
ESTABLISHING MYCOBACTERIOLOGY LABORATORY SERVICES
60
ESTABLISHING MYCOBACTERIOLOGY LABORATORY SERVICES Dr.T.V.Rao MD
-
Upload
drtv-rao -
Category
Health & Medicine
-
view
148 -
download
0
Transcript of ESTABLISHING MYCOBACTERIOLOGY LABORATORY SERVICES
ESTABLISHING MYCOBACTERIOLOGY
LABORATORY SERVICESDr.T.V.Rao MD
TUBERCULOSIS – A TRIBUTE TO ……
Dr.T.V.Rao MD 2

TUBERCULOIS IS NOT ONLY A DISEASE OF POOR BUT RICH AND POWERFUL TOO GET
Dr.T.V.Rao MD 3

India Profile• No of Govt. hospitals 12760,
• CHCs 4510, PHCs 23391, Sub-centers 145894
• Beds in Government Sector, 576793;
• Population per Government Hospital Bed 2012.
• No of medical colleges 314 +; Blood banks - 2445, Eye Banks -586,
• Diverse socio-economic, cultural, political conditions
•Large unregulated private sector in health careDr.T.V.Rao MD 4
WHY NEED FOR ESTABLSHING MYCOBACTERIOLOGY LABORATOREIS •A high-quality laboratory system that uses modern diagnostics is a prerequisite for early, rapid and accurate detection of TB. Lack of diagnostic capacity has been a crucial barrier preventing an effective response to the challenges of HIV-associated and drug resistant tuberculosis (TB) Dr.T.V.Rao MD 5

PRIMARY STEP IN CARING THE TUBERCULOSIS PATIENTS
•Care of patients with TB starts with a quality assured diagnosis, obtained by identifying Mycobacterium tuberculosis from clinical specimens and conducting DST of the organism to confirm or exclude resistance.
Dr.T.V.Rao MD 6
Why we failed ( Cont )
•Diagnostic services are poor, and so we failed at Individual and community levels.
•Patients are diagnosed late.
•Many patients are never diagnosed before death.
Early deaths are burden to Social Infrastructure and Economic loss.
Dr.T.V.Rao MD 7

WHO MONITORS THE DIAGNOSTIC TOOLS
• Research on new TB diagnostic tools has been accelerated over the last few years and the diagnostic pipeline has been growing rapidly as a result. At the same time, an unprecedented effort to improve and expand TB laboratory capacity is currently being lead by WHO and the Stop TB Partnership Global Laboratory Initiative (GLI) together with the GLI network of international collaborators
Dr.T.V.Rao MD 8

Enhancement of Diagnostic Capacity
•Enhancement of diagnostic capacity for TB and MDR-TB is urgently needed to scale-up access to care and treatment of MDR-TB. To help meet this challenge
Dr.T.V.Rao MD 9

Development of laboratory norms and standards
• Including WHO policy recommendations on the use of new diagnostics, specifications for TB laboratory equipment, laboratory biosafety, standard operating procedures for TB laboratories, and technical manuals for first-and second-line drug susceptibility testing
Dr.T.V.Rao MD 10

Prioritization of human resource development and training,
• Including development of comprehensive training and retention strategies, and proposals to train different cadres of laboratory consultants
Dr.T.V.Rao MD 11
Dr.T.V.Rao MD 12

Laboratory accreditation• Involving a WHO-led task
force with international experts and key partners, to develop a framework for a voluntary laboratory accreditation programme for national and regional TB reference laboratory networks
Dr.T.V.Rao MD 13

Laboratory biosafety guidance
• Under WHO and CDC leadership, to develop risk-based biosafety standards for laboratories in resource-constrained settings, supported by appropriate biosafety manuals and training packages
Dr.T.V.Rao MD 14

Core elements of laboratory services
• Laboratory infrastructure, appropriate biosafety measures and maintenance
• Equipment validation and maintenance• Specimen transport and referral mechanisms• Management of laboratory commodities and supplies• Laboratory information and data management systems• Laboratory quality management systems• Appropriate, adequate strategies and funding for laboratory human
resource development• Coordination of technical assistance• Integration of diagnostic algorithms in laboratory strengthening plans.
Dr.T.V.Rao MD 15

TB diagnostics and laboratory strengthening

Microscopy and Tuberculosis
Microscopy with Ziehl – Neelsen’s staining
A century old
procedure
Dr.T.V.Rao MD 17

Diagnosis of Pulmonary Tuberculosis
•Three specimens optimal
•Spot specimen on first visit; sputum container given to patient
•Early morning collection by patient on next day
•Spot specimen during second visit
Dr.T.V.Rao MD 18
19
WHO and IUATLDPositive and Negative Report
•Negative Report: Negative for AFB where no organisms observed in 100 oil immersion fields
•Positive Report: Positive for acid-fast bacilli; provide AFB quantification
Dr.T.V.Rao MD

20
WHO/IUATLD Quantification scale Ziehl Neelsen
Number of AFB Number of fields* examined What to report
No AFB in 100 fields 100 fieldsNo Acid Fast Bacilli detected
1–9 AFB in 100 fields
100 fieldsRecord exact figure
(1 to 9 AFB per 100 fields)
10– 99 AFB in 100 fields
100 fields1 +
1– 10 AFB in each field
50 fields 2 +
More than 10 AFB in each field
20 fields3 +
* Oil immersion fields Dr.T.V.Rao MD

Limitation of Microscopy for Tuberculosis.
• Repeated sample examinations. load on technical staff.
• Training and dedication of Microscopist.
• The load of bacilli must be more than 10,000 / 1 ml of sputum.
• Low in sensitivity < 50 %
• Repeated requests for samples
• High drop out by patients, for repeated samples.
• Not dependable in pediatric age group.
Dr.T.V.Rao MD 21

22
False Negatives and Consequences
False-negative means that the results that were reported negative were truly positive
Patients with TB may not be treated resulting in on-going disease, disease transmission, or death.
Intensive phase treatment may not be extended, resulting in inadequate treatment and potential drug resistance
Dr.T.V.Rao MD

23
False Positives and Consequences
False-positives mean that the results that were reported positive were truly negative
•Patients are treated unnecessarily
•Treatment may be continued longer than necessary
•Medications will be wasted
Dr.T.V.Rao MD

When Microscopy fails•Smear negative tuberculosis.
• In HIV infected patients, on many occasions prove negative. in spite of presence of bacilli, ( as few bacilli are expectorated).
•Needs concentration and liquefaction with chemicals.
•Time consuming, needs more technical manpower
Dr.T.V.Rao MD 24

QUALITY CONTROL TEACHES MANY MATTERS
Dr.T.V.Rao MD 25

Growing role ofFluorescent Microscopy
• There is a growing need for screening for AFB by Florescent Microscopy.
• Several studies prove, Florescent Microscopy in Diagnosis of Tuberculosis is a priority,
• Developing world should opt and initiate florescent microscopy.
Dr.T.V.Rao MD 26
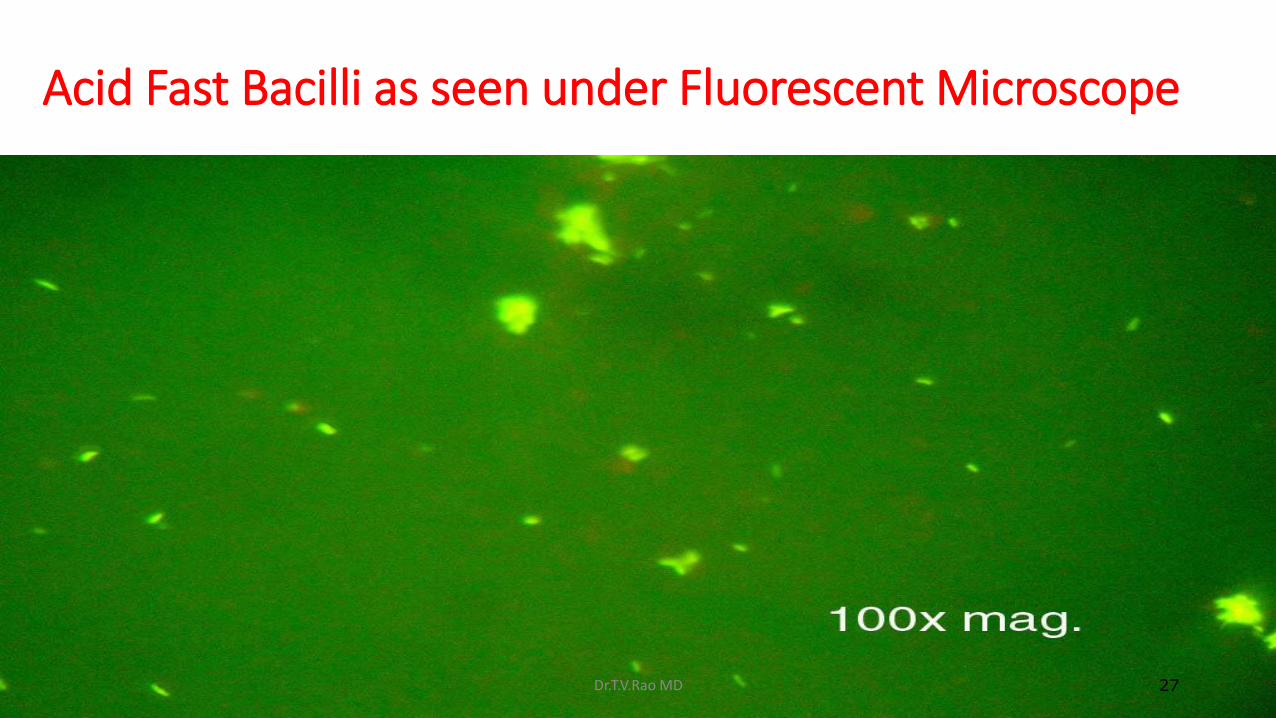
Acid Fast Bacilli as seen under Fluorescent Microscope
Dr.T.V.Rao MD 27

Light emitting diodes (LED)• The recent development of light
emitting diodes (LED), with the appropriate fluorescent light output for FM and low power consumption, has led to the development of simple, robust LED FM microscopes, requiring minimal mains or battery power and no dark room requirement. The WHO has recommended rolling it out as an alternative to LMs in resource-limited settings,
Dr.T.V.Rao MD 28

Culturing Most useful in
• Surveillance,
• Drug sensitivity testing patterns.
• Identify treatment failures.
• Useful in Patients presenting with respiratory symptoms, X-ray’s suggestive, but smear negative. Can prove culture positive.
• Cultures remain suggestive and helpful in early treatment periods, failed drug regimes.
Dr.T.V.Rao MD 29

Methods of Culturing.
•Culturing on Lowenstein Jenson’s culture medium remain the affordable ,economical method in developing world.
Dr.T.V.Rao MD 30

Limitation in Culturing
• Mycobacterium spp are slow growing.
• Need 6 – 8 weeks for growing.
• Specimens can be contaminated while growing, needs repeated specimens, in turn patients loose confidence in Laboratories.
Dr.T.V.Rao MD 31

Pitfalls in Culturing
• Specificity is lost due to contamination.•Can yield false positive
results in 1 – 4 % of the cases.•Cultures may be negative
in spite of x rays are suggestive of tuberculosis.
Dr.T.V.Rao MD 32

ADVANCES IN CULTURING TECHNIQUES.
There are emerging Modern Media with accurate detection, are replacing the Egg and Agar based medium.

Emerging methods in Culturing
• MGIT – Mycobacterium growth incubator tube method.
• Growth occurs in shorter than egg medium.
• Usefulness in HIV patients established.
• Contamination is less
• But expensive to people in Developing world.
Dr.T.V.Rao MD 34
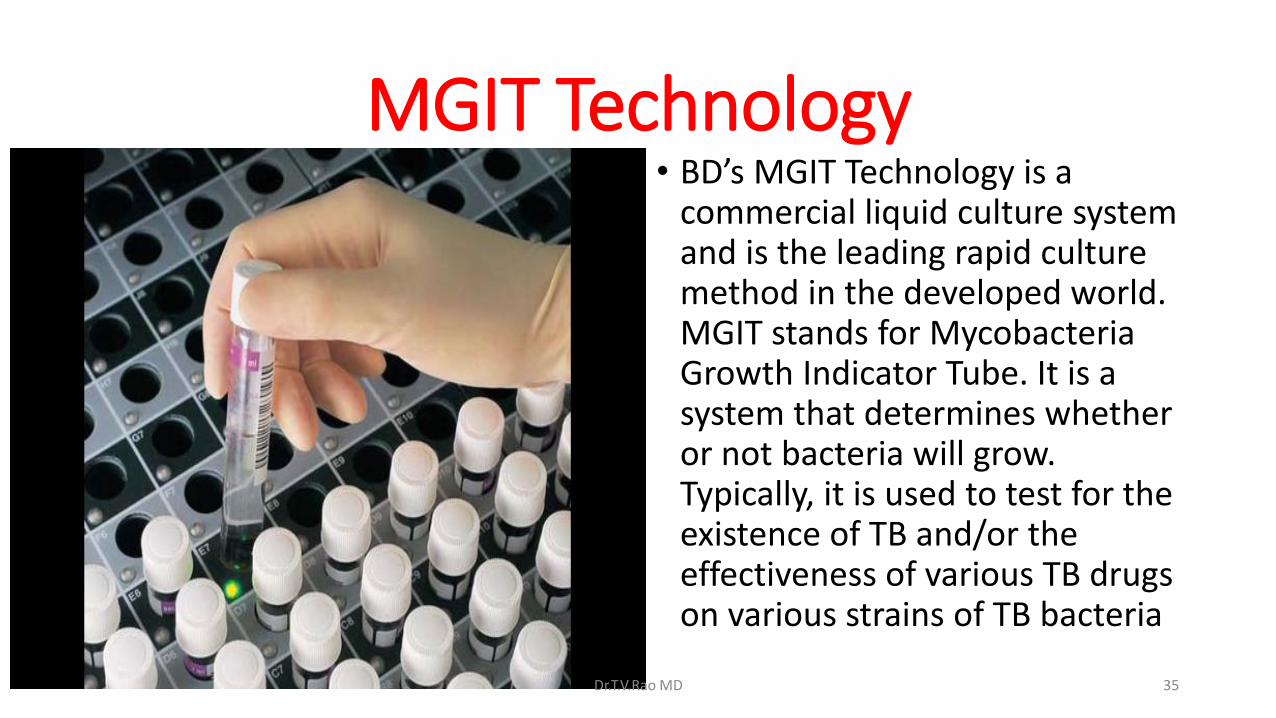
MGIT Technology • BD’s MGIT Technology is a
commercial liquid culture system and is the leading rapid culture method in the developed world. MGIT stands for Mycobacteria Growth Indicator Tube. It is a system that determines whether or not bacteria will grow. Typically, it is used to test for the existence of TB and/or the effectiveness of various TB drugs on various strains of TB bacteria
Dr.T.V.Rao MD 35

Molecular Methods in Diagnosis of Tuberculosis
Several methods are available, mainly used as
Research tools

Real Time PCR replacing older Methods
Dr.T.V.Rao MD 37
PCR How useful to our Patients?
•PCR ( Polymerase chain reaction ) used by several investigators.
•However most cases can be diagnosed with simple methods if effectively used.
• The definite role of PCR continues to be controversial
•Above all not cost effective to Developing countries.
Dr.T.V.Rao MD 38

Emerging Rapid Methods.
1. Fast Plaque TB uses phage amplification technology.
2. ELISA ( QuantiFERON – TB )
3. Enzyme-Linked immunospot
( ELISPOT )
ELISPOT proved highly useful to detect active
tuberculosis in Adults and children.
Dr.T.V.Rao MD 39

Emerging TechnologyMODS
•Microscopic observation drug susceptibility assay. ( MODS )
•A new method gained importance in several reviews.
•Use a tissue culture plate based assay with use of Middle Brook 7HG.
•Needs a inverted light microscope.
• Even the drug resistance can be tested with Rifampicin, and Isoniazid.
• Safe to work with cultures.Dr.T.V.Rao MD 40

DETECTION OF ANTIBODIES
•Although the detection of antibodies against MTB in the blood is a relatively simple and cost-effective method, recent meta-analyses and systematic reviews concluded that commercial serological tests provided inconsistent results. As the overall test performance and data quality of these assays were poor, the WHO currently recommends against their use for the diagnosis of pulmonary and extra pulmonary TB.Dr.T.V.Rao MD 41

( Mantoux Test )
Dr.T.V.Rao MD 42

Tuberculin Test( Mantoux Test )
• Test to be interpreted in relation to clinical evaluation.• Even the induration of 5
mm to be considered positive when tested on HIV patients.• Lacks specificity.
Dr.T.V.Rao MD 43

Extra Pulmonary Tuberculosis
Poses several challenges, Yet no optimal, specific diagnostic methods

Extra pulmonary Tuberculosis
•A real challenge to Clinicians and Laboratories.
•Optimal specimen collection a priority,
•Molecular Methods are growing need.
•Clinicians start drug regimes on empirical basis.
•Several serological tests for antibody determinations are evaluated. But of No Use
Dr.T.V.Rao MD 45

WHO monitoring of Xpert MTB/RIF roll-out
•Xpert MTB/RIF is an automated, cartridge-based nucleic amplification assay for the simultaneous detection of TB and rifampicin resistance directly from sputum in under two hours.
Dr.T.V.Rao MD 46

GeneXpert platform
• The technology is based on the GeneXpert platform and was developed as a partnership with support from the US National Institutes of Health. WHO recommended use of the technology in December 2010 and is monitoring the global roll-out of the technology to promote coordination.
Dr.T.V.Rao MD 47
GeneXpert MTB/RIF• The Xpert MTB/RIF is a cartridge-based, automated
diagnostic test that can identify Mycobacterium tuberculosis (MTB) and resistance to rifampicin (RIF). It was co-developed by Cepheid, Inc. and Foundation for Innovative New Diagnostics, with additional financial support from the US National Institutes of Health (NIH) and technical support from the University of Medicine and Dentistry of New Jersey
Dr.T.V.Rao MD 48
How the test works
•The Xpert MTB/RIF detects DNA sequences specific for Mycobacterium tuberculosis and rifampicin resistance by polymerase chain reaction It is based on the Cepheid GeneXpert system, a platform for rapid and simple-to-use nucleic acid amplification tests (NAAT).
Dr.T.V.Rao MD 49

How the test works
•The Xpert® MTB/RIF purifies, concentrates, amplifies (by real-time PCR) and identifies targeted nucleic acid sequences in the Mycobacterium tuberculosis genome, and provides results from unprocessed sputum samples in 90 minutes, with minimal biohazard and very little technical training required to operate
Dr.T.V.Rao MD 50
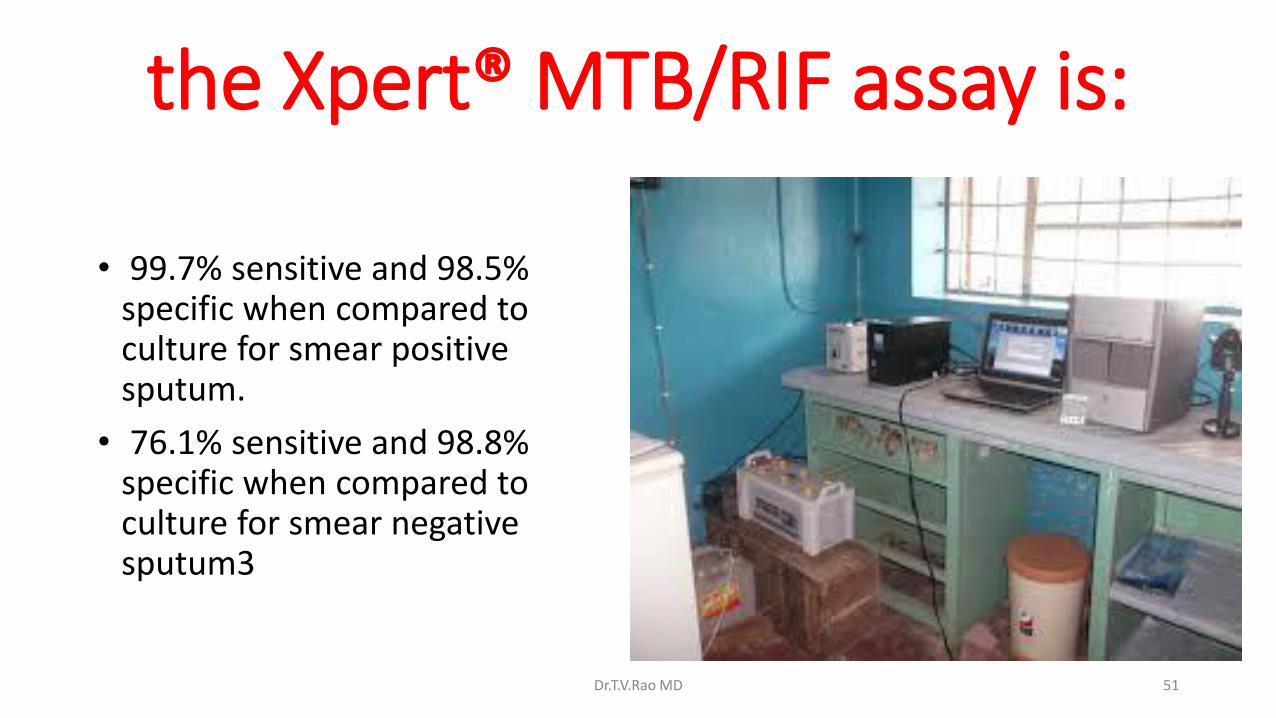
the Xpert® MTB/RIF assay is:
• 99.7% sensitive and 98.5% specific when compared to culture for smear positive sputum.
• 76.1% sensitive and 98.8% specific when compared to culture for smear negative sputum3
Dr.T.V.Rao MD 51
Microscopy in TuberculosisTODAY
In spite of several scientific, and molecular advances Microscopy in Tuberculosis continues to be back bone in Diagnosis.
Dr.T.V.Rao MD 52
Do not neglect Fundamentals in Microbiology
Dr.T.V.Rao MD 53
REAL PCR NEEDED TODAY IN MICROBIOLOGY

MICROBIOLOGISTS NEED
•P Patience
•C commitment to work
•R Responsibility
•or else we will be ignored
Dr.T.V.Rao MD 55

WHAT ARE ESSENTAILS TO START LABORATORY
• A separate Ventilated Room with proper exhaust
• Minimal Laboratory Equipment as Bacteriology culture laboratory
• Biosafety Cabinet grade 3 ?
• Two technicians having basic experience in handling Biohazard Specimens
• Documentation facilities
• A GREAT DETERMINATION
Dr.T.V.Rao MD 56
We can train and learn many things at this Internet site
•Essentials for the Mycobacteriology Laboratory:•Promoting Quality Practices•The Association of Public Health Laboratories works to strengthen laboratories serving the public's health in the US and globally. - See more at: http://www.aphl.org/AboutAPHL/Pages/default.aspx#sthash.A9SaRJiV.dpuf
Dr.T.V.Rao MD 57
NEVER FORGET
• India spends least on patients with just 28$ among the BRICS Countries
•Many believe India has Million Missing patients
• India has close to 1,00,000 cases of Multidrug resistant TB which is hard to diagnose and treat
•Most Important Undocumented and untreated
Dr.T.V.Rao MD 58

Dr.T.V.Rao MD 59

I THANK YOU AND MICROSCPE
Dr.T.V.Rao MD 60


















