
Treatment of Acute Coronary Syndrome with ST elevation ESC guidelines 2008
ESC Guidelines for the management of acute
coronary syndromes in patients presenting
without persistent ST-segment elevation
Chairpersons
JeanJean--Pierre BassandPierre Bassand
Department of CardiologyDepartment of Cardiology
University Hospital Jean University Hospital Jean MinjozMinjoz
BesançonBesançon, France, France
Christian W. HammChristian W. Hamm
Medical Clinic IMedical Clinic I
University Hospital GiessenUniversity Hospital Giessen
& & KerckhoffKerckhoff Heart and Thorax CenterHeart and Thorax Center
Bad Bad NauheimNauheim, Germany, Germany

Members of the Task Force
Christian W. Hamm (Chairperson) (Germany),
Jean-Pierre Bassand (Chairperson), (France),
Stefan Agewall (Norway), Jeroen Bax (The Netherlands), Eric Boersma
(The Netherlands), Hector Bueno (Spain), Pio Caso (Italy), Dariusz Dudek (Poland), (The Netherlands), Hector Bueno (Spain), Pio Caso (Italy), Dariusz Dudek (Poland),
Stephan Gielen (Germany), Kurt Huber (Austria), Magnus Ohman (USA), Mark C.
Petrie (UK), Frank Sonntag (Germany), Miguel Sousa Uva (Portugal), Robert F.
Storey (UK), William Wijns (Belgium), Doron Zahger (Israel).
DisclosuresDisclosures
Honoraria/Consulting/Speakers bureauHonoraria/Consulting/Speakers bureau
Astra ZenecaAstra Zeneca
BayerBayer
Eli LillyEli LillyEli LillyEli Lilly
GSKGSK
IrokoIroko
MSD MSD SheringShering PloughPlough
SanofiSanofi AventisAventis

European Heart Journal Advance Access published August 26, 2011

ESC Guidelines for the Management of NSTE-ACS (6)ESC Guidelines for the Management of NSTE-ACS (6)
European Heart Journal Advance Access published June 14, 2007European Heart Journal Advance Access published June 14, 2007

What is new?• Diagnostic
• High-sensitive troponin introduced
• Echocardiography standard
• Coronary CT for rule-out in low/intermediate risk patients
• Risk Stratification
• 3-hour fast rule-out protocol• 3-hour fast rule-out protocol
• Bleeding risk score (CRUSADE)
• Medical Treatment
• Ticagrelor and prasugrel introduced
• Revascularisation
• Timing of revascularisation

Recommendations for diagnosis and risk stratification 1
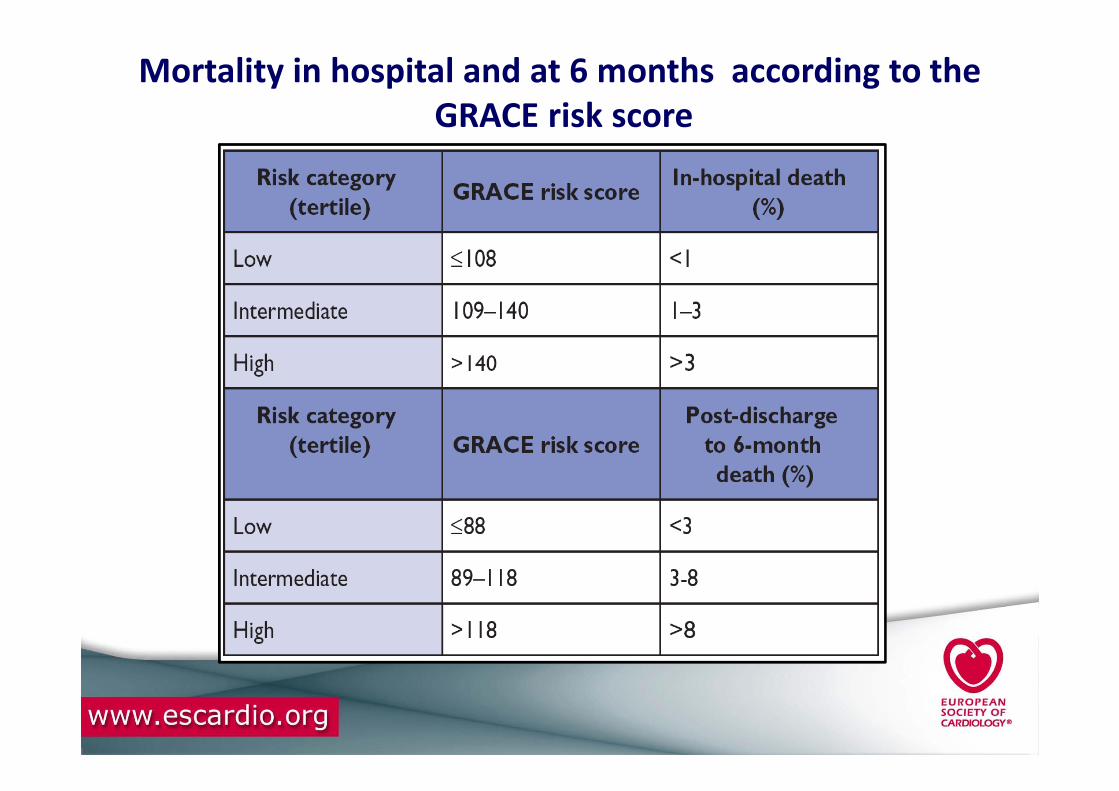
Mortality in hospital and at 6 months according to the
GRACE risk score
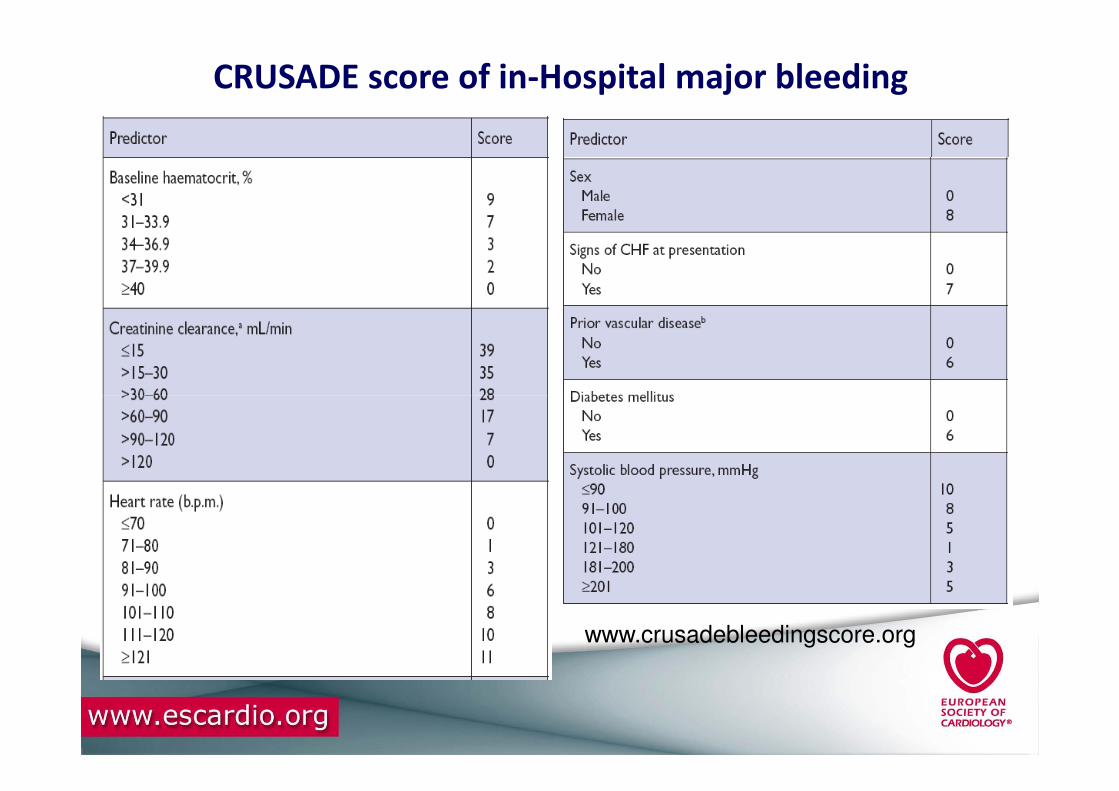
CRUSADE score of in-Hospital major bleeding
www.crusadebleedingscore.org

Risk of major bleeding across the spectrum of CRUSADE bleeding score
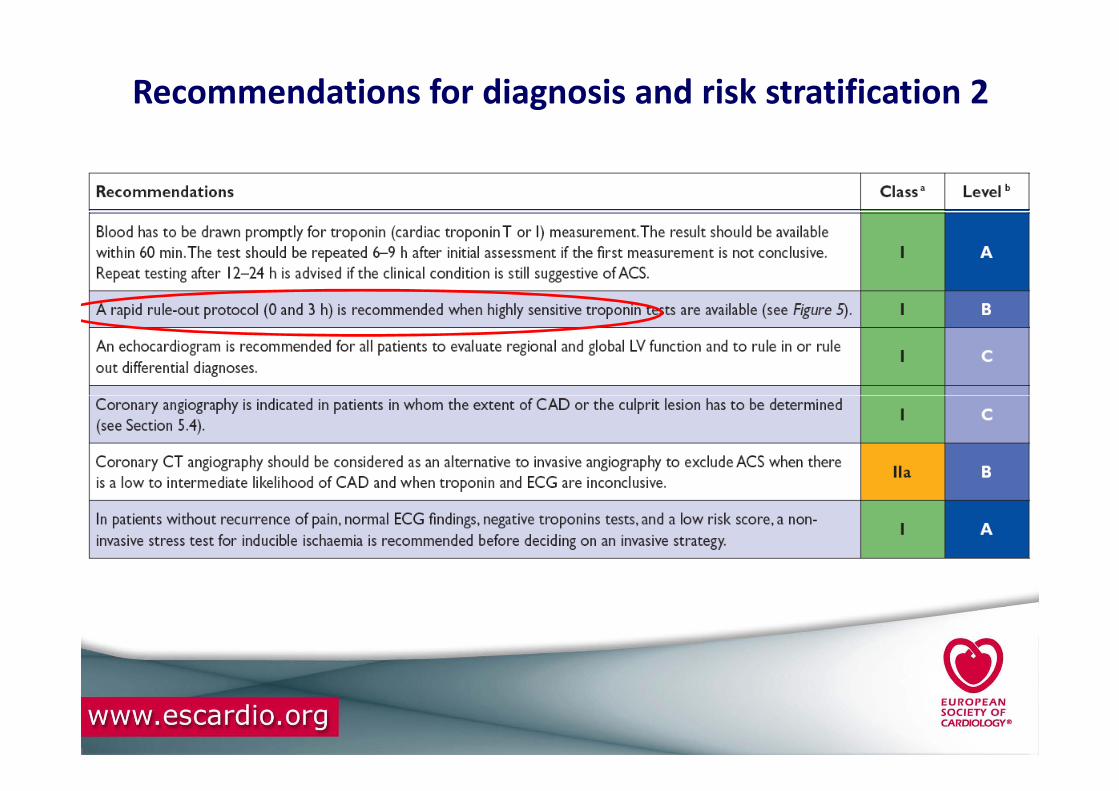
Recommendations for diagnosis and risk stratification 2
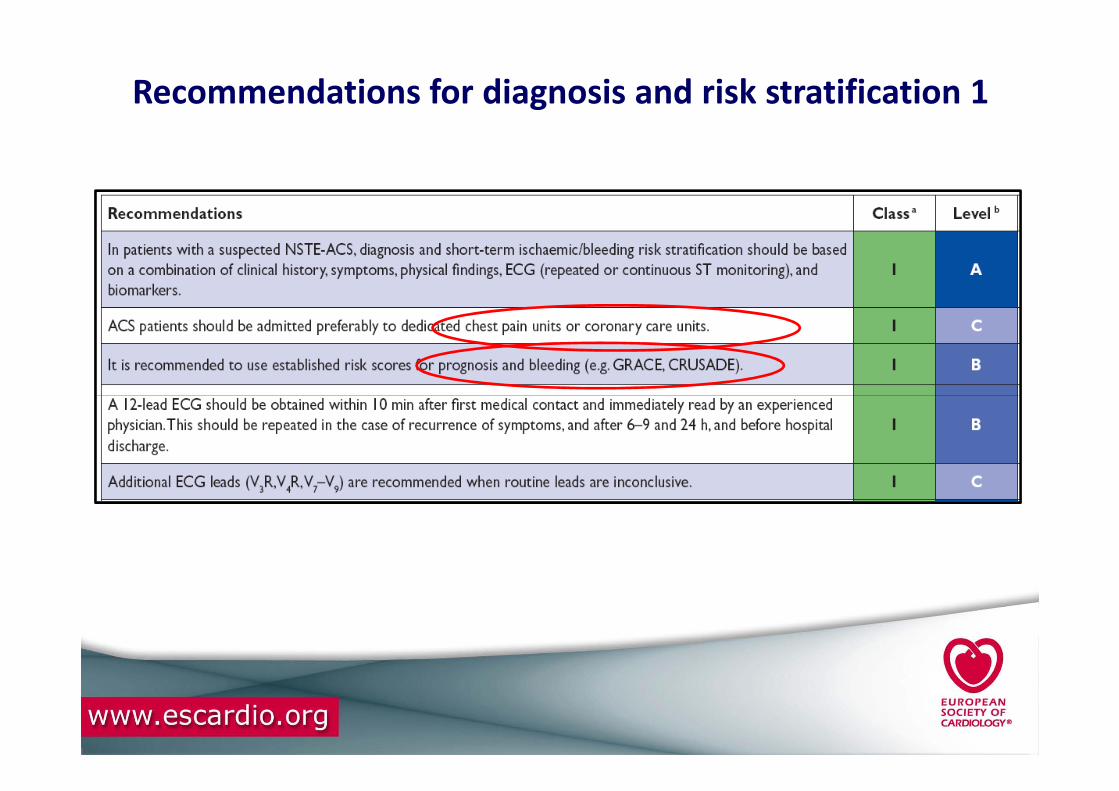
Recommendations for diagnosis and risk stratification 1

Rapid rule-out of ACS with high-sensitivity troponin.

HsTroponin I HsTroponin I AssayAssay and and EarlyEarlyDiagnosisDiagnosis of MIof MI
Keller T JAMA 2011; 306:2684
Hs Troponin I assay at 99 percentile cut-off
At 3 hours:
Sensitivity is 98.2%
NPV is 99.4%
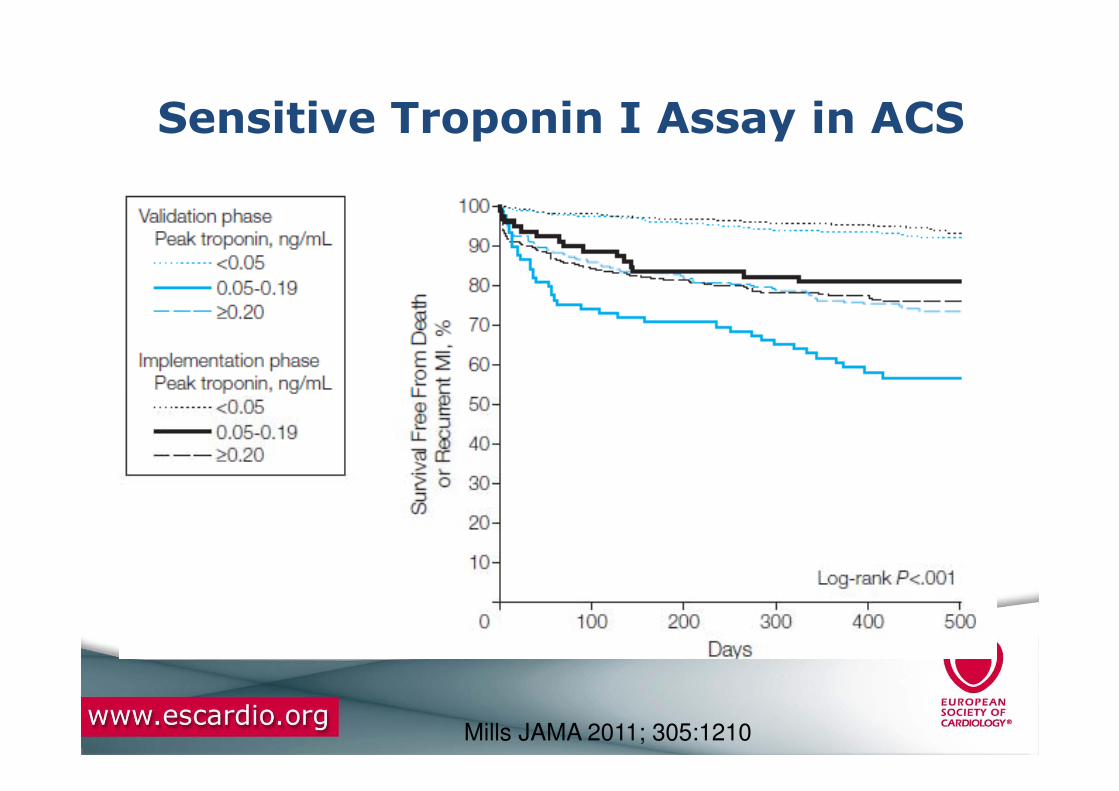
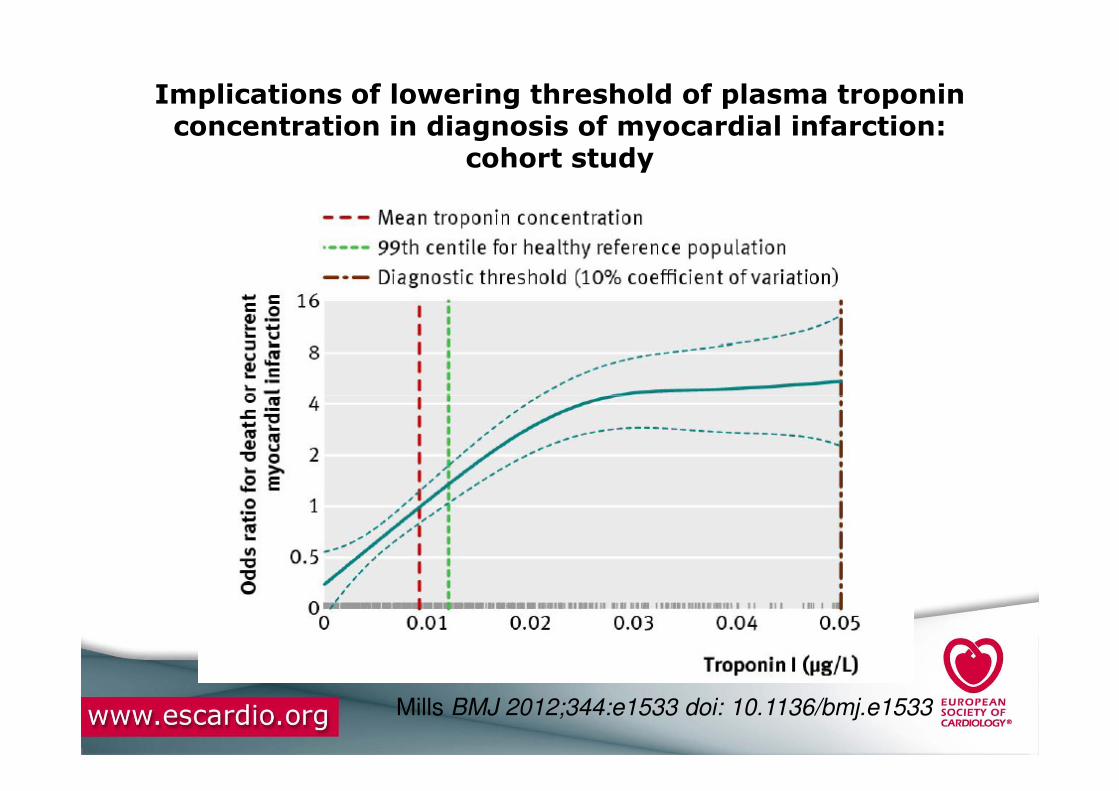
Sensitive Troponin I Assay in ACS
Mills JAMA 2011; 305:1210

Implications of lowering threshold of plasma troponinconcentration in diagnosis of myocardial infarction:
cohort study
Mills BMJ 2012;344:e1533 doi: 10.1136/bmj.e1533
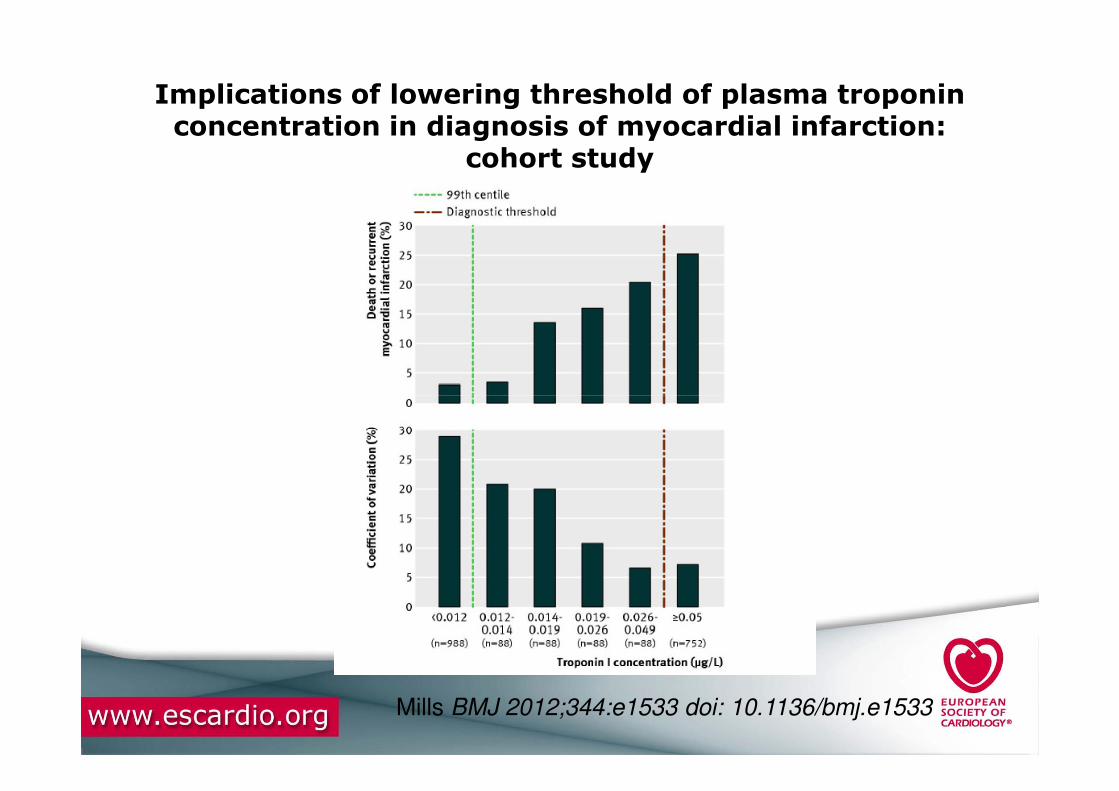
Implications of lowering threshold of plasma troponinconcentration in diagnosis of myocardial infarction:
cohort study
Mills BMJ 2012;344:e1533 doi: 10.1136/bmj.e1533
Implications of lowering threshold of plasma troponinconcentration in diagnosis of myocardial infarction:
cohort study
Mills BMJ 2012;344:e1533 doi: 10.1136/bmj.e1533

Keller T N Engl J Med 2009; 361:868

Keller T N Engl J Med 2009; 361:868

Troponin elevation
Possible non-acute coronary
syndrome causes syndrome causes
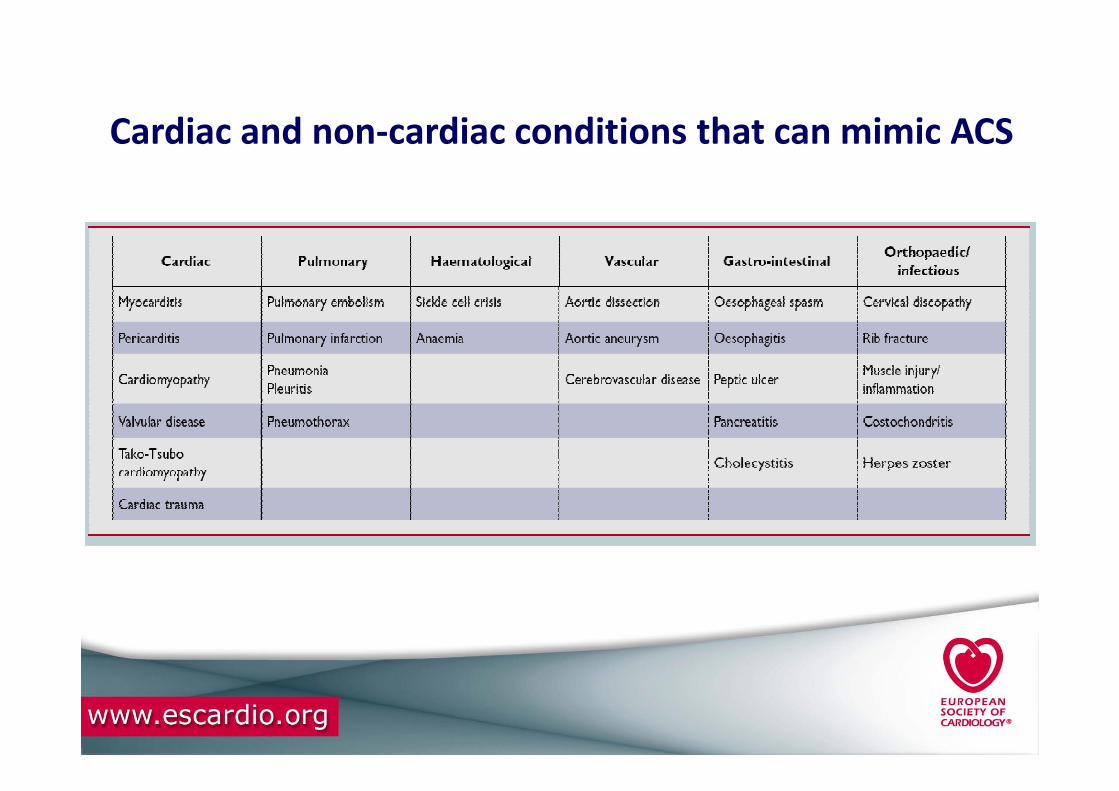
Cardiac and non-cardiac conditions that can mimic ACS
What is new?• Diagnostic
• High-sensitive troponin introduced
• Echocardiography standard
• Coronary CT for rule-out in low/intermediate risk patients
• Risk Stratification
• 3-hour fast rule-out protocol• 3-hour fast rule-out protocol
• Bleeding risk score (CRUSADE)
• Medical Treatment
• Ticagrelor and prasugrel introduced
• Revascularisation
• Timing of revascularisation

AspirinAspirin
Class Level
25

P2Y12 Inhibitors

Class Level
P2YP2Y1212 inhibitor recommendations 1inhibitor recommendations 1
27
Class Level

Class Level
P2YP2Y1212 inhibitor recommendations 2inhibitor recommendations 2
28

PLATO: time to first primary efficacy PLATO: time to first primary efficacy
event (composite of CV death, MI or stroke)event (composite of CV death, MI or stroke)
12111098765
13
Cum
ula
tive incid
ence (
%)
9.8
11.7Clopidogrel
Ticagrelor
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,521
8,628
8,362
8,460
8,124
Days after randomisation
6,743
6,743
5,096
5,161
4,047
4,147
0 60 120 180 240 300 360
543210Cum
ula
tive incid
ence (
%)
8,219
HR 0.84 (95% CI 0.77–0.92), p=0.0003
Curves are Kaplan-Meier rates, HR = hazard ratio; CI = confidence interval

6
5
4
3
7
Cu
mu
lative
in
cid
en
ce
(%
)
Clopidogrel
Ticagrelor
5.8
6.9
6
4
3
Clopidogrel
Ticagrelor
4.0
5.1
7
5
Myocardial infarction Cardiovascular death
Cu
mu
lative
in
cid
en
ce
(%
)
Secondary efficacy endpoints over time Secondary efficacy endpoints over time
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,560
8,678
8,405
8,520
8,177
Days after randomisation
6,703
6,796
5,136
5,210
4,109
4,191
0 60 120 180 240 300 360
3
2
1
0
Cu
mu
lative
in
cid
en
ce
(%
)
8,279
HR 0.84 (95% CI 0.75–0.95), p=0.005
0 60 120 180 240 300 360
3
2
1
0HR 0.79 (95% CI 0.69–0.91), p=0.001
9,291
9,333
8,865
8,294
8,780
8,822
8,589
Days after randomisation
7079
7119
5,441
5,482
4,364
4,4198,626
Cu
mu
lative
in
cid
en
ce
(%
)

TicagrelorTicagrelor
Class Level
31
10
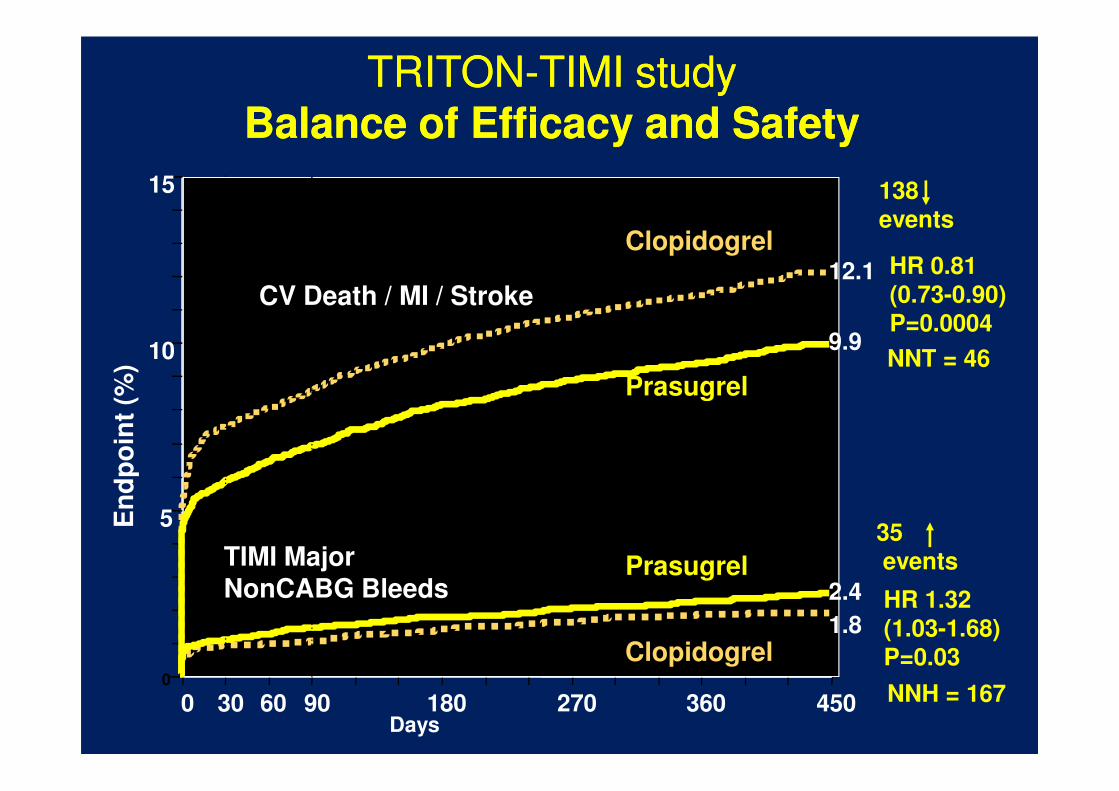
15
HR 0.81(0.73-0.90)
P=0.0004
Prasugrel
Clopidogrel
En
dp
oin
t (%
)
12.1
9.9
138
events
TRITONTRITON--TIMI study TIMI study Balance of Efficacy and SafetyBalance of Efficacy and Safety
CV Death / MI / Stroke
NNT = 46
0
5
0 30 60 90 180 270 360 450
Prasugrel
Days
En
dp
oin
t (%
)
HR 1.32
(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.8
2.4
35
events TIMI Major NonCABG Bleeds
NNH = 167
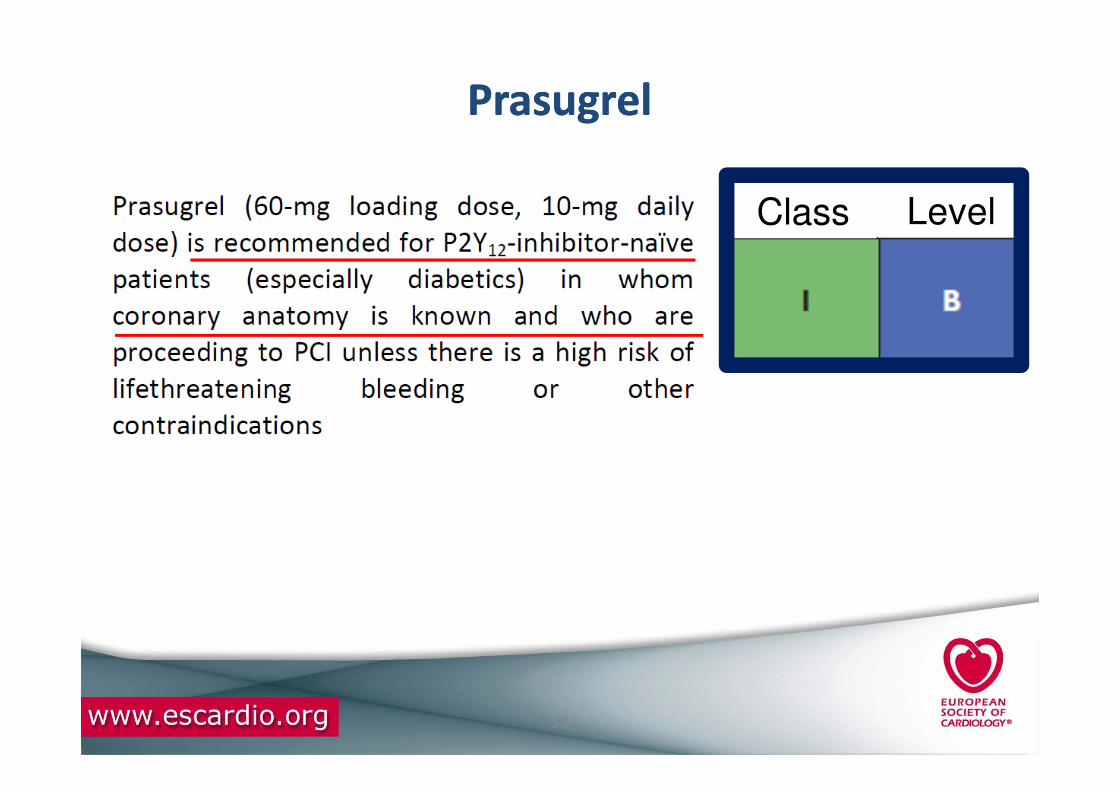
PrasugrelPrasugrel
Class Level
33

ClopidogrelClopidogrel dosingdosing
Class Level
Class Level
34
Class Level

ClopidogrelClopidogrel response variabilityresponse variability
Class Level
35
Class Level

GP IIb/IIIa receptor inhibitorGP IIb/IIIa receptor inhibitor
Class Level
36
Class Level

15
20
Death/MI/UTVR, %
ISAR-REACT 2: Outcomes according to Tn level
Troponin-Positive: RR=0.71 [0.54-0.95]
0
5
10
0 5 10 15 20 25 30
Days after randomization
Abciximab vs. Placebo
Troponin-Negative: RR=0.99 [0.56-1.76]
Kastrati A et al. JAMA 2006

ACUITY TimingACUITY Timing
11,7% 11,7%
30 d
ay e
ve
nts
(%
)
Routine Upstream IIb/IIIa (N=4605) Deferred PCI IIb/IIIa (n=4602)
Routine Upstream IIb/IIIa vs. Deferred PCI IIb/IIIaRoutine Upstream IIb/IIIa vs. Deferred PCI IIb/IIIa
PNI <0.0001
PSup = 0.93
PNI = 0.044
PSup = 0.13
PNI < 0.0001
PSup = 0.009
7,1%6,1%
4,9%
7,9%
Net clinical
outcome
Ischemic
composite
Major bleeding
30 d
ay e
ve
nts
(%
)
Stone, G. W. et al. JAMA 2007;297:591-602
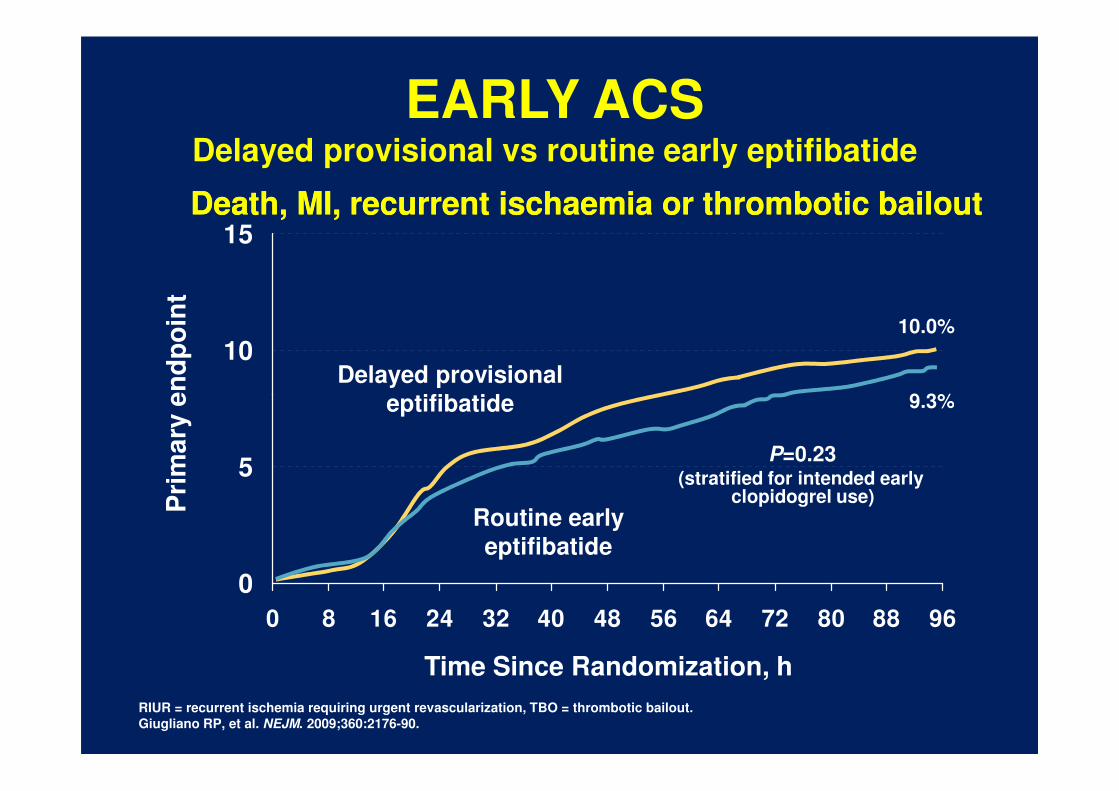
10
15Death, MI, Death, MI, recurrent recurrent ischaemiaischaemia or thrombotic bailoutor thrombotic bailout
Pri
ma
ry e
nd
po
int
10.0%
9.3%
Delayed provisionaleptifibatide
EARLY ACSDelayed provisional vs routine early eptifibatide
0
5
0 8 16 24 32 40 48 56 64 72 80 88 96
RIUR = recurrent ischemia requiring urgent revascularization, TBO = thrombotic bailout.
Giugliano RP, et al. NEJM. 2009;360:2176-90.
Pri
ma
ry e
nd
po
int
Time Since Randomization, h
9.3%
P=0.23(stratified for intended early
clopidogrel use)
eptifibatide
Routine early
eptifibatide
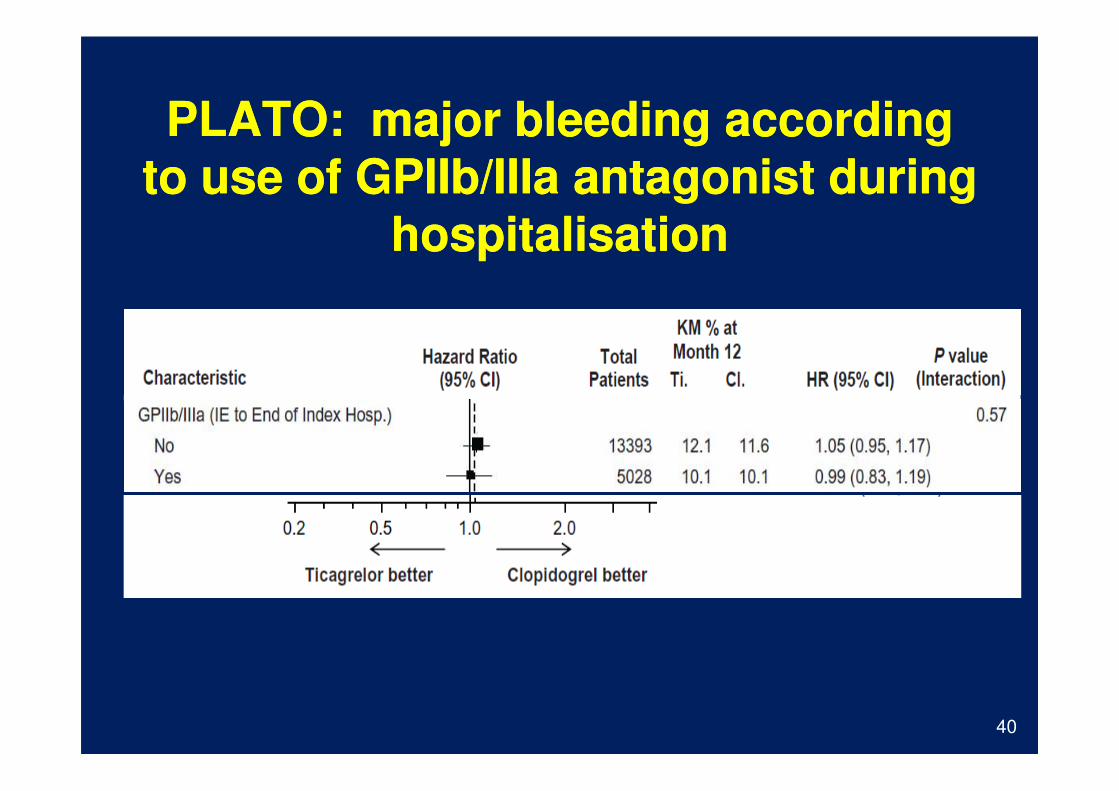
PLATO: major bleeding according PLATO: major bleeding according
to use of to use of GPIIbGPIIb//IIIaIIIa antagonist during antagonist during
hospitalisationhospitalisation
40

Upstream GP IIb/IIIa receptor inhibitorUpstream GP IIb/IIIa receptor inhibitor
Class Level
Class Level
41
Class Level
Class Level
BivalirudinBivalirudin vsvs GPIIbGPIIb//IIIaIIIa antagonistsantagonists
Class Level
42

AnticoagulantsAnticoagulants
Class Level
43
Class Level

Death/MI/RI: Day 9C
um
ula
tive
Ha
za
rd
0.0
30
.04
0.0
50.0
6
Days
Cu
mu
lative
Ha
za
rd
0.0
0.0
10
.02
0.0
3
0 1 2 3 4 5 6 7 8 9
Enoxaparin
Fondaparinux
HR 1.01
95% CI 0.90-1.13
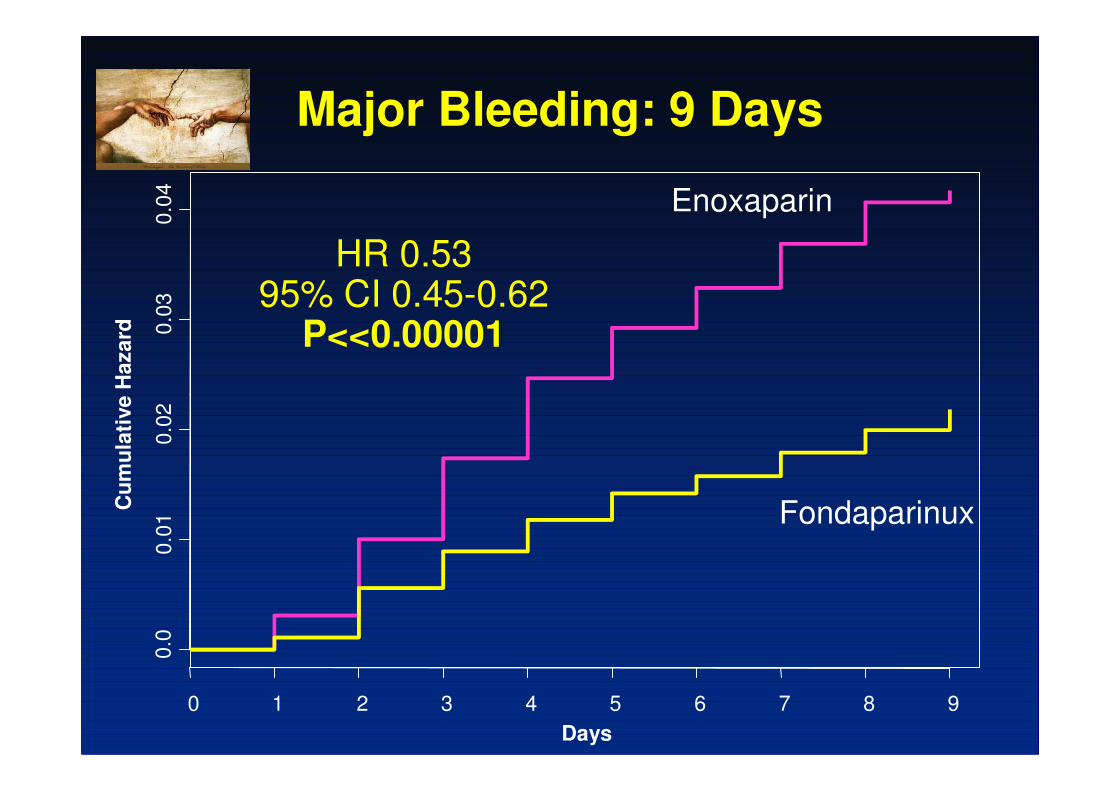
Major Bleeding: 9 DaysC
um
ula
tive H
azard 0
.03
0.0
4
HR 0.53 95% CI 0.45-0.62
P<<0.00001
Enoxaparin
Days
Cu
mu
lati
ve H
azard
0.0
0.0
10.0
2
0 1 2 3 4 5 6 7 8 9
Fondaparinux
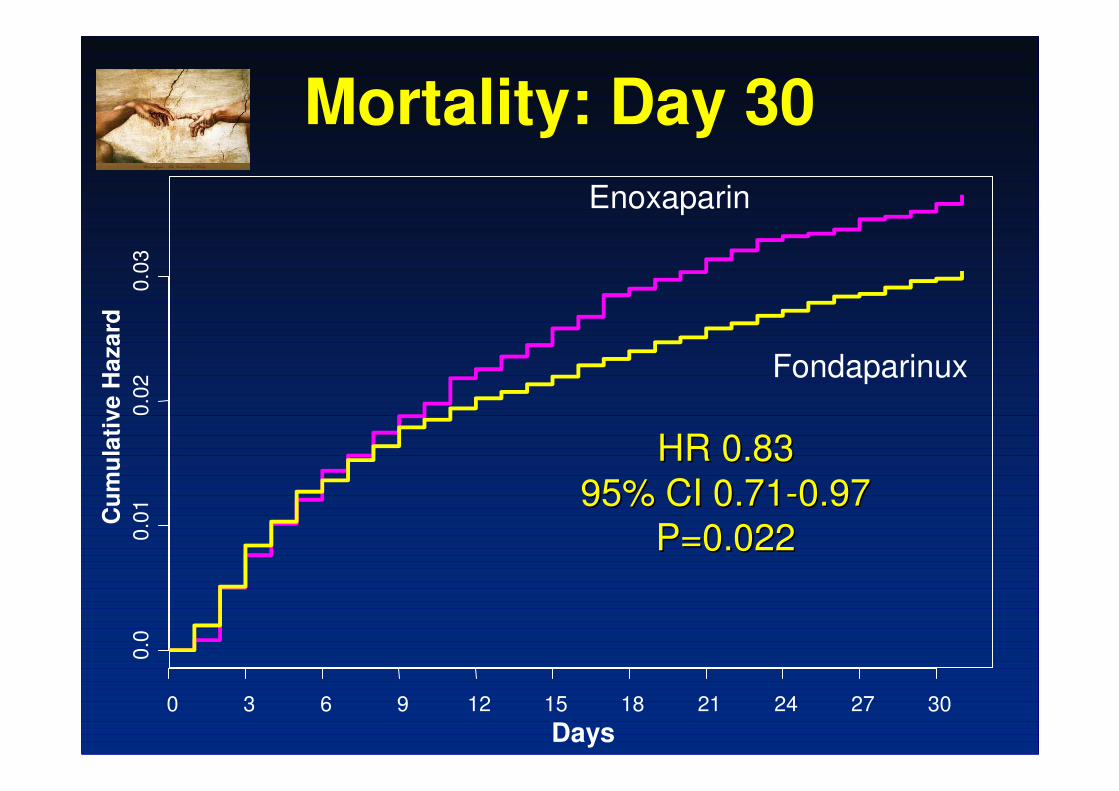
Mortality: Day 30C
um
ula
tive H
aza
rd0.0
20.0
3
Enoxaparin
Fondaparinux
Days
Cu
mu
lati
ve H
aza
rd0.0
0.0
10.0
2
0 3 6 9 12 15 18 21 24 27 30
HR 0.83 HR 0.83
95% CI 0.7195% CI 0.71--0.970.97
P=0.022P=0.022
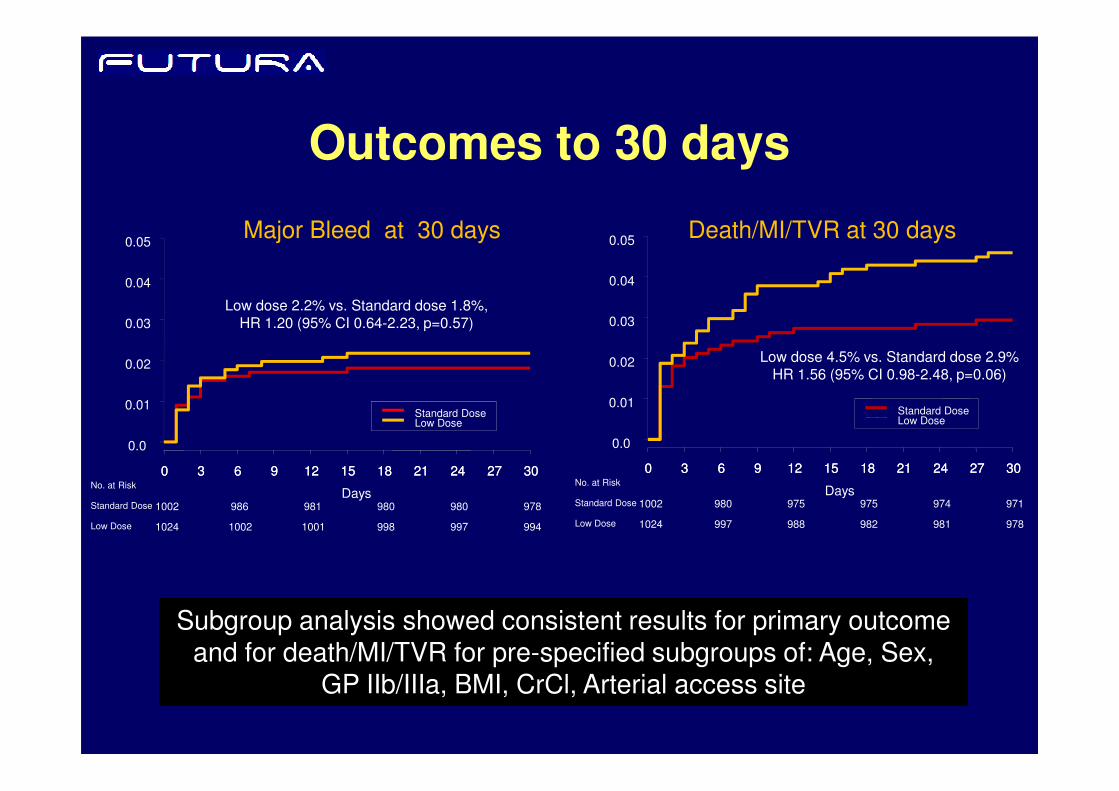
Outcomes to 30 days
Low dose 2.2% vs. Standard dose 1.8%, HR 1.20 (95% CI 0.64-2.23, p=0.57)
Major Bleed at 30 days
0.02
0.03
0.04
0.05
0.01
0.02
0.03
0.04
0.05Death/MI/TVR at 30 days
Low dose 4.5% vs. Standard dose 2.9%HR 1.56 (95% CI 0.98-2.48, p=0.06)
Subgroup analysis showed consistent results for primary outcome and for death/MI/TVR for pre-specified subgroups of: Age, Sex,
GP IIb/IIIa, BMI, CrCl, Arterial access site
Days
3 6 9 12 15 18 21 24 27 303 6 9 12 15 18 21 24 27 3000
0.0
0.01Standard DoseLow Dose
No. at Risk
Standard Dose
Low Dose
1002 986 981 980 980 978
1024 1002 1001 998 997 994
Days
0 3 6 9 12 15 18 21 24 27 300 3 6 9 12 15 18 21 24 27 30
0.0
0.01Standard DoseLow Dose
No. at Risk
Standard Dose
Low Dose
1002 980 975 975 974 971
1024 997 988 982 981 978

FondaparinuxFondaparinux
Class Level
48
Class Level

HeparinsHeparins
Class Level
Class Level
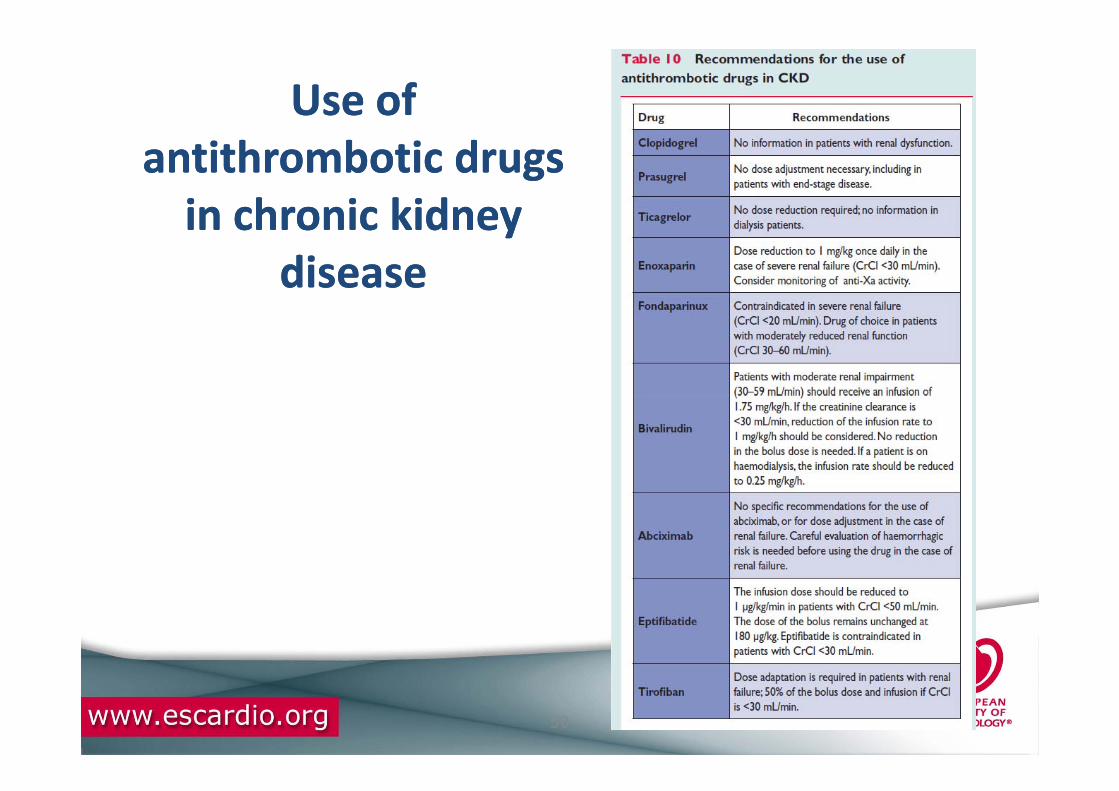
Use of Use of
antithrombotic drugs antithrombotic drugs
in chronic kidney in chronic kidney
diseasedisease
50

Recommendations for oral antiplatelet agents 1
PLATO
TRITON-TIMI 38

Recommendations for GP IIb/IIIa receptor inhibitorsCH9

Dia 52
CH9 Tabelle teilen, nebeneinander auf 1 SeiteProf. Dr. Christian Hamm; 21-8-2011
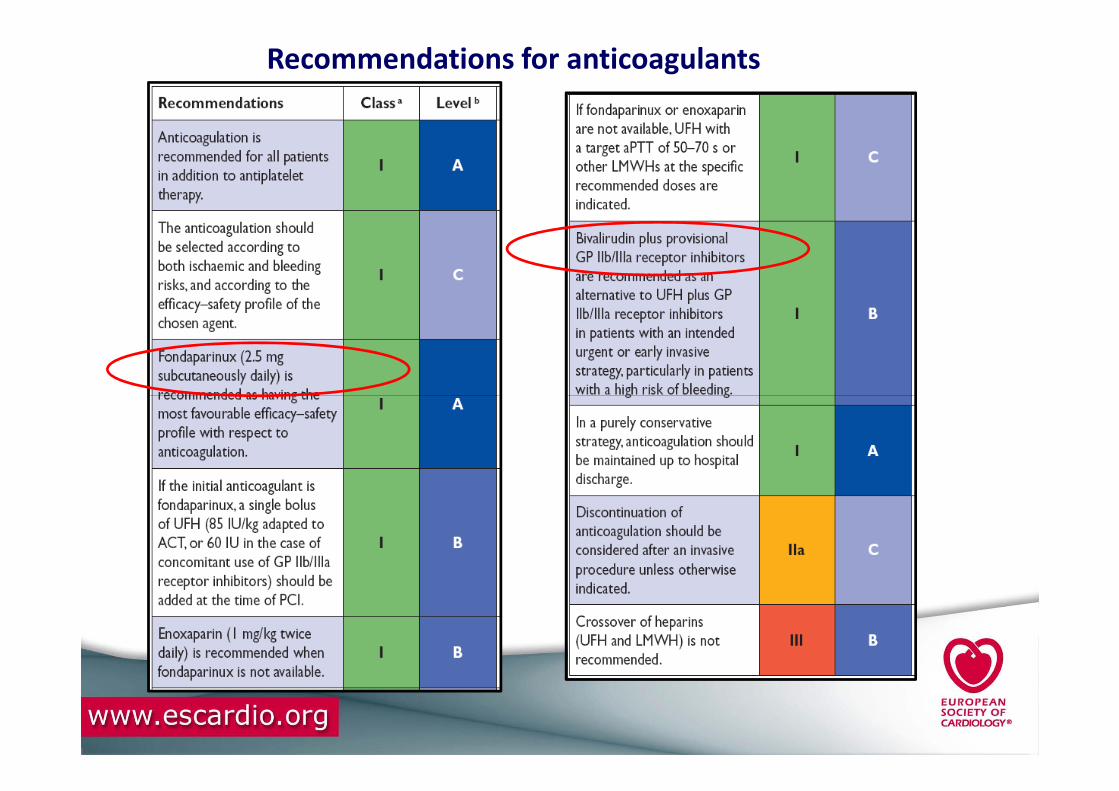
Recommendations for anticoagulants
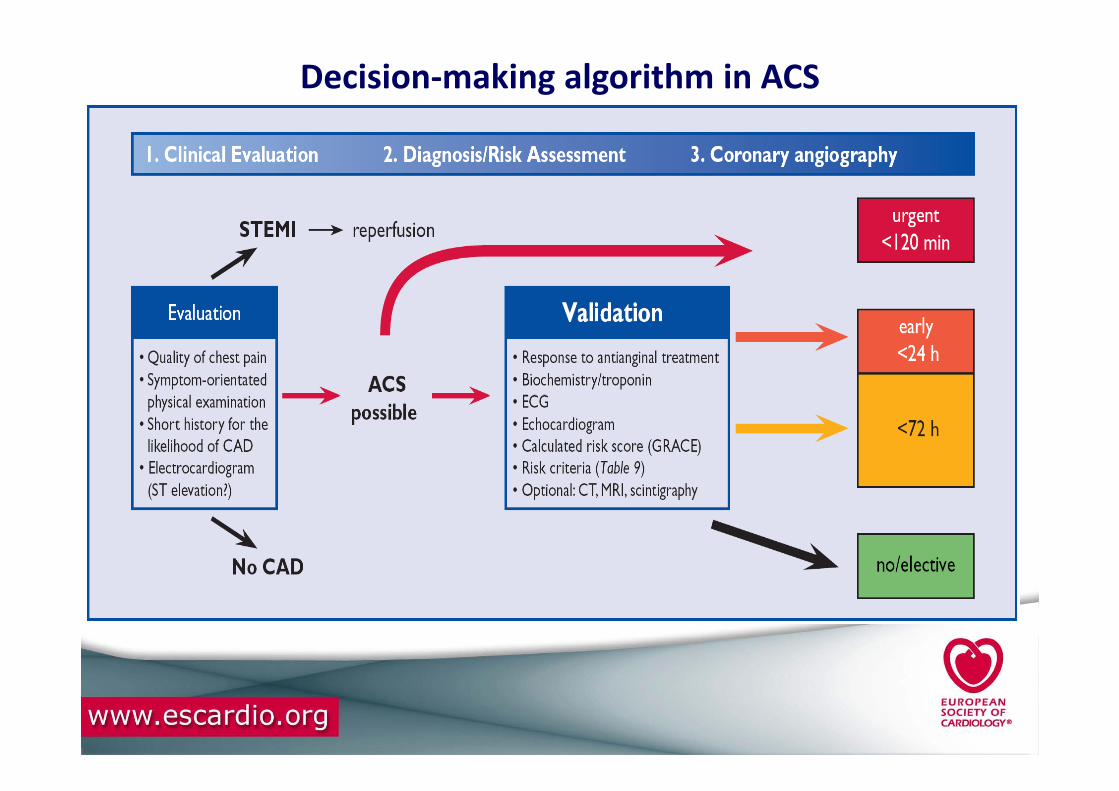
Decision-making algorithm in ACS
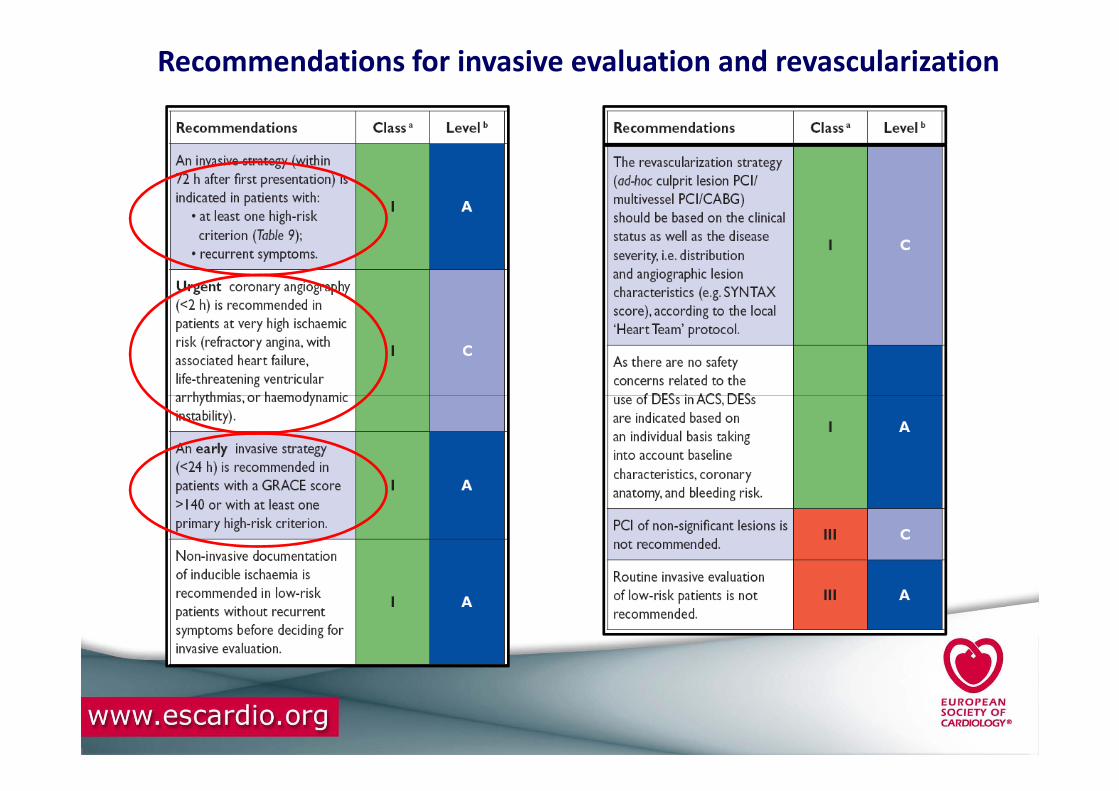
Recommendations for invasive evaluation and revascularization
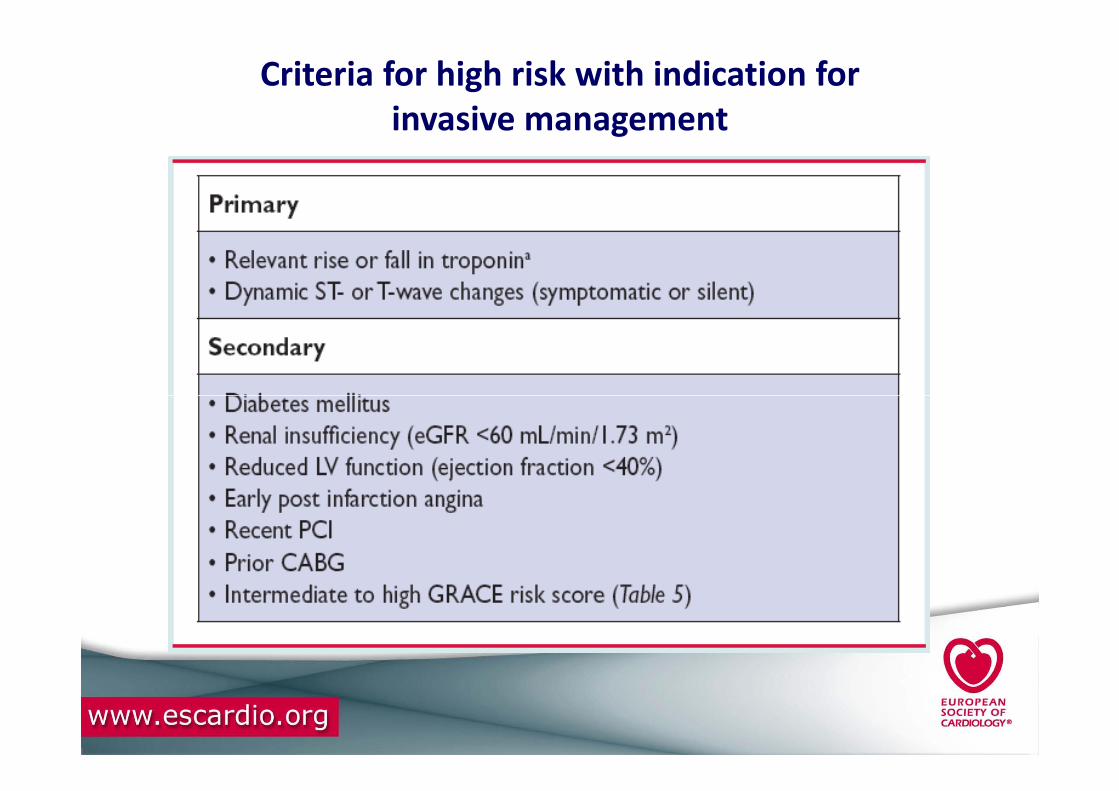
Criteria for high risk with indication for
invasive management
“Management Strategy”
of NSTE - ACSof NSTE - ACS

Management of NSTE - ACS
• Step 1: Initial evaluation
• Step 2: Diagnosis validation and
risk assessment
• Step 3: Invasive strategy• Step 3: Invasive strategy
• Step 4: Revascularisation modality
• Step 5: Hospital discharge and
post-discharge

Initial therapeutic measures
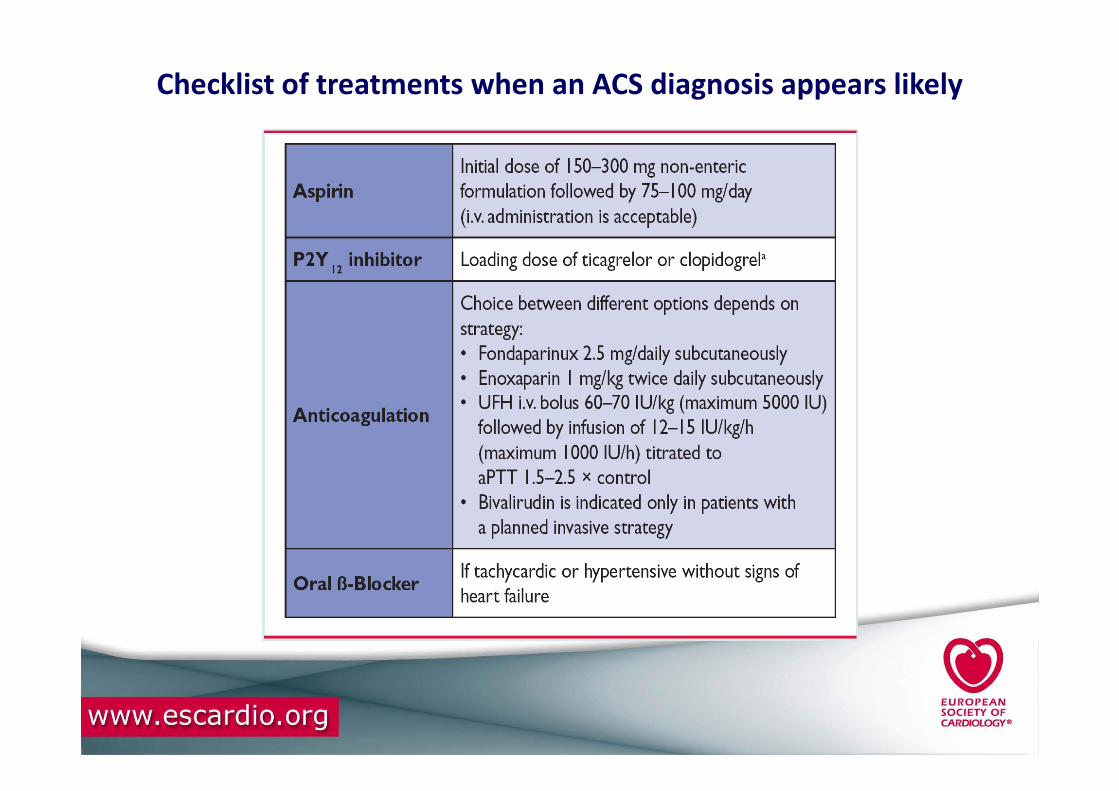
Checklist of treatments when an ACS diagnosis appears likely

Checklist of antithrombotic treatments prior to PCI
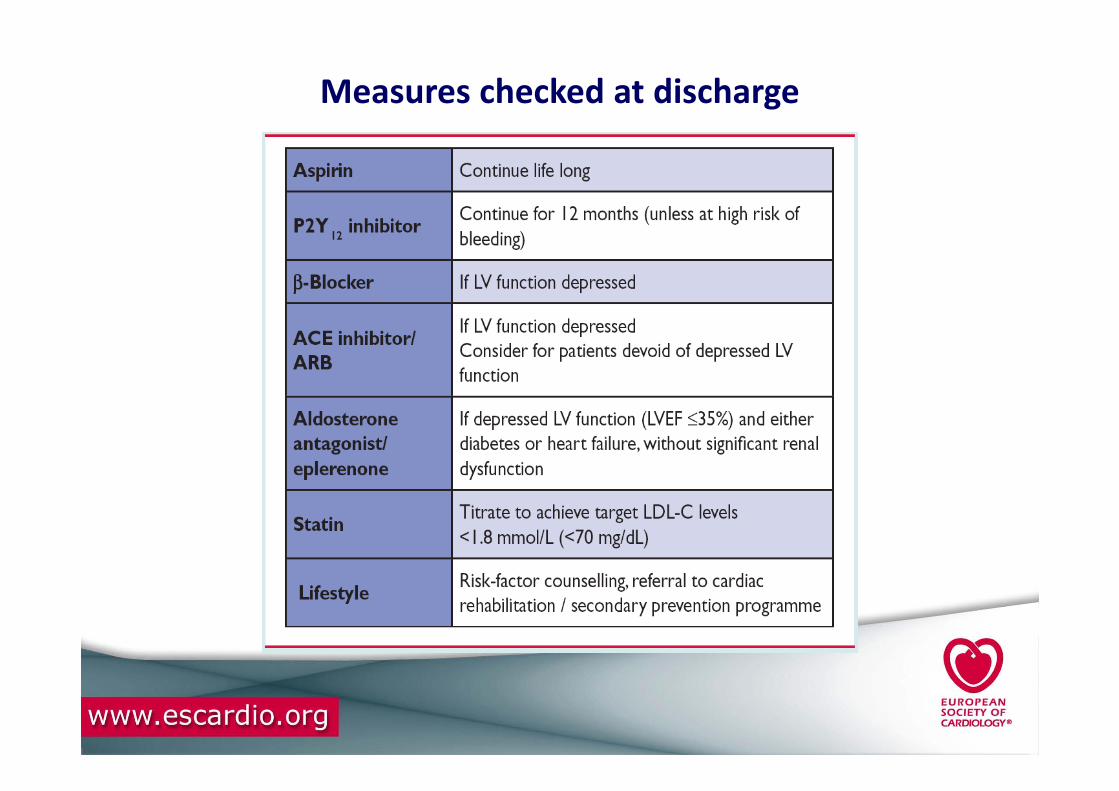
Measures checked at discharge
Take Home messages
• NSTE-ACS is a frequent cause of hospitalization
Heterogenous population as regards risk
• Diagnostics
• Clinical presentation, ECG, troponin
• High-sensitive troponin introduced
• Echocardiography for everybody
• Coronary CT for rule-out in low/intermediate risk patients
• Risk Stratification
• 3-hour fast rule-out protocol based on hs-troponin
• Ischaemic risk (GRACE score )
• Bleeding risk (CRUSADE score )

Take Home messages (continued 1)
• First line antithrombotic treatment
• Ticagrelor and prasugrel recently introduced
• Revascularisation
• Timing of revascularisation customized according to risk
– Within 72 hours anyway, but
– Within 2 hours for very high risk patients (lifethreatening symptoms)
– Within 24 hours for patients with high risk criteria (GRACE score > 140,
troponin release, ST-T changes)
• Non invasive evaluation for low risk patients
Take Home messages (continued 2)
• Special populations and situations
• Diabetes, elderly, women, CKD, anaemia.....
• Bleeding complications ...
• Long term secondary prevention
• Secondary prevention programmes
• Lifestyle
• Drug therapy

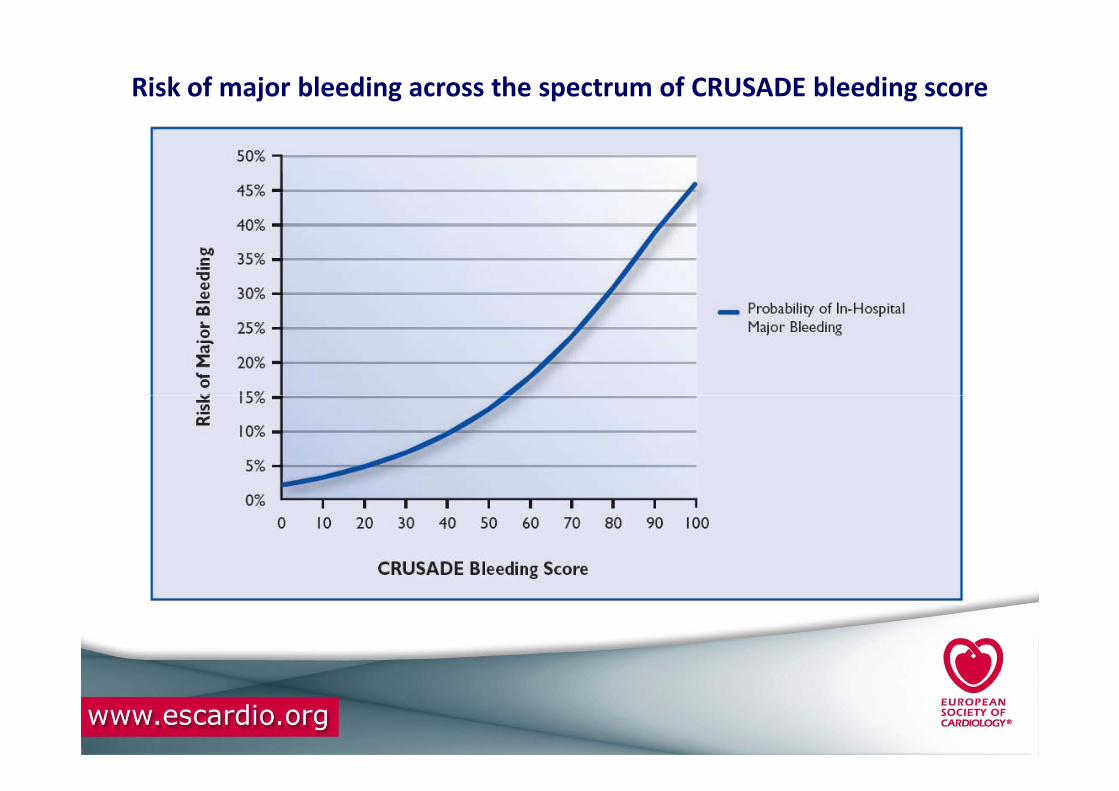
Risk of major bleeding across the spectrum of CRUSADE bleeding score

Ten Take home messages
1 - NSTE-ACS is a frequent cause of hospitalization
2 - Heterogenous population as regards risk
3 - Diagnostic• Clinical presentation
• ECG
• (High-)sensitive troponin
• Echocardiography standard for all
• Coronary CT for rule-out in low/intermediate risk patients
4 - Risk Stratification• 3-hour fast rule-out protocol based on hs-troponin
• Ischaemic risk (GRACE score )
• Bleeding risk (CRUSADE score )

5 - Antischaemic Therapy
6 - Antiplatelet treatment • Aspirin lifelong for all, plus
• Ticagrelor (12 months) or
• Prasugrel (only prior PCI)
• Clopidogrel , if ticagrelor and prasugrel not available
• Glycoprotein IIb/IIIa in high risk patients, but not
Ten Take home messages
• Glycoprotein IIb/IIIa in high risk patients, but not routinely upstream
7 - Anticoagulation• Fondaparinux best benefit/ risk profile (add UFH if PCI)
• Enoxaparin, other low molecular weight heparins or unfractionated heparin are less recommended options
• Bivalirudin in high risk bleeding as alternative to GP IIb/IIIa + UFH in patients undergoing PCI
8 - Revascularisation• Timing of revascularisation customized according to risk
– Within 72 hours all patients at risk, but
– Within 2 hours for very high risk patients (lifethreateningsymptoms)
– Within 24 hours for patients with high risk criteria (GRACE score > 140, troponin release, ST-T changes)
• Non invasive evaluation for low risk patients
Ten Take home messages
• Non invasive evaluation for low risk patients
9 - Special populations and situations• Special attention to diabetes, elderly, women, CKD,
anaemia.
• Adjust medication doses according to renal function
10 - Long term management, secondary prevention

Thank you !Thank you !


















