
ESRD Network 18 Annual Meeting: What is New for Clinical …esrdnetwork18.org/pdfs/Admin - Annual...
127
ESRD Network 18 Annual Meeting: What is New for Clinical Staff? What is New for Clinical Staff? ESRD Network 18 California Dialysis Council 27 th Annual Educational California Dialysis Council 27 th Annual Educational Conference, Palm Springs, CA April 17, 2009
Transcript of ESRD Network 18 Annual Meeting: What is New for Clinical …esrdnetwork18.org/pdfs/Admin - Annual...

ESRD Network 18 Annual Meeting:What is New for Clinical Staff?What is New for Clinical Staff?
ESRD Network 18California Dialysis Council 27th Annual EducationalCalifornia Dialysis Council 27th Annual Educational
Conference, Palm Springs, CAApril 17, 2009p ,
Objectives:Provide an overview of the ESRD Network organizations mission and goals g gOutline major changes in the new ESRD Conditions for Coverage (CFC)Conditions for Coverage (CFC)Explain involuntary discharge processU d t th CROWN W bUpdate on the CROWN Web implementation status
2

Health Care Quality ImprovementHealth Care Quality Improvement Program (HCQIP)
The Center for Medicare & Medicaid Services (CMS) contracts with 18 ESRD Network Organization throughout the United StatesThe ESRD Network perform oversight activities to
i f i d i fassure appropriateness of services and protection for ESRD patients. Thi h h b d th ESRD H lth CThis approach has been named the ESRD Health Care Quality Improvement Program (HCQIP)
3

4
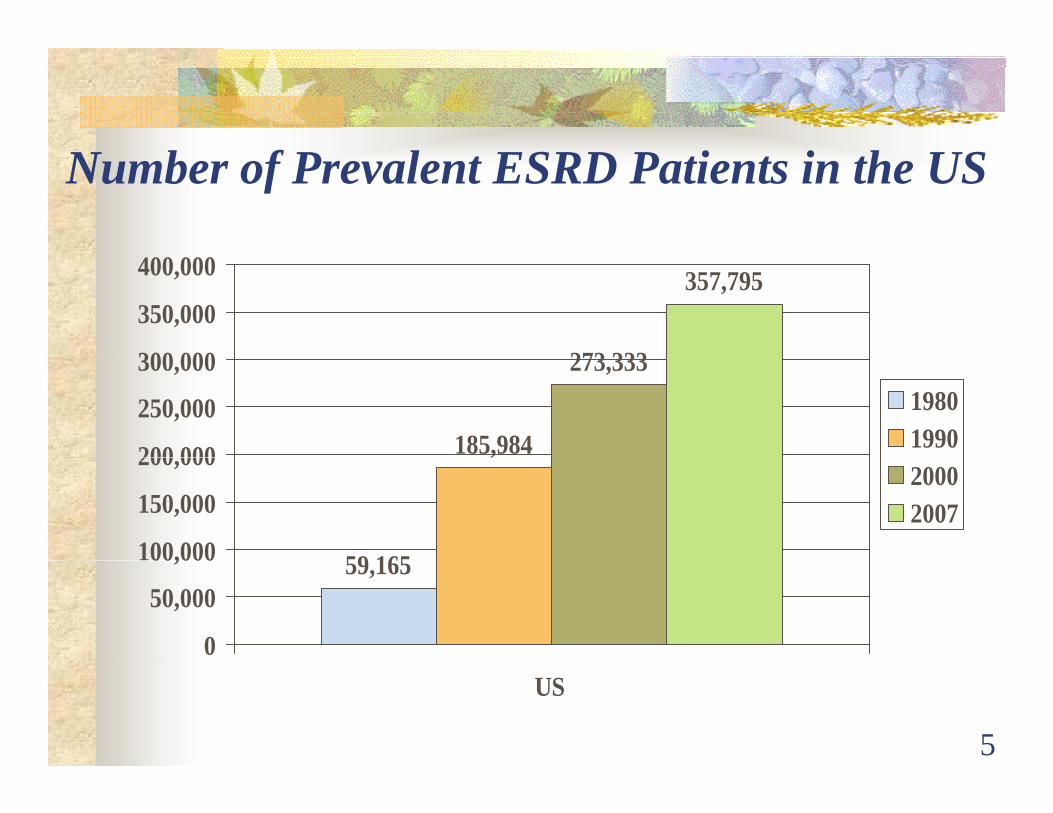
Number of Prevalent ESRD Patients in the US
273 333
357,795
300 000
350,000
400,000
185,984
273,333
200 000
250,000
300,00019801990
59 165
,
100,000
150,000
200,00020002007
59,165
0
50,000
00,000
5
US

ESRD Network National GoalsImprove the quality of health services & qualityImprove the quality of health services & quality of life for ESRD beneficiariesImprove data reporting, reliability, & validity p p g, y, ybetween providers, NWs, and CMSEvaluate and resolve patient grievancesp gSupport the marketing, deployment, and maintenance of CMS approved software
CMS, ESRD NW Organization Manual
6
ESRD Network National GoalsEstablish & improve partnerships &Establish & improve partnerships & cooperate activities with
Providers & OwnersProviders & OwnersNWs, Quality Improvement Organizations (QIOs)(QIOs)State Survey AgenciesProfessional Groups & Patient OrganizationsProfessional Groups & Patient Organizations
CMS ESRD NW Organization Manual
7
CMS, ESRD NW Organization Manual
Network 18 Mission Statement
To provide leadership and assistance to renal dialysis and transplant facilities in adialysis and transplant facilities in a
manner that supports continuous i i iimprovement in patient care, outcomes,
safety and satisfaction.
8
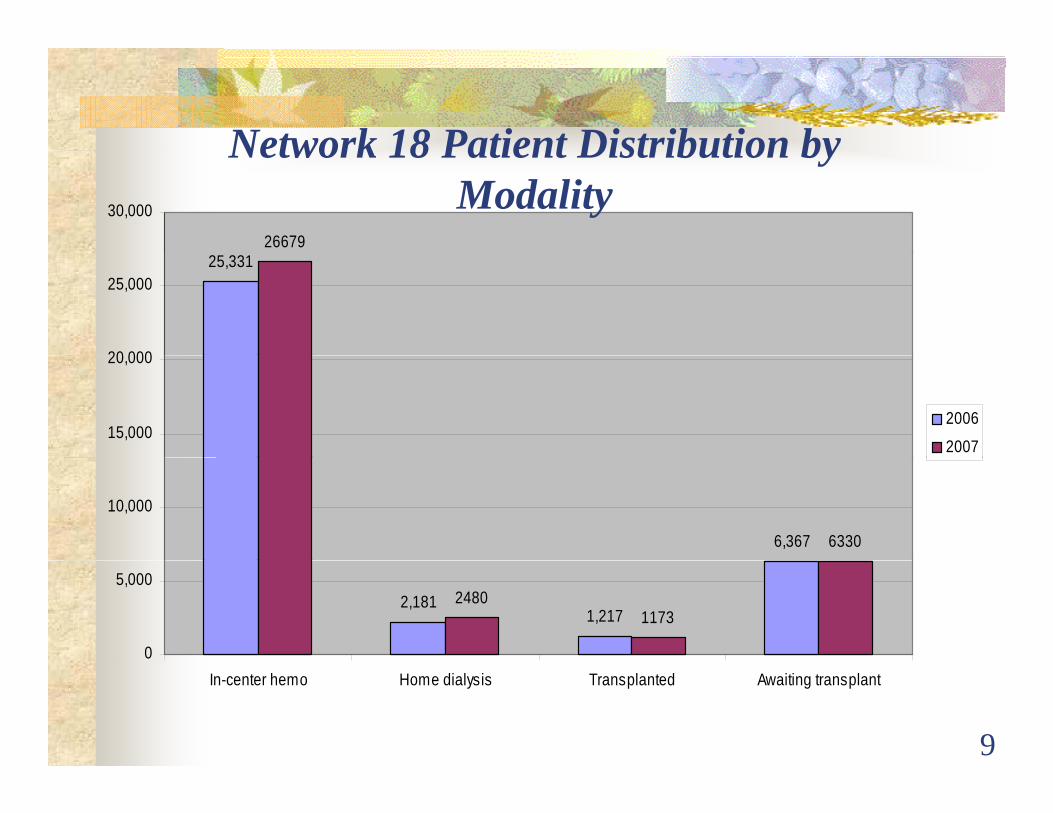
Network 18 Patient Distribution by
26679
30,000
Network 18 Patient Distribution by Modality
25,331
20 000
25,000
15,000
20,000
2006
2007
6,367 6330
10,000
2,1811,217
24801173
0
5,000
9
In-center hemo Home dialysis Transplanted Awaiting transplant
Definition of Healthcare Quality“Quality of care is the degree to which healthQuality of care is the degree to which health
services for individuals and populations increase the likelihood of desired outcomesincrease the likelihood of desired outcomesand are consistent with current professional knowledge ”knowledge.
I f M dInstitute of Medicine
10

What is the cost of Poor Quality?
No show rates?Lost charts?Lost labs?Train wreck visits?Lost revenue – improper billing?Staff turnover?Staff turnover?
11
12

Network 18 Definition of Quality
“Doing the right thing correctlyDoing the right thing correctlythe first time.”
13

New ESRD Regulations:What are some of the major
changes?changes?
14
Special Thanks for the Content Contribution to the
CMS Transition TeamCMS Transition Team
Glenda Payne, Judith KariTeri Spencer Kelly FrankTeri Spencer, Kelly Frank
Rosemary Miller, Bonnie GreenspanBeth WittenBeth Witten

The ESRD Regulation Timeline
1976: First ESRD regulations published
70’s-90’s: Technical updates
1994 C it F M ti t b i1994: Community Forum Meeting to begin complete rewrite of ESRD regulations
2008: New ESRD regulations published
16
M j Ch R l iMajor Changes to Regulations
Subpart A: GeneralSubpart A: General1. Compliance with Federal State & local laws
and regulationsand regulations
Subpart B: Patient Safety2. Infection control3. Water and dialysate quality4. Reuse of hemodialyzersy5. Physical environment

M j Ch t R l tiMajor Changes to Regulations Subpart C: Patient Care
6. Patients’ rights7. Patient assessment7. a e assess e8. Patient plan of care9 Care at home9. Care at home10. QAPI11 Special purpose dialysis facilities11. Special purpose dialysis facilities12. Laboratory services
Major Changes to Regulations Subpart D: AdministrationSubpart D: Administration
13. Personnel qualifications14. Responsibilities of
the Medical Director15. Medical records16. Governance

P i f I l i D lPreparing for Implementation: Development of the Interpretative Guidance
Community involvementDraft document to listserv of 10K+ stakeholdersCommunity Forum (120 attended)Revised draft to listserv
1600 comments received and reviewed; used to craft final1600 comments received and reviewed; used to craft final document
Evolutionary processBegan with a focus of surveyor guidanceCommunity feedback wanted moreEvolved in a broader way to address needs ofEvolved in a broader way to address needs of community as well as the needs of surveyors

D l f h I iDevelopment of the Interpretative Guidance
Focus on defining terms for clarityAim to ensure consistent interpretation by providers and surveyorssurveyors
Involvement of CDC / AAMIActive on-going dialog with CDC Repeated review of the Water & Dialysate portion by the AAMI RD Committee
Survey Process separatey pDeveloping specific process guides for initial and resurveysDirected at the needs of the surveyorsyWill be part of the State Operations Manual
The WaiversN F ili I l i RNew Facility: Isolation Room
Based on distance and travel time to a facility with isolation capacity and willingness to accept patientsisolation capacity and willingness to accept patients
Qualifications of the Medical DirectorTime limited, potentially renewable, p yBased on outcomes list
Life Safety CodeIf compliance presents an unreasonable hardshipIf the waivered requirement will not present a risk to
ti t f tpatient safety
Phased-In Time Extensions
Single-Use Vials (end of June, 2009)Water Storage Tanks (dependent on waterWater Storage Tanks (dependent on water cultures)Interdisciplinary Patient Assessment (October 14,Interdisciplinary Patient Assessment (October 14, 2009)CROWN Web Data Submission (phased-in time (pline)

S O tSurvey Outcomes Early Report: April 2009Early Report: April 2009

Condition Level Citations
I f ti C t lInfection ControlWater & Dialysate Quality Governance QAPIQAPI Responsibilities of the Medical Director Patient Plan of Care Physical EnvironmentPhysical Environment
2008 Ci i F R f2008 Citation Frequency Report for California ESRD Facilities:
Total Number of Surveys conducted = 490Number of providers cited = 476 (97.1%)p ( )
26Source: CASPER report
Most Frequently Cited Deficiencies
Infection Control Clean & Disinfect surfacesClean & Disinfect surfacesWear gloves/hand hygieneItems taken to station: D/D/DClean/dirty areas; med prep areaClean/dirty areas; med prep areaWear gowns/PPE

Infection Control: Why Would This Be Cited?
All aboutHANDSHANDSSuppliesMeds
SalineHeparin
PPEPPE
Gloves & Hand Hygiene“Hand washing is the most important measure to
prevent contaminant transmission.”--CDC
V113 requires: Wear gloves Whenever caring for a patient orWear gloves – Whenever caring for a patient or touching the patient’s equipment.
Remove/change gloves – Must perform hand hygiene after removal of gloves between each patient or station.
29
patient or station.
PPE: Must Wear GownsV115 requires:
A gown or lab coat must be worn when theA gown or lab coat must be worn when the spurting or spattering of blood, body fluids, potentially-contaminated substances or chemicals
i htmight occurAprons are not sufficient PPE during procedures that may result in the spurting or spattering of blood y p g p g
Clarifies when staff, patients, & visitors should wear PPE & when the PPE should be changed
30

I T k I h Di l iItems Taken Into the Dialysis Station
V116 iV116 requires:Items taken into the dialysis station
Dispose, dedicate, or clean & disinfect (DDD)Unused supplies or medications should not be ppreturned to a common area or used on other patients
31
Clean/Dirty Areas & MedicationClean/Dirty Areas & Medication Preparation AreasV117 requires:
Separate clean from contaminated areas
Prepare individual patient meds in a centralized area away epa e d v dua pat e t eds a ce t a ed a ea awayfrom the treatment area
Designate area only for medication prepDeliver separately to each patientDeliver separately to each patient
Do not move the medication cart from patient station to patient station to deliver medicationspatient station to deliver medications
If trays are used, clean between patients
32
Single Use Vials = Single UseV118 requires:
Single dose vials cannot be punctured more than onceMust be used for only one patientNot entered more than onceIf entered, may not be stored for future use., y
BRAND NEW: MMWR August 15, 2008 retracts the 2002 CDC communication allowing multiple use of single use vialssingle use vials
Multi-use vials: residual medication from two or more i l b l d i i l i l
33
vials must not be pooled into a single vial
Supply Cart & Supplies
V119 requires: If l i d dIf a common supply cart is used, do not move the cart from patient station to patient
i d li listation to deliver suppliesDo not carry supplies, patient care items, or medications in pockets
34

Cleaning & Disinfecting of ContaminatedCleaning & Disinfecting of Contaminated Surfaces, Medical Devices, & Equipment
V122 requires:Protocols for cleaning & disinfecting surfaces &
iequipmentManufacturer’s DFUs followedCDC recommended disinfection proceduresCDC recommended disinfection procedures
Cleaning & disinfection of environmental surfaces completed between patient uses
Ch i b d hi & t i i t d ithChairs, beds, machines & containers associated with prime waste, adjacent tables & work surfaces
35
Cleaning & Disinfecting of ContaminatedCleaning & Disinfecting of Contaminated Surfaces, Medical Devices, & Equipment
V122 requires: Clean & disinfect medical devices & equipment after each patient
Scissors, hemostats, clamps, stethoscopes, blood , , p , p ,pressure cuffs
Blood spills cleaned effectively & immediately“Intermediate-level” disinfectant
36
H i i B R i T i V i iHepatitis B Routine Testing, Vaccination, Screening, & Seroconversion (V124-127)
Routine testing for HBV (V124)HBV status of all patients known before admission to the HD itHD unitTest all patients as required by the CDC schedule
Results of HBV testing promptly reviewed (V125)g p p y ( )Vaccination of susceptible patients & staff members (V126)
All tibl ti t & t ff ff d h titi BAll susceptible patients & staff are offered hepatitis B vaccination
37
HBV+ Isolation Room/AreaV128 & V129: Isolation of HBV+ PatientsV128 & V129: Isolation of HBV+ Patients
Effective Feb 9, 2009, every new facility MUST include an isolation room for treatment of HBV+ patients, unless the facility is granted a waiver of this requirementF i ti it i hi h t i tFor existing units in which a separate room is not possible, there must be a separate area for HBsAg positive patientsp p
38

Isolation of HBV+ PatientsDedicated machines, equipment, supplies, & , q p , pp ,medications (V130)
Used only for HBV+ patients until patient is discharged from facilitfrom facility
Staff assigned to care for HBV+ patient (V131):Staff assigned to care for HBV+ patient (V131):May only care for other HBV+ patients or HBV immune patients
39
Most Frequently Cited Deficiencies PA/POCPA/POC
Assess B/P & fluid mgmt needsManage volume status
Medical Director Responsibilities Ensure all adhere to P&P
Physical Environment yPM; follow manufacturer’s DFU
M j Ch CFC N LTPMajor Change new CFC: No LTP (Long-Term Plan)
No expectation for a long term program or “signature” of transplant surgeonRequirements for patients to be informed of all modalities (transplant & therapies not offered at their current clinic) are addressed under:
Patients’ RightsP ti t A tPatient AssessmentPlan of Care
41

Patient Assessment (V501) and Patient Plan of Care (V541)f ( )
These 2 Conditions:Are interrelated (“can’t have one without theAre interrelated ( can t have one without the other”)Address patient assessment & care deliveryAddress patient assessment & care delivery requirements in “care areas” associated with complications of ESRD
42
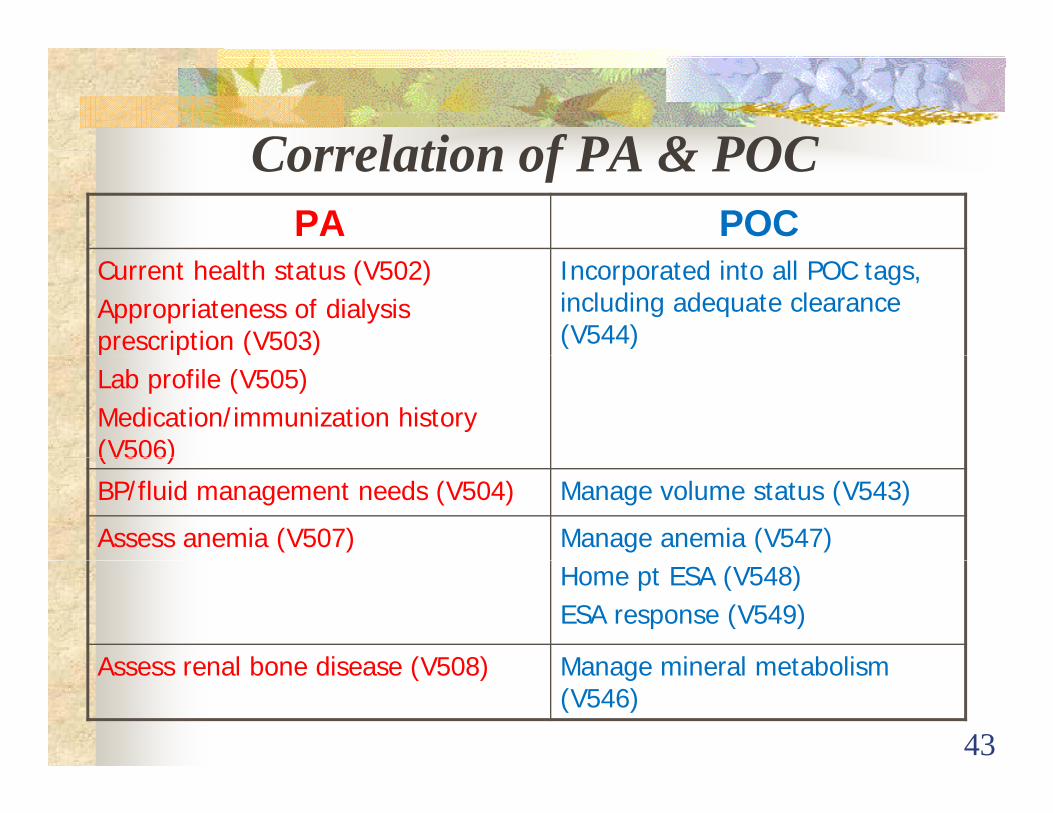
Correlation of PA & POCCorrelation of PA & POCPA POC
Current health status (V502)Appropriateness of dialysis prescription (V503)
Incorporated into all POC tags, including adequate clearance (V544)
Lab profile (V505) Medication/immunization history (V506)(V506)
BP/fluid management needs (V504) Manage volume status (V543)
Assess anemia (V507) Manage anemia (V547)Home pt ESA (V548)ESA response (V549)
Assess renal bone disease (V508) Manage mineral metabolism
43
Assess renal bone disease (V508) Manage mineral metabolism (V546)

C l ti f PA & POCCorrelation of PA & POCPA POC
Nutritional status (V509) Effective nutritional status (V545)
Psychosocial needs (V510)Evaluate family support (V514)
Psychosocial counseling/referrals/ assessment tool (V552)Evaluate family support (V514) assessment tool (V552)
Access type/maintenance (V511) VA monitor/referral (V550) Monitor/prevent failure (V551)
Evaluate for self/home care (V512) Home dialysis plan (V553)
Transplantation referral (V513) Transplantation status: plan or why not (V554)
Evaluate current physical activity Rehab status addressed (V555)
44
Evaluate current physical activity level & voc/physical rehab (V515)
Rehab status addressed (V555)

How Is This Supposed to Work? PA: identifies intradialytic weight gains (IDWG) ofPA: identifies intradialytic weight gains (IDWG) of greater than 12 pounds/treatmentPOC:
IDT members (all) to work with patient on risks of excessive fluid gains and (RD) on ways to handle thirstAgree to a goal for IDWG to be reduced by 10% each weekAgree to a goal for IDWG to be reduced by 10% each week until goal of no greater than 5 pounds is reached Monitor IDWG each treatment. Praise positive actions (RN, PCT)PCT)If IDWG remains at same levels at end of one month, review and revise POC

P ti t A t A B/P A dPatient Assessment: Assess B/P And Fluid Management Needs
Why would this be cited?• Review of flow sheets = no evidence B/P is
b i it dbeing monitored • Post weight does not = goal and no comment is
mademade• Fluid removed and weights do not match and no
comment is madeNote: Surveyors are being taught to look at flow
sheets for the implementation of the assessment-b d l fbased plan of care
Another Word about PA/POC
Here is a REAL opportunity to CHANGE the way care is delivered!
Here is a REAL opportunity to:INCREASE patient involvement andINCREASE patient involvement and INCREASE patient independence
= Improved Satisfaction & Better Working Improved Satisfaction & Better Working Conditions For Everyone!

I t di i li CInterdisciplinary Care vs. Multidisciplinary CareMultidisciplinary Care
Interdisciplinary MultidisciplinaryWork collaboratively Work sequentially
Communication by Medical record is theCommunication by regular discussions about patient status &
Medical record is the chief means of communication p
the evolving plan of care
48
The Interdisciplinary Team (IDT)Includes at a minimum:
The patient or their designee (if the patient p g ( pchooses)A registered nurseA ph sician treating the patient for ESRDA physician treating the patient for ESRDA social workerA dietitianA dietitian
49

Interdisciplinary Team:
Show Me The ProgressThe Progress
50

Timelines: Starting 10/14/08I i i l A f N P iInitial Assessments for New Patients:
• PA=30 days/13 treatments whichever is later• POC implemented within this same timeline
Reassessment for New Patients:• 3 months after initial assessment completed• POC updated and implemented within 15 days of
reassessment
51

Then what?
Stable patients = Annual reassessmentPOC updated and implemented within 15 days
All patients: Continuous monitoring = any aspect f h th t t i t t i th tof care where the target is not met = revise that
aspect of POC
Unstable patients = monthly reassessmentPOC updated and implemented within 15 days
52

Who Is “Unstable?” Per V520, includes but is not limited to:
Extended or frequent hospitalization (>8 days or q p ( y> 3 X a month)Marked deterioration in health statusSignificant change in psychosocial needsConcurrent poor nutritional status, unmanaged
i d i d t di l ianemia and inadequate dialysis
53

What About Current Patients? As of October 12, 2008:,
Expect a plan to implement this new systemSome assessments/POCs completed each month until So e assess e ts/ OCs co p eted eac o t u tall are doneAll current patients to be included in the new system p ywithin 12 months of 10/12/08Do not expect 3 month reassessment for current patientsExpect updates for any aspect of care that does not
54
meet targets

Transfer of Current Patients
After 10/14/08, when a patient is transferred, expect:Copy of most current IDT assessment and POC from
f i f ili i i di l dtransferring facility in patient’s medical recordReassessment within 3 months of admissionR i i d i l t ti f POC ithi 15 dRevision and implementation of POC within 15 days of completion of the reassessment
55

F Ci i MDFrequent Citations: MD Responsibilities: All Adhere To P&P
Why would this be cited? Ad i i li iAdmission policies
OrdersBaseline H&PNursing assessment prior to 1st treatmentg p“Adhere to P&P”
F Ci i Ph i lFrequent Citations: Physical Environment: Equipment Maintenance; q p
Follow DFU Wh ld thi b it d?Why would this be cited? Equipment Repair & Maintenance
*DFU= Directions for use
Physical Environment
Life Safety Code (LSC) Requirements: Must meet provisions of NFPA 2000Grandfather clause for current facilities in non-sprinklered buildings if built prior to 1/1/2008State fire safety codes may be used in lieu of LSCState fire safety codes may be used in lieu of LSCSpecific provisions of LSC may be waived in some casessome cases
58
Physical EnvironmentE f ilit t h AED d fib ill tEvery facility must have an AED or a defibrillator
(& ACLS qualified staff)
All equipment maintained & operated according to manufacturer’s directionsmanufacturer s directions
Emergency preparedness for staff & patients, i l di di t t t k l lincluding disaster prep—get to know your local Emergency Ops Center
59
Condition 494.110:Quality Assessment and Performance Q y f
Improvement Project (QAPI)QAPI)Interdisciplinary team (IDT)Interdisciplinary team (IDT)Must report problems to Medical Director and QAPIProcess continuous & on-goingg gOutcome focused: use community accepted standards as targets
l d i i f i i f i l di lInclude patient satisfaction, infection control, medical injuries & medication errorsPlan/Do/Check/Act: Close the loop!
60
Plan/Do/Check/Act: Close the loop!Refer to the 2008 QI Manual for more QAPI Resounces

PDCA Style
PLANACT
DOCHECK
61
V626 QAPI Condition Statement
The dialysis facility must develop, implement, maintain and evaluate an effective, data driven, , ,quality assessment and performance improvement program with participation by the professional members of the interdisciplinary team...…The dialysis facility must maintain and
i f i idemonstrate evidence of its quality improvement and performance improvement program for review by CMS
62
program for review by CMS
63

P f M (S MAT)Performance Measures (See MAT)(V629) Adequacy Kt/V URR(V629) Adequacy Kt/V, URR
(V630) Nutrition Albumin, body weight
(V631) B di PTH C + Ph(V631) Bone disease PTH, Ca+, Phos
(V632) Anemia Hgb, Ferritin
(V633)Vascular access Fistula, catheter rate
(V634) Medical errors Frequency of specific errors
V635) Reuse Adverse outcomes
(V636) Pt satisfaction Survey scores
64
(V637) Infection control Infections, vaccination status

Monitoring Performance Improvement
(V638) The facility must:Continuously monitor its performanceContinuously monitor its performanceTake actions that result in performance improvementimprovementTrack to assure improvements are sustained over time
65

Prioritizing Improvement Activities(V639) Considerations in prioritization
Prevalence of problemPrevalence of problem Severity of problemImpact on clinical outcomesImpact on clinical outcomesImpact on patient safety
66

Immediate CorrectionExamples of serious health and safety threats:Examples of serious health and safety threats:
Unsafe water or dialysateDefective clinical equipmentDefective clinical equipmentUnsafe reprocessing of dialyzers Epidemiological risksEpidemiological risksInsufficient number of competent staff to perform scheduled treatments:perform scheduled treatments:
Preserve accessesMonitor patients
67
pAssure safe machine function
PersonnelDefines individual qualifications:q
Medical DirectorNurses: nurse manager, home training nurse, g , g ,charge nurse, staff nurseDietitianSocial Worker
Defines group qualifications:Patient care techniciansWater treatment system technicians
68
PersonnelPatient Care TechnicianPatient Care Technician
High school diploma or equivalency or 4 years of employmentp yComplete a (defined) training course, approved by Medical Director & Governing Body; under di ti f RNdirection of RNBe certified by a State or national program
New employees: within 18 months of hire dateNew employees: within 18 months of hire date (starts after 10/4/08) Current employees: within 24 months of 4/4/08
69
Current employees: within 24 months of 4/4/08

National Organi ations ApprovedNational Organizations Approved by CMS to Certify Technicians:
BONENT (Board of Nephrology Examiners for N i d T h lNursing and Technology NNCC (Nephrology Nursing Certification CommissionCommission NNCO (National Nephrology Certification Organization)Organization)
70

M di l DiMedical DirectorAccountable to the Governing Body
Responsible for patient care and outcomes
Responsible for effective QAPI and InfectionResponsible for effective QAPI and Infection Control programs
Responsible to assure all staff, physicians & non-physician providers “adhere” to all policies
Must be engaged in any involuntary patient transfer or discharge
71
or discharge

Medical Records
Traditional rules on completeness & protection of medical recordsmedical records
Transfer requested records to the receiving facility within one day
72
Staffing: Governance RequirementsAdequate number of qualified & trained staff
Patient/staff ratio appropriate to the level of care & t th d f th ti t (V757)meets the needs of the patients (V757)
RN, MSW, RD available to meet patient needs (V758)RN present at all times in-center patients are beingRN present at all times in center patients are being treated (V759)All staff have orientation to the facility & their work responsibilities (V760) & continuing education (V761)
73

Condition: Governance
Separate Standards within this Condition: Identifiable governing body/designated personIdentifiable governing body/designated person (CEO/Administrator) (V751-752)Medical staff appointments (V762)Internal grievance system in place (V765)Involuntary discharge process (V766-767)E (V768 770)Emergency coverage (V768-770)Electronic data submission (V771) Relationship with the ESRD Network (V772)
74
Relationship with the ESRD Network (V772)

Emergency Preparedness: S ff i i /k l d (V409 & V411)Staff training/knowledge (V409 & V411)Staff CPR certification (V410)Patient orientation & training (V412)
75

Emergency Preparedness (cont).Emergency preparedness – ImplementEmergency preparedness Implement processes & procedures to manage medical & non-medical emergencies (V408)(V408)Staff & patient training – Training & orientation, including what to do, where to go & who to contact (V409)where to go, & who to contact (V409)Emergency plans – Evaluate/update annually, make contact with local E M (V416)Emergency Management (V416)
76
4 K T B i P d f4 Keyes To Being Prepared for a Disaster (KCER)
Determine what kind of disaster you may expectEvaluate the readiness of your dialysis facilityEvaluate the readiness of your dialysis facilityPrepare your staffPrepare your patientsPrepare your patients

Northridge Earthquake ~ 1994
Northridge Earthquake ~ 1994

California Firestorms ~ 2007-2008
Facility Readiness
Secure the facilityKeep patient and business records secureKeep patient and business records secureHave a back-up utility planRefer to CMS Manual “Emergency PreparednessRefer to CMS Manual Emergency Preparedness for Dialysis Facilities” (CMS-11025)
Prepare Your StaffPrepare Your StaffIdentify the disaster Organizational StructureDevelop a communication plan and test itDevelop a communication plan and test it regularlyEducate key personal in their role during disastery p gHave a back-up facility agreementKnow in advance who to contact for assistance and information:
- ESRD NetworkCi C d S E R- City, County and State Emergency Response
Teams- American Red Cross ChapterAmerican Red Cross Chapter
- Security Company
Prepare Your PatientsHanding out a copy of a facility’s disaster planHanding out a copy of a facility s disaster planDisaster drills (do not discontinue dialysis treatment during a drill)g )Emergency disconnect (Clamp and Cut or Clam and Disconnect)Distributing medical emblems identifying patients as dialysis patientsPatient Emergency ID Card (wallet size)Patient Emergency ID Card (wallet-size)Distributing a copy of the CMS booklet: “Preparing for Emergencies: A Guide for PeoplePreparing for Emergencies: A Guide for People on Dialysis”.

Prepare Your Patients (cont)Gather and carry important medical informationAwareness about alternative arrangements for treatmentPreparing an emergency stock of supplies, food, and medicationand medicationKnow “survival diet” to follow if dialysis treatment must be delayedtreatment must be delayed

Patient Provider TrackingESRD N k ill b i i f iliESRD Networks will be monitoring facility Open/Closed status Web site on nephron.comDisaster Patient Activity ReportDisaster Patient Activity Report
Through ESRD Networks Begins DAY 5 post emergencyBegins DAY 5 post emergencyContinues twice a week

KCER Tools & ResourcesKCER Tools & Resourceswww.kcercoalition.comResponse Team PagesResponse Team Pages
Information & educationDrills & educationHelpful links
ESRD & disaster-related informationinformationwww.kidney.org/help
86

ESRD Network 18 EmergencyESRD Network 18 Emergency Preparedness Efforts
Collaborated with Medical and Health Coordination programsp gDeveloped the Annual Update form and the Document of UnderstandinggProvided EMS Contact List to FacilitiesKCSC Coalition changed its focus from CKD to gemergency preparednessParticipated in the Great Shakeout Drill p(November 13, 2008)
87
Network Relationship (V772)
Receive and acts upon recommendations from their NWParticipate in NW activities and pursue NW goals
Improve the quality & safety of servicesp q y yImprove independence, QOL, rehab for all pts.Encourage activities to ensure achievement of these goalsImprove the collection, reliability, timeliness and use of data
88
of data

ESRD Network 18 Assistance:
Survey tools and resources are posted on the Network 18 website at www.esrdnetwork18.orgg2008 QI Manual has many CFC informationContinue to provide educational opportunitiesContinue to provide educational opportunities for providersConduct Quality Improvement Project to assist Q y p jfacilities with compliance to new CFC

Sign up for 5 Diamond PatientSign-up for 5-Diamond Patient Safety Program!
Developed by ESRD Networks 1 & 5Promotes commitment to patient safety openPromotes commitment to patient safety , open communication and blame-free environmentBuilds a patient safety culture in every dialysisBuilds a patient safety culture in every dialysis unitEmployee & Physician Involvement &Employee & Physician Involvement & Accountability
90

Program Componentsg pPatient Safety Principles (required)Hand HygieneHand HygieneFlu VaccinationSlips Trips and FallsSlips, Trips, and FallsMedication ReconciliationEmergency PreparednessEmergency PreparednessSharps SafetyD i P ti t & P id C fli tDecreasing Patient & Provider ConflictMissed Treatments 91

Program Benefits:Supports QAPI Activities related to CFCPromotes staff development and educationSupports national CMS goal to promote patient safetyParticipating facilities will be recognizedContact the Network is you are interested
92

Changes in Regulations: NewChanges in Regulations: New Requirements on Involuntary Discharges
Network Role
• To guide staff in dealing with conflict situations appropriately and consistently andsituations appropriately and consistently and in accordance with CMS guidelines
• To protect the rights of patients under the Federal Regulations
• Assist providers meet the New Conditions for Coverage
94
Coverage

Involuntary Discharges
Involuntary Discharges should only occur as a last resort and only when all other forms oflast resort and only when all other forms of intervention have been exhausted.
95

Definition of Involuntary Discharge
Patient has been discharged or is asked to transfer-out from the facility against his/hertransfer-out from the facility against his/her will. A patient is considered involuntarily discharged if they have received written ordischarged if they have received written or verbal notice that they will no longer be allowed to receive dialysis at your facilityallowed to receive dialysis at your facility.
96

494 70 C di i P i ’ Ri h494.70 Condition: Patient’s Right Be informed regarding transfer and dischargingBe informed regarding transfer and discharging policies
Be informed of facility's policies for transfer routine orBe informed of facility s policies for transfer, routine or involuntary discharge, and discontinuation of servicesReceive written notice 30-days in advance of an yinvoluntary discharge, after the facility follows the involuntary discharge procedure described in 494-180 (f) (4)(4) In the case of immediate threats to the health and safety of others an abbreviated discharge procedure may be
97
of others, an abbreviated discharge procedure may be allowed
494 150 C diti494-150 Condition: Responsibilities of Medical Director
Policies and procedures the medical director must:Be responsible to assure all staff physicians andBe responsible to assure all staff, physicians, and non-physician providers “adhere” to all policiesBe engaged in any involuntarily patient transfer orBe engaged in any involuntarily patient transfer or dischargeMust ensure that the reasons for involuntaryMust ensure that the reasons for involuntary discharge or transfer are consistent with the requirement
98

494.180 Condition: Governance
Involuntary discharge transfer policies andInvoluntary discharge, transfer policies, andprocedures
The medical director ensures that no patient is dischargedThe medical director ensures that no patient is discharged or transferred from the facility unless1. The patient or payer no longer reimburses p p y g2. The facility ceases to operate3. Is necessary for the patient’s welfare; facility can no
longer meet the patient’s needs4. The patient’s behavior is disruptive and abusive to the
extent that the delivery of care to the patient or the
99
extent that the delivery of care to the patient or the ability of the facility operations is seriously impaired

494 180 C diti G ( t )494.180 Condition: Governance (cont.)
Efforts to resolve the problem are documented as well as on-going problemsMust have a written physician order signed by both theMust have a written physician order signed by both the medical director and patient’s attending physicianProvide a 30-day written notice to the patient with copyProvide a 30 day written notice to the patient with copy to the local ESRD NetworkContact other facilities in attempt to place the patient and documents that effortNotify the local ESRD Network and State Survey A f h i l di h f
100
Agency of the involuntary discharge or transfer
R iReporting
When the decision to involuntarily discharge aWhen the decision to involuntarily discharge a patient is made, please do the following:
• Notify the Patient Services Department at Network 18 to review the situation and decision
• Fax or mail a copy of the discharge letter and• Fax or mail a copy of the discharge letter and all documents on the involuntary discharge checklist after speaking with the Patient
101
checklist after speaking with the Patient Services Department

Reporting (cont.)
R h i l di h h• Report the involuntary discharge on the monthly Patient Activity Report (PAR) under
t “6 ” ( t C i th l l )event “6c” (category C in the losses column)• Use this event for all involuntary discharges
regardless of where the patient received services after discharge. As the business rule f h N k l d T ffor the Networks related to Transfer-out-Category C reads: “Patient has been di h d f f ilit i t hi /h ill”
102
discharged from facility against his/her will”
Involuntary Discharge Guidelines
Facility must have and follow written policiesFacility must have and follow written policies and procedures for involuntary discharge and transferstransfersSurveyors will review patient’s individual
d li i h l irecords to ensure compliance with regulation and facility policy
103

Involuntary Discharge Guidelines
Facility can only involuntary discharge or transfer a patient for those reasons listed in 494.180 of Condition for Coverage:1. The patient or payer no longer reimburses
the facility for the ordered services2. The facility ceases to operate3. The transfer is necessary for the patient’s
welfare because the facility can no longer
104
meet the patient’s documented medical needs

Involuntary Discharge Guidelines (cont.)
4. The facility has reassessed the patient and determined that the patient’s behavior is di ti d b i t th t t th t thdisruptive and abusive to the extent that the delivery of care to the patient or the ability of the facility to operate effectively is seriouslythe facility to operate effectively is seriously impaired.
Th t b itt d b th tt diThere must be a written order by the attending physician and the Medical Director for the facility to involuntary discharge or transfer a
105
facility to involuntary discharge or transfer a patient

Guidelines: Interpretive Guidance
N P t f FNon-Payment of FeesThere must be evidence in the patient’s medical record that facility staff (e.g. billing personnel, financial counselor, social worker) made good f ith ff t t h l th ti t lfaith efforts to help the patient resolve non-payment issues
106
Guidelines: Interpretive Guidance (cont.)
Facility Ceases to OperateGoverning body must notify CMS, State g y ySurvey Agency and applicable ESRD NetworkFacility interdisciplinary team must assist patients to obtain another facilitypatients to obtain another facility
107

Guidelines: Interpretive Guidance (cont.)
Discharge or Transfer for Patient’s WelfarePatient’s medical record must include documentation of the medical need and reasons why facility no longer meet that needy y g
108

Guidelines: Interpretive Guidance (cont.)
Determined that Patient’s Behavior is Disruptive/Abusive
Patient’s should not be discharged for failure to comply with facility policy unless the p y y p yviolation adversely affects clinic operation (e.g. violating facility rules for eating during ( g g y g gdialysis should not warrent a discharge)
109

Guidelines: Interpretive Guidance (cont.)
Patients should not be discharged for shortened or missed treatments unless behavior has a significant adverse effect on other patient’s treatmentpPatient’s should not be discharged for failure to reach facility set goals for clinical y goutcomes
110

Immediate Discharge(According to Interpretive Guidance)
Defined: “Immediate Severe Threat” considered to be a threat or physical harm. The health and safety of other patients or staff are at risk.
Ex: If a patient has a gun or a knife or is makingEx: If a patient has a gun or a knife or is making “credible” threats of physical harm. (This considered an “immediate severe threat”))
An angry verbal outburst or verbal abuse is not considered to be an immediate severe threat
111
considered to be an immediate severe threat.

Abb i t d I l t Di h P dAbbreviated Involuntary Discharge Procedure(According to Interpretive Guidance)
Immediate protective actions: call “911” ask for police assistanceNo time or opportunity for reassessment, intervention, or contact with another facility for transferStaff must notify the patient’s physician and
di l di t ( bt i i tmedical director (obtain signatures as soon as possible after the event)
112

Abb i t d I l t Di h P d ( t )Abbreviated Involuntary Discharge Procedure (cont.)(According to Interpretive Guidance)
Staff must notify the State Agency and ESRD Network of the involuntary discharge (please also contact your risk management/legal department)Document the contacts made and the exact nature of the “immediate severe threat”the immediate severe threatContinue to follow remaining involuntary discharge guidelinesguidelines
(Provider may use their own abbreviated
113
involuntary discharge procedure as long as it meets interpretive guidance)

Abb i t d I l t Di h P d ( t )Abbreviated Involuntary Discharge Procedure (cont.)(According to Interpretive Guidance)
A 30- Day notice is not required in the case of imminent severe threat to safety of other patients or staffGoal of contacting another dialysis facility is for continuity of care the HIPPA privacy rule does notcontinuity of care, the HIPPA privacy rule does not require patient consent to contact another dialysis facility. However, does limit sharing of protectedfacility. However, does limit sharing of protected health information to medical records requested by the other provider and prohibits sharing information
114
obtained through hear say.
I l Di h R iInvoluntary Discharge Requirements(According to the Conditions for Coverage)
1. Notify the Network of the potential IVD2. Provide the patient with a 30- day notice planned
discharge3. Copy of medical records documented:
On going problemOn going problemImpact of the problem on other patients/staff, if anyanySteps to resolve the problem (include behavioral contracts and patient/staff meetings
115
Patient response to each step taken and the reassessment of the situation
I l Di h R i ( )Involuntary Discharge Requirements (cont.)(According to the Conditions for Coverage)
4. Written physician’s order signed by both medical director and patient’s attending physician agreeing with the discharge
5. Send all contracts, letters of notification of discharge or other written communication with the patient toor other written communication with the patient to the Network
6. Contact another facility, attempt placement, and6. Contact another facility, attempt placement, and document efforts
7. Notify State Survey Agency
116

I l Di h R i ( )Involuntary Discharge Requirements (cont.)(According to the Conditions for Coverage)
8. In case of immediate severe threat to the health and safety of others, the facility may use an abbreviated procedure
9. Report the patient as an IVD (6c) in the monthly PAR (patient activity report)PAR (patient activity report)
117
C f C S IVDC of C: Summary on IVD1. Facility must have a 4. Attempts to find placement y
patient discharge/transfer policy & procedure
2. Medical Director has
p pfor the patient and documents the effort
5 N tifi th t t2. Medical Director has oversight to ensure appropriate reason for discharge or transfer
5. Notifies the state survey agency and ESRD Network of the involuntary transfer or discharge or transfer
3. Must have a written physicians order that must be signed by both the
discharge6. In case of immediate severe
threats to the health andbe signed by both the medical director and patient’s attending physician concurring with
threats to the health and safety of others, the facility may utilized an abbreviated
118
physician concurring with the patient’s discharge or transfer
involuntary discharge procedure
Fi l StFinal Steps
When the decision to involuntary discharge has
• The facility should inform their legal counsel of the decision t i l t di h d th ( ) f it
When the decision to involuntary discharge has been made, the following steps should be taken:
to involuntary discharge and the reason (s) for it
• Notify the patient in writing. Send copies of the letter to the patient via certified mail return receipt requested and viapatient via certified mail, return receipt requested, and via regular mail, or present to the patient in person
• A last treatment date is set in writing. The patient must be g pgiven reasonable notice, thirty (30) days as directed by Conditions of Coverage
A th ti t th t th f ilit ill ti t id
119
• Assure the patient that the facility will continue to provide treatment up to the termination date period, unless patient behavior warrants immediate discharge
Fi l St ( t )Final Steps (cont.)• Attempt to find placement for the patient. If patient refuses p p p p
assistance provide a list of facilities for the patient to contact for placement
E h i t th ti t i t f fi di th• Emphasize to the patient importance of finding another facility and/or physician for continued care
• The Administrator/Medical Director should ensure that all• The Administrator/Medical Director should ensure that all steps taken are consistent with federal regulations, state law, and corporate/facility policy
• Involuntary Discharge should not be used by the facility to remove a patient who is non-adherent with diet, medication, etc.
120• Not the responsibility of the dialysis staff to end the
physician/patient relationship
Physician Terminates Relationship
• Physician (Nephrologist) provides a 30-day notice on his/her letter head with date of last day
• Documents in medical record reason for discharge
• Provides the patient/family a list of other nephrology groups in the area
• Involuntary Discharge should not be used to remove a patient who is non adherent with diet medication etcwho is non-adherent with diet, medication, etc.
• Follows the rest of the involuntary discharge requirements
121
CROWNWeb Implementation
QIPS Forms
Phase I Results
Phase II Preparation
Phase I Results
Phase II Preparation
122
O er ie and Agenda for QIPS/CROWNWeb Training
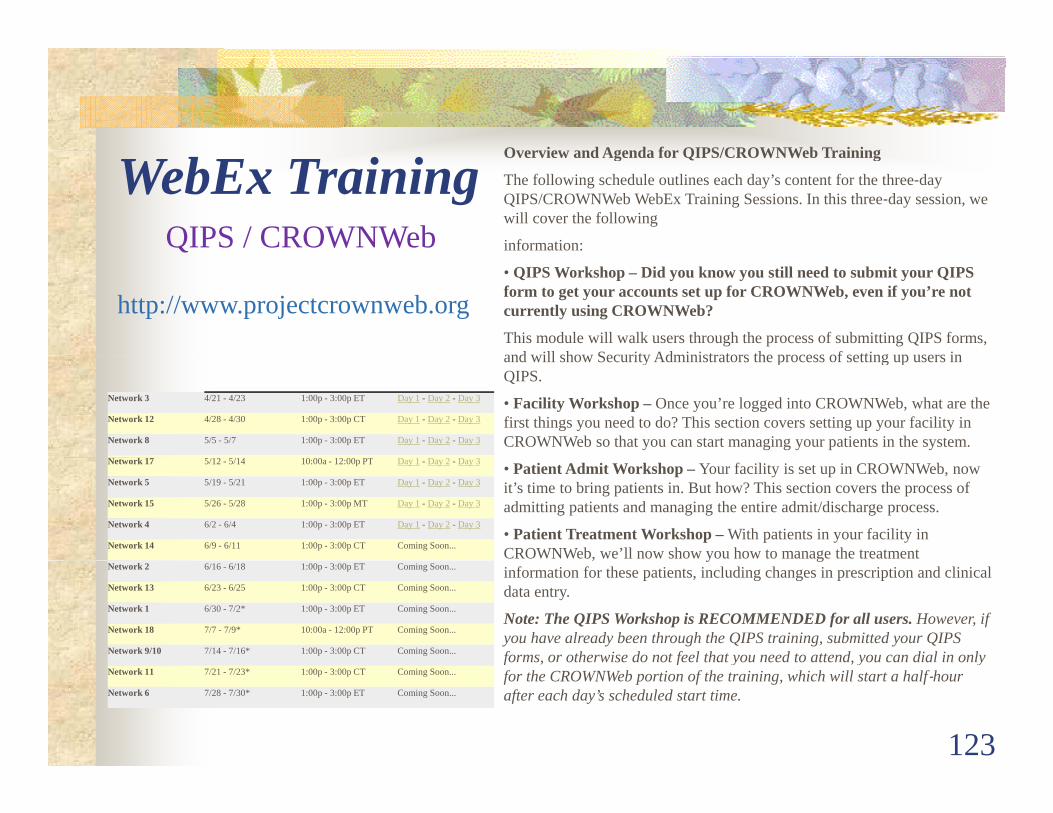
WebEx Training Overview and Agenda for QIPS/CROWNWeb Training
The following schedule outlines each day’s content for the three‐day QIPS/CROWNWeb WebEx Training Sessions. In this three‐day session, we will cover the following
information:QIPS / CROWNWeb• QIPS Workshop – Did you know you still need to submit your QIPS form to get your accounts set up for CROWNWeb, even if you’re not currently using CROWNWeb?
This module will walk users through the process of submitting QIPS forms, and will show Security Administrators the process of setting up users in
http://www.projectcrownweb.org
Q
Network 3 4/21 - 4/23 1:00p - 3:00p ET Day 1 - Day 2 - Day 3
Network 12 4/28 - 4/30 1:00p - 3:00p CT Day 1 - Day 2 - Day 3
Network 8 5/5 - 5/7 1:00p - 3:00p ET Day 1 - Day 2 - Day 3
N k 17 5/12 5/14 10 00 12 00 PT D 1 D 2 D 3
and will show Security Administrators the process of setting up users in QIPS.
• Facility Workshop – Once you’re logged into CROWNWeb, what are the first things you need to do? This section covers setting up your facility in CROWNWeb so that you can start managing your patients in the system.
Network 17 5/12 - 5/14 10:00a - 12:00p PT Day 1 - Day 2 - Day 3
Network 5 5/19 - 5/21 1:00p - 3:00p ET Day 1 - Day 2 - Day 3
Network 15 5/26 - 5/28 1:00p - 3:00p MT Day 1 - Day 2 - Day 3
Network 4 6/2 - 6/4 1:00p - 3:00p ET Day 1 - Day 2 - Day 3
Network 14 6/9 - 6/11 1:00p - 3:00p CT Coming Soon...
• Patient Admit Workshop – Your facility is set up in CROWNWeb, now it’s time to bring patients in. But how? This section covers the process of admitting patients and managing the entire admit/discharge process.
• Patient Treatment Workshop – With patients in your facility in CROWNWeb, we’ll now show you how to manage the treatment
Network 2 6/16 - 6/18 1:00p - 3:00p ET Coming Soon...
Network 13 6/23 - 6/25 1:00p - 3:00p CT Coming Soon...
Network 1 6/30 - 7/2* 1:00p - 3:00p ET Coming Soon...
Network 18 7/7 - 7/9* 10:00a - 12:00p PT Coming Soon...
Network 9/10 7/14 - 7/16* 1:00p - 3:00p CT Coming Soon...
, y ginformation for these patients, including changes in prescription and clinical data entry.
Note: The QIPS Workshop is RECOMMENDED for all users. However, if you have already been through the QIPS training, submitted your QIPS forms, or otherwise do not feel that you need to attend, you can dial in only
123
Network 11 7/21 - 7/23* 1:00p - 3:00p CT Coming Soon...
Network 6 7/28 - 7/30* 1:00p - 3:00p ET Coming Soon...
f , f y , y yfor the CROWNWeb portion of the training, which will start a half‐hour after each day’s scheduled start time.

Communication!
PHI PII
124
PHI PII

COMPLIANCE
CMS-2728 Patient AddressPatient Address
Facility InformationCMS-2746
Monthly PAR
Vascular Access LogCMS-2744
E
Involuntary Discharge
Emergency Preparedness
125
Discharge

126

Harriet L Edwards MSW/ MSG Executive DirectorHarriet L. Edwards, MSW/ MSG, Executive [email protected]
Svetlana (Lana) Kacherova, RN, MPH, CPHQ, QI [email protected]@nw18.esrd.net
Cecilia Torres-Correa, RN, BSN Patient Services Director [email protected]
Patrick Ciriello, MSIM, IS Director
6255 S t B l d S it 2211 L A l CA 90028
127
6255 Sunset Boulevard • Suite 2211 • Los Angeles • CA • 90028(323) 962-2020 • (323) 962-2891/Fax • www.esrdnetwork18.org


















