
EST 18 Day 1 Track 1 Session 1 Sax ID Update
13
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes. 9:45 - 10:45am 2018 Infectious Diseases Update SPEAKER Paul E. Sax, MD Infectious Diseases Update Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women’s Hospital Professor of Medicine Harvard Medical School ID Update • Case‐based review of common ID problems faced by clinicians in the outpatient setting • Urinary tract infections • Skin and soft tissue infections • Respiratory tract infections • Prevention of herpes zoster • Treatment of hepatitis C Case Presentations Participation required!
Transcript of EST 18 Day 1 Track 1 Session 1 Sax ID Update

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
9:45 - 10:45am
2018 Infectious Diseases UpdateSPEAKERPaul E. Sax, MD Infectious Diseases Update
Paul E. Sax, M.D.Clinical Director, Division of Infectious Diseases
Brigham and Women’s HospitalProfessor of MedicineHarvard Medical School
ID Update
• Case‐based review of common ID problems faced by clinicians in the outpatient setting
• Urinary tract infections• Skin and soft tissue infections• Respiratory tract infections• Prevention of herpes zoster• Treatment of hepatitis C
Case PresentationsParticipation required!

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
24 y.o. female with dysuria, frequency
•No systemic symptoms• Two prior UTIs that she can remember – received TMP‐SMX once, developed total body rash
•PE negative for fever or flank pain
Therapy for Lower UTI in Women
• Optimal therapy for UTI will not eradicate non‐pathogenic vaginal flora (in particular, lactobacillus)
• Over one‐third of bacterial strains causing UTI resistant to amp and amox; 10‐22% to TMP‐SMX
• 2011: Guidelines on “preferred” regimens
Clinical Infectious Diseases 2011; 52:e103-e120
Preferred Initial Regimens for UTI
• Nitrofurantoin 100 mg BID x 5 days• TMP/SMX DS 1 PO BID x 3 days• Fosfomycin 3 gm as a single dose• 2nd Line: Amox‐clav, cefdinir, cefaclor, cefpodoxime• Not recommended
• Fluoroquinolones – highly effective, but may lead to “collateral damage”• Amoxicillin and ampicillin
Clinical Infectious Diseases 2011; 52:e103‐e120
• Randomized clinical trial of nitrofurantoin 100 mg TID X 5 days vs fosfomycin 3 gm X 1
• Primary endpoint: clinical response at day 28• N=513, median age 44• Clinical response to nitrofurantoin (70%) significantly better than fosfomycin (58%); microbiologic response also favored nitrofurantoin
• Results raise questions about usefulness of fosfomycin for uncomplicated UTI
Huttner A, et al. JAMA 2018.

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Therapy of Acute Pyelonephritis
• Need antibiotics with high tissue and blood concentration – not nitrofurantoin or fosfomycin
• Oral options: TMP‐SMX and ciprofloxacin• Parenteral options: ceftriaxone, gentamicin, and ertapenem
• For susceptible strains, ciprofloxacin for 7 days recommended
• Superior to TMP‐SMX for 14 days• Non‐inferior to ciprofloxacin for 14 days
Clinical Infectious Diseases 2008;47:1150‐8; Clinical Infectious Diseases 2011; 52:e103‐e120; Lancet 2012;380:484‐490. N Engl J Med 2018; 378:48‐59.
28 y.o. man with “spider bite”
• Noted painful nodules approximately 1 week ago• Started himself on oral cephalexin that happens to be left over in his medicine cabinet
• Worried it might be a spider bite – did not actually see a spider• Two days later, he is no better: T = 100.8; two nodules noted (buttock, inner thigh), largest 5 x 8 cm with surrounding erythema and purulent drainage
Non‐prescription Antibiotic Use is Common
• Survey of 400 patients in 2 primary care settings in USA
• 40% willing to take antibiotics without prescription
• 5% had done so within the past year• 14% had antibiotics stored at home for this purpose
• 20% had obtained antibiotics from friend or relative
• Respiratory, GI, and GU symptoms the most common indication
Zoorob R et al., Antimicrob Agents Chemother 2016.
Skin and Soft‐tissue Infections
• Most community‐acquired cases caused by Staph aureus, beta‐hemolytic streptococci
• Staph: abscesses• Strep: cellulitis, lymphangitis, erysipelas
• Special cases:• DM with ulcer: GNR, anaerobes – but also staph, strep• Bites: P. multocida, Capnocytophaga spp, mixed flora• Water: Aeromonas, Vibrio spp. (esp. with liver disease), M. marinum• Thorns: Sporothrix schenkii
Open Forum Infectious Diseases 2016; doi.org/10.1093/ofid/ofv181.
Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
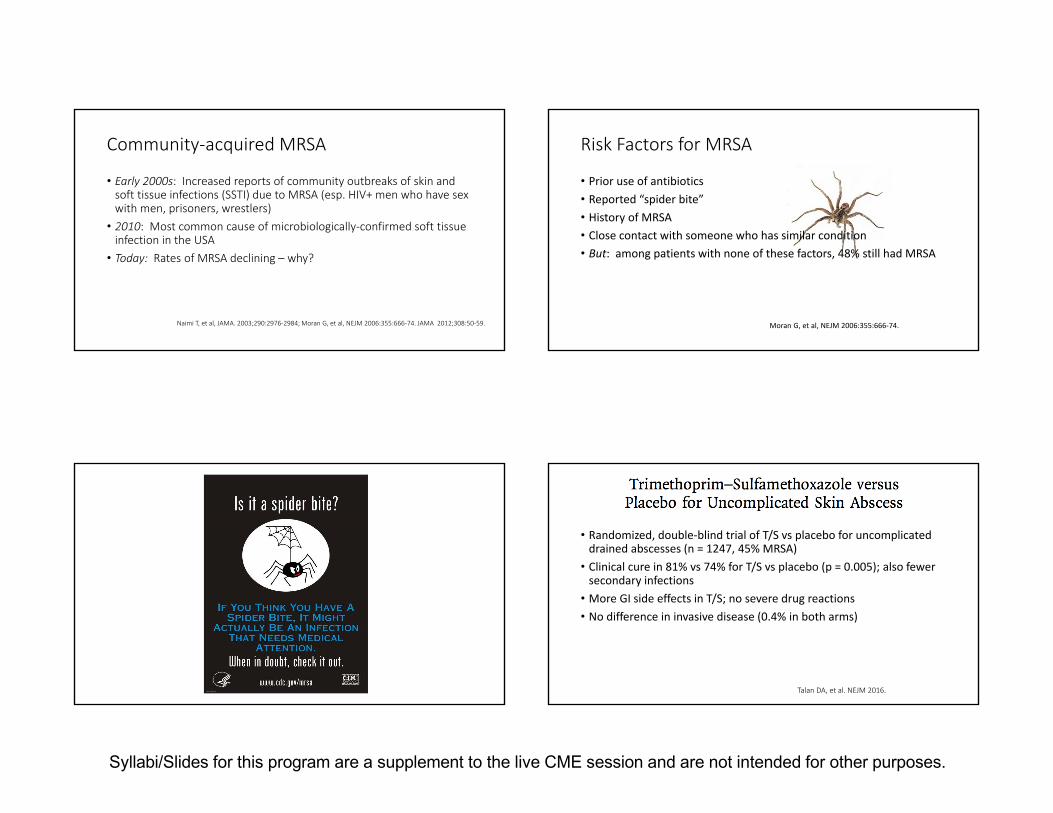
Community‐acquired MRSA
• Early 2000s: Increased reports of community outbreaks of skin and soft tissue infections (SSTI) due to MRSA (esp. HIV+ men who have sex with men, prisoners, wrestlers)
• 2010: Most common cause of microbiologically‐confirmed soft tissue infection in the USA
• Today: Rates of MRSA declining – why?
Naimi T, et al, JAMA. 2003;290:2976‐2984; Moran G, et al, NEJM 2006:355:666‐74. JAMA 2012;308:50‐59.
Risk Factors for MRSA
• Prior use of antibiotics• Reported “spider bite”• History of MRSA• Close contact with someone who has similar condition• But: among patients with none of these factors, 48% still had MRSA
Moran G, et al, NEJM 2006:355:666‐74.
• Randomized, double‐blind trial of T/S vs placebo for uncomplicated drained abscesses (n = 1247, 45% MRSA)
• Clinical cure in 81% vs 74% for T/S vs placebo (p = 0.005); also fewer secondary infections
• More GI side effects in T/S; no severe drug reactions• No difference in invasive disease (0.4% in both arms)
Talan DA, et al. NEJM 2016.

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Summary: Approach to Skin Abscess
• Any patient with purulent SSTI (furuncles, abscesses) may or may not have MRSA• Obtain cultures for confirmation – can even do on dry nodules• Low threshold for incision and drainage• Empiric oral treatment: TMP‐SMX, or doxycycline/minocycline, or clindamycin (rising resistance – 40%), or linezolid
• IV options include vancomcyin, linezolid, daptomycin, telavancin, oritavancin, dalbavancin
• Antibiotics strongly recommended for large abscesses (5 cm), systemic illness, immunocompromised hosts, diabetes, face/hands/genitalia
NEJM 2008; 359:1063‐1067; Liu Clin Infect Diseases 2011; N Engl J Med 2014; 370:1039‐1047
Linezolid – Now an Option for Outpatient Care• Active against staph (including MRSA) and strep• Excellent oral absorption and tissue penetration• Dose: 600 mg twice daily• Adverse effects – main risk factor is duration of therapy
• Asthenia (the “blahs”)• Cytopenias• Neuropathy – peripheral and optic (may be irreversible)
• Drug interactions: Potential for serotonin syndrome when co‐administered with SSRIs
• Price down substantially due to generics – but shop around!
Price Range for 2 Weeks of Linezolid
Goodrx.com, accessed October 2018.
!!!
Recurrent MRSA is a
Very Challenging Problem!

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Very Recurrent MRSA: Strategies for Prevention• Topical antibiotics: Mupirocin nasal ointment anterior nares BID
• Systemic antibiotics: TMP‐SMX 1 DS BID, +/‐ rifampin 300 mg PO BID – all for 7‐10 days
• Not endorsed in latest guidelines
• Household contacts (including pets) cultured/treated
• Local measures• COVER WOUNDS• Bathe for 10 minutes; 1 tsp bleach/gallon of water
• Using a bath sponge, lather armpits, groin, anus, and under the breasts with chlorhexidine topical antiseptic (Hibiclensscrub) after draining bath water
• Shower Hibiclens off
• Frequent laundering of towels, sheets, clothing
Daum RS, et al. N Engl J Med 2007;357:380; Liu Clin Infect Dis 2011.
“Never, ever, think outside the box.”
47 y.o. man with 7 days of cough
• Previously‐healthy non‐smoker, well until 1 week prior when he developed sore throat, rhinorrhea
• Now with 3 days of progressive cough, in AM productive of thick sputum, “yellow‐green”; requests antibiotics
• PMHx: PCN allergy. Exam: normal
“Don’t forget to take a handful of our complimentary antibiotics on the
way out.”

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Antibiotics for URIs and Patient Satisfaction
“Few physicians achieved even the 50th percentile of satisfaction while maintaining low rates of antibiotic prescribing. To reach the top quartile, a physician had to prescribe antibiotics at least half the time; almost all physicians above the 90th percentile had a rate of antibiotic prescribing greater than 75%.”
Martinez KA, et al. JAMA Int Med 2018.
NYC Subway Advertisement for
Capsule Pharmacy, 2017.
Antibiotic Use in Office Setting Increases Risk of Resistance
Costelloe, C. et al. BMJ 2010;340:c2096
Beware “Pirate” bacteria!

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Selected Conditions Linked to Alteration of the Human Microbiome• Obesity• Type II diabetes• Asthma• Food allergies• Esophageal reflux• Gluten sensitivity
Choose Your
Language Carefully! Survey of 459 patients regarding treatment
dissatisfaction if no antibiotic given for “cough with grey phlegm for 1 week”, and illness called:• “Bronchitis” 26%• “Viral illness” 17%• “Cold” 13%
J Am Board Fam Pract. 2005 Nov-Dec;18(6):459-63.
Antibiotic Prescribing for Bronchitis is Common
JAMA. 2014;311(19):2020-2022. Llor C et al. BMJ 2013;347:bmj.f5762
• Amox‐clav vs ibuprofen vs placebo for “uncomplicated cough illness•No significant difference between arms•One week after entry, 65% still had frequent cough

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Education of Providers Reduces Antibiotic Use for RTI• Randomized intervention in 12 Family Practice clinics in Quebec• Intervention: 2‐hour on‐line tutorial followed by 2‐hour on‐site workshop – encouraged “shared decision making” with patients
• Post intervention Abx use: 27.2% vs 52.2% (RR 0.5 (95% CI 0.3‐0.7)• No difference in clinical outcomes
Legare F, et al CMAJ 2012.
Legare F, et al CMAJ 2012 (online appendix).
Can the Lab Help?
• C‐reactive protein – non‐specific marker of inflammation, rises more with bacterial infection
• Procalcitonin• Bacterial infection increases levels, while interferon gamma blocks production
• Effect is rapid (within hours), and half‐life is short
• Rapid viral diagnostic tests• Studies support the use of these tests in reducing antibiotic exposure – but point‐of‐care availability and rapid turnaround are critical for implementation
Cals JW et al. Ann Fam Med 2010; Rhee C et al OFID 2016; Keske S, et al Eur J Clin Microbiol Infect Dis. 2018.
74 y.o. man with concerns about zoster vaccine• Received original zoster vaccine live (ZVL, Zostavax) at age 65, no side effects
• More recently, received first dose of recombinant zoster vaccine (RZV, Shingrix) – developed moderate arm pain, malaise, and low‐grade fever for 48 hours
• Now due for second dose – he has concerns that side effects will be worse

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Recombinant Adjuvanted Subunit Zoster Vaccine
Advantages• More effective in preventing both zoster and post‐herpetic neuralgia
• Efficacy wanes less over time• Not a live‐virus vaccine• Broader target population – age > 50 in ACIP recommendations
Disadvantages• Two doses required, 2‐6 months apart
• More minor side effects• Less long term safety data• Widespread shortages
https://www.cdc.gov/vaccines/vpd/shingles/hcp/shingrix/recommendations.html
Recombinant Zoster Vaccine (RZV): Common Questions Answered Here!• Who should get it?
• Essentially all patients over 50
• Is there an upper age limit?• No … but …
• How long after ZVL should one wait to give RZV?• At least 2 months
• What do you do if a patient is due for second dose, and you don’t have it?
• Give it when available – no need to restart series
• Does a reaction to the first dose predict a bad reaction to the second?
• No!
• What if someone never had chicken pox?http://www.immunize.org/askexperts/experts_zos.asp
Acceptable Evidence of Varicella Immunity
• US‐born before 1980• Documentation of 2 doses of varicella vaccine given at least 28 days apart
• Post‐vaccination serologic testing not recommended in any group; unreliable correlate with protection
• History of varicella or herpes zoster based on physician diagnosis
• Laboratory evidence of immunity• Laboratory confirmation of disease
MMWR 2007;56:RR‐4.
58 year old man newly diagnosed with hepatitis C• Underwent testing for the first time as recommended by his primary care clinician
• Likely acquired HCV during a period of cocaine use in the 1980s• Asymptomatic; physical examination normal• Labs show mild elevation of ALT/AST, otherwise normal• HCV RNA: 2.8 million copies/mL

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
HCV Screening Guidelines
• Injection drug use – even once• Received blood transfusion prior to 1992• Health care workers with occupational exposures
• Born to HCV‐infected mothers• Sex partners of HCV‐infected persons• HIV‐positive persons• Anyone born between 1945‐1965 (65% of HCV infections)
http://www.cdc.gov/mmwr/preview/mmwrhtml/rr6104a1.htm, Aug 2012
Recommendations on HCV Testing
No HCV antibody detected
HCVantibody
STOP*
ReactiveNonreactive
Additional testing as appropriate**
Link to care
Current HCV infection
No current HCV infection
Not detected DetectedHCVRNA
* For persons who might have been exposed to HCV within the past 6 months, testing for HCV RNA or follow-up testing for HCV antibody is recommended; for persons who are immunocompromised, testing for HCV RNA can be considered. ** To differentiate past, resolved HCV infection from biologic false positivity for HCV antibody, testing with another HCV antibody assay can be considered. Repeat HCV RNA testing if the
person tested is suspected to have had HCV exposure within the past 6 months or has clinical evidence of HCV disease, or if there is concern regarding the handling or storage of the test specimen. CDC. MMWR. 2013;62(18).
Once HCV Antibody Positive, Then What?
• History – risk factors, complications, contraindications to treatment, prior therapy
• Physical exam, with attention to stigmata of liver disease• Labs: CBC, AST, ALT, Alk Phos, Tbili, Albumin, coagulation studies, HCV RNA, HIV Ab
• If HCV RNA positive:• HCV genotype• Assess degree of liver fibrosis
• Make sure HAV and HBV vaccines are up to date!
Fibrosis Staging in HCV
SVR = sustained viral responseGhany MG, et al. Hepatology. 2009;49(4):1335-1374; AASLD/IDSA. Recommendations for Testing, Managing, and Treating HCV. www.hcvguidelines.org. Accessed 7/18/18.Images courtesy of Zachary Goodman, MD.
METAVIR Scale
Score F0 F1 F2 F3 F4Fibrosis (scarring)
No damageMild
Portal fibrosis without septa
Moderate
Portal fibrosis with rare septa
Advanced
Numerous septa, not cirrhosis
Severe
Cirrhosis
Determining fibrosis level is important as it may affect treatment regimen, duration of treatment, and determines the need for HCC screening post-cure

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
Liver Fibrosis Assessment: Alternatives to Biopsy• Eyeball test: PLT (<160K), albumin, PT• AST to platelet ratio index (APRI)
• (AST elevation/platelet count) x 100• APRI > 0.7 strongly suggests F2 or higher; > 1.0 suggests F4
• FibroSure, FibroTest, others• Liver elastography (FibroScan)
• No food for 3‐4 hours pre‐procedure• Takes 10‐15 minutes• Offered at many medical centers, some liver/ID clinics
HCV Treatment Can Seem Complex …
… But It Has Become Incredibly Simple!
• Almost all newly diagnosed patients can be treated with either of these two strategies
• Sofosbuvir/velpatasvir (SOF/VEL, Epclusa) – one pill daily for 12 weeks• Glecaprevir/pibrentasvir (GLE/PIB, Mavyret) – three pills daily for 8 (sometimes 12) weeks
• Both pan‐genotypic• Both highly effective (>95% cured)• Both much less expensive than earlier treatment options
www.hcvguidelines.org
Practical Issues with SOF/VEL and GLE/PIB
• SOF/VEL• Important drug interactions – amiodarone, PPIs, rifamycins, efavirenz, carbamazepine, phenytoin
• Cannot use with eGFR < 30
• GLE/PIB• Avoid in patients with history of decompensated cirrhosis• Extend treatment to 12 weeks if compensated cirrhosis• Important drug interactions – simvastatin, rifamycins, carbamazepine, phenytoin, efavirenz, HIV protease inhibitors
www.hcvguidelines.org

Syllabi/Slides for this program are a supplement to the live CME session and are not intended for other purposes.
ID Update: Summary
• Nitrofurantoin more effective than fosfomycin for lower UTI
• TMP/SMX preferred for purulent skin infections, along with I and D
• Growing data support the importance of limiting antibiotic use
• Resistance• Alteration in the microbiome• Shared decision making and passive education are effective strategies to reduce antibiotic use
• Recombinant zoster vaccine is much more effective –but also more reactogenic – than the live virus vaccine
• HCV treatment – simple and highly effective











![Pavane [opus 50] - Free-scores.com...Violin Flute 1 Flute 2 Alto Sax. 1 Alto Sax. 2 Tenor Sax. 1 Tenor Sax. 2 Baritone Sax. Trumpet in B 1 Trumpet in B 2 Trombone 1 Trombone 2 Acoustic](https://static.fdocuments.us/doc/165x107/6102dad8c239672c8f179d8d/pavane-opus-50-free-violin-flute-1-flute-2-alto-sax-1-alto-sax-2-tenor.jpg)






