
EST 18 PCU Track 1 Session 3 pmiCME GLP-1 RA
12
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes. 11:15 AM - 12:30 PM The Expanding Role of GLP-1 Receptor Agonists in the Changing Landscape of T2DM SPEAKERS John E. Anderson, MD Jessica R. Castle, MD Disclosures ► John E. Anderson, MD: Advisory Board for Abbott; AstraZeneca; Boehringer Ingelheim Pharmaceuticals, Inc.; Janssen Pharmaceuticals, Inc.; Lilly; Merck & Co., Inc.; and Sanofi US. Services Provided for Promotional Purposes (not for CME/CE) for Janssen Pharmaceuticals, Inc.; Lilly; and Sanofi US. Speaker's Bureau for AstraZeneca; Boehringer Ingelheim Pharmaceuticals, Inc.; Janssen Pharmaceuticals, Inc.; Lilly; and Sanofi US. ► Jessica R. Castle, MD: No financial relationships to disclose. The following relationships exist related to this presentation: Off-Label/Investigational Discussion ► In accordance with pmiCME policy, faculty have been asked to disclose discussion of unlabeled or unapproved use(s) of drugs or devices during the course of their presentations. This session is supported by an independent educational grant from Lilly . 30.3 million Americans (9.3% of US population) have diabetes 92 million Americans have pre-diabetes (increased from 79 million in 2010) 1 in 3 adults will have T2DM in 2050 90% of all diabetes management occurs within the primary care setting (1) Unger J. Diabetes Management in Primary Care, 2nd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2012. WHY BOTHER ATTENDING YET ANOTHER DIABETES LECTURE? The World is Changing! ► Tendency is to intensify therapy based on sampling availability rather than pathogenetic targets ► Concern of possible AEs of newer agents ► Currently 257 drug combinations can be used to manage patient with T2DM ► As therapy is intensified, patients experience an increase risk of weight gain, hypoglycemia and even mortality T2DM SIGNIFICANTLY REDUCES LIFE EXPECTANCY (1) Emerging Risk Factors Collaboration. JAMA. 2015;314:52–60. (2) World Heart Federation. http://www.world-heart- federation.org/fileadmin/user_upload/documents/Fact_sheets/2012/PressBackgrounderApril2012RiskFactors.pdf. Accessed August 10, 2017. -6.7 years -11.2 years -15.7 years T2DM T2DM History of MI T2DM History of MI History of Stroke
Transcript of EST 18 PCU Track 1 Session 3 pmiCME GLP-1 RA

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
11:15 AM - 12:30 PM
The Expanding Role of GLP-1 Receptor Agonists in the Changing Landscape of T2DMSPEAKERSJohn E. Anderson, MDJessica R. Castle, MD
Disclosures
► John E. Anderson, MD: Advisory Board for Abbott; AstraZeneca; Boehringer Ingelheim Pharmaceuticals, Inc.; Janssen Pharmaceuticals, Inc.; Lilly; Merck & Co., Inc.; and Sanofi US. Services Provided for Promotional Purposes (not for CME/CE) for Janssen Pharmaceuticals, Inc.; Lilly; and Sanofi US. Speaker's Bureau for AstraZeneca; Boehringer Ingelheim Pharmaceuticals, Inc.; Janssen Pharmaceuticals, Inc.; Lilly; and Sanofi US.
► Jessica R. Castle, MD: No financial relationships to disclose.
The following relationships exist related to this presentation:
Off-Label/Investigational Discussion► In accordance with pmiCME policy, faculty have been asked to disclose discussion of
unlabeled or unapproved use(s) of drugs or devices during the course of their presentations.
This session is supported by an independent educational grant from Lilly .
30.3 million Americans (9.3% of US population) have diabetes
92 million Americans have pre-diabetes (increased from 79 million in 2010)
1 in 3 adults will have T2DM in 2050
90% of all diabetes management occurs within the primary care setting
(1) Unger J. Diabetes Management in Primary Care, 2nd ed. Philadelphia, PA: Lippincott, Williams & Wilkins; 2012.
WHY BOTHER ATTENDING YET ANOTHER DIABETES LECTURE?
The World is Changing!
► Tendency is to intensify therapy based on sampling availability rather than pathogenetic targets
► Concern of possible AEs of newer agents► Currently 257 drug combinations can be used to manage patient with T2DM► As therapy is intensified, patients experience an increase risk of weight gain, hypoglycemia and
even mortality
T2DM SIGNIFICANTLY REDUCES LIFE EXPECTANCY
(1) Emerging Risk Factors Collaboration. JAMA. 2015;314:52–60. (2) World Heart Federation. http://www.world-heart-federation.org/fileadmin/user_upload/documents/Fact_sheets/2012/PressBackgrounderApril2012RiskFactors.pdf. Accessed August 10, 2017.
-6.7 years
-11.2 years
-15.7 years
T2DMT2DMHistory of MI T2DM
History of MIHistory of Stroke

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Even
ts p
er 1
0,00
0 ov
eral
lad
ult p
opul
atio
n
Gregg et al. N Engl J Med 2014;370:1514–23
DIABETES-RELATED COMPLICATIONS IN THE USACUTE MYOCARDIAL INFARCTION AND STROKE
Overall population
Population with diabetesOverall population
Acute myocardial infarctionStroke
1990 1995 2000 2005 20100
150
125
25
100
75
50
Age-
adju
sted
Rel
ativ
e R
isk
Body mass index (BMI) (kg/m2)
Men
Women
<22 <23 23-23.9
24-24.9
25-26.9
27-28.9
29-30.9
31-32.9
33-34.9
35+
1.02.91.0
4.31.0
5.01.5
8.12.2
15.8
4.4
27.6
40.3
54.0
93.2
6.7 11.6
21.3
42.1
0
25
50
75
100
(1) Chan JM, et al. Diabetes Care. 1994;17:961-969. (2) Colditz GA, et al. Ann Intern Med. 1995;122:481-486.
RELATIONSHIP BETWEEN BMI AND RISK OF T2DM
BILL – 67 YEARS OLD
FAMILY HISTORYMother (died age 71): T2DM, CVD, hypercholesterolemiaFather (died age 75): T2DM, diverticulosis, hypercholesterolemia
MEDICAL HISTORYT2DM x 6 yrsHTN x 7 yrs
MEDICATIONSMetformin 1000 mg BIDGlimepiride 8 mg QDLisinopril 30 mg QDAtorvastatin 40 mg QD
VITALSHeight: 5’ 11”Weight: 205 lbsBMI: 32 kg/m2
BP: 130/82 mm Hg
LABSFPG: 102 mg/dLPPG average: 150 mg/dLHbA1c: 7.7%LDL: 89 mg/dL
HDL: 51 mg/dLTG: 97 mg/dLeGFR: 96 mL/min/1.73 m2
INITIAL VISIT
2018 ADA STANDARDS OF MEDICAL CARE IN DIABETES
American Diabetes Association Diabetes Care 2018;41:S73-S85
HbA1c goal <7%
Monitor for hypoglycemia
Prevent weight gain

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
HYPERGLYCEMIA
Pancreas Insulin secretionGlucagon secretion
Liver Hepatic
glucose secretion
Muscle andadipose tissueGlucose uptake
CNSDelayed satiety
Neurotransmitter dysfunction
KidneyGlucose reabsorption
Adipose tissueLipolysis
PATHOPHYSIOLOGIC MECHANISMS IN HYPERGLYCEMIA OF T2DM
GutDiminished incretin
effect Altered intestinal glucose absorption
2018 ADA STANDARDS OF MEDICAL CARE IN DIABETES
American Diabetes Association Diabetes Care 2018;41:S73-S85
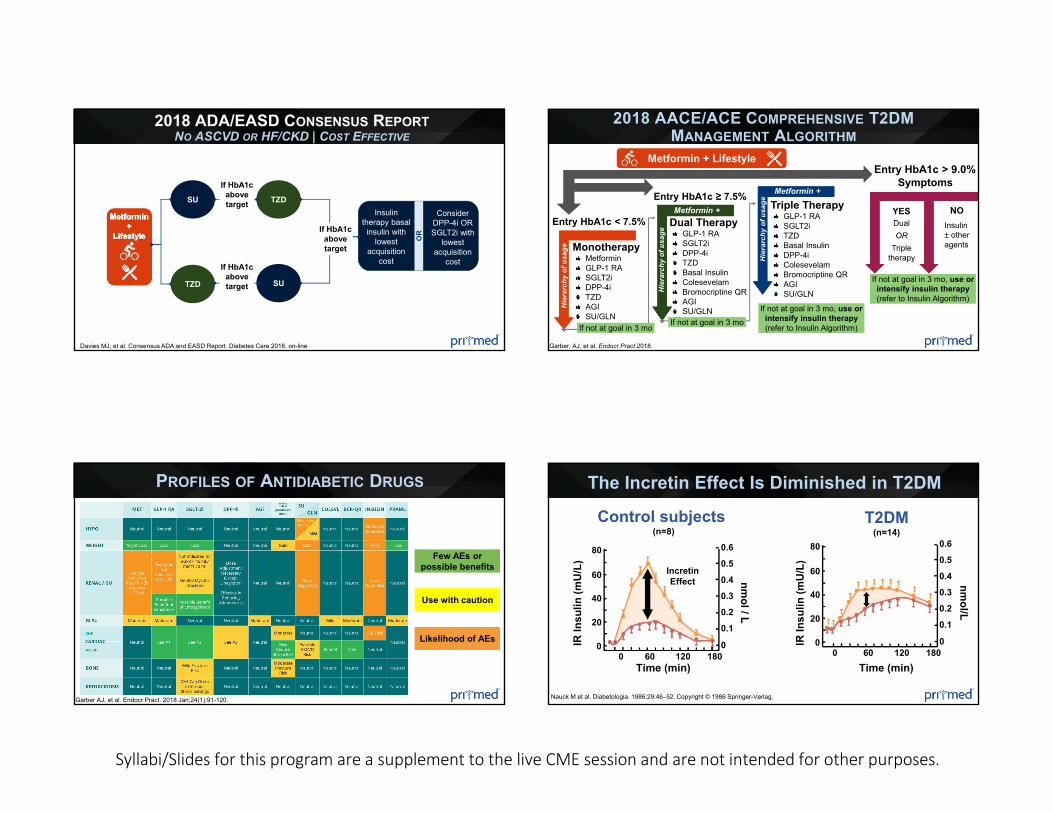
2018 ADA/EASD CONSENSUS REPORTNO ASCVD OR HF/CKD | NEED TO MINIMIZE HYPOGLYCEMIA
Davies MJ, et al. Consensus ADA and EASD Report. Diabetes Care 2018, on-line
Metformin +
Lifestyle
Metformin +
Lifestyle
Metformin +
Lifestyle
ORSGLT2i GLP-
1 RADPP-
4i OR
ORGLP-1
RA TZDDPP-4i O
R
ORSGLT2i TZD
ORSGLT2i TZDDPP-4iDPP-4i
GLP-1 RA
GLP-1 RA
SGLT2iSGLT2i
TZDTZD
If HbA1c above target
If HbA1c above target
If HbA1c above target
If HbA1c above target
• Choose later generation of SU with lower risk of hypoglycemia
• Consider basal insulin with lower risk of hypoglycemia
• Choose later generation of SU with lower risk of hypoglycemia
• Consider basal insulin with lower risk of hypoglycemia
Consider the addition of SU or basal insulin
If HbA1c above
target…
Continue with addition
of other agents
If HbA1c still above
target….
2018 ADA/EASD CONSENSUS REPORTNO ASCVD OR HF/CKD | NEED TO MINIMIZE WEIGHT GAIN OR PROMOTE WEIGHT LOSS
*With good weight loss efficacy
Davies MJ, et al. Consensus ADA and EASD Report. Diabetes Care 2018, on-line
GLP-1 RA*
SGLT2i
GLP-1 RA*
SGLT2i
If HbA1c above target
• PREFERABLYDPP-4i (if not on GLP-1 RA) based on weight neutrality
If triple therapy required or SGLT2i and/or GLP-1 RA not tolerated or
contraindicated use regimen with lowest
risk of wt gain• PREFERABLY
DPP-4i (if not on GLP-1 RA) based on weight neutrality
If triple therapy required or SGLT2i and/or GLP-1 RA not tolerated or
contraindicated use regimen with lowest
risk of wt gain
EITH
ER/O
REI
THER
/OR
GLP-1 RA*GLP-1 RA* SGLT2iSGLT2i
EITH
ER/O
R
GLP-1 RA* SGLT2i
If HbA1c above target
If HbA1c above target
• SU• TZD• Basal insulin
If DPP-4i not tolerated or
contraindicated or patient already on
GLP-1 RA, cautiously add…
• SU• TZD• Basal insulin
If DPP-4i not tolerated or
contraindicated or patient already on
GLP-1 RA, cautiously add…
Metformin +
Lifestyle
Metformin +
Lifestyle
Metformin +
Lifestyle
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
2018 ADA/EASD CONSENSUS REPORTNO ASCVD OR HF/CKD | COST EFFECTIVE
Davies MJ, et al. Consensus ADA and EASD Report. Diabetes Care 2018, on-line
Metformin +
Lifestyle
Metformin +
Lifestyle
Metformin +
Lifestyle
SU
TZD SU
TZD
If HbA1c above target
If HbA1c above target
OR
Insulin therapy basal
insulin with lowest
acquisition cost
Consider DPP-4i OR SGLT2i with
lowest acquisition
cost
If HbA1c above target
Garber, AJ, et al. Endocr Pract.2018.
2018 AACE/ACE COMPREHENSIVE T2DM MANAGEMENT ALGORITHM
Entry HbA1c < 7.5%
MonotherapyMetforminGLP-1 RASGLT2iDPP-4iTZDAGISU/GLN
Hie
rarc
hy o
f usa
ge
Triple TherapyGLP-1 RASGLT2iTZDBasal InsulinDPP-4iColesevelamBromocriptine QRAGISU/GLN
Metformin +
Hie
rarc
hy o
f usa
ge Metformin +
If not at goal in 3 moIf not at goal in 3 mo
Hie
rarc
hy o
f usa
ge
Entry HbA1c ≥ 7.5%
Dual TherapyGLP-1 RASGLT2iDPP-4iTZDBasal InsulinColesevelamBromocriptine QRAGISU/GLN
Metformin +
If not at goal in 3 moIf not at goal in 3 moIf not at goal in 3 mo, use or
intensify insulin therapy (refer to Insulin Algorithm)
If not at goal in 3 mo, use or intensify insulin therapy (refer to Insulin Algorithm)
Entry HbA1c > 9.0%Symptoms
YES NODualOR
Triple therapy
Insulin ± other agents
If not at goal in 3 mo, use or intensify insulin therapy (refer to Insulin Algorithm)
If not at goal in 3 mo, use or intensify insulin therapy (refer to Insulin Algorithm)
Metformin + Lifestyle
PROFILES OF ANTIDIABETIC DRUGS
Garber AJ, et al. Endocr Pract. 2018 Jan;24(1):91-120.
Few AEs or possible benefits
Likelihood of AEs
Use with caution
Time (min)
IR In
sulin
(mU
/L)
nmol/L
0.6
0.5
0.40.3
0.2
0.1
0
80
60
40
20
018060 1200
T2DM(n=14)
Control subjects (n=8)
Time (min)
IR In
sulin
(mU
/L)
nmol/ L
0.6
0.5
0.40.3
0.2
0.1
0
80
60
40
20
018060 1200
IncretinEffect
The Incretin Effect Is Diminished in T2DM
Nauck M et al. Diabetologia. 1986;29:46–52. Copyright © 1986 Springer-Verlag.
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
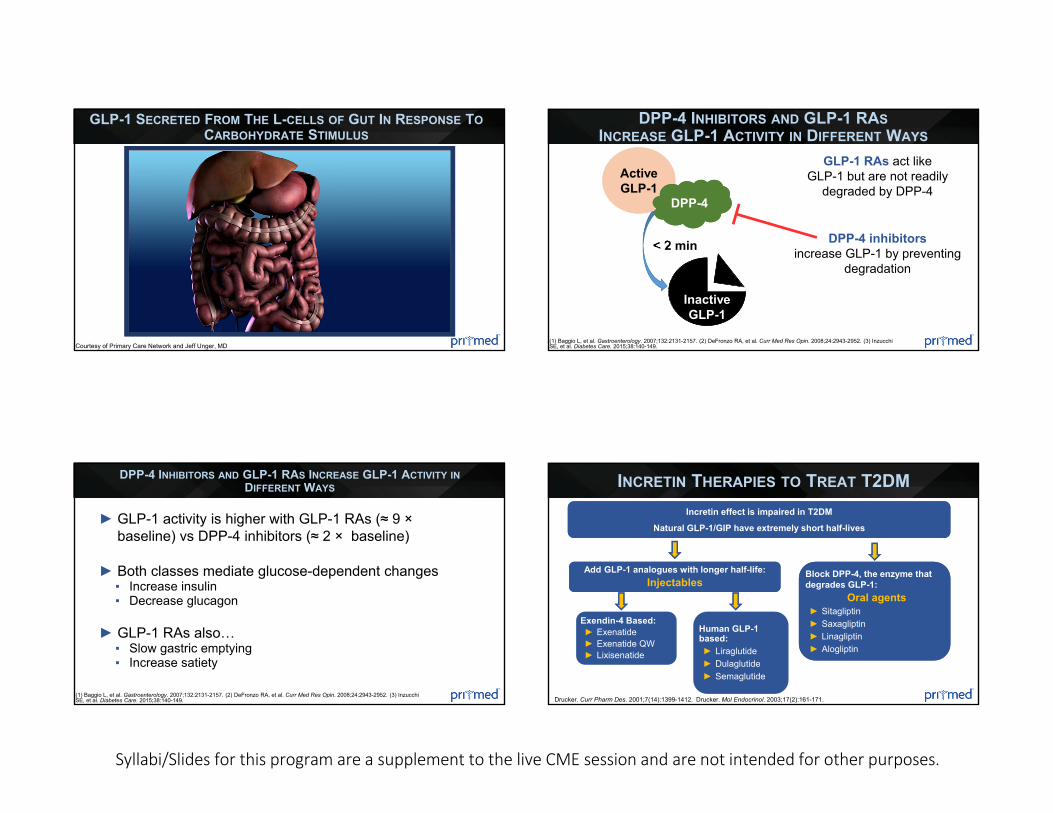
Courtesy of Primary Care Network and Jeff Unger, MD
GLP-1 SECRETED FROM THE L-CELLS OF GUT IN RESPONSE TOCARBOHYDRATE STIMULUS
(1) Baggio L, et al. Gastroenterology. 2007;132:2131-2157. (2) DeFronzo RA, et al. Curr Med Res Opin. 2008;24:2943-2952. (3) Inzucchi SE, et al. Diabetes Care. 2015;38:140-149.
DPP-4 INHIBITORS AND GLP-1 RASINCREASE GLP-1 ACTIVITY IN DIFFERENT WAYS
< 2 min DPP-4 inhibitors increase GLP-1 by preventing
degradation
GLP-1 RAs act like GLP-1 but are not readily
degraded by DPP-4Active GLP-1
DPP-4
Inactive GLP-1
(1) Baggio L, et al. Gastroenterology. 2007;132:2131-2157. (2) DeFronzo RA, et al. Curr Med Res Opin. 2008;24:2943-2952. (3) Inzucchi SE, et al. Diabetes Care. 2015;38:140-149.
DPP-4 INHIBITORS AND GLP-1 RAS INCREASE GLP-1 ACTIVITY INDIFFERENT WAYS
► GLP-1 activity is higher with GLP-1 RAs (≈ 9 ×baseline) vs DPP-4 inhibitors (≈ 2 × baseline)
► Both classes mediate glucose-dependent changes▪ Increase insulin▪ Decrease glucagon
► GLP-1 RAs also…▪ Slow gastric emptying▪ Increase satiety
Add GLP-1 analogues with longer half-life:Injectables
Incretin effect is impaired in T2DM
Natural GLP-1/GIP have extremely short half-lives
Block DPP-4, the enzyme that degrades GLP-1:
Oral agents ► Sitagliptin► Saxagliptin► Linagliptin► Alogliptin
Drucker. Curr Pharm Des. 2001;7(14):1399-1412. Drucker. Mol Endocrinol. 2003;17(2):161-171.
INCRETIN THERAPIES TO TREAT T2DM
Exendin-4 Based:► Exenatide► Exenatide QW► Lixisenatide
Human GLP-1 based:► Liraglutide► Dulaglutide► Semaglutide

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
CANDIDATES FOR GLP-1 RA THERAPY
(1) Garber AJ, et al. Endocr Pract. 2018 Jan;24(1):91-120. (2) American Diabetes Association Diabetes Care 2018;41:S73-S85
☑Add-on therapy for patients who do not achieve their HbA1c target after 3 months of metformin therapy1
☑ In combination with metformin (and/or another oral agent*) when:1,2
▪ Weight loss or avoidance of hypoglycemia is a primary consideration
▪ The HbA1c level is close to target (within 1-1.5%)
▪ Cost or injection therapy are not major barriers
☑1st-line therapy as an alternative to metformin in patients who cannot tolerate or are contraindicated for metformin
*Use with DPP-4 inhibitors is NOT RECOMMENDED
due to similar mechanisms and lack of additional therapeutic
benefit
ANTIDIABETIC AGENTS: EFFECT ON WEIGHT
(1) ADA. Diabetes Care. 2017;40(suppl 1):S1-S135. (2) Garber AJ, et al. Endocr Pract. 2017;23:207-238. (3) Zhong X, et al. Diabetes Res Clin Pract. 2015;109:451-460.
Agent Weight ChangeMetformin Slight loss
Sulfonylureas Gain
TZDs Gain
DPP-4 inhibitors Neutral
SGLT2 inhibitors Loss
GLP-1 RAs Loss
Basal insulin Gain
HYPOGLYCEMIC RISK WITH ANTIDIABETIC AGENTS
(1) ADA. Diabetes Care. 2017;40(suppl 1):S1-S135. (2) Garber AJ, et al. Endocr Pract. 2017;23:207-238.
Agent Risk of HypoglycemiaMetformin NeutralSulfonylureas High
TZDs Neutral
DPP-4 inhibitors LowSGLT2 inhibitors Low
GLP-1 RAs Neutral*Insulin High* Increased risk if used in combination with sulfonylureas or insulin
Zoungas S, et al. N Engl J Med. 2010;363:1410-1418.
FREQUENCY OF ADVERSE OUTCOMES IN PATIENTS WITH T2DM EXPERIENCINGSEVERE HYPOGLYCEMIA
25
No.
of A
dver
se O
utco
mes
Severe Hypoglycemia to Event (months)
20
15
10
5
00-12 13-24 25-36 37-48
Macrovascular eventMicrovascular eventDeath from any causeCV deathNon-CV death
The median time from an episode of severe hypoglycemia until death in T2DM is ≤ 1.05 years!
The median time from an episode of severe hypoglycemia until death in T2DM is ≤ 1.05 years!
Conclusion − severe hypoglycemia is associated with a higher risk of mortalityConclusion − severe hypoglycemia is associated with a higher risk of mortality
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
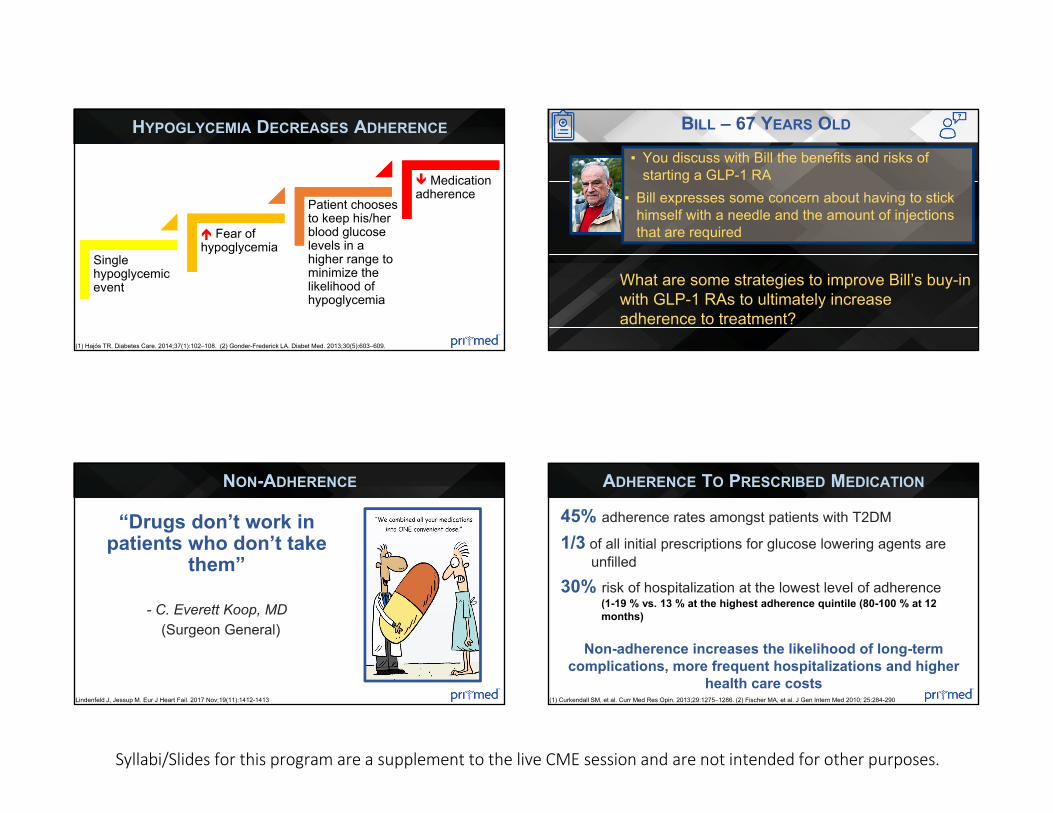
(1) Hajós TR. Diabetes Care. 2014;37(1):102–108. (2) Gonder-Frederick LA. Diabet Med. 2013;30(5):603–609.
HYPOGLYCEMIA DECREASES ADHERENCE
Single hypoglycemic event
Fear of hypoglycemia
Patient chooses to keep his/her blood glucose levels in a higher range to minimize the likelihood of hypoglycemia
Medication adherence
BILL – 67 YEARS OLD
▪ You discuss with Bill the benefits and risks of starting a GLP-1 RA
▪ Bill expresses some concern about having to stick himself with a needle and the amount of injections that are required
What are some strategies to improve Bill’s buy-in with GLP-1 RAs to ultimately increase adherence to treatment?
“Drugs don’t work in patients who don’t take
them”
- C. Everett Koop, MD (Surgeon General)
Lindenfeld J, Jessup M. Eur J Heart Fail. 2017 Nov;19(11):1412-1413
NON-ADHERENCE
45% adherence rates amongst patients with T2DM
1/3 of all initial prescriptions for glucose lowering agents are unfilled
30% risk of hospitalization at the lowest level of adherence (1-19 % vs. 13 % at the highest adherence quintile (80-100 % at 12 months)
Non-adherence increases the likelihood of long-term complications, more frequent hospitalizations and higher
health care costs(1) Curkendall SM, et al. Curr Med Res Opin. 2013;29:1275–1286. (2) Fischer MA, et al. J Gen Intern Med 2010; 25:284-290
ADHERENCE TO PRESCRIBED MEDICATION

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
► Discussions between patients and clinicians related to risk:benefit ratio is critical.
► Choose therapies which reduce risk of hypoglycemia and weight gain (hypoglycemia risk increases with duration of disease and age of patient)
► Hypoglycemia increases risk of mortality
► Consider use of drugs which may improve CV outcomes (death from MI, nonfatal MI, stroke, CHF) - and/or renal disease progression
► Decisions which are “patient-centered” are likely to improve clinical outcomes
► Injection therapies are NOT threatening and could improve ß-cell mass and function - THIS IS A GOOD THING!
Garcia-Perez LE, et al. Diabetes Ther. 2013;4:175–194
IMPROVING PATIENT ADHERENCE
Mody R, et al. Diabetes Jul 2018, 67 (Supplement 1) 1264-P.
LESS FREQUENT INJECTION = IMPROVED ADHERENCE
67%
51% 51%60%
38%
62%
PDC, mean(SD) in %
Adherence (%) Patients whodiscontinuedtherapy (%)
67%
51% 51%51%
32%
71%
PDC, mean(SD) in %
Adherence (%) Patients whodiscontinuedtherapy (%)
Dulaglutide Liraglutide Exenatide QW
PATIENT PRIORITIES FOR INJECTABLE AGENTS
Boegelund M, et al. Diabetes. 2015;64(suppl 1):A349 [abstract 1341-P].
4
1
2
3
4
5Will
ingn
ess
to P
ayW
illin
gnes
s to
Pay
Greater glycemic efficacy
Low risk of hypoglycemia
Weight loss (2-3 kg)
Avoid mixing (resuspension)
Fewer daily injections
Holst JJ, Vilsbøll T. Diabetes Obes Metab. 2013;15(1):3-14.
HOW TO SELECT GLP-1 RAS
PREFERENTIAL EFFECT ON…LONG-ACTING GLP-1 RAS DulaglutideLiraglutideExenatide QWSemaglutide
FASTINGPLASMA GLUCOSE
SHORT-ACTING GLP-1 RAS LixisenatideExenatide BID
POST-PRANDIALPLASMA GLUCOSE

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Medication Adverse Events Dosing
Shor
t-act
ing
Exenatide BID Nausea, vomiting, dyspepsia Start 5 mcg twice daily (1 hour before morning and evening meals), may increase to 10 mcg after 1 month
Lixisenatide Nausea, vomiting, diarrhea, headache
Start 10 mcg daily (1 h before 1st meal of day), may increase to 20 mcg daily after 14 days
Long
-act
ing
Liraglutide Nausea, vomiting, diarrhea, headache, dyspepsia, fatigue
Start 0.6 mg once daily, may increase to 1.2 mg after 1 week. Max dose 1.8 mg daily
Exenatide QW Nausea, diarrhea, headache, dyspepsia, vomiting 2 mg once weekly
Dulaglutide Nausea, diarrhea, vomiting Start 0.75 mg once weekly, may increase to 1.5 mg once weekly
Semaglutide Nausea, vomiting, diarrhea, constipation, abdominal pain
Start 0.25 mg once weekly, may increase to 0.5 mg once weekly. Max dose 1 mg per week
1. Byetta. Summary of Product Characteristics; 2. Lyxumia. Summary of Product Characteristics; 3. Victoza. Summary of Product Characteristics; 4. Marbury T et al. Diabetes 2014;63(Suppl.1):A260(1010-P); 5. Kapitza C et al. J Clin Pharm 2015;55:497–504; 6. Barrington et al. Diabetes Obes Metab 2011;13:434–438; 7. PI Tanzeum 8. Fineman M et al. Clin Pharmacokinet 2011;50:65–74; Ozempic prescribing information; Trulicity prescribing information.
FDA APPROVED GLP-1 RAS
*Albiglutide to be discontinued July 2018
-0.78
-1.5
0.08
-1
0.1
-0.79-0.96 -0.99
-0.71
-0.32
-1.5
-1.1
-1.8
-1.4
-2
-1.5
-1
-0.5
0
0.5
EXEBID
EXEQW PLB
LIRA1.8 mg PLB LIXI
EXEBID
DULA1.5 mg
DULA0.75mg SITA
SEMA0.5 mg
DULA0.75mg
SEMA1 mg
DULA1.5 mg
EFFICACY OF GLP-1 RAS ADDED TO METFORMIN
ΔH
bA1c
,%
P<0.001
P<0.01 P = NI P<0.001
P<0.0001P<0.0001
NI = non-inferior
(1) DeFronzo RA, et al. Diabetes Care. 2005;28(8):1092-1100; (2) Bergenstal RM, et al. Lancet. 2010;376:431-439. (3) Nauck M, et al. Diabetes Care. 2009;32(1):84-90. (4) Ahren B, et al. Diabetes Care. 2014;37(8):2141-2148. (5) Weinstock RS, et al. Diabetes Obes Metab 2015; 17:849. (6) Rosenstock J. Diabetes Care. 2013 Oct;36(10):2945-2951. (7) Pratley R, et al. Lancet Diabetes Endocrinol. 2018.
-1.25% -1.26% -1.33%
-1.09%
-1.50%
-1.30%
-1.08%
-0.63%
-1.60%
-1.40%
-1.20%
-1.00%
-0.80%
-0.60%
-0.40%
-0.20%
0.00%
ExenatideBID
Insulinglargine Liraglutide
Insulinglargine
ExenatideQW
Insulinglargine Dulaglutide
Insulinglargine
EFFICACY OF GLP-1 RAS VS BASAL INSULIN
ΔH
bA1c
,%
(1) Davies MJ, et al. Diabetes Obes Metab. 2009;11:1153-1162. (2) Russell-Jones D, et al. Diabetologia. 2009;52:2046-2055. (3) Diamant M, et al. Lancet. 2010;375:2234-2243.(4) Giorgino R, et al. Diabetes Care. 2015;38:2241-2249.
-3.24 -3.7-2.68
-1.53
-2.9
-4.3
-3-2.87-3.6 -3.57
-0.99
-3.61 -3.7
-6.5
LEAD-6 DURATION-1 DURATION-6 AWARD-1 AWARD-6 LIRA-LIXI SUSTAIN-7
p=0.0001
Baseline 93.1 93.0 102.0 102.0 90.9 91.7 96.0 97.0 94.4 93.8 102 101 Average 95Weight(kg)
Cha
nge
in W
eigh
t (kg
)
p=0.089
p=0.474
p<0.01p<0.01
p=0.022
GLP-1 RAS CAN LEAD TO WEIGHT LOSS
(1) Buse JB et al. Lancet. 2009;374:39–47 (LEAD-6). (2) Drucker DJ et al. Lancet. 2008;372:1240–50 (DURATION-1); (3) Buse JB et al. Lancet. 2013;381:117–24 (DURATION-6). (4) Wysham C et al. Diabetes Care. 2014;37(8):2159–67 (AWARD-1). (5) Dungan KM et al. Lancet. 2014; 384(9951):1349–1357 (AWARD-6). (6) Nauck M et al. Diabetes Care. 2016 Sep;39(9):1501-9. (7) Pratley R, et al. Lancet Diabetes Endocrinol. 2018 (SUSTAIN 7).
Liraglutide 1.8 mg
Exenatide 10 µg BID
Exenatide 2 mg QW
Dulaglutide 1.5 mg Semaglutide 1.0 mg
Lixisenatide
p<0.0001
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
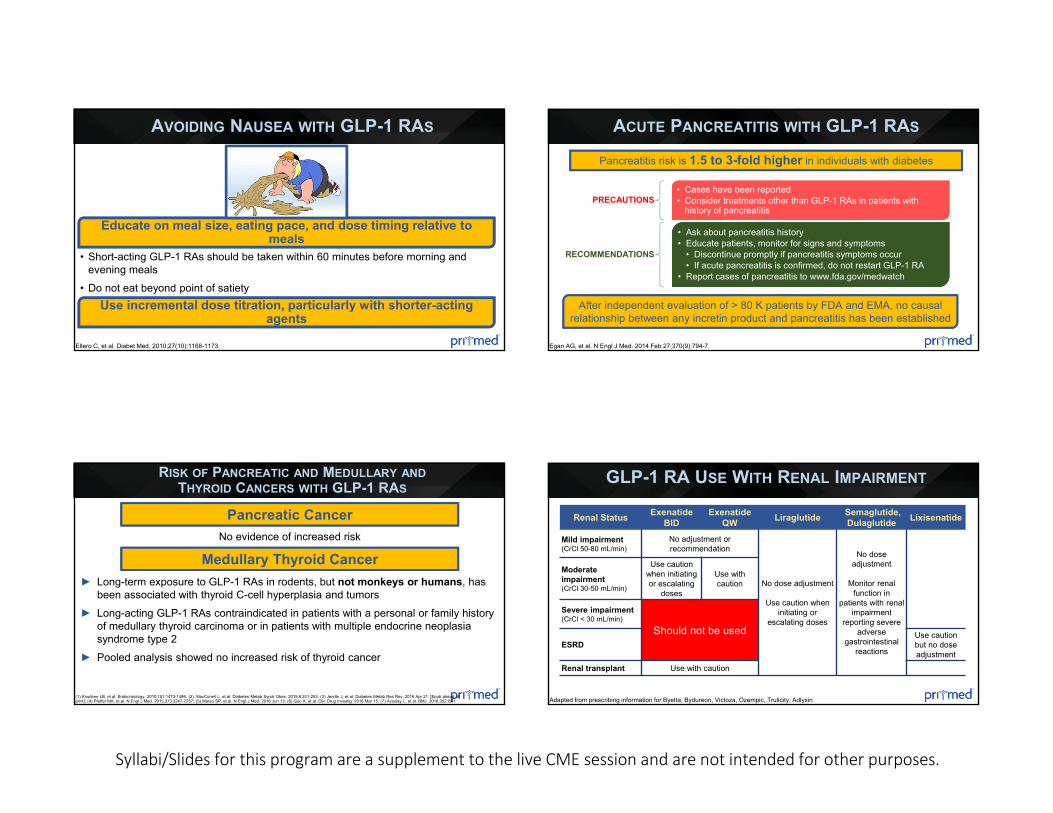
AVOIDING NAUSEA WITH GLP-1 RAS
Ellero C, et al. Diabet Med. 2010;27(10):1168-1173.
Educate on meal size, eating pace, and dose timing relative to meals
• Short-acting GLP-1 RAs should be taken within 60 minutes before morning and evening meals
• Do not eat beyond point of satietyUse incremental dose titration, particularly with shorter-acting
agents
ACUTE PANCREATITIS WITH GLP-1 RAS
Egan AG, et al. N Engl J Med. 2014 Feb 27;370(9):794-7.
Pancreatitis risk is 1.5 to 3-fold higher in individuals with diabetes
PRECAUTIONS• Cases have been reported• Consider treatments other than GLP-1 RAs in patients with
history of pancreatitis
RECOMMENDATIONS
• Ask about pancreatitis history• Educate patients, monitor for signs and symptoms
• Discontinue promptly if pancreatitis symptoms occur • If acute pancreatitis is confirmed, do not restart GLP-1 RA
• Report cases of pancreatitis to www.fda.gov/medwatch
After independent evaluation of > 80 K patients by FDA and EMA, no causal relationship between any incretin product and pancreatitis has been established
RISK OF PANCREATIC AND MEDULLARY ANDTHYROID CANCERS WITH GLP-1 RAS
(1) Knudsen LB, et al. Endocrinology. 2010;151:1473-1486; (2) MacConell L, et al. Diabetes Metab Syndr Obes. 2015;8:241-253; (3) Jendle J, et al. Diabetes Metab Res Rev. 2016 Apr 21. [Epub ahead of print]; (4) Pfeffer MA, et al. N Engl J Med. 2015;373:2247-2257; (5) Marso SP, et al. N Engl J Med. 2016 Jun 13. (6) Guo X, et al. Clin Drug Investig. 2016 Mar 15. (7) Azoulay L, et al. BMJ. 2016;352:i581
Pancreatic Cancer
Medullary Thyroid Cancer► Long-term exposure to GLP-1 RAs in rodents, but not monkeys or humans, has
been associated with thyroid C-cell hyperplasia and tumors► Long-acting GLP-1 RAs contraindicated in patients with a personal or family history
of medullary thyroid carcinoma or in patients with multiple endocrine neoplasia syndrome type 2
► Pooled analysis showed no increased risk of thyroid cancer
No evidence of increased risk
GLP-1 RA USE WITH RENAL IMPAIRMENT
Adapted from prescribing information for Byetta, Bydureon, Victoza, Ozempic, Trulicity, Adlyxin
Renal Status Exenatide BID
Exenatide QW Liraglutide Semaglutide,
Dulaglutide Lixisenatide
Mild impairment(CrCl 50-80 mL/min)
No adjustment or recommendation
No dose adjustment
Use caution when initiating or
escalating doses
No dose adjustment
Monitor renal function in
patients with renal impairment
reporting severe adverse
gastrointestinal reactions
Moderate impairment(CrCl 30-50 mL/min)
Use caution when initiating or escalating
doses
Use with caution
Severe impairment(CrCl < 30 mL/min)
Should not be usedESRD
Use caution but no dose adjustment
Renal transplant Use with caution
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
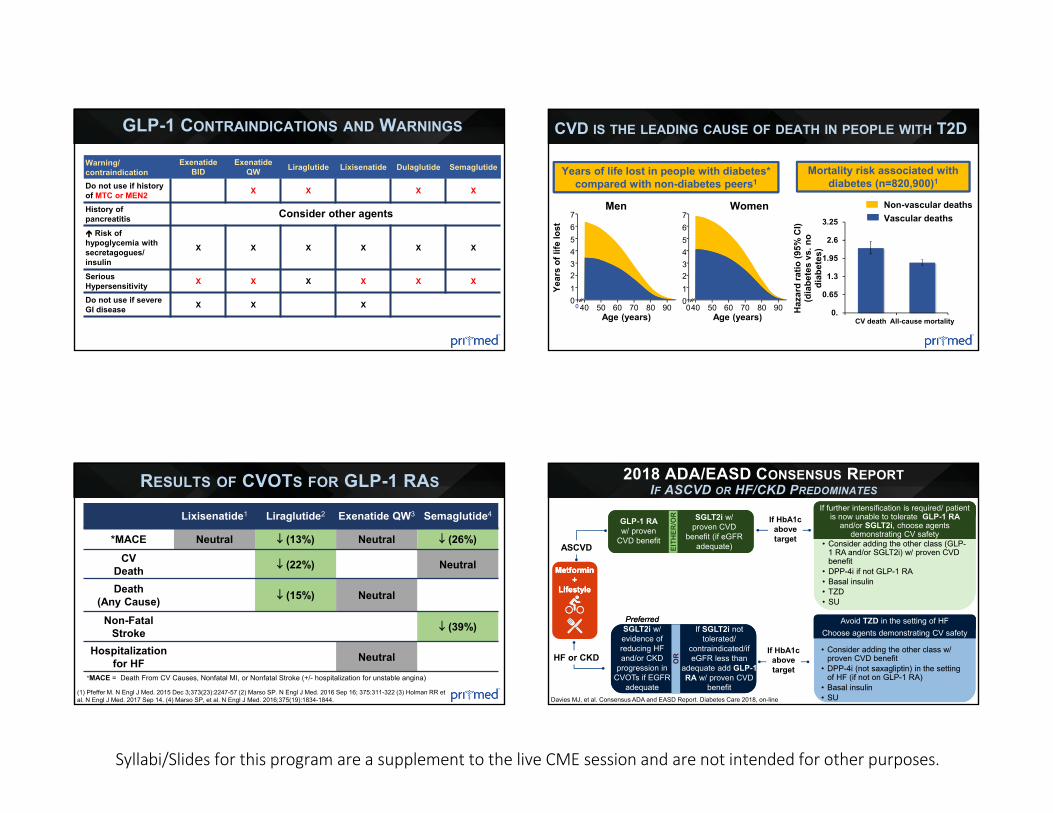
Warning/contraindication
Exenatide BID
Exenatide QW Liraglutide Lixisenatide Dulaglutide Semaglutide
Do not use if history of MTC or MEN2 X X X X
History of pancreatitis Consider other agents Risk of hypoglycemia with secretagogues/ insulin
X X X X X X
Serious Hypersensitivity X X X X X X
Do not use if severe GI disease X X X
GLP-1 CONTRAINDICATIONS AND WARNINGS
0.
0.65
1.3
1.95
2.6
3.25
CV death All-cause mortality
Haz
ard
ratio
(95%
CI)
(dia
bete
s vs
. no
diab
etes
)
CVD IS THE LEADING CAUSE OF DEATH IN PEOPLE WITH T2D
Mortality risk associated with diabetes (n=820,900)1
0
7
40 50 60 70 80 90Age (years)
Year
s of
life
lost 6
543210
76543210
Men
40 50 60 70 80 900Age (years)
Women Non-vascular deathsVascular deaths
Years of life lost in people with diabetes* compared with non-diabetes peers1
RESULTS OF CVOTS FOR GLP-1 RAS
Lixisenatide1 Liraglutide2 Exenatide QW3 Semaglutide4
*MACE Neutral (13%) Neutral (26%)CV
Death (22%) Neutral
Death (Any Cause) (15%) Neutral
Non-Fatal Stroke (39%)
Hospitalization for HF Neutral
*MACE = Death From CV Causes, Nonfatal MI, or Nonfatal Stroke (+/- hospitalization for unstable angina)
(1) Pfeffer M. N Engl J Med. 2015 Dec 3;373(23):2247-57 (2) Marso SP. N Engl J Med. 2016 Sep 16; 375:311-322 (3) Holman RR et al. N Engl J Med. 2017 Sep 14. (4) Marso SP, et al. N Engl J Med. 2016;375(19):1834-1844.
2018 ADA/EASD CONSENSUS REPORTIF ASCVD OR HF/CKD PREDOMINATES
Davies MJ, et al. Consensus ADA and EASD Report. Diabetes Care 2018, on-line
EITH
ER/O
REI
THER
/OR
GLP-1 RA w/ proven
CVD benefit
GLP-1 RA w/ proven
CVD benefit
SGLT2i w/ proven CVD
benefit (if eGFR adequate)
SGLT2i w/ proven CVD
benefit (if eGFR adequate)EI
THER
/OR
GLP-1 RA w/ proven
CVD benefit
SGLT2i w/ proven CVD
benefit (if eGFR adequate)
• Consider adding the other class w/ proven CVD benefit
• DPP-4i (not saxagliptin) in the setting of HF (if not on GLP-1 RA)
• Basal insulin• SU
Avoid TZD in the setting of HFChoose agents demonstrating CV safety
• Consider adding the other class w/ proven CVD benefit
• DPP-4i (not saxagliptin) in the setting of HF (if not on GLP-1 RA)
• Basal insulin• SU
Avoid TZD in the setting of HFChoose agents demonstrating CV safety
• Consider adding the other class (GLP-1 RA and/or SGLT2i) w/ proven CVD benefit
• DPP-4i if not GLP-1 RA• Basal insulin• TZD• SU
If further intensification is required/ patient is now unable to tolerate GLP-1 RA
and/or SGLT2i, choose agents demonstrating CV safety
• Consider adding the other class (GLP-1 RA and/or SGLT2i) w/ proven CVD benefit
• DPP-4i if not GLP-1 RA• Basal insulin• TZD• SU
If further intensification is required/ patient is now unable to tolerate GLP-1 RA
and/or SGLT2i, choose agents demonstrating CV safety
Metformin +
Lifestyle
Metformin +
Lifestyle
Metformin +
Lifestyle
ASCVD
OR
OR
PreferredSGLT2i w/ evidence of reducing HF and/or CKD
progression in CVOTs if EGFR
adequate
If SGLT2i not tolerated/
contraindicated/if eGFR less than
adequate add GLP-1 RA w/ proven CVD
benefit
If SGLT2i not tolerated/
contraindicated/if eGFR less than
adequate add GLP-1 RA w/ proven CVD
benefitO
R
PreferredSGLT2i w/ evidence of reducing HF and/or CKD
progression in CVOTs if EGFR
adequate
If SGLT2i not tolerated/
contraindicated/if eGFR less than
adequate add GLP-1 RA w/ proven CVD
benefit
HF or CKD
If HbA1c above target
If HbA1c above target
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
SUMMARY
► Long-acting GLP-1 RAs preferred due to patient convenience► Reduction in HbA1c is greater with the longer-acting GLP-1 RAs► Avoid combination therapy with GLP-1 RAs and DPP-4 inhibitors as
there are no proven additive glucose-lowering effects► The risk of hypoglycemia is small with GLP-1 RAs (as compared to
insulin, sulfonylureas, glinides)► Select GLP-1 RAs with consideration of renal impairment creatinine /
eGFR► Consider selection of GLP-1 RAs based on comparative effectiveness
to reduce glycemia and weight, as well as impact on CV risk


















