Esophageal perforation: a rare complication of Zollinger-Ellison syndrome
2
CASE REPORTS Esophageal Perforation: A Rare Complication of Zollinger-Ellison Syndrome Thomas Ng, MD, Donna E. Maziak, MDCM, and Farid M. Shamji, MD Division of Thoracic Surgery, University of Ottawa, Ottawa, Ontario, Canada Spontaneous perforation of the esophagus is a rare man- ifestation of Zollinger-Ellison syndrome (ZES). Failure to recognize its existence can lead to an unsuccessful treat- ment of the esophageal perforation. We present a rare case of reflux esophagitis–induced esophageal perfora- tion in a patient with ZES. Presence of a gastrinoma should be considered when recurrent or complicated reflux esophagitis is encountered. (Ann Thorac Surg 2001;72:592–3) © 2001 by The Society of Thoracic Surgeons I n the largest reported series of Zollinger-Ellison syn- drome (ZES), esophageal complications are rarely cited [1]. We report a case of hyperacidic reflux causing spontaneous esophageal perforation in a patient with a gastrinoma. Early recognition of ZES is essential in pre- venting complications of inappropriate or inadequate therapy for the esophageal perforation. A 59-year-old woman was referred to the thoracic sur- gery service for urgent treatment of disabling dysphagia. Esophageal cancer was suspected. Her symptoms began 4 years earlier with diarrhea, duodenitis, and severe esophagitis seen on endoscopy, and she was placed on proton pump inhibitor therapy. On this admission, en- doscopic examination of the esophagus revealed a tight stricture beginning at 28 cm. Only the upper end of the stricture could be examined where the mucosa was found to be inflamed and sloughing. No biopsy was taken and no attempt was made to advance past or dilate the stricture. The stomach and duodenum could not be examined therefore a barium contrast study was per- formed revealing a long tight stricture in the lower 10 cm of the esophagus (Fig 1) and a normal-appearing stomach and duodenum. Twenty-four hours later, severe right-side chest pain suddenly developed and a chest radiograph revealed a right-side tension hydropneumothorax. There was no history of vomiting. Free perforation of the lower esoph- agus into the right chest was confirmed by a water soluble contrast study. Within 2 hours of onset of the acute illness, an emergent right thoracotomy with subto- tal esophagectomy was performed and in the absence of mediastinal or pleural sepsis, reconstruction with gastric conduit and cervical esophagogastric anastomosis was undertaken. Both the stomach and duodenum appeared healthy at laparotomy. Pathology examination revealed a gastric lesser curvature with normal mucosa and a per- forated esophageal ulcer just above the gastroesophageal junction. The esophageal mucosa was completely de- nuded and replaced by necrotic fibrinopurulent material consistent with severe damage from reflux disease. In the postoperative period, the only abnormal finding consistently documented was clear nasogastric drainage in excess of 2 L per day. On the seventh postoperative day, bile was noted to drain from the right chest tube. A water soluble contrast study through the nasogastric tube showed extravasation in the mid portion of the gastric conduit and an intact esophagogastric anastomosis. An urgent right thoracotomy was performed with the finding of two gastric perforations. The patient underwent sub- total gastrectomy and cervical esophagostomy. Pathology revealed two perforated ulcers in the gastric body 3.5 cm apart in an otherwise healthy stomach with normal mucosa and no ischemia. At this point ZES was sus- pected. A fasting serum gastrin level of more than 2,000 pg/mL confirmed the diagnosis (normal , 150 pg/mL). Accepted for publication July 19, 2000. Address reprint requests to Dr Maziak, Division of Thoracic Surgery, Ottawa Hospital, Civic Campus, 1053 Carling Ave, CPC Room 162, Ottawa, Ontario, Canada, K1Y 4E9; e-mail: [email protected]. Fig 1. Barium esophagram revealing a long mid esophageal stricture. © 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00 Published by Elsevier Science Inc PII S0003-4975(00)02308-0
Transcript of Esophageal perforation: a rare complication of Zollinger-Ellison syndrome

CASE REPORTS
Esophageal Perforation: A RareComplication of Zollinger-EllisonSyndromeThomas Ng, MD, Donna E. Maziak, MDCM, and FaridM. Shamji, MD
Division of Thoracic Surgery, University of Ottawa, Ottawa,Ontario, Canada
Spontaneous perforation of the esophagus is a rare man-ifestation of Zollinger-Ellison syndrome (ZES). Failure torecognize its existence can lead to an unsuccessful treat-ment of the esophageal perforation. We present a rarecase of reflux esophagitis–induced esophageal perfora-tion in a patient with ZES. Presence of a gastrinomashould be considered when recurrent or complicatedreflux esophagitis is encountered.
(Ann Thorac Surg 2001;72:592–3)© 2001 by The Society of Thoracic Surgeons
In the largest reported series of Zollinger-Ellison syn-drome (ZES), esophageal complications are rarely
cited [1]. We report a case of hyperacidic reflux causingspontaneous esophageal perforation in a patient with agastrinoma. Early recognition of ZES is essential in pre-venting complications of inappropriate or inadequatetherapy for the esophageal perforation.
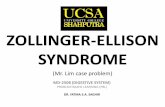
A 59-year-old woman was referred to the thoracic sur-gery service for urgent treatment of disabling dysphagia.Esophageal cancer was suspected. Her symptoms began4 years earlier with diarrhea, duodenitis, and severeesophagitis seen on endoscopy, and she was placed onproton pump inhibitor therapy. On this admission, en-doscopic examination of the esophagus revealed a tightstricture beginning at 28 cm. Only the upper end of thestricture could be examined where the mucosa was foundto be inflamed and sloughing. No biopsy was taken andno attempt was made to advance past or dilate thestricture. The stomach and duodenum could not beexamined therefore a barium contrast study was per-formed revealing a long tight stricture in the lower 10 cmof the esophagus (Fig 1) and a normal-appearing stomachand duodenum.
Twenty-four hours later, severe right-side chest painsuddenly developed and a chest radiograph revealed aright-side tension hydropneumothorax. There was nohistory of vomiting. Free perforation of the lower esoph-agus into the right chest was confirmed by a watersoluble contrast study. Within 2 hours of onset of theacute illness, an emergent right thoracotomy with subto-tal esophagectomy was performed and in the absence ofmediastinal or pleural sepsis, reconstruction with gastricconduit and cervical esophagogastric anastomosis was
undertaken. Both the stomach and duodenum appearedhealthy at laparotomy. Pathology examination revealed agastric lesser curvature with normal mucosa and a per-forated esophageal ulcer just above the gastroesophagealjunction. The esophageal mucosa was completely de-nuded and replaced by necrotic fibrinopurulent materialconsistent with severe damage from reflux disease.
In the postoperative period, the only abnormal findingconsistently documented was clear nasogastric drainagein excess of 2 L per day. On the seventh postoperativeday, bile was noted to drain from the right chest tube. Awater soluble contrast study through the nasogastric tubeshowed extravasation in the mid portion of the gastricconduit and an intact esophagogastric anastomosis. Anurgent right thoracotomy was performed with the findingof two gastric perforations. The patient underwent sub-total gastrectomy and cervical esophagostomy. Pathologyrevealed two perforated ulcers in the gastric body 3.5 cmapart in an otherwise healthy stomach with normalmucosa and no ischemia. At this point ZES was sus-pected. A fasting serum gastrin level of more than 2,000pg/mL confirmed the diagnosis (normal , 150 pg/mL).
Accepted for publication July 19, 2000.
Address reprint requests to Dr Maziak, Division of Thoracic Surgery,Ottawa Hospital, Civic Campus, 1053 Carling Ave, CPC Room 162,Ottawa, Ontario, Canada, K1Y 4E9; e-mail: [email protected]. Fig 1. Barium esophagram revealing a long mid esophageal stricture.
© 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(00)02308-0

Computerized tomography and arteriography (Fig 2) local-ized the gastrinoma to the uncinate process of the pancreas.
The patient returned to the operating room 6 weekslater to undergo a successful local resection of the gas-trinoma, completion gastrectomy, and esophageal recon-struction with substernal isoperistaltic left colon interpo-sition into a Roux-en-Y loop of jejunum. Pathologyrevealed an increased prominence of parietal cells withinthe body-type mucosa of the gastric remnant and aneuroendocrine tumor of the pancreas consistent withgastrinoma. The patient has remained well after 5 yearsof follow-up and serum gastrin remains low at 40 pg/mL.
CommentIn 1964, Ellison and Wilson [1] reported on 260 cases ofZES. Common presentations of this syndrome of acidhypersecretion included recurrent or refractory gastroin-testinal ulcer despite maximal medical and surgical ther-apy, severe complications of ulcer disease, multiple ul-cers in atypical locations, and diarrhea. Esophagealinvolvement was seen in only 2 of 260 cases; however, thedetails were not elaborated upon. Esophageal complica-tions in ZES were thought to be rare.
Recent studies have noted a high incidence of esoph-ageal involvement in ZES [2, 3]. With close surveillanceusing endoscopy, biopsy, and pH monitoring, refluxesophagitis was found to be as high as 40% of patientswith ZES [2, 3]. However, complicated reflux disease inZES remains less common. There have been severalreports of stricture and Barrett’s epithelium in ZES [2, 3],and one report of adenocarcinoma arising from Barrett’sepithelium [4] but none of perforation until now. Perfo-ration of the esophagus in patients with ZES has beenreported in two cases but they were secondary to emesis[5] and paraesophageal hernia [6] and not as a directresult of acid reflux as in our case.
In our patient, free perforation occurred in a damagedesophagus, denuded of its mucosa by unrecognized long-standing acid hypersecretion. After the first operation,persistent hyperacidity, despite truncal vagotomy andresection of the lesser curvature of the stomach, wasresponsible for the subsequent acute ulceration andperforation of the interposed gastric conduit.
Once the syndrome is recognized, the treatment ofchoice for ZES is surgery with excision of the gastrinoma.Medical therapy with a proton pump inhibitor and so-matostatin is reserved for unresectable disease, meta-static disease, multiple gastrinomas, and medically inop-erable patients. As with gastric or duodenal ulcer disease,when refractory or complicated esophageal reflux dis-ease occurs, ZES should be considered.
References1. Ellison EH, Wilson DS. The Zollinger-Ellison syndrome: re-
appraisal and evaluation of 260 registered cases. Ann Surg1964;160:512–30.
2. Miller LS, Vinayek R, Frucht H, Gardner JD, Jensen RT,Maton PN. Reflux esophagitis in patients with Zollinger-Ellison syndrome. Gastroenterology 1990;98:341–6.
3. Strader DB, Benjamin SB, Orbuch M, et al. Esophagealfunction and occurrence of Barrett’s esophagus in Zollinger-Ellison syndrome. Digestion 1995;56:347–56.
4. Symonds DA, Ramsey HE. Adenocarcinoma arising in Bar-rett’s esophagus with Zollinger-Ellison syndrome. Am J ClinPathol 1980;73:823–6.
5. Goldstein LA, Thompson WR. Esophageal perforations: a 15year experience. Am J Surg 1982;143:495–502.
6. Bondeson AG, Bondeson L, Thompson NW. Stricture andperforation of the esophagus: overlooked threats in theZollinger-Ellison syndrome. World J Surg 1990;14:361–3.
Minimally Invasive Ivor LewisEsophagectomyNinh T. Nguyen, MD, David M. Follette,MD, Philippe H. Lemoine, MD, Peter F. Roberts, MD,and James E. Goodnight, Jr, MD, PhD
Department of Surgery, University of California, Davis,Medical Center, Sacramento, California
Ivor Lewis esophagectomy consists of a laparotomy andright thoracotomy for resection of the intrathoracic esoph-agus. Recent advances in minimally invasive surgical tech-nology have allowed surgeons to apply laparoscopy andthoracoscopy to perform esophagectomy. However, therehave been few reports that describe a totally minimallyinvasive Ivor Lewis esophagectomy. We present a case ofcombined laparoscopic and thoracoscopic resection of thedistal third esophagus with an intrathoracic esophagogas-tric reconstruction for esophageal carcinoma.
(Ann Thorac Surg 2001;72:593–6)© 2001 by The Society of Thoracic Surgeons
Accepted for publication Aug 2, 2000.
Address reprint requests to Dr Nguyen, Department of Surgery, Univer-sity of California, Davis, Medical Center, 2221 Stockton Blvd, 3rd Floor,Sacramento, CA 95817-1418; e-mail: [email protected].
Fig 2. Celiac arteriography showing the contrast blush of a hyper-vascular tumor supplied by the gastroduodenal artery (arrow).
593Ann Thorac Surg CASE REPORT NGUYEN ET AL2001;72:593–6 MINIMALLY INVASIVE ESOPHAGECTOMY
© 2001 by The Society of Thoracic Surgeons 0003-4975/01/$20.00Published by Elsevier Science Inc PII S0003-4975(00)02261-X