Esophageal Perforation in a Labrador Retriever Case Study: Make ...
20
Volume 10 Issue 1 • 2016 Esophageal Perforation in a Labrador Retriever See page 4 Case Study: Make Your Diagnosis See page 8 Medical Math: Constant Rate Infusion See page 16
Transcript of Esophageal Perforation in a Labrador Retriever Case Study: Make ...

Volume 10 Issue 1 • 2016
Esophageal Perforation in a Labrador Retriever See page 4
Case Study: Make Your DiagnosisSee page 8
Medical Math: Constant Rate InfusionSee page 16

Ron Morgan, CEO
Ron Morgan President & Chief Executive Officer, DoveLewis Emergency Animal Hospital
Dr. Herold writes about the concept of power in her column this issue – what it means to her and how the idea can and should play out on the hospital floor among staff. It is interesting to consider how
power plays out in a medical environment, especially one that has a lot of passion and stress like an ER/ICU setting.
One of the things I like most about DoveLewis’ evolution over the past several years is that we have worked hard not to behave like we have the power in our relationships with referring veterinarians. I remember when I joined Dove in late 2003. It was common to hear feedback that we acted and talked in elitist tones with other veterinarians. While that was surely not always the case, the feedback was consistent enough that it had to be frequent. I often heard “ivory tower” when people described our small, somewhat-rundown clinic that did indeed practice high-quality medicine. While the medicine we practiced was respected and appreciated, at times it may have lacked a tone of partnership and respect.
Today, I believe that most of our referring veterinarians would say we work much more collegially and in the spirit of partnership. This did not happen by accident. We worked to change that “ivory tower” attitude and reset our relationship with our referring veterinary partners. Our mutual patients need a continuum of care from all of us to survive the many obstacles they may encounter while in our respective care. They deserve that partnership during their much-too-brief lives.
Through collaboration, communication and partnership, I hope you see in today’s DoveLewis an organization that organically grows and changes to meet the needs of our clients, patients and partners in veterinary medicine. We will continue to build on the work we’ve done these past several years so our bond grows even stronger. That willingness to grow and collaborate for the benefit of our community and patients, I believe, is what sets DoveLewis apart – that and the best ER/ICU staff in the region.
A Message from Ron Morgan, President & CEOW
EL
CO
ME
DoveLewis’ internist Barbara Davis, DVM, DACVIM is here to provide internal medicine consultations and case management for your patients. Dr. Davis will work collaboratively with you, the primary care veterinarian, to direct the chronic care of patients referred to the internal medicine service. Additionally, with access to DoveLewis’ ICU, critical care, surgical and diagnostic imaging services, you can rest assured your patients will receive a seamless approach to internal medicine for cases requiring critical hospitalization or surgeries.
Internal Medicine
REFERRING PATIENTS TO DOVELEWIS INTERNAL MEDICINEcall 503.228.7281
Barbara Davis, DVM, DACVIM

From the Desk of the CMO
Lee Herold, DVM, DACVECCChief Medical Officer, DoveLewis Emergency Animal Hospital
COVER PHOTO: Superhero Rema donating blood to the DoveLewis Blood Bank, accompanied by Blood Bank Director, Jill Greene, Technician Assistant, Jolie Kaner and her dad, Robert.
Many people believe that power is granted by things outside of ourselves including status, wealth and title.
Power has become synonymous with control and authority. There is an understanding that acts of power must be grand gestures, or executive mandates to fit the definition of power. These narrow views imply that those not in traditional positions of power are less able to affect the course of events or change – and this is simply not true. Power is less about authority than it is about the will to make decisions for the benefit of others and the perseverance to see things through.
Anyone can feel power when they assist a stranger to change a tire on the side of the road. They can feel power when they
act to help a friend, client or animal. In veterinary medicine we have the power to ease suffering with treatment, euthanasia, gentle nursing care, kind words and more. I am reminded daily that the power of DoveLewis comes from our dedicated team members. I’m sure that you also observe this within your clinics, your staff and among your fellow co-workers. I witness power enacted on the hospital floor by our newest to our most veteran staff members. I don’t need to transfer power to my staff, but need to allow them to act on the power which they already wield far more effectively than I can. I recognize and celebrate these daily acts of power and I urge everyone to seize the power!
Lee Herold DVM, DACVECC
Board of DirectorsPresident & Chief Executive OfficerRon MorganDoveLewis Emergency Animal Hospital
ChairKatharine Wilson, DVMForest Heights Veterinary Clinic
Vice ChairCarol Opfel, DVMPDX Visiting Vet, LLC
SecretaryAndrew FranklinMember at Large
TreasurerBill Rouse, CPAKern & Thompson, LLC
Elizabeth Altermatt Herman, DVMMurrayhill Veterinary Hospital
Scott BontempoWelsh, Carson, Anderson & Stowe
Courtney Anders, DVMPearl Animal Hospital
Thomas Mackowiak, DVMHeartfelt Veterinary Hospital
Alexandra McLaughry, DVMBarbur Boulevard Veterinary Hospital
Maridith Rounsavell, DVMBanfield Pet Hospital
Steven Skinner, DVM, DACVIMOregon Vet Specialty Clinic
Terry TaillardPepsiCo
Angelique Whitlow, CPATalbot, Korvola & Warwick, LLP
DoveLewis Emergency Animal Hospital is recognized as a charitable organization under Internal Revenue Code, Section 501(c)(3). All donations are tax deductible
as allowable by law. Federal Tax ID No. 93–0621534.
main 503.228.7281backline 971.255.5990fax 503.228.0464
online dovelewis.org email [email protected]
Contact UsAVAILABLE AT DOVELEWIS:
Vacuum-Assisted Wound Therapy
Vacuum-assisted closure (VAC) is a type of therapy where fluid is drawn from the wound for faster, more efficient healing. This technique may be used over closed suture lines as well as over open wounds (chronic or acute). For open wounds, VAC may be a means to prepare the wound to close primarily or with a graft. It may also be used to get a granulation bed healthy enough for closure on its own. Due to the nature of cases seen at DoveLewis (trauma and complex wounds), VAC is an advantageous form of wound therapy management. This form of therapy is regarded as financially favorable compared to conventional treatments in the management of challenging wounds.
Volume 10 Issue 1 VetWrap 3

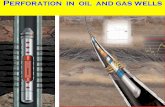
Fisher, an 11-month-old Labrador Retriever presented on emerg-
ency after sustaining a stick impalement injury. During a game of fetch, the young dog dove for the stick (Figure 1) inadvertently shoving one end deep into the back of his oropharynx. Following stick removal, he appeared in pain, was drooling (normal appearing saliva)
and had a dry cough prompting a visit to DoveLewis.
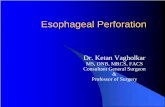
On presentation Fisher was quiet with a normal temperature (100.6˚ F) and respiratory rate and pattern. He was tachycardic (HR 120 bpm) with a systolic blood pressure of 130 mmHg. No ocular or nasal discharge was noted and he was no longer drooling. Subcutaneous emphysema was palpable in the cranial cervical region. The dog was given oxymorphone (0.07 mg/kg IV) and an intravenous catheter was placed in anticipation of anesthesia. An extended data base was unremarkable and he was started on ampicillin/sulbactam, maropitant and pantoprazole IV. Radiographs were obtained of his cervical and thoracic regions showing pneumomediastinum, but no pneumothorax or other significant abnormalities (Figure 2).
After discussion with the owner, Fisher was anesthetized and moved to sternal recumbency for endoscopy. He was intubated routinely with no hemorrhage or injury noted in the oropharynx. A flexible videoendoscope was passed into the esophagus where
Esophageal Perforation in a Labrador RetrieverCoby Richter, DVM, DACVS
a full thickness longitudinal perforation was documented (beginn- ing at 25 cm from the left upper canine tooth and extending approximately 3 cm). Anticipating post-surgical care, the endoscope was passed into the stomach and a 20 Fr percutaneous endoscopic gastrostomy tube (PEG tube) was placed in routine fashion. The endoscope was removed and Fisher was prepped for surgery to repair the esophageal perforation.
At surgery, a 2.5 cm dorsal esophageal tear was encountered. A culture of the deep tissues was collected. An oroesophageal tube was passed to aid in visualization and manipulation of the esophagus. After lavage and debridement, the perforation was closed in two layers (3-0 Maxon simple interrupted in the mucosa/ submucosa followed by 3-0 Maxon simple continuous in the muscular and adventitial layer). A 10 Fr round Jackson-Pratt (JP) drain was placed between the esophagus and stylohyoid muscle prior to closure of more superficial tissue planes. Following skin closure, the videoendoscope was advanced again to examine the repair. No suture was visible in the lumen of the esophagus and the perforation appeared completely sealed during dilation.
Fisher remained hospitalized for three days following surgery. The JP drain produced on average 2.5 ml/hr or less of serosanguinous discharge and was removed immediately prior to discharge. PEG tube feedings began 24 hours after surgery and were uncomplicated. The initial wound culture (collected at surgery) grew an Escherichia coli and Stenotrophomonas maltophilia and Fisher was maintained on amoxicillin/clavulanate for two weeks post discharge. At six days post discharge, he was re-presented
after having partially con-sumed his PEG tube. A new PEG tube was placed endoscopically through the same stoma, and during this procedure the esophageal repair site was evaluated. The repair was intact and maintained a seal during examination and dilation. The PEG tube was removed 18 days after the initial injury at which time Fisher was doing well and was on all oral medication and feedings. He has experienced no complica-tions since that time.
Surgical repair of esophageal perforation has a higher complication rate (dehiscence, local infection, fistula and
Figure 1: Fisher post-surgery shown with the offending stick.
SU
RG
ICA
L
4 VetWrap Volume 10 Issue 1

stricture) than repair of other portions of the intestinal tract. Factors that impede success include contamination with foreign material, motion (during swallowing and neck movement), lack of serosa and segmental blood supply. Contamination is best dealt with by early surgical intervention and thorough lavage and culture of the deep wound. Motion at the site can be minimized (but not eliminated) by use of a gastrostomy tube and use of a neck/head harness to restrict extension. Meticulous dissection and anatomic identification during surgery to preserve existing vascular supply, coupled with control of inflammation (NSAIDs, dead space elimination, bandaging, warm/cool compressing etc.) are important to maintain tissue viability. A 2008 retrospective reported a mortality rate of 36% (5/14) in dogs with acute esophageal stick penetration.
As with most surgical cases, early repair carries the best prognosis. Fisher was in the surgical suite less than a few hours after perfora- tion. Copious lavage at surgery and providing a mechanism for the removal of wound fluid are keys to a successful repair. In Fisher’s case, the perforation was located dorsally in the esophagus which meant that dead space and potential pocketing was several tissue planes from the skin. Penrose drains may have been employed but a closed suction system is preferred for several reasons in this location. First, it allows for measurement and
analysis of fluid. This enables the clinician to make an educated decision about when to remove a drain. Secondly, motion and compression of the muscles and tissue planes superficial to the repair will not impact the effectiveness of the drain. Finally, Penrose drains not only let fluid out but are a potential ingress for bacteria which could complicate healing further.
Placement of a PEG tube in this dog allowed immediate feeding while bypassing the repair site. All medications were able to be transitioned to oral forms quickly (which can be given via the PEG tube). Owner compliance with medications which can be given via the PEG tube tends to be very good (higher than with multiple oral medications). The PEG tube also allows a gentle transition back to oral feeding. Gastrostomy tubes are usually maintained at least 10 days post-placement to allow an adhesion to form between the body wall and the stomach.
DoveLewis would like to thank Fisher’s family for allowing his case to be shared with the veterinary community.
Selected References1. Doran IP, et al: Acute oropharyngeal and esophageal stick injury in forty-one dogs.
Vet Surg 37:781, 2008.
2. Kyles AE: Esophagus. In Tobias and Johnston editors: Veterinary Surgery Small Animal. 2012 St. Louis, Elsevier.
Figure 2: Lateral radiograph of Fisher at presentation demonstrating pneumomediastinum.
Volume 10 Issue 1 VetWrap 5

All too often, injured or sick animals require blood transfusions as part of
their treatment and recovery. Whether necessary due to anemia, blood loss, complicated surgeries, trauma, or another cause, a transfusion can often save the life of an animal. To meet this important need, DoveLewis runs one of the largest nonprofit, volunteer-based blood banks in the United States. This blood bank not only provides plasma and blood for the treatment of animals in-house, but also blood products to veterinarians across Portland, as well as throughout the U.S. Some 125 canine and feline donors make this possible, providing the program with enough blood to conduct over 500 transfusions for cats and dogs every year – many of them lifesaving.
Last December, the program provided one such transfusion for an 8-week-old stray kitten, who was later named Milo. Severely anemic, Milo suffered from a serious flea infestation that verged on becoming fatal. He arrived at DoveLewis emaciated and showing little sign of activity. The Blood Bank program provided Milo with two transfusions. He immediately responded after the first, and fully recovered after the second. Following treatment and care the young short-hair was returned to Multnomah County Animal Services where he was fostered in the hopes of finding his forever home.
These and other stories of animals getting their lives back, thanks to a blood transfusion, keep our blood bank growing. In addition, patients needing blood transfusions, like Milo, are becoming more common.
In fact, the demand for animal blood products is rising due to advances in veterinary medicine and increasing treatment options for trauma and disease. With the recent addition of Internal
98
2011 2012 2013 2014 2015
400
350
300
250
200
150
100
50
0
333
106
303
107
383
156
240
171
327
Units Supplied to Clinics Units Transfused at DoveLewis
The Blood Bank Program at DoveLewis
Medicine at DoveLewis, more blood is needed than ever before to maintain an adequate supply for community clinics and veterinary professionals.
DoveLewis is dedicated to securing donations to meet this demand both in-house as well as from other clinics. To keep up, DoveLewis is actively seeking new donor volunteers – also called “Superheroes” for the lifesaving effort they support. Healthy dogs and cats who meet specific requirements can qualify for the program, which includes a host of free benefits for animals and their owners. All volunteers are blood typed and screened for infectious disease prior to giving a blood donation to ensure they are safe and healthy donors.
Without the participation of these volunteers, animals in need might not be able to receive critical transfusions in time. Their continued support, coupled with the support of the animal-loving community, ensures that animals requiring a transfusion will be able to receive the care and treatment they deserve.
In addition to supplying in-house patients with blood transfusions, the DoveLewis Blood Bank offers a variety of blood products to local veterinarians and clinics throughout the state, tailored to meet patient and client needs. All DoveLewis blood products come with complete instructions including proper storage temperatures, transfusion set up and transfusion rates. We also include a transfusion record to help you track your patient’s stats with a reminder of how often to repeat TPRs.
For questions or assistance with determining which product may best suit a particular client case, contact a DoveLewis critical care specialist by calling our DVM backline at 971.255.5990. To find out how to get a new donor signed-up to become a Superhero or other information, please contact Blood Bank Director Jill Greene at 971.255.5920 or [email protected], or visit dovelewis.org.
Milo receiving a blood transfusion
CO
MM
UN
ITY
P
RO
GR
AM
S
6 VetWrap Volume 10 Issue 1

DoveLewis Blood Bank Helps Save Oregon Zoo’s Speke’s Gazelle Calf
Prior to the recent birth of the Oregon Zoo’s Speke’s gazelle Juliet, the
veterinary team there considered the possibility that if she were rejected by her mother when born, she would need a plasma transfusion for antibody transfer. Kristin Spring, CVT, veterinary hospital manager at the zoo, had previously worked at DoveLewis, so she knew exactly where to find the resources they needed to be prepared for the arrival of the new calf.
Before the gazelle’s mother Pansy gave birth, Kristin reached out to DoveLewis Blood Bank Director Jill Greene, CVT, to get the supplies she would need to obtain a blood donation from Pansy. Because the calf would need just the plasma, Jill planned to come to the DoveLewis hospital when Juliet was born to process the blood in the blood bank’s centrifuge.
The DoveLewis Blood Bank only takes donations from, and provides blood for cats and dogs, so large animal blood processing is not common. Jill prepared by researching large animal blood separation and transfusion techniques. She used protocols for horse blood separation, which would work for the gazelle’s needs.
When Juliet was born, it was deter- mined that she did need a plasma transfusion so the zoo’s veterinary team jumped into action. They took blood from Pansy and called Jill to meet Kristin at DoveLewis. Jill proceeded to process Pansy’s donated blood which was later transfused to Juliet. “That’s what we do as an organization – we work hard and we save lives” said Jill. “I was happy to do it and I would certainly do it again.”
As soon as Jill was done processing the blood at DoveLewis’ Blood Bank, Kristin was able to take the fresh plasma back to Juliet. The transfusion was successful and with much love and care from the veterinary staff at the Oregon Zoo, Juliet is doing well.
Volume 10 Issue 1 VetWrap 7
Looking for blood products? As a local donor-based community blood bank, we are here to work with you for your clinic’s blood product needs. We are available 24/7 to answer any questions you may have.
All blood products come with complete instructions, including proper storage temperatures, transfusion set up and transfusion rates. We also include a transfusion record to help you track your patient’s stats with a reminder of how often to repeat TPRs.
PRODUCTS INCLUDE:
FelinePacked red blood cells . . . . . . . . . $207.50Fresh frozen plasma . . . . . . . . . . . $184.75Frozen plasma . . . . . . . . . . . . . . . . $139.75Whole blood . . . . . . . . . . . . . . . . . . $331.50Matched unit . . . . . . . . . . . . . . . . . $452.00
CaninePacked red blood cells . . . . . . . . . $208.00Fresh frozen plasma . . . . . . . . . . . $183.00 (pediatric units available) Frozen plasma . . . . . . . . . . . . . . . . $141.75 (pediatric units available) Cryoprecipitate. . . . . . . . . . . . . . . . $210.00Cryo-poor. . . . . . . . . . . . . . . . . . . . . . $99.50Whole blood (by request). . . . . . . . $293.25 Matched unit . . . . . . . . . . . . . . . . . $430.25
Please call ahead to ensure availability.
OTHER SERVICES & SUPPLIES:Blood typing. . . . . . . . . . . . . . . . . . . $63.50Major crossmatch . . . . . . . . . . . . . $100.00Filters. . . . . . . . . . . . . . . . . . . . . . . . . $20.00 (Canine, Feline and Hemo-nate)Splitting fee . . . . . . . . . . . . . . . . . . . $32.50
Blood Bank
FOR MORE INFORMATION, PLEASE CONTACT:
Jill Greene, Blood Bank Director
971.255.5920 [email protected]
Oregon Zoo’s Speke’s gazelle, Juliet
“That’s what we do as an organization, we work hard and
we save lives.”– Jill Greene, Blood Bank Director
Photo by Shervin Hess, courtesy of the Oregon Zoo

Case Study: Make Your Diagnosis Barbara Davis, DVM, DACVIM
An 11-year-old female, spayed Chihuahua was referred
to DoveLewis for lethargy of a few days duration and marked anemia. The only remarkable findings on physical examination were very pale mucus membranes and a grade 3/6 systolic heart murmur, which had been present for years. Rectal examination did
not reveal any melena or hematochezia. Laboratory findings (Table 1), included a severe macrocytic, hypochromic regenerative anemia, marked hypoalbuminemia, mild hypoglo-bulinemia and mild hyperbilirubinemia. Slide agglutination was negative. A pathologist review of the blood smear did not reveal any abnormal red blood cell morphology (no spherocytes, etc.) or any red blood cell parasites. Prothrombin time was slightly prolonged. A Coombs test was performed and revealed a very low titer. A FAST scan of the dog’s abdomen revealed a small amount of peritoneal effusion. A sample of the peritoneal effusion was obtained and found to be a pure transudate (TP < 0.5 g/dL, minimal cellularity).
An abdominal ultrasound was performed which revealed a large homogenous splenic mass (5.34 x 3.79 cm), which was not cavitary. The remainder of the abdomen was unremarkable, aside from the previously noted peritoneal effusion.
What are your differential diagnoses?
________________________________________________________
________________________________________________________
Can all of these findings be explained by one problem or multiple
problems?
________________________________________________________
________________________________________________________
Problem List
1. Regenerative anemia r/o hemolysis (immune mediated hemolytic anemia (IMHA), hemophagocytic histiocytic sarcoma, babesiosis, microangiopathic anemia) vs. blood loss (gastrointestinal from bleeding mass, ulceration, etc.).
2. Panhypoproteinemia r/o hemophagocytic histiocytic sarcoma vs. blood loss vs. protein losing enteropathy vs. other.
3. Hyperbilirubinemia r/o hemolysis vs cholestasis of inflammatory disease vs. (less likely) pancreatitis vs. intrahepatic cholestasis (neoplasia, etc) vs. other.
4. Peritoneal effusion r/o secondary to the hypoalbuminemia.
5. Splenic mass r/o malignant (histiocytic sarcoma, hemangiosarcoma, etc) vs. benign (extramedullary hematopoiesis,etc).
INT
ER
NA
L
ME
DIC
INE
Table 1: Summary of Main Laboratory Finding
Parameter Value Reference Range
Hematocrit 12.5% 38 – 55%
Reticulocyte Count 276 10 – 110 K/uL
Platelet Count 187 143 – 448 K/uL
Serum Albumin 1.1 2.2 – 3.9 g/dL
Serum Globulin 2.0 2.5 – 4.5 g/dL
Serum Cholesterol 131 110 – 320 mg/dL
Total Bilirubin 1.1 0 – 0.9 mg/dL
Prothrombin Time 13 sec 12 – 19 sec
Partial Thromboplastin Time 82 sec 59 – 87 sec
Coombs 1:2
Slide Agglutination Negative
Spherocytes None seen
PCV/TS 12%/3.6, Icteric serumcontinues on page 15
8 VetWrap Volume 10 Issue 1

© 2011 IDEXX Laboratories, Inc. All rights reserved. • 9304-00 • All ®/TM marks are owned by IDEXX Laboratories, Inc. or its affiliates in the United States and/or other countries. The IDEXX Privacy Policy is available at idexx.com.
Knowledge you can put into practice™
IDEXX Learning Center
Education rewards everyone it touches{ }Reward Theory
CE should reward not only you, but also your patients, clients and practice. So the IDEXX Learning Center provides a comprehensive curriculum. And learning options that’ll have every member of your team wagging their tail: the veterinarian who wants to learn from experts face-to-face, techs who love the convenience of online courses, and the practice manager who’s eager to have protocols communicated consistently across the practice—and with clients. To turn theory into reality, visit idexxlearningcenter.com.
Experience you can trust to care for your patients overnight.
Dove overnight monitoring includes exam, ER or ICU monitoring as determined by a DoveLewis veterinarian with fluids, pain management – antibiotics, or oral medications as prescribed by the referring veterinarian (if indicated) and patient status lab work (if necessary).
$250 for 12-hour block in ER or ICU
The medical team at Frontier Veterinary Hospital is so thankful and appreciative of Dove’s overnight monitoring package and their shuttle service. We have utilized both services many times. It is such a relief to be able to send over our stable post-operative/milder medical patients and know that we don’t have to worry about them at home overnight – essentially the overnight monitoring package is an extension of our hospital’s continued care... Thank you, Dove!
– Lisa Yung, DVM
main 503.228.7281 • backline 971.255.5990 • fax 503.228.0464
Volume 10 Issue 1 VetWrap 9

Pericardiocentesis – A Review Deena Relucio, DVM
Pericardiocentesis is a potent- ially life-saving therapeutic
procedure commonly performed on the ER floor. Although considered relatively safe, this invasive procedure may be associated with serious complications. If left un-treated, increased intrapericardial pressure can lead to compression of the atria and ventricles (cardiac
tamponade) resulting in decreased cardiac output and hemody-namic compromise to the patient. Pericardiocentesis is often an emergent procedure and it is essential to efficiently and effectively communicate the suspected diagnosis, prognosis and goals of the pericardiocentesis to the client. In addition, it is important to prepare them for the potential complications, the immediate costs associated with the procedure and financial investment ahead. This review summarizes how to recognize a patient in need of pericardiocentesis and the technical approach to the procedure.
Clinical Findings
A typical history may be reported as acute collapse, exercise intolerance and weakness. Patients may present in cardiac arrest or already deceased with a client-reported history of peracute onset of clinical signs. The physical exam may reveal a prolonged capillary refill time, pale mucous membranes, muffled heart sounds, tachycardia, tachypnea, dyspnea, weak pulses or pulses paradoxus (weaker pulse during inspiration with cardiac tamponade), jugular distention or abdominal distention (cranial organomegaly, ascites). Only a few of these may be present upon physical examination.
Diagnostics
A brief ultrasound scan provides definitive diagnosis for pericardial effusion. Sonographically pericardial effusion will appear as an anechoic rim of fluid between the cardiac muscle walls and the hyperechoic pericardium. Diagnosis can be complicated by the presence of pleural effusion as some cases of large volumes of pleural effusion can mimic pericardial effusion. It can be helpful to look for an anechoic effusion surrounding the “floating” auricular appendage, which is indicative of fluid within the pericardium.
On ECG, there may be sinus tachycardia, ventricular premature complexes, ventricular tachycardia or electrical alternans (alter-nating variation in the amplitude of QRS complexes with every other beat as the heart swings inside a voluminous pericardial sac).
Thoracic radiographs will be distinct and demonstrate a globoid cardiac silhouette with well-defined margins and distended caudal vena cava on all views. The films may also show pleural effusion and ascites in the cranial abdomen. If only a small amount of pericardial effusion is present, it may be difficult to differentiate pericardial effusion with various other causes of cardiac silhouette
enlargement on radiographs alone. However, radiography is an important tool if your practice does not have ultrasound capabilities. The films can be used as a guide for the proposed pericardio-centesis site. On the VD/DV view, take notice which rib space has the most contact with the cardiac silhouette. A post-procedural radiograph may be helpful in identifying underlying pathology (pulmonary nodules, mediastinal mass), or pneumothorax once the majority of the fluid has been removed.
Bloodwork that includes complete blood count and chemistries may be non-specific, but may show anemia, hypoproteinemia, leukocytosis, possible liver enzyme elevation, or azotemia. If time allows, a coagulation profile may be performed to check PT/aPTT in-house. This can be valuable information prior to pericardiocentesis.
Considerations
Physical and diagnostic findings will be dependent on the volume of pericardial effusion, speed of accumulation, and underlying pathology. The severity of intrapericardial pressure is greater with acute and large volumes of fluid. In chronic cases, the pericardium can stretch to accommodate even large volumes without decompensating. If the patient is relatively stable and has minimal pericardial effusion based on diagnostics, it will be beneficial to have an echocardiogram performed by a cardiologist or trained sonographer as a small quantity of pericardial fluid allows for greater visualization of auricular masses. This can provide valuable prognostic information for the owner.
Preparing Your Patient and Setup
Place an IV catheter in the event that emergency medications need to be administered. ECG leads should be placed to monitor and track cardiac activity during and after the pericardial tap. If possible, 2-3 people should be recruited for the procedure – the clinician who performs the actual tap, an assistant who restrains the patient, and another assistant who controls the suction under the direction of the clinician.
Equipment
• Sterile prep – clippers, scrub, sterile gloves
• IV catheter, depending on size of patient
18-14 g peripheral IV catheter or abbocath catheters for larger or obese dogs
• 3-way stopcock
• Extension set
• Syringe – 20, 35, or 60 ml
• Collection bowl
• Red top tube and lavender top tube
DV
M
10 VetWrap Volume 10 Issue 1

Analgesics and Emergency Drugs
The majority of patients may be very weak and will be more receptive to handling. If necessary a light sedation may be given such as butorphanol (0.1-0.3 mg/kg). Lidocaine may be used as a local anesthetic at the proposed site at 0.5-1 ml/site into the subcutaneous space and intercostal muscle layers. Anesthetize the proposed site cranial to the rib, avoiding the neuromuscular bundle and vessels caudal to the rib. Be prepared to intubate and have pre-calculated emergency drugs in case of cardiac arrest.
• Lidocaine should be drawn and ready in the event of ventricular tachycardia: 2 mg/kg IV slowly (dogs), 0.25-0.5 mg/kg IV slowly (cats)
• Epinephrine: high dose (0.1 – 0.2 mg/kg) and low dose (0.01 – 0.02 mg/kg) IV
• Atropine: 0.04 – 0.05 mg/kg IM, IV
Procedure
The patient can be placed in either sternal or left lateral recumb-ency depending on patient stability and comfort. Oxygen supple- mentation should be provided. The right hemithorax is the preferred site as this approach lessens the chance of coronary artery laceration. Additionally, the cardiac notch is larger on the right lung lobes, which reduces accidental puncture of lung parenchyma. This procedure is not without risk. However, theoretically it is possible to puncture the thin-walled right ventricle with this approach. The deoxygenated blood can have the same port wine color as typical pericardial effusion but the clinician will generally feel movement or “bounce” through the needle and the ECG will reveal disturbances in cardiac activity so it is unlikely to go unnoticed.
Clip and surgically scrub the proposed site from the second to the seventh intercostal space (ICS) from the sternum to the mid-thorax. Some clinicians prefer fenestrating the catheter to allow for better drainage. However, this may compromise the integrity of the catheter and increase the risk for breakage while inside the pericardium. If desired, two to three small 1-2 mm fenestra-tions at the distal end of the catheter can be made with a #11 blade while the stylet is still in place. Do not burr the catheter or allow the fenestrations to exceed 40% of the diameter of the catheter. In veterinary medicine, pericardiocentesis is often performed blindly. Use radio-graphs to determine the point at which the cardiac silhouette is closest to the body wall if ultrasound is not available. While monitoring the ECG, palpate for the point of maximum intensity (PMI), typically at ICS-5. Insert the catheter perpendicularly at the locally anesthetized site cranial to the rib and apply light suction. A light pop may be felt once the pleural space is entered. Fluid may be obtained if pleural effusion is present. While monitoring the ECG, slowly advance the catheter further until the needle
encounters the pericardial sac. Some clinicians report feeling a “scratching” sensation, then advance another 3-4 mm until pericardial fluid is obtained. The stylet can be removed once the correct location is achieved. Hold the catheter steady, and then connect to an extension set, 3-way stopcock and syringe. The assistant can control the syringe and suction under the guidance of the clinician. It will be important to communicate if any complications are encountered, as the majority of adverse events occur during the active pericardial tap. Slight adjustments in catheter positioning can be made if the patient develops arrhythmias or negative pressure is encountered. Progress may be checked intermittently with ultrasound. Withdraw the catheter under light suction once negative pressure is obtained or if only a small amount of fluid remains. It will not be possible to remove all pericardial fluid. In most cases the puncture left behind into the pericardial sac will continue to leak out into the larger pleural space. The patient’s vital signs usually improve rapidly and dramatically due to the decreased intrapericardial pressure and increased cardiac output. Compare the aspirated effusion with peripheral blood PCV and total protein. Generally speaking, if the blood does not clot, it is likely effusion. Blood may also not clot in cases of actively bleeding tumors, atrial tears and coagulopathy. If the fluid removed clots in 1-2 minutes, it is suspicious for ventricular blood. Effusion generally has a lower PCV than peripheral blood with xanthrochromic (yellow) supernatant once spun down. Pericardial fluid can be submitted for cytologic analysis (+/- culture), but it is typically not highly diagnostic for the cause of the effusion.
Equipment for pericardiocentesis
continues on next page
Volume 10 Issue 1 VetWrap 11

Considerations
Cats are at higher risk for complications during pericardiocentesis due to size and smaller volumes of effusion. Most respond well to medical therapy as pericardial effusion is often associated with congestive heart failure. This procedure is generally reserved for patients with severe tamponade and who are quite hemody-namically unstable. A smaller peripheral or butterfly catheter may be used in lieu of a larger gauge catheter if attempted. All the same preparations apply, but almost all cats will require more tranquilization for this procedure than dogs.
Complications
Statistically, pericardiocentesis carries a low rate of complication in the canine patient. It is important to classify between procedural complications from progression or effects of underlying disease. In most cases, it may not be possible to distinguish the difference. Most complications associated with pericardiocentesis occur during or shortly after the procedure (<1 hour). Arrhythmias are the most common and may be attributable with underlying disease, needle contact with the epicardium or reperfusion syndrome. Ventricular tachycardia will often require lidocaine therapy. Other less common complications include hemorrhage, pneumothorax and cardiac arrest. Ideally, the patient should be monitored during the next 24 hours for cardiac arrhythmias and serial ultrasound scans to check for refilling of the pericardium. Requirement for a second pericardiocentesis within a short window is a poor prognostic indicator but may be necessary if cardiac tamponade recurs.
Prognosis
Prognosis is generally poor to guarded depending on the underlying cause (Table 1).
Conclusion
When performed correctly, pericardiocentesis can be a relatively safe procedure that carries a low rate of complication and provides valuable prognostic information for the client. Effective and efficient communication with the client regarding the pet’s condition as well as the cost and potential risks of pericard-iocentesis are key in gaining owner consent for this potentially life-saving intervention. Quickly identifying a patient in cardiac tamponade and providing potentially life-saving treatment is crucial. A good understanding of the pericardiocentesis procedure and anticipating complications can increase clinician preparedness and satisfactory outcomes in this often-emergent situation. References
1. Beardow, A. The Diagnostic and Therapeutic Approach to the Patient in Acute Congestive Heart Failure. Clinical Techniques in SmallAmmal Practice, Vol 15, No 2 (May), 2000, pp 70-75.
2. Gildlewski, J & Petrie, JP. Pericardiocentesis and Principles of Echocardiographic Imaging in the Patient with Cardiac Neoplasia. Clinical Techniques in Small Animal Practice, Vol 18, No 2 (May), 2003, pp 31-134.
3. Humm, K, et al. Adverse events associated with pericardiocentesis in dogs: 85 cases (1999-2006). Journal of Veterinary Emergency and Critical Care 19(4) 2009, pp 352–356
4. Scansen, B. Interventional cardiology for the criticalist. Journal of Veterinary Emergency and Critical Care 21(2) 2011, pp 123–136.
5. Silverstein, D & Hopper, K. Small Animal Critical Care, 2e. 2014.
Table 1
Type of Pericardial Effusion Differential Diagnosis Key features
Hemorrhagic Heart based tumors Older brachycephalic breed dogs
Right atrial hemangiosarcoma Non clotting blood
Metastatic neoplasia (lymphoma) Older large breed dogs
Idiopathic Middle aged, large breed
Trauma
Left atrial rupture Older dogs with valvular disease
Coagulopathy (rodenticide, other)
Transudate Congestive heart failure
Hypoproteinemia
Sequela after repair of PPDH
Exudate Infectious pericarditis Coccidioidomycosis, Actinomyces, Nocardia
Suppurative pericarditis Foreign body, Hematogenous
continued from previous page
12 VetWrap Volume 10 Issue 1

Elizabeth A. Semler is a Partner in the firm’s business litigation group and Chair of Sussman Shank LLP’s Employment Law Group. You can reach Elizabeth at 503.227.1111 or [email protected]. For additional information on this topic or Sussman Shank LLP, please visit the firm’s website at www.sussmanshank.com.
Paid advertisement by Sussman Shank LLP. This article is not an endorsement by DoveLewis for the organization, products, services, advice or information contained within.
Most veterinary practices have both hourly and salaried employees. The salaried
employees are either exempt from overtime because of the duties they perform, or non-exempt and entitled to overtime if they work more than 40 hours per week. At some point in 2016, the Department of Labor plans to issue new regulations that substantially increase the salary threshold for employees who are classified as exempt from overtime because they are executive or administrative employees. The proposed increase will raise the minimum salary from $455.00 per week to $970.00 per week. This means that once the new regulations are introduced, an employee who performs the duties of an executive or administrative employee will have to be paid a minimum annual salary of at least $50,440.00 to be exempt from overtime.
Generally, non-exempt employees (or hourly employees) are entitled to be paid overtime if they work more than 40 hours per week. Employees who are employed in “a bona fide executive, administrative, or professional capacity” are exempt from overtime, provided they are paid on a salaried basis. 29 U.S.C. § 213(a)(1). To be exempt from overtime, the employees have to perform certain duties to qualify as executive, administrative, or professional employees and have to be paid the same salary every week regardless of how many hours they work (with a few exceptions).
Under federal law, the duties that an employee must perform to qualify as an administrative employee include:
• The performance of office or non-manual work directly related to the management or general business operations of the employer or the employer’s customers (i.e., the employee must perform work directly related to assisting with the running or servicing of the business);
• The exercise of discretion and independent judgment with respect to matters of significance.
To qualify as an exempt executive employee:
• An employee’s primary duty must be managing a business, or a department or subdivision of the business;
• The employee must customarily and regularly direct the work of at least two or more employees;
• The employee must have the authority to hire or fire other employees, or the employee’s recommendations with respect to hiring, firing, advancement, or promotion of other employees must be given particular weight.
To qualify as an exempt learned professional:
• An employee’s primary duty must be the performance of work requiring advanced knowledge in the field of science or learning acquired by a prolonged course of specialized intellectual instruction. Veterinarians typically qualify as exempt learned professionals. Vet Techs are generally not exempt as learned professionals.
www.dol.gov/whd/overtime/fs17o_technicians.htm
If your practice has Vet Techs, or other employees who are currently classified as exempt because the duties they perform meet the criteria for administrative or executive employees, you need to consider whether to increase their salaries to meet the $970.00 weekly threshold, or reclassify the employees as non-exempt and pay the employees overtime (if earned). Among the factors to consider when making this decision is how many hours per week you think your exempt employees are working. If your exempt employees rarely work more than 40 hours per week, then reclassifying these employees as non-exempt should not have a significant economic impact on your practice. However, if your current exempt employees typically work more than 40 hours per week,
you will have to do some math to calculate your potential exposure for overtime and compare that exposure to the increased salary you will have to pay to keep the employees exempt. The comparison might result in a decision to reclassify some or all of your exempt employees, or to hire additional hourly employees and schedule shifts to avoid paying overtime.
For positions that you decide to reclassify as non-exempt, you should also consider:
• Whether to switch the employees to an hourly wage as opposed to paying the non-exempt employees a salary
• How non-exempt employees who continue to be paid a salary are going to keep track of the hours they work so you can make sure they are paid properly
• Whether your payroll system is set up so you can calculate a regular rate of pay based on the non-exempt employees’ salaries and pay overtime based on that regular rate of pay
• What kind of incentives or programs, if any, you want to introduce to retain management employees who become non-exempt
• Adopting a policy that prohibits non-exempt employees from working overtime without advance permission and imposes discipline for employees who work unauthorized overtime
There is no “right” answer for whether a particular employee should be reclassified. The decision has to be based on the economics of your practice and whether, based on the duties the employee actually performs, the employee should have been classified as exempt at the outset.
What Veterinary Businesses should know about Reclassifying Exempt Employees for 2016

Only the best care for your best friend.
*Visit Ban� eld.com/o� er to download the coupon. Ban� eld.com
Find your partner in pet care at
Ban� eld.
Proud sponsor of
Dogtoberfest!
*Visit Ban� eld.com/o� er
Find your partner in pet care at
Dogtoberfest!
A Big HeartUSI works with many Northwest organizations and we understand the varied and complex issues you face in growing your business and protecting your assets.
We specialize in providing:We specialize in providing:
· Health & Wellness Benefits · Retirement Plan Services· Commercial Insurance· Risk Management· Private Client Wealth Management
Elizabeth TempletonVice President
Employee Benefi ts503.417.9231
WHO SAYS WE CAN’T BE MORE THAN A BANK?
Pacific Continental Bank proudly supports DoveLewis Emergency Animal Hospital.
503-350-1205 therightbank.com

Sign up to receive our TALENT NETWORK emails. We’ll keep you updated on job opportunities at DoveLewis. www.dovelewis.org/about-us/open-positions-applications
Diagnosis
Fine needle aspirate of the splenic mass revealed splenic neoplastic infiltration by histiocytic sarcoma. Occasional cells showed evidence of erythrophagocytosis.
Case Discussion
Hemophagocytic histiocytic sarcoma (HHS) can be a very difficult diagnosis as it mimics other disease processes, mainly immune mediated hemolytic anemia, Evan’s syndrome and blood loss. In this current case, blood loss, presumably from the GI tract as there was no loss into a large cavity, was a possibility; however, it did not fit with the mild hyperbilirubinemia. The elevated bilirubin could have been a spurious finding from a hemolyzed sample; however, the icteric serum proved that it was a real finding. In addition, while melena certainly does not need to be present for GI blood loss, an acute anemia of 12% with no melena made it less likely as well. IMHA was also on the list of differentials, but the dog lacked any other criteria such as spherocytosis, slide agglutination or suggestive Coombs titer. In addition, the hypoproteinemia did not fit with IMHA. Therefore, the dog either had two independent problems, such as IMHA and a protein losing enteropathy or GI bleeding and pancreatitis. The only single differential that seemed to fit all of this dog’s findings was HHS.
Some dogs may only exhibit a regenerative anemia which mimics IMHA, but lacks spherocytes, agglutination and/or a Coombs positive. These patients often will not respond to immuno-suppressive therapy as is expected with true IMHA patients; their hematocrit may remain stable but often does not increase back into the normal range. Therefore HHS should remain on the list of differential for patients presumed to have IMHA which are not responding as expected, especially if other clinicopathologic abnormalities associated with HHS are also present.
Hemophagocytic Histiocytic Sarcoma
HHS is a rare histiocytic sarcoma (HS) which arises from the macrophages of the red pulp and bone marrow macrophages, while classic histiocytic sarcoma arises from interstitial dendritic cells. It commonly affects the spleen and the bone marrow simultaneously and will often metastasize to the lungs and liver without an obvious mass formation in those locations.
HHS is found in the same breeds affected by local or disseminated HS: Bernese Mountain Dog, Golden Retriever, Rottweiler, Labrador Retriever and Flat Coated Retrievers. It is important to remember that it can occur in any breed, including uncommon breeds such as the Chihuahua. HHS has also been reported in cats.
The most common clinicopathologic findings associated with HHS are a Coombs negative regenerative anemia, hypoalbuminemia, thrombocytopenia, and hypocholesterolemia. Hypoglobulinemia and mild hyperbilirubinemia can also be present. The anemia, hypoalbuminemia, thrombocytopenia and hypoglobulinemia are due to phagocytosis by the neoplastic macrophages. Another cause of the hypoalbuminemia and the cause of hypocholesterolemia is downregulation of synthesis of albumin and cholesterol by the liver due to expression of interleukins by the neoplastic cells. A mild hyperbilirubinemia is also a feature in about 50% of dogs with HHS, with one paper reporting a mean total bilirubin of 0.6 (RR, 0-0.4), with a range of 0.1-2.2 in those dogs with HHS.
An abdominal ultrasound may be unremarkable; however, diffuse splenomegaly with ill-defined masses is a common finding. Other findings that may be seen include diffuse hepatomegaly and lymphadenopathy. Even if the liver is infiltrated, discrete masses are not commonly seen.
HHS can be diagnosed via aspirate of the spleen, bone marrow, liver or abdominal lymph nodes if enlarged. Even if the spleen and liver do not look abnormal on ultrasound, a fine needle aspirate of the spleen and the liver are indicated if a strong index of suspicion for HHS exists. A bone marrow aspirate is also recommended if cytology of the spleen and liver do not yield a diagnosis. Unfortun- ately, sometimes a splenectomy is required for definitive diagnosis.
The treatment for HHS is splenectomy followed by chemotherapy – most commonly CCNU. Unfortunately, the prognosis for HHS is very poor. Even with splenectomy and chemotherapy, the median survival time is about 3 months. A study in 2006, which documented HHS in 17 dogs, reported the clinical course from initial onset of clinical sign to death or euthanasia ranged from 2-32 weeks (mean of 7.1 weeks). However that study did not discuss therapies that the dogs received. If surgery and chemotherapy are not elected, treatment with prednisone (1 mg/kg/day) may help with overall well-being. However, it will not treat the neoplasia itself. References:
1. Moore P.F, Affolter V.K., Vernau W. Canine hemophagocytic histiocytic sarcoma: a proliferative disorder of CD11d+ macrophages. Vet Pathol 2006; 43: 632-645.
2. Soare T, Noble P.J., Hetzel U, Fonfara S, et al. Paraneoplastic syndrome in haemophagocytic histiocytic sarcoma in a dog. J Comp Path 2012; 146:168-174.
3. Friedrichs K.R., Young K.M. Histiocytic sarcoma of macrophage origin in a cat: case report with literature review of feline histiocytic malignancies and comparison with canine hemophagocytic histiocytic sarcoma. Vet Clin Pathol 2008: 121-128.
continued from page 8
Volume 10 Issue 1 VetWrap 15

This calculation should be taken one step further to determine how many milligrams of metoclopramide are in each milliliter of fluid so if the fluid rate changes, the dose is known. If the dog’s fluid rate is changed to 75 ml/hr, how much metoclopramide is the dog receiving?
For example, a 17 kg dog has fluids running at 65 ml/hr. You are asked to make a metoclopramide (5 mg/ml) CRI at a dose of 1 mg/kg/day. How many ml of metoclopramide do you add to a liter of fluids that will run at 65 ml/hr?
Medical Math: Constant Rate InfusionMegan Brashear, BS, CVT, VTS (ECC)
A Constant Rate Infusion (CRI) is utilized to administer a continuous dose of drug in intravenous fluids. We are most used to CRIs for pain management, as in this form the drug can be maintained
at effective plasma concentrations for the duration of treatment and avoid pain peaks and valleys. CRIs are also utilized for blood pressure management medications, electrolyte supplementation, GI motility medications, anesthesia, and insulin administration. Drugs can be administered without dilution, calculated to be mixed in to IV fluids running at a pre-determined rate, or prepared to be titrated to different rates depending on patient needs.
Calculations for Fluids Running at a Pre-Set Rate
If the drug is to be added to fluids running at a set rate, you will need to know:
• The dose for the CRI (like mg/kg/day)
• The concentration of the drug
• The hourly fluid rate
TE
CH
NIC
IAN
10.8 mg metoclopramide ÷ 1000 ml = 0.0108 mg metoclopramide/ml(mg of medication added ÷ ml of fluid it is added to = dose per ml of fluid)
STEP 1
19.44 mg metoclopramide/day ÷ 17 kg = 1.14 mg metoclopramide/kg/day (dose per day ÷ patient weight in kg = dose for patient weight in kg per day)
STEP 4
This new dose of 1.14 mg metoclopramide/kg/day can be compared to the therapeutic dose for metoclopramide and steps taken as needed to ensure patient safety.
RESULT
0.0108 mg metoclopramide/ml x 75 ml/hr = 0.81 mg metoclopramide/hr (mg of medication needed per ml of fluid x fluid rate = dose per hour)
STEP 2
17 kg x 1 mg/kg/day = 17 mg metoclopramide/day(1 mg/kg/day means the dog needs 17 mg/day (24 hours) of metoclopramide)
STEP 1
15.4 hr/L x 0.7 mg metoclopramide/hr = 10.8 mg metoclopramide/L (hours of fluids in liter x drug dose per hour = medication needed per liter of fluids)
STEP 4
10.8 mg metoclopramide/L ÷ 5 mg metoclopramide/ml = 2.16 ml metoclopramide (drug dose ÷ drug concentration = drug dose needed in total fluids)
STEP 5
If you add 10.8 mg metoclopramide (5 mg/ml) to 1 liter of fluids running at 65 ml/hr, a 17 kg dog will receive 1 mg/kg/day of metoclopramide
RESULT
17 mg/day ÷ 24 hr/day = 0.7 mg metoclopramide/hr
STEP 2
1000 ml/L ÷ 65 ml/hr = 15.4 hr/L (1000 ml in a liter ÷ hourly fluid rate = hours of fluids in liter)
STEP 3
0.81 mg metoclopramide/hr x 24 hr/day = 19.44 mg metoclopramide/day (dose per hour x hours in a day = dose per day)
STEP 3
16 VetWrap Volume 10 Issue 1

Calculations for Titratable CRIs
Some CRIs are calculated to be titratable, meaning the dose of drugs is changed by adjusting the fluid rate until the appropriate response from the patient is reached. There is often a dose range as opposed to a set dose per hour. These CRIs will be created and managed separate from the IV fluids as the rate may need to be changed frequently. A simple way to approach these calculations is to make the CRI so that if it runs at 1 ml/hr, the patient receives 1 mcg/kg/hr (or 1 mcg/kg/min, depending on the drug dosage). If this is how the CRI is calculated, the math is done prior to the rate change and adjustments can be made quickly. Because 1 ml/hr = 1 mcg/kg/hr, a fluid rate of 4 ml/hr will deliver 4 mcg/kg/hr. A fluid rate of 9 ml/hr will deliver 9 mcg/kg/hr. Doses can be quickly changed without needing to perform more math equations. For example:
A 21 kg dog has been hit by a car and needs pain management administered as a CRI. You are asked to calculate a fentanyl (50 mcg/ml) CRI and place the patient at 3 mcg/kg/hr of fentanyl with the ability to titrate the dose as needed. You plan on making this CRI in a 60 ml syringe of NaCl and delivering it on a syringe pump.
1 ml/hr needs to = 4.5 mcg/min (the patient weighs 4.5 kg, you want 1 ml/hr to deliver 4.5 mcg/min)
STEP 1
100 ml ÷ 1 ml/hr = 100 hr(total fluid bag ÷ hourly fluid rate = hours per fluid bag)
STEP 4
0.27 mg dobutamine/hr x 100 hr = 27 mg dobutamine/100 ml(hourly dose x hours per fluid bag = drug dose)
STEP 5
27 mg dobutamine ÷ 12.5 mg/ml = 2.16 ml dobutamine needed (drug dose ÷ drug concentration = dose of drug to be in total fluids)
STEP 6
Run the CRI at 2 ml/hr to deliver 2 mcg dobutamine/kg/min to the cat
RESULT
4.5 mcg/min x 60 min/hr = 270 mcg/hr (because your fluid rate is in ml/hr, you must convert your dose into mcg/hr)
STEP 2
270 mcg /hr ÷ 1000 mcg/mg = 0.27 mg/hr (because your drug concentration is in mg/ml, you must convert mcg/hr to mg/hr)
STEP 3
1 ml/hr needs to = 21 mcg fentanyl/hr (the patient weighs 21 kg, so you want 1 ml/hr to deliver 21 mcg/hr)
STEP 1
1260 mcg fentanyl ÷ 50 mcg fentanyl/ml = 25.2 ml fentanyl(drug dose ÷ drug concentration = drug dose needed in total fluids)
STEP 4
Run the CRI at 3 ml/hr to deliver 3 mcg/kg/hr to the 21 kg dog
RESULT
60 ml x 1 ml/hr = 60 hr (amount of total fluids x hourly fluid rate = hours of CRI)
STEP 2
21 mcg fentanyl/hr x 60 hr = 1260 mcg fentanyl(hourly dose x hours of CRI = drug dose)
STEP 3
Because the equation used 60 ml as the total amount of fluids in the CRI (including the drug you are adding), the total amount of fluids and drug in the syringe must be 60 ml. Prior to adding any drug, you must remove an equal amount of fluid from the syringe or bag of fluids. In this case, 25.2 ml of fentanyl is added to 34.8 ml of NaCl equaling a total volume of 60 ml. The label on the syringe should read:
Fentanyl 1260 mcg qs 60 ml NaCL The “qs” means quantity sufficient, meaning the entire volume of drug and NaCl is 60 ml.
Some drugs are dosed as mcg/kg/min. Dobutamine is one such drug. The dose needed is titrated up depending on patient response and weaned down as improvement is seen. Having this CRI calculated so that 1 ml/hr = 1 mcg/kg/min will make frequent dose changes a simple process and prevent complicated math each time the dose is changed.
A 4.5 kg cat has been battling hypotension and you are asked to calculate a dobutamine (12.5 mg/ml) CRI and then start administering 2 mcg dobutamine/kg/min to the cat. For ease of titrating, you will make the CRI so that 1 ml/hr = 1 mcg/kg/min. You will be making the CRI in a 100 ml bag of NaCl.
The equation used 100 ml as the total amount of fluids needed including the drug we are adding. From the 100 ml bag, remove 2.16 ml of NaCl then add 2.16 ml of dobutamine. Label the bag: Dobutamine 0.27 mg qs 100 ml NaCl
With small patients or those that cannot tolerate high rates of intravenous fluids, it may not be appropriate to run a CRI at 10 or 15 ml/hr. In those patients it may be better to calculate their CRI so that 1 ml/hr = 10 mcg/kg/min, or 1 ml/hr = 5 mcg/kg/hr. The remainder of the math remains the same.
continues on next page
Volume 10 Issue 1 VetWrap 17

Test Your Knowledge:Test your skills with this medical math quiz!
QUESTION 1
You are asked to make a 1 mg/kg/day metoclopramide (5 mg/ml) CRI for a patient that weighs 12 kg. The fluids are running at 45 ml/hr. How many milliliters of metoclopramide will you add to a full liter of fluids for this patient?
QUESTION 2
You are asked to make a 1.5 mg/kg/day metoclopramide (5 mg/ml) CRI for a patient that weighs 5.5 kg. Their fluid rate is 15 ml/hr. How many milliliters of metoclopramide will you add to a full liter of fluids for this patient? If their fluid rate is increased to 20 ml/hr, how many mg/kg/day of metoclopramide will they be receiving?
QUESTION 3
You are asked to make a dopamine (40 mg/ml) CRI for a 24 kg dog. For ease of dosing, you need to make the CRI so that 1 ml/hr = 1 mcg/kg/min. You will be making the CRI in 250 ml NaCl. How many milligrams of dopamine will you qs to 250 ml NaCl?
QUESTION 4
You are asked to make a fentanyl (50 mcg/ml) CRI for a 7 kg cat. For ease of dosing, you need to make the CRI so that 1 ml/hr = 1 mcg/kg/hr. You will be making the CRI in 100 ml NaCl. How many micrograms of fentanyl will you qs to 100 ml NaCl?
ANSWERS CAN BE FOUND ONLINE AT: www.dovelewis.org/resources-for-veterinarians/vetwrap
MAKINGA DIFFERENCEFOR FAMILIES & THEIR LOVED ONES.
Calculating CRIs can seem intimidating, and these preparations need special care and attention paid, but the benefit to the patient makes it worth the work. It is important when administering a CRI to ensure that all medications going through the fluid line (including any that are injected separately, like bolus pain management or antibiotics) are compatible. Drugs like metoclopramide, lidocaine, and morphine will need to be protected from light if they are to be hung for more than 24 hours. Constant Rate Infusions must be labeled with the drug name, the drug dose per milliliter, the time and date the CRI was mixed, and the initials of the person who created the CRI. The fluid bag must be labeled as well as noting the dose and calculation in the medical record. It is vital that CRIs are calculated correctly, as incorrect doses administered over multiple hours can be detrimental and even deadly to patients. Once a CRI is utilized, the fluid rate should be checked at least every four hours and matched to the dose ordered by the medical record.
When in doubt, double check your calculations and always clearly label all CRIs. Practice makes perfect; use the following CRI orders to practice your new-found skills in CRI calculations.
continued from previous page
18 VetWrap Volume 10 Issue 1

Surgery
main 503.228.7281 • backline 971.255.5990 • fax 503.228.0464
DoveLewis surgeons Ashley Magee, DVM, DACVS and Coby Richter, DVM, DACVS are here to provide surgical advice to you and expertise for your patients 7 days a week.In addition to being available for your patients requiring emer-gency surgery, they are available for telephone consultations regarding cases you are undertaking at your practice and consultations on cases you would like to refer for non-emergent surgery.
Why DoveLewis?DoveLewis is the ideal resource for your patients requiring urgent or emergent surgery for many reasons:
• Coverage 7 days a week by board-certified surgeons
• After-hours surgeries performed by the surgeons or boarded criticalists trained in trauma surgery
• Experienced ICU staff for post-op monitoring
• Criticalist expertise for pre-op, intra-op and post-op monitoring
• Immediate access to blood products
• Availability of independent radiologist, cardiologist and neurologist for consultation when needed
Surgeries Commonly Performed at DoveLewis
• Abdominal and urogenital surgery
• Upper and lower respiratory / thoracic surgery
• Oncologic surgery
• Complex wound management and reconstruction
• Treatment of traumatic musculoskeletal injuries
• Endoscopy, cystoscopy, rhinoscopy, tracheal and urethral stenting
Note: Due to our caseload of emergency procedures and staffing/equipment limitations, we do not perform elective orthopedic procedures, portosystemic shunt surgery, or cardiac surgery (except pericardiectomy).
REFERRING PATIENTS TO DOVELEWIS FOR SURGERYEmergency/urgent Surgical Cases: Call the main line 503.228.7281 and speak to a surgeon or staff DVM prior to the patient’s arrival.
Less urgent surgeries (to be scheduled within a few days): Call the main line 503.228.7281 and ask to speak with Dr. Magee, or Dr. Richter to schedule a surgical consultation.
The DoveLewis surgery department is also available by email for general surgical inquiries related to non-emergent matters.
Dr. Magee: [email protected] Dr. Richter: [email protected]
CONSULTSCall the DoveLewis main line 503.228.7281 and ask to speak to a surgeon. If a surgeon is not on the hospital floor at the time of your call, ask to speak with a staff DVM. If you have an immediate request, the DVM will contact the on-call surgeon by phone.
EMERGENCIESIn an emergency that requires immediate attention call:
Main Line: 503.228.7281DVM Backline: 971.255.5990
Ashley Magee, DVM, DACVS Coby Richter, DVM, DACVS
The Northwest’s Nonprofit 24-Hour Emergency Animal Hospital

Volume 10 Issue 1 • 2016
Knowledge You Can Use, Experience You Can Trust
DoveLewis Emergency Animal Hospital1945 NW Pettygrove StreetPortland, Oregon 97209
New and improved website, name and logo with the same expert training and education you have come to trust. If you haven’t had a chance to experience it yet, visit atdove.org.
Knowledge You Can Use, Experience You Can TrustJoin our digital training platform to cut costly procedural errors, cultivate smart culture and streamline staff training. Our extensive library of procedural shorts, CE and articles feature real procedures from DoveLewis. Make us your ally.