
ESSENTIAL MEdIcINES MONITOR - World Health Organization€¦ · standardized asthma management ......
10
sthma is one of the world’s most common chronic diseases, with an estimated 300 million people worldwide currently suffering from it. Asthma kills approximately 250 000 people every year (1). Although asthma cannot be cured, it can be treated and managed effectively. e severity of the condition can be dramatically reduced and a person’s quality of life can be significantly improved. Asthma has been recognised as a major global public health problem. Managing asthma is one of the objectives defined in the WHO Plan for Non-Communicable Diseases 2008-2013, (2) international guidelines (1) exist and selected medicines are in the WHO Model List of Essential Medicines. However, in low- and middle-income countries, where the majority of the world’s asthmatics live, most cases of asthma go undiagnosed, untreated or mistreated. By causing unnecessary disability and expense, asthma is significantly increasing the poverty of individuals and countries. People with asthma are less able to work or look aſter their families. Children with asthma are likely to miss much of their primary education. Emergency visits, hospitalization and inappropriate treatments are a huge financial drain on struggling health systems. Access to essential asthma medicines WHO’s 17th Model List of Essential Medicines published in 2011 (3) includes affordable inhaled corticosteroids (e.g. beclometasone 100µg HFA) and bronchodilators (e.g. salbutamol 100µg HFA). A standardized asthma management strategy (4) using these medicines and adapted for low- and middle- income countries has been clearly demonstrated to be cost-effective. So why aren’t all countries using essential asthma medicines? The main barrier is access – poor availability and affordability of these medicines. For example, beclometasone is not available in many low-income countries. Where it is available, its price is almost always unnecessarily high. Neither health services nor patients can afford it. The Asthma Drug Facility In response to this situation, the International Union Against Tuberculosis and Lung Disease (e Union) created the Asthma Drug Facility (ADF). e ADF’s mission is Access to essential asthma medicines: the response of the Asthma Drug Facility = Cécile Macé, Karen Bissell, Nils E. Billo. A Learn more about the work of the Asthma Drug Facility in combating one of the world’s most common chronic diseases We look at a Chinese intervention project to improve rational use of antibiotics in surgical practice Contact us at: [email protected] IN THIS ISSUE: MONITOR Issue 5 (August 2011) ESSENTIAL MEDICINES Cécile Macé Karen Bissell Nils E. Billo
Transcript of ESSENTIAL MEdIcINES MONITOR - World Health Organization€¦ · standardized asthma management ......

sthma is one of the world’s most common chronic diseases, with an estimated 300 million
people worldwide currently suffering from it. Asthma kills approximately 250 000 people every year (1). Although asthma cannot be cured, it can be treated and managed effectively. The severity of the condition can be dramatically reduced and a person’s quality of life can be significantly improved. Asthma has been recognised as a major global public health problem. Managing asthma is one of the objectives defined in the WHO Plan for Non-Communicable Diseases 2008-2013, (2) international guidelines (1) exist and selected medicines are in the WHO Model List of Essential Medicines.
However, in low- and middle-income countries, where the majority of the world’s asthmatics live, most cases of asthma go undiagnosed, untreated or mistreated. By causing unnecessary disability and expense, asthma is significantly increasing the poverty of individuals and countries. People with asthma are less able to work or look after their families. Children with asthma are likely to miss much of their primary education. Emergency visits, hospitalization and inappropriate treatments are a huge financial drain on struggling health systems.
Access to essential asthma medicinesWHO’s 17th Model List of Essential Medicines published in 2011 (3) includes affordable inhaled corticosteroids (e.g. beclometasone 100µg HFA) and bronchodilators
(e.g. salbutamol 100µg HFA). A standardized asthma management strategy (4) using these medicines and adapted for low- and middle-income countries has been clearly demonstrated to be cost-effective. So why aren’t all countries using essential asthma medicines? The main barrier is access – poor availability and affordability of these medicines. For example, beclometasone is not available in many low-income countries. Where it is available, its price is almost always unnecessarily high. Neither health services nor patients can afford it.
The Asthma Drug FacilityIn response to this situation, the International Union Against Tuberculosis and Lung Disease (The Union) created the Asthma Drug Facility (ADF). The ADF’s mission is
Access to essential asthma medicines: the response of the Asthma Drug Facility = Cécile Macé, Karen Bissell, Nils E. Billo.
A
Learn more about the work of the Asthma Drug Facility in combating one of the world’s most common chronic diseases We look at a Chinese intervention project to improve rational use of antibiotics in surgical practice
Contact us at: [email protected]
I N T H I S I S S U E :
MONITORIssue 5 (August 2011)
E S S E N T I A L M E d I c I N E S
cécile Macé Karen Bissell Nils E. Billo

2 E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
to provide access to quality assured essential asthma medicines for low- and middle-income countries. The ADF is a procurement mechanism that obtains reduced prices for quality assured products. These low prices mean substantial savings for patients and public health systems. The ADF concept drew many lessons from the experiences of the Global Drug Facility, which has made tuberculosis drugs widely accessible and affordable, and also from the UN/WHO Prequalification Programme.
Quality assurance The Prequalification Programme – a UN programme, managed by WHO - comprehensively evaluates the quality, safety and efficacy of selected priority medicines, mainly antiretrovirals, antimalarials and antituberculosis medicines. (5) It does not currently evaluate asthma medicines. Therefore, the ADF had to take on the responsibility for assuring the quality of the asthma medicines it procures.
The ADF developed its own system of quality assurance (QA) based on current WHO standards. Three pharmacist consultants with recognized expertise in QA and experience in low-income settings were hired to write Standard Operating Procedures and to conduct the first qualification process.
The ADF QA system is based on international standards: WHO Model Quality Assurance
Sys tem for Pro c urement Agencies (6)
WHO norms and standards for the quality, safety and efficacy of medicines (7)
Internationally recognized pharmacopoeias – British, European, US, International Pharmacopoeia (WHO).
The system is also based on regulatory requirements for HFA inhalers in highly regulated countries. It should be noted, however, that the ADF found that some of the specifications in the regulatory requirements were not yet clearly enough defined.
The ADF created Standard Operating Procedures to cover key operations, such as: definitions and tools for evaluating and qualifying manufacturers and products; publication of Expressions of Interest; selection of auditors; audits and technical visits of manufacturing sites and related reporting; general procedures for the qualification process; preshipment inspection; and quality control.
The ADF’s qualification process has two steps:1. Assessment of the manufacturer
and the manufacturing site2. Assessment of each product.
The process involves qualifying a “product/manufacturing site pair”. The “pair” refers to a specified product manufactured at a specified site according to accepted specifications. The exact specifications of the qualified product are recorded on an “ADF Product Specification Sheet”. The ADF uses this formal record to check that manufacturers continue throughout their contract to comply with the documentation they submitted during the qualification process.
The ADF QA system also includes ongoing quality control and monitoring. All ADF orders are subject to pre-shipment inspections. Random quality control checks are performed by an international independent laboratory on samples taken after delivery to ADF clients. Qualification of manufacturing sites and products is valid for two years. During this time, the ADF pharmacist may make follow-up visits to check on various aspects of quality; for example, that manufacturing batch records conform to ADF specifications.
ProductPrimary supplier
(country)Price per unit FCA
(Euro)
Beclometasone 100µg/puff 200 doses, HFA inhaler
Beximco(Bangladesh) 1.07
Salbutamol 100µg/puff200 doses, HFA inhaler
Beximco(Bangladesh) 0.83
Budesonide 200µg/puff 200 doses, HFA inhaler
cipla/Medispray(India) 2.69
Fluticasone 125µg/puff120 doses, HFA inhaler
cipla/Goa(India) 3.23
To these prices, add costs of transport, insurance, preshipment inspection, 10% fees for AdF services (including random quality control)2009 MSH Price Indicator (Supplier Lowest Prices): Beclometasone 100µg: US$3.09= €2.24; Salbutamol 100µg: US$1.36= €0.99
Table 1. ADF product prices for 2010

3E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
Lower pricesThe ADF keeps prices down by organizing regular tenders based on yearly estimated volumes. The tenders are restricted, i.e. only product/manufacturing site pairs qualified by the ADF are able to make submissions. The outcome of the tender determines which products will be supplied by the ADF. Long-term contracts are established with the manufacturers.
Benefits at country level Benin and El Salvador were the first two countries to receive deliveries of asthma inhalers purchased through the ADF. By ordering through the ADF, the cost of the medicines for treating asthma dropped by nearly half in these two countries. For example, in Benin, one CFC-free (HFA) inhaler of beclometasone 100µg now costs a patient around 1400 CFA francs or 2.13 euros. In El Salvador, the same inhaler now costs the Ministry of Health only 1.59 euros. More recently, Kenya, Sudan and Burundi received also their first delivery from ADF. Burundi is the first country to purchase asthma
inhalers through the ADF using funds received from the Global Fund to Fight AIDS, Tuberculosis and Malaria to help them implement the Practical Approach to Lung Health (PAL) strategy.
Previously, the lowest cost in Benin for treating a patient with severe asthma was 79 euros per year. By ordering through the ADF, this cost has been reduced to 48 euros. In El Salvador, the savings per patient are even more dramatic – the cost has reduced from 83 to 35 euros per year.
The final cost of the medicines purchased through the ADF varies from country to country due to differences in transportation costs, importation taxes, customs clearance costs and other local factors.
All countries purchased through the ADF not only to obtain inhalers, but also to improve their management of asthma. In addition to the ADF procurement mechanism, The Union offers a technical package for improving the management of
asthma in the general health services. It contains training materials, an information system and a technical guide to help them provide quality services.
ConclusionLow- and middle-income countries now have an easily accessible source of affordable asthma medicines through the ADF. This removes one major barrier to the implementation of effective asthma programmes and integrated approaches to respiratory health (such as the Practical Approach to Lung Health Strategy) (8). With affordable medicines and standardized case management of asthma, countries have the potential to improve the quality of life of people with asthma and to make huge cost savings for their health systems, patients and communities. This model could also be applied to the essential medicines used for the management of other noncommunicable diseases, in particular respiratory diseases, such as chronic obstructive pulmonary disease. n
Product
Price per unit for the NTP in Benin
Price per unit for
the patient in Benin*
Price per unit for the MoH
in El Salvador
Price per unit for
the patient in El
Salvador**
Price per unit for KAPTLD in Kenya
Price per unit for
patient in Kenya***
Price per unit for Epi-Lab in Sudan
Price per unit for
patient in Sudan****
Beclometasone 100µg/puff, 200 doses, HFA inhaler
€1.90 €2.13 €1.59 For free €1.60 €1.84 €1.63 €1.93
Salbutamol 100µg/puff, 200 doses, HFA inhaler €1.50 €1.68 €1.23 For free €1.25 €1.44 – –
* Benin has a 12% local margin and a revolving fund for asthma medicines ** Paid by the Ministry of Health (MoH)***15% margin applied by the Kenya Association for Prevention of Tuberculosis and Lung diseases (KAPTLd)**** 18% margin applied in SudanHFA = HydrofluoroalkanePrices in Euros
Table 2. Analysis of prices for ADF’s first deliveries

4 E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
References1. GINA Report, Global Strategy
for Asthma Management and Prevention, 2009.
2. 2008/2013 Action plan for the global strategy for the prevention and control of noncommunicable diseases. Geneva, World Health Organization, 2009. Available at: http://www.who.int/nmh/publications/9789241597418/en/index.html
3. WHO Model List of Essential Medicines, 17th List, March 2011. Available at http://www.who.int/medicines/publications/essentialmedicines/Updated_sixteenth_adult_list_en.pdf
4. http://www.theunion.org/index.php/en/resources/scientific-publications/lung-health
5. WHO Prequal i f icat ion of Medicines Programme web site: http://apps.who.int/prequal/
6. A Model Quality Assurance System for Procurement Agencies. Geneva, World Health Organization, 2007WHO/PSM/PAR/2007.3. Available at: http://www.who.int/medicines/publications/ModelQualityAssurance.pdf
7. WHO Expert Committee on Specifications for Pharmaceutical Preparations web site available at: http://apps.who.int/medicinedocs/fr/cl/CL7.6/clmd,50.html
8. Practical Approach to Lung Health (PAL). Geneva, World Health Organization, 2005 WHO/HTM/TB/2005.351, WHO/NMH/CHP/CPM/CRA/05.3. Available at: http://whqlibdoc.who.int/hq/2005/WHO_HTM_TB_2005.351.pdf
Cécile Macé, Pharmacist, ADF Coordinator, The Union; Karen Bissell, ADF Deputy Coordinator, The Union; Nils E. Billo, ADF Director, Executive Director, The Union. For more information contact: [email protected] and visit: http://www.GlobalADF.org
The first delivery of medicines from the Asthma Drug Facility arrives in El Salvador. Photo: R. Armengol.

5E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
BackgroundWorld Health Assembly (WHA) resolutions in 1998, 2005 and 2007 urged WHO Member States to formulate measures to encourage appropriate and cost-effective use of medicines (1). Countries were also encouraged to develop sustainable systems to monitor the volumes and patterns of medicine use and the impact of control measures, and to develop and implement effective interventions to improve the use of medicines. The Chinese Ministry of Health committed to work with WHO on this aspect of medicines use. A series of regulations and rules, working mechanisms and approaches have been developed and implemented in health facilities to improve the use of medicines, especially antibiotics.
To monitor the volume and patterns of antibiotic use and the impact of control measures, a National Monitoring Network on Clinical Antibiotics Use (the Network) was established in China in 2005, and has been regularly collecting antibiotic use data from 120 tertiary general hospitals around the country. The 2006-2007 monitoring report shows that the proportion of irrational antibiotic use in surgical practice was widespread and serious (2). With the support of WHO, the Ministry of Health initiated an intervention project to promote rational antibiotic prophylaxis in clean surgeries in 2008–2009.
Methods
Hospital samplingThe sampling frame is within the Network, which consists of 164 tertiary hospitals in 31 provinces. All the provinces were divided into three groups based on their annual Gross Domestic Product per capita in 2007. Three hospitals were randomly selected from each group, nine hospitals were selected as the intervention group (IG). Three hospitals volunteered to join the IG, so a total of 12 tertiary general hospitals were included in the IG.
Target surgeries Three common clean surgeries (thyroidectomy, mastectomy and hernia) were targeted for the intervention.
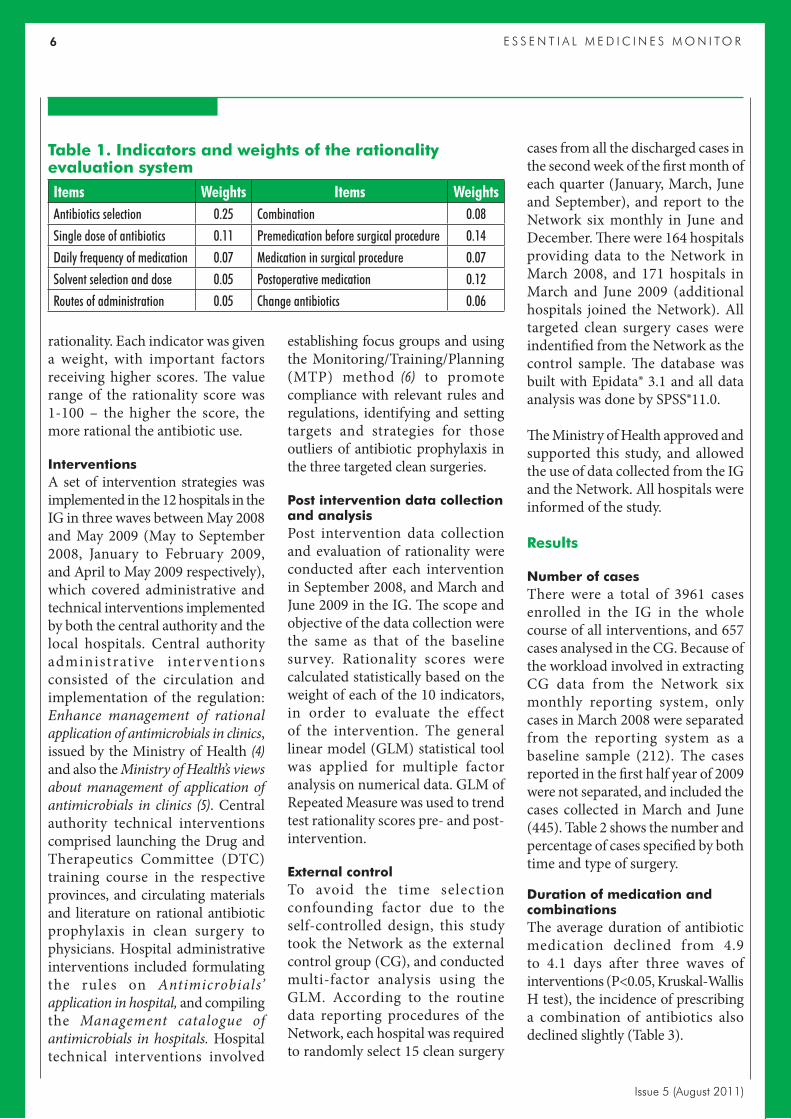
Baseline survey and evaluation of rationality Hospitals in the IG were required to collect all the medical records of patients who underwent one of the three targeted surgeries, and were discharged in March 2008. Two trained clinical pharmacists were responsible for evaluating the rationality of antibiotic prophylaxis of these cases, based on the National Guideline (3). If no antibiotic was used in a case, it was judged as rational . Non-indicated cases treated with antibiotics were judged as irrational. For those indicated cases using antibiotics, a rational use measurement system (Table 1) was formulated by a group of senior clinical specialists. Ten indicators were identified for evaluating
Promoting rational antibiotic prophylaxis in clean surgeries in China = Yingdong Zheng, Jing Sun, Ying Zhou, Ning Chen, Liang Zhou, Qing Yan
Yingdong Zheng Jing Sun Ying Zhou
Ning chen Liang Zhou Qing Yan
6 E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
rationality. Each indicator was given a weight, with important factors receiving higher scores. The value range of the rationality score was 1-100 – the higher the score, the more rational the antibiotic use.
Interventions A set of intervention strategies was implemented in the 12 hospitals in the IG in three waves between May 2008 and May 2009 (May to September 2008, January to February 2009, and April to May 2009 respectively), which covered administrative and technical interventions implemented by both the central authority and the local hospitals. Central authority administrat ive inter ventions consisted of the circulation and implementation of the regulation: Enhance management of rational application of antimicrobials in clinics, issued by the Ministry of Health (4) and also the Ministry of Health’s views about management of application of antimicrobials in clinics (5). Central authority technical interventions comprised launching the Drug and Therapeutics Committee (DTC) training course in the respective provinces, and circulating materials and literature on rational antibiotic prophylaxis in clean surgery to physicians. Hospital administrative interventions included formulating the rules on Antimicrobials’ application in hospital, and compiling the Management catalogue of antimicrobials in hospitals. Hospital technical interventions involved
establishing focus groups and using the Monitoring/Training/Planning (MTP) method (6) to promote compliance with relevant rules and regulations, identifying and setting targets and strategies for those outliers of antibiotic prophylaxis in the three targeted clean surgeries.
Post intervention data collection and analysisPost intervention data collection and evaluation of rationality were conducted after each intervention in September 2008, and March and June 2009 in the IG. The scope and objective of the data collection were the same as that of the baseline survey. Rationality scores were calculated statistically based on the weight of each of the 10 indicators, in order to evaluate the effect of the intervention. The general linear model (GLM) statistical tool was applied for multiple factor analysis on numerical data. GLM of Repeated Measure was used to trend test rationality scores pre- and post-intervention.
External controlTo avoid the time selection confounding factor due to the self-controlled design, this study took the Network as the external control group (CG), and conducted multi-factor analysis using the GLM. According to the routine data reporting procedures of the Network, each hospital was required to randomly select 15 clean surgery
cases from all the discharged cases in the second week of the first month of each quarter (January, March, June and September), and report to the Network six monthly in June and December. There were 164 hospitals providing data to the Network in March 2008, and 171 hospitals in March and June 2009 (additional hospitals joined the Network). All targeted clean surgery cases were indentified from the Network as the control sample. The database was built with Epidata® 3.1 and all data analysis was done by SPSS®11.0.
The Ministry of Health approved and supported this study, and allowed the use of data collected from the IG and the Network. All hospitals were informed of the study.
Results
Number of casesThere were a total of 3961 cases enrolled in the IG in the whole course of all interventions, and 657 cases analysed in the CG. Because of the workload involved in extracting CG data from the Network six monthly reporting system, only cases in March 2008 were separated from the reporting system as a baseline sample (212). The cases reported in the first half year of 2009 were not separated, and included the cases collected in March and June (445). Table 2 shows the number and percentage of cases specified by both time and type of surgery.
Duration of medication and combinationsThe average duration of antibiotic medication declined from 4.9 to 4.1 days after three waves of interventions (P<0.05, Kruskal-Wallis H test), the incidence of prescribing a combination of antibiotics also declined slightly (Table 3).
Items Weights Items WeightsAntibiotics selection 0.25 combination 0.08Single dose of antibiotics 0.11 Premedication before surgical procedure 0.14daily frequency of medication 0.07 Medication in surgical procedure 0.07Solvent selection and dose 0.05 Postoperative medication 0.12Routes of administration 0.05 change antibiotics 0.06
Table 1. Indicators and weights of the rationality evaluation system

7E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
Rationality evaluation of antibiotic useTable 4 shows the composition of three categories of cases (Pearson χ2 test, P<0.01). The percentage of cases not using antibiotics (rational) after the first intervention increased significantly from 3.5% to 11.5%, and remained at that level following the second (12.3%) and third interventions (11.9%). As these were elective clean cases, these were very low figures. The percentage of non-indicated cases treated with antibiotics (irrational) was reduced from 61.9% to 53.1% after two waves of interventions, but rose again to 60.9% in June 2009 following the third intervention.
Table 5 shows the rationality scores of the indicated cases treated with antibiotics before and after each intervention. Calculating the average rationality score of the 12 hospitals
in the IG using GLM analysis, we found that the rationality score of the IG significantly increased from 55.4 to 71.1 after the first round of interventions (P<0.05), while improvements after the second and third waves of interventions were not obvious, the score increased to 77 following the third intervention.
Key problems following interventions The key irrational antibiotic prophylaxis problems existing after three waves of interventions were: antibiotic selection, medication given at the wrong time, and the long duration of medication, which occurred in 28.1%, 34% and 69.6% of the total indicated cases respectively (see Table 6).
Comparison of the IG and CGBaseline: The percentage of cases using antibiotics without indications
in the IG and CG was 61.9% and 84.4% respectively, with the number of IG cases significantly lower than CG (χ2 test, P<0.01). There was no significant difference in the rationality scores for the cases using antibiotics with indications between the IG (55.4) and CG (57.6) (t test , P>0.05).
Post interventions: The proportion of patients who were prescribed antibiotics without indications in the IG decreased from 61.9% to 60.9%, with decreases following the 1st and 2nd interventions, and an increase again following the 3rd intervention. The decreasing range between baseline and post 3rd intervention was not as much as in the CG, which was from 84.4% to 59.1%. The difference between the proportions in the IG and CG after the 3rd intervention was not significant (χ2 test, P>0.05) (Figure 1). The rationality scores of the cases using
IG CG
TimeThyroidectomy Mastectomy Hernia Total cases Total cases
N (%) N (%) N (%) N N2008.3 (baseline) 382 (39.8) 324 (33.8) 253 (26.4) 959 2122008.9 (following 1st intervention) 317 (38.9) 320 (39.3) 178 (21.8) 815 –2009.3 (following 2nd intervention) 423 (39.5) 435 (40.6) 213 (19.9) 1071
4552009.6 (following 3rd intervention) 469 (42.0) 437 (39.2) 210 (18.8) 116Total 1591 (40.2) 1516 (38.3) 854 (21.6) 3961 (100) 657
N = Number of cases
Table 2. Number and percentage of cases enrolled in the project
TimeDuration of medication
Cases with 1 antibiotic
Cases with2 antibiotics
Cases with 3+ antibiotics
Mean±SD N N (%) N (%) N (%)2008.3 (baseline) 4.9±3.3 922 724 (75.5) 162 (16.9) 39 (4.1)2008.9 (following 1st intervention) 4.3±3.5 721 549 (67.4) 127 (15.6) 45 (5.5)2009.3 (following 2nd intervention) 4.1±2.6 939 782 (73.0) 134 (12.5) 23 (2.1)2009.6 (following 3rd intervention) 4.1±2.9 983 766 (68.6) 181 (16.2) 36 (3.2)
Mean±Sd = Nnumber of daysSd = Standard deviationN = Number of cases
Table 3. Duration of medication and combination of antibiotics

8 E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
antibiotics with indications in the IG increased from 55.4 to 77.0 following the 3rd intervention, and that in the CG also increased from 57.6 to 64.3; the rationality scores of the IG were significantly higher than that in CG following the 3rd intervention (t test, P<0.01) (Figure 2). Conducting multi-factor analysis with GLM, we found that there was an interaction between the grouping variables in terms of hospitals (IG and CG) and times (before and after interventions) (Figure 2).
DiscussionFol lowing three rounds of interventions, the antibiotic prophylaxis of the three targeted clean surgeries in the IG was improved overall, although only a small proportion of patients did not receive antibiotics. There was limited effect on changing the behaviour of using antibiotics for non-indicated cases. Further efforts still need to be made to address remaining problems, principally for the following reasons:
Absence of consistent operational regulations and guidelines: Although the Ministry of Health issued a series of regulations, such as the National Guidelines (3) the Guideline on Infection Control with Antibiotics in Surgeries (7), the Notice of Further Strengthening the Regulation on Antibiotics Clinical Use (4), putting them into practice has been problematic. For example, the dose recommended in the Clinical Pathway for Nodular Goiter (2009) (8) is not applicable to cases that may
Time
Indicated cases
Antibiotic selectionMedication given at the
wrong time Long duration of medication% N % N % N
2008.3 (baseline) 51.7 (171/331) 68.0 (225/331) 86.4 (286/331)2008.9 (following 1st intervention) 37.0 (87/235) 38.3 (90/235) 76.2 (179/235)2009.3 (following 2nd intervention) 35.4 (129/364) 34.6 (126/364) 81.0 (295/364)2009.6 (following 3rd intervention) 28.1 (85/303) 34.0 (103/303) 69.6 (211/303)
N = Number of indicated cases with respective problem/total number of indicated cases
Table 6. Proportion of indicated cases with major irrational antibiotic prophylaxis problems
TimeThyroidectomy Mastectomy Hernia repair Pooled
Mean±SD N Mean±SD N Mean±SD N Mean±SD N2008.3 (baseline) 57.9±25.2 43 53.2±21.7 113 56.1±20.7 175 55.4±21.6 3312008.9 (following 1st intervention) 68.7±17.3 56 74.2±15.9 106 68.4±17.1 73 71.1±16.8 2352009.3 (following 2nd intervention) 69.6±19.4 60 73.0±21.0 179 74.7±17.2 125 73.0±19.6 3642009.6 (following 3rd intervention) 75.4±17.1 77 79.7±17.1 121 75.0±14.5 105 77.0±16.4 303
Mean±Sd = Rationality scoresN = Number of cases
Table 5. Rationality scores of the indicated cases
TimeNo antibiotic Antibiotic without indication Antibiotic with indication Total cases
N (%) N (%) N (%) N2008.3 (baseline) 34 (3.5) 594 (61.9) 331 (34.5) 9592008.9 (following 1st intervention) 94 (11.5) 486 (59.6) 235 (28.8) 8152009.3 (following 2nd intervention) 132 (12.3) 569 (53.1) 370 (34.5) 10712009.6 (following 3rd intervention) 133 (11.9) 680 (60.9) 303 (27.2) 1116
N = Number of cases
Table 4. Composition of cases not using antibiotics, and using antibiotics with and without indications

9E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
Intervention intensity: Promoting rational use of medicines needs cont inued ef for t , one-t ime administrative intervention will inevitably be unsustainable. Hospitals in the IG followed the same technical approaches, but with a different variety and intensity of administrative measures. Effective technical interventions always require relevant administrative interventions, to maintain the sustainability of the intervention effect.
L i m i t a t i o n s o f t e c h n i c a l interventions for health system problems: Technical interventions have a limited effect in convincing doctors not to use antibiotics for cases for which they are not indicated, as comprehensive problems exist that go beyond the knowledge and prescribing habits of doctors. Perverse incentives that exist in the health system have driven doctors to use antibiotics even for those cases for which they are not indicated (9). Placing the responsibility of proof on doctors in medical disputes about unexpected infections due to failure to control hygiene risks in operating theatres may also be a factor in risk avoidance by over-prescribing.
Limitations All hospitals in the IG were in
the Network. In addition, the three hospitals that volunteered also brought selective bias to the project.
Constrained by the CG data from the available Network database, and the data collection workload, the sampling methods for the cases in the IG and CG are different, so there is a large gap in the number of cases included in the data analysis between the IG and CG. Also the CG data did not exclude the data contributed to the Network database by the 12 hospitals in the IG. All these
Figure 2. Rationality scores for indicated cases treated with antibiotics
55%
65%
70%
80%
55.4
Baseline March2008
50%
Following the 3rd interventionJune 2009
Time
77.0
57.6
64.3
Intervention group
Control group
60%
75%
Score
Figure 1. Proportion of cases using antibiotics without indication
60%
70%
80%
90%
84.4
Baseline March2008
50%
Following the 3rd interventionJune 2009
Time
60.9
61.9
59.1
Intervention group
Control groupScore
develop into cancer but in most instances it is very difficult to evaluate such a risk before surgery takes place.
Authoritativeness of different guidelines: There is no well organized expert consultation process, and no standardized evidence-based mechanism for guideline development. For example, in terms of medication
time for antibiotic prophylaxis, the National Guidelines require that antibiotics should not be permitted for 24 hours following surgery in non-exceptional circumstances. However, the Clinical Pathway for Breast Cancer guidelines (2009) do not allow antibiotics for 72 hours following surgery (8). Doctors do not know which guidelines to follow.

10 E S S E N T I A L M E D I C I N E S M O N I TO R
Issue 5 (August 2011)
factors meant the control is not a perfect external control.
This project targeted frequently performed simple clean surgeries. More common surgeries could be included and the project expanded to outpatients in the future. Electronic prescription and advanced health information systems could also enable more advanced evaluation methods for future studies.
Conclusion The baseline investigation indicates
that in China the problem of irrational antibiotic prophylaxis for clean surgeries is very serious, with 80%-90% of cases irrationally treated with antibiotics.
The intervention was effective overa l l , with stat ist ica l ly s igni f icant improvements following the interventions, but 50–60% of the cases were still treated irrationally.
The key problem is using antibiotics without indication. Among the cases with indications, the key irrational antibiotic prophylaxis problems are antibiotic selection, medication given at the wrong time and the long duration of medication.
There was a statistically significant improvement in performance after the first intervention, the improvements that followed the second and third interventions were slight, with some indicators getting worse, which indicates the difficulty of changing established “wrong” prac t ices . More comprehensive approaches and continued efforts are needed.
There was a s igni f icant improvement in cases treated with antibiotics with indication after the interventions, but very little improvement in the cases not using antibiotics without an
indication. This indicates that there may be other factors that affect the doctors’ decision not to use antibiotics, such as health system problems and patients’ expectations. n
References1. Wor l d He a l t h As s e mbly
Resolutions: 51.17, Emerging and other communicable diseases: antimicrobial resistance; 58.27, Improving the containment of antimicrobial resistance; 60.16, Progress in the rational use of medicines, including better medicines for children.
2. Report of the National Monitoring Network on Clinical Antibiotics Use. Beijing, Ministry of Health, 2008: 50-54.
3. Guideline on clinical antibiotics use. Beijing, Department of Drug Management Research, the Institute of Hospital Management, Ministry of Health, 2007.
4. Enhanced management of rational application of antimicrobials in clinics, No.48. Beijing, Ministry of Health, 2008.
5. Views about management of application of antimicrobials in clinics, No.38. Beijing, Ministry of Health, 2009.
6. Suryawati S, Santoso B. MTP approach is effective in reducing inappropriate medicines use in hospitals. Presentation at the 2nd International Conference on Improving Use of Medicines, 30 March–2 April 2004, Chiang Mai, Thailand. Available at: http://archives.who.int/icium/icium2004/resources/ppt/AD009.ppt#270,2,Abstract
7. Guideline on infection control with antibiotics in surgeries. Beijing, Department of Drug Management Research, Institute of Hospital Management, Ministry of Health, 2007.
8. Guidelines on management by clinical pathways, No. 99. Beijing, Ministry of Health, 2009.
9. Chen W, Tang SL, Sun J, Ross-Degnan D, Wagner A. How to perform a critical analysis of a randomized controlled trial. BMC Health Services Research, 2010, 10:211.
Yingdong Zheng, Department of Epidemiology and Biostatistics, School of Public Health, Peking University, 38 Xueyuan Road, Haidian District, 100083, Beijing, China.
*Jing Sun, Department of International Health, China Nat ional Health Development Research Center, Ministry of Health, P.O. Box 218, 38 Xueyuan Road, Haidian District, 100191, Beijing, China. E-mail: [email protected]
Ying Zhou, Department of Pharmacy, First Teaching Hospital of Peking University, Beijing, China.
Ning Chen, Department of Pharmacy, Jishuitan Hospital, Beijing, China.
Liang Zhou, Department of Pharmacy, Chinese PLA Hospital 304, Beijing, China.Qing Yan, Department of Pharmacy Management, Institute of Hospital Management, Ministry of Health, Beijing, China.


















