfaclozine, sulfamethoxazole, and
ESVNU Pre-Congress Day - PROCEEDINGS Page 31
sulfaquinoxaline) have been found in excessive amounts in some chicken jerky treats, however, there is no evidence to associate their presence with the observed illnesses. There also seem to be large quantities of glycine and lysine in some products. Furthermore, other (antiviral, antiparkinsonian) drugs and chemicals (DEET) have been found in small quantities.
Nearly all the dogs affected are from North America and Australia but there are recent reports from United Kingdom, continental Europe and Japan. Affected dogs (and rarely cats) include toy to small breed dogs, such as Chihuahuas, Maltese, and Yorkshire, Jack Russell and West Highland White Terriers, but not brachycephalic breeds except Shih Tzus. Their predisposition may be related to the proportionally larger amount of jerky treats ingested by small breeds compared to large breed dogs, or may reflect a broader hypersensitivity of the smaller breeds.
Clinical signs of intoxication may occur within days to months of ingesting jerky treats, are unspecific, and may include lethargy, inappetence, vomiting, and diarrhea. Polydipsia and polyuria are the most common clinical signs of Fanconi syndrome, while other signs of Fanconi syndrome are highly variable and may be related to the ensuing renal failure. In the past, a diagnosis of Fanconi syndrome resulted in a guarded to poor prognosis. However, well treated and closely monitored Basenjis may reach a near normal life expectancy. Moreover, if the trigger is removed, such as withdrawal of Chinese jerky treats, the renal damage may be more minimal and reversible within weeks to months. Routine serum chemistry and urinalysis as well as venous blood gas analysis are indicated to define the extent of the tubular defect and acidosis and monitor progression or resolution while managed. Liver enzymes may be elevated suggesting a hepatopathy as may be seen with pet jerky treat exposure and copper-associated hepatopathy. Venous blood gases may show a metabolic acidosis (with blood pH normal to near 7), low bicarbonate concentration and a reduced base excess. A total CO2 level on a chemistry screen is not sensitive enough to detect the metabolic acidosis due to compensatory hyperventilation. Serum chemistry also will reveal deficiencies in sodium, potassium, calcium and phosphorous. Osteopenia is apparently not a feature of Fanconi syndrome in dogs as it is in humans. Some dogs develop azotemia, which worsens over time, with renal failure being the most common cause of death.
Urinalysis typically reveals glucosuria without hyperglycemia. In fact, the marked glucosuria in light of a normal blood glucose level is generally the reason to diagnostically pursue a Fanconi syndrome. Urine metabolic screening from dogs with Fanconi syndrome shows often massive generalized aminoaciduria and lactic aciduria (and the glucosuria is also confirmed). Metabolic screening at the University of Pennsylvania (PennGen; http://research.vet.upenn.edu/penngen/PennGenHome/tabid/91/Default.aspx) can document the generalized aminoaciduria, the hallmark finding of Fanconi syndrome. Dogs with Fanconi syndrome have much higher urinary concentrations of cystine and dibasic amino acids in comparison to cystinuria, as well as exhibit massive excretion of all other amino acids. Paradoxically, despite a severe degree of cystinuria in any dog with Fanconi syndrome, they rarely if ever develop cystine calculi and urinary obstruction; the dilute, alkaline urine and other products in urine from dogs with Fanconi syndrome may prevent the crystal and calculi formation. Moreover, while there is severe aminoaciduria, there is either no or only mild proteinuria. The University of Missouri offers DNA testing for Basenjis (http://www.caninegeneticdiseases.net ). However, the molecular basis in other breeds is unknown.
The therapeutic protocol (https://www.basenji.org/ClubDocs/fanconiprotocol2003.pdf) developed and modified over the years by Steve Gonto, a human anesthesiologist as well as a critical care/life support clinician and owner of Basenjis, has been used widely. While there are no formal comparative trials of different therapeutic modalities, the life expectancy and quality of life of Basenjis have been greatly improved by using this protocol. It focuses on aggressive correction of the various losses with particular attention to bicarbonate, normalizing electrolytes and minerals, and providing a high-quality diet. Bicarbonate is dosed to increase pCO2 and HCO3 levels. Unless the animal is in renal failure, a high protein diet is recommended to replenish the amino acid (and protein) losses and to rebuild muscle mass. Renal dialysis may be considered in the acute management of severe renal failure.

ESVNU Pre-Congress Day - PROCEEDINGS Page 32
In a survey of medical records, Basenjis with Fanconi syndrome received between 2.6-15.6 grams of sodium bicarbonate in tablet form divided per day. Multivitamin and calcium/phosphorus may be supplemented as needed. Treatment of Fanconi syndrome can be rewarding if the disease is recognized early. The median survival time for Basenjis was 5 years after the diagnosis was made. This medical protocol can be used to manage dogs with the acquired form, as long as the trigger is removed. The treatment must be adjusted for the breed size and severity of the metabolic derangements. Dogs that ingested Chinese jerky treats are known to have improved and even resolved their metabolic derangements within a few weeks to months after withdrawing the treats, unless they had already developed severe renal defects and failure by the time of diagnosis. Labrador Retrievers and other dogs with copper-associated hepatopathy and Fanconi syndrome may also require copper chelation and low copper diets. Supported in part by grants from the NIH (OD 010939). Dr. Adrian Sewell is also acknowledged for his collaboration. Conflict of Interest: The author’s laboratory (PennGen) offers metabolic screening for Fanconi Syndrome. Biocontrol and Laboklin are offering screening for Fanconi syndrome.
Selected References
Appleman EH, Cianciolo R, Mosenco AS, Bounds ME, Al-Ghazlat S (2008): Transient acquired Fanconi
syndrome associated with copper storage hepatopathy in 3 dogs. J Vet Intern Med 22: 1038-1042. Bovee KC. Fanconi syndrome in the dog (1980): In: Kirk RW, ed. Current Veterinary Therapy VII.
Philadelphia: WB Saunders Co 1075-1078. Bovee KC, Joyce T, Reynolds R, et al (1978). The Fanconi syndrome in Basenji dogs: a new model for renal
transport defects. Science 201: 1129-1131. Carmichael N, Lee J, Giger U (2014): Fanconi syndrome in dog in the UK. Vet Rec 174: 357-358. Escolar E, Perez-Alenza D, Diaz M (1993): Canine Fanconi syndrome. J Small Anim Pract 34: 567-570. Farias F, Mhlanga-Mutangadura T, Taylor JF, O’Brien DP, Schnabel RD, Johnson GS (2012): Whole genome
sequencing shows a deletion of the last exon of Fan1 in Basenji Fanconi syndrome. Proceedings of the Advances in Canine and Feline Genomics and Inherited Diseases Conference, Visby 51.
FDA Updates http://www.fda.gov/AnimalVeterinary/SafetyHealth/ProductSafetyInformation . Fieten H, Hooijer-Nouwens BD, Biourge VC, Leegwater PA, Watson AL, van den Ingh TS, Rothuizen J (2012).
Association of dietary copper and zinc levels with hepatic copper and zinc concentration in Labrador Retrievers. J Vet Intern Med 26:1274-1280
Gonto S (2017) Fanconi disease management protocol for veterinarians. www.basenji.org /fanconiprotocol Hill TL, Breitschwerdt EB, Cecere T, Vaden S (2008): Concurrent hepatic copper toxicosis and Fanconi’s
syndrome in a dog. J Vet Intern Med 22: 219-222. Hoffmann G, Jones PG, Biourge V, van den Ingh TS, Mesu SJ, Bode P, Rothuizen J (2009): Dietary
management of hepatic copper accumulation in Labrador Retrievers. J Vet Intern Med 23: 957-963. Hooijberg EH, Furman E, Leidinger E, Brandstetter D, Hochleitner C, Sewell A, Leidinger J, Giger U (2015): A
case of transient Fanconi syndrome in a dog exposed to chicken jerky treats. Tierärztl Prax 43: 188–192.
Hooper AN, Roberts BK (2011): Fanconi syndrome in four non-basenji dogs exposed to chicken jerky treats. J Am Anim Hosp Assoc. 47(6): e178-187.
Hostutler RA, DiBartola SP, Eaton KA (2004): Transient proximal renal tubular acidosis and Fanconi syndrome in a dog. J Am Vet Med Assoc 224: 1611-1614.
Klootwijk ED et al (2014) Mistargeting of peroxisomal EHHADH and inherited renal Fanconi's syndrome. N Engl J Med 370: 129-138.
Igase M, Baba K, Shimokava T, Noguchi S, Mizuno T Okuda M (2015): Acquired Fanconi syndrome in a dog exposed to jerky treats in Japan. J Vet Med Sci 77: 1507–1510.

ESVNU Pre-Congress Day - PROCEEDINGS Page 33
Langlois DK, Smedley RC, Schall WD, Kruger JM (2013): Acquired proximal renal tubular dysfunction in 9 Labrador Retrievers with copper-associated hepatitis (2006–2012). J Vet Intern Med 27: 491-499.
Major A, Schweighauser C, Hinden, Francey T (2014): Transient Fanconi syndrome with severe polyuria and polydipsia in a 4-year old Shih Tzu fed chicken jerky treats. Schweiz Arch Tierheilk 156: 591-596.
Noonan CH, Kay JM (1990): Prevalence and geographic distribution of Fanconi syndrome in Basenjis in the United States. J Am Vet Med Assoc 197: 345-349.
Ohmes OM, Davis EG, Beard LA, Vander Werf KA, Bianco AW, Giger U (2016): Transient Fanconi syndrome in Quarter horses. Can Vet J 55(2): 147–151.
Reinert NC, Feldman DG (2016): Acquired Fanconi syndrome in four cats treated with chlorambucil. J Feline Med Surg 18: 1034-1040.
Sheridan R, Mirabile, J, Hafler K (2014): Determination of six illegal antibiotics in chicken jerky dog treats. J Agri Food Chem 62: 3690-3696
Slutsky J, Raj K, Yunke S, Bell J, Fretwell N, Hedhammar A, Wade C, Giger U (2013) A web resource on DNA tests for canine and feline hereditary diseases. Vet J 197:182-187.
Slutsky J, Fitzgerald CA, Store V, Sewell A, Giger U (2014): Results of urinary metabolic screening in dogs with acquired and hereditary Fanconi syndrome. Submitted.
Thompson MF, Fleeman LM, Kessell AE, Steenhard LA, Foster SF (2013): Acquired proximal renal tubulopathy in dogs exposed to a common dried chicken treat: retrospective study of 108 cases (2007–2009). Austral Vet J 91: 368-373.
Yabuki A, Iwanaga T, Giger U, Sawa M, Kohyama M, Yamato O (2017): Acquired Fanconi syndrome in two dogs following long-term consumption of pet jerky treats in Japan: case report. J Vet Med Sci. 2017 May; 79(5): 818–821.
Yearly JH, Hancock DD, Mealey KL (2004): Survival time, lifespan and quality of life in dogs with Fanconi syndrome. J Am Vet Med Assoc 225: 377-383.