esophagus: Case report anddownloads.hindawi.com/journals/cjgh/1993/378058.pdf · Heterotopic...
7
CASE RECORD Heterotopic gastric mucosa in the esophagus: Case report and discu ss ion CY SrREAn , MD, RJ RAILEY , MD CY SPREAD, RJ B AI LEY. H eter otopic gast ric mucosa in the eso ph agus: Ca se report and discussion. Ca n J Gastroenterol 1993;7(8):589-594. The case of an elderly man with hete ro top ic gastric mucosa of the ce rvi ca l esoph agus associ- ated with an esophageal web, as well as a d iscussion o fh ete rotopic gastric mucosa, arc presented. T he presen ce of an 'inlet patch ' is a commo n e ndoscopic fi nd in g; abo ut 10% of the popul at i on will have the hctcrotopic mucosa just below the upper esophageal sphinc te r. Al though there is controversy regarding pathogene- si s, a congenita l orig in is fa voured over an acquired lesion, The parches may be single, multiple or circu mf erent ia l. Histol ogica lly, just ove r half arc ectopic gast ric fu ndic mucosa and 90% of the patches contain bo th parietal and c hief cells. Most patie nts with the inlet patch remain asy mptomatic; about 1 5% w ith have mild pharyngea l discomfort and/or high d ys phagi a. Sy mptoms will often accompa ny the deve lo pme nt o f a co mplication, such as ulceration, that may be associated wit h bl eed in g, a s tricture at the squ amoco lumnar j unction or an eso phageal web. Diagn ostic mano eu vres to id e nt ify the mucosa include barium studies, end oscopy, Co ngo red sraining to visualize acid production and nuclea r medicine sca ns. No tre atmen t is necessary unless co mp lica tions d eve lop. Com- pl i cat ions can be treated successfu lly with Hz bl ock e rs a nd/o r endoscopic d il a- tion. No fo ll ow-up appea rs to be necessary as there is no proof fo r malignant transfo rma tion of the ectopic mucosa. Key Words: Abe rrant gas tric mucosa, Ectopic gas tric mu cosa, Inlet paic li , Up/)er esop/iageal web Mugueuse gastrique heterotope au niveau de l'oeso phage: Rapport de cas et discussion RESUME : Le cas d' un vieillard prese nta nt une muqueuse gastrique hetcrotopc au niveau Je l'oesoph age ce rvi ca l associ ee au tissu oesoph agicn est presence ici, avec une d i scuss ion sur la muqueuse gastrique het eroto pe. La presence d 'e nclaves pres de ['o rifice d' e ntrec n'est pa~ un phenomene rare a !'e ndoscopic; environ 10 % de la pop ul ation prcse ntera un 1m1queuse hcte rotopc juste sous le sphincter oesoph agien superi eu r. Bien qu'il y ait une concrovcr se au suj et de sa pa thogcnese, on privilegie en gene rale l'e ci ol og ie co ngenitale plutot qu' acquise. Les e ncla ves peuvent etre uniques ou multiples, ou enco re, circonf erentie ll es. Au plan histolo- gique, un peu plus de la mo itie prov ie nn en t de muqucusc gastrique fundique ectopique et 90 % d es e nclaves renfcrment des ce llul es gastri ques pr incipales ct Coms r,1 mdc 11 ce: /)r R./ Bailey, Suite 3 1 0, 1101 0- 10 I Stree t, E dmomm,, Alhena TS /-/ 4B9 R eceived for /nihlic(l[ion) une 30. 1992. Accer,r e cl AJ>ril 15 , 1993 CAN J G ASTROENTERl) I. VOL 7 Nt) 8 N UVE MBER/D ECFMRER 1993 H f'TERl)TOl'l( '( ,ASTRl< 'MU(\)S:\ IS a c om nHin endoscopic finding in th e ce rvical e~n phagus 1( the mucosa lying just hcnc, ll h th e upper c" ,ophageal sphincre r (UES) is carefully examined. Alt h Li ugh pnrients with :m 'inl et patch' are usu.illy asymptoma r ic , r;i re comp li- cations me ide nt ified. The authllrs rL'- port a case of an eso ph ngeal web wirhi n a patch of hctcrrn opic ga~tr ic mu cosa (including diagnostic ~tud ie s and pa- rlw logy) and hr ic!ly discus:- this tnpic. CASE PRESENTATION A 79-yc ar-o ld man wa s seen in c on - sultat inn hccnuse of ,, single episudc nf d ys phagia. The p,11 ient was eat ing wh en he felt a holus of mea t stick in h is throat . The sensat ion wa:; fel t in the throat rather th an the chest, and was not accompani ed by pain. The sensa- tion co n ti nued fo r 12 h, then com- pletely resolved, and he w,1s able to ca t again wi thout an y difficulty. Further questioning reveal ed that fo r the previous month, the patient wa s consta n t ly hot hcrcd by a n ee d to clear his thrnat. Otherwise, he deni ed any sympto ms. I le had no past his tory of u lc ers or ga strnesophageal re fl ux dis- ea sr . T he patient wa s exceedingly healthy fo r his age. I le had no serious illnesses, previously ha d minor surgery on ly c1 nd was on no medi cat ions. l le ha d smoked one-half tn one pack of cigaret res per d ay f or at least 60 ye ars
Transcript of esophagus: Case report anddownloads.hindawi.com/journals/cjgh/1993/378058.pdf · Heterotopic...

CASE RECORD
Heterotopic gastric mucosa in the esophagus: Case report and
discussion
CY SrREAn , MD, RJ RAILEY, MD
CY SPREAD, RJ B AILEY. H eterotopic gastr ic mucosa in the esophagus: Case repor t and discussion . Can J Gastroenterol 1993;7(8):589-594. The case of an elderly man with hete rotopic gastric mucosa of the cervical esophagus associated with an esophageal we b, as well as a d iscussion ofheterotopic gastric mucosa, arc presented. T he presen ce of an ' in le t patch ' is a commo n endoscopic finding; about 10% of the population will have the hc tc ro topic mucosa just below the upper esophagea l sphincter. Although th ere is controversy regarding pathogenesis, a congenital origin is favoured over an acquired lesion, The parches may be single, multiple or c irc umferentia l. His tologically, just over ha lf a rc ectopic gastric fundic mucosa and 90% of the pa tches conta in both parie ta l and chief cells. Most patients with the inlet patch remain asympto matic; about 15% with have mild pharyngeal discomfort and/or high dysphagia. Symptoms will often accompa ny the deve lopment of a comp lication, such as ulceration , that may be associated with bleeding, a stricture at the squamocolumnar junctio n or an esophageal web. Diagnost ic manoeuvres to identify the mucosa include barium studies, endoscopy, Congo red sra ining to visua lize ac id production and nuclear medic ine scans. No treatmen t is necessary unless complications develop. Compl ications can be treated successfully with H z blocke rs and/or e ndoscopic dilation. N o follow-up appears to be necessary as the re is no proof for malignan t transformation of the ectopic mucosa.
Key Wo rds: Aberrant gastric mucosa, Ectopic gastric mucosa, Inlet paicli , Up/)er esop/iageal web
Mugueuse gastrique heterotope au niveau de l'oesophage: Rapport de cas et discussion
RESUME : Le cas d 'un vie illard presentant une muqueuse gastrique hetcrotopc au niveau J e l'oesophage cervical associee a u t issu oesophagicn est presence ic i, avec une d iscuss ion sur la muqueuse gastrique h eterotope. La presence d 'enclaves pres de ['o rifice d'entrec n'est pa~ un phen omene rare a !'endoscopic; environ 10 % de la popula tion prcsente ra un 1m1q ueuse hcte rotopc juste sous le sphincter oesophagien supe rieur. Bien qu'il y a it une concrovcrse au sujet de sa pa thogcnese, on privilegie en generale l'eciologie congeni ta le pluto t qu'acquise. Les enclaves peuvent etre uniques ou multiples, ou encore , c irconferen tie lles. Au plan histologique, un peu plus de la moit ie proviennen t de muqucusc gastrique fundique ectopique et 90 % des enclaves renfcrmen t des cellules gastriques princ ipales ct
Comsr,1mdc11ce: /)r R./ Bailey, Suite 310, 11010- 10 I Street, Edmomm, , Alhena TS/-/ 4B9 Received for /nihlic(l[ion)une 30. 1992. Accer,recl AJ>ril 15, 1993
CAN J GASTROENTERl)I. VOL 7 Nt) 8 N UVEMBER/D ECFMRER 1993
H f'TERl)TOl'l( ' ( ,AST Rl< ' MU(\)S:\ IS
a comnHin e ndoscopic finding in the cervica l e~nphagus 1( t he mucosa lying just hcnc,ll h the uppe r c",ophageal sphincrer (UES) is ca refully examined. AlthLiugh pnrien ts with :m 'inlet patch' are usu.illy asymptomar ic , r;i re complications me identified. T he authllrs rL'port a case of an esophngea l web wirhi n a patch of hctcrrn opic ga~tric mucosa ( inc lud ing d iagnost ic ~tud ies and parlwlogy) and hric!ly discus:- t his tnpic.
CASE PRESENTATION A 79-ycar-old man was seen in con
sul tat inn hccnuse of ,, single episudc nf dysphagia. T he p,11 ie nt was eat ing when he felt a holus of mea t st ick in h is throat . The se nsat ion wa:; fel t in the t hroat rathe r than the chest, and was not accompanied by pain. The sensation con ti nued for 12 h, then completely resolved, and he w,1s able to cat aga in wi thout any diffic ulty.
Further questioning revealed that for the previous month , the pat ient was constant ly hothcrcd by a need to clear h is thrnat. O therwise, he denied any symptoms. I le had no past history of ulcers or gast rnesophageal refl ux diseasr.
T he patien t was exceedingly hea lthy for his age. I le had no serious illnesses, previously had minor surge ry on ly c1 nd was on no medicat ions. l le had smoked one-half tn one pack of cigare t res pe r d ay for at least 60 years

SPREAD AND BAILEY
bordantes. La plupart des patients por teurs de telles enclaves demeurent asymptomatiques; enviro n I 5 % souffri ronr d 'un lcger inconfort pharyngc ou d'une importance dysphagie. Les symptomes accompagneron t souvent le J eveloppement d'une complication , comme !'ulceration , avec possiblement hcmorragie et stric tures a la jonction des cellules epidermo'ides et J es cellu les a p lateau st rie ou du tissu oesophagien. Les techn iques diagnostiqucs pour identi fie r la muqueuse incluent !cs eprcuves au baryum, l'endoscopie et la coloration a u rouge Congo pour visualiser la production d'acide et les scintigraphies en medecine nuclcairc. A ucun tra itemen t n 'cst necessaire a moins que n 'appara issen t des complications. Les complications peuvent etre cra itees avec succes a l'a ide d 'anci-H z ou de dilatations e ndoscopiques. A ucun suivi ne semble necessaire puisque rien ne tend a demontrcr qu'il y aurait evolu tion vers une neoplusie a partir de muqucuses eccopiques.
a nd usua lly hctd one drink per day. Prior to retiring from work, he had been a carpenter.
Phy~ical examination revealed a th in man in excel lent shape. The examination was completely normal. I nvestigations: The initial investigation was a barium swallow. This study revea led a small web on the left s ide of the esophagus at the region o( the Lhoracic inle t and, just inferior to the web, a small area of c irc umferential narrowing of the esophagus with ulce ration anteriorl y. The lower esophagus was no rmal with no ev idence of hiatus hernia or reflux (Figu re 1 ).
The next investigat ion was esophagogastroscopy. The ororharynx was normal. Upon entering the esophagus, gastri c mucosa was iden t ified begi nning l cm below the UES (Figure 2). The patch of gastric mucosa was c ircumfcremial and was 2 cm in length (19 to 21 cm from the incisors). At 20 cm, the scope passed through a defin ite narrowing of the esophagus which resembled a web. The remainder of the esophagus was normal in appearance. The gastroesophageal junct ion occ urred at 39 cm; a small I to 2 cm hiatus hernia was abo identified . Bior sics were taken from the normal mucosa above the patch, from the patch and from the gastroesorhageal junction. Congo red srnining was used to demonstrate acid product ion by the 'inlet
patc h'. The patient was given 250 µg pentagastrin, and an endoscope was aga in passed into the esophagus 40 mins later. The ratch was first washed with 20 ml 4.5% sod ium bicarbonate
solution, then irrigated with 10 mL I % Congo red solution . Ten minutes after the Congo red irrigation, only a very smal l patch of black sta ined mucosa was identified (Figure 3 ), representing a sma ll area o( acid production.
Gastric mucosa! imaging (99m Tcpertechnetate scintigrarh y) was carried out wiLh multiple images of the cervical area and uppe r thorax. Tomographic imaging and three-d imensional reconstruction revealed an abnormal focus of inc reased uptake in the upper esophagus behind the lowe r pole of the thyrnid gland. This was thought to represent the area of ectopic gastric mucosa (Figure 4) . Path ology: The presence of a patch of gastric mucosa in the cervical esophagus was confirmed by light microscopy (Figure 5). The inle t patch was like ly antral in type (Figure 6), with on ly occasional parietal cells ide ntified and no chief cells. lmmunopcroxidasc staining for gastrin, bombesin and somaLOsrntin was carried out. The gastrin and bombesin stains were negative wh ile the biopsies fro m the mucosa! patch stained positively for somatostatin. Mild esophagitis was found in the surrounding squamous mucosa. There was no evidence of esophagi tis or Barrett's change in biopsies from the lower esophagus of the patient. Treatment: The web was easily Jilated with a 60 French dilator during the initial esophagogastrnscopy. The patient experienced relief from his symptoms after the dilation and remains completely asympLomaLic afte r one year of follow-up.
DISCUSSION I le terotopic gast ri c mucosa has been
identified throughout the gast ro intesti na l tract (oral cavity, esophagus, small bowel, Meckel's diverr icula, appendix and rec LUm) as well as in the gallhladder, pancreas, sl1 livary glm,ds, umhilicus and spinal cord ( I). It has also been found in small pa tches, ;is the lining of such anomalies as extrainLest inal cys ts and duplications (2), and in rhc esophageal pnuch of Lracheoesophageal fistulas (3). Incidence: Aberrant gastric mucosa or the inlet pa1ch in the upper third of the esophagu~ was first dcscrihed hy Schmidt ( 4) in 1805. Accordi ng ll) sporadic reports up to 1927, the inc idence of ecropic gastric mucosa in the esophagus varied from 0.67 to 70 '>h (5). A 1904 study by Schridde ( 6) lcx,ked at
the inlet of the esophagus alone and with minute serial sect ions. I le found heteroropic gastric glands or mucosa in 70% of patienrs studied. Most of the glands lay beneath normal squamo us mucosa; only 20'M, were surface patches (6). Rector and Connerley (5) puhlish ed the firsL extensive autopsy study in 194 l , examining IOOO infants and children by random section only-1 1.8% of cases had some type of ahe rrant gastric mucosa present in the esophagus. with 8% of the lesions within the lower third of the esophagus, 41 % in the middle th ird , and 51 % in th e upper th ird, and usua lly at or just below the UES.
More recent studies have attempted ro est imate the more useful prevale nce of heterotopic gastric mucosf1 n( the esophagus visible to the n aked eye. A 10% incidence of inlet patches was found on gross inspection al autopsy of the esophagi of 300 infants and chil dren aged birth ro 14 years (7). Endoscopically, prevale nces of 3.8 and 10% have been found during 420 and 634 consecutive upper gm,trointestinal studies, respectively (8,9). Most of the lesions were less than I cm in diamecer and asymptomatic, and most were ll)catcd jusl below the UES (approxima tely 15 to 20 cm from the incbor teeth). The inle t patch in nur patient was located in this L ypical local inn , just beneath the UES.
590 CAN J GASTilOENTERllL VU! 7 Nt) 8 N,Wl:MIWR/DH'FMBFR 1991

Heterotopic gastric mucosa in the esophagus
Figure 1) Barium swallow study revealing a small iveb on the lefr side of the esophagus at the tharacic in/er and, just inferior w rhe web, a small area of circumferenrial narrowing of the esophagus t<'ith ulceration cnueriorly
Figure 2) Hererowpic gmrric mucosa (inlet (>atch) in the cervical eso/1/iagi1s 1howing a/rn1pr junction of gastric and e.1opliageal mucosa
Figure 3) Congo red sraining of rhe inlet />atch showing a small area of acid /Jroduction
Pathogenesis: Controversy has surrounded the pa thogenesis of heterotopic gastric mucosa of the esophagus. When locatcJ in the lower third of the esophagus, often called BarreLt's esophagus, Lhe mucosa appears to be acquired secondary to reflux of gastric acid, injury ro the squamous mucosa and metaplas ia. For he temtopic gastric mucosa found at the UES, most authors favour a congenital origin, although this has heen cha llenged , especially when concurrent Barreu's esophagus has been identified.
Weaver, a proponent of nn acquired origin for heLerotopic gastric mucosa,
Figure 4) A comtiosite phowgra/>h of rhe gastric mucosa/ imaging (99m Tc-/,enechnetace 1cinrigraphy) . On the lefr is the anterior view of the neck and un the righr (lower />howgi·a/>h) is rhe lateral view, both showing a disrincr area of u/>tal<.e in the cervical esophagus, se(>arate (f)()~tericn· and mf eriur) from the rhyroid gland
proposed that the UES may form a distinct barrier to reflux and, therefore, ulceration occurs just below the UES, with re-epithelialization of the damaged area with more acid-resisLant gastric mucosa ( LO).
Support for a congenital origin of heterotopic gastric mucosa includes scuJies of embryology, the low rare of concurrent Barren's esophagus and the
histology of the gastric gland~. Embryo logically, the patches are fe lt to be sequestered islands of gastric mucosa remaining in the esophagus after replacement of the early columnar mucosa hy stratified squamous epi thel ium (5). The gastric swell ing forms an<l descends from the 4 to 17 mm stage in the embryo. Ry Lhc 40 mm stage, the trarified columnar epithelium of the primi-
CAN) 0ASTROENTERl1L VOi 7 No 8 NOVEMBER/DECEMBER 1993 591

SPREAD AND B AILEY
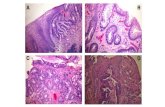
Figure 5) Low Jiower view of the antral ty/)e lieterotopic gastric mucosa identified in tlie Jlresentecl patient ( liemawxylin and eosin , XI 00)
Figure 6) Antral mucosa of clie inlet J>atch showing occasional parietal cells (am>w) and no chief celL1 (hematoxylin and eosin, x400)
Live esophagus is replaced by c iliated columnar epithelium, and by the 130 mm stage, the c iliated epithelium i~ replaced by srratified squamous mucosa, first appearing in the middle third of the esophagus and progressing cephalad and caudad ( I ! ).
As further support for a congenital origin, concurrent Barrett's esophagus is not frequently identified; only five of 64 patients with gastric mucosa in the upper esophagus had Barrett's change (9) and, in another study, one of 16 cases of heterotopic gastric mucosa had
concurrent Barrett's esophagus (8). Comparison of 21 l cases of heterotopic gastric mucosa with 354 cases of Barrett's change yielded only 12 patients with both abnormalities (1 2). In almost a ll the cases, a different type of gastric mucosa is identified for the upper esophageal patches and Barrett's esophagus, typically fundic glands or, occasionally, an tral mucosa is seen in heterotopic gastric mucosa while Barrett's change is usually cardiac-type mucosa (9). In agreement with a congenita l o rigin, our patient was thought
to have antral-type gastric mucosa in the cerv ical esophagus and no evidence of Barrett's esophagus. Pathology: 1-leterotopic gastric mucosa may be e ither localized or circumferential in distribution ( I 0, 13) - 45% are single, whi le 40% of the parches a re multiple and on opposite sides, and 15% are multiple and on the same wall of the esophagus (9). The pa1ch in our patient was single and c ircumferentia l.
Microscopically, columnar mucosa usually abuts abruptly on squamous mucosa. The appearance of the gastric pits define three types of gastric mucosa that may be idenrified: first, cardiac zone mucosa containing colloid glands lined with mucous-producing columnar epithelium, and some parietal and chief cells; second, mucosa of the body or fundus of the stomach with straight fundic-typc glands comaining pepsinsecreting ch ief cells and acid-secreting parietal cells in the lower half; finally, antral mucosa contain ing shorter, more tortuous glands fu II of G eel ls, no chief cells and very few parie tal cells. Cardiac-type mucosa usually is found with Barrett's esophagus near rhe ga~troesophageal junction. A thin body-type mucosa with fundic glands is seen in 52% of heterocopic gastric mucosa and a pure antral type in 20%. T he remainder of cases represent a mixture of fundic and antral glands (9). About 80 to 90% of inlet patches contain both parietal and chief cells (8, 14 ). Most of the specimens also show mild to mlxlerate ch ronic inflammation with lymphocytes and plasma cells, even in the few cases where parietal cells a rc not identified (5,8,15). ln the present case, examination of biopsies of the inlet patch revealed few parietal cells and no chief cells, most consistent with amral mucosa.
lmmunoperoxidase stain ing of lesions appears to lead to a different hormonal profi le in symptomatic and asymptomat ic patients, although this association was not confirmed in our symptomatic patient ( 16). Gastrin and bombcsin, b1)th staining negative in our patient, arc wbstances known to
stimu late acid secretion e ither directly or indirectly and seem to be found most frequently in symptomatic patients. Somatostatin, stain ing posirive in our
592 CAN J GASTROENTEROL VOL 7 No 8 NOVEMF\ER/DECEMI\ER 1993

Heterotopic gastric mucosa in the esophagus
patient, is known to block acid secretion and is found more frequently in asymptomatic patients. Presentation: Most people with ectopic gastric mucosa in the upper esophagus are asymptomatic. It would seem that in a minority of cases, some degree of inflammation and ulceration, possibly secondary to trauma or acid secretion, leads to dysphagia with or without complications. Based on the weak Congo red test and the histological finding of only a few parietal cells, it is unlikely that symptoms eventually developed in our patient from acid- induced ulceration. Even if significant acid is secreted, in most cases it appears to be neutralized by swallowed saliva (17). The reason why our patient suddenly became symptomatic after 79 years is unclear.
Recently, a role for campylobacterlike organisms has been proposed in heterotopic gastric mucosa of the upper esophagus (1 8). Although campylobacter-like organisms are rarely identified (5.3%), they appear to be associated with severe inflammatory changes in the patch. Unfortunately, no previous studies have attempted to correlate campylobacter- like organisms with symptoms. As our patient's patch was negative for Helicobacter pylori, no further conclusions can be drawn.
Overall, only 9% of patients with heterotopic gastric mucosa experience pharyngeal discomfort and 6% complain of high dysphagia (9). The mechanism of the dysphagia, if not accompanied by web formation or stricture, is not completely clear, but has been explained by increased cricopharyngeal UES muscle tone. Very rarely, the patch is pedunculated or polypoid and then may be associated with respiratory symptoms and aspiration (13,19,20). Diagnosis: Barium swallow will demonstrate no abnormality in uncomplicated heterotopic gastric mucosa, except in the rare situation when the lesion is polypoid. Barium is useful for symptomatic patients to help rule out a stricture, upper esophageal ring (Figure l) and the rare case of an adenocarcinoma.
Gastroscopy will demonstrate a vel-
very salmon- or red-coloured patch with a distinct border (Figure 2). The upper third of the esophagus is the most neglected area during the procedure and thus inlet patches may easily be missed. Blind introduction of the endoscope misses the area and the endoscope often is withdrawn rapidly at the completion of the procedure withoul adequate inspection. Repeated contractions of the UES require vigorous air insuffiation to visualize the area just below the sphincter (9). Lugol's solution can help to identify a suspected patch. The solution stains squamous mucosa brown, but does not stain the heterotopic gastric mucosa ( 14). Biopsy serves to confirm further the presence of heterocopic gastric mucosa.
During gastroscopy, acid production by the heterotopic mucosa can be demonstrated by Congo red staining (21). The Congo red technique was used in our patient, but due to the rarity of parietal cells, only a t iny patch of acid production was identified (Figure 4).
99m Tc-pertechnetate scintigraphy has been used to detect ectopic gastric mucosa, but its use has previously been confined to patients with a total thyroidectomy or those caking suppressive thyroid hormone supplements. In pat ients with a normal thyroid gland, there was overlapping activity between the uptake in the thyroid gland and the ectopic esophagea l mucosa, as both lie at the same level (22). As shown in Figure 3, using tomographic technique and three-dimensional reconstruction we were able to demonstrate the patch of heterotopic gastric mucosa in our patient, even though it lay behind a normally functioning thyroid gland. Complications: Heterotopic gastric mucosa of the upper esophagus can occasionally be complicated by bleeding or formation of a stricture, upper esophageal ring, adenocarcinoma or acquired trachesophageal fistula. Early stud ies also associate ectopic gastric mucosa with esophageal scars and as lead points for pulsion d iverticula.
Strictures are usually smooth and tapering, but must be biopsied to rule out malignancy. A circumferential, rather than localized, distribution of the gas-
CAN J GASTROENTEROL VOL 7 No 8 NOVEMBER/DECEMBER 1993
tric mucosa is associated with stricture formation, probably due to a greater localized reduction in pH and increase in peptic injury (5). Adenocarcinoma in a focus of ectopic gastric mucosa is exceedingly rare, with most authors doubting its existence. Carrie reported a case within the upper third of the esophagus in 1950 (23 ). Unlike the acquired Barrett's change, a recent study followed 211 patients with inlet patches for over six years and found that none progressed to adenocarcinoma (12). As a very rare complication, a trachesophageal fistu la has been reponed secondary to perforation of a peptic ulcer within a patch of heterotopic gastric mucosa (24 ).
The radiographic and endoscopic appearance in our patient is most consistem with a web or ring formation in tbe upper esophagus. In 1979, Weaver (10) first described a web in a patch of heterotopic gastric mucosa and proposed it as an alternate explanation for the Paterson-Kelly or Plummer-Vinson syndrome. The article included a case report of an elderly woman with severe dysphagia and a typical upper esophageal web on barium swallow, but no anemia. Gastroscopy revealed heterotopic gastric mucosa with a mucosa! ring at the junction of squamous mucosa and the band of gastric mucosa. Similarly, our panent had a web at the junction of squamous and gastric mucosa, and no anemia.
TREATMENT In the vast majority of cases, no
treatment is necessary. Routine need for follow-up and biopsy, as in Barrett's esophagus, is unnecessary as no proof for progression of the inlet patch to adenocarcinoma has been found (12).
For patients who are symptomatic, or if ulceration or possibly even acid production can be demonstrated on gastroscopy or with Congo red staining, treatment with Hz-blockers or omeprazole is warranted (20,25).
Strictures and upper esophageal rings are amenable to endoscopic dilation with good success, as seen in the presented case. Only very rarely will surgical management of complications be necessary.
593

SPREAD AND BAILEY
REFERENCES I. Wolff M. Heterotopic gastric
epithelium in the rectum: A report of three new cases with a review of 87 cases of gastric heterotopia in the alimentary canal. Am J Clin Pathol 1971;55:604-16.
2. Kaneko E, Kohda A, Honda N, Kino I. Incomplete tubular duplication of esophagus with heterotopic gastric mucosa. Dig Dis Sci l 989;34:948-51.
3. Emery JL, Haddadin AJ. Gastric-type epithelium in the upper esophageal pouch in children with tracheoesophageal fistula. J Ped Surg 1971 ;6:449-53.
4. Schmidt FA. De mammalium oesophago atque ventriculo. lnaug Oissert, Halle, in off. Batheana, 1805.
5. Rector LE, Connerley ML. Aberrant mucosa in the esophagus in infants and in children. Arch Path 1941 ;31 :285-94.
6. Schridde H. Uber magenschlelmhauc-lnseln vom bau der cardialdrusenzone und fundus drusenregion und den unteren, oesophagealen cardial drusen gleichen de drusen im oberscen oesophagusabschnitt. Virchows Arch Pathol Anac 1904;175:1-16.
7. Variend S, Howat AJ. Upper esophageal gastric heterocopia: A prospective necropsy study in children. J Clin Pathol 1988;41:742-5.
8. Jabbari M, Goresky CA, Lough J, Yaffe C, Daly 0, Cote C. The inlet patch: Heterotopic gastric mucosa in the upper esophagus. Gastroenterology 1985;89:352-6.
594
9. Borhan-Manesh F, FamumJB. Incidence of heterotopic gastric mucosa in the upper esophagus. Gut 1991;32-968-72.
10. Weaver GA. Upper esophageal web due to a ring formed by the squamocolumnar junction with ectopic gastric mucosa (another explanation of the Paterson-Kelly, Plummer-Vinson Syndrome). Dig Dis Sci 1979;24:959-63.
11. Johns BAE. Developmental changes in the esophageal epithelium in man. J Anat 1952;86:431-42.
12. Ollyo JB, Savary M, Monnier PH, er al. ls heterotopic columnar epithelium in the upper esophagus clinically relevant? Gastroenterology l 988;94:A333.
13. Raine CH. Ectopic gastric mucosa in the upper esophagus as a cause of dysphagia. Ann Oto! Rhino! Laryngol 1983;92:65-6.
14. Van Asche C, Rahm AE, Goldner F, Crumbaker 0. Columnar mucosa in the proximal esophagus. Gastrointest Enclose l 988;34:324-6.
15. TcherckoffV, Lee BY. Ulcerative esophagicis with hererotopic gastric mucosa. Am J Gastroencerol 1962;37:174-9.
16. Shah KK, DeRidder PH, Shah KK. Ectopic gastric mucosa in proximal esophagus: Its clinical significance and hormonal profile. J Clin Gastroenterol 1986;8:509-13.
17. Wang MM], Spear M, McGrew W. Heterotopic gastric mucosa of the esophagus. South Med J 1986;79:633-5.
18. Flejou JF, Poree F, Molas G.
Campylobaccer-like organisms in heterotopic gastric mucosa of the upper esophagus. J Clin Pacho! l 990;43:961. (Leet)
19. Powell RW, Luck SR. Cervical esophageal obstruction by ectopic gastric mucosa. J Ped Surg l 988;23:632-4.
20. Libcke JH. Heterotopic gastric mucosa in the cervical esophagus: A possible cause of fatal aspiration. Pediatrics 1969; 44:44 7-8.
21. Hamilton JW, Thune RG, Morrissey JF. Symptomatic ectopic gastric epithelium of the cervical esophagus: Demonstration of acid production with Congo red. Dig Dis Sci 1986;31:337-42.
22. Chen CH, De Ridder PH, Fink-Bennett 0, Alexander TJ. Detection of hecerotopic gastric mucosa in the upper esophagus with 99m Tc-pertechnectace scintigraphy. J Clin Gasrroenterol 1989;11:23-5.
23. Carrie A. Adenocarcinoma of the upper end of the esophagus arising from ectopic gastric epithelium. Br J Surg 1950;37:474.
24. Kohler 8, Kohler G, Riemann JF. Spontaneous esophagotracheal fistula resulting from ulcer in heterotopic gastric mucosa. Gastroemerology 1988;95:828-30.
25. Truong LO, Stroehlein JR, McKechnie JC. Gastric heteroropia of the proximal esophagus: A report of four cases detected by endoscopy and review of the literature. Am J Gastroenterol 1986; 81:1162-5.
CAN J GASTROENTEROL VOL 7 NO 8 NOVEMBER/DECEMBER 1993

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com