Erin Clare Laing - minerva-access.unimelb.edu.au
306
Understanding nutrition-related symptoms, complications and health-related quality of life in patients with gastroenteropancreatic neuroendocrine tumours Erin Clare Laing ORCID ID: 0000-0003-1296-6948 Doctor of Philosophy February 2021 Department of Nursing Faculty of Medicine, Dentistry and Health Sciences The University of Melbourne Submitted in total fulfilment of the requirements of the degree of Doctor of Philosophy
Transcript of Erin Clare Laing - minerva-access.unimelb.edu.au
Understanding nutrition-related symptoms, complications and
health-related quality of life in patients with
gastroenteropancreatic neuroendocrine tumours
Erin Clare Laing
ORCID ID: 0000-0003-1296-6948
Doctor of Philosophy
February 2021
Department of Nursing
Faculty of Medicine, Dentistry and Health Sciences
The University of Melbourne
Submitted in total fulfilment of the requirements of the degree of
Doctor of Philosophy


iii
Abstract
Gastroenteropancreatic neuroendocrine tumours (GEP NET) can lead to complex
symptoms and reduced health-related quality of life (HRQoL). The management of
GEP-NETs is challenging. To date there has been development of clinical practice
guidelines and consensus guidelines for GEP-NETs; however, the supportive care needs
and optimal nutritional management of patients affected by GEP-NETs remains under-
researched and evidence to guide clinical practice is lacking. These malignancies have
the potential to significantly impact on patient morbidity, HRQoL and nutrition due to
the tumour location, functional status (secretion of hormones), symptoms and
treatment. A limited number of published cross-sectional studies have indicated the
presence of nutritional issues among patients with a GEP NET, including malnutrition
(in 14-25%) and the presence of vitamin (niacin and fat-soluble vitamin) deficiencies.
There is mostly anecdotal evidence for dietary change among patients with a GEP NET,
and few studies have explored this phenomenon and its impact on patients.
The aim of this thesis was to comprehensively describe the nutritional complications of
GEP NET, and to explore the nutritional knowledge and practices of health
professionals managing patients with a NET, enabling the first summary of NET health
professional practices in regard to nutrition. A prospective longitudinal mixed-methods
study was undertaken to comprehensively explore the prevalence of nutritional
complications in patients diagnosed with a GEP NET. Patients recruited to this study
had reduced HRQoL, specifically social functioning; and the presence of anxiety,
depression and financial toxicity was observed. Common symptoms, reported in 40-
80% of participants, were fatigue, abdominal discomfort, pain, bloating, wind/gas and
diarrhoea. Results of this study showed that malnutrition was prevalent in up to 29%
of patients, as was weight loss (up to 51%), loss of muscle mass (up to 62%) and
dietary change (up to 56%), and all nutritional complications remained so over the six-
month study period. Patient interviews conducted during the study period
demonstrated the negative impact of a GEP NET diagnosis on patient’s HRQoL, and
that dietary change and food restriction was often initiated by patients in response to

iv
their symptom burden. Nutrition and dietary information/management was identified
by patients as an un-met need. Results of an exploratory mixed-methods health
professional study showed that only 38% of NET health professionals are routinely
performing screening for nutrition-related complications. Nutrition advice and
management was varied and inconsistent, with health professionals identifying a lack
of NET-specific nutrition evidence and guidelines as barriers to their practice.
Results of the studies reported in this thesis contribute evidence and knowledge
towards the presence and severity of nutritional complications among patients with a
GEP NET, which are often under-recognised and impact on patient HRQoL. Results also
provide the first summary of NET health professional nutrition-related practices.
Results highlight the importance of identifying nutritional complications in this unique
patient group and provide key insights into the nutrition risk factors relevant to
patients with a GEP NET. This thesis will contribute to the future development of NET-
specific nutrition guidelines and establishment of a robust nutrition risk screening
process for NETs.

v
Declaration
This is to certify that:
i. This thesis comprises only my original work towards the PhD except where
indicated in the preface,
ii. Due acknowledgement has been made in the text to all other material used,
iii. This thesis is fewer than 100,000 words in length, exclusive of tables, maps,
bibliographies and appendices
Signed
………………………………………………………………


vii
Preface
This thesis and the work that contributed to it was carried out primarily by the PhD
candidate, Erin Laing, with contribution from all supervisors (Professor Meinir
Krishnasamy, Dr Nicole Kiss and Professor Michael Michael). Statistical support was
received from statistician Associate Professor Karla Gough, with the statistical planning
and analysis undertaken by EL.
The results of the comprehensive literature review in Chapter 1 were published in April
2020. This manuscript was written in collaboration with my supervisors (MK, NK, MM)
and the final published version has been included in Chapter 1.
The research protocol for the Phase 1 longitudinal mixed-methods study in Chapter 2
was published in December 2018. This manuscript was written in collaboration with
my supervisors (MK, NK, MM) and a statistician (KG), and the final published version
has been included in Chapter 2.
The results of the international online survey of NET health professionals, discussed in
Chapter 6, have been prepared as two manuscripts for publication. These manuscripts
were written in collaboration with my supervisors (MK, NK, MM) and a statistician
(KG). The word document of final approved manuscripts is included as unpublished
material in Chapter 6. EL conceived and designed the study with assistance from NK,
MM, MK and KG. EL conducted recruitment and data collection. EL performed data
analysis with assistance from KG. EL drafted the manuscript. All authors revised the
manuscripts critically for important intellectual content and approved the final version
for submission. The final version of these manuscripts included in Chapter 6 are
planned for submission to a journal in October 2020.
The research presented in this thesis was primarily supported by funding received
from the Victorian Cancer Agency, Victorian Government, Melbourne, Australia; and
Austin Health, Melbourne, Australia; through the Olivia Newton John Cancer, Wellness

viii
and Research Centre (ONJCWRC) Supportive Care Research PhD Scholarship awarded
to EL in December 2016. EL received funding through this scholarship towards their
PhD stipend and research costs. EL received initial seed funding for their PhD stipend
between August to December 2016 from the Nutrition and Speech Pathology
Department, and Neuroendocrine Unit at Peter MacCallum Cancer Centre, Melbourne,
Australia. EL received additional funding from Ipsen Australia and NeuroEndocrine
Cancer Australia (formerly Unicorn Foundation Australia) towards PhD research costs.
Funding sources were not involved in the conception, preparation or writing of any
research studies or manuscripts.

ix
Acknowledgements
The journey to PhD completion has been full of hard work and some challenges,
combined with inspiring moments and contributions from surrounding researchers,
clinicians, patients, and support people all of who I wish to thank.
To my supervisors Mei Krishnasamy, Nicole Kiss and Michael Michael, thank you for
your unwavering support and inspiration. I have considered myself very lucky to have
such a dedicated and supportive supervision team throughout my PhD. Mei, I thank
you for your constant leadership and encouragement, I have learnt so much from you
about research and your passion for helping patients through research has been an
inspiration. Nicole, I thank you for pushing me to commence a PhD and for the
constant support, nutrition expertise and opportunities you’ve provided throughout
the process. Michael, I thank you for your guidance and professional insight, and for
helping me shape a profile in the NET clinical and research space.
To my advisory committee, led by Anna Boltong, and including Snezana Kusiljic and
Judy Bauer, thank you for all your professional advice and support. To Karla Gough,
thank you for your invaluable guidance and support with my statistical analysis. I have
appreciated learning from you. To the Cancer Nursing Research team, I really valued
my time sitting in your department, and thank you for your support, research guidance
and friendship. I particularly wish to thank Cath Devereux and Carol Jewell who
assisted me as co-facilitators during my health professional focus groups.
To the Peter Mac Nutrition and Speech Pathology team, your support and interest in
my research has been very encouraging and kept me motivated. Special thanks to
Jenelle Loeliger and Belinda Steer for supporting me to work part-time and develop as
a clinician researcher. Thanks to Kirsty Rowan and Jacq Black for assisting with data
collection when I had to take leave.

x
To the NET unit and multidisciplinary team at Peter Mac, thank you for welcoming me
into the team as a dietitian and researcher. I am thankful to work so closely with such
as professional and patient-cantered group. Thank you to Niall Tebbutt at Austin
Health for assisting to coordinate recruitment at that site.
I’d like to acknowledge my funders, including the Victorian Cancer Agency and Austin
Health (ONJCRWC) scholarship that supported and enabled me to complete this PhD. I
also wish to acknowledge NeuroEndocrine Cancer Australia (formerly the Unicorn
Foundation) and Ipsen Australia for additional funding support towards my PhD
research. To all the staff at NeuroEndocrine Cancer Australia, your passion for helping
people living with NETs is inspirational. Special thanks to Simone Leyden and Kate
Wakelin who have consistently supported my research and continued to raise
awareness of nutrition needs among people with NETs.
Steve Jobs once said, ‘The only way to do great work is to love what you do’, which is
how I have felt throughout my PhD. I have learnt so much about the experiences of
patients with NETs and have enjoyed telling their story through my research. As a
researcher and a clinician this has been invaluable, and I will continue to love working
with and supporting these patients throughout my career. Thank you to all the
patients and health professional participants who invested their time for my research
and brought much enthusiasm to help drive nutrition research for NETs.
Finally, thank you so much to my family, my husband Josh, and my son Hayden. Josh,
thank you for your patience, and for putting up with my PhD talk and late-night work.
Your constant love and support has kept me going right to the end. To Hayden, you are
too young to appreciate what I have been working on, but your birth during my PhD
candidature has provided a positive distraction and kept me grounded.

xi
Table of Contents
Abstract............................................................................................................................. iii
Declaration ........................................................................................................................ v
Preface ............................................................................................................................. vii
Acknowledgements .......................................................................................................... ix
Chapter 1: Introduction and literature review ................................................................. 1
1.1 Thesis overview .................................................................................................. 1
1.2 Comprehensive literature review ...................................................................... 5
1.3 Additional literature ......................................................................................... 18
Chapter 2: Research methodology ................................................................................. 21
2.1 Aims and Objectives ............................................................................................ 21
2.1.1 Thesis aims ................................................................................................ 21
2.1.2 Thesis objectives ....................................................................................... 21
2.2 Methodology .................................................................................................... 23
2.3 Conceptual Framework .................................................................................... 24
2.4 Research design overview ............................................................................... 27
2.4.1 Phase 1: Prospective, embedded longitudinal mixed-methods study ..... 28
2.4.2 Phase 2: Exploratory study with health professionals ............................. 28
2.5 Phase 1: Prospective longitudinal mixed-methods study................................ 29
2.5.1 Recruitment .............................................................................................. 39
2.5.2 Study setting ............................................................................................. 39
2.5.3 Measures and data analysis approaches .................................................. 40
2.5.4 Health related quality of life ..................................................................... 41
2.5.5 Symptoms ................................................................................................. 42
2.5.6 Anxiety and depression ............................................................................ 43
2.5.7 Financial toxicity ....................................................................................... 44
2.5.8 Nutritional status and weight change ...................................................... 44
2.5.9 Nutrient testing ........................................................................................ 45

xii
2.5.10 Dietitian Contact ................................................................................... 46
2.5.11 Dietary habits ........................................................................................ 47
2.5.12 Medication use ..................................................................................... 47
2.5.13 Patient interviews (qualitative) ............................................................ 48
2.5.14 Statistical analysis ................................................................................. 48
Chapter 3: Nutrition-related symptoms and health-related quality of life in people with
NETs ................................................................................................................................ 51
3.1 Introduction ..................................................................................................... 51
3.2 Aims and objectives ......................................................................................... 54
3.2.1 Objectives ................................................................................................. 55
3.4 Results .............................................................................................................. 55
3.4.1 Patients ..................................................................................................... 55
3.4.2 Health-related quality of life .................................................................... 61
3.4.3 Symptom prevalence and severity ........................................................... 65
3.4.4 Anxiety and depression ............................................................................ 66
3.4.5 Financial toxicity ....................................................................................... 68
3.5 Discussion......................................................................................................... 69
3.6 Conclusion ........................................................................................................ 75
Chapter 4: Nutritional status in people with NETs ......................................................... 77
4.1 Introduction ..................................................................................................... 77
4.2 Aims and objectives ......................................................................................... 79
4.2.1 Chapter aim .............................................................................................. 79
4.2.2 Objectives ................................................................................................. 79
4.3 Method ............................................................................................................ 80
4.4 Results ............................................................................................................. 80
4.4.1 Participants ............................................................................................... 80
4.4.2 Nutritional status ...................................................................................... 80
4.4.3 Weight change .......................................................................................... 83
4.4.4 Body composition ..................................................................................... 86
4.4.5 Dietary change .......................................................................................... 88
4.4.6 Vitamin status ........................................................................................... 91

xiii
4.4.7 Medication use ......................................................................................... 92
4.4.8 Dietitian contact ....................................................................................... 93
4.5 Discussion......................................................................................................... 94
4.6 Conclusion ...................................................................................................... 103
Chapter 5: Living with a NET and the impact on nutrition ........................................... 105
5.1 Introduction ................................................................................................... 105
5.2 Aims and objectives ....................................................................................... 106
5.2.1 Aim .......................................................................................................... 106
5.2.2 Objectives ............................................................................................... 106
5.3 Methodology .................................................................................................. 106
5.4 Methods ......................................................................................................... 109
5.4.1 Recruitment and sampling ..................................................................... 109
5.4.2 Interview questions ................................................................................ 110
5.4.3 Thematic content analysis ...................................................................... 111
5.5 Results ............................................................................................................ 112
5.5.1 Patients ................................................................................................... 112
5.5.2 Insights from the baseline interviews .................................................... 113
5.5.3 Uncertainty ............................................................................................. 118
5.5.4 Complexity .............................................................................................. 120
5.5.5 Conflicting advice.................................................................................... 125
5.5.6 Self-management and seeking information ........................................... 127
5.5.7 Six-month interviews .............................................................................. 129
5.6 Discussion....................................................................................................... 132
5.7 Conclusion ...................................................................................................... 134
Chapter 6: Health professional practices in relation to screening and management of
nutritional issues in people with NETs ......................................................................... 137
6.1 Introduction ................................................................................................... 137
6.2 Phase 2 ........................................................................................................... 137
6.2.1 Online structured survey of health professionals .................................. 137
6.2.2 Focus groups ........................................................................................... 137
6.2.3 Prepared manuscripts ............................................................................ 138

xiv
6.2.4 Manuscript 1 ........................................................................................... 138
6.2.5 Manuscript 2 ........................................................................................... 164
Chapter 7: Managing nutritional issues in NETs from a health professional point of view
...................................................................................................................................... 183
7.1 Introduction ................................................................................................... 183
7.2 Aims and Objectives ....................................................................................... 184
7.2.1 Aim .......................................................................................................... 184
7.2.2 Objectives ............................................................................................... 184
7.3 Methodology .................................................................................................. 185
7.3.1 Mixed-methods approach ...................................................................... 185
7.3.2 Participants ............................................................................................. 186
7.3.3 Focus group facilitation .......................................................................... 187
7.3.4 Focus group questions ............................................................................ 187
7.3.5 Data management and Content analysis ............................................... 188
7.4 Results ............................................................................................................ 191
7.4.1 Participant characteristics ...................................................................... 191
7.4.2 Results of initial content analysis ........................................................... 192
7.4.3 Results of latent content analysis ........................................................... 196
7.5 Discussion....................................................................................................... 214
7.6 Conclusion ...................................................................................................... 220
Chapter 8: Conclusions and implications for research and practice ............................ 223
8.1 Summary of research findings ....................................................................... 223
8.1.1 Quality of life and symptoms in GEP NET patients................................. 223
8.1.2 Prevalence of nutritional complications in NET patients ....................... 225
8.1.3 Dietary change and it’s impact on NET patients .................................... 227
8.1.4 NET health professional nutrition-related knowledge and practices .... 228
8.2 Strength and limitations ................................................................................ 230
8.3 Implications for clinical practice .................................................................... 232
8.3.1 Health professional education and nutrition information resources .... 233
8.3.2 Nutrition screening and assessment in patients with GEP NETs............ 235
8.4 Directions for future research ....................................................................... 239

xv
References .................................................................................................................... 243
Appendices ................................................................................................................... 259
Appendix 1: Nutrition in NETs Questionnaire 1.0 .................................................... 261
Appendix 2: HRQoL raw scores and comparisons to general/NET population ........ 269
Appendix 3: Complete results for symptom impact on dietary change .................. 273
Appendix 4: Phase 1 patient interview schedule ..................................................... 275
Appendix 5: Health professional focus group question schedule ............................ 279
Glossary ........................................................................................................................ 283

xvii
List of Tables
Table 2.1 Schedule of data collection variables and measures ..................................... 40
Table 2.2 EORTC QLQ-C30 and GI.NET21 items used for symptom scoring ................. 42
Table 2.3: References ranges for vitamin analysis ......................................................... 46
Table 3.1 Baseline demographics .................................................................................. 58
Table 3.2 Baseline disease characteristics ..................................................................... 59
Table 3.3 Health-related quality of life and symptom scores over-time ...................... 63
Table 3.4 Symptom prevalence and severity over-time................................................ 66
Table 3.5 Paired t-test results for HADS scales.............................................................. 67
Table 3.6 Caseness of anxiety and depression as per HADS scoring ............................. 67
Table 3.7 Caseness of anxiety and depression as per alternative HADS scoring .......... 68
Table 3.8 COST-FACIT scores per percentile.................................................................. 69
Table 4.1 Nutritional characteristics at recruitment ..................................................... 80
Table 4.2 Prevalence of nutritional status at all time-points ........................................ 81
Table 4.3 Prevalence of malnutrition by NET grade ....................................................... 82
Table 4.4 Prevalence of malnutrition by NET site ......................................................... 82
Table 4.5 Weight change over-time for all participants ................................................ 83
Table 4.6 Weight change over-time for participants with complete data .................... 84
Table 4.7 Percent body weight change over-time of participants with weight loss or
gain ................................................................................................................................. 85
Table 4.8 Change in fat-free mass over-time ................................................................ 87
Table 4.9 Median fat-free mass loss over-time .............................................................. 87
Table 4.10 Other foods and drinks reduced/avoided by participants .......................... 89
Table 4.11 Prevalence of vitamin deficiency amongst participants .............................. 92

xviii
Table 5.1 Participant characteristics............................................................................ 112
Table 5.2 Themes identified ........................................................................................ 115
Table 5.3 Reported dietary changes ............................................................................ 122
Table 7.1 Focus group participant characteristics ....................................................... 191
Table 7.2 Results of initial coding per topic area ........................................................ 193
Table 7.3 Latent content analysis and identification of themes ................................. 197

xix
List of Figures
Figure 2.1 Phase 1 embedded mixed methods design................................................... 25
Figure 2.2 Phase 2 embedded mixed methods design................................................... 27
Figure 3.1 Participant recruitment map according to STROBE criteria .......................... 57
Figure 4.1 Meal pattern changes as a result of NET diagnosis ....................................... 89
Figure 4.2 Food and drink reduced as a result of a NET diagnosis ................................. 89
Figure 5.1 Mixed-methods approach to Phase 1 study................................................ 108
Figure 7.1 Focus group content analysis ...................................................................... 190
Figure 8.1 Nutrition Risk Framework ............................................................................ 236

1
Chapter 1: Introduction and literature review
1.1 Thesis overview
This thesis reports on two studies designed to explore the nutritional complications
and quality of life (QOL) of people diagnosed with a neuroendocrine tumour (NET).
NETs, commonly found in the gastrointestinal tract and pancreas, are referred to as
gastroenteropancreatic (GEP) NETs and are the focus of this research. Whilst their
incidence is increasing, GEP NETs are considered a rare disease and often poorly
understood due to their heterogeneous nature, complex presentation and the variety
of symptoms which patients experience. They are commonly underdiagnosed, with
patients often experiencing debilitating symptoms (diarrhoea, abdominal discomfort,
food intolerance, fatigue, flushing) for many years before a diagnosis is confirmed.
Despite their low incidence, the prevalence of GEP NETs is greater than for other
gastrointestinal cancers, and many patients live for several years with prolonged
symptom burden leading to significant functional and emotional impacts on their
quality of life. There is some evidence from small published cross-sectional studies that
malnutrition, vitamin deficiency and dietary change exist among patients with GEP
NETs. The extent of these nutrition-related complications requires further exploration
in regard to prevalence, severity, and their impact on quality of life. Guidance on the
nutritional management of GEP NETs and NETs in general is absent in current
evidence-based clinical practice guidelines, and the practices of health professionals in
regard to nutritional complications of NETs has not been explored. This thesis
therefore aimed to provide a comprehensive description of nutritional complications
experienced by patients with a GEP NET, and to explore health professional knowledge
and management of these nutritional complications. The overall goal of this research is
to contribute evidence towards future interventional nutrition-research and lead to
the development of nutrition management guidelines for NETs.
Research described in this thesis was undertaken in two Phases. Phase 1 explored the
nutritional complications and their impact on the quality of life of patients living with a

2
GEP NET, and Phase 2 explored the knowledge and practices of health professionals in
regard to nutrition. The aims, objectives and methodology of these two phases of
research are described in detail in Chapter 2.
In Phase 1, patients with GEP NETs were recruited to a prospective, longitudinal mixed-
methods study, during which the prevalence and severity of nutritional complications
(weight change, fat-free mass change, dietary change, and vitamin deficiency), receipt
of dietitian intervention, symptoms and health-related quality of life (HRQoL) were
recorded quantitatively over a six-month period. In addition, a purposive sample of
patients also participated in semi-structured interviews to explore their experience of
living with a GEP NET, and its impact on their nutrition and quality of life. An
embedded mixed methods approach was used for Phase 1 to enable a comprehensive
description of nutritional complications via quantitative prevalence data, and
qualitative in-depth exploration of patient experience in regard to nutrition and quality
of life. The mixed-methods approach is discussed in detail within Chapter 2.
Chapters 3 to 5 report results of the Phase 1 prospective, longitudinal mixed-methods
study. Participant demographics, their HRQoL and symptoms are discussed first in
Chapter 3 in order to introduce and describe the population, and their HRQoL status.
Results for nutritional complications are then presented and discussed in Chapter 4,
followed by presentation of qualitative insights from patient interviews in Chapter 5,
providing in-depth insights regarding the impacts of living with a GEP NET on
nutritional complications.
Chapter 3 reported the results for self-reported symptoms and HRQoL among
participants, including anxious and depressive symptomatology, and financial toxicity.
Results showed that anxiety and depression were prevalent among participants (at
least 50%) and remained prevalent across the six-month data collection time period.
Financial toxicity was also an issue for participants but showed some improvement
over-time. Participants reported various symptoms, with fatigue, pain, abdominal
discomfort, bloating and diarrhoea the most common throughout the study period
3
(reported by at least 60% of participants). Social functioning showed the greatest
decline of all HRQoL scales over-time.
Chapter 4 reports the prevalence of nutritional complications among participants in
Phase 1, including weight change, body composition (fat-free mass) change, change in
dietary habits, and presence of vitamin deficiency. Results demonstrated that 17 (29%)
participants were malnourished at recruitment to the study, with nutritional status
improving for some participants over-time. Weight loss was observed in a greater
proportion of participants (44% had weight loss after two-months, 48% had weight
loss after six-months) than malnutrition (29% malnourished at baseline, 13%
malnourished after six-months). Fat-free mass (muscle) loss was observed in some
participants, even those who recorded stable weight or weight gain over the study
time period, indicating underlying body composition change. Over half of participants
reported changing their diet as a result of their NET diagnosis. There was considerable
variation in the kinds of dietary change reported, with food avoidance and smaller
meals being among the most common changes. The proportion of participants who
had contact with a dietitian over the study period (15-22%) was lower than the
proportion who experienced weight loss, malnutrition, dietary change.
Chapter 5 describes the aims, methodology and results of semi-structured interviews
completed with a purposive sample of participants enrolled in the Phase 1 study.
Results of these interviews provide in-depth exploration of patient experience with
regard to the nutritional complication and quality of life impacts of living with a GEP
NET, adding richness and depth of insight to data reported in Chapters 3 and 4. Insights
from the interviews describe how people experience and try to adjust to the complex
and uncertain context of their NET diagnosis, prognosis and ongoing treatment.
Interview participants reported making dietary changes mostly in an attempt to
manage their symptoms which were impacting heavily on their HRQoL. People talked
about self-imposed dietary restrictions and difficulty in accessing expert and tailored
information about their NET, diet and nutrition. Participants described nutrition and
symptom-control as a priority for them. They spoke about frequently seeking advice

4
and guidance on appropriate diets from other people living with a NET and internet
resources, rather than through health professionals. Results from this chapter provide
important context to the experiences and dietary changes of patients with a GEP NET,
which provide important patient-centred data to inform future nutrition interventions
in combination with data presented in Chapters 3 and 4.
Phase 2 of this research, which explored the knowledge and practices of health
professionals in regard to the nutritional complications of NETs, is described in
Chapters 6 and 7. Phase 2 also used an embedded mixed-methods approach.
Quantitative data were collected via a structured survey, providing a current
description of international health professional nutrition-related practices. Qualitative
data were collected via focus groups undertaken in Victoria, Australia to gather in-
depth information regarding the experience of, rationale for, and barriers to health
professional nutrition-related practices.
Chapter 6 reports results of the structured survey distributed internationally to
multidisciplinary NET health professionals (doctors, nurses, dietitians). The survey data
provide a current description of health professional knowledge and experience in
regard to nutrition-related symptoms and complications among patients with a NET.
Results showed that 28 (38%) health professionals who took part in the survey
reported screening for malnutrition or vitamin deficiency when consulting with
patients. Provision of nutrition advice to patients varied and lack of NET-specific
nutrition guidelines was highlighted as a barrier to provision of NET-specific nutrition
advice and routine nutrition screening practices.
Chapter 7 describes results of health professional focus groups, completed with
clinicians working in the NET unit at one of the research study sites in Victoria,
Australia. Questions proposed to participants during the focus groups aligned with
questions included in the structured survey, so as to explore these concepts in more
detail. During the focus groups, health professionals described malnutrition, weight
loss and vitamin deficiency as being present among patients with a NET, but these

5
were considered less of an issue than for other gastrointestinal cancers. Malnutrition
and vitamin screening were not conducted systematically, although health
professionals felt that further work needed to be done to improve nutrition screening
practices, and to develop evidence to guide practice. Health professionals reported
observing the presence of dietary change and restriction among the people they cared
for with a NET, which aligned with results in Phase 1. Results from both Chapters 6 and
7 contribute a summary of current nutrition practices among NET health professionals
and provide evidence to inform the development of health professional education
strategies and NET-specific nutrition guidelines.
Chapter 8 (final chapter) presents a summary of the main findings from the body of
work undertaken for this PhD study. Within this chapter there is a detailed discussion
of research strengths and limitations, implications for clinical practice and directions
for future research.
1.2 Comprehensive literature review
A comprehensive literature review was conducted at the commencement of this PhD
to evaluate the current state of evidence for nutritional complications in patients
diagnosed with a NET. Upon initial review of the literature various nutrition issues
were identified, but there was insufficient volume and quality of evidence available to
contribute to a systematic literature review. Therefore, a narrative review was
conducted. The literature review was accepted for publication in Neuroendocrinology
in 2019 (Neuroendocrinology 2020;110(5):430-441, DOI: 10.1159/000507500 (Laing et
al., 2020). A copy of the publication is attached below. The literature review provided a
comprehensive description of current literature investigating nutritional complications
in patients diagnosed with a NET and contributed to the evidence guiding the
methodology of this thesis.
A literature search was also conducted to evaluate the availability of published
literature examining health professional knowledge and practices in regard to
nutrition, however no relevant literature was found.

6

7

8

9

10

11

12

13

14

15

16

17

18
1.3 Additional literature
The original literature search strategy undertaken in February 2019 was repeated in
June 2020 to obtain any additional relevant literature in preparation for completing
the final thesis. A further two review articles were found. Clement et al. (World Journal
of Gastroenterology, 2019) published a review article summarising literature and
evidence for nutritional and vitamin status in patients with NETs (D. Clement et al.,
2019). Poblicki et al. (Nutrients, 2020) published a review article summarising
literature on nutrition and the role of biogenic amines in the treatment of patients
with NETs (Pobłocki et al., 2020).
When searching for observational or interventional research relating to nutrition, only
one additional publication was found. Kikut et al. (2020) published an observational
study examining the nutritional intake of 26 patients with GEP NETs, in comparison
with 20 healthy controls (Kikut et al., 2020). A 24-hour dietary consumption
assessment was completed with participants by a dietitian to determine nutrient
intake and dietary adequacy as per the healthy diet indicator (HDI), diet quality index
(DQI) and national estimated average requirements (EAR) for healthy adults. In
comparison to the diet of the control group, reduced intake of energy, fat and animal
proteins, and increased intake of fibre and fish, was observed in the GEP NET group
(Kikut et al., 2020). Inadequate intakes for some vitamins and minerals (vitamin D,
folate, niacin, calcium, magnesium, potassium) was also observed (Kikut et al., 2020).
Limitations of this study included a small sample size and mostly limited quantitative
assessment of dietary intake, which limited exploration of reasons for dietary change
and the impact of this change on patients’ quality of life and nutritional status overall,
i.e. malnutrition risk. The comparison of dietary intake to national estimated average
dietary requirements may not be appropriate. Patients in the study by Kikut were
undergoing active NET treatment with somatostatin analogue therapy, and 61% had
undergone prior surgery, therefore likely to have had altered nutrient requirements.
The symptomatology of patients was not recorded, and therefore the relationship
between dietary intake or change and symptoms, was not explored. Body mass (kg)

19
and history of weight loss since GEP NET diagnosis was recorded at the
commencement of the study, but nutritional status was not assessed. At time of
recruitment, female participants had averaged 8.4kg loss of weight, and male
participants had averaged 9.5kg loss of weight since diagnosis (over 4 years on
average), which provides descriptive data regarding the potential presence of weight
loss in GEP NEN patients not previously explored in other studies (Kikut et al., 2020).
As discussed in the published literature review (Laing et al., 2020), the occurrence of
nutritional complications in GEP NETs such as malnutrition, vitamin deficiency and
dietary change has been identified only in a limited number of published studies.
Larger studies providing prospective longitudinal data on the prevalence of nutritional
complications, their impact on patients’ quality of life, and guidance for optimal
nutrition screening tools in NETs is required. Generation of this evidence will
contribute to future NET-specific nutrition guideline development.


21
Chapter 2: Research methodology
As introduced in Chapter 1, this thesis aimed to provide a comprehensive description
of the nutritional complications experienced by patients living with a GEP NET, and a
summary of the management of nutritional complications as described by NET health
professionals. The research described in this thesis used a mixed-method study
approach to explore in depth the nutritional complications experienced by patients
diagnosed with GEP NET. This included gathering quantitative description of the
prevalence of complications and undertaking qualitative exploration of patients and
health professionals’ experiences of living with and managing nutritional impacts of
GEP NETs.
This chapter sets out to describe the research design of this thesis, detail the aims and
objectives of the research, and justify the methods used across the mixed methods
studies undertaken in each phase of the research.
2.1 Aims and Objectives
2.1.1 Thesis aims
1. To describe the impact of GEP NETs and their treatment on patients’ nutritional
status and HRQoL.
2. To generate evidence to inform a future program of research, including the
development and implementation of evidence-informed, early nutritional
screening to guide tailored nutrition information for patients with GEP NETs
2.1.2 Thesis objectives
Objective 1
To determine the point prevalence, severity, and patient experience of nutritional
complications and HRQoL amongst patients with GEP NETs, including:

22
a. The prevalence of objectively assessed malnutrition in patients with GEP
NETs.
b. The prevalence and severity of symptoms as reported by patients with GEP
NETs.
c. To determine the prevalence of objectively measured vitamin deficiencies in
patients with GEP NETs.
d. To explore and describe patients’ experiences of a diagnosis and treatment
for GEP NETs on their nutrition and dietary habits.
e. To explore and describe patients experience of a diagnosis and treatment for
GEP NET, between baseline and six-months, on patient-reported HRQoL
including day-to-day life, function, social activities and emotional wellbeing.
Secondary objective:
a. If appropriate, to examine differences in nutritional outcomes (e.g. nutritional
status) between subgroups of patients with a GEP NET, defined by disease and
treatment related characteristics.
Objective 2
To describe health professional’s current knowledge and management of nutritional
complications in patients with GEP NETs and summarise current international practice:
a. To describe current knowledge of nutritional complications amongst health
professionals working with NET patients.
b. To describe current nutrition management practices amongst health
professionals working with NET patients.
23
c. To summarise current international practice relating to nutritional screening
and management of NET patients.
Secondary objectives
a. To describe similarities and differences in practice amongst health
professionals working with patients diagnosed with a NET in regard to
screening and management of nutrition issues.
b. To explore whether there is a difference between reported nutrition issues
amongst patients with GEP NETs and the perception of nutrition issues
amongst health professionals caring for them.
The study was designed in two phases, with Phase 1 focusing on exploration of the
nutritional complications experienced by patients diagnosed with a GEP NET, and
Phase 2 exploring the knowledge and management of nutritional complications by NET
health professionals.
2.2 Methodology
As a dietitian working in the Upper gastrointestinal and NET Unit, it was observed that
unlike other gastrointestinal cancers (e.g. gastric, oesophageal and pancreatic
adenocarcinoma), where rates of malnutrition and nutrition-related treatment
complications are well known and documented, there is limited evidence for the
nutritional management of GEP NETs and nutritional guidelines specific to GEP NETs.
Therefore, I identified the importance of and a need to explore the nutritional
complications of NET through research, in order to contribute evidence to guide and
optimise health professional practice. It was evident through my clinical practice that
the experiences and clinical presentation of GEP NET patients varied greatly,
particularly in regard to their nutrition issues, and therefore a research approach that
enabled data to be collected that addressed the heterogeneity of experience, clinical
presentation and impact was important.

24
2.3 Conceptual Framework
In terms of GEP NET management and research, this study set out to explore an area
of practice and patient experience about which little is known (Miller and Crabtree,
2005), and to better understand an event (the nutritional and HRQoL impacts of a GEP
NET) from diverse conceptual positions or frameworks, that is, constructivist and
positivist paradigms (or frameworks). In order to address the study aims, data that
related to an individuals’ subjective experience of an event (in this case patients’
experiences of their GEP NETs - constructivism) and clinical and quantifiable data that
relate to an objective reality (for example, weight loss - positivism) were necessary. A
mixed methods approach was therefore chosen to enable depth and breadth of
perspective through data collection, with qualitative approaches guided by the
quantitative data collected (Mark, 2015). A mixed methods approach enabled in-depth
exploration of nutritional issues and patients and health professionals’ experiences of
GEP NETs, in a way that would not have been possible through a quantitative approach
alone (Mark, 2015). Identifying and describing the prevalence of nutritional
complications was important, but the impact of nutritional complications on patients
themselves was considered essential data to guide patient-centred clinical practice.
This research therefore used an embedded mixed methods approach. An embedded
design is appropriate when one data type provides a secondary and supportive role to
the primary data set (Creswell, 2007; Creswell and Plano Clark, 2011). In both phases
of research, the primary data sets were quantitative, with the qualitative data sets
providing additional in-depth information not possible to explore through quantitative
methods alone. In Phase 1, quantitative data were collected via a prospective
longitudinal observational study, providing description of the prevalence and severity
of nutritional complications over-time, among patients diagnosed with a GEP NET.
Qualitative data collected for Phase 1 allowed in-depth exploration of patient
experience with regard to precursors to and impacts of nutritional complications on
their lives (Figure 2.1).

25
Figure 2.1 Phase 1 embedded mixed methods design
The purpose of this research was to provide a comprehensive description of the
nutritional complications and HRQoL impacts among patients with a GEP NET, by
exploring prevalence of nutritional complications among patients (Phase 1), and
exploring health professionals’ knowledge and practice in regard to nutritional
complications (Phase 2). Data were also gathered to contribute evidence towards a
framework to guide future interventional research. Through a comprehensive review
of nutrition-related literature in NETs (reported in Chapter 1, Section 1.2), potential
nutritional complications in NETs were identified and contributed to the design of this
research. Data were captured from health professionals in addition to patients due to
the absence of clinical practice guidelines and documented consensus for the
nutritional management of patients living with NETs. This PhD will be the first
(published) study to include exploration of health professional knowledge and
management of nutritional complications among patients with NET.
Nutrition-related complications identified in the comprehensive literature review
(described in Chapter 1, Section 1.2) included malnutrition, risk and presence of

26
vitamin deficiency, dietary change and food intolerances. The impact of NETs on
patients’ HRQoL and potential nutrition-related symptoms were also identified during
the review. These insights informed the research approach and data collection
methods for Phase 1. In order to perform a comprehensive exploration of nutritional
complications, all potential nutritional complications identified in existing literature;
including malnutrition, vitamin deficiency, and dietary change were included in the
methodology, and explored in this research. HRQoL data, including symptoms,
financial toxicity and presence of anxiety and depression were also explored to provide
in-depth description of domains of life impacted by a diagnosis of GEP NET and its
nutritional impacts, and if possible, to explore relationships between HRQoL domains
and GEP-NET associated nutrition changes.
For the Phase 2, mixed methods study, quantitative data were collected via an online
structured survey of health professionals. The survey introduced questions addressing
themes of symptom prevalence and impact, screening and management of
malnutrition and vitamin deficiencies, provision of nutrition advice and use of
nutrition-related evidence-based guidelines. Questions included in the survey were
informed by international evidence and data generated in Phase 1. An overall
description of the nutritional practices of international NET health professionals was
generated through quantitative analysis. In-depth information on the rationale for
nutrition-related health professional practices and gaps to current knowledge and
guidelines was obtained through qualitative focus groups undertaken with a purposive
sample of NET health professionals (Figure 2.2). The qualitative data obtained from
focus groups in Phase 2 provided a more in-depth context and rationale for responses
to the structured survey, and both data sets were used to guide future research and to
identify opportunity to advance practice.

27
Figure 2.2 Phase 2 embedded mixed methods design
2.4 Research design overview
In keeping with the intent of the work, a prospective, descriptive observational design
was chosen within which the mixed methods studies were undertaken. Descriptive,
observational designs allow for observation and description of a naturally occurring
(that is uncontrolled) event or events in order to identify patterns, similarities or
differences among a cohort of people (Mann, 2003; Caruana et al., 2015).
A prospective longitudinal design was chosen to enable observation of the occurrence
and prevalence of nutritional complications over-time, given the prolonged disease
course for the majority of these patients. Current published literature provides cross-
sectional prevalence data for nutritional complications but does not explore the timing
of these complications or any improvement or worsening over-time during NET
treatment. A prospective, longitudinal design allowed comprehensive description of
nutritional complications occurring over the course of a patient’s medical management
and treatment.

28
2.4.1 Phase 1: Prospective, embedded longitudinal mixed-methods study
In Phase 1, a prospective, embedded longitudinal mixed-methods study was conducted
at two hospital sites in metropolitan Melbourne, Australia; Peter MacCallum Cancer
Centre and Austin Hospital. Participants were involved in a six-month data collection
period, with bi-monthly data collection points (Recruitment, T0; two-months, T2; four-
months, T4; six-months, T6). Quantitative data were collected to describe the
prevalence of nutritional complications including malnutrition, weight loss and dietary
change. A purposive sample of participants completed qualitative interviews at T0 and
T6 to explore in-depth the occurrence and experiences of nutritional complications
and their impact on HRQoL.
2.4.2 Phase 2: Exploratory study with health professionals
Health professionals working with patients living with a NET took part in an exploratory
embedded mixed methods study to describe their perceptions of nutrition issues
amongst patients with NETs, and to describe current nutrition screening and
management practices.
Online structured survey of health professionals
Information was collected from an international group of health professionals working
with patients living with a NET, using a structured online survey. Questions addressed
the following topics: health professional knowledge and experience in regard to
nutritional complications, nutrition screening and management practices and use and
availability of evidence-based guidelines.
Health professional focus groups
Focus groups were conducted face to face with Australian health professionals from
the participating recruitment sites. Focus group discussions were guided using semi-

29
structured interview schedules, with questions aligned with responses from the survey
to allow a more in-depth discussion of key topic areas.
Design and methodology of Phase 2
Detail and discussion of the design and methodology relating to Phase 2 research, is
discussed in Chapter 6 and Chapter 7, in addition to consideration of the results of
these studies.
The following section will focus on describing Phase 1 research methodology as an
introduction to Phase 1 results that are discussed in Chapter 3 and Chapter 4.
2.5 Phase 1: Prospective longitudinal mixed-methods study
Details of the recruitment approach and research methods for the first phase of the
study were published as a protocol in the Journal of Medical Internet Research (JMIR)
Research Protocols (JMIR Res Prot 2018; 7(12), DOI: 10.2196/11228) (Laing et al.,
2018).

30

31

32

33

34

35

36

37

38
39
The following sections describe additional details regarding the methodology from
Phase 1 that was not included in the published protocol due to space limitations.
2.5.1 Recruitment
The recruitment approach in Phase 1 aimed to ensure that the study sample was
representative of a heterogeneous GEP NET population. Whilst potential nutritional
complications relevant to this population of patients were identified through the
literature review, there was inadequate evidence to define a sub-group appropriate to
address the goals of this study, that is to generate a comprehensive description of
nutritional complications amongst patients with a GEP NET. As such, a heterogeneous
sample of patients with a GEP NET was sought. Heterogeneity was achieved by
recruiting all eligible patients with confirmed diagnosed of GEP NET upon their initial
referral to the study sites. Recruitment occurred over a 12-month period from June
2017 – June 2018.
2.5.2 Study setting
One of the study sites, the Peter MacCallum Cancer Centre, is a tertiary referral
hospital for people with NETs and an accredited European Neuroendocrine Tumor
Society (ENETS) Centre of Excellence with a dedicated multidisciplinary NET unit and
relevant clinics. The other study site, Austin Hospital, is a tertiary referral hospital for
NETs where NET patients are managed within the multidisciplinary Upper
Gastrointestinal Unit and clinic.
A six-month data collection period with bi-monthly data collection points (baseline –
T0, two-months – T2, four-months – T4, six-months -T6), was chosen to allow for
longitudinal data collection and observation of patient outcomes over-time. This was
to ensure data collection could be completed within a reasonable time frame, thus
allowing for data analysis and results write-up within the three-year period of a PhD
degree. Where possible, data collection was aligned with patient’s existing
appointments to reduce travel burden to address study data completion requirements.

40
To facilitate this, a decision was made that a patient was able to complete data
collection if they were attending the study site within two weeks of their scheduled
data collection point at T2 and T4, or within one month of their scheduled data
collection point at T6. If a patient was not attending the study site at the scheduled
time of data collection, their data was marked as missing for that time-point, and they
remained enrolled in the study. Missing data were accounted for during statistical
analysis (refer to Section 2.5.13).
2.5.3 Measures and data analysis approaches
A schedule of data collection variables and measures for the Phase 1 study is included
as an online appendix in the published protocol and is attached below in Table 2.1.
Table 2.1 Schedule of data collection variables and measures
Data Measure
Time after initial appointment at recruitment site (months)
0 1 2 3 4 5 6
HRQoL EORTC QLQ C-30 X* X* EORTC QLQ GI.NET21 X* X* COST-FACIT X X HADS X X
Symptoms EORTC QLQ C-30 X* X X X* EORTC QLQ GI.NET21 X* X X X*
Vitamins Niacina X X Vitamin Db X X Vitamin Eb X X Vitamin Ab X X Vitamin B12b X X Folateb X X Iron studiesb X X
Nutritional status PG-SGA (Malnutrition) X X X X BIA (FFM) X X X X Weight X X X X Height X BMI X X X X
Dietitian contact Questionnaire 1.0 Section 1
X X X X
Dietary habitsc Questionnaire 1.0 Section 2
X X X X
41
Data Measure
Time after initial appointment at recruitment site (months)
0 1 2 3 4 5 6
Medicationc Questionnaire 2.0 X X X X
Interview X X
Notes.
a. 24 hr urine sample, b. Blood sample, c. Data collected from medical record
*EORTC questionnaires only completed once at each time point in order to record information for both HRQoL and symptoms
BIA, bioelectrical impedance analysis; FFM, fat-free mass; BMI, body mass index
2.5.4 Health related quality of life
Participants completed the European Organisation for Research and Treatment of
Cancer (EORTC) QLQ-C30 questionnaire and EORTC GI.NET21 module to record HRQoL
and symptom prevalence and severity (Table 2.2). As discussed in the published
protocol, the EORTC-QLQ C30 and EORTC GI.NET21 modules were chosen because
they are tools validated for assessing HRQoL and symptoms in patients with GEP NETs
(Yadegarfar et al., 2013), and enabled identification of all potential symptoms that a
patient with a GEP NET may experience, as per the previous literature review (Chapter
1).
EORTC QLQ-C30 scores for the global health status scale and four of the functional
scales (physical, role, emotional and social), and EORTC GI.NET21 scores for the social
function scale and disease related worries scale, were analysed to assess HRQoL at
recruitment (T0) and six-months (T6). Scores for each scale/item were converted to a
score of 0-100 as per the EORTC scoring manual (Aaronson et al., 1993). A high score
for a functional scale represents a high or healthy level of functioning, and a high score
for the global health status scale represents a high quality of life. The size of observed
differences (small, medium, large), considered a clinically meaningful change in scores,
was calculated using guidance from Kazis et al. (1989) and Cohen’s d effect sizes
(Cohen, 1988; Kazis, Anderson and Meenan, 1989).

42
2.5.5 Symptoms
Symptom severity was recorded using the three symptom scales (fatigue, pain, nausea
and vomiting) and four of the single symptom items (dyspnoea, loss of appetite,
constipation, diarrhoea) of the EORTC QLQ-C30; and three of the symptom scales
(endocrine function, GI symptoms, and treatment-related symptoms) of the GI.NET21.
Prevalence of a symptom to any degree and the prevalence of high-intensity
symptoms was calculated using scores of single items relating to particular symptoms
(Table 2.2). Table 2.2 demonstrates the symptoms included in the analysis and the
single question items of the EORTC QLQ-C30 and EORTC QLQ GI.NET21 that were used
for scoring prevalence for each symptom. A symptom was classified as present if a
participant selected ‘2- somewhat’, ‘3-quite a bit’ or ‘4-very much’. If a score of 3
(‘quite a bit’) or 4 (‘very much’) was selected for the item, the symptom was classified
as being high-intensity.
Table 2.2 EORTC QLQ-C30 and GI.NET21 items used for symptom scoring
Question Related symptom
EORTC QLQ-C30
Q8. Were you short of breath? Short of breath - Dyspnoea
Q9. Have you had pain? Pain
Q13. Have you lacked appetite? Loss of appetite
Q14. Have you felt nauseated? Nausea
Q15. Have you vomited? Vomiting
Q16. Have you been constipated? Constipation
Q17. Have you had diarrhoea? Diarrhoea
Q18. Were you tired? Fatigue
EORTC QlQ-GI.NET21

43
Question Related symptom
Q31. Did you have hot flushes? Hot flushes
Q33. Did you have night sweats? Night sweats
Q34. Did you have abdominal discomfort? Abdominal discomfort
Q35. Did you have a bloated feeling in your abdomen? Bloating
Q36. Did you have a problem with passing wind/gas/flatulence?
Wind/gas
Q37. Did you have acid indigestion or heartburn? Indigestion/heartburn
Q45. Has weight loss been a problem for you? Weight loss
Q46. Has weight gain been a problem for you? Weight gain
2.5.6 Anxiety and depression
The presence of anxiety and/or depression were recorded using the Hospital Anxiety
and Depression Scale as described in the protocol (Section 2.5). Scores for anxiety
(HADS-A) and depression (HADS-D) were calculated and compared against criteria for
the presence of anxiety and depression (score of 8-10), and the probable presence of a
disorder (score 11 and above) (Zigmond and Snaith, 1983; Snaith, 2003). Recent
literature has suggested that thresholds for caseness of anxiety and depression should
be lower when using the HADS in cancer patients in order to detect a high proportion
of possible cases (Morse, Kendell and Barton, 2005; Singer et al., 2009). The HADS is
validated for use in cancer populations and considered a reliable tool to assess the
presence of anxiety and depression cases (Morse, Kendell and Barton, 2005; Singer et
al., 2009; Martinez et al., 2012). However, the original validation of the HADS was
performed in a primary care setting, not an acute oncology setting, and has been
shown to underestimate the caseness of depression and anxiety of cancer patients
(Morse, Kendell and Barton, 2005). Cancer patients undergoing treatment are at a
high-risk of mental health issues including depression and distress, which are often
under-diagnosed (Morse, Kendell and Barton, 2005). Studies have examined the

44
clinical relevance of HADS scoring in various cancer populations and found that to
ensure identification of all potential cases of anxiety and depression in cancer patients,
the score threshold should be lowered (Morse, Kendell and Barton, 2005; Singer et al.,
2009; Martinez et al., 2012). Therefore, given that the patients who took part in this
study were mostly undergoing active cancer treatment, with demonstrated symptom
burden and reduced quality of life, revised scoring with a lower threshold for anxiety
and depression caseness was considered appropriate and applied to results. For HADS-
A and HADS-D the recommended cut-off score for caseness in cancer patients is >6,
and for HADS-T (total score) is >13 (Morse, Kendell and Barton, 2005; Singer et al.,
2009; Martinez et al., 2012).
2.5.7 Financial toxicity
Financial burden experienced by participants during the study period was measured
using the Comprehensive Score for Financial Toxicity Functional Assessment of Chronic
Illness Therapy (COST-FACIT) (Version 1), which is a validated patient-reported
outcome measure in cancer patients (de Souza et al., 2014, 2017). The COST-FACIT
contains 11-items and is scored using a 5-point Likert scale. The total score can range
between 0 to 44, and the higher the total score the better the financial well-being.
Participant scores for the COST-FACIT were also categorised into percentiles (0-15, 16-
30, 31-44) to enable description of the spread of results.
2.5.8 Nutritional status and weight change
The validated PG-SGA was used to measure nutritional status and the presence of
malnutrition, as discussed in the published protocol (Section 2.5) (Ottery, 1996; Bauer,
Capra and Ferguson, 2002). The PG-SGA tool was developed as a standardised
assessment of malnutrition for patients with cancer and other chronic catabolic
conditions (Ottery, 1996). It incorporates assessments of weight change, food intake,
symptoms impacting food intake, and functional status, to be completed by the
patient; and disease state, metabolic state and the physical examination of muscle and
fat stores, as assessed by the health professional (Ottery, 1996).

45
Body weight was determined using a digital scale (Tanita inc., Tokyo, Japan, model T1
SC 330S), which was calibrated prior to the commencement of the study. Participants
were weighed clothed, without shoes, and weight was measured to the nearest 0.1kg.
Percentage weight change (loss or gain) between baseline and each time-point (two-
months (T0), four-months (T4) and six-months (T6)) was calculated for each participant
and the proportion of participants that experienced weight change or weight stability
during the study period was subsequently calculated. Weight stable over the study
period was classified as a weight loss or gain of less than 0.8 percent body weight
(Rosenbaum, Wang and Kotler, 2000). At time of body weight measurement, the
participant was asked whether any weight change recorded was intentional, or
unintentional.
2.5.9 Nutrient testing
Niacin status was evaluated by measuring the 24-hour output of urinary niacin
metabolite N1-methylnicotinamide (NMN) and N1-methyl-2-pyridone-5-carboxylamide
(MCP) and analysis by HPLC-Flourescence (Delange and Joubert, 1964; NHMRC, 2006).
Serum levels of vitamin B12, folate, iron, vitamin D, vitamin E and vitamin A were
analysed using blood samples collected from participants. Vitamin B12, folate and
vitamin D analysis was performed using Chemiluminescent Immunoassay. Serum iron
studies were analysed using the Ferrozine Reaction method. Vitamin E and A analysis
was performed by a HPLC-UV assay. Iron, Folate, vitamin B12 and vitamin D were
analysed through the Peter MacCallum Cancer Centre Pathology Department
(Melbourne, Australia). Niacin, vitamin A and vitamin E were transported on ice to
Sydney South West Pathology Service (Sydney, Australia) for analysis, as this was the
only centre accredited to perform these analyses. If a measured level of a vitamin was
below the defined optimal reference range (Table 2.3) it was classified as deficient.

46
Table 2.3 References ranges for vitamin analysis
Vitamin Reference range Source
Niacin (B3) MCP: 25 – 110 μmol/day
NMN: 10-75 μmol/day
MCP:NMN Ratio: 1.3 – 4,
<1.0 considered latent niacin deficiency
(Delange and Joubert, 1964; NHMRC, 2006)
Vitamin B12 150 -750pmol/L Peter Mac Pathology
Folate 12-31nmol/L Peter Mac Pathology
Iron Ferritin:
(Male 25 – 400 ug/L, Female 20 – 300 ug/L)
Iron: 10 – 30 umol/L
Transferrin: <60yo 1.8 – 3.2 g/L, >60yo 1.5 – 3.2 g/L
Transferrin Saturation: 15 – 50%
Peter Mac Pathology
Vitamin D Optimal level: >50 nmol/L
Mild deficiency: 25 – 50 nmol/L
Moderate deficiency: 12.5 – 25 nmol/L
Severe deficiency: <12.5 nmol/L
(Diamond et al., 2005; NHMRC, 2014)
Vitamin E 8 – 30 μmol/L Peter Mac Pathology
Vitamin A 1.4-4.0 μmol/L Peter Mac Pathology
2.5.10 Dietitian Contact
Dietitian contact was recorded using a 5-item questionnaire designed specifically for
the study, and from information in the medical records where available. The
questionnaire required participants to report if they had contact with a dietitian in the
month prior to data collection at T0, T2, T4 and T6. The location of dietitian contact,

47
source of referral and reason for contact were recorded using the questionnaire,
attached in Appendix 1. For questions where participants were able to select multiple
answers (Question 5), this was indicated in the title of the question and verbally
discussed with the participant by the researcher.
2.5.11 Dietary habits
A 5-item questionnaire designed specifically for this study was used to record changes
to participant dietary habits as a result of their NET diagnosis or treatment. Design of
the questionnaire was informed by the comprehensive literature review discussed in
Chapter 1. Validated food frequency questionnaires are available for use with cancer
patients, but most include more than 70-items, but the burden of completion was
deemed greater than the potential gain of information. Before recruitment, three NET
patient advocates from the NeuroEndocrine Cancer Australia (formerly the Unicorn
Foundation) Consumer Advisory Group completed the 5-item questionnaire to
determine its readability and completion time. Only minor changes to wording of the
questionnaire were required after this testing. The final dietary questionnaire is
attached in Appendix 1. Questions where participants were able to select multiple
answers (Questions 2-5) had this either indicated in the title of the question or were
indicated verbally to participants by the researcher.
2.5.12 Medication use
Participants were asked to report all current medication use in consultation with the
researcher at each data collection time-point. Only the medications considered
relevant to nutrition and the treatment of nutrition-related symptoms (vitamin
supplements, herbal or complimentary medicines including probiotics, pancreatic
enzymes, anti-diarrhoeal, anti-emetics) were reported in the study results. Some
participants reported use of a multivitamin which is defined as a supplement
containing a combination of multiple vitamins and minerals.

48
2.5.13 Patient interviews (qualitative)
The research design and methodology of patient interviews conducted as the
qualitative arm of the Phase 1 research study will be discussed in detail in Chapter 5,
along with results.
2.5.14 Statistical analysis
Additional detail of statistical analysis methods after publication of the protocol paper
are described as below.
Responses to patient-reported outcome measures were scored according to author
guidelines. Where relevant, recodes were applied as described above. Descriptive
statistics were used to summarise patient demographic and clinical characteristics, and
responses to patient-reported outcomes measures (EORTC QLQ-C30, EORTC QLQ-
GI.NET21, COST-FACIT and HADS) at each assessment. These included counts and
percentages for nominal valued variables; and means and standard deviations or
medians and interquartile ranges, as appropriate, for continuous valued variables.
Analysis of outcomes assessed by the EORTC measures was carried out by a fitting
linear mixed model to each outcome separately using the ‘lme4’ package. Models
included a fixed effect for time, as well as a random participant effect; an unstructured
covariance structure was used to guard against model misspecification. All models
were estimated via maximum likelihood. Differences between baseline and T6
assessments were estimated with 95% confidence intervals. Effect size estimates, as
described by Kazis and colleagues (Kazis, Anderson and Meenan, 1989), were used to
characterise the size of observed differences. These are interpreted as per Cohen’s d,
with 0.2, 0.5 and 0.8, reflecting small, medium and large-sized differences, respectively
(Cohen, 1988).
McNemar’s test was used to assess differences between proportions of participants
who were malnourished at follow-up assessments compared with baseline. Confidence

49
intervals (95%) were calculated using the method described by Carlin and Doyle (Carlin
and Doyle, 2001).
Due to sample size limitations statistical sub-analysis of the difference in nutritional
outcomes (malnutrition status) between sub-groups defined by disease- and
treatment-related characteristics was not performed. Instead, crosstabulations were
used to generate the joint frequency distributions of patients based on nutritional
status and disease and treatment characteristics (NET site, NET grade).
Scoring and descriptive analysis was performed in SPSS Version 25 (Chicago, IL, USA).
Mixed model analysis was performed in R Version 3.6.1, using the ‘lme4’ and ‘lsmeans’
packages. Kazis effect sizes were calculated manually in Excel.


51
Chapter 3: Nutrition-related symptoms and health-related
quality of life in people with NETs
This chapter describes results from the Phase 1 longitudinal mixed-methods study of
patients with GEP NETs, and focuses on nutrition-related symptoms and HRQoL, as
described by patients who took part in the study.
The chapter includes details of participant demographics, clinical characteristics,
symptomatology and HRQoL. It begins with an overview of published literature
relevant to these findings. Nutritional outcomes from the Phase 1 study are discussed
in Chapter 4.
3.1 Introduction
Patients with GEP NETs can experience numerous and complex symptoms relating to
the presence of their disease or various treatment modalities (Burgess, 2005; Kaupp-
roberts, Srirajaskanthan and Ramage, 2015). Up to 30 percent of patients with GEP
NETs have carcinoid syndrome, whereby their tumours secrete endogenous amine
hormones, in particular serotonin, which can give rise to symptoms including flushing,
fatigue, severe diarrhoea, food intolerance, restlessness and fluctuations in mood and
pain (Haugland et al., 2013; Kaupp-roberts, Srirajaskanthan and Ramage, 2015). NET
related symptoms may persist for long periods (median 9.2 years) prior to diagnosis,
and have the potential to place substantial HRQoL burden on the patient and health
service utilisation impact on the health care system (Vinik et al., 2010; Kaupp-roberts,
Srirajaskanthan and Ramage, 2015; Singh et al., 2017). Although potential side-effects
of the disease and its treatment have been documented (Kaupp-roberts,
Srirajaskanthan and Ramage, 2015), there is limited published information on the
incidence and prevalence of symptoms and description of their impact on patients
themselves, particularly in an Australian population. The specific impact on nutritional
status is also still largely unknown
52
Presenting symptoms from a NET can be a result of the mass tumour effect, such as
bowel obstruction, pain, bleeding and jaundice; generalized symptoms of cancer
presence, such as fatigue, low appetite, cachexia and loss of weight; or hormonal
effects, such as flushing, diarrhoea, reflux, gastric ulceration, bowel ischemia, glucose
intolerance and hypoglycaemia (Burgess, 2008). In people with NETs symptoms are
generally related to the secretion of hormones (Pearman et al., 2016).
Many of the symptoms experienced by people with NETs can potentially affect
nutritional intake and nutritional requirements. For example, altered glucose
metabolism has implications for carbohydrate requirement and intake (Sheard et al.,
2004). Symptoms such as abdominal pain and loss of appetite can cause patients to
alter their dietary intake, putting them at risk of weight loss and malnutrition (Borre et
al., 2018). Diarrhoea can be associated with nutrient malabsorption, electrolyte
disturbance and dehydration, particularly if steatorrhea is present (Van Der Horst-
Schrivers et al., 2004). The diverse nature of symptoms experienced by people with a
NET can also result in significant delays to or misdiagnosis (Toth-Fejel and Pommier,
2004). People with NETs, particularly those with carcinoid syndrome, are commonly
misdiagnosed with other conditions such as irritable bowel syndrome, food allergies or
intolerances (Toth-Fejel and Pommier, 2004). Treatment for these conditions regularly
involves dietary modification and can lead people to alter their diets unnecessarily.
Various treatment modalities are used for disease and symptom control in patients
with GEP NETs. These may include surgery (curative or debulking, including bowel and
nodal resection, pancreatectomy or liver resection), somatostatin analogue treatment
(SSA, lanreotide or octreotide), chemotherapy, peptide-receptor targeted radiotherapy
(PRRT) and targeted therapy such as everolimus and sunitinib (Öberg et al., 2012). All
of these treatments have the potential to cause side-effects and symptoms that impact
HRQoL and nutritional health. Curative surgery may be performed if disease is localised
or palliative non-curative “debulking” resection may be used to assist with symptom
control and to improve quality of life (Ramage et al., 2012). Side-effects of
gastrointestinal surgery depend on the location and extent of resection but can include

53
altered gut function, and malabsorption by reduced absorptive surface, bacterial
overgrowth or blind loops (Lambert, 2008). SSA treatments have an anti-secretory
effect by inhibiting secretion of bioactive peptides, hence reducing hormone related
symptoms. In addition SSAs have tumoural anti-proliferative effects in patients with
NETs, preventing or reducing risk of disease progression (Rinke et al., 2009; Caplin et
al., 2014). Adverse effects of SSAs have been reported and include abdominal pain,
nausea, constipation, diarrhoea, cholelithiasis, steatorrheoa and disturbances of
glucose homeostasis (Caplin et al., 2014; Lamarca et al., 2018). SSA treatment can also
influence the secretion of intestinal fluid, pancreatic enzymes and bile acids, thus
impacting digestion and absorption processes (Fröjd et al., 2007; Modlin et al., 2010).
The symptoms experienced by people affected by NETs impact their physical and
mental well-being (Fröjd et al., 2007; Haugland et al., 2009; Kaupp-roberts,
Srirajaskanthan and Ramage, 2015; Pearman et al., 2016). The most commonly
occurring symptoms reported to impact HRQoL are fatigue, diarrhoea and flushing
(Haugland et al., 2009; Kaupp-roberts, Srirajaskanthan and Ramage, 2015; Pearman et
al., 2016). In an international survey of 1928 patients, most participants (71%)
reported that a NET diagnosis had substantially negatively impacted their personal
life, resulting in reduced energy levels and ability to perform household chores (Singh
et al., 2017). In an online survey of 663 German patients with NETs, the increased
frequency of bowel movements and presence of flushing were associated with
decreased quality of life (Pearman et al., 2016). Observational studies have also
identified that NET patients experience distress as a result of symptoms of fatigue and
diarrhoea, which impact people’s ability to perform daily physical activities (Larsson,
Haglund and Von Essen, 2003; Fröjd et al., 2007). People living with NETs in the US,
Norway and Sweden have been shown to have significantly lower HRQoL than the
general population when matched for age and gender (Fröjd et al., 2007; Haugland et
al., 2009; Beaumont et al., 2012).

54
Whilst this highlights an important need for effective symptom control and side-effect
management in people with NETs, there is limited information available to target
clinical care, research and education for Australians living with NETs, compared with
people living with other gastrointestinal disorders or cancers. Depression and anxiety
have also been reported to be prevalent amongst people with NETs, particularly at
time of diagnosis; however some studies have reported that the mental health of
patients with NETs may not be significantly different from the general population, and
rates of anxiety and depression may remain stable or improve over time from
diagnosis (Larsson et al., 2001; Fröjd et al., 2007). These studies were limited by small
sample sizes, n=24 and n=36 respectively, and with high attrition rates, but this picture
is replicated in other cancer groups where the emotional impact of the disease and its
treatment abates over time as people become more familiar with the expectations of
treatment, their treating team, and the shock of diagnosis subsides. Limitations of the
current literature on the HRQoL and symptom burden experienced by people with
NETs include, the heterogeneity of participant samples and the inconsistent
methodological approaches (Chau et al., 2013; Martini et al., 2016). For example,
most studies have used generic HRQOL measures to assess HRQoL with NET cohorts,
with only a few having used the NET specific module, EORTC QLQ GI.NET21 which is
validated and designed to assess quality of life in patients with gut and pancreatic NETs
(Yadegarfar et al., 2013).
The remainder of this chapter describes results from the Phase 1 longitudinal mixed-
methods study of patients with GEP NETs, including participant demographics, clinical
characteristics, symptomatology and HRQoL. Nutritional outcomes from the Phase 1
study are presented in Chapter 4.
3.2 Aims and objectives
As set out in Chapter 2, the aim of Phase 1 was:
To describe the impact of GEP NETs and their treatment on patients’ nutritional status
and HRQoL.
55
3.2.1 Objectives
1. To describe the nutrition-related symptoms and HRQoL of people living with a
GEP NET, including:
a. The prevalence and severity of patient-reported physical symptoms
b. Anxious and depressive symptomatology
c. Financial burden
d. Health-related quality of life
2. To explore any differences in HRQoL scores between baseline (T0) and six-months
(T6)
This was a prospective, embedded mixed-methods longitudinal study as described in
Chapter 2, Section 2.4.
3.4 Results
3.4.1 Patients
During the study recruitment period (June 2017 – June 2018), 188 newly referred
patients attending Upper Gastrointestinal (UGI) and NET clinics at study sites, were
available to assess their eligibility for the study. Thirty patients being investigated for a
GEP NET diagnosis were screened but were deemed ineligible after they received a
revised diagnosis of squamous cell carcinoma or adenocarcinoma. Other reasons for
ineligibility included: patient was for observation only (n=24), was receiving primary
medical treatment outside of the study site (n=19), NET disease found to be
completely resected and in remission (n=15), and patient was greater than 6 weeks
from initial referral to the study site (n=14). Of the 75 patients assessed as eligible, 61
patients were recruited to the study (Figure 3.1). Two participants were withdrawn
from the study immediately after recruitment and initial baseline data collection due
to changes in their diagnosis or treatment plan causing them to no longer meet

56
eligibility criteria; therefore, data from 59 participants was used for analysis. Figure 3.1
outlines the recruitment process and data available at each data collection time-point.
There were 35 counts of missing data due to a participant not attending the study site
at the time they were due for data collection. In total 28 of 59 (47%) participants had
complete data sets at all four time-points.
Whilst there were two recruitment sites, Peter MacCallum Cancer Centre and Austin
Health, 58 of 59 participants were recruited from the Peter MacCallum Cancer Centre.
As this study was undertaken in part-fulfilment of a PhD, participant recruitment and
data collection were undertaken by the same person (Coordinating principal
investigator (CPI), PhD student) at both sites. As the CPI was based at the Peter
MacCallum Cancer Centre, they had regular access to multidisciplinary meeting and
clinic lists which were used for screening potential participants. At Austin Health
screening of patients was undertaken by the site principal investigator (PI), who
communicated details of potential participants to the CPI, who then approached the
patient about the study. Over the recruitment period the CPI was notified of two
potential participants at Austin Health, of which one was eligible and approached to
participate.

57
EXCLUDED AT RECRUITMENT (total n = 127) INELIGIBLE (n = 113)
Observation only/not returning n = 24 Resected disease/remission n = 15 Treatment outside recruitment site n = 19 NET primary location outside GI tract n = 5 >6 weeks post initial appointment n = 14 Diagnosis/plan unclear n = 3 Revised diagnosis, not NET n = 30 Not new to service n = 2 End-stage disease/palliative n = 1
ELIGIBLE BUT NOT RECRUITED (n = 14) Declined participation n = 9 Researcher away/unwell n = 2 Missed in clinic n = 2 Unable to contact n = 1
Assessed for eligibility n = 188
Total recruited n = 61
DATA AVAILABLE FOR ANALYSIS
Baseline (T0) n = 59 Two-month follow-up (T2) n = 45
Four-month follow-up (T4) n = 39
Six-month follow-up (T6) n = 47
T2 MISSING DATA (n = 14)
Not attending site n = 13
Deceased (withdrawn) n = 1
WITHDRAWN (n = 2)* Revised diagnosis/not NET n = 1 Primary treatment for other cancer n = 1 *Excluded from all analysis
T0
T4
MISSING DATA (n = 19) Not attending site n = 16 Palliative/not returning (withdrawn) n = 2
Transfer to another hospital (withdrawn) n = 1
T6
MISSING DATA (n = 8) Not attending site n = 6 Deceased (withdrawn) n = 1 Personal reasons (withdrawn) n = 1
Figure 3.1 Participant recruitment map according to STROBE criteria
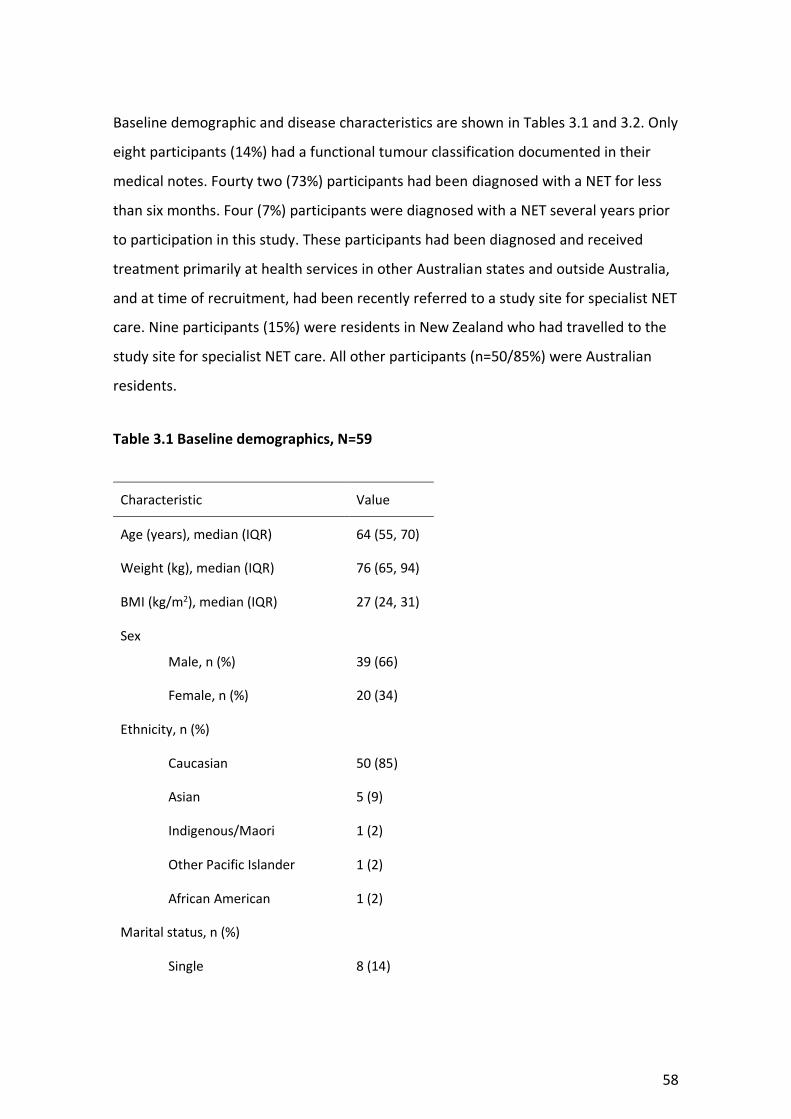
58
Baseline demographic and disease characteristics are shown in Tables 3.1 and 3.2. Only
eight participants (14%) had a functional tumour classification documented in their
medical notes. Fourty two (73%) participants had been diagnosed with a NET for less
than six months. Four (7%) participants were diagnosed with a NET several years prior
to participation in this study. These participants had been diagnosed and received
treatment primarily at health services in other Australian states and outside Australia,
and at time of recruitment, had been recently referred to a study site for specialist NET
care. Nine participants (15%) were residents in New Zealand who had travelled to the
study site for specialist NET care. All other participants (n=50/85%) were Australian
residents.
Table 3.1 Baseline demographics, N=59
Characteristic Value
Age (years), median (IQR) 64 (55, 70)
Weight (kg), median (IQR) 76 (65, 94)
BMI (kg/m2), median (IQR) 27 (24, 31)
Sex
Male, n (%) 39 (66)
Female, n (%) 20 (34)
Ethnicity, n (%)
Caucasian 50 (85)
Asian 5 (9)
Indigenous/Maori 1 (2)
Other Pacific Islander 1 (2)
African American 1 (2)
Marital status, n (%)
Single 8 (14)

59
Characteristic Value
Divorced 4 (7)
Widowed 3 (5)
Married 37 (63)
De-facto 7 (12)
Education level, n (%)
Not university educated 37 (63)
Bachelor degree/higher 20 (34)
Not specified 2 (3)
Employment status, n (%)
Full-time 20 (34)
Part-time 8 (14)
Retired 24 (41)
Not employed/student 2 (3)
Medical disability 5 (9)
BMI, body mass index
Table 3.2 Baseline disease characteristics, N=59
Characteristic Value
Primary Tumour site, n (%)
Small intestine 27 (46)
Pancreas 21 (37)
Colon 6 (10)
Other 5 (9)
Tumour grade, n (%)

60
Characteristic Value
NET G1 17 (29)
NET G2 22 (37)
NEC G3 10 (17)
Other 1 (2)
Unknown 9 (15)
Functional tumour classification, n (%)
Gastrinoma 4 (7)
Insulinoma 2 (3)
Glucagonoma 2 (3)
Unspecified 51 (86)
Metastatic, n (%) 45 (76)
Time from diagnosis, n (%)
<1 month 23 (40)
2-5 months 19 (33)
6-11 months 6 (11)
1-2 years 5 (9)
>3 years 4 (7)
Treatment received for NET, n (%)
Surgery 13 (22)
PRRT 5 (9)
Chemotherapy 8 (14)
SSA 24 (41)
Interferon 1 (2)
Other 2 (3)
No treatment 24 (41)

61
Characteristic Value
Co-morbid conditions with dietary consequences, n (%)
IBS 7 (12)
Food intolerance/allergy 5 (9)
Diabetes 17 (29)
IBD 3 (5)
Symptoms duration pre-study, n (%)
Nil 6 (10)
<6 months 7 (12)
6-11 months 14 (24)
1-2 years 15 (25)
3-5 years 7 (12)
6-10 years 7 (12)
>10 years 2 (3)
Unsure 1 (2)
PRRT, peptite receptor radionucleotide therapy; SSA, somatostatin analogue; IBS, irritable bowel
syndrome; IBD, inflammatory bowel disease
3.4.2 Health-related quality of life
Raw HRQoL scores (mean and standard deviation) for EORTC scales and items at all
time-points are provided in Appendix 2. The mean and standard error (model
estimates) for T0, T2, T4 and mean change in scores from T0 to T6 (with 95%
confidence intervals) are provided in Table 3.3. Kazis effect sizes for each difference
between T0 and T6 are also included in Table 3.3. The mean global health status score
of participants at baseline was 62.9 which is 5-points lower than general Australian
population scores indicating worse HRQoL for GEP NET patients in this study. Mean
global health status showed no significant change over-time (p = 0.30, Kazis effect size

62
= 0.13). The difference between scores (Kazis effect size) over-time (from T0 to T6) for
all of the EORTC QLQ-C30 functional scales (physical, role, emotional and social) were
trivial, indicating no clinical relevance. A medium-sized difference between T0 and T6
was observed for the disease-related worries scale, which was also statistically
significant (p = 0.002) indicating this improved over-time. There was a statistically
significant reduction between T0 and T6 for the social function scale of the EORTC
GINET21 (p = 0.02), indicating this worsened over-time, but the Kazis effect size was
less than 0.2 suggesting this change may not be clinically significant. Body image and
sexual function both had a small-sized reduction (Kazis effect size = 0.28 and 0.23,
respectively, both p > 0.05), indicating worsening over-time between T0 and T6.

63
Table 3.3 Health-related quality of life and symptom scores over-time
Recruitment (T0) 2-months (T2) 4-months (T4) 6-months (T6)
Kazis effect size Scale/item M SE M SE M SE M chg
from T0 95% CI
EORTC QLQ-C30
Global health status 62.9 3.2 62.4 3.4 67.2 3.5 2.6 (-2.6, 7.9) 0.13
Physical functioning 81.5 2.9 78.3 3.2 80.6 3.3 -1.7 (-7.2, 3.8) 0.09
Role functioning 77.7 4.1 69.2 4.5 77.3 4.9 -2.2 (-11.1, 6.7) 0.07
Emotional functioning 73.3 2.9 74.4 3.2 80.7 3.5 2.6 (-4.1, 9.4) 0.14
Cognitive functioning 77.9 2.7 75.8 3.0 83.0 3.2 -1.7 (-8.1, 4.6) 0.09
Social functioning 73.8 3.7 70.9 4.0 77.4 4.3 -3.3 (-10.8, 4.3) 0.12
Fatigue 34.5 3.4 41.1 3.8 32.3 4.0 0.2 (-7.0, 7.4) 0.01
Nausea/vomiting 10.5 2.2 11.9 2.6 6.9 2.8 -3.4 (-9.5, 2.6) 0.17
Pain 29.2 3.9 26.9 4.3 21.9 4.6 -3.7 (-12.0, 4.7) 0.12
Dyspnoea 12.9 3.0 17.4 3.4 13.5 3.7 0.7 (-6.5, 8.0) 0.03
Insomnia 41.7 4.2 37.9 4.6 27.3 4.8 -7.4 (-15.5, 0.7) 0.26
Appetite loss 19.2 3.5 23.0 4.0 18.4 4.4 -4.0 (-13.5, 5.4) 0.15
Constipation 14.6 2.6 13.2 3.0 7.5 3.3 -0.8 (-7.4, 5.8) 0.03

64
Recruitment (T0) 2-months (T2) 4-months (T4) 6-months (T6)
Kazis effect size Scale/item M SE M SE M SE M chg
from T0 95% CI
Diarrhoea 22.5 3.8 23.9 4.1 24.7 4.4 1.7 (-5.7, 9.1) 0.06
Financial problems 22.9 4.0 22.6 4.3 17.4 4.4 1.2 (-5.0, 7.4) 0.04
EORTC GINET21
Endocrine 17.9 2.1 9.6 2.4 12.2 2.6 -7.4 (-12.5, -2.2) 0.23
Gastrointestinal 27.4 2.4 23.7 2.8 22.9 3.0 -4.2 (-10.0, 1.6) 0.13
Treatment-related symptoms 16.6 3.5
17.6 3.0 15.6 3.4 3.5 (-5.5, 12.5)
0.12
Social function 41.8 3.0 38.7 3.2 28.7 3.4 -6.5 (-11.9, -1.2) 0.15
Disease-related worries 55.7 3.6 47.6 3.9 37.3 4.1 -10.4 (-17.0, -3.8) 0.53
Muscle/bone pain 30.3 3.7 28.5 4.1 19.4 4.4 1.7 (-6.6, 9.9) 0.08
Sexual function 33.9 5.9 30.4 6.3 16.2 6.8 -5.0 (-18.2, 8.1) 0.23
Information/ communication function
15.0 3.1 10.0 3.5 7.2 3.8 -4.3 (-12.4, 3.9) 0.18
Body image 29.5 5.0 28.5 5.3 20.2 5.6 -7.5 (-16.0, 0.9) 0.28
All p > 0.05 for score comparisons between 6 months post-baseline and baseline, excepting GINET21 Endocrine (p = 0.01), Social function (p = 0.02) and Disease-related worries (p = 0.002).
Kazis effect size interpretation: >0.2 = small-sized difference, >0.5 = medium-sized difference, >0.8 = large-sized difference

65
3.4.3 Symptom prevalence and severity
Of the symptom scales in the EORTC QLQ-C30, fatigue and insomnia had the highest
mean value indicating they were the most severe and burdensome on participants in
this study, followed by pain and diarrhoea (Table 3.3). There was a small-sized
reduction in the mean score for insomnia between T0 and T6, indicating the burden of
this symptom may have improved over-time (Kazis effect size = 0.26, p > 0.05). There
was no statistically or clinically significant change in mean scores for other symptom
scales and items of the EORTC QLQ-C30 over the six-month data collection period
(Table 3.3). The endocrine scale of the EORTC GINET21 showed a small-sized reduction
(Kazis effect size = 0.23, p = 0.01) between T0 and T6, indicating the symptoms of
flushing and hot flushes improved over-time. All other symptom scales of the EORTC
GINET21 showed no clinically or statistically significant change over-time from T0 to
T6.
Table 3.4 presents results for symptom prevalence, calculated using particular EORTC
QLQ-C30 and EORTC GI.NET21 item scores (Chapter 2, Table 2.2). Fatigue, abdominal
discomfort, pain and bloating were the most prevalent symptoms at baseline with at
least 36 (60%) of participants reporting them. Symptoms of wind/gas, hot flushes,
diarrhoea, night sweats, reflux/heartburn and loss of appetite were also prevalent with
at least 24 (40%) participants reporting to experience these at baseline (T0). These
symptoms and weight loss were also the most prevalent high-intensity symptoms
(Table 3.4). The symptoms that reduced in prevalence by T6 included wind/gas (-21%),
hot flushes (-18%), night sweats (-18%), pain (-12%), weight loss (-11%), vomiting (-
10%) and loss of appetite (-6%) (Table 3.4). Abdominal discomfort, bloating, and
reflux/heartburn remained prevalent through the study period but were of reduced
intensity by T6. The symptom of fatigue remained prevalent throughout the study
period and was the only symptom to increase in reported intensity by T6 (Table 3.4).
Sixteen of 59 (27%) participants at T0 and 12 of 47 (25%) participants at T6 reported
experiencing both diarrhoea and flushing, indicating presence of carcinoid syndrome.
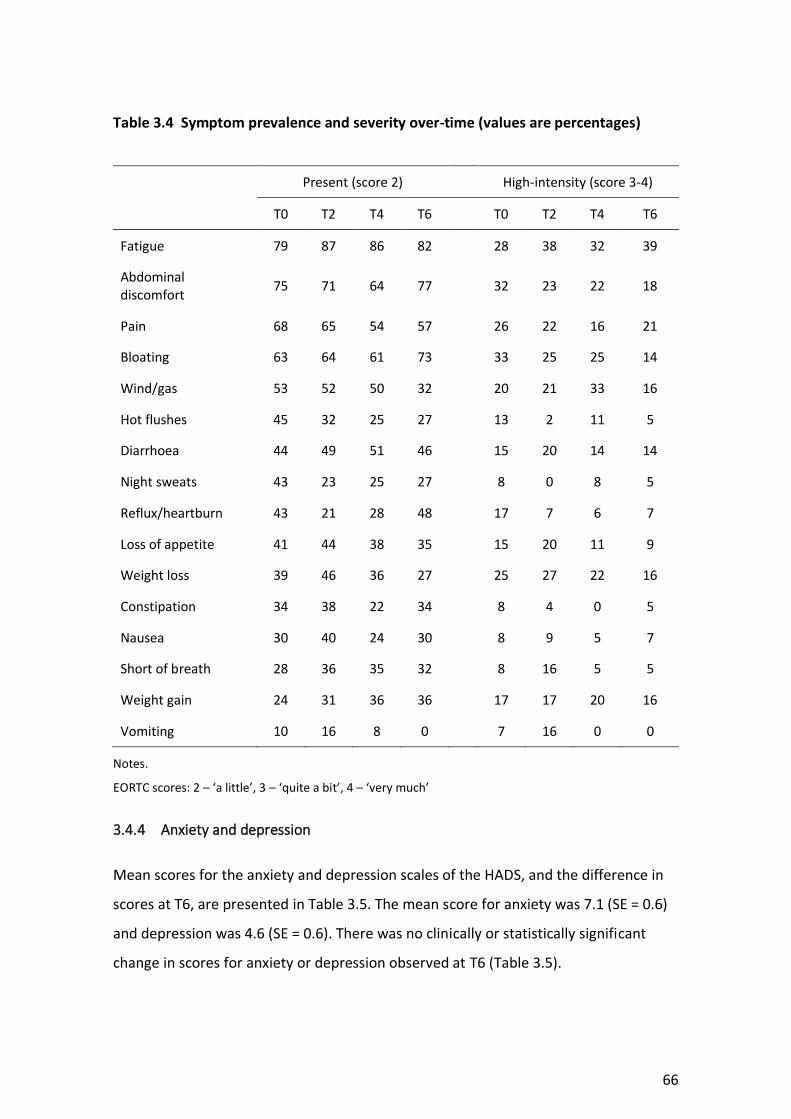
66
Table 3.4 Symptom prevalence and severity over-time (values are percentages)
Present (score 2) High-intensity (score 3-4)
T0 T2 T4 T6 T0 T2 T4 T6
Fatigue 79 87 86 82 28 38 32 39
Abdominal discomfort
75 71 64 77 32 23 22 18
Pain 68 65 54 57 26 22 16 21
Bloating 63 64 61 73 33 25 25 14
Wind/gas 53 52 50 32 20 21 33 16
Hot flushes 45 32 25 27 13 2 11 5
Diarrhoea 44 49 51 46 15 20 14 14
Night sweats 43 23 25 27 8 0 8 5
Reflux/heartburn 43 21 28 48 17 7 6 7
Loss of appetite 41 44 38 35 15 20 11 9
Weight loss 39 46 36 27 25 27 22 16
Constipation 34 38 22 34 8 4 0 5
Nausea 30 40 24 30 8 9 5 7
Short of breath 28 36 35 32 8 16 5 5
Weight gain 24 31 36 36 17 17 20 16
Vomiting 10 16 8 0 7 16 0 0
Notes.
EORTC scores: 2 – ‘a little’, 3 – ‘quite a bit’, 4 – ‘very much’
3.4.4 Anxiety and depression
Mean scores for the anxiety and depression scales of the HADS, and the difference in
scores at T6, are presented in Table 3.5. The mean score for anxiety was 7.1 (SE = 0.6)
and depression was 4.6 (SE = 0.6). There was no clinically or statistically significant
change in scores for anxiety or depression observed at T6 (Table 3.5).

67
Table 3.5 Paired t-test results for HADS scales
T0 T6
Scale M SE M diff 95% CI p-value
HADS
Anxiety 7.1 0.6 0.8 (-0.2, 1.8) 0.12
Depression 4.6 0.6 0.1 (-1.0, 1.3) 0.82
Notes.
M = Mean, SE = Standard Error, M diff = Mean difference
Table 3.6 presents results for anxiety and depression data using HADS scoring
(Zigmond and Snaith, 1983; Snaith, 2003). At baseline (T0) there were 12 (22%) cases
of anxiety, and 5 (9%) cases of depression identified (Table 3.6). There was no
difference in cases of anxiety at T6 and a small reduction in cases of depression at T6.
Table 3.6 Caseness of anxiety and depression as per HADS scoring
T0
(N = 55)
n (%)
T6
(N = 42)
n (%)
% diff T6-T0
Anxiety
Present 9 (17) 9 (21) 5
Disorder 12 (22) 9 (21) -1
Depression
Present 7 (13) 7 (17) 4
Disorder 5 (9) 2 (5) -4
Notes.
HADS scoring – 0-7 = normal, 8-10 = presence of anxiety/depression, 11-21 = disorder; Disorder, defined as definite case of anxiety/depression

68
Recent exploration of HADS cut-off scores has suggested that the traditional cut-off
scores may not be appropriate for cancer patients, and may underestimate the burden
of anxiety and depression in cancer populations, as discussed in Chapter 2 (Morse,
Kendell and Barton, 2005; Singer et al., 2009; Martinez et al., 2012). Therefore, revised
scoring recommended for cancer patients was performed (Table 3.7). Table 3.7
presents results for presence of anxiety and depression amongst participants using
revised cancer-specific scoring of the HADS. Using the revised cancer-specific scoring,
the prevalence of anxiety cases at T0 and T6 respectively was n=39 (71%) and n=32
(76%). The prevalence of depression cases using the revised cancer-specific scoring at
T0 and T6 was n=29 (53%) and n=23 (55%) (Table 3.7).
Table 3.7 Caseness of anxiety and depression as per alternative HADS scoring (values are counts and percentages)
T0
(N = 55)
n (%)
T6
(N = 42)
n (%)
% diff T6-T0
Anxiety 39 (71) 32 (76) 5
Depression 29 (53) 23 (55) 2
Total 38 (69) 28 (67) -2
Notes.
HADS scoring – HADS-A and HADS-D Score >6 = presence of anxiety/depression, HADS-T score >13 =
presence of any disorder (case)
3.4.5 Financial toxicity
The mean score for the COST-FACIT was 27 (SD = 17) and there was no significant
change in score at T6 (M chg = -1.4, 95% CI [-3.7, 1.0], p = 0.24). At T0, one participant
had the lowest possible score of 0 indicating very poor financial well-being and four
participants had the highest possible score of 44, indicating very good financial well-
being. At T6 there were no participants with a score of 0, and five participants had a
score of 44. When data at T0 was categorised, 12 (22%) participants had a low score

69
(0-15), 21 (38%) participants had a moderate score (16-30), and 22 (40%) participants
had a high score (31-44) (Table 3.8). At T6 the number of participants with a low score
decreased to 3 (7%) and the number of participants with a moderate score increased
to 26 (59%), indicating that overall, participants had improved financial well-being over
time (Table 3.8). Eight of 12 participants who had a high degree of financial toxicity
(score <15) on the COST-FACIT at T0, and all 3 participants who had a high degree of
financial toxicity at T6, also had a low global health status score (<50) on the EORTC-
QLQC30 indicating a relationship between worse financial toxicity and low HRQoL.
Table 3.8 COST-FACIT scores per percentile (values are counts and percentages)
Score range
T0
(n = 55)
T6
(n = 44)
0-15 12 (22) 3 (7)
16-30 21 (38) 26 (59)
31-44 22 (40) 15 (34)
3.5 Discussion
The symptom burden and HRQOL of patients with GEP NETs, including financial toxicity
and presence of anxiety and depression were explored over a period of six-months,
from patients’ initial consultation at a NET referral hospital.
A large proportion of participants were symptomatic at recruitment and throughout
the study period, with many reporting fatigue, abdominal discomfort, pain and
bloating. Symptoms of wind/gas, hot flushes, diarrhoea and loss of appetite were also
prevalent. Previous studies have indicated fatigue (35-69%), diarrhoea (27-92%),
abdominal discomfort (22-50%) and flushing (19-53%) to be amongst the most
prevalent symptoms experienced by patients diagnosed with a GEP NET (Fröjd et al.,
2007; Haugland et al., 2013; Lind, Wängberg and Ellegård, 2016; Singh et al., 2016).

70
The highest rates of diarrhoea have been recorded in GEP NET patients post-small
bowel surgery and diagnosed with carcinoid syndrome (Lind, Wängberg and Ellegård,
2016). In this PhD study only 13 (22%) participants had undergone surgery prior to
recruitment, and a further eight underwent surgery during the study period, which
may explain why the prevalence of diarrhoea in this PhD study is lower than other
studies. The proportion of patients diagnosed with carcinoid syndrome was not
formally recorded in this study. However, the presence of particular symptoms
(diarrhoea and flushing) associated with carcinoid syndrome, as reported by
participants on the EORTC QLQ-C30 and GINET21 module, was 27% and 25% of
patients at T0 and T6 respectively.
The burden of weight loss amongst GEP NET patients is not well documented. Only one
other study to date has documented the prevalence of weight loss to be 21%, as
reported by NET patients in a large international survey (N=1928) (Singh et al., 2017).
In this PhD study, weight loss was reported as a symptom by 23 (39%) participants at
T0 (25% at high-intensity) and 13 (27%) at T6. The participants in Singh’s study (Singh
et al., 2017) were longer after diagnosis (41% of participants more than five years after
diagnosis), whereas in this PhD study 55 (93%) participants were under three years
from diagnosis. This may indicate that weight loss is more prevalent soon after
diagnosis. In this PhD study and Singh’s study, weight loss was assessed by participant
responses to one question. The amount of weight loss and period of time over which
weight loss had occurred was therefore not recorded. Further observation and
assessment of weight and changes over time is required to determine the degree to
which weight loss and its trajectory impacts patients with NETs. In Chapter 4 the
measured prevalence of nutritional complications among study participants is
described in more detail, including participants’ weight change, recorded prospectively
on scales over the study period.
Fatigue was the most prevalent and severe symptom reported by participants in this
study. Cancer-related fatigue has been recognized as a common and distressing side-
effect of cancer and it’s treatment, with an average of 30-60% of cancer patients

71
reporting a moderate to severe burden of fatigue during treatment (Bower, 2014).
Fatigue can impact on ability to work, maintain social and family relationships,
maintain basic daily activities including cooking, and worsen mood (Bower, 2014).
Fatigue therefore has the potential to impair nutrition through impacts on meal
preparation, subsequent dietary intake, and physical deconditioning due to decreased
exercise capacity (Inglis et al., 2019). Other prevalent symptoms among participants in
this study that have potential to impact on nutrition included; abdominal discomfort,
bloating and loss of appetite which could impact the desire for eating; and diarrhoea
which is potentially indicative of digestive malabsorption or nutrient losses. Available
literature fails to examine the relationship between symptom burden and nutritional
complications among people diagnosed and treated for a NET. Further longitudinal
observational and qualitative studies are required to explore the relationship between
such symptoms and nutritional issues. Chapter 4 of this thesis will describe the
prevalence and severity of nutritional complications as reported by participants in the
Phase 1 study, and Chapter 5 will report results of qualitative interviews with Phase 1
participants, providing in-depth insight of the impact of symptoms on nutrition and
HRQoL.
The EORTC QLQ-C30 and EORTC GI.NET21 are frequently used validated tools for the
assessment of HRQoL in GEP NET patients (Jimenez-Fonseca et al., 2015; Martini et al.,
2016). In a study by Strosberg et al (2018) a group of patients (N = 231) with advanced
progressive mid-gut NETs of low/intermediate grade had similar scores for global
health status (M = 67, SD = 22), as well as all functional scales and all symptom
scales/items relative to the patients in this PhD study (Strosberg et al., 2018). Larsson
et al. (2001) assessed HRQoL using the EORTC QLQ-C30 in a group of 24 patients with
carcinoid syndrome on either somatostatin analogue or interferon treatment, and
found a similar global health status score of 68 (SD = 23) (Larsson et al., 2001). Baseline
scores for most HRQoL scales were also similar in the study by Larsson et al (2001),
except for role functioning which was 13 points lower (M = 65, SD = 33) than in this
study; and social functioning which was 11 points higher (M = 85, SD = 20) than in this
study (Larsson et al., 2001). In comparison to general Australian population scores for

72
the EORTC QLQ-C30 (Mercieca‐Bebber et al., 2019), participants in this study at
recruitment (T0) had a lower score (mean difference of 10 points or greater) for role
functioning, cognitive functioning and social functioning indicating that performance at
work and hobbies, memory and concentration, family life and social activities was
impaired. A difference in mean scores between groups of >10 points is considered
clinically significant (Cocks et al., 2012). This observed functional impairment of
patients in this PhD study may have been present prior to GEP NET diagnosis, but could
also be in part due to the burden of the disease and related symptoms; including
fatigue, diarrhoea, pain and bloating; which have been demonstrated to cause distress
among patients with a NET and impact their quality of life (Fröjd et al., 2007; Pearman
et al., 2016). The generalised gastrointestinal symptoms of GEP NET patients are often
misdiagnosed and prolonged even prior to formal NET diagnosis (Modlin et al., 2010).
Data from the symptom scales/items in this study indicated that participants had
higher scores for insomnia, appetite loss and diarrhoea than the general Australian
population, supporting the theory that increased symptom burden may impact HRQoL.
There was no change in participants’ global health status score over the six-month
period from recruitment. A statistically significant reduction in the disease-related
worries scale and social function scales of the EORTC QLQ-GI.NET21 over-time,
indicated an improvement in participant concerns regarding disease recurrence and
future health, but worsening of social aspects including relationships and concern for
the impact of their NET on their family and friends. This suggests that despite specialist
NET information and medical management, a NET diagnosis and treatment has
prolonged impacts on people’s home life and social relationships. A study by Snyder et
al. (2015) has shown that a mean score change of 10 points identifies a clinically
meaningful change in the supportive care needs of cancer patients (Snyder et al.,
2015). The mean score for the social functioning scale reduced by 10 points at T4,
indicating worsening of social function leading to a change in supportive care needs.
Data from this study show that assessment of patient’s emotional health and social
supports is an important aspect of supportive care for NET patients, irrespective of
their level of physical function and overall HRQoL.

73
Using traditional HADS scoring, one fifth of participants in this study were assessed as
having a likely case for anxiety at both T0 and T6, and less than 10% had a likely case
for depression at both time-points. Using the revised scoring for cancer, the
prevalence of caseness for anxiety and depression amongst participants was high
across each of the study data collection time points. Based on these results, it would
be reasonable to suggest that patients living with a NET are at risk of anxiety and
depression, and screening for presence of anxiety and depression is important for all
NET patients at diagnosis and during treatment. Other studies in mid-gut NETs, which
used the HADS, found similar results for presence of depression, but lower results for
presence of anxiety (Larsson et al., 2001). Increased symptom burden has been
associated with distress in patients diagnosed with a NET (Fröjd et al., 2007; Haugland
et al., 2009; Beaumont et al., 2012). Results of this PhD study showed no obvious
correlation between HADS score for anxiety or depression and presence of symptoms,
or time from diagnosis, although formal sub-analysis was limited by sample size.
Further qualitative exploration of the impact of psychological aspects including
distress, anxiety and depression on quality of life, and nutritional issues is important.
As mentioned above, Chapter 5 will report results of qualitative interviews conducted
with a purposive sample of participants enrolled in the Phase 1 study, exploring the
HRQoL and nutritional impacts in depth.
Financial well-being varied amongst participants in this study and improved over time.
The COST-FACIT is a relatively new tool available to assess the financial burden of a
cancer diagnosis on patients and has been validated for use in cancer populations (de
Souza et al., 2017). The financial consequences of cancer treatment can include
considerable out-of pocket medical expenses, loss of income due to inability to work,
and burden on caregivers (Northouse et al., 2012; Bestvina et al., 2014; de Souza et al.,
2017). The mean COST-FACIT score for participants was 27 (SD = 1.7), which is higher in
comparison to the mean score of other studies, indicating better financial toxicity of
participants in this PhD study (de Souza et al., 2017; D’Rummo et al., 2019). The COST-
FACIT validation study found a mean score of 22.2 (SD=11.9) in 236 patients with
advanced stage IV cancer undergoing chemotherapy (de Souza et al., 2017). Another

74
study which assessed 167 patients undergoing radiation therapy with the COST-FACIT
found a mean result of 21.9 (SD=9.3) (D’Rummo et al., 2019). Overall patients in the
study had better financial well-being than patients in other studies, which could be
explained by the fact that the majority of study participants were early in their
diagnosis and treatment planning. Compared to other gastrointestinal cancer types,
GEP NETs have a higher prevalence and better survival rates, therefore it is important
to explore in future studies the impact of living longer with a complex disease on
patient’s finances. The study site was a public hospital so we can assume that
participants would have had fewer out-of-pocket medical expenses than if they were
treated in the private setting. The site at which patients are receiving treatment, is
therefore an important consideration for future studies examining the prevalence and
impact of financial toxicity in patients with GEP NETs.
Factors documented in the literature to be associated with a lower COST-FACIT score
and worsening financial toxicity included being unemployed, non-caucasian race,
higher level of psychological distress and frequent (>3) in-patient admissions (de Souza
et al., 2017; D’Rummo et al., 2019). The majority of participants in this study were
Caucasian, remained in the outpatient setting for the duration of the study, and were
either employed or retired. Increased financial toxicity has been associated with
worsening symptom burden and HRQoL, and should therefore be a priority to address
(Zafar et al., 2015; Lathan et al., 2016). In this PhD study some participants who scored
lower (below 50) for global health status also scored low on the COST-FACIT, indicating
a high degree of financial toxicity. However no clear association between HRQoL and
financial toxicity was found. Only one other study has examined the financial toxicity of
patients living with a NET. In a survey of 204 Australian NET patients, many were
burdened by medical expenses, and their quality of life was adversely affected by
increasing financial toxicity (Gordon et al., 2020). In this study, and the study by
Gordon et al. (2020), show that financial toxicity does exist among NET patients and it
is therefore important to screen for financial issues in this population (Gordon et al.,
2020).

75
3.6 Conclusion
This chapter has reported data on HRQoL and symptom burden amongst a
heterogeneous population of GEP NET patients from Phase 1 of the PhD. The inclusion
of patients with various NET primary sites, grades and treatment history is a strength
of the study as it is representative of the heterogeneous NET population within a
specialist NET referral centre. Patients with GEP NET in this study had poorer HRQoL
than the general Australian population, and social functioning declined over-time
despite medical intervention and treatment received at a NET referral hospital. Anxiety
and depression were prevalent, as was financial distress, although the degree of
financial distress was less than documented in other cancer populations. Participants
reported a variety of symptoms, including fatigue, pain, abdominal discomfort,
bloating, wind/gas and diarrhoea, which remained prevalent throughout the study
period. Overall, symptom severity improved over-time, except for fatigue. Some
symptoms, if prolonged and severe, have the potential to impair nutritional status due
to impacts on dietary intake and ability or desire to prepare food. Results highlight the
need to monitor symptoms and HRQoL among patients with GEP NETs regardless of
their stage of treatment, in order to identify and address their supportive care needs.
The relationship between the HRQoL and symptoms described in this chapter and the
presence of nutritional complications requires further exploration. The nutritional
complications experienced by patients with a GEP NET is described in Chapter 4 and
Chapter 5 to provide in-depth information on the impact of GEP NETs and treatments
on HRQoL, symptoms and nutritional wellbeing.


77
Chapter 4: Nutritional status in people with NETs
In Chapter 3 initial data from the Phase 1 prospective mixed-methods study showed
that symptoms of fatigue, abdominal discomfort, pain, bloating and diarrhoea, were
prevalent amongst study participants. Participants reported lower quality of life scores
than the general Australian population for several functional scales indicating impaired
work performance, family life and social activity as a result of their NET diagnosis. This
chapter focuses in detail on the nutritional status of participants and describes and
discusses the nutritional complications of participants who took part in the Phase 1
study.
4.1 Introduction
Cancer has the potential to impact on a person’s diet, weight and nutritional status
due to the presence of a tumour mass, and the symptoms of the tumour or its
treatment. The prevalence of malnutrition amongst gastrointestinal cancer patients
varies between 24-61%, and nutrition support has been highlighted as an important
aspect of cancer care, known to improve morbidity and treatment outcomes
(Nitenberg and Raynard, 2000; Marín Caro, Laviano and Pichard, 2007; J. Arends et al.,
2017; Marshall et al., 2019). Research exploring the nutrition support needs of
gastrointestinal cancer patients has focused on gastric, colorectal and oesophageal
adenocarcinoma and squamous cell carcinoma. In regard to NETs of the
gastrointestinal tract, tumoural-related symptoms and side-effects are well
documented; however, the impact of a GEP NET on nutritional status and dietary
factors continues to require further exploration. There is limited published evidence on
the specific nutritional impact of GEP NETs and their influence on people’s
requirement for nutrition support and intervention. As discussed in Chapter 1 and
Chapter 3, GEP NETs can have a unique symptomatology relating to their hormonal
hypersecretion and side-effects of NET-specific treatments, including somatostatin
analogue (SSA) therapy. GEP NETs overall have a far longer disease course due in part,
to being an indolent cancer, and hence have a better prognosis than other

78
gastrointestinal cancer types. As a result there is a high prevalence rate in the
community, with many people living with symptoms of a NET or with the
consequences of prolonged NET treatments (Modlin et al., 2010; Dasari et al., 2017).
The occurrence and severity of these NET associated physical symptoms have the
potential to significantly impact on a patient’s nutritional status through potential
effects on nutrient absorption, dietary habits, weight change, appetite and desire to
eat (Gallo et al., 2017; Altieri et al., 2018; D. Clement et al., 2019; Laing et al., 2019).
Reduced HRQoL and the presence of anxiety, distress or depression amongst people
diagnosed with GEP NET may also impact further on these factors and contribute to
risk of nutrition complications including malnutrition. Review articles have commented
on the essential role of nutrition in the diagnosis and management of patients with
NETs (Gallo et al., 2017; Altieri et al., 2018; D. S. V. M. Clement et al., 2019; Laing et al.,
2019), but a thorough description of nutritional issues and their management, through
longitudinal and interventional studies, is lacking. There are currently no data available
describing the extent of nutrition intervention, including dietitian referral and
consultation among NET patients. Internationally, only two pilot cross-sectional studies
have assessed malnutrition in people diagnosed with a NET, with results indicating
malnutrition rates of 14-25% (Qureshi et al., 2016; Maasberg et al., 2017). Food
intolerance and dietary modification have been highlighted by studies to-date but not
explored in detail (Haugland et al., 2009; Lind, Wängberg and Ellegård, 2016; Gallo et
al., 2017). These studies indicate that dietary modification occurs among patients with
a NET but provide limited information about the type and cause for dietary change,
and the impact this has on HRQoL and nutrition issues such as weight loss and
malnutrition. The presence of a NET can lead to altered vitamin metabolism and
absorption, including niacin in people diagnosed with a serotonin-producing NET, and
fat-soluble vitamins in people treated with long-term SSA therapy (Shah et al., 2005;
Fiebrich et al., 2010; Lind, Wängberg and Ellegård, 2016; Qureshi et al., 2016). Studies
of vitamin deficiency in NET patients have been cross-sectional and focused on specific
GEP NET groups and treatments. Further evidence is required to explore this
phenomenon across all GEP NET types, and identify an appropriate screening approach

79
in order to establish optimal identification and management of vitamin deficiencies.
Despite the presence of the limited evidence that nutritional complications occur in
patients with GEP NETs, acknowledgement of any nutritional complications and
nutritional management of people affected by NETs remains absent in clinical
guidelines.
4.2 Aims and objectives
4.2.1 Chapter aim
The aim of this chapter is to describe data collected on the impact of GEP NETs and
their treatment on nutritional status and nutritional complications in a cohort of
patients referred for medical management at a NET referral hospital.
4.2.2 Objectives
To describe point prevalence and severity of nutritional complications among people
living with a GEP NET, including:
a. Objectively assessed malnutrition and changes in weight and fat-free mass
b. Objectively assessed vitamin deficiencies
c. Patient-reported dietary habits
Secondary objective
If appropriate, to examine differences in nutritional outcomes (e.g. nutritional status)
between subgroups of patients defined by disease and treatment related
characteristics (e.g disease type and stage) at recruitment and six-months follow-up.

80
4.3 Method
This was a prospective mixed-methods longitudinal study as described in Chapter 2,
Section 2.5.
4.4 Results
4.4.1 Participants
Fifty nine patients were recruited over 12 months (June 2017 – June 2018). The
demographics and clinical characteristics of participants were presented in Chapter 3,
Tables 3.1 and 3.2. The nutritional characteristics of participants at recruitment (T0)
are presented in Table 4.1.
Table 4.1 Nutritional characteristics at recruitment, N=58
Characteristic Value
Weight (kg), median (IQR) 76 (65, 94)
BMI (kg/m2), median (IQR) 27 (24, 31)
Underweight, n (%) 6 (10)
Healthy weight, n (%) 21 (36)
Overweight, n (%) 19 (33)
Obese, n (%) 12 (21)
Fat free mass (kg), median (IQR) 56 (46, 63)
Notes.
Underweight: <65yo: BMI <18.5, >65yo: BMI <22, Healthy weight: <65yo: BMI 18.5-25, >65yo: BMI 22-27, Overweight: <65yo: BMI 25-30, >65yo: BMI 27-32, Obese: <65yo: BMI >30, >65yo: BMI >32
BMI, body mass index
4.4.2 Nutritional status
At baseline (T0), 17 of 58 participants (29%) were malnourished (PG-SGA score B or C).
Of the 46 patients assessed at six-months post baseline (T6), six (13%) were

81
malnourished. Results for nutritional status at all time-points are summarised in Table
4.2.
Based on paired analysis, the proportional differences in malnourished patients at
follow-ups were: -0.09 at T2 (95% CI: -0.28, 0.10), -0.14 at T4 (95% CI: -0.32, 0.05), and
-0.11 at T6 (95% CI: -0.27, 0.05). All point estimates suggested fewer malnourished
patients at follow-up, but in every instance confidence intervals were wide and
included zero.
Table 4.2 Prevalence of nutritional status at all time-points
T0
(N = 58)
T2
(N = 45)
T4
(N = 38)
T6
(N = 46)
n (%) n (%) n (%) n (%)
Well nourished (PG-SGA A) 41 (71) 33 (73) 33 (87) 40 (87)
All malnourished (PG-SGA B and C) 17 (29) 12 (27) 5 (13) 6 (13)
Suspected/moderate malnutrition (PG-SGA B) 15 (26) 7 (16) 4 (11) 5 (11)
Severe malnutrition (PG-SGA C) 2 (3) 5 (11) 1 (3) 1 (2)
Four malnourished patients were withdrawn prior to T6 due to death or transfer to
palliative care, and therefore their nutritional status was not assessed at T6, which
could have affected results at this time-point. Of the participants with complete data
at T0 and T6 (n=46), 30 (65%) remained well-nourished throughout the study, 10 (21%)
who were malnourished at T0 had improved nutritional status by T6, 3 (7%) remained
malnourished throughout the study, and 3 (7%) developed malnutrition during the
study (1 at T2, 1 at T6).

82
At recruitment (T0), 48 of 59 participants (81%) had an available classification of NET
grade and 58 (98%) had a classification of primary NET site. Nutritional status was
compared between patients grouped by NET grade and by primary NET site (Tables 4.3
and 4.4).
Table 4.3 Prevalence of malnutrition by NET grade
T0 T6
N Malnourished, n (%) N Malnourished, n (%)
NET G1 16 3 (19) 13 3 (23)
NET G2 22 6 (27) 20 1 (5)
NEC G3 10 4 (40) 6 0 (0)
All 48 13 (27) 39 4 (10)
Notes.
Malnourished, PG-SGA score B or C
Participants with ‘other’ or ‘unknown’ grade excluded from analysis
Table 4.4 Prevalence of malnutrition by NET site
T0 T6
N Malnourished, n (%) N Malnourished, n (%)
Small intestine 27 7 (26) 23 5 (22)
Pancreas 21 6 (29) 17 1 (6)
Other 10 4 (40) 6 0 (0)
All 58 17 (29) 46 6 (13)
Notes.
Malnourished, PG-SGA score B or C
‘Other’ included those with colon and unknown GI NET primary

83
At recruitment (T0) a higher proportion of participants diagnosed with neuroendocrine
carcinoma (NEC) Grade 3 were malnourished compared to NET Grade 1 or 2 (Table 4.3
and Table 4.4). Three participants with a NEC G3 of the colon, and one participant with
NEC G3 of unknown gastrointestinal site were malnourished at T0, but they were
withdrawn later in the study due to death or transfer to palliative care. This would
have impacted the data available for ‘NEC G3’ and ‘Other’ NET site at T6 and may
explain the low prevalence of malnutrition in those sub-groups at T6. There was a
reduction in the prevalence of malnutrition among participants with a pancreatic NET
(13%) at T6. Of the 10 participants who were malnourished at T0/T2 but had improved
nutritional status (well-nourished) by T6, six underwent PRRT during the study and
four underwent surgery during the study period. All participants who were
malnourished at T6 (n-6) were undergoing active treatment (n= 6 on SSA; n=2
underwent surgery; n = 1 receiving radiotherapy, n=1 receiving PRRT). Statistical sub-
analysis of these results was not performed due to low sample size of sub-groups.
4.4.3 Weight change
Participants weight change over the study period, using all available data, is presented
in Table 4.5. Weight change of participants with complete data at all-time points
(n=23) is presented in Table 4.6.
Table 4.5 Weight change over-time for all participants (values are counts and
percentages)
T2-T0
N = 45
T4-T0
N = 37
T6-T0
N = 44
Stable 12 (27) 2 (5) 7 (16)
Gain 13 (29) 16 (43) 16 (36)
Loss – any 20 (44) 19 (51) 21 (48)
>5% loss 8 (18) 4 (11) 9 (20)

84
>10% loss 2 (4) 2 (5) 5 (11)
Notes.
Weight gain, defined as increase of >0.8% body weight; Weight loss, defined as decrease of >0.8% body weight
Table 4.6 Weight change over-time for participants with complete data, N=23
(values are counts and percentages)
T2-T0 T4-T0 T6-T0
Stable 6 (26) 1 (4) 3 (13)
Gain 8 (35) 10 (44) 8 (35)
Loss – any 9 (39) 12 (52) 12 (52)
>5% loss 7 (30) 3 (13) 7 (30)
>10% loss 1 (4) 3 (13) 3 (13)
Notes.
Weight gain, defined as increase of >0.8% body weight; Weight loss, defined as decrease of >0.8% body
weight
Weight loss was prevalent throughout the study period. The proportion of participants
with stable weight reduced over-time, with a third (36%) gaining weight and half (48%)
losing weight by T6. One in five participants had clinically significant weight loss of >5%
body weight and 11% had lost >10% body weight by T6. Of the participants that had
complete data sets at the end of the study, 12 progressively lost weight and seven
progressively gained weight throughout the study period. Of the participants with data
available at both T0 and T6 (n=36), 16 had progressive weight loss from T2 onwards.
Of the participants that had recorded weight loss or gain over-time, median values are
presented in Table 4.7. Both the mean weight loss and mean weight gain of
participants increased by T6, but the degree of weight change varied amongst
participants.

85
Table 4.7 Percent body weight change over-time of participants with weight loss or gain
T2-T0 T4-T0 T6-T0
Median IQR Min Max Median IQR Min Max Median IQR Min Max
Loss, % 2.3 1.5, 6.5 0.8 12.6 2.6 1.9, 4.9 0.9 13.9 4.7 1.9, 7.6 0.8 21.2
Gain, % 2.1 1.0, 4.9 0.8 11.8 4.3 2.2, 5.7 1.1 23.1 5.9 2.1, 10.2 0.9 27.5

86
Eleven participants reported intentional weight change over the study period, mostly
in relation to weight gain. Two participants reported intentional weight loss; one at T0
(8% body weight) and one at T6 (5% body weight). The median weight loss of
participants was below 5% body weight at all time-points (Table 4.7). Of the 10
participants who lost more than 5% of their body weight by T6, the degree of weight
loss ranged between 5-21%. One participant with a Grade 2 small intestinal NET
undergoing PRRT and SSA treatment lost 17% of their body weight by T6, and another
participant with a small intestinal NET (unknown grade) who underwent surgery and
SSA treatment, lost 21% of their body weight by T6.
A high degree of weight gain, 14% and 27% body weight, was recorded for two
participants who were both on SSA treatment; the first had a Grade 2 small intestinal
NET and underwent surgery between T0 and T2, the second had a pancreatic NET of
unknown grade and underwent PRRT throughout the study period.
Six participants recorded weight loss of 5% body weight or above by T6 but were
assessed as well-nourished (PG-SGA A). Upon further examination of the PG-SGA
scoring, these participants had either minimal or stabilised weight loss in the two-
month period between T4 and T6 (2% body weight or less) and had reported good oral
intake, suggesting an acute shift from a catabolic to anabolic state. An anabolic state is
optimal for protein synthesis and maintenance of lean/muscle mass (Langer, Hoffman
and Ottery, 2001; Jager-Wittenaar and Ottery, 2017).
4.4.4 Body composition
A majority of participants had a clinically significant change (classified as gain or loss of
at least 0.5kg) in their fat-free mass (FFM) over the study period (Table 4.8).

87
Table 4.8 Change in fat-free mass over-time (values are counts and valid
percentages)
T2-T0
N = 44
T4-T0
N = 36
T6-T0
N = 42
Stable 14 (32) 5 (14) 5 (12)
Gain 9 (20) 11 (31) 11 (26)
Loss 21 (48) 20 (56) 26 (62)
The degree of FFM loss over-time is presented in Table 4.9. At T6, 62 (62%)
participants had lost FFM (Median=1.9kg, IQR=0.9, 4.5), and 11 (26%) had gained FFM
(Median=1.5kg, IQR=0.7, 2.4).
Table 4.9 Median fat-free mass loss over-time
T2-T0 T4-T0 T6-T0
Median IQR Min Max Median IQR Min Max Median IQR Min Max
Loss, kg
1.6 0.8, 3.6
0.5 5.8 1.0 1.1, 4.0
0.5 8.4 1.3 1.3, 4.6
0.5 6.7
Available FFM data at T6 was compared against weight data at T6 (N=41). At T6, 15
(36%) participants recorded loss of both FFM and weight, 6 (15%) participants
recorded gain of both FFM and weight. Eleven (27%) participants recorded loss of FFM
by T6 (range: 0.5-5.3kg) but stable/gain in weight, indicating a reduction in lean body
mass and deconditioning over-time despite no change in their overall weight. Of this
subgroup, 9 of 11 had either Grade 1 or Grade 2 NET, and eight of 11 had received
treatment (surgery (n=2), SSA (n=4) or PRRT(n=4)) during the study period. Five (12%)
participants recorded gain of FFM (range: 0.7-2.5kg) but loss of weight indicating
preserved lean body mass in these cases.

88
4.4.5 Dietary change
Dietary change as a result of NET diagnosis was reported by over half of participants (n
= 34, 56%) at recruitment, and remained prevalent throughout the study period (58%,
n = 26 at T2; 54%, n = 20 at T4 and 53%, n = 25 at T6). Figure 4.1 summarises the meal
pattern changes of participants that reported dietary change. Figure 4.2 summarises
the food or drinks that participants reported to avoid or reduce. The foods and drinks
most likely reduced at T0 were alcohol (56%), red meat (32%), milk (21%), bread (21%),
and nuts (18%). At T6, a higher proportion of participants were avoiding yoghurt (28%),
coffee (24%), cheese (20%) and fruit (20%). Participants also reported additional food
types that they had reduced that were not listed in the study survey (Table 4.10).

89
Notes.
Avoid foods, patient avoids any food types; avoid drinks, patient avoids any drink types
Figure 4.1 Meal pattern changes as a result of NET diagnosis (values are percentages)
Figure 4.2 Food and drink reduced as a result of a NET diagnosis (values are
percentages)
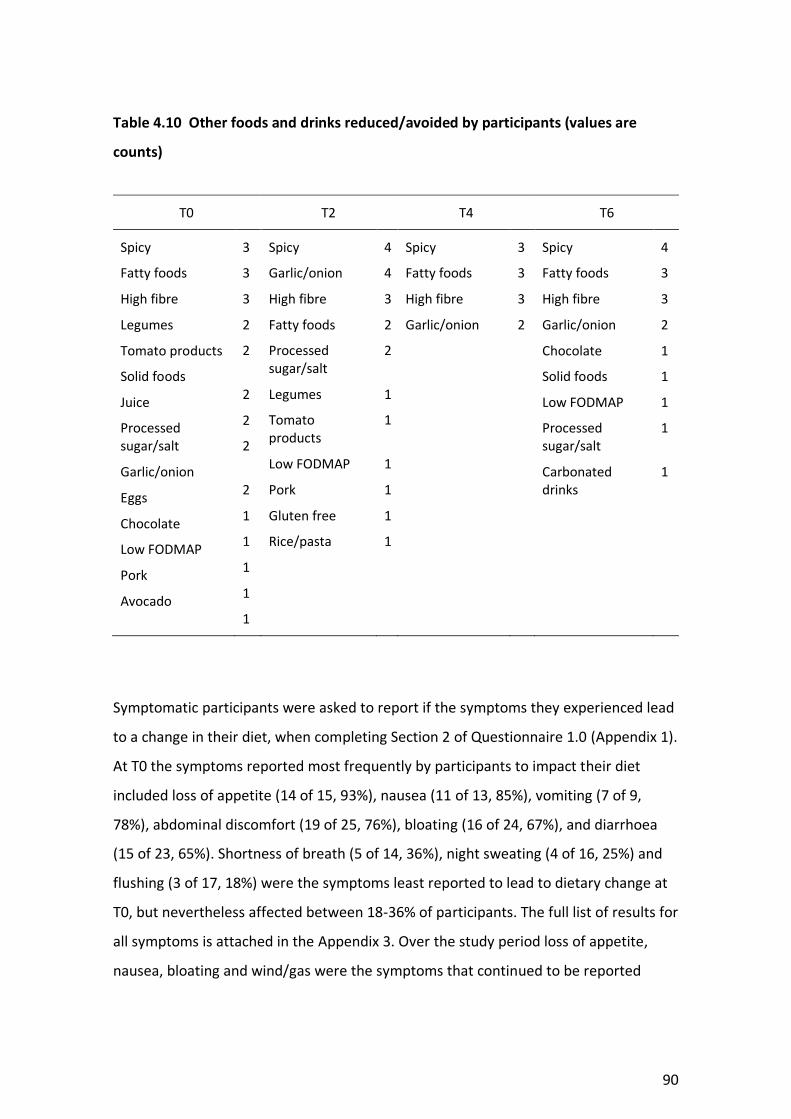
90
Table 4.10 Other foods and drinks reduced/avoided by participants (values are
counts)
T0 T2 T4 T6
Spicy
Fatty foods
High fibre
Legumes
Tomato products
Solid foods
Juice
Processed sugar/salt
Garlic/onion
Eggs
Chocolate
Low FODMAP
Pork
Avocado
3
3
3
2
2
2
2
2
2
1
1
1
1
1
Spicy
Garlic/onion
High fibre
Fatty foods
Processed sugar/salt
Legumes
Tomato products
Low FODMAP
Pork
Gluten free
Rice/pasta
4
4
3
2
2
1
1
1
1
1
1
Spicy
Fatty foods
High fibre
Garlic/onion
3
3
3
2
Spicy
Fatty foods
High fibre
Garlic/onion
Chocolate
Solid foods
Low FODMAP
Processed sugar/salt
Carbonated drinks
4
3
3
2
1
1
1
1
1
Symptomatic participants were asked to report if the symptoms they experienced lead
to a change in their diet, when completing Section 2 of Questionnaire 1.0 (Appendix 1).
At T0 the symptoms reported most frequently by participants to impact their diet
included loss of appetite (14 of 15, 93%), nausea (11 of 13, 85%), vomiting (7 of 9,
78%), abdominal discomfort (19 of 25, 76%), bloating (16 of 24, 67%), and diarrhoea
(15 of 23, 65%). Shortness of breath (5 of 14, 36%), night sweating (4 of 16, 25%) and
flushing (3 of 17, 18%) were the symptoms least reported to lead to dietary change at
T0, but nevertheless affected between 18-36% of participants. The full list of results for
all symptoms is attached in the Appendix 3. Over the study period loss of appetite,
nausea, bloating and wind/gas were the symptoms that continued to be reported

91
frequently as impacting on diet. Vomiting at T4 and T6 was less frequently reported to
impact diet, which may be partially due to the reduced prevalence of vomiting among
the study sample, and the medical intervention available to manage it.
4.4.6 Vitamin status
A total of 24 (41%) and 14 (30%) participants, at T0 and T6 respectively, consented to
24-hour urine collection for measurement of niacin status. Participants declined a 24-
hour urine collection due to logistical issues including the burden of collection or
returning the collection to the study site. At T0, 56 participants (95%) consented to a
blood test to measure serum vitamin levels (vitamins D, E, A, B12, Folate and Iron); and
at T6, 39 participants (83%) consented to a blood test for repeat testing of serum
vitamin levels. After testing, serum vitamin levels were unavailable in some cases due
to laboratory processing error; vitamin A and E (n = 6 at T0, n = 2 at T6), vitamin D (n =
2 at T0), vitamin B12 and folate (n = 1 at T0).
At T0 and T6 respectively, 15 (27%) and 11 (29%) participants were assessed as vitamin
D deficient. Prevalence of other vitamin deficiencies was low in this study (Table 4.11).
Three participants were deficient in both vitamin D and vitamin A at T0. Two of the
three had a NEC G3 and had received treatment with an SSA. The majority of
participants assessed as deficient in one or more vitamins were not taking vitamin
supplements. Some participants had elevated vitamin E (n=11, range: 38-49 at T0; n=9,
range: 41-47 at T6) and elevated vitamin A (n=13, range: 2.4-4.4 at T0; n=12, range:
2.4-3.1 at T6).

92
Table 4.11 Prevalence of vitamin deficiency amongst participants
Vitamin deficiency
T0 T6
n (%) n (%)
Niacin 2 (8)a 0 (0)
Vitamin D
Mild
Moderate
11 (20)
4 (7)
10 (26)
1 (3)
Vitamin E 0 (0) 0 (0)
Vitamin A 3 (6) 1 (2)
Vitamin B12 3 (5) 2 (4)
Folate 1 (2) 0 (0)
Iron 2 (4) 0 (0)
Notes.
a1 result borderline (niacin ratio = 1.0)
4.4.7 Medication use
Use of vitamin supplements was prevalent amongst participants with 26 (44%) taking
vitamin supplements and 10 (17%) taking more than one vitamin supplement at T0.
Vitamin supplementation usage continued throughout the study (n = 18 at T2, n = 16
at T4, n = 22 at T6). Nine (19%) were taking more than one vitamin supplement at T6.
The most commonly consumed vitamin supplement was vitamin D (n = 15 at T0; n = 8
at T2; n = 10 at T4; n = 14 at T6) and a multivitamin supplement (n = 5 at T0, n = 3 at
T2, n = 6 at T4, n = 7 at T6). Vitamin supplements consumed less frequently included
vitamin B12, vitamin B1, iron, vitamin K, zinc, calcium. One participant was taking
niacin (vitamin B3) and another participant was taking vitamin A and E.

93
Participant use of vitamin supplements was compared against results for vitamin
deficiency. The majority of participants (90% at T0, 72% at T6) assessed as deficient in
one or more vitamins were not taking vitamin supplements. At T0, one of 15
participants who were assessed as vitamin D deficient was taking a vitamin D
supplement, and one of two participants who were assessed as niacin deficient was
taking a niacin (B3) supplement. At T6, three of 11 participants who were assessed as
vitamin D deficient were taking a vitamin D supplement.
Seven participants used herbal or alternative medicines throughout the study period.
Herbal and alternative medicines consumed included hemp seed oil, medicinal
cannabis, mutton bird oil, herbal teas (valerian root, fennel, marigold), milk thistle,
blushwood berry, turmeric and maca. Other medications frequently used by
participants included creon (n = 6, gastrostop (n = 6), probotics (n = 6 throughout
study), anti-emetics (n=5), questran lite (n=1).
4.4.8 Dietitian contact
The proportion of participants that had recent consultation (in the month prior to data
collection) with a dietitian over the study period varied; T0, n=13 (22%), T2: n=11
(24%), T4: n=6 (15%), T6: n=8 (17%). The most common location of dietitian contact
was hospital (n=10, 77% at T0; n=11, 100% at T2; n=6, 100% at T4; n=6, 75% at T6),
followed by private clinic (T0: n=2, 8%; T6: n=2, 25%). The source of the dietitian
referral was mostly reported to be a doctor (n = 7, 54% at T0; n = 4, 50% at T6). Three
participants reported requesting a dietitian appointment themselves at T6. Six and
three participants at T2 and T4 respectively, were referred for dietitian assessment by
the research team after completion of the PG-SGA for study purposes showed
presence of malnutrition. The main reason for consultation with a dietitian varied over
the study period and included ‘losing weight’ (25-81%), ‘to talk about diet’ (13 -17%),
and ‘to manage symptoms’ (9-17%).

94
4.5 Discussion
This chapter has presented data on the nutritional complications of patients diagnosed
with a GEP NET after commencing medical treatment at a specialist NET referral
hospital, and across the study period. The study population was heterogeneous, and
the participant sample included patients diagnosed with varied NET Grades and
primary tumour site. The majority of participants were within six months of their GEP
NET diagnosis and had a body mass index within a healthy or overweight range at
commencement of the study.
The study results demonstrate that malnutrition is prevalent among people diagnosed
with a NET, along with clinically significant weight and loss of FFM. One fifth of
participants lost 5% or more of their body weight over the six-month study period, and
more than 10% of participants lost 10% or more of their body weight over this same
period. Three participants had a large degree of weight loss of over 15% body weight
during the study period indicating some NET patients are at risk of clinically significant
weight loss and decline in nutritional status. Weight loss above 5% body weight is
considered clinically significant and can contribute to malnutrition risk (Jensen et al.,
2019). The recently published Global Leadership Initiative on Malnutrition (GLIM)
criteria for the diagnosis of malnutrition recommends consideration of phenotypic and
etiological factors when diagnosing malnutrition (Jensen et al., 2019). The presence of
at least 1 of 3 phenotypic criteria (non-volitional weight loss – above 5% over 6
months, low body mass index, and reduced muscle mass) and 1 of 2 etiological criteria
(reduced food intake, and inflammation or disease burden) is required for a diagnosis
of malnutrition (Jensen et al., 2019). The prevalence of more than 5% and 10% weight
loss in this study suggests it is one of key phenotypes contributing to malnutrition
diagnosis in a NET population.
Malnutrition in cancer patients has been associated with increased risk of infection,
hospital length of stay and overall morbidity (Nitenberg and Raynard, 2000; J. Arends
et al., 2017; Marshall et al., 2019). In people diagnosed with a NET, malnutrition has

95
been associated with prolonged length of stay and reduced survival (Maasberg et al.,
2017). This highlights the importance of malnutrition identification and management,
in order to manage subsequent complications and improve quality of life for patients.
The degree of weight loss observed among participants in this study highlights that
weight loss and malnutrition identification should be a priority among patients
diagnosed with a GEP NET.
The proportion of participants that lost weight was greater than the proportion
assessed as malnourished using the PG-SGA in this study. This was because the amount
of weight loss between T4 and T6 for some patients was minimal (below 2%), and for
others, their weight had begun to stabilise in the month prior to their T6 assessment
indicating transition to an anabolic state. In combination with a report of good food
intake, these factors are likely to contribute to an assessment of ‘well-nourished’ on
the PG-SGA. The prevalence of malnutrition in this study at recruitment/T0 (29%), and
T2 (27%), was comparable to other published studies in NET populations reporting a
malnutrition prevalence of 25% and risk of malnutrition in 14-38% (Qureshi et al.,
2016; Maasberg et al., 2017; Borre et al., 2018). The rate of malnutrition in this study
reduced over-time to 13% at T4 and T6, which could be due to a number of factors.
Some malnourished participants were withdrawn during the study period due to death
or transfer to palliative care. The majority of participants were newly diagnosed at
recruitment, so their nutritional status potentially improved over-time once they
received the appropriate medical care and NET treatment, which was observed in the
case of participants with a pancreatic NET. When examining participant data available
at both T0 and T6, there were a higher proportion of participants whose nutritional
status improved over the six-month study period (21%) than those whose nutritional
status declined (7%), supporting this hypothesis. The sample size was only sufficiently
powered to detect evidence of large-sized differences in nutritional status over-time. A
reduction to 13% after six-months of NET treatment is potentially clinically significant
and may highlight the impact of medical management and NET treatment in
supporting improvement in nutritional status.
96
The malnourished participants that were withdrawn due to death or palliative care
were all undergoing chemotherapy as their main NET treatment. Three of the four
participants had a diagnosis of Grade 3 NEC and three of four participants had a
primary NET of the colon. Results indicate that chemotherapy treatment, Grade 3 NET
and primary colon NET may be risk factors for malnutrition and nutritional decline,
which is consistent with previously published cross-sectional research (Maasberg et al.,
2017). Data from the Phase 1 study however, was not powered to statistically detect
an association between malnutrition and NET disease grade, and treatment
characteristics. The cross-sectional observational study of 203 NET patients by
Maasberg et al. (2017) reported an overall malnutrition prevalence of 25% using the
Subjective Global Assessment (SGA), and found that NET patients with a high-grade
(G3) NET, progressive disease, or undergoing chemotherapy were at a high risk of
malnutrition associated with a poorer outcome (Maasberg et al., 2017). Another cross-
sectional study by Qureshi et al. (2016) found 14% of participants with a GEP NET were
at risk of malnutrition (Qureshi et al., 2016). Those at greater risk of malnutrition in the
study by Qureshi (2016) were identified as patients with GEP NET undergoing SSA
treatment, or with a diagnosis of a colon or unknown primary tumour site (Qureshi et
al., 2016). Apart from similarities in the characteristics of malnourished participants
that were withdrawn from the PhD study due to death and medical deterioration,
there was no consistencies in the disease or treatment characteristics of participants
with malnutrition and declining nutritional status, throughout the study. Six of the 10
participants with improved nutritional status over the six-month study period were
undergoing PRRT treatment, potentially indicating this treatment has a positive impact
on nutritional status in some cases. Only one of the 14 participants undergoing PRRT at
T6 was assessed as malnourished, supporting this theory further. Due to the
longitudinal study design, the Phase 1 findings contribute additional insight and data
for malnutrition prevalence and variation in malnutrition rates among patients with
NETs over-time. This is an important contribution beyond what has been previously
published via cross-sectional research.

97
Maasberg et al (2017) assessed body composition using bioelectrical impedance
analysis (BIA) and found that malnourished patients (SGA score of B or C) had reduced
fat-free mass (Maasberg et al., 2017). In this Phase 1 PhD study, 37% of patients
recorded a loss of both weight and FFM over the study period. This PhD study is the
first to examine prevalence of weight change over-time, concurrently with change in
FFM in patient with GEP NETs. It was also observed that a third of participants at T6 (n
= 11, 27%) had recorded FFM loss despite stable weight or gain. This is an important
finding and indicates the potential for underlying body composition change and muscle
mass deterioration which is independent of total body weight. This PhD research did
not assess muscle mass, only relative changes in fat free mass using BIA. The GLIM
criteria recommending consideration of reduced muscle mass as part of malnutrition
diagnosis were not published at the time of study protocol development. Ideally,
assessment of muscle mass using a validated tool is optimal to aid in diagnosis of
malnutrition. Low muscle mass is associated with functional decline and worsening
morbidity and mortality (Cruz-Jentoft and Sayer, 2019). It can lead to negative
outcomes in people who are a healthy weight, overweight or obese, but is frequently
under-recognised (Barazzoni et al., 2018). There were no similarities found in the
disease and treatment characteristics of participants that had a large degree of weight
loss, and those that lost FFM in this PhD study. These results were likely limited by a
small sample size, and we were therefore unable to observe any clinical or treatment
factors associated with weight loss or body composition change. Weight loss and
muscle mass deterioration if prolonged and severe can lead to malnutrition, increasing
risk of morbidity and reduced survival in cancer patients (J. Arends et al., 2017).
Assessment of both weight change and muscle mass change in GEP NET patients is
therefore very important to identify and thus address these nutritional complications.
Weight gain was also prevalent over the study period, however, no similarities in
disease or treatment characteristics of participants who gained weight were observed.
The weight gain observed in some participants could have been an indicator of
improved nutritional status over-time, due to response to active treatment, or
worsening of overweight or obesity. Obesity is considered protective and has been

98
associated with reduced in-patient mortality in NET patients with abdominal NET
(Glazer et al., 2014). However, due to the indolent nature of some GEP NETs, patients
may be living with the presence of a GEP NET for many years and subsequent
morbidity. Continued weight gain and obesity in GEP NET patients with low-grade or
indolent cancer may therefore contribute to the development of other chronic
diseases such as cardiovascular disease and diabetes. However, the long-term impact
of obesity on patients with a GEP NET has not been studied and is still unknown.
Dietary change was prevalent throughout the study period indicating another
significant nutritional issue potentially under-recognised in this population. Whilst
more than half of participants reported making a change to their diet as a result of
their NET, less than a quarter of participants reported contact with a dietitian
throughout the study period. The main reason for dietitian contact was weight loss,
followed by diet and symptom management which was reported by less than 20% of
participants. Results for dietitian contact may also be over-estimated compared to the
usual GEP NET population, as six participants were referred to the dietitian by the
research team after completion of the PG-SGA found presence of malnutrition.
Therefore, it seems that a large proportion of people diagnosed and treated for a GEP
NET are making change to their diet without consultation with a dietitian. Whilst the
type of dietary change varied among participants, study results indicate that reduced
meal size and food avoidance were frequently reported. Reduced dietary intake and
food avoidance has the potential to lead to dietary inadequacy and nutritional
compromise, including malnutrition, if prolonged. Many of the foods avoided by
participants, including red meat, milk, nuts, yoghurt and cheese, are high in protein
which is an essential nutrient used to support the immune system and cell
repair/growth (Bender, 2014), particularly when undergoing cancer treatment. Severe
food restriction and dietary change also has social implications and may also impact on
patient’s enjoyment of food. The precursors and reasons for high prevalence of dietary
change among GEP NET patients is not known and has not been well explored through
research. Only one small study (n=25) recorded dietary change in a group of GEP NET
patients, and found that gastrointestinal symptoms of diarrhoea and gas contributed

99
to their dietary changes, including avoidance of fermentable carbohydrates and high
fat foods (Lind, Wängberg and Ellegård, 2016). Further research is required to explore
this phenomenon and the association between symptoms and dietary change.
Through a questionnaire posed to participants in the Phase 1 study it was possible to
explore the impact of symptoms on dietary change and results highlight several
symptoms; including loss of appetite, nausea, vomiting, abdominal discomfort,
bloating, diarrhoea, wind or gas and pain that frequently lead to a change in dietary
intake among people with GEP NET. Borre et al. (2018) assessed nutritional risk using
the Nutritional Risk Screening Tool (NRS) and hand-grip strength (HGS) in a cohort of
183 NET patients, and found that symptoms of nausea, vomiting, abdominal
discomfort and loss of appetite were associated with reduced HGS and higher
nutritional risk (high NRS score) (Borre et al., 2018). Results of the PhD study and that
of Borre (2018) suggest that patients diagnosed with GEP NET that are burdened by
particular symptoms such as abdominal discomfort, nausea, wind or gas, bloating and
loss of appetite, should be routinely screened for both dietary change and risk of
malnutrition and if identified, referred to a dietitian for nutritional management. These
symptoms were identified as prevalent and burdensome for GEP NET patients who
took part in the Phase 1 study, as described in Chapter 3 Section 3.4.3. Symptoms of
fatigue, bloating, and abdominal discomfort remained prevalent among participants
throughout the study period indicating their potential to continuously impact on
nutrition intake over-time. Results for dietary change show a broad range and
variation of food and drink types avoided by GEP NET patients, and this potentially
indicates a need for individualised assessment of dietary change to ensure diet is
nutritionally adequate, and that dietary change is evidence-based and managed
appropriately. Further research is required to determine the factors that prompt
dietary change among GEP NET patients, and the impact of dietary change on
nutritional status and HRQoL. Chapter 5 presents insights from a series of qualitative
interviews conducted with participants enrolled in the Phase 1 study, exploring factors
relating to nutritional issues and dietary change and their impact on HRQoL.

100
Use of vitamin supplements was prevalent amongst study participants, in particular
use of vitamin D and multivitamin supplements. Whereas, the use of herbal and
alternative medicines was relatively low, compared to previous literature which has
reported a third of NET patients use complimentary medicines (Borre, Dam and
Grønbaek, 2019). This may be due to the fact that the majority of participants were
newly diagnosed (within 6 months), and therefore may not have considered use of
alternative medicines; compared to the study by Borre et al (2019) which was cross-
sectional and recruited NET patients at varying stages of diagnosis. In contrast to the
other nutritional issues described in this group of GEP NET patients, the prevalence of
vitamin deficiency was low. These results may be in part be explained by the high
refusal rate of vitamin testing, particularly for niacin, and also due to the majority of
participants being within six months of diagnosis at commencement of the study and
therefore too early in their NET treatment to develop vitamin deficiencies. Some
participants also recorded high levels of vitamin A and E, highlighting variability in
serum vitamin levels amongst the study population. Serum measurement of these
vitamins, however, is not considered a reliable indicator of liver stores and presence of
toxicity (Albahrani and Greaves, 2016). GEP NET patients most at risk of vitamin
deficiencies as identified in previous studies, includes patients on long-term SSA
treatment (over 18 months) who are at risk of fat-soluble vitamin deficiency; patients
with serotonin-producing small intestine NET and carcinoid syndrome, who are at risk
of niacin deficiency; and patients post-bowel surgery, who are at risk of vitamin B12
deficiency (Shah et al., 2005; Fiebrich et al., 2010; Lind, Wängberg and Ellegård, 2016).
Due to limited data available for vitamin testing in the study, it was likely there were
insufficient numbers of patients meeting the above criteria to demonstrate the
presence of vitamin deficiency in those groups. The majority of participants who were
assessed with a vitamin deficiency at T0 and T6 were not consuming a supplement or
being treated for the deficient vitamin. The use of vitamin supplements was recorded
at the same time of vitamin testing, and prior to test results. It was therefore not
possible to record commencement of vitamin supplementation after results of vitamin
testing at T6. If a participant was found to be deficient in a vitamin their treating

101
doctor was informed. Vitamin deficiencies would have potentially been unrecognised if
participants weren’t involved in the study. If un-recognised and un-treated, prolonged
vitamin deficiency can lead to severe clinical syndromes and complications; for
example Pellagra (niacin deficiency) can lead to clinical symptoms of diarrhoea, altered
conscious state and confusion (dementia), and death in severe cases (Castiello and
Lynch, 1972; Bender, 1983). Hence early identification and intervention for such
vitamin deficiencies would ensure appropriate treatment and reduction in risk of these
complications. Results for vitamin deficiency in this Phase 1 study were variable, and
therefore do not support the need for routine testing of potential at-risk vitamins such
as niacin and fat-soluble vitamins. Further research is required to investigate and
confirm the prevalence of vitamin deficiency in patients with a GEP NET; particularly in
those treated long-term with SSA and diagnosed with a serotonin-producing NET,
which are highlighted as groups at risk of vitamin deficiency by previous studies (Shah
et al., 2005; Fiebrich et al., 2010; Lind, Wängberg and Ellegård, 2016; Robbins et al.,
2018).
The moderate-to-high prevalence of dietary change, weight loss, and FFM loss among
participants in this study highlight the extent of nutrition issues among GEP NET
patients. Current NET clinical practice guidelines provide little advice on appropriate
identification and assessment of malnutrition and other nutrition issues. The PG-SGA,
used in this study, is validated for use in cancer populations and considered a semi-
gold standard of nutritional assessment (Jager-Wittenaar and Ottery, 2017; Keller et
al., 2020), incorporating all phenotypic and etiologic components of the GLIM criteria
(Jensen et al., 2019). In practice, health professionals may perform nutrition screening
to determine which patients are at risk of malnutrition and require a comprehensive
nutrition assessment using a tool such as the PG-SGA. Current nutrition screening tools
validated in cancer populations include the Malnutrition Screening Tool (MST),
Malnutrition Universal Screening Tool (MUST) and Nutrition Risk Screening Tool (NRS-
2002) (Bauer et al., 1997; Kondrup et al., 2003; Boléo-Tomé et al., 2012). These
screening tools focus on identification of weight loss, change to total food intake, and
identification of contributing acute disease factors such as surgery, or requirement for
102
intensive care (leading to no nutritional intake for >5 days), in the case of the NRS-
2002. In NET patients, common nutrition-related issues such as symptom burden and
dietary changes, may contribute to nutritional risk, but may not be identified using
current available nutrition screening tools. The applicability and validity of current
nutrition screening tools therefore requires further detailed exploration in a GEP NET
population. The PG-SGA Short Form (PG-SGA SF) may be a suitable nutrition screening
tool for GEP NET patients, as it incorporates the first four questions of the PG-SGA,
including change in amount of food intake, change in energy and daily function,
change in weight and symptoms impacting diet (Gabrielson et al., 2013), which are
factors relevant to nutritional risk in GEP NET patients as found in the Phase 1 study.
The PG-SGA SF has been shown to be a practical and valid nutrition screening tool in
oncology outpatients (Gabrielson et al., 2013; Abbott et al., 2016). Potential symptoms
included in the PG-SGA SF that may be relevant to GEP NET patients include diarrhoea,
pain, loss of appetite and fatigue. The question addressing food intake, is designed to
identify change in total food intake but not detailed changes of food restriction or
avoidance of particular food types, which were identified as common dietary changes
observed in GEP NET patients in our Phase 1 study. Review of current valid nutrition
screening tools and their suitability for use in patient with GEP NETs is recommended.
The development of a NET-specific supplement to combine with existing nutrition
screening tools may also need to be considered, if existing validated tools are unable
to capture NET-specific nutrition risks such as dietary change and restriction.
Commonly used nutrition screening tools have been demonstrated to under-diagnose
the presence of muscle wasting, sarcopenia and cancer cachexia when compared with
computed tomography, a gold standard technique for assessment of muscle mass (Ní
Bhuachalla et al., 2018). In data from the Phase 1 study, FFM loss was identified among
several participants who had stable weight and an assessment of well-nourished on
the PG-SGA, indicating deterioration in muscle mass is an underlying and unrecognised
problem in some cases. Clinicians should consider assessment of muscle mass in their
practice using validated body composition measures (BIA, ultrasound, computed
tomography (CT) or magnetic resonance imaging (MRI)) where available, in order to

103
assess underlying muscle mass changes, which is a concept supported by the recently
published GLIM criteria (Jensen et al., 2019). Assessment methods such as BIA, calf
circumference and the subjective muscle mass assessment on the PG-SGA, may be
more accessible and therefore suitable measures to be used in routine clinical practice
by health professionals, in comparison to the use of CT body composition analysis and
MRI. Validated assessment of muscle mass change would be particularly useful to
identify nutritional compromise in patients on prolonged treatment and those
reporting restricted diets, without evidence of overall body weight loss.
4.6 Conclusion
This is the first study to comprehensively assess the occurrence of nutritional
complications over-time among GEP NET patients, concurrently with the dietitian
intervention received. Study results show that malnutrition and nutritional
complications are prevalent but under-recognised among people diagnosed with a GEP
NET. Nutritional complications including weight loss, reduction in FFM and dietary
change are more prevalent than malnutrition, and under-recognised when using
available validated cancer nutrition assessment tools. More than half of the GEP NET
patients in this study reported a dietary change due to their diagnosis and symptoms,
but the precursor to this dietary change and the impact on nutrition and quality of life
requires further evaluation through qualitative methods. The prevalence of vitamin
deficiency was low in this study and larger multi-site trials are required to explore the
risk and prevalence of vitamin deficiency among GET NET patients. Nutritional
complications in GEP NETs are likely multi-factorial, due to the heterogeneous
population and high burden of symptoms. Under-recognition of nutritional
complications can lead to worsening morbidity and HRQoL for patients. Results
highlight the need to determine an appropriate method of screening and identification
of nutritional complications among and specific to GEP NET patients. Further
exploration of the impact of nutritional complications on the HRQoL of patients is also
required. Chapter 5 will consider insights from qualitative interviews completed with a

104
purposive sample of participants from the Phase 1 study and provide an in-depth
description of the occurrence and impact of nutritional issues on HRQoL.

105
Chapter 5: Living with a NET and the impact on nutrition
This chapter describes the aims, methods and insights from qualitative interviews
undertaken with patients within the context of the Phase 1 mixed methods study.
5.1 Introduction
The results of the Phase 1 longitudinal study presented in Chapters 3 and 4 showed
that social function and mental health are negatively impacted by a NET and its
treatment, and also that nutritional complications including weight loss, malnutrition
and dietary change are prevalent. Quantitative data showed that whilst dietary
changes were common, the nature of dietary changes (smaller meals, increased
frequency of eating, avoidance of specific food and drink types) varied amongst
participants. In this chapter, interview data from a purposive sample of Phase 1
participants, provides in depth insight to the types of dietary changes participants
engaged in, reasons why they altered or changed their diets in the way that they did,
and the impact of these changes on their HRQoL. There has been little exploration of
dietary habits among patients living with a NET, and although findings from a series of
small cross-sectional observational studies (Davies and Caplin, 2009; Lind, Wängberg
and Ellegård, 2016; Gallo et al., 2017; Barrea et al., 2018) indicate a similar presence of
dietary change to that described by participants in this study (phase 1), they provide
limited insight to types of changes made by people in response to their disease and
treatment, factors leading to those changes and whether the changes impact people’s
perceptions of their nutritional status and HRQoL.
An important aim of this component of the PhD study was to generate a new
understanding of the changes patients made to their dietary intake, their perceptions
of their nutritional status and symptoms experienced, and the perceived impact of
these on HRQoL. The extent of nutrition advice and intervention received to help
address nutritional issues was also explored to help contextualise patients’ responses
to the impact of nutritional issues. In order to address these aims, a purposive sample
106
of Phase 1 participants were invited to take part in two semi-structured, audio-
recorded interviews at entry to the study and at six month follow up.
5.2 Aims and objectives
5.2.1 Aim
To explore and describe the experiences of people living with a GEP NET, to better
understand the impact of disease and treatment-related nutritional and dietary
changes on HRQoL.
5.2.2 Objectives
1. To explore and describe how and whether NET and treatment-related nutritional
changes impact peoples’ HRQoL
2. To explore and describe whether nutrition needs (nutritional status and dietary
intake patterns) change after a diagnosis of NET
3. To explore and describe what help (if any) participants reported receiving from
clinicians regarding their nutrition issues
5.3 Methodology
The interviews were undertaken within the context of the Phase 1 mixed-methods
study (Chapter 2). They were undertaken to ensure opportunity for patients to
describe their experiences of nutritional changes and impacts through interviews,
offering rich insights to complement the Phase 1 quantitative data. The research
perspective underpinning this qualitative data component was realist, that is, the
intent was to provide participants with an opportunity to report their personal
experience, of nutritional complications and what this meant for them in their unique
contexts.

107
An exploratory, descriptive approach was used to inform the qualitative study. As
described by Braun and Clarke (2006), an exploratory, descriptive approach is used to
generate data when a person describes their reality and experience of a specific event
or occurrence, in their own words (Braun and Clarke, 2006). As such the approach
aligned with the realist perspective underpinning the study. An exploratory, descriptive
approach enables focus on topics of interest, explored through tailored or targeted
interview questions; i.e. in this study, the experience of participants in regard to
nutritional complications (dietary change, weight change), HRQoL and access to
nutrition information. These insights were considered important to guiding future
interventional research and patient-centred, educational and preparatory information
solutions.
Data were generated through semi-structured interviews. A semi-structured format
was chosen to focus participant responses towards topics of interest (nutrition, dietary
change and HRQoL), but also so as not to restrain discussion of their experience and
issues of importance to them. Interviews were chosen to explore individual patient
experience, acknowledging that this could be different due to specific disease and
treatment factors, personal beliefs or social influences. For this reason, individual
interviews were chosen as the data collection method of choice over other qualitative
data collection approaches, for example, focus group.
A thematic content analysis approach was applied to the data generated (following
Braun and Clarke) allowing for identification of unique and shared experiences across
the participant interviews, and details of the processes undertaken are described
below.
The context of the qualitative patient interviews within the Phase 1 study is
demonstrated in Figure 5.1.
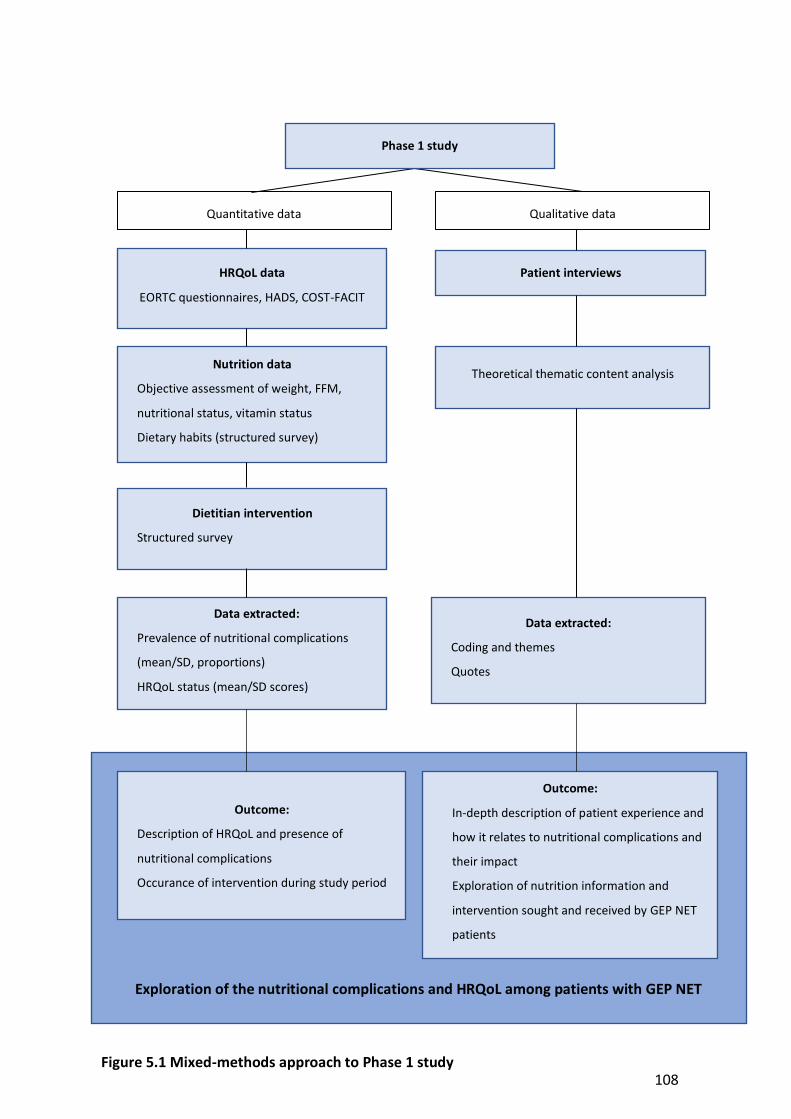
108
Dietitian intervention
Structured survey
HRQoL data
EORTC questionnaires, HADS, COST-FACIT
Nutrition data
Objective assessment of weight, FFM,
nutritional status, vitamin status
Dietary habits (structured survey)
Quantitative data Qualitative data
Patient interviews
Data extracted:
Prevalence of nutritional complications
(mean/SD, proportions)
HRQoL status (mean/SD scores)
Data extracted:
Coding and themes
Quotes
Theoretical thematic content analysis
Exploration of the nutritional complications and HRQoL among patients with GEP NET
Outcome:
Description of HRQoL and presence of
nutritional complications
Occurance of intervention during study period
Outcome:
In-depth description of patient experience and
how it relates to nutritional complications and
their impact
Exploration of nutrition information and
intervention sought and received by GEP NET
patients
Phase 1 study
Figure 5.1 Mixed-methods approach to Phase 1 study

109
5.4 Methods
5.4.1 Recruitment and sampling
A purposive sample of participants who had consented to take part in the Phase 1
study were invited, at time of recruitment, to take part in two semi-structured, audio-
recorded interviews - one at recruitment and another six-months later. A purposive
sampling method was used for two reasons: to ensure a diverse representation of
participant experiences as part of the interview data, and to focus on inclusion of
participants from the Phase 1 study that had reported making a dietary change as a
result of their NET diagnosis. Where possible, it was intended to achieve diversity with
regard to participant demographics, diagnosis, and treatment type; which enabled a
heterogeneous sample representative of the NET population. A benefit of purposive
sampling in qualitative research is identification of individuals or groups that have
experience with or are knowledgeable about an aspect of interest to the research
question (Patton, 2015). In the case of these interviews, the focus was to explore
patient experience in regard to nutritional issues and dietary change, therefore it was
considered important to ensure sampling of participants that reported making a
dietary change during the Phase 1 quantitative questionnaires. Therefore, participants
who reported making a dietary change due to their NET diagnosis in the Phase 1
questionnaire, 1.0 Section 2.0 (details in Chapter 2, Section 2.5.11), were approached
to consider taking part in the interviews. A maximum of 15 interviews were intended
to be completed based on evidence that data saturation (where no new themes
emerge from interviews) commonly occurs after 10-12 interviews (Creswell, 2007).
Interviews were undertaken six months apart, to explore whether participants
described different experiences over time, after medical management and treatment
at a specialist NET referral hospital.
Eligible patients were approached to participate in an interview by the lead researcher
(PhD student) after completion of baseline data collection for the Phase 1 study.
Responses to Questionnaire 1.0 Section 2.0 was checked prior to determine the
patient’s eligibility for an interview. It was explained that consent to the interview at

110
baseline would also mean consent to participate in a repeat interview in six-months
(although this was verbally re-checked at the six month interview timepoint). Eligible
participants were told interviews were optional and they could continue to participate
in data collection the Phase 1 study if they chose to decline the interview. Verbal
consent was obtained from those willing to participate in an interview at time of
baseline data collection, and a time to complete the baseline interview by phone
within the following two-weeks was scheduled with the participant. Interviews were
audio-recorded.
Interviews were conducted via phone, or in-person at the request of the participant,
within two weeks of initial recruitment to the Phase 1 study for the baseline interview,
and within 2 weeks of the six-month (T6) data collection point for the six-month
interview. All interviews were conducted by the same researcher (PhD student). Verbal
consent was audio-recorded prior to the start of each interview. Ethics approval for
patient interviews was obtained from the Peter MacCallum Cancer Centre Human
Research Ethics Committee (HREC/17/PMCC/7) in April 2017.
5.4.2 Interview questions
A semi-structured interview schedule was developed by the lead researcher (PhD
student) and reviewed by supervisors, one of whom is experienced in qualitative
research methodology. Questions were informed by the teams’ clinical expertise as
well as published evidence available. A total of 12 key questions (with corresponding
prompts) were designed for the first interview, and 11 questions (again with prompts)
for the six-month interview. Questions were structured to prompt discussion of
patients’ experiences in regard to the aims described above in Section 5.2. Interview
questions at six-months were aligned with those at baseline, with language modified
to reflect the period of time that had passed since the previous interview. The
interview schedule is included in Appendix 4. Four questions addressed participant
experience of dietary and nutritional changes and impact on quality of life before and
after their diagnosis, with a focus on symptoms and access to information; two
111
questions addressed emotional health and coping with the diagnosis; and six questions
addressed the impact of the NET diagnosis on nutrition including weight change,
eating, and the extent of nutrition advice and intervention received. Questions were
piloted with two consumers from NeuroEndocrine Cancer Australia (formerly the
Unicorn Foundation), who had a diagnosis of a NET to test clarity and flow of
questioning.
5.4.3 Thematic content analysis
Interviews were audio-recorded and transcribed verbatim by a party external to the
research team. Thematic content analysis as described by Braun and Clarke informed
the approach to data analysis (Braun and Clarke, 2006). The transcripts were read and
re-read to ensure familiarity with the content and to begin to identify recurring themes
or issues raised by participants. Content from individual interviews were initially coded
against interview questions (theoretical approach at semantic level analysis) to identify
recurrent themes common to or unique to individuals across the data sets (at baseline
and at six months). Interview data were coded into data extracts (quotes or lines of
text) by the lead researcher (PhD student) and extracts grouped into emergent
themes. Themes did not necessarily reflect content most commonly talked about, but
rather represented areas of particular relevance to the topic areas of interest for the
research. That is, things were not regarded as important by virtue of how often they
were referred to, but rather by how meaningful they were to participants in response
to questions answered. Interview data were coded against the 12 key interview
questions to enable initial description of content, then further exploration of coded
responses and overall content was conducted to generate themes from the baseline
and six months-interviews. As the same questions were asked at both the interview
time points, themes identified at the first interview were used to guide the six months-
interview questions, but this did not exclude opportunity for new themes to emerge,
or for participants’ changing experiences over time.

112
A cross-section of interviews was independently coded by a supervisor to check inter-
rater reliability across common themes identified. There was minimal inter-researcher
variation in theme recognition at both time points, and all themes were discussed to
ensure consensus.
5.5 Results
5.5.1 Patients
Between September 2017 and August 2018, 12 patients enrolled in the Phase 1 study
who met the criteria for and to achieve the quota for each group within the purposive
sample, were approached to participate in an interview at T0. Eleven patients
consented to an interview, and participant characteristics are summarised in Table 5.1.
There was variation in sex, age, NET site, NET grade and nutritional status of
participants, which met the criteria of the purposive sample. Of the 11 participants
who took part in an interview at T0, nine participated at T6. Reasons for not taking
part in the six-month interview included patient deceased (n=2).
Table 5.1 Participant characteristics (N=11)
Characteristic Value
Age (years), mean 56 (range:29 - 71)
Sex, n
Male 8
Female 3
NET Grade, n
NET G1 3
NET G2 4
NET G3 2
Unknown 2

113
Characteristic Value
NET site, n
Small intestine 6
Pancreas 3
Gastric 1
Unknown 1
Nutritional statusa
A (well nourished) 5
B (suspected/moderate malnutrition)
5
C (severely malnourished) 1
Notes.
aAs calculated by PG-SGA global status score
5.5.2 Insights from the baseline interviews
Four key themes were identified from the baseline interviews. The themes were
uncertainty, complexity, conflicting advice from health professionals, and self-
management/seeking information. For each theme, a number of sub-themes were also
identified. These are presented in Table 5.2, along with quotes to help illustrate each
theme.
Participants reported a variety of symptoms related to their NET, including diarrhoea,
fatigue, pain, flushing, bloating and wind, bowel obstruction and difficulty swallowing,
and altered blood sugar levels. Diarrhoea was a symptom frequently described by
participants to be a significant burden on their day-to-day activities and quality of life.
When asked about how they were coping with their diagnosis, common responses
from participants included ‘fear’, ‘poor quality of life’, ‘draining’, and ‘feel depressed’
and general concern for the impact of their diagnosis on their lives and their family.

114
The impact of a NET on quality of life was frequently reported by participants, partially
in relation to work and the inability to perform their work to the same degree as prior
to diagnosis, which had negative financial impacts as well. The impact of a NET
diagnosis on family and social relationships and activities was reported by some
participants. They reported that family members were burdened by the uncertainty of
a NET diagnosis and observing the patient be unwell or experience symptoms. As a
result, family members often attempted to help by providing nutrition advice or
suggesting dietary modification to help them feel better. Due to various symptoms
experienced by participants; in particular gastrointestinal symptoms such as diarrhoea,
bloating and abdominal cramps/wind; social activities and eating out were restricted
due to fear of experiencing symptoms in public and the limitations of restricted eating
habits.
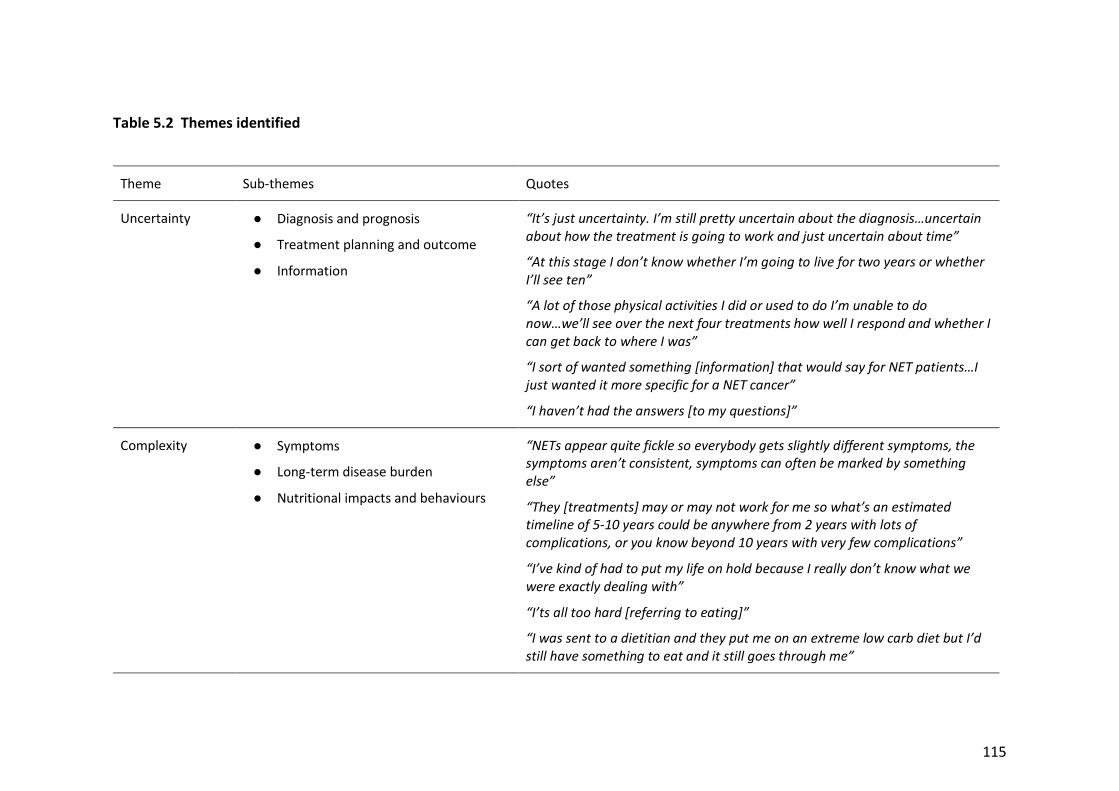
115
Table 5.2 Themes identified
Theme Sub-themes Quotes
Uncertainty ● Diagnosis and prognosis
● Treatment planning and outcome
● Information
“It’s just uncertainty. I’m still pretty uncertain about the diagnosis…uncertain about how the treatment is going to work and just uncertain about time”
“At this stage I don’t know whether I’m going to live for two years or whether I’ll see ten”
“A lot of those physical activities I did or used to do I’m unable to do now…we’ll see over the next four treatments how well I respond and whether I can get back to where I was”
“I sort of wanted something [information] that would say for NET patients…I just wanted it more specific for a NET cancer”
“I haven’t had the answers [to my questions]”
Complexity ● Symptoms
● Long-term disease burden
● Nutritional impacts and behaviours
“NETs appear quite fickle so everybody gets slightly different symptoms, the symptoms aren’t consistent, symptoms can often be marked by something else”
“They [treatments] may or may not work for me so what’s an estimated timeline of 5-10 years could be anywhere from 2 years with lots of complications, or you know beyond 10 years with very few complications”
“I’ve kind of had to put my life on hold because I really don’t know what we were exactly dealing with”
“I’ts all too hard [referring to eating]”
“I was sent to a dietitian and they put me on an extreme low carb diet but I’d still have something to eat and it still goes through me”

116
Theme Sub-themes Quotes
“Just [avoid] fruit, meats and low carb potatoes and things like that. Green veggies and not to eat anything that, you know sweet things like that”
“I’ve eliminated stone fruits and dried fruit and onions and garlic, and all the things I used to love eating”
Conflicting advice ● Limited confidence in health professionals
● Confusion with nutrition messages
“Most GPs never see a NET in their careers”
“I’m not quite sure where I should be going with all of this, you know nutrition wise, what I should and shouldn’t eat”
“I was sent to a dietitian and after a little while they put me on a low carb diet…extreme low carb diet [but] I’d still have something to eat and it still goes through me”
“Nutrition-wise, what I should and shouldn’t eat or what’s best that I do or don’t do. That’s why I’m feeling a bit you know in the air about it at the moment”
“I went to some dietitian who was basically sitting there googling possibilities while we were in the room”
“She just said she didn’t know what advice to offer me and she just gave me a printout on the FODMAP diet”
Self-management and seeking information
● Responsibility to manage own care and information
● Nutrition important to patient
“The more I learnt about NET the more I learned it can have effects on absorption of vitamins and minerals, things like that then yeah they should [offer advice about]”
“I’ve just sort of been self-helping and looked up these discussion boards and they’ll talk about what sets them off worse and then I sort of take that on board and I’ll stop having that in my diet”

117
Theme Sub-themes Quotes
“I would’ve loved to have had a brochure sit up there amongst all the other cancers just giving all those basic advice…that was the biggest thing missing in my first six months of diagnosis”
“I think it would be brilliant to have an information sheet on nutrition [for NETs], because as I say the oncologists a) they don’t understand NET, b) if the do understand NET they focus on treating the cancer. They don’t focus on looking at side-effects”

118
5.5.3 Uncertainty
One of the key themes identified was uncertainty. This related to a NET diagnosis and
prognosis, which underpinned and contributed to patients’ experiences and
behaviours with regard to their well-being and relationships with friends and family.
People described the uncertainty of a living with a NET diagnosis on their quality of life,
with some describing the uncertainty as causing a feeling of lack of control over their
situation. Several patients experienced a prolonged time to diagnosis and prolonged
treatment planning, which added to their uncertainty of what illness they had and how
serious or impacting on their life it would be. Two participants emphasised their
uncertainty regarding prognosis and the impact of their NET on their length of life,
after being told by medical professionals that they were unable to provide a clear
prognosis. This had an emotional impact on these participants, causing distress, and a
lack of control. One participant said:
“It’s just uncertainty. I’m still pretty uncertain about the
diagnosis…uncertain about how the treatment is going to work and just
uncertain about time”- Patient 3
Another participant said:
“At this stage I don’t know whether I’m going to live for two years or
whether I’ll see ten” – Patient 7
There was uncertainty regarding expectations of treatment, how it would impact their
current symptoms (i.e. would they improve or worsen), and the impact on their length
and quality of life. One participant said:
“A lot of those physical activities I did or used to do I’m unable to do
now…we’ll see over the next four treatments how well I respond and
whether I can get back to where I was” – Patient 1
119
Uncertainty regarding symptoms and their impact on quality of life over time was
particularly pronounced for some participants, specifically those who reported
experiencing diarrhoea. Diarrhoea was reported to have a considerable impact on
quality of life, particularly if severe (more than 6-10 times per day), as it inhibited their
ability to leave the house. As many participants had only commenced treatment or
were still in the treatment planning phase, they were unsure as to how long they
would be burdened with severe diarrhoea and how it would impact their life longer-
term. One participant described the severity of their diarrhoea:
“I could be going [to the toilet] up to 20 to 30 times a day” – Patient 6
The same participant described the impact of their diarrhoea on their ability to leave
home:
“It’s like you’d go to the toilet and then 10 minutes later you need to go
again and it was just fluids you know, coming out, it was just terrible…I
couldn’t go anywhere because I needed to near a toilet” – Patient 6
Participants spoke about the emotional burden of their diagnosis on themselves and
their families, particularly because they felt uncertain and fearful about the impact on
their length of life (risk of death) and how their diagnosis and treatment might impact
how they live their life and their ability to physically and financially support their
family. Those with partners and children described the impact of this uncertainty on
those close to them. One participant said:
“The cancer is affecting my family, my wife and my children because you
know it’s something hard to get your head around but as I say you can’t do
much about it you just gotta keep on going on” – Patient 4
Most participants were aware that their disease was rare and learnt, often through
their own research, that information and guidance about their disease management

120
was not readily available to them. Some participants reported being unsure where to
access timely and accurate information about NETs but were also unsure regarding
what information would be helpful for them. This was particularly heightened for
participants who had received care or treatment at a health service that did not have a
specialist NET referral centre, unlike the centre where this PhD project was
undertaken. These participants spoke about having initial contact with health
professionals that had limited experience in the management of NETs. In these cases,
they felt unable to access sufficient information or support for their disease, and
experienced uncertainty regarding their prognosis and expectations of treatment.
Participants who’s first contact with medical professionals after a NET diagnosis was at
the study site, reported good receipt of information, and improved clarity regarding
treatment planning, in comparison with participants who had initial contact with
medical professionals at non-NET specialist health services.
5.5.4 Complexity
The theme of complexity was evident throughout all of the interviews and related to
several factors including pathway to diagnosis, morbidity and symptom burden,
nutritional impacts of a NET and nutrition-related behaviours. The path to NET
diagnosis and treatment was reported as complex, with some participants recalling
multiple conversations with different doctors before having a clear diagnosis, and
some participants undergoing tests and treatment at other centres with limited clarity
on their diagnosis, before being referred to the study site. One participant said:
“Nobody seemed to know anything about it [NET] and even recently well
certainly in Wellington um the first oncologist I was under there had no
understanding of NET and he just assumed you’d be dead.” – Patient 1
Another participant spoke about his experience over-time since his NET diagnosis:

121
“I feel as though I’ve been neglected um quite a bit over my journey with
not having treatment, not getting the right scans done. I’ve had to it wasn’t
until I went to a support group of my own volition that I found out about
the PRRT um treatment” – Patient 6
People described experiencing various symptoms related to their NET including
diarrhoea, fatigue, pain, flushing, bloating, wind, difficulty swallowing and altered
blood sugar levels. Complexity surrounding symptom burden was observed due to the
variation in symptom type and severity reported by participants, and the range of
impacts symptoms had on quality of life and daily function. Examples of symptom
burden impacting quality of life included reducing their confidence to leave their
home, reducing their ability to socialise with friends or family (particularly over food),
and persistent symptoms causing mental distress. One participant described the
impact of their diarrhoea on their ability to leave the house:
“I have to probably go to the toilet three times before I can leave the
house…safely leave the house”- Patient 1
Another participant also described their trouble with diarrhoea:
“worry about you know that you’re gonna get diarrhea or not or have to
leave early because of it or you know you got to cancel before you even
went out because it was um a bit rife so yeah it’s had had a big negative on
my life actually” – Patient 6
Another participant spoke about the impact of their NET diagnosis on their social life:
“Apart from not being out go out socially um on a weekend or an evening I
lost my social circle” – Patient 8
Participants reported continuously monitoring their symptoms and searching for
strategies to manage or improve them, which often involved attempts at dietary

122
change, including food avoidance and altered meal patterns. Some participants
described the ongoing impact of symptom burden on their quality of life, whereas
others reported finding a way to live with their symptoms, by mentally accepting them
as part of the disease process and through developing strategies to enable
continuation of daily activities.
Complex nutritional impacts and nutrition-related behaviours
Participants reported various changes to their diet and nutrition as a result of their NET
symptoms and diagnosis. Table 5.3 outlines the type of dietary changes reported in the
interviews and the frequency in which it was reported.
Table 5.3 Reported dietary changes
Food/drinks avoided (n) Other changes (n)
Milk/dairy (4) Smaller meals/eats less (5)
Alcohol (2) Healthy food (4)
Spicy (2) Avoids sweets (2)
Egg (2) FODMAP diet (2)
Bread (2) Vegan diet (1)
Meat (1) Low carb (1)
Stone fruit (1) Avoid preservatives (1)
Dried fruit (1)
Onion/garlic (1)
Tomato (1)
Cauliflower (1)

123
There was considerable variation in the types of dietary changes reported by
participants (Table 5.3). The majority of dietary changes were in response to a degree
of symptom burden, but dietary change was also reported by people who were
asymptomatic. People who were asymptomatic described attempts to change their
diet to be more healthy (commonly increasing fruit and vegetables, reducing fat), as
they felt it would improve their treatment and recovery from their NET.
There were numerous symptoms reported by participants to impact their diet,
including early satiety/feeling full, bloating, wind/gas, nausea, diarrhoea, pain,
dysgeusia, vomiting, flushing and high/low blood sugar levels. Participants were most
likely to reduce their meal size and eat less overall if experiencing symptoms of early
satiety, bloating, diarrhoea, and vomiting. Participants who reported experiencing
regular diarrhoea, would generally eat less overall or modify the foods they ate for fear
of worsening diarrhoea and needing to use the toilet. One person said:
“It doesn’t matter what I eat. Whatever I ate came out” – Patient 2,
another stated,
“I realized certain foods like milk so dairy products that used to bring on
bouts of diarrhoea” – Patient 6
Dietary changes initiated due to diarrhoea included reduced meal size or eating less,
less spicy food, less dairy or milk, less meat, less bread, less fruit, and less onion and
garlic. Participants reporting dairy and spicy food contributing to their diarrhoea, but
the dietary changes were based upon individual experience. Participants experiencing
symptoms of bloating, wind/gas and abdominal pain reported these being worsened
by some food types including dairy, garlic, meat, tomato or acidic products, and spicy
foods, but there was observed variation in individual experiences and attitudes
towards the types of food that were worsening their symptoms. Weight loss was
reported more often than weight gain by participants at baseline. Despite their weight
history or status, it was evident that many were continuously monitoring their weight
124
and used it as a measure of their overall health status. One participant described their
experience with weight loss and managing their changing body shape:
“just trying to um maintain my weight at least rather than lose any more
but you know and just to put some back – all the weight that I had put
back’s gone straight to me stomach. Nothing in my arms or legs or anything
like that but yeah....it’s not exactly where I want it but at least I’ve turned
the corner of losing weight so....I’ll just try and manage my shape now” –
Patient 6
Impact of diet and weight change on quality of life
The impact of dietary change on quality of life was described by many participants.
People talked about the impact on social activities and relationships, with several
describing difficulty in eating out and socialising with friends during a meal due to
restrictions on their diet and tolerance of food. One participant said:
“I can’t eat this and I can’t eat that and it’s becoming harder and harder
because you can’t go to all places or have all different sorts of food…It
affects you socially because everyone has to change what they want
because you can’t have what’s [food] on offer” – Patient 8
Another said in reference to meeting friends out for dinner:
“I went out but I just couldn’t eat anything” – Patient 9
One participant described the impact of their diet and symptoms on his/her ability to
travel outside the house and on holiday, citing a need to pack their own food:
“I often take food with me you know if I go on a plane trip I’ve always got a
packet of rice biscuits and boiled eggs, things like that”. – Patient 5

125
The impact of weight change on quality of life was described but less pronounced than
dietary change. Participants who had experienced weight loss were regularly
monitoring their weight and conscious of their weight status. They reported that
weight loss contributed to the symptom of fatigue and limited their function in regard
to physical activity. One participant who had experienced weight gain reported
concern about their body image:
“self esteem-wise it’s not good…I feel very, yeah unattractive” – Patient 8
5.5.5 Conflicting advice
Participants who had previous contact with health professionals at non-NET specialist
centres, with limited experience in diagnosis and managing NETs, found advice
received on their prognosis and treatment planning unclear and often unsatisfying.
The information and support received after referral to the study site was reported as
being better coordinated, and participants spoke positively about information received
from health professionals that they knew had experience in managing NETs.
Participants were aware they had a rare diagnosis and that there were limited health
professionals with experience and knowledge in NET diagnosis and management.
Participants described being uncertain about information received from health
professionals without experience in NETs. One participant described her experience
with receiving basic nutrition advice from her medical team:
“they said they’re not sure themselves because in New Zealand there’s not
much research about this Neuroendocrine Tumour um but that’s where
they fall short here um but yeah then they just told me to eat and eliminate
all what makes me flush and stop eating it” – Patient 3
Most participants had received some level of nutrition advice from health
professionals after their NET diagnosis. Some participants also sought nutrition advice
prior to their NET diagnosis whilst they were experiencing symptoms that were
eventually attributed to their NET. The satisfaction with nutrition information and

126
advice varied among participants, with most reporting that their nutrition information
needs were not fully met, and they wished for more advice. One participant described
his consultation with a private dietitian who had limited experience in NETs:
“She was in an area where she wasn’t familiar with ah so it made it a bit
hard for her to do any good but I was coming to her giving her money so
she had to sort of do the work” – Patient 5
Participants described feeling uncertain about the quality of information given to them
by health professionals they felt had limited experience in managing NETs, and
described the issue of unmet information needs when their initial NET medical
management was provided at a health centre that didn’t routinely manage NETs.
Participants who only received brief information about nutrition and dietary advice
were more likely to report unmet information needs, and this was found with those
who had received brief nutrition-related advice from medical professionals (surgeon,
GP, oncologist) at time of diagnosis and during treatment planning. One participant
reported:
“When I raised [concern about absorption of nutrients after surgery] with
the oncologists I get the impression they’re preoccupied with treating the
cancer and they’re not so involved with treating any side effects” – Patient
1
Another participant reported, in reference to her requesting information about
management of her symptoms (flushing, diarrhoea) with diet:
“They [oncologist] said they’re not sure themselves because in New
Zealand there’s not much research about this neuroendocrine tumour but
that’s where they fall short here, but yeah they just told me to eat and
eliminate all what makes me flush” – Patient 3

127
Some participants described having limited confidence in advice received during
consultation with private dietitians to manage their symptoms. One participant said:
“she had some funny ideas but the low FODMAP thing is sort of a work in
progress, there’s some old data which she came up with which has been
discounted more recently…so she was a bit out of her depth basically” –
Patient 5
Another participant said:
“she just said I dunno, I dunno what to say, maybe FODMAP and that was
all I got” – Patient 8
Another participant said:
“I went to some dietitian who was basically just googling possibilities while
we were in the room” – Patient 5
A recurring theme among all participant interviews was their need for information on
optimising their nutrition and managing their diet amidst complex symptoms. All
participants reported that at some stage since their NET diagnosis they had wished for
nutrition advice but found this difficult to source. They felt that nutrition information
was a priority for them, but not necessarily a priority among their health professionals.
5.5.6 Self-management and seeking information
As a result of limited or conflicting advice received from health professionals on
nutrition, participants spoke of a need to seek their own information and direct their
own nutrition management. The responsibility to manage one’s own care and
information, was a strong theme among interviews, and related to nutrition
information along with general information on NETs. Many participants spoke about
the value of nutrition information provided or found through peer support via NET

128
patient forums, blogs and discussion groups, the internet, patient support foundations
(NeuroEndocrine Cancer Australia), and family/friends. Several dietary changes
reported by participants were prompted by experiences of other NET patients. One
participant said:
“I looked at these [NET patient] discussion boards and they’ll talk about
what sets them off worse and then I sort of take that on board and I’ll stop
having that in my diet” – Patient 8
Influence from family and friends was also a factor in receipt of nutrition information
and dietary change, with some participants reporting changes to their diet in response
to advice from family and friends who had either previously been treated for cancer or
had an interest in nutrition. All interview participants reported feeling nutrition was
important in the context of their overall NET diagnosis and management, but that
nutrition was not necessarily a priority for health professionals, particularly doctors.
The nutrition advice received from health professionals was often prompted by
questions from the patient and not initiated by health professionals as part of their
general information provision. Several participants also reported wishing they had
received general information on nutrition management for NETs at the time of their
diagnosis. Information that was evidence-based and specific to NETs was identified as
important to participants, rather than general advice for cancer patients, but
participants identified that NET-specific information was difficult to source. One
participant described frustration with receiving general advice on the FODMAP diet to
help manage her NET symptoms:
“you don’t trust it because you think it’s not for NET it’s for IBS. And that’s
not the same thing so that’s what is...I sort of wanted I wanted something
that would say for NET patients, I just wanted it more specific for a NET
cancer” – Patient 5

129
Another participant spoke about wishing for NET-specific dietary information early in
her diagnosis:
“my first six months [after diagnosis] I would’ve loved to have had a
brochure sit up there amongst all the other cancers um just giving all those
basic advices. I would have loved that...that was the big thing missing in my
first six months of diagnosis” – Patient 8
5.5.7 Six-month interviews
A repeat interview at six-months was conducted with nine of the eleven participants
who completed an initial interview. At the time of their six-month interview,
participants had undergone various types of NET treatment including Peptide Receptor
Radionucleotide Therapy (PRRT) (n=3), surgery to remove their primary NET (n=3),
somatostatin analogue (SSA) treatment (n-3).
Content analysis for the six-month interviews focused on similarities and differences to
themes identified in the baseline interviews and change in experience over time.
Through a process of thematic analysis three key themes were identified: Monitoring
and managing symptoms, uncertainty, and self-management/information seeking. Two
themes identified at six-months, uncertainty and self-management/information
seeking, aligned with themes identified at the baseline interviews, indicating that these
themes remained strong evident throughout the study period.
Monitoring and managing symptoms
In general, participants reported improved symptoms and weight stabilisation after six-
months of medical management and treatment. However, several participants still
reported the burden of symptoms caused by their NET or treatment, which lead to
continuous monitoring and management of these symptoms. Participants who were
symptomatic reported continuing to modify their diet in an attempt to manage
symptoms, including changes to their dietary patterns (smaller meals) and avoiding

130
certain foods they perceived as ‘triggers’ for their symptoms. One participant who was
receiving SSA treatment for their small bowel NET, reported modifying their diet to
remove broccoli, garlic, tomato and meat in an attempt to manage symptoms of pain
and abdominal discomfort. Despite these attempted dietary changes they were still
experiencing symptoms, and reported struggling to find a strategy to improve them.
This participant described looking for food causes:
“it’s been challenging because I just don’t know what to eat is basically um
what it comes down to. I sort of have to weigh up um what, like I I’ve sort of
heard all different things that we should avoid” – Patient 8
Uncertainty
The theme of uncertainty remained evident during the six-month interviews, with
patients reporting that despite undergoing treatment and some improvement in
symptoms, they still felt uncertain about their prognosis and treatment outcomes from
a disease perspective. Participants also reported being unsure how long they would be
living with particular symptoms of their NET, which remained after undergoing their
recommended treatment but continued to impact negatively on their quality of life.
This led to an underlying level of anxiety and distress among some participants, and for
some this had remained since the baseline interview:
“at an emotional level ah I I’ve you know got depression, anxiety a few of
those sorts of things, I’ve also come off the antidepressants which I was on
at the last interview so I’ve been just struggling with a lot of ah struggling
with a whole range of emotions and ah you know they hit you at different
times” – Patient 7
Self-management and seeking information

131
The theme of self-management remained dominant in the six-month interviews.
Participants reported improved confidence in their medical management over the six-
months treated at the study site, in comparison to treatment and medical advice
received at non-specialist centres. However, supportive care and nutrition-support
remained lacking, with most participants reporting a continued responsibility to seek
their own information regarding nutrition management for NETs and continued to do
this via sources on the internet, patient support groups and blogs. One participant
described doing this:
“I’m sort of reading those things and just taking it from the experience of
other patients. Um what upsets them and what doesn’t and what to try and
things like that so that’s where I’ve been getting most of my guidance
from” – Patient 8
It was evident that participants used symptom burden and nutrition issues as a
barometer for their own success and improvement, and therefore prioritised these
aspects within their overall cancer care. For example, if participants had some ongoing
symptoms despite an improvement in their symptom burden overall, they still
reported the necessity to optimise their symptom management as much as they felt
was in their control. Diet and eating were perceived as being within their control, and
therefore were opportunities to retain some autonomy in the process of managing
their disease. One participant spoke about their belief that eating the right foods
would help manage their NET disease:
“If I eat certain things and not certain things will that help my NET
outcome” – Patient 7
Some participants reported receiving helpful nutrition advice from a dietitian at the
study site, but many through their own research, were aware of the lack of NET-
specific nutrition information and research. Information from, and comparison with

132
other NET patients was frequently considered the most relevant source of nutrition
information, rather than through contact with health professionals.
5.6 Discussion
This chapter describes insights from interviews undertaken with 11 people who had
contributed to the Phase 1 study. Data from the interviews offer insight into
participants’ perceptions of their HRQoL and their experiences of living with a NET, its
symptoms and its impact on nutrition and dietary changes. Participants spoke about
living with the uncertainty of their NET disease and its prognosis, which contributed to
their desire to search for information about their disease, and also influenced
behaviours in regard to nutrition issues experienced and their management of them.
Participants experienced numerous symptoms as a result of their NET, in particular
gastrointestinal symptoms such as diarrhoea, abdominal cramps/pain, bloating,
wind/gas, and fatigue. For some, symptoms improved over time, but for many the
burden of symptoms remained, with ongoing impact on their quality of life including
limitations to social activities, eating out, daily function and working.
Whilst all participants reported making some change to their diet as a result of their
NET, the interviews highlighted the complexity of these changes and suggested that
dietary change was more often initiated by patients themselves, rather than through
advice from health professionals. Therefore, dietary change and food avoidance
among NET patients may be under-recognised by health professionals, which may be
unhelpful, potentially even detrimental for patients, if the diet changes they make are
restrictive and unnecessary. Dietary restriction can lead to poor dietary intake and
nutritional adequacy, and if prolonged may put patients at risk of weight loss and
malnutrition (Jensen et al., 2019). Dietary restrictions were also reported by
participants to impact negatively their quality of life, including enjoyment of food and
ability to participate in social activities that involved food. Participants reported being
unable to eat out or share meals with friends due to their dietary restrictions and the
limitations on the types of food they could comfortably consume. Participants

133
reported excluding multiple food items from their diet as a result of their symptoms.
Without health professional support and over-sight there is a risk that unnecessary
dietary changes are made by NET patients which have the potential to unnecessarily
impact on their quality of life and food enjoyment.
Barriers to consultation with health professionals about diet and nutrition advice
included the perception that it was not a priority for health professionals to address
these issues, and knowledge that there was limited evidence for nutritional
recommendations specific to NETs based on patients’ own research. Patients
prioritised their own search for nutrition information and advice through peers (via
patient support groups, blogs and discussion boards) and internet sources. Several
review articles discussing the nutritional issues and management of patients with NET
have highlighted the importance of individualised dietary advice based upon
symptoms, disease and treatment characteristics (Go, Srihari and Kamerman Burns,
2010; Gallo et al., 2017; Altieri et al., 2018; D. Clement et al., 2019; Laing et al., 2019),
which is ideally achieved in consultation with experienced NET health professionals.
To our knowledge, this is the first in-depth qualitative exploration of patient
experience of dietary changes and impacts following a NET diagnosis. Only one
published abstract by Davies and Caplin (2009) was found in preparation for the PhD,
which documented the experiences of six patients interviewed with carcinoid
syndrome, who reported changing their diet to some degree and reducing meal size
due to symptoms (Davies and Caplin, 2009). In the Davis and Caplin study, lack of
professional guidance concerning nutrition issues was highlighted as a barrier for
patients, which coincides with results found in this study.
Insights from the interviews in this study highlight a disparity between the degree of
nutrition information and intervention provided by health professionals, and the
nutrition information needs of NET patients. Appropriate methods for screening and
identification of nutrition information needs are important at time of diagnosis and
during treatment to ensure information is provided from evidence-based sources and

134
tailored to individual needs. Health professional education regarding the potential
impact of symptom burden on dietary change and patients’ request for information is
likely to be beneficial, ensuring that these needs are identified and addressed
appropriately. As illustrated by results of this PhD study, there is a great need to
increase awareness of NETs and their impacts on nutrition among health professionals,
including dietitians who only have occasional contact with patients with NETs through
their health services, and therefore limited expertise in the specific nutritional
management of NETs. Professional associations such as the Dietitian Association of
Australia (DAA) and the New Zealand Dietitians Association (NZDA) represent
appropriate targets for dissemination of education on nutrition in NETs to the broader
dietitian professional group. Identification of a NET-suitable nutrition screening tool
and evidence-based guidelines for nutrition management will assist multidisciplinary
health professionals to improve the management of NET-related nutrition issues and
address patient information needs.
5.7 Conclusion
Insights from the interviews highlight the complex and uncertain environment in which
patients diagnosed with a NET exist, despite referral and management at a specialist-
NET referral hospital. A key finding in this study was the identification of nutrition and
diet as a key supportive care priority area for patients, and that they perceived their
diet and nutrition as a higher priority than it was for their treating medical team. Lack
of confidence in health professionals, particularly from non-specialist centres with
limited knowledge in NET management, was also reported by participants. The
complexity of dietary changes, and the patient knowledge and assumptions that
prompted them, indicate that generalised nutrition advice is unlikely to be helpful for
this patient group, and an individualised approach is needed. Quantitative results for
nutritional status and complications reported in Chapter 4, indicate that nutritional
complications of weight loss, malnutrition and dietary change are under-recognised by
health professionals. Results of the qualitative interviews re-enforce this under-
recognition in regard to symptoms and dietary management, particularly given the

135
impacts they have on patients’ quality of life. Further evidence is required to
determine whether there is a relationship between dietary intake and NET-related
symptom severity. Interventional studies that include patient-reported experience and
outcome data should be encouraged to test the impact of dietary restriction on
symptoms. The development of formal guidelines for the dietary screening and
management of NETs would be of significant benefit in assisting health professionals in
identifying and addressing dietary change and it’s impacts among patients living with a
NET. Guidelines should also support exploration of the nutrition information needs of
patients with a NET. Once evidence for the presence of nutritional complications is
well-established, prospective interventional studies testing the effect of dietary or
nutrition interventions will aid in exploring optimal management approaches for
nutrition support in this patient group.


137
Chapter 6: Health professional practices in relation to
screening and management of nutritional issues in people
with NETs
6.1 Introduction
The second objective of this thesis was to describe health professional knowledge and
management of nutritional complications in patients with GEP NETs and summarise
current international practice. To achieve this health professionals took part in an
exploratory study to describe their perceptions of nutrition issues among patients with
NETs as well as their current nutrition screening and management practices. Phase 2
was also undertaken using an embedded mixed methods approach as described in
Chapter 2 (Section 2.3).
6.2 Phase 2
6.2.1 Online structured survey of health professionals
An international cohort of multidisciplinary health professionals; including doctors
(medical oncologists, surgeons, gastroenterologists, nuclear medicine physicians,
endocrinologists), nurses and allied health; who regularly provide care for NET
patients, participated in a 21-item online structured survey. Survey questions asked
about symptom prevalence, nutrition screening and assessment practices, use of
evidence-based guidelines and provision of nutrition advice.
Methods and results for this study are described in Sections 6.2.4 and 6.2.5 of this
chapter (Chapter 6).
6.2.2 Focus groups
Multidisciplinary health professionals working regularly with NET patients at one of the
two recruitment sites participated in semi-structured focus groups and interviews.

138
Focus group questions asked health professionals about their knowledge, experience
and opinion in regard to the presence, assessment and management of nutritional
complications among NET patients. Questions were aligned with the questions asked
in the structured online survey, in order to provide more in-depth exploration of these
topics.
Methods for the qualitative study are described in Chapter 7: Managing nutritional
issues in NETs from a health professional point of view.
6.2.3 Prepared manuscripts
Two manuscripts have been prepared for publication, describing methodology and
results of the health professional survey. The manuscripts are proposed as a joint
submission, with the first manuscript introducing and discussing in detail results of the
international survey for symptom prevalence, nutritional screening and management,
and the second manuscript focusing on results and discussion of vitamin screening and
supplementation practices. The second manuscript allows comprehensive discussion
of vitamin deficiency management in NETs, which is where the nutrition literature in
NETs is currently focused. Final versions of both manuscripts have been approved by
all authors and will be submitted in October 2020.
6.2.4 Manuscript 1
Exploring international health professional knowledge and management
of nutritional complications in neuroendocrine cancer patients
Erin Lainga,b*, Nicole Kissc,d, Meinir Krishnasamya,e,f, Karla Goughg, Michael
Michaelh,i,
aDepartment of Nursing, School of Health Sciences, The University of Melbourne,
305 Grattan Street, Melbourne VIC 3000, Australia

139
bNutrition and Speech Pathology Department, Peter MacCallum Cancer Centre,
Victorian Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC
3000, Australia
cInstitute for Physical Activity and Nutrition (IPAN), Deakin University, Geelong,
Australia,
dAllied Health Research, Peter MacCallum Cancer Centre, Victorian
Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC 3000,
Australia
eVictorian Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC
3000, Australia
fCentre for Cancer Research, The University of Melbourne, Grattan Street,
Melbourne VIC 3000, Australia
gCancer Experiences Research, Peter MacCallum Cancer Centre, Victorian
Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC 3000,
Australia
hDepartment of Medical Oncology & Neuroendocrine Unit (ENETs COE), Peter
MacCallum Cancer Centre, Victorian Comprehensive Cancer Centre, 305 Grattan
Street, Melbourne VIC 3000, Australia
iThe Peter MacCallum Department of Medical Oncology, University of
Melbourne, Grattan Street, Melbourne VIC 3000, Australia
Abstract
Introduction
Patients with neuroendocrine tumours (NET) are at nutritional risk due to
symptoms and side-effects of treatment. Current evidence-based guidelines lack
information regarding optimal nutritional management and supportive care.
Objective

140
This study aimed to describe health professional knowledge and management of
nutrition complications in GEP NET patients and summarise current international
practice.
Methods
Multidisciplinary health professionals who regularly provide care for NET
patients, were invited to participate in a 21-item online survey. Survey questions
asked about symptom prevalence and their impact, and nutrition screening and
assessment practices. General demographic information was recorded.
Results and Conclusions
In total 73 health professionals completed the survey. The majority worked in
Australia (52%) and the United Kingdom (19%). Most responses were provided
by medical oncologists (25%), nurses (23%) and dietitians (30%). Fifty percent
reported managing NET patients for more than seven years. Diarrhoea and
fatigue were reported as the most common symptoms (86% and 60%,
respectively) and of greatest concern to patients with NET (80% and 52%,
respectively). Provision of advice for symptom management, weight loss and
food intolerances was reported by 92%, 59% and 41%, respectively. Thirty-eight
percent carried out screening or assessment for malnutrition. Health
professionals commented on the lack of NET-specific nutrition guidelines and
used general oncology nutrition guidelines to direct their practice. This is the first
international survey of nutrition knowledge and practices among NET health
professionals. Results highlight variations in nutrition screening and assessment
practices and identify a gap in NET-specific guidelines addressing nutrition issues
in this at-risk patient group.
Introduction
Neuroendocrine tumours (NET) are a heterogenous, often indolent group of
cancers, with varying prognoses. They are commonly located in the

141
gastrointestinal (GI) tract, pancreas and lung, and have the unique potential to
secrete hormones resulting in a variety of clinical functional syndromes. They can
impact on nutrition due to several factors including the sites of disease, clinical
functional syndromes as well as treatment complications [1]. For example, the
carcinoid syndrome due to excess secretion of serotonin, commonly elicits
symptoms such as diarrhoea, fatigue, flushing and abdominal discomfort [2–6].
Literature has indicated that up to 50% of patients with a NET of the GI tract or
pancreas experience diarrhoea, flushing and abdominal discomfort, and up to
70% experience fatigue [4,6–9]. These symptoms can have significant impact on
patients’ physical and emotional quality of life [7,10,11], as well as the potential
to impact on nutritional intake and digestion.
For example, diarrhoea can reflect altered gut function and malabsorption as a
consequence of NET hormonal syndromes, or iatrogenic causes such as surgery
or somatostatin analogues. Up to 58% of patients with a NET have reported
making changes to their diet as a result of their diagnosis, and up to 89%
reported suffering a food intolerance [4,12].
Recent literature has indicated that up to 25% of patients with a NET are
malnourished and a higher proportion are at risk of poor nutritional status [13–
15]. Studies reporting on malnutrition prevalence recommend that all NET
patients should be screened for malnutrition, particularly those with higher
grade NETs and those undergoing chemotherapy [14,15]. Despite this, there are
currently no nutrition guidelines that focus on the needs of NET patients. There
is also a lack of guidance on screening and assessment for malnutrition and other
nutrition complications, in current NET clinical practice guidelines.
To-date, evidence available has only focussed on the prevalence of nutrition
complications and dietary change amongst NET patients. On the other hand
there has been little focus on symptoms or factors contributing to dietary
change, or on the screening and assessment practices of health professionals

142
working to address the nutritional consequences of a NET. A formal survey of
health professional knowledge and management of nutrition complications in
NET patients has not been reported.
Aim and objectives
The main aim of this study was to describe health professional knowledge and
management of nutrition complications in NET patients. The secondary aim was
to summarise current international nutrition practices. The aim of this paper is
to report on health professional nutrition screening and assessment practices
and provision of nutrition advice and management.
Materials and Methods
Survey design
A customised online survey was developed for this study, because a relevant
validated tool was not available. Survey content was identified based on a review
of published literature; then content relevance, representativeness and technical
quality were appraised by expert judgement using a dietitian, senior nurse and
NET Unit medical oncologist at the research site. This included an appraisal of
readability and burden [16]. Only minor revisions to wording were required.
The finalised survey consisted of 21-questions including one open- and 14
closed-ended questions, as well as, six questions responding to a visual analogue
scale (0-100). The first four questions were demographic questions. These
included the geographical location of the participant’s place of work, their
profession, the length of time they had been managing NET patients (in years),
and the approximate number of NET patients managed per year. Subsequent
questions addressed the following themes: symptom prevalence and impact in
NET patients (4 items), extent of nutrition issues in NET patients (5 items),
malnutrition screening and assessment practices (1 item), vitamin screening and
supplementation practices (2 items), nutrition management practices (4 items)

143
and importance of nutrition (1 item). This paper reports on responses to
questions covering five of the six survey themes. Questions covering the theme
of vitamin screening and supplementation practices (Q15 and Q16) are reported
elsewhere (‘Exploring vitamin testing and supplementation practices of
international health professionals managing neuroendocrine cancer patients’,
Laing et al. 2020).
The survey was designed to be anonymous, with no identifying information
collected from the participants. A copy of the survey is provided in online
supplemental appendix. The survey was designed with branching logic; in this
case, participants were prompted to answer additional questions based upon
prior responses. For customised questions about symptoms (Q5 to Q8), the list of
possible symptoms a NET patient may experience was drawn from the European
Organisation for Research and Treatment of Cancer (EORTC) quality of life
questionnaire QLQ-C30 and the QLQ-GI.NET21 module [17,18], as well as from a
comprehensive literature review undertaken prior to the design of the survey.
The EORTC QLQ-C30 was designed for use with cancer patients and the QLQ-
GINET21 module was specifically designed for use with NET patients. Most
questions required a tick box response while questions 9 to 13 and 21 were
answered using a visual analogue scale, as stated previously. Visual analogue
scales were used to obtain opinion from participants on nutrition issues in
patients with NET.
Study population
Invitations to participate were distributed via email through the following
organisations and specialist NET societies (Commonwealth Neuroendocrine
Tumour Society, CommNETS; European Neuroendocrine Tumor Society, ENETS;
Unicorn Foundation Australia health professional network; Australasian
Gastrointestinal Trials Group, AGITG; Clinical Nursing Society of Australia, CNSA;
New Zealand Southern District Health Board Gastrointestinal and NET

144
multidisciplinary teams; United States Academy of Nutrition and Dietetics
oncology nutrition dietetics practice group). Specialist NET clinicians were also
identified and invited to participate through listings on the websites of NET
organisations and professional contacts of the research team.
Health professionals were eligible for participation in the survey if they worked in
a multidisciplinary NET referral centre and in one of the following professional
areas: Medical Oncology, Surgical Oncology, Radiation Oncology, Endocrinology,
Gastroenterology, Nuclear Medicine, Cancer Nursing, Palliative Care, Dietitians
and Allied Health. In the email invitation health professionals were provided a
letter explaining the purpose of the survey; that responses were voluntary and
anonymous, and that consent was assumed with completion of the online
survey. A web-link to access the survey was included in the invitation email.
Information about the survey, an invitation to participate, eligibility criteria, and
a web-link to the survey were also sent via organisations and societies’
newsletters to potential participants. If possible, reminder emails were sent one
week after the initial email invitation. Ethics approval for this study was obtained
from the Peter MacCallum Cancer Centre Human Research Ethics Committee
(EC00235) on April 20, 2017.
Statistical analysis
Counts and percentages were used to summarise participant characteristics and
responses to the online survey, excepting questions 9 to 13 and 21. For the
latter, means and standard deviations were used to summarise the scores of
dietitians; then, mean differences with 95% confidence intervals were estimated
between dietitians and medical professionals, and dietitians and nurses. Cohen’s
d was calculated for each comparison to characterise the size of observed
differences and interpreted using existing conventions; that is, 0.2 for a small-
sized difference, 0.5 for a medium-sized difference and 0.8 for a large-sized
difference [19]. IBM SPSS Statistics Version 23 (Chicago IL, USA) was used for

145
descriptive analysis. Summarising content analysis was used to code open text
responses [20].
Results
Information about and invitations to take part in the survey were distributed
between September 2017 and April 2018. A total of 64 individual NET health
professionals were sent email invitations. The number of NET health
professionals who received an invitation to the survey via organisations, group
emails and newsletter dissemination was indeterminate.
In total, 73 health professionals completed the online survey. Thirty-eight (52%)
worked in Australia, 14 (19%) in the United Kingdom, seven (10%) each in the
remainder of Europe and the United States, six (8%) in New Zealand and one
(1%) in Canada. Participant characteristics are summarised in Table 1. A majority
were medical professionals (n = 31, 42%) or dietitians (n = 22, 30%) and
approximately half (n = 37, 51%) reported managing NET patients for at least
seven years. Most reported having a dietitian available in their centre to assist
with managing nutritional issues with NET patients (93%).
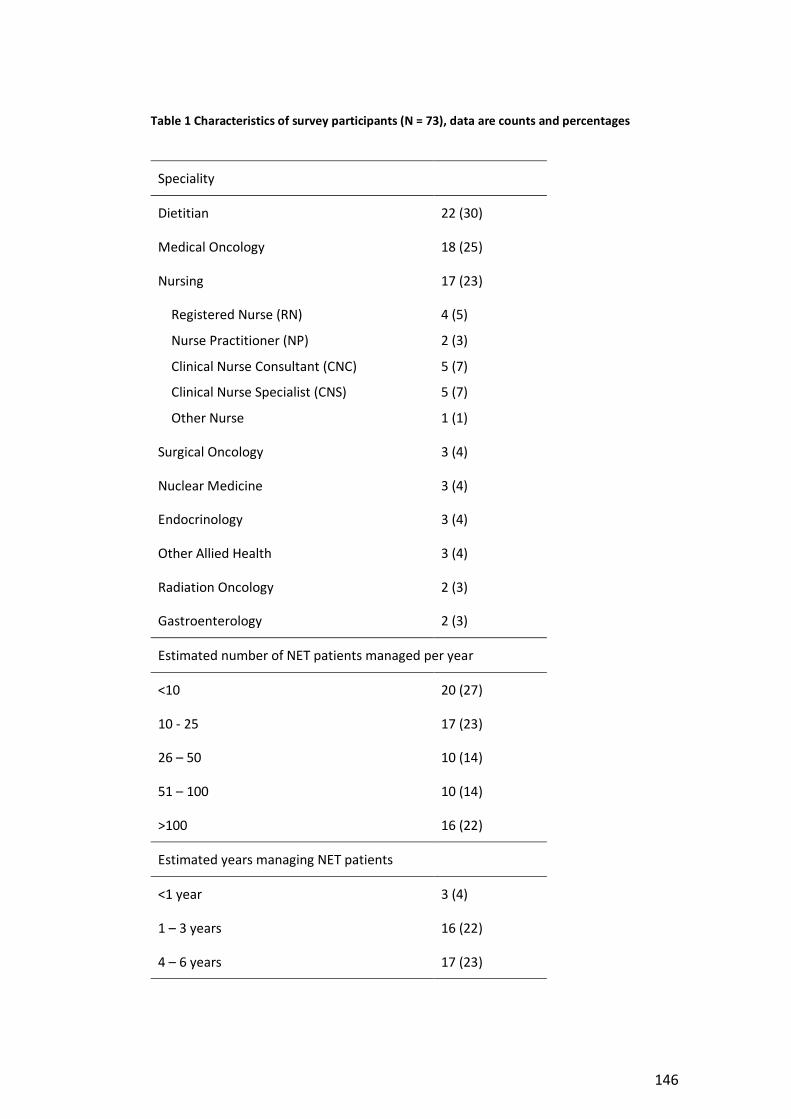
146
Table 1 Characteristics of survey participants (N = 73), data are counts and percentages
Speciality
Dietitian 22 (30)
Medical Oncology 18 (25)
Nursing 17 (23)
Registered Nurse (RN)
Nurse Practitioner (NP)
Clinical Nurse Consultant (CNC)
Clinical Nurse Specialist (CNS)
Other Nurse
4 (5)
2 (3)
5 (7)
5 (7)
1 (1)
Surgical Oncology 3 (4)
Nuclear Medicine 3 (4)
Endocrinology 3 (4)
Other Allied Health 3 (4)
Radiation Oncology 2 (3)
Gastroenterology 2 (3)
Estimated number of NET patients managed per year
<10 20 (27)
10 - 25 17 (23)
26 – 50 10 (14)
51 – 100 10 (14)
>100 16 (22)
Estimated years managing NET patients
<1 year 3 (4)
1 – 3 years 16 (22)
4 – 6 years 17 (23)

147
Speciality
7 – 10 years 15 (21)
>10 years 22 (30)
Symptoms
Responses to questions regarding symptom presence and impact in NET patients
are summarised in Table 2.
Table 2 Symptom presence and impact in NET patients (N = 73), data are counts and valid
percentages (multiple responses allowed)
Most commonly reported symptom by NET patients
Most concerning symptom as reported by NET patients
Symptoms that can lead to reduced dietary intake in NET patients
Symptoms that can lead to weight loss in NET patients
Diarrhoea 63 (86) 58 (80) 53 (73) 61 (84)
Fatigue/tiredness
44 (60) 38 (52) 31 (43) 31 (43)
Abdominal discomfort
43 (59) 35 (48) 49 (67) 47 (64)
Flushing 35 (48) 23 (32) 6 (8) 2 (3)
Weight loss 34 (47) 33 (45) 6 (8) -
Bloating 32 (44) 16 (22) 49 (67) 40 (55)
Wind/gas 22 (30) 15 (21) 29 (40) 33 (32)
Loss of appetite
18 (25) 17 (23) 56 (77) 60 (82)
Pain 15 (21) 21 (29) 38 (52) 33 (45)
Nausea 14 (19) 11 (15) 50 (69) 51 (70)
Night sweats 10 (14) 6 (8) 4 (6) 6 (8)
Other 10 (14)a 6 (8)b 5 (7)c 1 (1)d

148
Most commonly reported symptom by NET patients
Most concerning symptom as reported by NET patients
Symptoms that can lead to reduced dietary intake in NET patients
Symptoms that can lead to weight loss in NET patients
Indigestion/
heartburn
5 (7) 3 (4) 37 (51) 29 (40)
Constipation 4 (6) 4 (6) 25 (34) 22 (30)
Weight gain 3 (4) 4 (6) 6 (8) -
SOB/wheeze 2 (3) 4 (6) 7 (10) 11 (15)
Vomiting 1 (1) 6 (8) 31 (43) 46 (63)
Notes.
a Reduced physical function, falls, hypoglycaemia, light-headedness, steatorrhoea, taste changes, anxiety depression
b Reduced physical function, falls, anxiety, depression, bowel urgency and incontinence
c Taste changes, post-surgery, treatment adverse events, anxiety/stress
d Malabsorption
According to health professionals, the most common symptoms reported by
patients were diarrhoea (n = 63, 86%), fatigue (n = 44, 60%), abdominal
discomfort (n = 43, 59%), flushing (n = 35, 48%) and weight loss (n = 34, 47%).
These symptoms were also thought to be of most concern to NET patients.
Twenty of 22 (91%) dietitians, 27 of 31 (87%) medical professionals and 11 of 17
(65%) nurses reported diarrhoea as a concerning symptom for NET patients. A
greater proportion of dietitians selected weight loss as a commonly reported
symptom (17 of 22, 77%) compared with medical (8 of 31, 26%) and nursing
professionals (8 of 17, 47%). Nursing and medical professionals, on the other
hand, were more likely to select fatigue as a commonly reported symptom (14 of
17, 82% and 22 of 31, 71%, respectively) compared with dietitians (5 of 22, 23%).
Symptoms thought to most likely reduce dietary intake and cause weight loss
included diarrhoea, loss of appetite and nausea (Table 2). Bloating and
abdominal discomfort were also frequently reported as a cause of reduced

149
dietary intake. Reponses to questions regarding symptom impact on dietary
intake and weight did not differ between medical, nursing and dietitians, except
for nausea. Nurses were more likely to report nausea to impact dietary intake
(15 of 17, 88%), than medical professionals (18 of 31, 58%) and dietitians (15 of
22, 68%).
Nutrition screening and assessment
When asked about practices relating to malnutrition, 28 (38%) participants
reported screening for or assessing malnutrition when consulting with NET
patients, and 25 (34%) indicated that a colleague performed this task. Twelve of
22 (55%) dietitians indicated that they performed malnutrition
screening/assessment themselves, a larger proportion than nurses (6 of 17, 35%)
or medical professionals (10 of 31, 32%). Nurses were the most likely to report
that a colleague performed malnutrition screening/assessment (10 of 17, 59%).
Of those that reported their colleague performed malnutrition screening, 13 of
25 reported the dietitian, 6 of 25 reported the nurse and 5 of 25 reported the
doctor was responsible for screening.
Of the 53 participants who reported that either themselves or a colleague
performed malnutrition screening or assessment, overall the most common tool
used for this purpose was the Malnutrition Screening Tool (MST) (n = 15, 21%)
(Table 3). More than a quarter of participants reported screening by themselves
or a colleague without a validated tool (n = 19, 36% of all respondents). Nine of
the 16 dietitians (41%) who reported screening did not use a validated tool.

150
Table 3 Tools used by professionals who perform malnutrition screening or assessment (n =
53), data are counts and valid percentages (multiple responses allowed)
Tool
Do not use a validated tool 19 (36)
Malnutrition Screening Tool (MST) 15 (28)
Malnutrition Universal Screening Tool (MUST) 4 (8)
Subjective Global Assessment (SGA) 3 (6)
Patient Generated Subjective Global Assessment (PG-SGA) 3 (6)
National Risk Screening Tool (NRS) 2 (4)
Patient Generated Subjective Global Assessment Short Form (PG-SGA-SF)
1 (2)
Unsure 12 (23)
Other 2 (4)
Nutrition advice and management
Symptom management advice was the most common form of advice provided by
all professions (Table 4). Responses for dietitians, medical and nursing
professionals are summarised in Figure 1. A majority of the dietitians surveyed
provided advice on symptom management (22 of 22, 100%), weight loss (21 of
22, 96%), food intolerances (17 of 22, 77%) and vitamin deficiency (13 of 22,
59%). Nurses mainly provided advice on symptom management (14 of 17, 82%)
and weight loss (10 of 17, 59%), whereas medical professionals tended to mainly
focus on symptom management (29 of 31, 94%), with few providing advice on
weight gain (5 of 31, 16%), food intolerances (9 of 31, 29%) and vitamin
deficiency (6 of 31, 19%).

151
Table 4 Issues that are the subject of routine advice (n=73), data are counts and valid
percentages
Issue
Symptom management 67 (92)
Weight loss 43 (59)
Food intolerance(s) 30 (41)
Vitamin deficiencies 23 (32)
Weight gain 14 (19)
None of the above 5 (7)
s
Figure 1 Provision of types of nutrition advice by medical, nursing and dietitian profession
(Q17, multiple responses allowed), values are percentage
Forty-seven (64%) of all participants routinely provided advice to NET patients to
help improve their nutrition. Compared with nurses (12 of 17, 71%) and medical
professionals (14 of 31, 45%), dietitians were more likely to provide nutrition
advice (21 of 22, 96%). The most common nutrition advice provided by
0
10
20
30
40
50
60
70
80
90
100
Medical
Nursing
Dietitians
152
participants related to diarrhoea or bloating management (including modified
fibre diet) (13 of 47, 28%), advice on high energy and/or high protein diet (11 of
47, 23%), general dietary advice before referring to a dietitian (9 of 47, 19%), and
individualised dietary advice based on present symptoms (7 of 47, 15%). Other
less frequently reported advice included management of fat malabsorption and
pancreatic enzyme replacement therapy, risk of malnutrition, encouraging small
frequent meals, general healthy eating, and diet suitable for carcinoid syndrome.
Of the 47 participants who routinely provided nutrition advice to NET patients,
28 (38%) reported that these practices were based on evidence or best-practice
guidelines. Guidelines most frequently used included the European Society for
Clinical Nutrition and Metabolism (ESPEN) guidelines on nutrition in cancer, the
National Institute for Health and Care Excellence (NICE) guidelines on nutrition
support for adults and ENETS guidelines. Other sources of evidence included
published journal articles on nutrition and NETs, guidelines for pancreatic
enzyme replacement therapy, and websites and resources from the Unicorn
Foundation Australia, Royal Free Hospital London and the Carcinoid Cancer
Foundation. Fourteen participants (50%) commented on the lack of availability of
NET-specific nutrition guidelines and instead used consultation or training with
NET specialist dietitians, general symptom guidelines or oncology best practice
guidelines to inform their practice.
Health professional experience and opinion of nutrition issues in NET patients
Dietitian’s responses to the visual analogue scales are summarised in Table 5, as
are the differences between the responses of dietitians and those of the nursing
and medical professionals. There was considerable variation in dietitians’
responses and confidence intervals on the differences between dietitians and the
other professional were wide.

153
Based on their responses to question 13, medical professionals receive reports of
dietary changes to a lesser extent than dietitians (M difference = -12 [95% CI -23
to 0], medium-sized difference). Similarly, based on their responses to question
21, medical professionals thought nutrition was less important than dietitians (M
difference = -18 [95% CI -28 to 9], large-sized difference). None of the differences
between dietitians and nurses met the threshold for a medium-sized difference.

154
Table 5 Summary of comparisons on visual analogue scale questions
Question
Dietitian Medical Nursing
M SD M diff 95% CI Cohen’s d
M diff 95% CI Cohen’s d
9 To what extent are NET patients concerned about their nutrition overall?
74 19 -8 -19, 2 0.47 0 -11,12 0.03
10 To what extent is weight loss a problem for NET patients? 66 19 -9 -21, 2 0.46 -5 -17, 8 0.25
11 To what extent is weight gain a problem for NET patients? 32 20 0 -12, 11 0.00 2 -12, 15 0.08
12 To what extent to NET patients report food intolerance(s)? 63 21 -9 -22, 4 0.39 -8 -24, 7 0.37
13 To what extent do NET patients report changing their diet as a result of symptoms relating to their NET diagnosis or treatment?
74 18 -12 -23, 0 0.56 -9 -22, 4 0.46
21 Is addressing nutrition important in the overall context of a NET patients treatment?
91 13 -18 -28, -9 1.10 3 -4, 10 0.27
Notes.
M difference = M other specialty - M dietitian
Scale ranges for VAS: 0 to 100
Anchors for question 9: not at all to very concerned
Anchors for question 10 and 11: not at all to serious problem
Anchors for question 12 and 13: never report to frequently report
Anchor for question 21: not at all to extremely important
Cohen’s d interpreted as: 0.2 small-sized difference; 0.5 medium-sized difference; and 0.8 large-sized difference

155
Discussion/Conclusion
This survey provides the first summary of international health professionals’
nutrition screening and management practices for patients living with a NET.
Research undertaken to date has focussed on prevalence of malnutrition and
other nutrition issues in patients with a NET [13–15], but health professional
experience, attitudes and practices regarding the nutritional management of
NETs has not previously been explored. This research has clarified aspects of
current health professional practice, illustrates considerable inconsistencies in
practice and highlights possible targets for future research and education.
Patient symptom burden reported by the health professionals who participated
in this study is consistent with literature on patient-reported symptom burden
[7,10]. Symptoms of diarrhoea (27-92%), fatigue (25-69%) and abdominal
discomfort (22-50%) are common in patients with NET [4,6,7,9,14,21], and also
amongst the most common symptoms reported by health professionals in this
study. Symptoms reported in this study as most burdensome to patients -
diarrhoea, fatigue and flushing - have also been reported by patients in other
studies to have the most impact on their quality of life [7,10,11]. These findings
indicate that NET health professionals, regardless of type of profession, are
aware of the symptoms experienced by patients with a NET and suggests that
health professionals are discussing symptom burden in their consultations. In this
study 92% of health professionals reported providing advice on symptom
management in their consultations with NET patients, supporting this theory.
Weight loss was selected as a common symptom by 47% of health professionals
in this study, including by three quarters of dietitians and a quarter of medical
professionals, but few patient studies have reported on the prevalence of weight
loss. This is therefore an issue for NET patients requiring further exploration.
Dietitians were more likely to report weight loss as a common symptom than
other professions, which is expected due to weight management being a key

156
aspect of dietitian assessment and intervention. Nursing and medical
professionals were more likely to report common symptoms as fatigue, pain and
flushing, potentially reflecting these symptoms as their focus of assessment.
Our results have indicated that only 38% of health professionals perform
screening or assessment for malnutrition in NET patients themselves and 28%
reported no one screened for malnutrition in their health service. Results suggest
that there is a large proportion of NET patients not being formally screened for
malnutrition, and consequently malnutrition may be going unrecognised and
untreated. Malnutrition in cancer patients is associated with increased morbidity
and mortality, worsening quality of life, and increased health care costs [22–24].
NET patients with malnutrition are known to have a higher risk of complications
and mortality, and screening for malnutrition has been recommended for all NET
patients [14,15,25].
There is also inconsistency in the types of malnutrition screening tools used and
many are not using a validated tool. ESPEN recommends the use of validated
malnutrition screening and assessment tools, particularly those that consider a
combination of data on body weight, nutritional intake, inflammatory markers
and physical changes such as muscle or fat [26]. Issues unique to patients with a
NET with the potential to impact on nutrition include symptom burden
(diarrhoea, flushing), altered dietary habits and food intolerances, may not be
adequately captured using traditional nutrition screening tools. This study did
not explore the reason for use (or lack of) validated nutrition screening tools;
however, these nutrition issues unique to NETs may prompt health professionals
to provide individualised assessment instead. Adaptation of existing tools or
development of a nutrition screening tool designed and validated to identify the
specific nutritional issues and symptoms of people with a NET are therefore
required, along with guidelines for incorporating this into health professional
practice.

157
There was variation in the type of nutrition advice provided by health
professionals to NET patients; and dietitians, medical and nursing professionals
all reported providing nutrition advice to some degree. As expected, dietitians
provided a wider range of nutrition advice including advice on weight loss, food
intolerances, vitamins and symptoms; whereas doctors and nurses mostly
provided advice on symptoms. For the purpose of this survey, information was
not collected on the setting or context of this advice, but it would be useful to
explore this in future studies. Access to a dietitian may be limited for some NET
patients and therefore exploration of the medical and nursing role in nutrition
screening, information provision and dietitian referral is warranted, including
education for these professions on the importance of nutrition in the context of
a NET patient’s care.
Participants mostly reported a reliance on general oncology and nutrition
guidelines and commented on the lack of NET-specific nutrition guidelines.
General cancer nutrition guidelines may provide adequate information for the
management of nutrition issues common to a range of cancer patients such as
malnutrition and post-surgery management, but not issues specific to patients
diagnosed with a NET including carcinoid syndrome, NET-diarrhoea
management, malabsorption and vitamin deficiencies. Without NET-specific
nutrition guidelines, there is risk of misdiagnosis and variation in assessment and
management of these nutrition issues, as highlighted by results in this study.
In this survey the majority of health professionals indicated they felt nutrition
was important to address during a patient’s NET treatment, however, there was
large variation in response for this question, and for most of the other visual
analogue scale questions. This indicates that health professionals currently have
varied opinion about the importance and prevalence of nutrition issues amongst
NET patients. Several factors could have contributed to this variation including
country of work and organisational environment, their profession, and the type
of NET patients they are exposed to in their practice. This survey only asked

158
questions generally about all NETs so it would be worthwhile in future studies to
explore whether there are certain NET types or sub-groups that health
professionals believe are more likely to have nutrition issues or require nutrition
management. When asked about provision of routine nutrition advice
participants most frequently reported being given advice on diarrhoea and
bloating, which may indicate that these symptoms are considered a priority for
nutrition intervention. Diarrhoea and bloating were also amongst the symptoms
reported in this survey to impact most on dietary intake and weight loss, along
with nausea, loss of appetite and vomiting.
The circulation of survey invitations via organisation email listings and
newsletters was a limitation to this study, as health professionals are more likely
to respond to a survey if sent an individual invitation [27]. When recruiting for
this survey, individual email contacts were only available for a certain number of
health professionals. Due to the recruitment strategy it was also not possible to
report an exact response rate and therefore comment on the proportion of NET
health professionals that participated. There was a potential for selection bias in
this survey, in particular non-response bias, as the health professionals that
responded to the survey invitation may have more interest or knowledge in
nutrition and NETs. The international representation from various countries was
a strength of this study, however, there were only small numbers of respondents
from some areas including Europe and the United States. This potentially limits
the generalisability of results to these areas, particularly given the practices of
nutrition screening and assessment, and use of nutrition tools, may vary among
different countries. All efforts were made to recruit participants from Europe and
the United States using available contacts and resources within the recruitment
timeframe.
A strength of this study was the multidisciplinary sample of medical, nursing and
dietitian professionals. Whilst the medical profession had good representation in
this survey (42% of respondents), the majority worked in medical oncology (18 of

159
31) and only a few in other medical specialities including surgical oncology,
nuclear medicine, endocrinology and gastroenterology. This survey did not
explore barriers to nutrition screening practices and whether specific types of
NET patients were being prioritised for malnutrition screening and assessment,
by those health professionals performing screening in their practice. In other
studies organisational factors, insufficient time, knowledge of malnutrition risk
factors and appropriate screening practices, and a culture of avoidance have
been identified as barriers to assessment and management of cancer
malnutrition [28–31].
This paper presents the first summary of nutrition practices amongst an
international group of NET health professionals. Variation in the nutrition
screening and management practices of NET health professionals was
highlighted and it is possible that current available nutrition screening tools may
not be suitable to identify malnutrition and other nutrition issues specific to
patients with a NET. In this study health professionals reported a lack of NET-
specific nutrition guidelines, with many relying on general cancer guidelines to
inform their practice. These results both inform and offer an opportunity to
evaluate the priorities for health professional education and development of
NET-specific nutrition guidelines. Diarrhoea, fatigue and flushing were
highlighted throughout the survey results as a key problem for patients with a
NET. Guidelines specific for NET diarrhoea management are crucial to ensure it is
assessed and managed appropriately and should be an initial focus during
development of future NET clinical practice guidelines. Further research
evaluating the barriers and enablers to nutrition screening and advice would be
beneficial to guide health professional education. The development of future
NET nutrition clinical practice guidelines and a nutrition screening tool validated
for use with NET patients hence must be a priority.
References
[1] Kunz PL, Reidy-Lagunes D, Anthony LB, Bertino EM, Brendtro K, Chan JA,

160
et al. Consensus guidelines for the management and treatment of
neuroendocrine tumors. Pancreas 2013;42:557–77.
doi:10.1097/MPA.0b013e31828e34a4.
[2] Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, Caplin ME, et al.
Guidelines for the management of gastroenteropancreatic neuroendocrine
(including carcinoid) tumours (NETs). Gut 2012;61:6–32. doi:10.1136/gutjnl-
2011-300831.
[3] Kaupp-roberts S, Srirajaskanthan R, Ramage JK. Symptoms and Quality
of Life in Gastroenteropancreatic Neuroendocrine Tumours. EMJ Oncol
2015;3:34–40.
[4] Haugland T, Veenstra M, Vatn M, Wahl A. Improvement in Stress,
General Self-Efficacy, and Health Related Quality of Life following Patient
Education for Patients with Neuroendocrine Tumors: A Pilot Study. Nurs Res
Pract 2013;2013:695820. doi:10.1155/2013/695820; 10.1155/2013/695820.
[5] Van Der Horst-Schrivers ANA, Machteld Wymenga AN, Links TP,
Willemse PHB, Kemac IP, De Vries EGE. Complications of midgut carcinoid tumors
and carcinoid syndrome. Neuroendocrinology 2004;80:28–32.
doi:10.1159/000080737.
[6] Singh S, Granberg D, Wolin E, Warner R, Sissons M, Kolarova T, et al.
Patient-Reported Burden of a Neuroendocrine Tumor (NET) Diagnosis: Results
From the First Global Survey of Patients With NETs. J Glob Oncol 2017;3:43–53.
doi:10.1200/JGO.2015.002980.
[7] Fröjd C, Larsson G, Lampic C, von Essen L. Health related quality of life
and psychosocial function among patients with carcinoid tumours. A
longitudinal, prospective, and comparative study. Health Qual Life Outcomes
2007;5:18. doi:10.1186/1477-7525-5-18.
[8] Fiebrich H-B, Van Den Berg G, Kema IP, Links TP, Kleibeuker JH, Van
Beek AP, et al. Deficiencies in fat-soluble vitamins in long-term users of
somatostatin analogue. Aliment Pharmacol Ther 2010;32:1398–404.
doi:10.1111/j.1365-2036.2010.04479.x.

161
[9] Lind A, Wängberg B, Ellegård L. Vitamin D and vitamin B12 deficiencies
are common in patients with midgut carcinoid (SI-NET). Eur J Clin Nutr
2016;70:990–4. doi:10.1038/ejcn.2016.40.
[10] Pearman TP, Beaumont JL, Cella D, Neary MP, Yao J. Health-related
quality of life in patients with neuroendocrine tumors: an investigation of
treatment type, disease status, and symptom burden. Support Care Cancer
2016;24:3695–703. doi:10.1007/s00520-016-3189-z.
[11] Larsson G, Haglund K, Von Essen L. Distress, quality of life and strategies
to “keep a good mood” in patients with carcinoid tumours: patient and staff
perceptions. Eur J Cancer Care (Engl) 2003;12:46–57. doi:10.1046/j.1365-
2354.2003.00322.x.
[12] Singh S, Asa SL, Dey C, Kennecke H, Laidley D, Law C, et al. Diagnosis and
management of gastrointestinal neuroendocrine tumors: An evidence-based
Canadian consensus. Cancer Treat Rev 2016;47:32–45.
doi:10.1016/j.ctrv.2016.05.003.
[13] Qureshi SA, Burch N, Druce M, Hattersley JG, Khan S, Gopalakrishnan K,
et al. Screening for malnutrition in patients with gastro-entero-pancreatic
neuroendocrine tumours: a cross-sectional study. BMJ Open 2016;6:e010765.
doi:10.1136/bmjopen-2015-010765.
[14] Borre M, Dam GA, Knudsen AW, Grønbaek H. Nutritional status and
nutritional risk in patients with neuroendocrine tumors. Scand J Gastroenterol
2018;53:284–92. doi:10.1080/00365521.2018.1430848.
[15] Maasberg S, Knappe-Drzikova B, Vonderbeck D, Jann H, Weylandt KH,
Grieser C, et al. Malnutrition Predicts Clinical Outcome in Patients with
Neuroendocrine Neoplasia. Neuroendocrinology 2017;104:11–25.
doi:10.1159/000442983.
[16] Messick S. Validity of Psychological Assessment: Validation of Inferences
from Persons’ Responses and Performances as Scientific Inquiry into Score
Meaning. ETS Res Rep Ser 1994;1994:i–28. doi:10.1002/j.2333-
8504.1994.tb01618.x.

162
[17] Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, et
al. The European Organization for Research and Treatment of Cancer QLQ-C30: A
Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J
Natl Cancer Inst 1993;85:365–76. doi:10.1093/jnci/85.5.365.
[18] Yadegarfar G, Friend L, Jones L, Plum LM, Ardill J, Taal B, et al. Validation
of the EORTC QLQ-GINET21 questionnaire for assessing quality of life of patients
with gastrointestinal neuroendocrine tumours. Br J Cancer 2013;108:301–10.
doi:10.1038/bjc.2012.560.
[19] Cohen J. Statistical power analysis for the behavioral sciences. L.
Erlbaum Associates; 1988.
[20] Flick U. An introduction to qualitative research. London: Sage
Publications; 2002.
[21] Laing E, Kiss N, Michael M, Krishnasamy M. Nutritional complications
and the management of patients with gastroenteropancreatic neuroendocrine
tumours. Neuroendocrinology 2019. doi:10.1159/000503634.
[22] Arends J, Bodoky G, Bozzetti F, Fearon K, Muscaritoli M, Selga G, et al.
ESPEN Guidelines on Enteral Nutrition: Non-surgical oncology. Clin Nutr
2006;25:245–59. doi:10.1016/j.clnu.2006.01.020.
[23] Nitenberg G, Raynard B. Nutritional support of the cancer patient:
Issues and dilemmas. Crit Rev Oncol Hematol 2000;34:137–68.
doi:10.1016/S1040-8428(00)00048-2.
[24] Arends J, Bachmann P, Baracos V, Barthelemy N, Bertz H, Bozzetti F, et
al. ESPEN guidelines on nutrition in cancer patients. Clin Nutr 2017;36:11–48.
doi:10.1016/j.clnu.2016.07.015.
[25] Glazer ES, Stanko K, Ong ES, Guerrero MA. Decreased inpatient
mortality in obese patients with abdominal nets. Endocr Pract 2014;20:1309–14.
doi:10.4158/EP14203,OR.
[26] Arends J, Baracos V, Bertz H, Bozzetti F, Calder PC, Deutz NEP, et al.
ESPEN expert group recommendations for action against cancer-related
malnutrition. Clin Nutr 2017;36:1187–96. doi:10.1016/j.clnu.2017.06.017.

163
[27] Heerwegh D. Effects of Personal Salutations in e-mail Invitations to
Participate in a Web Survey. vol. 69. 2005.
[28] Cooper C, Burden ST, Cheng H, Molassiotis A. Understanding and
managing cancer-related weight loss and anorexia: insights from a systematic
review of qualitative research. J Cachexia Sarcopenia Muscle 2015;6:99–111.
doi:10.1002/jcsm.12010.
[29] Adams NE, Bowie AJ, Simmance N, Murray M, Crowe TC. Recognition by
medical and nursing professionals of malnutrition and risk of malnutrition in
elderly hospitalised patients. Nutr Diet 2008;65:144–50. doi:10.1111/j.1747-
0080.2008.00226.x.
[30] Green SM, James EP. Barriers and facilitators to undertaking nutritional
screening of patients: A systematic review. J Hum Nutr Diet 2013;26:211–21.
doi:10.1111/jhn.12011.
[31] Craven DL, Pelly FE, Isenring E, Lovell GP. Barriers and enablers to
malnutrition screening of community-living older adults: A content analysis of
survey data by Australian dietitians. Aust J Prim Health 2017;23:196–201.
doi:10.1071/PY16054.

164
6.2.5 Manuscript 2
Exploring vitamin testing and supplementation practices of international
health professionals managing neuroendocrine cancer patients
Erin Lainga,b*, Nicole Kissc,d, Meinir Krishnasamya,e,f, Karla Goughg, Michael
Michaelh,i,
aDepartment of Nursing, School of Health Sciences, The University of Melbourne,
305 Grattan Street, Melbourne VIC 3000, Australia
bNutrition and Speech Pathology Department, Peter MacCallum Cancer Centre,
Victorian Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC
3000, Australia
cInstitute for Physical Activity and Nutrition (IPAN), Deakin University, Geelong,
Australia,
dAllied Health Research, Peter MacCallum Cancer Centre, Victorian
Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC 3000,
Australia
eVictorian Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC
3000, Australia
fCentre for Cancer Research, The University of Melbourne, Grattan Street,
Melbourne VIC 3000, Australia
gCancer Experiences Research, Peter MacCallum Cancer Centre, Victorian
Comprehensive Cancer Centre, 305 Grattan Street, Melbourne VIC 3000,
Australia
hDepartment of Medical Oncology & Neuroendocrine Unit (ENETs COE), Peter
MacCallum Cancer Centre, Victorian Comprehensive Cancer Centre, 305 Grattan
Street, Melbourne VIC 3000, Australia

165
iThe Peter MacCallum Department of Medical Oncology, University of
Melbourne, Grattan Street, Melbourne VIC 3000, Australia
Abstract
Purpose
Neuroendocrine tumours (NET) and their treatment can lead to altered vitamin
synthesis and absorption, including risk of niacin and fat-soluble vitamin
deficiency. The current management of at-risk vitamins by NET health
professionals is unknown. This study aimed to explore the vitamin screening and
supplementation practices of NET health professionals and summarise current
international practices.
Methods
Multidisciplinary health professionals who regularly provide care for NET
patients, were invited to participate in an online survey. In two survey items,
participants were asked to report their vitamin screening and supplementation
practices, and reasons for this practice. General demographic information was
recorded.
Results
In total 73 health professionals completed the survey: 38 (52%) worked in
Australia and 14 (19%) in the United Kingdom. Most responses were provided by
dietitians (30%), medical oncologists (25%), and nurses (23%). Thirty eight
percent of participants reported screening for vitamin deficiencies in their
practice and 34% reported recommending vitamin supplementation to NET
patients. Vitamin B12, vitamin D and folate were the most commonly tested.
Reasons for not recommending vitamin screening or supplementation in practice
included uncertainty about how or what to screen/supplement, and not
believing this practice was part of their role.

166
Conclusion
This is the first description of vitamin screening and supplementation practices of
international NET health professionals. Results indicate that screening for
vitamin deficiencies is not common practice. Further research is required to
determine the optimal management of vitamin deficiencies in NET patients.
Introduction
Neuroendocrine tumours (NET) are a type of carcinoma typically found in the
gastrointestinal tract, pancreas and lung, often characterised by their propensity
to secrete hormones. The presence of a NET and their hormone secretion can
lead to various symptoms including diarrhoea, abdominal discomfort, fatigue and
flushing [1,2]. Although the incidence of NETs is relatively low, their prevalence is
higher than for other gastrointestinal cancers and there are increasing numbers
of people living with a NET and its associated symptoms. Hormonal
hypersecretion arising from functional NETs can inhibit nutrient absorption and
synthesis, and NET treatments such as surgery and somatostatin analogue (SSA)
therapy can lead to altered gut function and nutrition malabsorption.
Niacin deficiency has been reported in NET patients with carcinoid syndrome,
which is characterised by a cluster of symptoms including diarrhoea, fatigue,
abdominal discomfort and flushing caused by the hypersecretion of the hormone
serotonin [1,3,4]. When serotonin production is increased it displaces the
synthesis of niacin as both are derived from the amino-acid tryptophan [5–7].
The prevalence of niacin deficiency ranges from 28% to 45% in patients with
carcinoid syndrome or serotonin-producing NETs [8,9]. Patients with serotonin-
producing NETs also have significantly lower niacin levels than healthy controls
[9]. Niacin is available as an oral supplement on its own and in combination with
other B vitamins. Supplementation of niacin has been shown to correct niacin
deficiency in up to 86% of NET patients [9].

167
Fat-soluble vitamins A, E, D and K are at risk of deficiency in people with a NET,
particularly those who have undergone gastrointestinal surgery or being treated
with an SSA. Surgery to the small intestine and pancreas can alter the gut’s
absorption processes by reducing the release of bile and enzymes that aid in
absorption of fat and fat-soluble vitamins. SSA therapy is used to supress the
hormone secretion of NETs and subsequently reduce symptom burden. A by-
product of this can be the suppression of pancreatic hormone and enzyme
function, leading to pancreatic exocrine insufficiency and malabsorption of fat.
Up to 80% of patients with a mid-gut (ileal, jejunal, caecal) NET on long-term SSA
for longer than 18 months had deficiency of at least 1 fat-soluble vitamin
according to a study conducted by Fiebrich et al (2010) [10]. Vitamin D has been
the most commonly tested fat-soluble vitamin in the literature, and rates of
deficiency in NET patients are reported between 46-81% [10–15], which is
greater than the general population rates of 23% [16]. Oral vitamin D
supplementation is effective in increasing serum vitamin D in NET patients,
however, vitamin D supplementation may not improve bone density in some NET
patients [11,15].
The literature to date has focused on examining the prevalence of niacin and fat-
soluble vitamins, particularly vitamin D, amongst NET patients. Limited research
is available on risk of deficiency for other vitamins and trace elements. Few NET
clinical guidelines highlight the risk of vitamin deficiencies in NET patients [17],
and specific recommendations for vitamin testing and supplementation are
rarely included. Recent review articles have recommended testing of niacin and
fat-soluble vitamins in some NET patients [18–20], however, the vitamin
screening and supplementation practices of health professionals is currently
unknown. It would be beneficial to explore the health professional management
of vitamin deficiencies to determine whether this is common practice, if any
inconsistencies exist, and to allow specialist NET health professionals to provide
opinion about the need to screen and supplement at-risk vitamins. This
information would also aid the planning and development of clinical practice

168
guidelines advising the management of nutrition complications and vitamin
deficiencies in NET patients.
Aim and objectives
The main aim of this study was to describe health professional knowledge and
management of nutrition complications in NET patients. The secondary aim was
to summarise current international nutrition practices. The aim of this paper is to
report on health professional practices in regards to vitamin screening and
supplementation in NET patients.
Materials and Methods
Survey design and methodology
A customised online survey was developed for this study and invitations to
participate were distributed to NET health professionals via group email listings,
and through newsletters and websites of NET organisations. Multidisciplinary
NET clinicians, including medical oncologists, surgeons, radiation oncologists,
endocrinologists, gastroenterologists, nuclear medicine physicians, nurses,
dietitians and allied health clinicians, were eligible to participate if they worked
in a multidisciplinary NET referral centre. Details of the study methodology are
published in ‘Exploring international health professional knowledge and
management of nutritional complications in neuroendocrine cancer patients’
(Laing et al. 2020).
The 21-item, study-specific survey included a combination of closed-ended (tick
box, 14 items), open-ended (1 item) and visual analogue scale questions (6
items), and addressed several themes including: symptom prevalence and impact
on NET patients, extent of nutrition issues in NET patients, malnutrition
screening and assessment practices, vitamin screening and supplementation
practices, nutrition management practices and importance of nutrition. This
paper will report on responses relating to the theme of vitamin screening and

169
supplementation practices (2 items). Other themes and results have been
reported previously (Laing et al. 2020). A copy of the survey questions is attached
in Online Resource 1. The survey was anonymous with no identifying information
recorded about participants, and consent was assumed upon completion of the
survey. Demographic information including the participant’s geographical
location of work (country), their profession, length of time managing NET
patients (in years), and approximate number of NET patients managed per year,
was recorded. Ethics approval for this study was obtained from the Peter
MacCallum Cancer Centre Human Research Ethics Committee (EC00235) on April
20, 2017.
Statistical analysis
As the aim of this study was to explore health professional practices, descriptive
analysis was performed. Counts and percentages were used to summarise
participant characteristics and responses to the online survey. IBM SPSS Statistics
Version 23 (Chicago IL, USA) was used for descriptive analysis. Summarising
content analysis was used to code open text responses [21].
Results
Participants
Sixty-four NET health professionals were sent individual email invitations. The
number of health professionals who received a survey invitation via NET
organisations and newsletters was indeterminate. A total of 73 health
professionals completed the online survey between September 2017 and April
2018. Most participants worked in Australia (n = 38, 52%), the United Kingdom (n
= 14, 19%), Europe (n = 7, 10%) and the United States (n = 7, 10%). Participant
characteristics are summarised in Table 1. The majority of participants were
medical professionals (42%, n = 31), dietitians (30%, n = 22) or nurses (23%, n =
17).

170
Table 1 Demographics of survey participants (N = 73), data are counts and percentages
Speciality
Dietitian 22 (30)
Medical Oncology 18 (25)
Nursing 17 (23)
Registered Nurse (RN)
Nurse Practitioner (NP)
Clinical Nurse Consultant (CNC)
Clinical Nurse Specialist (CNS)
Other Nurse
4 (5)
2 (3)
5 (7)
5 (7)
1 (1)
Surgical Oncology 3 (4)
Nuclear Medicine 3 (4)
Endocrinology 3 (4)
Other Allied Health 3 (4)
Radiation Oncology 2 (3)
Gastroenterology 2 (3)
Estimated number of NET patients managed per year
<10 20 (27)
10 - 25 17 (23)
26 – 50 10 (14)
51 – 100 10 (14)
>100 16 (22)
Estimated years managing NET patients
<1 year 3 (4)
1 – 3 years 16 (22)
4 – 6 years 17 (23)
7 – 10 years 15 (21)
171
Speciality
>10 years 22 (30)
Vitamin screening and supplementation practices
A third of participants (38%, n = 28) reported screening for vitamin deficiencies in
NET patients and a similar number reported to recommend vitamin
supplementation (34%, n = 25). Dietitians were most likely to perform vitamin
screening (55%, n = 12) followed by medical professionals (36%, n = 11) and
nurses (29%, n = 5). Vitamins that were most commonly screened for included
vitamin B12, vitamin D, folate and iron (Table 2). Niacin (vitamin B3) screening
was performed by 32% (n = 9) of participants and screening of fat-soluble
vitamins ranged from 18 - 43%. Vitamin screening and supplementation practices
for each discipline group are summarised in Figure 1 and Figure 2.
Dietitians were more likely to screen for niacin, the fat-soluble vitamins (A, E, D,
K) and zinc; and recommend supplementation of niacin, vitamin D and
multivitamin, than other disciplines. Four participants reported screening for
‘other’ vitamins and minerals not listed in the survey, these included selenium (n
= 3), magnesium and copper (n = 1) and one participant reported testing clotting
to give an indication of vitamin K status.
In regard to vitamin supplementation, the vitamins most commonly
supplemented by participants included vitamin D (60%, n=15), niacin (B3) (52%,
n=13) and vitamin B12 (36%, n=9) (Table 2). Seven participants selected ‘other’ in
regard to their vitamin supplementation practices. Of these, six reported only
providing supplementation after testing results or if deficiency is present, and
three participants reported recommending a combined vitamin B supplement
(i.e. combination of multiple B vitamins). One participant commented that they
only supplement vitamins in certain conditions; for example, niacin

172
supplementation only if the patient is diagnosed with carcinoid syndrome and
vitamin B12 supplementation if the patient has stomach/ileal problems.
Table 2 Vitamins screened and supplemented by NET health professionals, data are counts and
valid percentages (multiple responses allowed)
Vitamin Screened for (n = 28) Supplemented (n = 25)
Vitamin B12 22 (78.6) 9 (36)
Vitamin D 21 (75) 15 (60)
Folate 20 (71.4) 5 (20)
Iron 17 (60.7) 3 (12)
Vitamin A 12 (42.9) 4 (16)
Vitamin E 10 (35.7) 4 (16)
Niacin (B3) 9 (32.1) 13 (52)
Zinc 6 (21.4) 3 (12)
Vitamin K 5 (17.9) 4 (16)
Other 4 (14.3) 7 (28)

173
Figure 1 Do you screen for any of the following vitamin deficiencies?
*Multiple responses allowed
Figure 2 Do you recommend supplementation of any of the following vitamins?
*Multiple responses allowed
0
10
20
30
40
50
60
70
80
90
100
Niacin Vit A Vit D Vit E Vit K Iron Zinc VitB12
Folate Other
Medical Nursing
0
10
20
30
40
50
60
70
80
90
100
Medical Nursing

174
Barriers to vitamin screening and supplementation
Sixty-one percent (n = 45) of participants reported not screening for vitamin
deficiencies, and 66% (n = 48) reported not recommending vitamin
supplementation to NET patients. Barriers to screening or supplementing
vitamins in NET patients are summarised in Table 3. Uncertainty about what
vitamin deficiencies to screen for/supplement to recommend, and feeling it is
not their role to screen/supplement were the most selected reasons.
Table 3 Barriers to vitamin screening and supplementation, data are counts and valid
percentages
Barrier Vitamin screening
(n = 44)
Vitamin supplementation
(n = 48)
It is not my role to do this 11 (25) 10 (21)
I refer patients to another clinician who will do this/provide supplementation
8 (18) 9 (19)
I am unsure what vitamin deficiencies to screen for/ what supplementation to recommend
12 (27) 19 (39)
Other 13 (30) 10 (21)
Other reasons for not screening vitamins were provided by 13 participants and
included: unsure how to screen (n = 2), limited evidence available on reliability of
micronutrient testing (n = 1), not aware of what to screen for (n = 1), will refer
concerns about vitamins to the oncologist (n= 1), not enough time (n = 1), not as
a routine (n = 1), is not wished for in our clinic (n = 1), no labs ordered (n = 1) and
blood markers are not a good way to assess deficiencies (n = 1). Two participants
reported only screening vitamin status if the patient was symptomatic, and one
175
participant reported reviewing the patient’s diet history before determining the
need for vitamin testing. Of the 10 participants reporting ‘other’ barriers to
vitamin supplementation in NET patients, five indicated that they would only
supplement vitamins in the case of deficiency, and three indicated that they
would only supplement vitamins in the case of certain symptoms such as chronic
diarrhoea. Two participants commented that they would assess the adequacy of
a patient’s diet before determining their need for supplementation.
Discussion/Conclusion
This is the first study to explore the screening and management of vitamin
deficiencies amongst NET health professionals. Results show that screening for
vitamin deficiencies and vitamin supplementation is inconsistent, and this is
despite literature indicating that vitamin deficiencies are prevalent in NET
patients [8–11,13,14]. Uncertainty about which vitamins to screen and what
supplementation to recommend were common barriers to these practices. Gaps
in health professional knowledge could be addressed by the inclusion of
information on potential vitamin deficiencies in NET clinical practice guidelines.
Review articles have analysed published prevalence data and recommended
screening for at-risk vitamins in some NET patients [19,20].
Niacin supplementation is recommended for patients with carcinoid syndrome or
increased serotonin production, and if deficiency is suspected [19,20].Of the
participants in this survey who recommended vitamin supplementation to NET
patients, niacin was commonly reported, indicating that some participants may
be aware of this recommendation. However, when taking into account all
participant responses only 17% recommended niacin supplementation to NET
patients. Supplementation of niacin deficiency was more common practice than
niacin screening. Measurement of urinary niacin excretion is the most reliable
method for niacin status testing [22], however, it requires a 24-hour urine
collection which may be considered burdensome. The availability of pathology

176
centres equipped to analyse niacin status is also limited. It is worth exploring in
future studies whether niacin testing is necessary prior to supplementation or
whether supplementation of at-risk patients (i.e. patients with carcinoid
syndrome) is adequate and appropriate. As little as 5% of NET patients show
symptoms of clinical niacin deficiency or pellagra [23,24]. Therefore,
identification and documentation of clinical reasons for niacin deficiency rather
than symptomatology is important to guide practice.
Testing for fat-soluble vitamins is recommended at least yearly for patients post
small bowel resection or on long-term SSA [20,25]. Vitamin D was more
commonly tested and supplemented by participants in this study than the other
fat-soluble vitamins. The reasons for this were not explored but may be due to
increased awareness and availability of vitamin D testing and analysis. Most
studies looking at prevalence of fat-soluble vitamin deficiencies in NET patients
have tested vitamin D rather than the other or all fat-soluble vitamins [11–14].
Vitamin B12 was the most commonly tested vitamin by participants in this study.
Only one small study has reported on the prevalence of vitamin B12 deficiency,
which was 32% in a cohort of NET patients post-small bowel resection [11].
Overall results indicate that vitamin deficiencies in patients with a NET are
potentially going undetected, particularly in the case of niacin and fat-soluble
vitamins. Whilst mild deficiencies may not impact patients symptomatically,
undiagnosed deficiencies long-term can lead to severe clinical syndromes
including pellagra in the case of niacin deficiency, characterised by dermatitis,
cognitive changes and diarrhoea; decreased bone density and osteoporosis due
to vitamin D deficiency; and night blindness and immune system defects in the
case of vitamin A deficiency [5,6,26–28]. In severe cases these vitamin deficiency
syndromes can also lead to death [28].
The international representation of multidisciplinary NET health professionals is
a strength of this study and results provide insight into practices of NET specialist

177
doctors, nurses and dietitians. A quarter of participants reported not believing it
was their role to screen for vitamin deficiencies when consulting with NET
patients. Further exploration of the discipline with which vitamin screening and
management best aligns with and appropriate multidisciplinary pathways for the
management of vitamin deficiency is needed. This information would aid in the
development of guidelines for vitamin deficiency prevention and management in
NET patients. Limitations to this study include partial recruitment via
organisation email listings and newsletters, and potential non-response bias, i.e.
respondents to the survey were possibly more likely to have an interest in
nutrition. As this was a structured survey we were unable to explore the
rationale for participant responses in detail. As the literature highlights, there are
particular NET types that may be more at risk of vitamin deficiencies than others.
This study was unable to distinguish between health professionals who screened
all NET patients for vitamin deficiencies, and those who screened on some
occasions or only certain patients. Ten participants did report that they would
consider either existing deficiency, symptoms or dietary adequacy before
supplementing vitamins, which indicates these may be useful considerations. In
combination with published prevalence data, research exploring the conditions
or factors that may prompt health professionals to perform vitamin screening
and supplementation would be useful to confirm the type of NET patients most
at risk of vitamin deficiencies and their complications.
Less than half of NET health professionals in this study considered vitamin testing
and supplementation whilst managing NET patients. This is despite literature
highlighting the prevalence of niacin and fat-soluble vitamin deficiency in NET
patients as high as 45-80%. Patient presentation (symptoms, diet), health
professional knowledge of at-risk vitamins, and knowledge of appropriate
screening and supplementation methods are factors affecting health professional
management of vitamin deficiencies. Results indicate that vitamin deficiencies in
NET patients risk under recognition without appropriate evidence-based
guidelines in place. Research exploring the patients most at risk of vitamin

178
deficiencies, and the optimal dosing required to prevent and correct vitamin
deficiencies, is warranted to contribute to future clinical practice guidelines. It
would also be helpful to establish a consensus amongst health professionals as
to who is responsible for vitamin screening and supplementation so that
education can be targeted correctly.
References
[1] Ramage JK, Ahmed A, Ardill J, Bax N, Breen DJ, Caplin ME, et al.
Guidelines for the management of gastroenteropancreatic neuroendocrine
(including carcinoid) tumours (NETs). Gut 2012;61:6–32. doi:10.1136/gutjnl-
2011-300831.
[2] Kaupp-roberts S, Srirajaskanthan R, Ramage JK. Symptoms and Quality
of Life in Gastroenteropancreatic Neuroendocrine Tumours. EMJ Oncol
2015;3:34–40.
[3] Pearman TP, Beaumont JL, Cella D, Neary MP, Yao J. Health-related
quality of life in patients with neuroendocrine tumors: an investigation of
treatment type, disease status, and symptom burden. Support Care Cancer
2016;24:3695–703. doi:10.1007/s00520-016-3189-z.
[4] Modlin I, Moss S, Oberg K, Padbury R, Hicks R, Gustafsson B, et al.
Gastrointestinal neuroendocrine (carcinoid) tumours: current diagnosis and
management. Med J Aust 2010;193:46–52.
[5] Fleischmajer R, Hyman AB. Clinical Significance of Derangements of
Tryptophan Metabolism. Arch Dermatol 1961;84:563.
doi:10.1001/archderm.1961.01580160027003.
[6] Castiello RJ, Lynch PJ. Pellagra and the Carcinoid Syndrome. Arch
Dermatol 1972;105:574. doi:10.1001/archderm.1972.01620070046016.
[7] Bender DA. Biochemistry of tryptophan in health and disease. Mol
Aspects Med 1983;6:101–97.

179
[8] Shah GM, Shah RG, Veillette H, Kirkland JB, Pasieka JL, Warner RRP.
Biochemical assessment of niacin deficiency among carcinoid cancer patients.
Am J Gastroenterol 2005;100:2307–14. doi:10.1111/j.1572-0241.2005.00268.x.
[9] Bouma G, Van Faassen M, Kats-Ugurlu G, de Vries EGE, Kema IP,
Walenkamp AME. Niacin (Vitamin B3) Supplementation in Serotonin Producing
Neuroendocrine Tumor Patients. Neuroendocrinology 2016;103:489–94.
doi:10.1159/000440621.
[10] Fiebrich H-B, Van Den Berg G, Kema IP, Links TP, Kleibeuker JH, Van
Beek AP, et al. Deficiencies in fat-soluble vitamins in long-term users of
somatostatin analogue. Aliment Pharmacol Ther 2010;32:1398–404.
doi:10.1111/j.1365-2036.2010.04479.x.
[11] Lind A, Wängberg B, Ellegård L. Vitamin D and vitamin B12 deficiencies
are common in patients with midgut carcinoid (SI-NET). Eur J Clin Nutr
2016;70:990–4. doi:10.1038/ejcn.2016.40.
[12] Motylewska E, Gawronska J, Niedziela A, Melen-Mucha G, Lawnicka H,
Komorowski J, et al. Somatostatin Analogs and Tumor Localization Do Not
Influence Vitamin D Concentration in Patients with Neuroendocrine Tumors.
Nutr Cancer 2016;68:428–34. doi:10.1080/01635581.2016.1152387.
[13] Massironi S, Zilli A, Bernasconi S, Fanetti I, Cavalcoli F, Ciafardini C, et al.
Impact of Vitamin D on the Clinical Outcome of Gastro-Entero-Pancreatic
Neuroendocrine Neoplasms: Report on a Series from a Single Institute.
Neuroendocrinology 2017;105:403–11. doi:10.1159/000456619.
[14] Robbins HL, Symington M, Mosterman B, Goodby J, Davies L, Dimitriadis
GK, et al. Supplementation of Vitamin D Deficiency in Patients with
Neuroendocrine Tumors Using Over-the-Counter Vitamin D3 Preparations. Nutr
Cancer 2018;70:748–54. doi:10.1080/01635581.2018.1470650.
[15] de Hosson LD, Stelwagen J, Bouma G, Sijtema B, Huitema S, van Faassen
HJR, et al. Towards optimal personalized diet and vitamin supplementation in

180
NET patients. Endocr Relat Cancer 2018;25:L23–6. doi:10.1530/ERC-17-0549.
[16] Australian Health Survey: Biomedical results for nutrients, 2011 - 2012.
Vitamin D. Aust Bur Stat 2014.
http://www.abs.gov.au/ausstats/[email protected]/Lookup/4364.0.55.006Chapter20020
11-12 (accessed November 4, 2016).
[17] Pavel M, Valle JW, Eriksson B, Rinke A, Caplin M, Chen J, et al. ENETS
Consensus Guidelines for the Standards of Care in Neuroendocrine Neoplasms:
Systemic Therapy - Biotherapy and Novel Targeted Agents. Neuroendocrinology
2017;105:266–80. doi:10.1159/000471880.
[18] Altieri B, Barrea L, Modica R, Muscogiuri G, Savastano S, Colao A, et al.
Nutrition and neuroendocrine tumors: An update of the literature. Rev Endocr
Metab Disord 2018;19:159–67. doi:10.1007/s11154-018-9466-z.
[19] Clement DS, Tesselaar ME, van Leerdam ME, Srirajaskanthan R, Ramage
JK. Nutritional and vitamin status in patients with neuroendocrine neoplasms.
World J Gastroenterol 2019;25:1171–84. doi:10.3748/wjg.v25.i10.1171.
[20] Laing E, Kiss N, Michael M, Krishnasamy M. Nutritional complications
and the management of patients with gastroenteropancreatic neuroendocrine
tumours. Neuroendocrinology 2019. doi:10.1159/000503634.
[21] Flick U. An introduction to qualitative research. London: Sage
Publications; 2002.
[22] NHMRC NH and MRC. Niacin. Nutr. Ref. Values Aust. New Zeal. Incl.
Recomm. Diet. Intakes, 2006, p. 79–84.
[23] Hegyi J, Schwartz RA, Hegyi V. Pellagra: dermatitis, dementia, and
diarrhea. Int J Dermatol 2004;43:1–5.
[24] Bax ND, Woods HF, Batchelor A, Jennings M. Clinical manifestations of
carcinoid disease. World J Surg 1996;20:142–6.
[25] Clement DSVM, Tesselaar MET, Leerdam ME van, Srirajaskanthan R,
Ramage JK. Nutritional and vitamin status in patients with neuroendocrine

181
neoplasms. World J Gastroenterol 2019;25:1171–84.
doi:10.3748/wjg.v25.i10.1171.
[26] Nowson CA, McGrath JJ, Ebeling PR, Haikerwal A, Daly RM, Sanders KM,
et al. Vitamin D and health in adults in Australia and New Zealand: a position
statement. Med J Aust 2012;196:686–7. doi:10.5694/mja11.10301.
[27] West KP, Darnton-Hill I. Vitamin A Deficiency. Nutr. Heal. Dev. Ctries.,
Totowa, NJ: Humana Press; 2008, p. 377–433. doi:10.1007/978-1-59745-464-
3_13.
[28] Bell HK, Poston GJ, Vora J, Wilson NJE. Cutaneous manifestations of the
malignant carcinoid syndrome. Br J Dermatol 2005;152:71–5.
doi:10.1111/j.1365-2133.2004.06273.x.


183
Chapter 7: Managing nutritional issues in NETs from a
health professional point of view
7.1 Introduction
This chapter presents data from a series of qualitative focus groups undertaken with
NET health professionals. The focus group data offer in-depth insight to enable further
elaboration and understanding of the quantitative survey data presented in Chapter 6.
Therefore, questions posed to focus group participants aligned with questions included
in the quantitative health professional survey. The ability to bring together both data
sets in this way demonstrates the benefit of undertaking a mixed-methods study in
Phase 2 of the PhD study.
Results of an international health professional survey discussed in Chapter 6 showed
inconsistencies in practice among a multidisciplinary sample of health professionals
from different countries. Data indicated that only a third of NET health professionals
screen for malnutrition and vitamin deficiency when consulting with NET patients, and
nutrition advice is focused primarily on symptom management rather than other
issues such as weight loss, malnutrition or food intolerances. Dietitians, as expected,
were more likely than other professions (doctors, nurses) to provide comprehensive
advice on nutrition issues, including a combination of advice on weight loss, vitamin
deficiency and symptoms. In the survey, NET health professionals were able to identify
common symptoms experienced by NET patients (diarrhoea, fatigue, abdominal
discomfort) which aligned with published symptom prevalence data. This survey
identified some barriers to vitamin screening practices, including poor knowledge of
what to screen for, and belief that this practice was the responsibility of another
health professional. However, the survey was mostly limited to quantitative responses,
and therefore factors contributing to nutrition knowledge and practices among NET
health professionals were unable to be explored or understood in-detail.

184
To address this limitation and provide a comprehensive summary of NET health
professional practices in regard to nutrition, a series of qualitative focus groups were
undertaken to generate rich insight into factors influencing nutrition practices. The
focus groups were undertaken at one study site with a purposive sample of
multidisciplinary NET health professionals. Focus group questions were aligned with
the topics addressed in the health professional survey: symptom prevalence and
impact on nutrition, nutrition screening and assessment practices, use of evidence-
based guidelines, provision of nutrition advice; to ensure in-depth exploration of these
aspects of nutrition screening and management. Chapter 7 describes the methodology
and insights gained from the NET health professional focus groups.
7.2 Aims and Objectives
7.2.1 Aim
To explore and describe health professional knowledge and management of nutrition
complications in patients living with/diagnosed with a NET, in order to summarise
current health professional nutrition-related practices and generate data to contribute
to future NET-specific nutrition clinical practice guidelines.
7.2.2 Objectives
Main objectives
a. To describe current knowledge of nutritional complications amongst health
professionals working with patients diagnosed with a NET
b. To describe current nutrition management practices amongst health
professionals working with patients diagnosed with a NET

185
Secondary objectives
i. To describe similarities and differences in practice amongst health
professionals working with patients with a NET in regard to screening and
management of nutrition issues
ii. To explore whether there is a difference between nutrition issues reported
by patients with GEP NET and those described by health professionals caring
for patient diagnosed with a NET
7.3 Methodology
7.3.1 Mixed-methods approach
Quantitative results from the health professional survey described in Chapter 6
provide a summary of the prevalence of nutrition-related practices, including
malnutrition and vitamin screening and the provision of nutrition advice to patients
diagnosed with a NET. Survey methodology allowed the capture of quantitative data
from a large cohort of multidisciplinary NET health professionals on an international
scale, but exploration of barriers and enablers to knowledge and practice, as well as
opinion regarding the optimal nutritional management of patients diagnosed with a
NET was limited by the use of a structured survey. Utilisation of one research method
only, i.e. quantitative methodology, enables a description of health professional
responses and practices, but also limits data to structured responses, without
providing context or reasoning behind their responses. The addition of qualitative
methodology, where aims, objectives and questioning align with the quantitative
methodology, enables further in-depth exploration of issues identified in the initial
survey, and whether qualitative results support those found in the quantitative study.
Therefore, focus groups were conducted with a sample of NET health professionals to
enable in-depth, qualitative exploration of these issues, and to identify opportunity for
future pathways for optimising the nutritional management of patients diagnosed with

186
a NET. Focus groups are useful to generate and explore ideas, thoughts, attitudes and
experiences in relation to a particular topic among a group of people (Plummer, 2017).
Discussion between participants encourages elaboration and justification of ideas and
has the potential to reveal more about participant’s knowledge and reasons for
thinking than individual interviews (Plummer, 2017). In addition to the data generated
by the survey described in Chapter 6, focus groups enabled exploration of similarities
and differences in opinion, and generation of new ideas and strategies for nutritional
screening and management of NETs among health professionals.
A purposive sample of multidisciplinary health professionals working in the NET unit at
the study site, were approached to participate in focus groups. A multidisciplinary
sample of participants was sought to explore similarities and differences in opinions
between different health professionals, and to generate ideas and discussion regarding
nutritional issues in patients diagnosed with a NET, within a multidisciplinary setting
similar to that of a NET unit. Focus group participants were recruited from one study
site only – Peter MacCallum Cancer Centre. Attempts were made to recruit
participants from the second study site, but it was not possible to undertake focus
groups at the second site within a timely manner due to clinical pressures and
therefore participants from this site were not included.
7.3.2 Participants
Multidisciplinary health professionals working in the NET unit at Peter MacCallum
Cancer Centre were invited to participate in a focus group via email. A purposive
sampling approach was taken to ensure health professionals involved were
experienced in the management of NETs, and a varied representation of different
disciplines was achieved. Health professionals were eligible for inclusion if they had
experience working regularly with NET patients (worked within the NET unit at Peter
Mac for >1 year) and were of one of the following disciplines: medical oncologist,
surgical oncologist, radiation oncologist, endocrinologist, gastroenterologist, nuclear

187
medicine physician, allied health (psychologist, psychiatrist, physiotherapist, social
worker, dietitian).
A Participant Information and Consent Form was sent to eligible health professionals
via email, with details regarding the study and the proposed focus groups. Health
professionals were asked to return an email to the lead researcher (PhD student), with
the signed consent form attached, if they agreed to participate. Focus groups were
then scheduled once consent was obtained from a minimum of ten health
professionals (to ensure adequate numbers for a meaningful focus group). An attempt
was made to include a minimum of three participants in each focus group (in addition
to the facilitators). Attempts were made to ensure a multidisciplinary sample of health
professionals in each focus group where possible. If a health professional provided
consent but was unable to participate in a scheduled focus group, they were offered
an individual phone interview with the lead researcher that addressed the same
questions as those addressed in the focus groups.
7.3.3 Focus group facilitation
Focus groups were facilitated by the lead researcher (PhD student) and one additional
facilitator who was external to the research team, for the purpose of monitoring and
addressing potential bias, as the lead researcher was known to some of the
participants. The lead researcher was responsible for asking participants the schedule
of questions (Appendix 5), whilst both facilitators asked follow-up or probing questions
as appropriate/required. At the end of the focus group, both facilitators reflected
together on the session to ensure that the lead researcher had not influenced the flow
or content of responses, and to check that the key aims of the focus group had been
achieved.
7.3.4 Focus group questions
Proposed questions for focus groups were established after completion of a
comprehensive review of relevant literature (literature review published in Chapter 1).

188
Further revision of questions occurred after review of results of the health professional
online survey described in Chapter 6. The focus group questions and schedule is
included in Appendix 5. Based on the literature review and survey responses,
questions were designed to address three key themes: the importance of nutrition
within the overall context of a NET patients care, screening and management of
malnutrition and vitamin deficiencies in NET patients, provision of nutrition advice. De-
identified demographic information was collected from each participant at the
commencement of a focus group or interview, including discipline (area of speciality),
length of time working with NET patients, and average number of NET patients they
manage per year.
During the focus groups, the lead facilitator proposed each question to participants as
outlined in the schedule (Appendix 5). As appropriate during the focus groups, further
probing questions were asked of participants to seek clarity or elaboration about
issues or concepts they were speaking about. An example of this probing is provided
below:
“There’s been a couple of points about diet changing or patients wanting to change
their diet to manage diarrhoea. In what way have they reported making changes in
that regard? Do you have any examples?”
7.3.5 Data management and Content analysis
Focus groups were audio recorded and audio data were stored electronically, and
password protected. Audio data were transcribed verbatim by a party external to the
research team. Analysis of transcriptions was undertaken by the lead researcher (PhD
student) and another researcher with qualitative research experience, who was
external to the research team.
A process of content analysis was applied to the focus group data as the intent was to
use a deductive approach, where analysis of focus group data was guided by evidence
from existing literature (as presented in Chapter 1), and results from the quantitative

189
health professional survey discussed in Chapter 6. Initial content analysis was
undertaken based upon a question-by-question format (Krueger, 2002), using the eight
key questions proposed to participants. The main purpose of focus groups was to
generate additional in-depth data relating to key topics of interest proposed in the
health professional survey. Therefore, initial content analysis of question responses
was performed to summarise and explore health professional practices in relation to
key topics, that were also explored in the Health professional survey (Chapter 6), that
is: health professional perceived occurrence and importance of nutritional
complications among NET patients (Questions 1, 2 and 3), malnutrition screening and
management practices (Question 4), vitamin deficiency screening and management
practices (Question 5), provision of nutrition advice (Question 6), and the use and
availability of evidence-based guidelines (Question 7). Data from transcripts were
coded against these questions using manifest content analysis, in order to summarise
responses based upon topics of interest and to identify commonality in responses to
questions.
Both researchers then re-visited the transcriptions and undertook further content
analysis, using a latent analytical approach, to identify emerging themes across all
health professional focus groups and interviews. A latent analytical approach seeks to
examine underlying ideas, assumptions and concepts that inform the content of the
data (Braun and Clarke, 2006). The intent of latent content analysis in this study was to
generate themes relating to the experiences of health professionals that influence
their practice and decisions regarding nutrition-related complications in NETs. This
approach enabled in-depth exploration and interpretation of the reasoning and
barriers behind nutrition-related practices, thereby contributing to the aim of
generating data that can inform future NET-specific nutrition guidelines. The content
analytical approach is summarised in Figure 7.1.

190
Figure 7.1 Focus group content analysis
Manifest content analysis
Coding against topics:
1) Health professional perceived occurrence and
importance of nutritional complications among NET
patients
2) Malnutrition screening and management practices
3) Vitamin deficiency screening and management
practices
4) Provision of nutrition advice
5) Use and availability of evidence-based guidelines
Related question:
Questions 1, 2, and 3
Question 4
Question 5
Question 6
Question 7
Latent content analysis
Health professional experience
and influential factors of their
nutrition-related knowledge and
practices
Themes

191
Descriptive statistics were used to report participant demographic data.
7.4 Results
7.4.1 Participant characteristics
Thirteen of 18 health professionals working in the NET unit at Peter Mac took part in
either a focus group or phone interview in July 2018. Three focus groups were
conducted, with a range of two to five participants in each group. All focus groups
were scheduled with a minimum of three participants, however, one participant had to
reschedule their attendance at last minute and therefore one group was conducted
with only two participants. Participant characteristics are described in Table 7.1. There
was a range of different professions represented in the focus groups and interviews.
Nine of thirteen participants reported working with NET patients for at least five years,
and nine reported managing over 50 NET patients per year on average (Table 7.1).
Table 7.1 Focus group participant characteristics
Characteristic n
Discipline
NET nurse 3
Medical oncologist 3
Surgeon 2
Nuclear medicine physician 2
Endocrinologist 1
Dietitian 2
Number of years working with NET patients, n (%)
< 1 year 1
1-2 Years 3
2-5 years 0

192
5-10 years 7
Number of years working with NET patients, n (%)
>10 years 2
Number of NET patients managed per year, n (%)
<10 1
10-20 3
20-50 0
50-100 6
>100 3
7.4.2 Results of initial content analysis
Responses to the each of the key questions proposed during the focus group were
summarised (manifest content analysis) and then reviewed by two researchers to
undertake latent content analysis to identify strong and recurring themes in the data
set.
Through a process of manifest content analysis there was considerable similarity in the
majority of responses to each question posed to focus group participants. A summary
of initial coding per topic area/question is provided in Table 7.2.

193
Table 7.2 Results of initial coding per topic area
Topic area Related question(s)
Summary of responses
Health professional
perceived occurrence and
importance of nutritional
complications among NET
patients
1, 2 and 3 - Responses varied when discussing if
nutrition was considered important
to patients, some believed it was
very important, others believed it
was less important that other issues
such as prognosis, treatment and
symptoms
- Symptom management was
considered by the majority to be
very important to address in NET
patients, and health professionals
said that symptoms (e.g. diarrhoea,
abdominal pain, bloating, weight
loss) often contributed to nutrition
issues
- The majority discussed that dietary
restriction and food intolerances
were common among NET patients
- The majority discussed that nutrition
issues, e.g. weight loss, malnutrition,
dietary restriction, impacted
negatively on patient quality of life
- The majority discussed that
malnutrition and weight loss is less
common in NETs than other
gastrointestinal cancers, but did
exist

194
Topic area Related question(s)
Summary of responses
- Malnutrition and weight loss were
considered issues mostly for patients
at end of life, with high-grade (grade
3) NET, and progressive disease
- Weight loss was considered less of
an issue for patients who were
undergoing PRRT, and who had
improved symptoms from their
treatment
Malnutrition screening and
management practices
4 - The majority said they did not
regularly or systematically screen for
malnutrition in their practice
- General questions to patients about
weight change or symptoms were
more common than routine
malnutrition screening, or use of a
validated nutrition screening tool
- Some health professionals said that
routine nutrition screening processes
in NETs could be improved, and
should form part of usual care
Vitamin deficiency screening
and management practices
5 - The majority of health professionals
did not screen for vitamin deficiency
in NET patients
- Some health professionals said it
was the responsibility of the dietitian
to prompt or perform screening for
vitamin deficiency
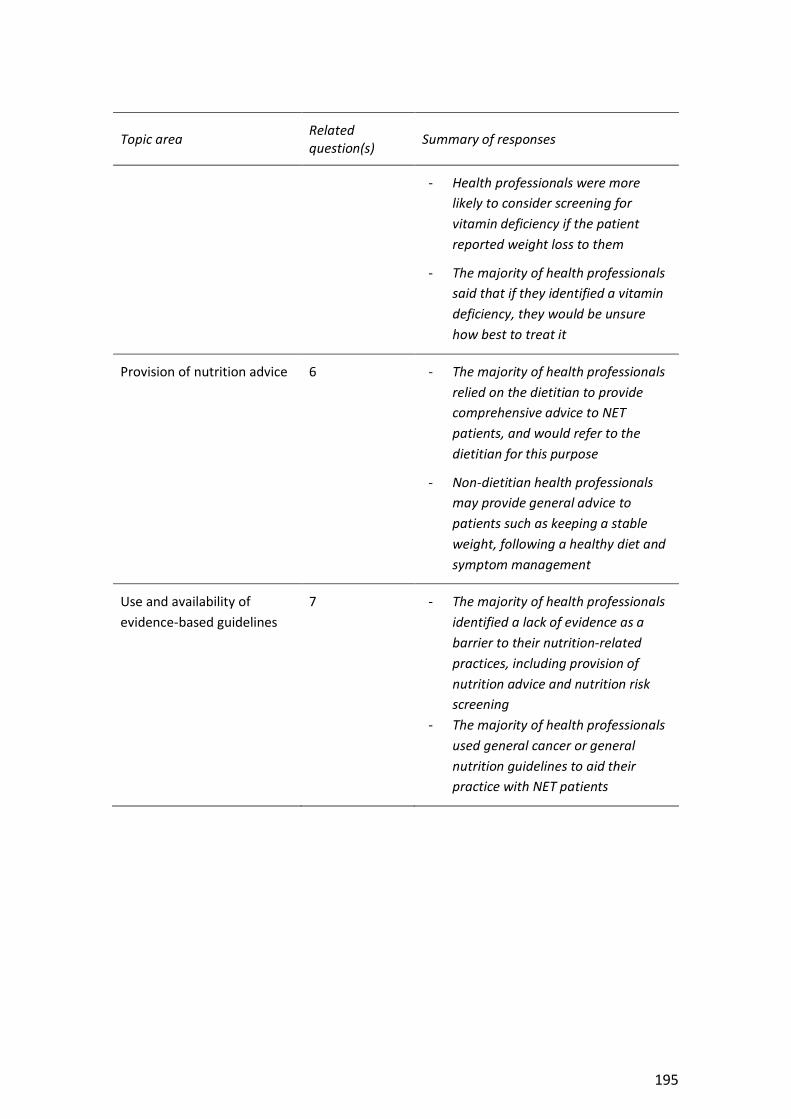
195
Topic area Related question(s)
Summary of responses
- Health professionals were more
likely to consider screening for
vitamin deficiency if the patient
reported weight loss to them
- The majority of health professionals
said that if they identified a vitamin
deficiency, they would be unsure
how best to treat it
Provision of nutrition advice 6 - The majority of health professionals
relied on the dietitian to provide
comprehensive advice to NET
patients, and would refer to the
dietitian for this purpose
- Non-dietitian health professionals
may provide general advice to
patients such as keeping a stable
weight, following a healthy diet and
symptom management
Use and availability of
evidence-based guidelines
7 - The majority of health professionals
identified a lack of evidence as a
barrier to their nutrition-related
practices, including provision of
nutrition advice and nutrition risk
screening
- The majority of health professionals
used general cancer or general
nutrition guidelines to aid their
practice with NET patients

196
Topic area Related question(s)
Summary of responses
- Some health professionals identified
a need for NET-specific nutrition
guidelines
- In the absence of NET-specific
nutrition guidelines, health
professionals discussed relying on
referral to a dietitian in their health
centre to aid in nutrition
management of patients
7.4.3 Results of latent content analysis
Latent content analysis was conducted after initial manifest content analysis, to
identify recurring themes in the data set, and provide in-depth exploration of health
professional experience and factors that influence their nutrition-related knowledge
and practices. Identified themes in some instances aligned closely with the key topics
of interest presented in Table 7.2, and some additional themes outside of those topics
of interest were identified.
Analysis generated seven key themes – symptoms are precursors of nutrition issues,
provision of nutrition information to patients, patient beliefs about food intolerances
and alternative diets, impact of nutrition issues on the quality of life of NET patients,
adequacy of malnutrition screening and barriers, adequacy of vitamin screening and
barriers, provision of specialised nutrition advice - along with one sub-theme (weight
change is dependent on treatment and symptom type), which are presented in Table
7.3 and described in detail below.

197
Table 7.3 Identification of themes
Theme Related topic Quotes
Symptoms are precursors of
nutrition issues
Health professional perceived occurrence
and importance of nutritional
complications among NET patients
“they will often describe things that make them [symptoms] worse if
we question them and ah there’s spicy foods typically and fatty foods
tend to upset them”
“we’ve all head I don’t wanna eat because it gives me diarrhoea”
“the most distressing weight loss is for patients who have had a
whipples by somebody and they get a lot of weight loss around the
time of surgery”
“the ones who have those sort of abdominal issues and the people
with high grade neuroendocrine tumours [lose weight]”
“PRRT from my perspective, we get these quite cachectic patient that
have been losing weight slowly for a long period of time and they can
put on quite a bit of weight if they have a good [treatment] response”
Provision of nutrition
information to patients Provision of nutrition advice
Use and availability of evidence-based
guidelines
“I think in this neuroendocrine space it’s suboptimal just because it’s a really complex area”
“there’s a lack of confidence [in providing information], maybe just from experience or knowledge with seeing these patients because they are you know more complicated”

198
Theme Related topic Quotes
Patient beliefs about food
intolerances and alternative
diets
Perceived occurrence and importance of
nutritional complications among NET
patients
“I’ve had lot of GI patients who’ve had gut symptoms and they think
that food is causing the issue, but yeah it’s hard to prove”
“there’s quite a bit of perception of food avoidances because they
think it could be contributing or someone told me it could be
contributing [to symptoms] which leads to avoidance”
Impact of nutrition issues on
the quality of life of NET
patients
Perceived occurrence and importance of
nutritional complications among NET
patients
“lots of people who have the well-meaning family or friends and
they’ve got this very restrictive diet and you wonder whether their
food enjoyments gone down as a consequence and that has
implications for overall quality of life”
“I think it’s very hard to live with really restrictive diets…in all sorts of
ways that’s really difficult”
“I think that there are people who are not eating well enough
probably [and] have reduced exercise tolerance and energy levels
because they’re constantly malnourished”
Adequacy of malnutrition
screening and barriers
Malnutrition screening and management
practices
“I don’t know if it’s as high and as obvious as oesophageal or gastric
cancer patients, I wouldn’t say as high as those patients but there’s
still a risk [of malnutrition]”
“I probably feel like we do it badly…it’s more reactive”
“I’m not familiar with the screening tool and if it’s a general screening
tool it may need to be tweaked for neuroendocrine patients”

199
Theme Related topic Quotes
“probably need some evidence base in terms of what screen, what
test, how often”
Adequacy of vitamin screening
and barriers
Vitamin deficiency screening and
management practices
“if we have someone with true carcinoid syndrome, flushing and
diarrhoea for example, perhaps at time point zero all those patients
should have niacin checked and at the moment they’re not”
“If I test them and they’re deficient what do I give them that they’ll
absorb so I just feel at the moment, I feel poorly guided in terms of if I
test, what are the concequences”
I guess we would need some sort of education about looking for
symptoms from deficiencies and also looking at special diets that we
need to look at”
Provision of specialised NET
nutrition advice
Provision of nutrition advice
Use and availability of evidence-based
guidelines
“Nutrition wise with NETs I am not the most knowledgeable person [in
nutrition] so I know where my limits are and yeah I will refer on if I
think there is a reason to do so”
“[I provide] very general advice. If I think they’re the kind of patient
who needs a lot of advice on that [nutrition] then I’d refer [to the
dietitian].”
“it’s a bit of a green field because we’re so focused on the cancer
perspective rather than the nutritional aspect”
200
Symptoms are precursors of nutrition issues
Some health professional participants mentioned nutrition as of interest to patients
with NETs in general, whilst others disagreed and said patients often wouldn’t initiate
questions about nutrition during their consultations, and therefore they believed it
was less important than other aspects such as prognosis and treatment planning.
Those that spoke about nutrition being of interest to patients, explained that it was
often dependent on the symptoms a patient was experiencing. Nutrition was
considered by participants to be important in the context of treatment or symptoms,
rather than its own consideration. The symptoms described by participants to impact
on the nutrition needs of patients varied and included diarrhoea, malabsorption,
bloating, flushing, cramping, nausea, abdominal pain, loss of appetite, carcinoid
syndrome, pancreatic insufficiency, poor blood sugar control and diabetes, and weight
loss. Diarrhoea was frequently reported and discussed by participants to potentially
lead to nutrition issues such as weight loss and dietary change, as well as reduced
quality of life. The diagnosis of an insulinoma was described as relevant to nutrition.
Health professionals discussed the need for patients diagnosed with an insulinoma to
control their blood glucose through modified carbohydrate intake. Some health
professionals described observing the challenge patients face when constantly
monitoring what they eat due to fear of food-related symptoms. One participant said:
“they often will describe things that might make them worse if we question
them and ah there’s spicy foods typically and fatty foods tend to upset
[them]” – Nuclear Medicine Physician
Another said:
“I think people really get to understand the vibe of their diarrhoea and this
particular food makes it worse and this makes it better”- Medical
Oncologist

201
When discussing patient symptoms and their impact on nutrition, health professional
participants related this to the impact that symptoms can have on patient’s quality of
life. The observed impact of treatment and its side-effects on patients’ quality of life
was described by participants, specifically the medical and nursing professionals, as a
problem that often prompted patients to analyse their nutrition and dietary intake in
order to manage symptoms.
Examples of dietary changes made by patients that were observed by health
professional participants, included avoiding spicy foods, fatty foods, reducing fibre and
dairy. Focus group participants explained that patients would attempt to identify foods
that would help control their symptoms. One focus group participant said:
“we’ve all heard ‘I don’t wanna eat because it gives me diarrhoea’” –
Medical Oncologist
Another said:
“so then they don’t eat when they go out” - Dietitian
Health professional observations of patient dietary changes in response to symptoms
is discussed further below in relation to the theme - ‘Patient beliefs about food
intolerances and alternative diets’.
Sub-theme: Weight change is dependent on treatment and symptom type
When asked about the presence of weight loss among patients with NETs, participants
discussed that they believed it occurred, but did not consider it a common issue for
patients. Estimations of prevalence were provided by some participants – one said
“approximately 20%”, whilst another said “30 to 40%”. During discussion about weight
loss, participants identified certain types of NETs or treatments that they believed put
patients at increased risk of weight loss. These included those undergoing surgery
(specifically “Whipples procedure”, “major surgery”), those with high grade or

202
progressing NET, and with extensive intra-abdominal disease. The impact of Whipples
surgery on weight loss was described by one participant:
“I think the most distressing weight loss is for patients who have had a
whipples by somebody and they get a lot of weight loss around the time of
surgery and they find it difficult to get the weight back on” - Nuclear
Medicine Physician
Another described the differences in risk of weight loss between high versus low grade
NETs:
“I think the ones who have those sort of abdominal issues and the people
with high grade neuroendocrine tumours as well they have very sort of
nasty aggressive, rapidly progressive disease, they can lose a lot of weight
very quickly but for the lower grade NETs no so much unless they’ve got
those specific circumstances” – Medical Oncologist
When asked about the prevalence of weight gain, focus group participants felt that
patients who were asymptomatic or had low-grade tumours were more likely to
experience weight gain. Certain types of treatment were also mentioned to lead to
weight gain, due an improvement in symptoms and NET disease as a result of
treatment. PRRT was a treatment described as leading to weight gain if patients
experienced a good disease response. One health professional participant referred to
PRRT saying:
“I think we alter the balance of insulin and glucagon in the pancreas and so
people tend to gain weight after our treatment” – Nuclear Medicine
Physician
Another said:

203
“PRRT from my perspective, we get these quite cachectic patients that have
been losing weight slowly for a long period of time and they can put on
quite a bit of weight if they have a good [treatment] response” – Nuclear
Medicine Physician
Patients receiving SSA treatment and those with insulinoma were also mentioned by
some participants to be prone to weight gain. One focus group participant commented
on how patients feel about treatment-induced weight gain:
“some patients with effective treatments gain weight and don’t like it. They
have a good response and they put on weight”- Nuclear Medicine Physician
Provision of nutrition information to patients
During the focus groups, participants were not formally asked about how NET patients
access information related to their disease, but through analysis it became evident
that ‘getting NET and nutrition information’ was a strong theme among participants’
discussion. Participants spoke about how they observed patients having difficulty
finding information about their NET, and that information about NETs and their
treatment is hard to access. Participants said they knew patients were often searching
for information outside their treating health service, i.e. the internet, the media or
family and friends. One participant said:
“I think in this neuroendocrine space it’s suboptimal [information available]
just because it is a really complex area. There’s terminology, patients don’t
know whether they have carcinoid syndrome or not so the advice they get
may not be specific or good for them. It’s just sort of general advice. It’s
quite hard for them to tease out truths and myths” – Nuclear Medicine
Physician

204
Participants spoke about the information provided to patients by health professionals
being influenced by their experience with other patients with a NET. As a result, the
information provided by health professionals inexperienced in NETs was not always
optimal or appropriate. Some participants spoke about health professionals being
unaware of the information available to patients, and therefore do not direct patients
to it. One participant said:
“there is a lack of confidence [in providing information], maybe just from
experience and knowledge with seeing these patients because they are you
know more complicated than just some of the other tumour streams” -
Dietitian
Another participant said:
“also they’re seeing specialists outside who don’t have much exposure with
NET patients and limited exposure and therefore the information is very
poor as well. We see this all the time” – Medical Oncologist
When talking about information patients sought from internet and media sources,
participants commented that this information is not reliable and may be mis-directing
patients. One participant described this:
“the site that most links show up on the top is not necessarily the one that’s
the most truest form” – Medical Oncologist
Participants discussed the patient information booklets available from NeuroEndocrine
Cancer Australia (formerly the Unicorn Foundation Australia) as a good source of
information for patients, but were unsure how many patients were accessing these
when receiving or searching for information. Some focus group participants reported
providing the NeuroEndocrine Cancer Australia information booklets to patients during
their consultation, whereas others did not do this routinely.
205
Patient beliefs about food intolerances and alternative diets
When talking about patients seeking information, health professionals spoke about
observing patients seek information regarding their diet and how this contributed to
patient beliefs about food intolerances and diet requirements in the context of a NET.
Health professionals spoke about patients investigating food intolerances due to the
symptoms they experience, including diarrhoea, carcinoid syndrome, flushing and
bloating. Patients with small bowel NETs were also identified by health professionals as
at a higher risk of experiencing of, or believing they suffer from food intolerances. One
participant mentioned that they felt patients with NETs were looking for a “quick fix”
to symptoms and their NET disease, when searching for diet information. Whilst
participants said patients reported food intolerances, they described being unsure
whether food intolerances actually existed to the extent patients believed that they
did. One participant described this:
“I’ve had a lot of GI patients who’ve had gut symptoms and they think that
food is causing the issue, but yeah it’s hard to prove” - Dietitian
Another said:
“there’s quite a bit of perception of food avoidances because they think it
could be contributing or someone told me it could be contributing which
can lead to avoidance, whereas whether there is an intolerance is different”
– Medical Oncologist
The food intolerances reported to health professionals by patients with NETs, included
caffeine, lactose, alcohol, fatty foods, spicy foods, dairy and high fibre foods.
Participants discussed that the changes to diet and suspected food intolerances were
often patient-initiated and rarely identified or suggested by health professionals. It was
also discussed that patients often set out to seek and find their own information

206
regarding recommended dietary changes and food intolerances, rather than obtaining
advice from health professionals. One participant said:
“people [in reference to those with irritable bowel syndrome] just kind of
make it up as they go and I suspect that some of the NET patients do that
too” – Medical Oncologist
Another participant said:
“people are quite keen to read stuff and [be] quite proactive with trying to
find out whatever they can about nutrition related to their disease” -
Dietitian
Participants also spoke about how interest in information on anti-cancer diets are
common among patients with NETs and they are for cancer patients in general. In
combination with dietary change for symptom management, this led to particularly
complex diet behaviours among patients with NETs, as described by participants:
“there would be a bit of an overlap with diets that are supposed to improve
cancer …so the people who are making dietary modification because I’ve
been told that if I avoid you, all meat, all dairy, all sugar, then my cancer
will get better. So there will be an overlap with general altered diets to try
and improve outcomes for people with cancer, overlapping with what I’m
doing to try and help diarrhoea” – Medical Oncologist
When talking about dietary changes and patients seeking information on ways to
improve their cancer and NET symptoms, participants spoke about observing NET
patients seeking vitamin supplements and alternative/herbal remedies. The intent of
patients to improve their cancer outcomes with vitamins/herbal remedies was
described by one participant:

207
“some of them out of desperation because if a medical professional tells
them look we are not going to cure you, they feel they can do better” -
Endocrinologist
Another participant spoke about how vitamin and herbal remedies were considered by
patients to be a natural alternative:
“it’s considered a natural treatment as opposed to like a chemical type of
medical treatment” - Dietitian
Impact of nutrition issues on the quality of life of NET patients
When asked about the quality of life of patients, participants spoke about the negative
impact of NET symptoms, dietary change and weight loss on a patient’s quality of life.
One participant described the impact of poor diet and weight loss:
“I think that there are people who are not eating well enough probably
[and] have reduced exercise tolerance and energy levels because they’re
constantly malnourished” – Nuclear Medicine Physician
Participants spoke about and agreed that diarrhoea was a symptom that commonly
reduced quality of life among patients. One participant said:
“inability to be able to move a certain distance from a bathroom when they
get diarrhoea it’s explosive to urgent...people are essentially housebound”
– Nuclear Medicine Physician
Another said:
“there’s definitely the social implications of diarrhoea. So I’m not going out
because I could have diarrhoea, or I’m not going to go because I don’t know
where the toilets are” – Medical Oncologist

208
Participants said diarrhoea was often difficult for health professionals to manage due
to the many potential causes (pancreatic insufficiency, treatment with SSA, small
intestinal bacterial overgrowth, bile salt malabsorption). When talking about patients
suffering diarrhoea, participants also talked about dietary changes they made to help
reduce their diarrhoea and that these changes subsequently impacted further on their
quality of life. The negative impact of diet changes for symptom management was
discussed in relation to social eating and food enjoyment. Participants spoke about
how diarrhoea and other symptoms lead to restricted diets and therefore further
impact on quality of life by restricting enjoyment of food and ability to eat comfortably
with family and friends. One participant described reduced food enjoyment among
NET patients:
“lots of people who have the well-meaning family or friends and they’ve got
this very restricted diet you wonder whether their food enjoyment’s gone
down as a consequence and that has implications for overall quality of life”
- Nurse
Another said:
“I think it’s very hard to live with really restrictive diets…in all sorts of ways
that’s really difficult” - Nurse
The same health professional spoke about the importance of diet in the context of
patients living with NET disease over a prolonged period:
“We’ve got patients who are living many, many years with NETs as a
chronic condition…and we want them to be able to know and feel free to
make choices with food…so that they can eat with their families and
interact socially and have a really great range of flavours and textures with
the minimal impact on their symptoms” - Nurse

209
Nutrition issues leading to reduced quality of life discussed by participants included;
not being able to eat as expected or comfortably among family and friends, financial
expense of special diets and supplements, and the impact of reduced dietary intake on
weight loss and malnutrition leading to fatigue and less ability to perform and enjoy
daily tasks.
Adequacy of malnutrition screening and barriers
When asked about the presence of malnutrition among patients with NETs,
participants mostly spoke about and agreed that malnutrition was a greater problem
among other patients with gastrointestinal cancers (gastric cancer, oesophageal
cancer, pancreatic adenocarcinoma) than among NET patients. When comparing
presence of malnutrition in patients with NETs compared with other cancers, one
participant said:
“I haven’t seen that many, I don’t know if it’s as high and as obvious as
oesophageal or gastric cancer patients, I wouldn’t say as high as those
patients but still there’s a risk” - Surgeon
There were particular types of NET disease and treatment characteristics that focus
group participants said were likely to lead to increased weight loss and malnutrition
risk, including patients at end of life, with malabsorption issues, severe diarrhoea,
high-grade NETs, presence of mesenteric fibrosis or bowel obstruction. Participants
also discussed and agreed that malnutrition is less likely to be a problem at the time of
NET diagnosis, as patients may not have had time to develop nutritional deficiencies.
Most participants said they did not screen for malnutrition on a regular basis or in a
systematic way. They were more likely to ask about weight loss and symptoms
(fatigue, poor appetite) in general rather than perform malnutrition screening. Nurses
and doctors said they would be prompted to consider malnutrition risk in their
consultation if a patient mentioned they had symptoms or had lost weight. Dietitians

210
said they were more likely to perform a comprehensive nutrition assessment than
simple screening. When asked how they manage malnutrition screening, participants
responded:
“I probably feel like we…I do it badly” and “it’s more reactive” – Nuclear
Medicine Physician
When discussing malnutrition screening, some doctors referred to this as checking
blood levels of vitamins and nutrition markers e.g. albumin, others referred to it as
assessing for weight loss.
Most participants agreed that malnutrition screening should be part of standard care
for NET patients and completed on a more systematic basis. Some commented on the
benefit of malnutrition screening in NET patients, due to the impact that weight loss
can have on quality of life. Reported barriers to regular malnutrition screening
included time, lack of evidence and lack of clarity regarding suitable process and tools
to use. One participant commented on the use of screening tools for malnutrition
screening in NET patients, and said they may have specific requirements for a
screening tool:
“I’m not familiar with the screening tool and if it’s a general screening tool
it may need to be tweaked for neuroendocrine patients coz every screening
assumes for every likelihood that there’s a problem that in NETs that’s
probably high particularly. So just…we get some unusual things with NETs”
– Medical Oncologist
Participants spoke about the presence of weight loss and poor dietary intake among
NET patients, which would contribute to their malnutrition risk, but felt that other
issues such as vitamin deficiency and symptoms also contributed to malnutrition risk.

211
One participant commented on barriers to evidence for the best malnutrition
screening process in NETs:
“probably need some evidence base in terms of what screen, what test,
how often, what’s the outcome, what’s the gain” – Medical Oncologist
During the focus groups there was discussion among participants as to which health
professional would be best to screen for malnutrition in NET patients. Some spoke
about the value of a dietitian and that comprehensive nutrition assessment
undertaken by a dietitian would be best for some patients. It was discussed that
identifying patients in need of timely dietitian assessment should be a priority for
screening. Some participants reported referring to the dietitian immediately after a
patient reports weight loss or difficulty with eating. Others discussed that malnutrition
screening should be a simple process and therefore could be done by any member of
the multidisciplinary team.
Adequacy of vitamin screening and barriers
Health professionals described rarely screening for vitamin deficiencies in their
consultation with patients with a NET. Medical and nursing professionals reported
believing it was the dietitian’s role to monitor vitamin deficiencies, prompt testing and
provide guidance on the best approach to this. In response to this, dietitians said they
didn’t routinely consider vitamin screening when consulting with patients. Participants
discussed the types of patients with a NET that may require monitoring of vitamin
deficiency, including those who had lost weight, experienced symptoms such as
diarrhoea, and who had major changes to their diet leading to insufficient nutrient
intake. Identification of these symptoms and factors did not necessarily lead to routine
vitamin screening, as described by one participant:
“If we have someone with true carcinoid syndrome, flushing and diarrhoea
for example, perhaps at time point zero all those patients should have

212
niacin checked and at the moment they’re not” – Nuclear Medicine
Physician
Barriers to vitamin screening included time, lack of evidence for appropriate screening
practices and knowledge of the best approach to screening for vitamin deficiency. One
participant described their uncertainty regarding vitamin testing and supplementation:
“If I test them and they’re deficient what do I give them that they’ll absorb
so I just feel at the moment, I feel poorly guided in terms of if I test, what
are the consequences”- Medical Oncologist
Another participant described the need for further education to guide vitamin
screening practices:
“from a dietitian point of view, if it’s something that we’re going to start
looking at then I guess we would need some sort of education about
looking for symptoms from deficiencies and also looking at special diets
that we need to look at”- Dietitian
When asked about the practice of vitamin supplementation, health professionals
described this only being done if a vitamin deficiency was identified. Some health
professionals supplemented for vitamin D or iron, if deficiency was identified in blood
testing, and others suggested the patient’s GP was the most appropriate person to
manage vitamin supplementation, including vitamin D and B12. After discussion,
participants did not agree on who was best to initiate vitamin screening or
supplementation with patients but did agree that this issue required further
exploration and research to guide best practice.
Lack of evidence was consistently discussed as a barrier to nutrition screening
practices (both malnutrition and vitamin screening) during focus groups. Participants
described a lack of evidence specific to the nutritional management of NETs as a
213
problem impacting their clinical practice. Some participants would use general cancer
guidelines and nutrition guidelines but were unsure on where to access evidence and
clinical guidance for their practice with patients with a NET.
Provision of specialised NET nutrition advice
When asked about provision of nutrition advice to NET patients, medical and nursing
participants reported this as minimal, due to a preference of referral to the dietitian
for nutrition assessment and advice. Participants described easy access and availability
of a dietitian in their hospital, leading to dietitian referral for nutrition assessment and
management if a patient reported issues with their weight or diet. Nutrition advice
from a dietitian was considered by participants as the most reliable source of
information. One participant said:
“Nutrition wise with NETs I am not the most knowledgeable person so I
know where my limits are and yeah I will refer on if I think there is a reason
to do so” - Nurse
Another said:
“[I provide] very general advice. If I think they’re the kind of patient who
needs a lot of advice on that [nutrition] then I’d refer [to the dietitian]. I
don’t have a lot of knowledge in the area, you know medical practitioners
are taught very badly about this, and I don’t have time when you add in all
the other things that you’ve got to discuss in clinic” and “I find it very
valuable having a dietitian in clinic” – Medical Oncologist
Advice provided by dietitians participating in focus groups was comprehensive, but
was as varied as their reports of their focus on assessment and management of
nutrition in practice. Dietitian-based nutrition advice included weight management,
high protein diets, and symptom management through diet. Medical and nursing

214
participants said they provided brief general advice to patients with NETs about
keeping a healthy weight, following a healthy diet, and avoiding severe dietary
restriction. Much of the nutrition advice provided was described as being prompted by
patient symptoms. Focus group participants acknowledged that nutrition and diet play
a role in symptom management in patients with NETs. One dietitian said:
“the advice that we’re giving is symptom based. The initial thing that we’re
looking at is weight, weight changes, and signs of malnutrition” - Dietitian
Barriers to provision of nutrition advice among participants who weren’t dietitians
included time, followed by not knowing what advice to provide. One participant spoke
about how health professionals are less focused on nutrition aspects of NET disease:
“it’s a bit of a green field because we’re so focused on the cancer
perspective rather than the nutritional aspect” – Nuclear Medicine
Physician
7.5 Discussion
Focus groups conducted with multidisciplinary health professionals in Phase 2 resulted
in a thorough description of NET health professional knowledge and practices in regard
to nutritional issues and their management with patients living with a NET. Insights
from the focus groups aligned with results found in the international health
professional survey, confirming survey data and also providing further in-depth
understanding of health professional responses to, and nutrition-related practices with
regard to NETs. Initial manifest content analysis summarised health professional
practices in regard to nutrition screening and management in patients diagnosed with
a NET, and results were similar to those from the Health Professional Survey for
malnutrition screening practices, vitamin screening practices, provision of nutrition
advice, and use of evidence-based guidelines. Latent content analysis led to further in-
depth exploration of health professional experience and opinion regarding nutritional

215
issues among patients diagnosed with a NET and provided rich insights into barriers
and enablers that contribute to nutrition-related practices.
Health professional perceptions of the quality of life and experience of patients
diagnosed with a NET has not been well studied. One small study (n=17), published in
1998, compared patient and staff perceptions of quality of life and found that patient
satisfaction with their quality of life was greater than health professionals perceived it
to be (Larsson, von Essen and Sjoden, 1998). The correlation between patient and
health professional perception of key patient issues and quality of life was a positive
result in that study, potentially indicating good communication and observation of
patient issues and priorities. However, evidence to guide the translation of issue
identification to relevant interventions, for example, malnutrition screening or
investigation and advice regarding dietary change, is lacking and should be the focus
for future health professional education and nutrition guidelines.
During focus groups, health professionals described diarrhoea, abdominal pain, and
weight loss as symptoms most concerning to patients and also most likely to impact on
nutrition. These symptoms were also described by patients in the Phase 1 interviews
(Chapter 5) as impacting on their quality of life, leading to dietary change. During focus
groups, health professionals spoke about their awareness of dietary change and food
restriction made by patients with a NET in an effort to manage their symptoms and to
improve their disease outcomes. They also spoke about how these behaviours are
often initiated by patients themselves rather than in consultation with health
professionals. The issues of dietary change and self-management of dietary restriction
was also highlighted in results of the Phase 1 study and patient interviews (Chapters 4
and 5). These findings indicate that health professionals are aware of dietary change
and restriction among NET patients, however, few health professionals spoke about
how they assisted patients in managing their diet appropriately in response to a NET.
Recommendation to avoid dietary restriction was discussed as part of general advice
provided to patients, but only in brief. Investigation of the occurrence of dietary
216
change and the impact this has on patient’s nutritional status and quality of life was
not mentioned as a consideration during consultation with NET patients.
Comprehensive dietary advice and investigation of food intolerances was presumed by
health professionals to primarily be the role of the dietitian. However, results from
Phase 1 (Chapter 4) indicated that less than 22% of patients with a NET in this study,
had consultation with a dietitian over the study period, whereas up to 56% of patients
with a NET reported making a dietary change to some degree. Despite awareness of
dietary change and restrictions as an issue amongst patients, it is evident that health
professionals are not routinely addressing this or referring patients with NETs to a
dietitian for individualised dietary assessment and management. Of note, the study
site where focus groups were undertaken and where the Phase 1 study was
undertaken, is an accredited European NET Society Centre of Excellence (CoE), and
therefore health professionals have regular access to a NET-specialist dietitian.
Patients diagnosed with a NET at health centres without specialist NET dietitian
support may therefore be less likely to be referred to a dietitian, or the dietary advice
they receive may not be specific to NETs.
Dietary change, if resulting in severe dietary restriction can lead to weight loss and
deterioration of nutritional status. Weight loss and malnutrition can have negative
consequences for patient morbidity and treatment outcomes and lead to increased
health care costs (Nitenberg and Raynard, 2000; Arends et al., 2006). Patients in the
Phase 1 interviews (Chapter 5) discussed the impact that dietary change had on their
social activity, enjoyment of food and overall quality of life, highlighting the
importance of addressing dietary change among NET patients. The best approach for
identifying or screening for patient dietary change by health professionals was not
discussed during focus groups but does require further exploration and consideration.
The risk of dietary restriction among patients with a NET should be considered when
NET-specific nutrition guidelines are developed. Health professionals in this study, and
patients in the Phase 1 study (Chapter 5) identified symptoms of diarrhoea, abdominal

217
cramps, bloating and weight loss as often leading to dietary change and restriction.
Therefore, presence of these symptoms should be considered a risk factor for dietary
change, and a prompt for screening for dietary issues and risk of impaired nutritional
status.
Insights from the focus groups indicate that nutrition-related screening practices,
including screening for dietary change, malnutrition and vitamin deficiencies, are not
routine or systematic among NET health professionals. This was also shown through
results of the health professional survey described in Chapter 6. Several evidence-
based guidelines for cancer management recommend routine screening for
malnutrition for all people with cancer, and at regular intervals (Jann Arends et al.,
2017; Kiss et al., 2020). Results of this research show that these guidelines are not
being incorporated by NET health professionals. Focus groups generated discussion
among health professionals regarding the importance of malnutrition and vitamin
screening in the context of the care of a patient with a NET. Health professionals
identified the need for improved nutrition screening practices with patients and
suggested the development of a systematic process for malnutrition or vitamin
screening was warranted. Limited knowledge of the prevalence of malnutrition and
vitamin deficiencies was identified as a barrier to screening practices, as was evidence
and guidance for the best approach or method to screening. As previously discussed in
Chapter 4, common malnutrition screening tools used with cancer patients include the
Malnutrition Screening Tool (MST), Malnutrition Universal Screening Tool (MUST) and
the Nutrition Risk Screening tool (NRS-2002). These could be appropriate for use with
NET populations, but these screening tools may miss identifying nutritional issues
unique to patients with NETs, for example their unique symptom profile and dietary
restriction. Literature exists identifying malnutrition and vitamin deficiency as
prevalent issues among NET patients (Shah et al., 2005; Fiebrich et al., 2010; Bouma et
al., 2016; Maasberg et al., 2017; Borre et al., 2018). Results presented in this thesis
from Phase 1 and Phase 2 also show that malnutrition, weight loss and dietary change
are prevalent among patients with NETs.

218
Development of nutrition guidelines that summarise evidence for the prevalence of
these nutrition issues among NET patients will assist in the education of health
professionals and prompt initiation of routine nutrition-screening practices. Health
professionals in the focus groups identified the dietitian as responsible for
comprehensive nutrition assessment in NET patients but were unable to agree upon
the most appropriate health professional to perform screening, which would occur
prior to dietitian referral. This is not an issue unique to NETs, with responsibility of
nutrition screening varying within other cancer populations and in hospitalised
patients more broadly. Health professional responsibility for nutrition screening in NET
contexts can therefore be explored using existing literature which focuses on cancer
patients in general. Further qualitative research targeting health professionals on a
broader scale (multiple centres), with a focus on establishment of optimal nutrition
screening practices and responsibilities is important. This process would also
contribute to recommendations for nutrition screening practices in future NET-specific
nutrition guidelines. Groups at greater risk of weight loss and malnutrition identified
by health professionals in these focus groups, included patients undergoing major
gastrointestinal surgery, with progressive NET disease, and with extensive abdominal
disease. Patients identified by health professionals to be the least at risk of weight loss
and prone to weight gain were those undergoing PRRT treatment, with good
treatment response, and those with improving symptoms as a result of treatment.
Existing cancer guidelines recommend all cancer patients are screened for malnutrition
risk, regardless of disease or treatment status (Kiss et al., 2020), but with a focus on
high risk groups in settings with limited resources, which is important to acknowledge
in future NET guidelines. The identification of at-risk NET groups through this research,
is useful to acknowledge the factors most likely to lead to nutrition issues in patients
with a NET, which can be utilised to prioritise and target nutrition resources when
required in practice.
A recurring theme among focus groups participant responses was ‘Provision of
nutrition information to patients’ which was identified by health professionals as
problematic for patients diagnosed with a NET. Health professionals acknowledged

219
that patients were often left to access nutrition information from the internet, family
or other NET patients through blogs or peer groups. They also discussed that health
professionals were themselves often unaware of available, reputable sources of
nutrition information, partially due to the rare nature of a NET diagnosis and the belief
that there was limited nutrition evidence available to support practice. This was
considered a greater issue among health professionals who had limited experience in
managing NETs. These results align with results of the Phase 1 patient interviews,
during which patients discussed the same issue with accessing NET-specific
information on nutrition and therefore confirms the priority of this as a target for
health professional and patient education. Difficulty in accessing NET-specific
information has also been identified in a large published survey of NET patients and
NET health professionals to be a considerable unmet need (Leyden et al., 2020).
Collation and development of NET-specific nutrition information resources would be
beneficial to address this issue, and revision or development of future nutrition
guidelines for NETs could be one way of addressing this gap.
Health professionals identified the role of a dietitian as important in the context of a
NET patients care and treatment, and that nutrition assessment and advice was best
provided by a dietitian who can focus on the individual needs of each patient. This
suggests that a dietitian has an integral role within the multidisciplinary team working
in a NET unit. Participants reported that a specialist NET dietitian was readily available
to receive referrals for patients with NETs within the NET unit of the study site, which
as discussed above was an ENETS CoE. A dietitian in some health centres managing
patients with NETs may not be readily available and given that NETs are rare in
incidence the availability of a dietitian with specialty knowledge and experience in
managing NETs, is likely to be limited to only certain health centres. As health
professionals in this study, and patients in Phase 1, identified expertise in NET
management as important to ensuring patients are managed appropriately and have
access evidence-based information, access to a dietitian with NET expertise would also
be ideal. However, if this is not possible, access to a dietitian with experience in
managing cancer patients during treatment would be appropriate helpful. Promoting

220
the occurrence and importance of nutrition issues in patients diagnosed with a NET
among practicing dietitians, and through professional groups such as the Dietitians
Association of Australia and international dietetic associations, would assist to raise
awareness of nutrition in this rare cancer group. These professional groups can also
provide useful avenues to disseminate appropriate patient education resources and
professional development opportunities specific to NETs, otherwise difficult to access
by dietitians who do not routinely care for patients diagnosed with a NET.
7.6 Conclusion
This qualitative study of multidisciplinary health professionals working with NET
patients, enabled a comprehensive exploration of their knowledge of nutritional
complications among patients and nutrition screening and management practices.
Health professionals perceived symptom burden, inadequate provision of NET-specific
nutrition information, and dietary restriction as key issues impacting patient quality of
life and nutrition, which correlates with results of patient interviews discussed in
Chapter 5. Focus groups identified inconsistencies in nutrition-related practices,
including limited conduct of malnutrition and vitamin screening, and varied provision
of nutrition information. A multidisciplinary approach to management of patients with
NETs was identified as important, as was the role of a dietitian in providing optimal
nutrition assessment and intervention. Health professionals identified barriers to their
NET-related nutrition knowledge and practices as limited evidence or knowledge of
available evidence, and lack of NET-specific nutrition guidelines. Study results provide
additional depth and contextual detail above what was obtained in the health
professional survey discussed in Chapter 6 and will contribute to development of
further NET nutrition research and NET-specific nutrition guidelines, which currently
do not exist. Particular NET types and treatments at greater risk of causing
malnutrition and dietary restriction were identified by health professionals in this
study. Factors leading to deteriorating nutritional status included surgery and presence
of a progressive NET. Factors leading to improvement in nutritional status included
PRRT, treatment response and improving symptoms. These factors are useful

221
considerations for future interventional nutrition research in NETs, and the
development of NET-specific nutrition guidelines. Current cancer guidelines
recommend all cancer patients undergo routine malnutrition screening regardless of
their disease or clinical state, which is not currently occurring with NET patients, as
found through this research. Further research and consultation with NET health
professionals is required to establish robust nutrition screening practices. The high
prevalence of dietary change and food restriction observed in patients should be
considered when establishing suitable nutrition screening processes and tools for use
in a NET population, particularly given the negative impact that dietary restriction can
have on a patient’s quality of life.


223
Chapter 8: Conclusions and implications for research and
practice
8.1 Summary of research findings
The studies presented in this thesis have explored the prevalence of nutritional
complications and their HRQoL impacts among a heterogeneous cohort of GEP NET
patients (Phase 1 research). In parallel they have explored health professional
knowledge and usual management of nutritional complications in GEP NET patients
(Phase 2 research). Results of the Phase 1 study have provided the first comprehensive
longitudinal description of the prevalence of nutritional complications; including
malnutrition, weight change, body composition change (fat-free mass), and dietary
modification; and how this relates to patient’s HRQoL and experience of nutritional
complications. Results of the Phase 2 study have provided the first detailed summary
of NET health professional knowledge and practices in regard to the nutritional
complications in NET patients and has contributed important insights about barriers
and enablers to the nutritional management of these patients. This chapter
summarises the main findings of these studies, the strength and limitations of this
research, and presents a discussion of the implications for clinical practice and
directions for future research.
8.1.1 Quality of life and symptoms in GEP NET patients
Chapter 3 described results for symptoms and quality of life scores among participants
enrolled in the Phase 1 longitudinal embedded mixed methods study. Symptoms were
prevalent among patients with GEP NETs enrolled in the Phase 1 study. The
commonest symptoms at time of recruitment included, in order of prevalence; fatigue
(80%), abdominal discomfort (76%), pain (68%), bloating (64%), wind/gas (53%),
diarrhoea (46%), hot flushes (45%), and reflux/heartburn (43%). After the six-month
study period, symptom prevalence remained high. Fatigue, diarrhoea, abdominal
discomfort and bloating have been identified as common symptoms among NET
224
patients in other studies, ranging between 20-90% (Fröjd et al., 2007; Lind, Wängberg
and Ellegård, 2016; Singh et al., 2017; Borre et al., 2018). Therefore, the symptom
profile of patients in this study were representative of the general GEP NET population
at baseline, and over a period of 6 months.
Compared to the general Australian population (Mercieca‐Bebber et al., 2019),
participants had lower scores for several functional (role, cognitive, social) suggesting
that patients with GEP NET had impaired quality of life, and demonstrated that their
HRQoL remained impaired over the six-month study period. Reduced HRQoL was
characterised through reduced work performance, hobbies, altered memory and
concentration, and a reduction in social activity. The presence of anxiety and
depression was observed among patients with GEP NETs and did not significantly
change or improve over-time. Financial toxicity was also observed among these
patients and remained prevalent throughout the six-month study period, however
evidence reviewed as part of the study suggests that they may have better financial
well-being than other cancer populations (de Souza et al., 2017; D’Rummo et al.,
2019).
Participants in the Phase 1 study were newly referred for medical management to the
NET/UGI unit at study sites, and therefore underwent new or revised treatment for
their GEP NET, throughout the study period. Results show that issues of reduced
HRQoL, anxiety, depression and financial toxicity remained prevalent in patients
despite specialist NET medical management and treatment, due to the ongoing burden
of GEP NET symptoms and morbidity from treatment. This signifies the need to screen
and address these issues at initial patient referral as well as repeat screening during
treatment. Symptom burden has been associated with increased distress amongst NET
patients (Larsson, Haglund and Von Essen, 2003; Fröjd et al., 2007) and the high
prevalence of anxiety and depression among study participants, may in part be
explained by the observed high symptom prevalence. The presence of financial toxicity
in patients with a NET has also been shown to have an adverse effect on their QOL
(Jensen et al., 2019). Therefore, screening and identification of financial issues, as well

225
as for presence of distress, anxiety and depression is essential in order to identify and
manage causes (e.g. symptoms), initiate and target supportive care interventions.
8.1.2 Prevalence of nutritional complications in NET patients
Results of the Phase 1 longitudinal study, described in Chapter 4, show that
malnutrition, clinically significant weight loss, fat free (muscle) mass change and
dietary change are prevalent among patients with GEP NETs, and remained prevalent
over-time during their treatment. Twenty nine percent of patients were assessed as
malnourished at recruitment to the Phase 1 study, comparable to the literature
(Maasberg et al., 2017). The prevalence of malnutrition in the Phase 1 study cohort
reduced to 13% by four-months, due to drop out/withdrawal of patients with high-
grade (Grade 3) GEP NET and undergoing chemotherapy. Improvement in nutritional
status seen among 10 (21%) participants, most of which were undergoing PRRT
treatment (n=6). Sub-analysis of malnutrition rate by treatment type was not
performed in this Phase 1 study due to sample size limitations. However, the trend in
results do align with other studies examining malnutrition risk and assessment in NET
patients (Qureshi et al., 2016; Maasberg et al., 2017).
In the cohort examined in this PhD study, up to 52% of participants experienced weight
loss (of at least 0.8% body weight), and up to 62% of participants experienced fat free
mass (FFM) loss (median 1.3kg (IQR 1.3, 4.6) at T6), throughout the study period,
which was greater than the proportion that were assessed as malnourished. Clinically
significant weight loss of >5% and >10% body weight was observed in up to 30% and
13% of GEP NET patients, respectively, over the study period. In addition, 27% (n=11)
recorded FFM loss despite having stable weight or weight gain, indicating underlying
body composition change and muscle mass deterioration, irrespective of total weight
loss. The prevalence of weight loss has not been well studied in the broader NET
population, and this PhD study was the first to prospectively record the prevalence of
weight loss over-time in patients with GEP NETs. Weight gain was observed among
some patients with GEP NETs patients (35-44%) in the Phase 1 study, indicating that

226
this is just as prevalent as weight loss. Few similarities in NET or treatment type was
found among patients who gained weight. Progressive weight gain can lead to
worsening of overweight and obesity status, which in the long-term can contribute to
chronic disease risk, such as diabetes and cardiovascular disease. This PhD study is the
first to comprehensively explore weight change, including weight loss and gain, among
patients with a GEP NET. This PhD study has highlighted the high prevalence of weight
loss among patients with GEP NETs, but further research is required to examine the
impact of this weight loss on patient morbidity, HRQoL and treatment outcomes, and
identify optimal nutrition interventions to manage risk and weight loss. More research
is required to determine the prevalence and degree of weight gain among GEP NET
patients, and whether long-term weight gain contributes to worsening morbidity and
chronic disease risk.
The prevalence of vitamin deficiency was assessed over-time in the Phase 1
longitudinal study (Chapter 4), and low rates of vitamin deficiency were found. Twenty
seven percent and 29% percent of participants were assessed as vitamin D deficient at
recruitment (T0) and six-months (T6) respectively, which are rates comparable with
the general Australian population (Australian Health Survey: Biomedical results for
nutrients, 2011 - 2012. Vitamin D., 2014). Deficiency for all other measured vitamins
was below 10%. This could be partially due to most participants being early in their
NET diagnosis and treatment (within six-months), and therefore vitamin deficiency had
yet to develop. Low presence of niacin deficiency may be explained by the low testing
rate, which was below 45%. As per published literature, patients at risk of niacin
deficiency include those with a serotonin-producing NET or carcinoid syndrome (Shah
et al., 2005; Bouma et al., 2016). Whilst a quarter of study participants reported
concurrent symptoms of diarrhoea and flushing, potentially indicating the presence of
carcinoid syndrome, patients in this study were undergoing active treatment for their
GEP NETs, which combined with low testing rates likely led to low detection of niacin
deficiency. Larger, multi-centre observational research trials assessing niacin status in
patients with serotonin-producing NETs or carcinoid syndrome is warranted to test this
association further. Longitudinal, prospective studies are preferable to measure the

227
occurrence and prevalence of niacin deficiency over-time in this patient group, and to
ensure collection of relevant and accurate data
8.1.3 Dietary change and it’s impact on NET patients
Dietary change among NET patients has not been explored well in previous research,
and this thesis provides the first comprehensive summary and exploration of dietary
change and it’s impacts on GEP NET patients. Dietary change was reported by over half
of participants in the Phase 1 longitudinal study, and the prevalence of dietary change
stayed consistent over the six-month study period (Chapter 4). Eating smaller meals
and avoiding particular food types were the dietary changes most likely to occur. There
was large variation in types of food avoided by participants, highlighting the
complexity of dietary change among patients with a GEP NET. The symptoms most
likely to cause dietary change, as reported by Phase 1 study participants, included loss
of appetite, nausea, vomiting, abdominal pain, bloating and diarrhoea. Over 60% of
patients experiencing these symptoms said that these impacted their diet.
Results of patient interviews described in Chapter 5 highlighted that dietary change
was often initiated by patients in an attempt to manage symptoms, particularly
gastrointestinal symptoms including diarrhoea, abdominal cramps/pain and bloating.
These gastrointestinal symptoms, particularly diarrhoea, were described as heavily
impacting on quality of life and ability to function during daily activities and socialise
with family and friends. Therefore, patients frequently monitored these symptoms and
sought strategies to improve them. Patients described avoiding particular foods that
they believed may exacerbate their symptoms, including avoidance of fruits,
vegetables, high fat or fibre foods, dairy, and reduction in meal size. Dietary changes
were extensive and complex, with limited consistency found between patients and the
diet they chose to follow for symptom management. Patients identified access to
evidence-based and reputable nutrition information as difficult and therefore
preferentially sought information from peers through NET patient foundations,
support groups and blogs. Patients described limited provision of nutrition and dietary

228
information from health professionals, and therefore sought autonomy in their own
management of these issues. Some patients described their diet as restrictive, leading
to limitations on social activities and enjoyment of food.
Patients’ dietary change, without assessment and oversight from health professionals,
may be unnecessarily restrictive leading to limitations on quality of life and also risk of
nutritional status decline, if a prolonged reduction in food intake and weight loss
occurs. Results of qualitative patient interviews in Phase 1 highlighted the disparity
between the extent of nutrition information provided by health professionals, and the
nutritional information needs of NET patients. Nutrition and dietary information was
rated as highly important to patients involved in the Phase 1 interviews. Health
professionals involved in the Phase 2b focus groups (Chapter 7) spoke about being
aware of the symptomatology and occurrence of dietary change among NET patients,
but rarely assessing dietary change or providing information on diet during their
consultations with patients. This confirms the marked disparity between nutrition
information needs of NET patients and the provision of nutrition information from
health professionals. It thus identifies this as a significant target for health professional
education. The establishment of suitable nutrition screening and dietary management
guidelines for NETs could assist in ensuring consistency among NET health
professionals and identify nutrition dietary management as a supportive care priority.
8.1.4 NET health professional nutrition-related knowledge and practices
In the Phase 1 longitudinal study described in Chapter 4, less than a quarter of GEP
NET patients had contact with a dietitian over the study period. A higher proportion of
patients recorded nutritional complications of weight loss, fat-free mass loss and
dietary change, highlighting potential under-recognition and management of these
issues. Furthermore, the proportion of patients with dietitian contact during the Phase
1 study may have been over-estimated.

229
Nutrition-related knowledge, screening and management practices of multidisciplinary
NET health professionals were explored for the first time, through a structured online
survey (Phase 2, Chapter 6) and health professional focus groups (Phase 2, Chapter 7).
Results from the Phase 2 study demonstrated that NET health professionals are aware
of common symptoms experienced by NET patients, as stated in published literature,
and aware that nutrition complications such as malnutrition, weight loss and dietary
restriction occur among NET patients. The Phase 2 survey identified that only 38% of
NET health professionals reported screening for malnutrition or vitamin deficiencies
during consultation with NET patients, and of greater note was that 28% reported that
no one conducted nutrition-related screening in their workplace. Of those that
reported screening, use of validated malnutrition screening tools was inconsistent.
Research presented in this thesis has shown that there are unique nutrition issues
relevant to patients with a NET that may contribute to malnutrition risk, including NET-
related symptoms and dietary restriction. These issues may not be well identified using
existing nutrition screening tools, and therefore may be why they are not well used by
NET health professionals. Issues of weight loss and malnutrition were considered less
prevalent among GEP NET patients than for other gastrointestinal cancers, as
highlighted during health professional focus groups (Phase 2, Chapter 7). Health
professionals believed conditions such as a progressive NET, and undergoing major
surgery put patients at increased risk of weight loss and malnutrition, and therefore
were more likely to screen for malnutrition in these groups. PRRT was identified as
commonly leading to weight gain, if the treatment was successful. This aligns with
published literature and the trend in results for malnutrition prevalence in the Phase 1
study. Health professional respondents to the Phase 2 survey (Phase 2, Chapter 7)
were more likely to report providing routine advice to NET patients on NET-related
symptoms (92%), than on other nutrition-related issues such as weight loss (59%), food
intolerances (41%) or risk of vitamin deficiency (32%).
Results of both the Phase 2 survey (Chapter 6) and Phase 2b focus groups (Chapter 7)
confirm that despite knowledge of the presence of nutritional complications among
NET patients, malnutrition and vitamin screening is not routine, and the provision of

230
nutrition advice and information is both limited and inconsistent. The lack of evidence,
lack of knowledge regarding appropriate screening practices, and lack of NET specific
nutrition guidelines were all identified by health professionals in the Phase 2 study as
barriers to nutrition-related screening and practices. Multidisciplinary health
professionals did discuss and agree during focus groups that systematic malnutrition
and vitamin screening practices among NET patients would be beneficial to establish,
but the most appropriate method for this requires further exploration, as does the
generation of prevalence data for nutritional complications among NET patients.
During focus groups (Chapter 7), health professionals discussed the importance of a
dietitian within the NET multidisciplinary team and reliance on the role of the dietitian
to provide individualised assessment and information regarding nutrition. Health
centres without access to a dietitian with NET expertise may therefore be limited by
this, leading to greater responsibility for nutrition management falling to medical and
nursing professionals, or alternatively NET patients receiving suboptimal nutrition
management. Referral of patients to dedicated NET centres with the appropriate
dietician expertise, should be considered by health professionals.
8.2 Strength and limitations
Results of studies presented in this thesis have provided a comprehensive description
of nutritional complications occurring in patients living with a GEP NET, and their
impact on patient HRQoL, not previously explored or reported in this detail. The
longitudinal approach of Phase 1 was a strength of this research, with previous
published nutrition research focussing primarily on cross-sectional data for
malnutrition and vitamin deficiencies. This research has contributed comprehensive
prevalence data for weight change, fat free mass change and dietary change among
patients with NETs over-time, for which there was limited evidence available
previously. The embedded mixed-methods approach to this research is also a major
strength, enabling in-depth insights, including precursors to, and impacts of nutritional
complications on patient HRQoL. The results and insights gained through the
qualitative data provide strong evidence and rationale for identifying and managing

231
nutritional complications among patients with GEP NETs. This approach also enabled
patients to discuss in-depth, their experiences regarding nutrition, and where nutrition
fits in their perceived priorities of care. The participants recruited to the Phase 1
longitudinal mixed-methods study were likely representative of the broader GEP NET
population because the sample was heterogeneous with various primary tumour sites
and NET grades represented. Also, the prevalence of symptoms reported by patients in
this study was similar to other published literature, and results for quality of life were
also comparable.
This thesis was strengthened by the combination of observational research examining
the prevalence and severity of nutritional complications among patients and the
exploration of health professionals’ practices in regard to nutrition. Health professional
nutrition-related knowledge and practices have not previously been explored. The
addition of exploratory health professional data through surveys and focus groups,
provided further perspective on nutritional complications occurring in patients with
GEP NETs and approaches to their current management. The Phase 2 research
presented in this thesis provides the first summary of international health professional
nutrition screening and management practices. The inclusion of a multidisciplinary
sample of health professionals was a strength of this research, as was the capture of
an international cohort through an online survey. The results and information
generated has the potential to aid the establishment of health professional education
resources and programs, and the development of NET nutrition guidelines.
One potential limitation of this research is sample size. Due to the resource and time
constraints of conducting a longitudinal study during a PhD candidature period, a
larger sample size was unable to be achieved. Attempts were made at including
additional study sites, and subsequently Austin Health was included as a recruitment
site. As this study was undertaken in part-fulfilment of a PhD, participant recruitment
and data collection was undertaken by the same person (Coordinating principal
investigator (CPI), PhD student) at both sites. As the CPI was based at Peter MacCallum
Cancer Centre, they had regular access to multidisciplinary meeting and clinic lists

232
which were used for screening potential participants. Only a small number of patients
were recruited from the second site (Austin Health) as the CPI was not available on site
to facilitate eligibility screening and instead relied on the local PI for this. At the
commencement of this research there was intent to perform statistical sub-analysis of
associations between malnutrition prevalence and disease and treatment factors (NET
site, NET grade, treatment type), however, this was not possible due to the sample
size. Alternatively, cross-tabulation was performed to explore any associations
descriptively. A limitation to longitudinal data collection is attrition over the data
collection period. At the commencement of the Phase 1 study, data was available for
59 participants. At T2, T4 and T6, respectively; 76% (n=45), 66% (n=39) and 80% (n=47)
of participants had available data for analysis. Descriptive analysis performed in the
Phase 1 study incorporated all available data where possible, to enable description of
the entire study population. Statistical analysis of change in results over-time, either
accounted for missing data (such as for HRQoL, using EORTC guidelines), or included
only available data within analysis (such as for malnutrition prevalence). When
scheduling focus groups for the Phase 2b study, attempts were made at inclusion of an
additional study site (Austin Health) however, it was not possible to secure scheduling
at this site. Further potential limitations of Phase 2a health professional survey are
discussed within the manuscripts included in Chapter 6.
8.3 Implications for clinical practice
Results presented in this thesis have identified significant under-recognition of
nutritional complications, despite their relatively high observed prevalence, in patients
diagnosed with a GEP NET. Despite the prevalence of nutritional complications, few
health professionals working in NET units are routinely screening for malnutrition or
nutritional issues when consulting with patients, and screening practices are reported
as inconsistent. The presence of nutritional complications in cancer patients such as
weight loss, muscle mass deterioration and malnutrition can lead to worsening
morbidity and quality of life for patients, including impaired recovery from treatment,
and increased risk of hospital admission and rising health care costs (Nitenberg and

233
Raynard, 2000; Arends et al., 2006). Optimising identification and management of
nutritional complications should therefore be a priority within the context of
comprehensive cancer supportive care initiatives for people affected by this disease.
The negative impact of dietary restriction and weight loss on patient’s HRQoL,
described by both patients and health professionals in Phase 1 and Phase 2 of this
research, further highlights the importance of addressing these problems.
8.3.1 Health professional education and nutrition information resources
In the Phase 2 study, health professionals identified that NET patients have trouble
accessing information on nutrition, and that apart from dietitians, health professionals
do not routinely provide advice on nutrition or screen for nutritional complications.
The differences in information provision from health professionals with expertise in
NETs versus those with limited experience managing NETs was also identified as an
issue. Patients were less likely to receive timely and appropriate nutrition information
from health professionals with limited NET experience. Therefore, health professionals
such as GPs, oncologists, nurses and allied health, with or without NET expertise must
be targeted for education. The limited availability of dietitians with expertise in the
nutritional management of NETs also poses a problem for provision of individualised
nutrition assessment and advice. Broad promotion of the nutritional complications
existing in patients with NETs and education on the optimal nutrition management of
NETs, targeting practising dietitians in Australia and internationally through
professional associations is important to improve patient care.
Results have highlighted the need for more robust health professional education on:
NETs and their nutritional impacts, and appropriate access to evidence-based nutrition
information for NETs. Collation of existing evidence-based nutrition information
resources through reputable organisations and websites, e.g. NeuroeEndocrine Cancer
Australia, Cancer Council Australia, would be beneficial. Identification of required
nutrition information and education resources, that are not currently available,
through patient and health professional surveys and focus groups, could assist to guide

234
the development of the required resources. Nutrition information priorities identified
through this research include symptom management and diet (with a focus on
managing common gastrointestinal NET symptoms such as diarrhoea, bloating,
abdominal discomfort), identifying and managing malnutrition and weight loss, and
general dietary advice (whilst living with a NET).
The development of NET-specific nutrition guidelines through a multidisciplinary
working group, is essential to educate health professionals on the importance of
nutrition in NET patients and guide consistent evidence-based nutrition practices. Lack
of nutrition guidelines specific to NETs and a paucity of evidence for prevalence of
nutritional complications was identified as a barrier to systematic health professional
nutrition screening and advice in this Phase 2 study. Prior to the development of NET-
specific nutrition guidelines, larger multi-site research is required to confirm the
prevalence and risk of vitamin deficiency among patients with NETs, and also the
prevalence and impact of dietary changes among NET patients, on HRQoL and
nutritional outcomes. The evaluation of feasible and effective nutrition interventions
(focusing on prevention and management of weight loss, malnutrition, dietary
restriction and the dietary management of symptoms) are necessary to inform content
of future guidelines.
Nutrition guidelines should refer to specific symptoms and nutritional complications
occurring in NET patients, rather than the nutritional impacts of cancer in general.
NETs are a unique, heterogenous type of cancer, with specific hormonal impacts not
seen in other cancers. Nutritional complications that are priorities to address in clinical
practice guidelines, as identified through research in this thesis, include:
• Malnutrition,
• Weight loss and muscle mass loss, and
• Dietary restriction,
• Risk of vitamin deficiency - whilst not explored in detail through this research,
should also be included in NET guidelines based upon existing literature
235
identifying vitamin deficiency (Niacin, fat-soluble vitamins) occurring among
NET patients.
Results of studies discussed in this thesis, combined with existing literature, suggest
that patients with advanced or progressive NET undergoing chemotherapy or major
surgery may be at increased nutritional risk; and patients with a lower grade NET
(Grade 1 NET) and undergoing PRRT or long-term SSA treatment with symptom
improvement, may be a lower nutritional risk. An appreciation of the impact of
treatment on nutritional risk will be important to incorporate into and guide future
individualised NET-specific nutrition guidelines.
8.3.2 Nutrition screening and assessment in patients with GEP NETs
Appropriate identification and management of nutritional complications in cancer
patients, relies on effective and consistent conduct of nutrition and malnutrition risk
screening (J. Arends et al., 2017; Jensen et al., 2019). Results from Phase 2 of research
in this thesis has highlighted, for the first time, that health professionals are not
routinely or systematically screening for nutritional complications among NET patients,
putting them at risk of under-detection and improper management. There is strong
evidence that all patients with cancer should be routinely screened for malnutrition (J.
Arends et al., 2017; Jann Arends et al., 2017; Jensen et al., 2019), and that routine
identification of malnutrition is important to prevent negative outcomes such as
worsening morbidity and quality of life.
Results from this thesis have provided comprehensive insights into the occurrence of
nutritional complications among patients with a GEP NET. The findings contribute
evidence to support the development of appropriate nutrition screening practices in
patients. Figure 8.1 presents a novel nutrition risk framework informed by evidence
generated through this comprehensive exploration of nutrition-related symptoms,
complications and health-related quality of life in patients with GEP NETs.

236
Figure 8.1 Nutrition Risk Framework
NUTRITION RISK
Nutrition factors
- Weight loss - Muscle loss - Malnutrition - Dietary change
Symptoms
- Diarrhoea - Abdo cramps - Bloating - LOA - Pain
NET characteristics and treatment
- High‐grade - Progressive - Chemo - SSA - Surgery
Patient attitudes and beliefs
COMPLEXITY

237
Through evaluation of results presented in this thesis, three main factors contributing
to nutrition risk in GEP NET patients were identified, amidst a complex context of
disease heterogeneity, symptomatology, uncertain prognosis, and varying treatment
modalities:
• Nutritional factors leading to nutrition risk include weight loss, muscle loss,
malnutrition and dietary change or restriction, which are largely consistent with
the GLIM criteria. However, dietary change was observed as mostly patient
directed and driven by their symptoms and did not necessarily present as a
reduction in dietary intake. Dietary change was also impacted by personal
attitudes and beliefs of patients regarding the importance of nutrition and
desire for control (through diet) over their disease and symptom management.
Malnutrition is included as a nutritional factor but presence of malnutrition is
influenced by weight loss, muscle mass loss and reduced dietary intake (Jensen
et al., 2019).
• Symptoms, whilst impacting on food consumption and dietary change, also can
subsequently lead to other nutritional factors such as weight loss, if prolonged
and severe. Key symptoms identified by patients and health professionals
through this research to impact on nutrition and diet included diarrhoea,
abdominal cramps/discomfort, bloating, loss of appetite and pain.
• NET disease characteristics and treatment modality contribute to nutrition risk
through adverse effects including inflammation and symptoms, leading to
difficulty eating and potential weight loss. High-grade NET, progressive disease,
chemotherapy and surgery have been identified as potentially at greatest risk
of causing nutritional issues.
Barriers to nutrition screening among NET health professionals included time, lack of
evidence/guidelines and belief the role sits with other clinicians (often the dietitian).
Due to the identified prevalence of malnutrition and other nutritional complications in
GEP NET patients, and strong evidence for routine malnutrition screening in patients
with cancer, all patients with NET should be screened for nutrition risk and

238
malnutrition. A nutrition screening tool that is optimal for NET patients should be
based upon evidence, be sensitive and specific enough to detect nutritional risk, and
also easy to use by health professionals. Existing malnutrition screening tools are
validated for use in the general cancer population and include the PG-SGA short form
(PG-SGA SF), malnutrition screening tool (MST), malnutrition universal screening tool
(MUST) and NRS 2002 (Bauer et al., 1997; Kondrup et al., 2003; Boléo-Tomé et al.,
2012; Abbott et al., 2016). To achieve a screening score, all consider factors of weight
change and change in appetite or total food intake. The MUST and NRS 2002 also take
into account the patients disease state (i.e. acute illness) and body mass index (BMI).
The PG-SGA SF includes symptoms impacting dietary intake. Of these existing validated
screening tools, the PG-SGA SF incorporates most of the factors contributing to
nutrition risk in NETs described in Figure 8.1, including nutrition factors (weight
change, reduction in total food intake) and symptom factors, and therefore may be a
suitable screening tool for use in patients with GEP NETs.
One key nutritional complication identified through this PhD research, that may not be
identified using existing nutrition screening tools, is the complex and varied dietary
restrictions initiated by patients with GEP NETs. Most nutrition screening tools focus
on the total reduction in food intake, which may contribute to risk of weight loss and
malnutrition but are not designed to detect more various dietary changes or
restrictions, such as those reported by patients with GEP NETs in this PhD research.
This PhD research has identified the significance of these dietary changes and
restrictions, including their high prevalence, and also the negative impact they can
have on patient HRQoL and social functioning. Therefore, identification of dietary
changes and restrictions need to be incorporated into a nutrition screening approach
for patients with NETs, in order to address this as a supportive care priority. The use of
an existing tool (e.g. the PG-SGA SF) in combination with a series of supplementary
questions addressing specific NET- and symptom-related dietary changes may be the
ideal approach. Development of a NET-specific nutrition screening tool supplement for
this purpose therefore would be beneficial to consider in future research.

239
Use of validated nutrition screening and assessment tools is an important
consideration for the identification of nutritional complications among GEP NET
patients. Further research is required to identify and validate the most appropriate
screening and assessment tools for use with GEP NET patients. The complexity of
symptomatology, and dietary restriction observed in patients in this research
highlights aspects of nutritional risk that may go undetected with use of existing tools.
Therefore, the establishment of nutrition risk criteria for GEP NET patients,
incorporated into future nutrition and clinical practice guidelines would be important,
as would the education of health professionals on factors contributing to nutrition risk
as discussed above.
8.4 Directions for future research
Results presented in this thesis, combined with existing literature suggest that
particular NET types and treatments (high-grade NET, progressive disease,
chemotherapy, major surgery) may be more susceptible to risk of weight loss and
malnutrition. Larger prospective longitudinal research studies are required to examine
the relationship between disease and treatment factors, and risk of malnutrition and
other nutritional complications such as weight loss and muscle mass loss. Larger
studies would also enable evaluation of symptom prevalence and severity, and the
occurrence of malnutrition.
This thesis describes the first comprehensive exploration of dietary change among
patients with a GEP NET and highlights high prevalence of dietary restriction in
response to symptoms. Further larger observational longitudinal studies are required
to examine the existence of any relationship between specific symptoms and
occurrence of dietary change, or if there is a relationship between dietary change and
symptom improvement. Once these relationships are explored, interventional research
testing the impact of specific dietary intervention on common GEP NET symptoms (e.g.
diarrhoea, abdominal pain/cramps, bloating) would be beneficial to contribute
evidence for optimal nutrition intervention in GEP NET patients. There are currently no

240
studies published, exploring the impact of nutrition education or intervention on
nutrition-related outcomes of GEP NET patients such as weight loss and malnutrition.
There are also no studies exploring the impact of nutrition education and intervention
on the dietary habits of GEP NET patients. As symptoms experienced by patients with a
GEP NET (diarrhoea, abdominal cramps, wind/gas), are potentially similar to those
experienced by people with other gastrointestinal disorders, such as irritable bowel
syndrome and inflammatory bowel disease, consideration of diets tested to be
effective in these other patient groups (e.g. low FODMAP, modified fibre) may be
helpful when planning future interventional nutrition research in NETs. The lack of
timely and NET-specific nutrition information was highlighted by patients involved in
this PhD research as a major issue, often prompting to them taking control of their
own nutritional monitoring and dietary change. The effect of early and pro-active
nutrition information provision to patients with a NET on the occurrence of self-
initiated dietary restriction would be useful to explore whether timely nutrition
information provision reduces the risk of unnecessary dietary change and subsequent
negative impacts on patients’ HRQoL.
Due to limitations on sample size, and sample heterogeneity, research in this thesis
was unable to clearly establish or confirm the presence of vitamin deficiencies in
patients with a GEP NET. This is particularly the case for niacin, with under 50% of
participants consenting to 24-hour urine sampling. Multi-centre trials are required to
thoroughly assess the presence of vitamin deficiency (niacin, fat-soluble vitamins) in a
larger cohort of GEP NET patients. Targeting recruitment of NET types that have been
identified in existing literature as at risk of vitamin deficiency would help to confirm
this relationship. For example, trials testing the presence of niacin deficiency should
target patients with diagnosed carcinoid syndrome or serotonin-producing NET.
The importance of establishing appropriate nutrition screening practices in GEP NET
patients has been discussed throughout this thesis. To advance progress in this work,
the establishment of an international, multidisciplinary working party, is required.
Qualitative research through surveys or focus groups and use of Delphi research

241
methodology, should be used to establish consensus for nutrition screening practices
and NET-specific nutrition guidelines. These insights will inform the next stages of
research in this important but under addressed area of oncology dietetics.


243
References
Aaronson, N. K. et al. (1993) ‘The European Organization for Research and Treatment
of Cancer QLQ-C30: A Quality-of-Life Instrument for Use in International Clinical Trials
in Oncology’, Journal of the National Cancer Institute, 85(5), pp. 365–376. doi:
10.1093/jnci/85.5.365.
Abbott, J. et al. (2016) ‘Patient-Generated Subjective Global Assessment Short Form
(PG-SGA SF) is a valid screening tool in chemotherapy outpatients’, Supportive Care in
Cancer, 24(9), pp. 3883–3887. doi: 10.1007/s00520-016-3196-0.
Albahrani, A. A. and Greaves, R. F. (2016) ‘Fat-Soluble Vitamins: Clinical Indications and
Current Challenges for Chromatographic Measurement.’, The Clinical biochemist.
Reviews. The Australian Association of Clinical Biochemists, 37(1), pp. 27–47.
Altieri, B. et al. (2018) ‘Nutrition and neuroendocrine tumors: An update of the
literature’, Reviews in Endocrine and Metabolic Disorders, 19(2), pp. 159–167. doi:
10.1007/s11154-018-9466-z.
Arends, J. et al. (2006) ‘ESPEN Guidelines on Enteral Nutrition: Non-surgical oncology’,
Clinical Nutrition, 25(2), pp. 245–259. doi: 10.1016/j.clnu.2006.01.020.
Arends, J. et al. (2017) ‘ESPEN expert group recommendations for action against
cancer-related malnutrition’, Clinical Nutrition, 36(5), pp. 1187–1196. doi:
10.1016/j.clnu.2017.06.017.
Arends, Jann et al. (2017) ‘ESPEN guidelines on nutrition in cancer patients’, Clinical
Nutrition, 36(1), pp. 11–48. doi: 10.1016/j.clnu.2016.07.015.
Australian Health Survey: Biomedical results for nutrients, 2011 - 2012. Vitamin D.
(2014) Australian Bureau of Statistics. Available at:

244
http://www.abs.gov.au/ausstats/[email protected]/Lookup/4364.0.55.006Chapter2002011-12
(Accessed: 4 November 2016).
Barazzoni, R. et al. (2018) ‘Sarcopenic obesity: Time to meet the challenge’, Clinical
Nutrition. Elsevier, 37(6), pp. 1787–1793. doi: 10.1016/J.CLNU.2018.04.018.
Barrea, L. et al. (2018) ‘Impact of Nutritional Status on Gastroenteropancreatic
Neuroendocrine Tumors (GEP-NET) Aggressiveness.’, Nutrients. Multidisciplinary
Digital Publishing Institute (MDPI), 10(12). doi: 10.3390/nu10121854.
Bauer, J. et al. (1997) ‘Validation of a Simple Quick Malnutrition Screening Tool’,
Journal of the American Dietetic Association. Elsevier, 97(9), p. A85. doi:
10.1016/S0002-8223(97)00619-6.
Bauer, J., Capra, S. and Ferguson, M. (2002) ‘Use of the scored Patient-Generated
Subjective Global Assessment (PG-SGA) as a nutrition assessment tool in patients with
cancer.’, European journal of clinical nutrition. Nature Publishing Group, 56(8), pp.
779–785. doi: 10.1038/sj.ejcn.1601412.
Beaumont, J. L. et al. (2012) ‘Comparison of Health-Related Quality of Life in Patients
With Neuroendocrine Tumors With Quality of Life in the General US Population’,
Pancreas, 41(3), pp. 461–466. doi: 10.1097/MPA.0b013e3182328045.
Bender, D. A. (1983) ‘Biochemistry of tryptophan in health and disease.’, Molecular
aspects of medicine, 6(2), pp. 101–97.
Bender, D. A. (2014) Introduction to nutrition and metabolism. Fifth Edition. CRC Press.
Bestvina, C. M. et al. (2014) ‘Patient-Oncologist Cost Communication, Financial
Distress, and Medication Adherence’, Journal of Oncology Practice, 10(3), pp. 162–167.
doi: 10.1200/JOP.2014.001406.
245
Boléo-Tomé, C. et al. (2012) ‘Validation of the Malnutrition Universal Screening Tool
(MUST) in cancer.’, The British Journal of Nutrition, 108(2), pp. 343–8. doi:
10.1017/S000711451100571X.
Borre, M. et al. (2018) ‘Nutritional status and nutritional risk in patients with
neuroendocrine tumors’, Scandinavian Journal of Gastroenterology, 53(3), pp. 284–
292. doi: 10.1080/00365521.2018.1430848.
Borre, M., Dam, G. A. and Grønbaek, H. (2019) ‘Use of biologically based
complementary medicines in patients with neuroendocrine tumors’, Scandinavian
Journal of Gastroenterology, 54(8), pp. 998–1002. doi:
10.1080/00365521.2019.1646799.
Bouma, G. et al. (2016) ‘Niacin (Vitamin B3) Supplementation in Serotonin Producing
Neuroendocrine Tumor Patients’, Neuroendocrinology, 103(5), pp. 489–94. doi:
10.1159/000440621.
Bower, J. E. (2014) ‘Cancer-related fatigue: Mechanisms, risk factors, and treatments’,
Nature Reviews Clinical Oncology, 11(10), pp. 597–609. doi:
10.1038/nrclinonc.2014.127.
Braun, V. and Clarke, V. (2006) ‘Using thematic analysis in psychology’, Qualitative
Research in Psychology, 3(2), pp. 77–101.
Burgess, A. (2005) ‘Diagnosing, treating and managing carcinoid tumours’, Nursing
Times, 101(29), pp. 32–34.
Burgess, A. (2008) ‘An overview of pancreatic neuroendocrine tumours.’, Nursing
Standard, 23(8), pp. 35-40 6p.
Caplin, M. E. et al. (2014) ‘Lanreotide in Metastatic Enteropancreatic Neuroendocrine
Tumors’, New England Journal of Medicine. Massachusetts Medical Society , 371(3),

246
pp. 224–233. doi: 10.1056/NEJMoa1316158.
Carlin, J. and Doyle, L. (2001) ‘Statistics for Clinicians 6: Comparison of means and
proportions using confidence intervals’, Journal of Paediatric and Child Health, 37, pp.
583–586.
Caruana, E. J. et al. (2015) ‘Longitudinal studies.’, Journal of thoracic disease. AME
Publications, 7(11), pp. E537-40. doi: 10.3978/j.issn.2072-1439.2015.10.63.
Castiello, R. J. and Lynch, P. J. (1972) ‘Pellagra and the Carcinoid Syndrome’, Archives of
Dermatology. American Medical Association, 105(4), p. 574. doi:
10.1001/archderm.1972.01620070046016.
Cella, D. et al. (2018) ‘Relationship Between Symptoms and Health-related Quality-of-
life Benefits in Patients With Carcinoid Syndrome: Post Hoc Analyses From TELESTAR’,
Clinical Therapeutics, 40(12). doi: 10.1016/j.clinthera.2018.10.008.
Chau, I. et al. (2013) ‘Quality of life, resource utilisation and health economics
assessment in advanced neuroendocrine tumours: a systematic review.’, European
Journal of Cancer Care, 22(6), pp. 714–25. doi: 10.1111/ecc.12085.
Clement, D. et al. (2019) ‘Nutritional and vitamin status in patients with
neuroendocrine neoplasms.’, World journal of gastroenterology, 25(10), pp. 1171–
1184. doi: 10.3748/wjg.v25.i10.1171.
Clement, D. S. V. M. et al. (2019) ‘Nutritional and vitamin status in patients with
neuroendocrine neoplasms’, World Journal of Gastroenterology, 25(10), pp. 1171–
1184. doi: 10.3748/wjg.v25.i10.1171.
Cocks, K. et al. (2012) ‘Evidence-based guidelines for interpreting change scores for the
European Organisation for the Research and Treatment of Cancer Quality of Life
Questionnaire Core 30’, European Journal of Cancer. Pergamon, 48(11), pp. 1713–

247
1721. doi: 10.1016/J.EJCA.2012.02.059.
Cohen, J. (1988) Statistical power analysis for the behavioral sciences. 2nd Ed.
Lawrence Erlbaum Associates.
Creswell, J. W. (2007) Qualitative inquiry and research design: Choosing among five
approaches. 2nd edn. Thousand Oaks, CA: Sage Publications.
Creswell, J. W. and Plano Clark, V. L. (2011) Designing and Conducting Mixed Methods
Research. 2nd Editio. Los Angeles: Sage Publications.
Cruz-Jentoft, A. J. and Sayer, A. A. (2019) ‘Sarcopenia’, The Lancet. Elsevier,
393(10191), pp. 2636–2646. doi: 10.1016/S0140-6736(19)31138-9.
D’Rummo, K. A. et al. (2019) ‘Assessing the Financial Toxicity of Radiation Oncology
Patients Using the Validated Comprehensive Score for Financial Toxicity as a Patient-
Reported Outcome’, Practical Radiation Oncology. doi: 10.1016/j.prro.2019.10.005.
Dasari, A. et al. (2017) ‘Trends in the Incidence, Prevalence, and Survival Outcomes in
Patients With Neuroendocrine Tumors in the United States’, JAMA Oncology, 3(10), pp.
1335–1342. doi: 10.1001/jamaoncol.2017.0589.
Davies, P. and Caplin, M. E. (2009) ‘Carciniod patients’ experiences of the influence of
diet and their symptoms’, in Neuroendocrinology, pp. 93–146. doi:
10.1159/000224772.
Delange, D. J. and Joubert, C. P. (1964) ‘Assessment of Nicotinic Acid Status of
Population Groups’, The American journal of clinical nutrition. American Society for
Nutrition, 15(3), pp. 169–74.
Diamond, T. et al. (2005) ‘Vitamin D and adult bone health in Australia and New
Zealand: a position statement’, Medical Journal of Australia, 182(6), pp. 281–285.

248
Fiebrich, H.-B. et al. (2010) ‘Deficiencies in fat-soluble vitamins in long-term users of
somatostatin analogue.’, Alimentary Pharmacology & Therapeutics, 32(11–12), pp.
1398–404. doi: 10.1111/j.1365-2036.2010.04479.x.
Fröjd, C. et al. (2007) ‘Health related quality of life and psychosocial function among
patients with carcinoid tumours. A longitudinal, prospective, and comparative study.’,
Health and Quality of Life Outcomes, 5, p. 18. doi: 10.1186/1477-7525-5-18.
Gabrielson, D. K. et al. (2013) ‘Use of an Abridged Scored Patient-Generated Subjective
Global Assessment (abPG-SGA) as a Nutritional Screening Tool for Cancer Patients in an
Outpatient Setting’, Nutrition and Cancer. Taylor & Francis Group , 65(2), pp. 234–239.
doi: 10.1080/01635581.2013.755554.
Gallo, M. et al. (2017) ‘The management of neuroendocrine tumours: A nutritional
viewpoint’, Critical Reviews in Food Science and Nutrition, pp. 1–12. doi:
10.1080/10408398.2017.1390729.
Glazer, E. S. et al. (2014) ‘Decreased inpatient mortality in obese patients with
abdominal nets.’, Endocrine Practice, 20(12), pp. 1309–14. doi: 10.4158/EP14203,OR.
Go, V. L. W., Srihari, P. and Kamerman Burns, L. A. (2010) ‘Nutrition and
gastroenteropancreatic neuroendocrine tumors.’, Endocrinology and Metabolism
Clinics of North America. Elsevier Ltd, 39(4), pp. 827–37. doi:
10.1016/j.ecl.2010.08.003.
Gordon, L. G. et al. (2020) ‘The Economic Impact on Australian Patients with
Neuroendocrine Tumours’, The Patient - Patient-Centered Outcomes Research.
Springer, 13(3), pp. 363–373. doi: 10.1007/s40271-020-00412-z.
Haugland, T. et al. (2009) ‘Health related quality of life in patients with neuroendocrine
tumors compared with the general Norwegian population’, Quality of Life Research,
18(6), pp. 719–726. doi: 10.1007/s11136-009-9487-x.

249
Haugland, T. et al. (2013) ‘Improvement in Stress, General Self-Efficacy, and Health
Related Quality of Life following Patient Education for Patients with Neuroendocrine
Tumors: A Pilot Study’, Nursing Research and Practice, 2013, p. 695820. doi:
10.1155/2013/695820; 10.1155/2013/695820.
Van Der Horst-Schrivers, A. N. A. et al. (2004) ‘Complications of midgut carcinoid
tumors and carcinoid syndrome’, Neuroendocrinology, 80(SUPPL. 1), pp. 28–32. doi:
10.1159/000080737.
Inglis, J. E. et al. (2019) ‘Nutritional Interventions for Treating Cancer-Related Fatigue:
A Qualitative Review’, Nutrition and Cancer. Taylor & Francis, 71(1), pp. 21–40. doi:
10.1080/01635581.2018.1513046.
Jager-Wittenaar, H. and Ottery, F. D. (2017) ‘Assessing nutritional status in cancer’,
Current Opinion in Clinical Nutrition & Metabolic Care, 20(5), pp. 322–329. doi:
10.1097/MCO.0000000000000389.
Jensen, G. L. et al. (2019) ‘GLIM Criteria for the Diagnosis of Malnutrition: A Consensus
Report From the Global Clinical Nutrition Community’, Journal of Parenteral and
Enteral Nutrition, 43(1), pp. 32–40. doi: 10.1002/jpen.1440.
Jimenez-Fonseca, P. et al. (2015) ‘Health-related quality of life in well-differentiated
metastatic gastroenteropancreatic neuroendocrine tumors’, Cancer and Metastasis
Reviews, 34(3), pp. 381–400. doi: 10.1007/s10555-015-9573-1.
Kaupp-roberts, S., Srirajaskanthan, R. and Ramage, J. K. (2015) ‘Symptoms and Quality
of Life in Gastroenteropancreatic Neuroendocrine Tumours’, EMJ Oncology, 3(1), pp.
34–40.
Kazis, L., Anderson, J. and Meenan, R. (1989) ‘Effect Sizes for Interpreting Changes in
Health Status’, Medical Care, 27(Suppl 3).

250
Keller, H. et al. (2020) ‘Global Leadership Initiative on Malnutrition (GLIM): Guidance
on Validation of the Operational Criteria for the Diagnosis of Protein‐Energy
Malnutrition in Adults’, Journal of Parenteral and Enteral Nutrition. John Wiley & Sons,
Ltd, 44(6), pp. 992–1003. doi: 10.1002/jpen.1806.
Kikut, J. et al. (2020) ‘Assessment and State of Nutrition of Patients with
Gastroenteropancreatic Neuroendocrine Neoplasms’, Nutrients, 12.
Kiss, N. et al. (2020) ‘Clinical Oncology Society of Australia: Position statement on
cancer‐related malnutrition and sarcopenia’, Nutrition & Dietetics. John Wiley & Sons,
Ltd, pp. 1747–0080.12631. doi: 10.1111/1747-0080.12631.
Kondrup, J. et al. (2003) ‘ESPEN Guidelines for Nutrition Screening 2002’, Clinical
Nutrition, 22(4), pp. 415–421. doi: 10.1016/S0261-5614(03)00098-0.
Krueger, R. A. (2002) Designing and Conducting Focus Group Interviews.
Laing, E. et al. (2018) ‘Investigating Nutrition-Related Complications and Quality of Life
in Patients With Gastroenteropancreatic Neuroendocrine Tumors: Protocol for a
Mixed-Methods Prospective Study’, JMIR Research Protocols, 7(12), p. e11228. doi:
10.2196/11228.
Laing, E. et al. (2019) ‘Nutritional complications and the management of patients with
gastroenteropancreatic neuroendocrine tumours’, Neuroendocrinology. doi:
10.1159/000503634.
Laing, E. et al. (2020) ‘Nutritional Complications and the Management of Patients with
Gastroenteropancreatic Neuroendocrine Tumors’, Neuroendocrinology. Karger
Publishers, 110(5), pp. 430–442. doi: 10.1159/000503634.
Lamarca, A. et al. (2018) ‘Somatostatin analogue-induced pancreatic exocrine
insufficiency in patients with neuroendocrine tumors: results of a prospective
251
observational study’, Expert Review of Gastroenterology & Hepatology. Taylor &
Francis, 12(7), pp. 723–731. doi: 10.1080/17474124.2018.1489232.
Lambert, G. (2008) ‘Does Intestinal Resection Affect the Absorption of Essential
Vitamins, Minerals, and Bile Salts? An Overview of the Literature’, Ostomy Wound
Management, 54(6), pp. 36–47.
Langer, C. J., Hoffman, J. P. and Ottery, F. D. (2001) ‘Clinical significance of weight loss
in cancer patients: rationale for the use of anabolic agents in the treatment of cancer-
related cachexia.’, Nutrition . Nutrition, 17(1 Suppl), pp. S1-20. doi: 10.1016/s0899-
9007(01)80001-0.
Larsson, G. et al. (2001) ‘Health-related Quality of Life, Anxiety and Depression in
Patients with Midgut Carcinoid Tumours’, Acta Oncologica, 40(7), pp. 825–831.
Larsson, G., von Essen, L. and Sjoden, P. O. (1998) ‘Quality of life in patients with
endocrine tumors of the gastrointestinal tract: Patient and staff perceptions’, Cancer
Nursing, 21(6), pp. 411–420. doi: 10.1097/00002820-199812000-00005.
Larsson, G., Haglund, K. and Von Essen, L. (2003) ‘Distress, quality of life and strategies
to “keep a good mood” in patients with carcinoid tumours: patient and staff
perceptions.’, European Journal of Cancer Care, 12(1), pp. 46–57. doi: 10.1046/j.1365-
2354.2003.00322.x.
Lathan, C. S. et al. (2016) ‘Association of Financial Strain With Symptom Burden and
Quality of Life for Patients With Lung or Colorectal Cancer’, Journal of Clinical
Oncology, 34(15), pp. 1732–1740. doi: 10.1200/JCO.2015.63.2232.
Leyden, S. et al. (2020) ‘Unmet needs in the international neuroendocrine tumor (NET)
community: Assessment of major gaps from the perspective of patients, patient
advocates and NET health care professionals’, International Journal of Cancer. John
Wiley & Sons, Ltd, 146(5), pp. 1316–1323. doi: 10.1002/ijc.32678.

252
Lind, A., Wängberg, B. and Ellegård, L. (2016) ‘Vitamin D and vitamin B12 deficiencies
are common in patients with midgut carcinoid (SI-NET)’, European Journal of Clinical
Nutrition, 70(9), pp. 990–994. doi: 10.1038/ejcn.2016.40.
Maasberg, S. et al. (2017) ‘Malnutrition Predicts Clinical Outcome in Patients with
Neuroendocrine Neoplasia.’, Neuroendocrinology, 104(1), pp. 11–25. doi:
10.1159/000442983.
Mann, C. J. (2003) ‘Observational research methods. Research design II: cohort, cross
sectional, and case-control studies.’, Emergency medicine journal : EMJ. British
Association for Accident and Emergency Medicine, 20(1), pp. 54–60. doi:
10.1136/emj.20.1.54.
Marín Caro, M. M., Laviano, A. and Pichard, C. (2007) ‘Nutritional intervention and
quality of life in adult oncology patients’, Clinical Nutrition, 26(3), pp. 289–301. doi:
10.1016/j.clnu.2007.01.005.
Mark, M. M. (2015) ‘The Oxford Handbook of Multimethod and Mixed Methods
Research Enquiry’, in Hesse-Biber, S. N. and Johnson, R. B. (eds). Oxford University
Press. doi: 10.1093/oxfordhb/9780199933624.013.15.
Marshall, K. M. et al. (2019) ‘Prevalence of malnutrition and impact on clinical
outcomes in cancer services: A comparison of two time points’, Clinical Nutrition,
38(2), pp. 644–651.
Martinez, P. et al. (2012) ‘Structural validity and distress screening potential of the
Hospital Anxiety and Depression Scale in cancer’, International Journal of Clinical and
Health Psychology, 12(3), pp. 435–447.
Martini, C. et al. (2016) ‘Systematic review reveals lack of quality in reporting health-
related quality of life in patients with gastroenteropancreatic neuroendocrine
tumours’, Health and Quality of Life Outcomes, 14(1), p. 127. doi: 10.1186/s12955-016-

253
0527-2.
Mercieca‐Bebber, R. et al. (2019) ‘The EORTC Quality of Life Questionnaire for cancer
patients ( QLQ ‐C30): Australian general population reference values’, Medical Journal
of Australia, 210(11), pp. 499–506. doi: 10.5694/mja2.50207.
Miller, W. L. and Crabtree, B. F. (2005) ‘Clinical Research’, in Denzin, N. and Lincoln, Y.
(eds) The Sage Handbook of Qualitative Research, 3rd Ed. 3rd edn. Sage Publications,
pp. 605–639.
Modlin, I. et al. (2010) ‘Gastrointestinal neuroendocrine (carcinoid) tumours: current
diagnosis and management’, Medical Journal of Australia, 193, pp. 46–52.
Morse, R., Kendell, K. and Barton, S. (2005) ‘Screening for depression in people with
cancer: the accuracy of the hospital anxiety and depression scale’, Clinical Effectiveness
in Nursing. Churchill Livingstone, 9(3–4), pp. 188–196. doi: 10.1016/j.cein.2006.08.012.
NHMRC (2006) ‘Niacin’, in Nutrient Reference Values for Australia and New Zealand
Including Recommended Dietary Intakes, pp. 79–84.
NHMRC (2014) Nutrient Reference Values for Australia and New Zealand: Vitamin D.
Ní Bhuachalla, E. et al. (2018) ‘Computed Tomography Diagnosed Cachexia and
Sarcopenia in 725 Oncology Patients: Is Nutritional Screening Capturing Hidden
Malnutrition?’, Journal of cachexia, sarcopenia and muscle. J Cachexia Sarcopenia
Muscle, 9(2). doi: 10.1002/JCSM.12258.
Nitenberg, G. and Raynard, B. (2000) ‘Nutritional support of the cancer patient: Issues
and dilemmas’, Critical Reviews in Oncology/Hematology, pp. 137–168. doi:
10.1016/S1040-8428(00)00048-2.
Northouse, L. et al. (2012) ‘Psychosocial Care for Family Caregivers of Patients With

254
Cancer’, Journal of Clinical Oncology, 30(11), pp. 1227–1234. doi:
10.1200/JCO.2011.39.5798.
Öberg, K. et al. (2012) ‘Neuroendocrine gastro-entero-pancreatic tumors: ESMO
Clinical Practice Guidelines for diagnosis, treatment and follow-up’, Annals of
Oncology, 23(SUPPL. 7), pp. vii124–vii130. doi: 10.1093/annonc/mds295.
Ottery, F. D. (1996) ‘Definition of standardized nutritional assessment and
interventional pathways in oncology.’, Nutrition (Burbank, Los Angeles County, Calif.).
Nutrition, 12(1 Suppl), pp. S15-9. doi: 10.1016/0899-9007(96)90011-8.
Patton, M. Q. (2015) Qualitative Research Evaluation Methods : Integrating Theory and
Practice. Fourth Edition. Sage Publications.
Pearman, T. P. et al. (2016) ‘Health-related quality of life in patients with
neuroendocrine tumors: an investigation of treatment type, disease status, and
symptom burden.’, Supportive care in cancer : official journal of the Multinational
Association of Supportive Care in Cancer, 24(9), pp. 3695–703. doi: 10.1007/s00520-
016-3189-z.
Plummer, P. (2017) ‘Focus group methodology. Part 1: Design considerations’,
International Journal of Therapy and Rehabilitation. MA Healthcare London , 24(7), pp.
297–301. doi: 10.12968/ijtr.2017.24.7.297.
Pobłocki, J. et al. (2020) ‘The Neuroendocrine Neoplasms of the Digestive Tract:
Diagnosis, Treatment and Nutrition’, Nutrients. Multidisciplinary Digital Publishing
Institute, 12(5), p. 1437. doi: 10.3390/nu12051437.
Qureshi, S. A. et al. (2016) ‘Screening for malnutrition in patients with gastro-entero-
pancreatic neuroendocrine tumours: a cross-sectional study.’, BMJ open. British
Medical Journal Publishing Group, 6(5), p. e010765. doi: 10.1136/bmjopen-2015-
010765.

255
Ramage, J. K. et al. (2012) ‘Guidelines for the management of gastroenteropancreatic
neuroendocrine (including carcinoid) tumours (NETs).’, Gut. BMJ Publishing Group Ltd
and British Society of Gastroenterology, 61(1), pp. 6–32. doi: 10.1136/gutjnl-2011-
300831.
Rinke, A. et al. (2009) ‘Placebo-controlled, double-blind, prospective, randomized
study on the effect of octreotide LAR in the control of tumor growth in patients with
metastatic neuroendocrine midgut tumors: a report from the PROMID Study Group.’,
Journal of clinical oncology : official journal of the American Society of Clinical
Oncology. J Clin Oncol, 27(28), pp. 4656–63. doi: 10.1200/JCO.2009.22.8510.
Robbins, H. L. et al. (2018) ‘Supplementation of Vitamin D Deficiency in Patients with
Neuroendocrine Tumors Using Over-the-Counter Vitamin D3 Preparations’, Nutrition
and Cancer. Taylor & Francis, 70(5), pp. 748–754. doi:
10.1080/01635581.2018.1470650.
Rosenbaum, K., Wang, J. and Kotler, D. (2000) ‘Time-dependent variation in weight and
body composition in healthy adults’, Journal of Parenteral and Enteral Nutrition, 24(2),
pp. 52–55. doi: 10.1177/014860710002400252.
Shah, G. M. et al. (2005) ‘Biochemical assessment of niacin deficiency among carcinoid
cancer patients.’, The American Journal of Gastroenterology, 100(10), pp. 2307–14.
doi: 10.1111/j.1572-0241.2005.00268.x.
Sheard, N. F. et al. (2004) ‘Dietary carbohydrate (amount and type) in the prevention
and management of diabetes: a statement by the american diabetes association.’,
Diabetes care. American Diabetes Association, 27(9), pp. 2266–71. doi:
10.2337/diacare.27.9.2266.
Singer, S. et al. (2009) ‘Hospital anxiety and depression scale cutoff scores for cancer
patients in acute care.’, British journal of cancer. Nature Publishing Group, 100(6), pp.

256
908–12. doi: 10.1038/sj.bjc.6604952.
Singh, S. et al. (2016) ‘Diagnosis and management of gastrointestinal neuroendocrine
tumors: An evidence-based Canadian consensus’, Cancer Treatment Reviews, pp. 32–
45. doi: 10.1016/j.ctrv.2016.05.003.
Singh, S. et al. (2017) ‘Patient-Reported Burden of a Neuroendocrine Tumor (NET)
Diagnosis: Results From the First Global Survey of Patients With NETs’, Journal of
Global Oncology. American Society of Clinical Oncology, 3(1), pp. 43–53. doi:
10.1200/JGO.2015.002980.
Snaith, P. (2003) ‘The Hospital Anxiety and Depression Scale’, Health and Quality of Life
Outcomes, 1(29). doi: 10.1186/s12955-014-0173-5.
Snyder, C. F. et al. (2015) ‘Identifying changes in scores on the EORTC-QLQ-C30
representing a change in patients’ supportive care needs.’, Quality of life research : an
international journal of quality of life aspects of treatment, care and rehabilitation. NIH
Public Access, 24(5), pp. 1207–16. doi: 10.1007/s11136-014-0853-y.
de Souza, J. A. et al. (2014) ‘The development of a financial toxicity patient-reported
outcome in cancer: The COST measure’, Cancer, 120(20), pp. 3245–3253. doi:
10.1002/cncr.28814.
de Souza, J. A. et al. (2017) ‘Measuring financial toxicity as a clinically relevant patient-
reported outcome: The validation of the COmprehensive Score for financial Toxicity
(COST).’, Cancer. Wiley-Blackwell, 123(3), pp. 476–484. doi: 10.1002/cncr.30369.
Strosberg, J. et al. (2018) ‘Health-Related Quality of Life in Patients With Progressive
Midgut Neuroendocrine Tumors Treated With 177Lu-Dotatate in the Phase III NETTER-
1 Trial.’, Journal of clinical oncology : official journal of the American Society of Clinical
Oncology. American Society of Clinical Oncology, 36(25), pp. 2578–2584. doi:
10.1200/JCO.2018.78.5865.

257
Toth-Fejel, S. and Pommier, R. F. (2004) ‘Relationships among delay of diagnosis,
extent of disease, and survival in patients with abdominal carcinoid tumors’, The
American Journal of Surgery, 187(5), pp. 575–579. doi: 10.1016/j.amjsurg.2004.01.019.
Vinik, A. I. et al. (2010) ‘NANETS consensus guidelines for the diagnosis of
neuroendocrine tumor.’, Pancreas, 39(6), pp. 713–734. doi:
10.1097/MPA.0b013e3181ebaffd.
Yadegarfar, G. et al. (2013) ‘Validation of the EORTC QLQ-GINET21 questionnaire for
assessing quality of life of patients with gastrointestinal neuroendocrine tumours.’,
British journal of cancer, 108(2), pp. 301–310. doi: 10.1038/bjc.2012.560.
Zafar, S. Y. et al. (2015) ‘Population-Based Assessment of Cancer Survivors’ Financial
Burden and Quality of Life: A Prospective Cohort Study’, Journal of Oncology Practice,
11(2), pp. 145–150. doi: 10.1200/JOP.2014.001542.
Zigmond, A. S. and Snaith, R. P. (1983) ‘The hospital anxiety and depression scale.’,
Acta psychiatrica Scandinavica, 67(6), pp. 361–70.


259
Appendices


261
Appendix 1: Nutrition in NETs Questionnaire 1.0
Nutrition in NETs - Questionnaire 1.0
Section 1: Dietitian Contact
The following questions will ask for information on any contact you have had with a
dietitian. Please answer each question as best as you can. If you are unsure of how to
answer a question, you can talk to the researcher who gave you this form.
Question 1. Have you seen a dietitian in the past month?
☐ Yes (Go to Question 2)
☐ No (Go to Section 2 Dietary Habits)
☐ Unsure (Go to Section 2 Dietary Habits)
If you have seen a dietitian please complete the following questions:
Question 2. Where did you see a dietitian?
☐ Hospital
☐ Community centre
☐ Private clinic
☐ Unsure
☐ Other___________________________________

262
Question 3. Who referred you to see a dietitian?
☐ My doctor
☐ My nurse
☐ Myself
☐ Unsure
☐ Other___________________________________
Question 4. What was the main reason you saw a dietitian?
☐ To talk about my diet
☐ I was losing weight
☐ I was gaining weight
☐ To help manage my symptoms
☐ I had difficulty tolerating some foods in my diet
☐ Other___________________________________
Question 5. Did you receive any of the following advice or management from the dietitian? (Tip: you can tick more than one)
☐ Information on changing my diet
☐ Information on managing my symptoms
☐ Taking oral supplements or high protein drinks

263
☐ Feeding through a tube
☐ Taking vitamin supplements
☐ Other____________________________________
Section 2: Dietary Habits
The following questions ask for information about your diet and any changes you may
have had to make since being diagnosed with a neuroendocrine tumour (NET). Please
answer each question as best as you can. If you are unsure of how to answer a
question, you can talk to the researcher who gave you this form.
Question 1. Have you had to make any changes to your diet or the way you eat since
you were diagnosed with a NET?
☐ Yes
☐ No (you do not need to complete any other questions, please hand the form back to
the researcher)
Question 2. If you answered yes to Question 1, are there any foods or drinks on the
following list that you avoid or consume less since your diagnosis of a NET?
☐ Fish ☐ Alcohol
☐ Red meat ☐ Coffee
☐ Chicken ☐ Tea
☐ Nuts ☐ Milk

264
☐ Fruit
☐ Cheese
☐ Yoghurt
☐ Bread
Is there any other type of food or drink, not listed, that you avoid or consume less?
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
_______________________________________________________________________
Question 3. Since you were diagnosed with a NET, have you had to make any of the
following changes to the way you eat? (Please tick any that apply to you)
Change: Tick
Size of meals – I have to eat smaller meals
Size of meals – I have to eat bigger meals
Type of food - I have to avoid particular foods
Type of drinks - I have to avoid particular drinks

265
How often you eat – I have to eat more frequently
How often you eat– I have to eat less frequently
How often you drink -– I have to drink fluids more frequently
How often you drink -– I have to drink fluids less frequently
Are there any other changes you have had to make? If yes, please write them
here:
Question 4. Have any of the following symptoms changed the way you eat? For
example, what you eat, when you eat or how much you eat? (You can tick more than
one)
Symptom Tick Not
applicable - I
do not have
this
symptom
Feeling tired/less energy
Short of breath
Pain
Loss of appetite
Discomfort in abdomen
Bloating
Wind or gas
Indigestion or heartburn

266
Nausea
Vomiting
Constipation
Diarrhoea
Feeling flushed or flushing
Night sweating
Weight gain
Weight loss
Are there any other symptoms you have that have changed
the way you eat – If yes, please write them here:
Question 5. Of the symptoms you ticked in Question 4 above do any bother you
more than others?
☐ Yes
☐ No
If yes, please tick which ones:
Symptom Tick

267
Feeling tired/less energy
Short of breath
Pain
Loss of appetite
Discomfort in abdomen
Bloating
Wind or gas
Indigestion or heartburn
Nausea
Vomiting
Constipation
Diarrhoea
Feeling flushed or flushing
Night sweating
Weight gain
Weight loss
Are there any others that are not listed?
Write them here:
For those you have ticked, please can you explain why they bother you more than
others

268
_____________________________________________________
_____________________________________________________
_____________________________________________________

269
Appendix 2: HRQoL raw scores and comparisons to general/NET population
Appendix 2 – Table 1: Raw scores for EORTC QLQ-C30 and GI.NET21 at all time-points, values are mean and standard deviation
Scale/item T0
(n = 59)
T2
(n = 45)
T4
(n = 37)
T6
(n = 44)
EORTC QLQ-C30
Global health status 63 (22) 61 (27) 68 (25) 68 (21)
Physical functioning 82 (21) 77 (25) 81 (21) 82 (22)
Role functioning 78 (31) 67 (37) 78 (29) 78 (28)
Emotional functioning 73 (23) 74 (24) 81 (20) 76 (21)
Cognitive functioning 78 (22) 76 (21) 83 (17) 77 (21)
Social functioning 74 (29) 68 (31) 78 (26) 77 (21)
Fatigue 35 (26) 43 (30) 33 (22) 34 (26)
Nausea/vomiting 11 (22) 12 19) 7 (13) 6 (12)
Pain 29 (32) 29 (30) 19 (25) 25 (31)
Dyspnoea 13 (23) 18 (27) 14 (20) 14 (24)
Insomnia 42 (32) 37 (32) 23 (29) 33 (31)
Appetite loss 19 (27) 24 (32) 17 (26) 15 (22)
Constipation 15 (23) 14 (19) 7 (14) 14 (22)
Diarrhoea 22 (29) 24 (30) 24 (30) 22 (30)
Financial problems 23 (32) 26 (34) 18 (30) 21 (36)
EORTC GI.NET21
Endocrine 19 (19) 10 (13) 12 (18) 11 (15)
Gastrointestinal 27 (20) 25 (21) 23 (18) 23 (17)
Treatment-related symptoms 16 (19) 18 (19) 16 (17) 20 (20)
Social function 42 (24) 42 (22) 28 (20) 35 (24)

270
Disease-related worries 56 (28) 52 (27) 36 (25) 46 (27)
Muscle/bone pain 30 (32) 30 (31) 18 (20) 31 (26)
Sexual function 36 (37) 32 (40) 19 (28) 31 (35)
Information/communication function
15 (27) 10 (21) 7 (16) 11 (26)
Body image 29 (41) 31 (40) 22 (34) 19 (36)

271
Appendix 2 – Table 2: Comparison of baseline (T0) HRQoL scale and item scores between study data and baseline scores from previously published data of general Australian population and NET populations, values are mean and standard deviation
Gen Pop NET Pop NET Pop NET Pop NET pop
Scale/item
Baseline score (T0)
N = 59
Mercieca-Bebber et al. 2019
N = 1821
Larsson et al. 2001
N = 24
Frojd et al.
2007
N = 59
Strosberg et al. 2018
N = 231
Cella et al. 2018
N = 135
EORTC QLQ-C30
Global health status 63 (22) 69 (22) 68 (23) 58 (19) 67 (22) 55 (19)
Physical functioning 82 (21) 89 (19) 85 (20) 80 (22) 83 (20) 78 (20)
Role functioning 78 (31) 89 (23)a 65 (33) a 53 (39) a 75 (30) 64 (31) a
Emotional functioning 73 (23) 81 (24) 73 (21) 77 (20) 75 (24) 71 (24)
Cognitive functioning 78 (22) 88 (22)a 83 (20) 85 (21) 83 (22) 77 (22)
Social functioning 74 (29) 91 (24)a 85 (20) a 77 (26) 77 (31) 67 (29)
Fatigue 35 (26) 24 (22)a 36 (24) 35 (26) 33 (26) 43 (26)
Nausea/vomiting 11 (22) 4.6 (17) 19 (24) 3 (8) 9 (15) 14 (18)
Pain 29 (32) 22 (26) 19 (24) a 20 (28) 28 (30) 34 (29)
Dyspnoea 13 (23) 12 (23) 19 (28) 27 (31) a 18 (27) 22 (26)
Insomnia 42 (32) 24 (30)a 24 (35) a 18 (24) a 28 (32) a 31 (33) a
Appetite loss 19 (27) 9 (22)a 25 (34) 10 (19) 15 (23) 20 (28)
Constipation 15 (23) 9 (23) 15 (29) 9 (22) 6 (16) 1 (6) a
Diarrhoea 22 (29) 6 (20)a 46 (39) a 25 (35) 43 (33) a 78 (27) a

272
Financial problems 23 (32) 6 (24)a 6 (16) a 14 (23) 23 (33) 24 (32)
EORTC GI.NET21
Endocrine 18 (19) - - - 22 (21) 32 (25)a
Gastrointestinal 27 (20) - - - 23 (20) 31 (20)
Treatment-related symptoms 17 (19) - - - 12 (14) 14 (17)
Social function 42 (24) - - - 33 (26) 43 (25)
Disease-related worries 56 (28) - - - 44 (28) a 40 (27) a
Muscle/bone pain 30 (32) - - - 29 (31) 33 (31)
Sexual function 34 (37) - - - 31 (39) 43 (39)
Information/communication function
15 (27) - - - 5 (14) a 6 (17)
Body image 30 (41) - - - 20 (32) a 31 (36)
Notes.
aDifference in mean score of 10 or greater in comparison to general Australian population, considered clinically significant between-group difference (Cocks et al., 2012)
Larsson study, median 62yo, mid-gut NETs, 75% metastatic, 83% carcinoid syndrome, interferon or SSA treatment (Larsson et al., 2001)
Frojd study, mean 60yo, confirmed carcinoid tumor (NET), 41% SSA treatment, 44% no treatment, all inpatients (Fröjd et al., 2007)
Strosberg study, mean 63-64yo, mid-gut NETs, 100% previous SSA (Strosberg et al., 2018)
Cella study, mean 64yo, 100% metastatic NETs, 100% carcinoid syndrome (Cella et al., 2018)

273
Appendix 3: Complete results for symptom impact on dietary change
Appendix 3 - Table 1 Symptoms reported by participants to impact on dietary change
T0 T2 T4 T6
n N n N n N n N
Loss of appetite 14 15 11 14 9 10 11 15
Nausea 11 13 10 17 5 11 6 9
Vomiting 7 9 5 8 0 4 1 3
Discomfort in abdomen 19 25 13 21 9 14 10 17
Bloating 16 24 12 16 8 13 11 14
Diarrhoea 15 23 10 17 8 15 9 13
Wind or gas 14 24 9 19 7 17 9 15
Pain 14 26 7 19 7 11 6 15
Constipation 7 14 5 10 1 6 4 9
Weight loss 10 21 8 15 6 14 8 11
Feeling tired/less energy 12 18 10 22 9 18 10 18
Indigestion or heartburn 7 19 4 8 2 8 3 11
Weight gain 4 11 3 8 3 6 8 12
Short of breath 5 14 3 12 2 7 1 10
Night sweating 4 16 1 10 1 8 1 9
Feeling flushed or flushing 3 17 3 12 3 7 1 11
Notes.
N = total number of participants reporting to experience that symptom at each time-point
n = total number of participants with the symptom reporting it impacted their diet


275
Appendix 4: Phase 1 patient interview schedule
Phase 1: Patient interviews
Overall research aim:
To describe the experience of people living with gastroenteropancreatic
neuroendocrine tumours, with particular focus on dietary intake, nutritional status and
the prevalence and severity of nutrition-related symptoms.
Focus:
Does a diagnosis and treatment of NET impact QOL?
Do nutrition needs change after a diagnosis of NET?
What extent of intervention has been received from clinicians regarding nutrition?
Baseline Interview
Potential questions:
1. Can you please tell me how things have been for you since you were first
diagnosed with a NET?
2. Had you been unwell or some time before your diagnosis – if so what
symptoms did you have?
3. Have you had any challenging or unexpected things to deal with since your
diagnosis?
4. Had you heard of a NET before you were diagnosed? Where/how did you get
information about the condition? Was it hard to get information?
Emotional health questions:
5. How are you coping/did you cope with your diagnosis?
6. How have you found support/information since your diagnosis?

276
Nutrition questions:
7. Have you noticed any issues with your eating since diagnosis?
8. Have you noticed any issues with your weight since diagnosis?
9. Have changes to your eating or weight impacted on your day to day life? If yes,
in what way?
10. Have you been offered any advice about managing your nutrition, eating or
weight?
If yes, can you please describe the advice you received? Who provided this
advice?
a. Prompt: Would you change the nutrition care you received?
b. Prompt: Has any of the advice been particularly helpful? If so, what?
11. Is there any information about nutrition that you have learnt since your
diagnosis that would have been helpful to know early on? If yes, what?
If they received treatment at another centre prior to referral to Peter Mac/ONJ
Centre:
12. Do you have any symptoms or side-effects from treatment you received prior
to attending Peter Mac/Olivia Newton John Cancer Centre that have affected
your eating or weight?
Six-month Interview
Potential questions:
1. Can you please tell me how you have been managing since you first attended
Peter Mac/Olivia Newton John Cancer Centre?
2. Have you felt unwell over the past few months - if so can you describe how?
What symptoms have you had?
3. Have you had any challenging or unexpected things to deal with since you
started receiving care or treatment at Peter Mac/Olivia Newton John Cancer
Centre?

277
Emotional health questions:
4. How have you been coping with your diagnosis?
5. How have you found support/information since your diagnosis? Is there any
other support or information you wish you had received?
Nutrition questions:
Begin with ‘Since you last interview six-months ago’ or ‘Since you started receiving care
at Peter Mac/Olivia Newton John Cancer Centre’
6. Have you noticed any issues with your eating?
7. Have you noticed any issues with your weight?
8. Do you have any symptoms or side-effects from treatment that have affected
your eating or weight?
9. Have changes to your eating or weight impacted on your day to day life? If yes,
in what way?
10. Have you been offered any advice about managing your nutrition, eating or
weight?
If yes, can you please describe the advice you received? Who provided this
advice?
a. Prompt: Would you change the nutrition care you received?
b. Prompt: Has any of the advice been particularly helpful? If so, what?
11. Is there any information about nutrition that you have learnt since your
diagnosis that would have been helpful to know early on? If yes, what?


279
Appendix 5: Health professional focus group question schedule
Phase 2b: Health professional focus groups
Demographic questionnaire (to be completed prior to focus group)
Please complete the following two questions prior to participation in the focus group:
1. What is your area of specialty (tick)?
☐ Medical oncology
☐ Surgical oncology
☐ Radiation oncology
☐ Nuclear medicine
☐ Gastroenterology
☐ Endocrinology
☐ Other physician (please specify________________)
☐ Nursing (please specify___________________)
☐ Dietitian
☐ Other allied health (please specify_______________________)
2. Please provide an estimate of the number of NET patients that you have contact with or manage each year (tick)?
☐ < 10 per year
☐ 10 – 25 per year
☐ 26 – 50 per year
☐ 51 - 100 per year
☐ > 100 per year
Phase 2b: Focus and questions for discussion during focus group
Overall research aim:
To describe health professional perceptions of nutrition issues amongst patients with NET and summarise current nutrition and management practices.
280
Focus:
Is nutrition considered important within the overall context of a NET patients management/treatment?
What similarities or differences are there amongst health professionals in regards to the screening and management of malnutrition in NET patients?
What similarities of differences are there amongst health professionals in regards to the management of nutrition issues overall (including vitamin deficiencies, change in diet, food intolerances)?
Potential questions:
1. In your experience, what issues are most important to a person newly diagnosed with a NET?
Prompts:
a. What kinds of things to people commonly ask you about or seem most concerned about for example, the disease itself or treatments available to them or prognosis?
2. Do NET patients usually ask you about nutrition issues? Can you describe this in more detail?
Prompts:
a. In regards to nutrition what do NET patients report to be most concerning?
b. What is the most common question you get asked relating to nutrition? c. Do NET patients talk to you about any particular symptoms that impact
on their eating or weight? d. Do you believe nutrition issues (weight loss, change in diet) affect the
quality of life of NET patients? If so, in what way? e. When do nutrition concerns usually arise? At diagnosis, during
treatment, post treatment?
3. In your experience, is malnutrition a concerning problem amongst NET patients? Can you describe why? (Note: describe definition of malnutrition as 5% unintentional weight loss over 3 months, or 10% unintentional weight loss over 6 months)
Prompts:
a. How common is weight loss amongst NET patients? Why? b. How common is weight gain amongst NET patients? Why? c. How common is malnutrition amongst NET patients? Why?

281
d. How common are food intolerances amongst NET patients? Why? e. Do you find that NET patients change their diet due to their NET disease
or treatment? Can you provide some examples?
4. Do you screen for malnutrition when you consult with NET patients? If yes, describe how?
a. Do you believe screening for malnutrition should be a part of standard care for NET patients? If so, by Who? Why?
5. Do you screen for vitamin deficiencies when you consult with NET patients? If you do, describe which ones and why?
a. Do you believe screening for vitamin deficiencies should be a part of standard care for NET patients? If so, by who? Why?
6. Do you routinely give advice about managing nutrition, eating or weight management to NET patients? If so, what kind of advice to you give?
7. Do you believe that there is adequate evidence to inform best practice for management of nutritional issues for patients with NETs?
8. Can you identify any area of research that if prioritised, could make a helpful contribution to the nutritional care of patients with NETs?


283
Glossary
Term Abbreviation Definition
Bioelectrical impedance analysis BIA Method for estimating body
fat and muscle mass, when a
weak electric current flows
through the body to
calculate resistance
(impedance)
Body mass index BMI Calculated by dividing a
person’s weight (kg) by their
height (m2)
Carcinoid syndrome Cluster of symptoms caused
by a neuroendocrine tumour,
usually located in either the
gut or lung, that secretes
hormones
Gastrinoma Tumour located in the
pancreas or duodenum that
produces excessive levels of
the hormone gastrin
Gastroenteropancreatic
neuroendocrine tumour
GEP NET Neurendocrine tumour of
the gastrointestinal tract or
pancreas
Global Leadership Initiative on
Malnutrition
GLIM

284
Glucagonoma Tumour located in the
pancreas that produces
excessive levels of the
hormone glucagon
Fat free mass FFM Encompasses components of
body tissue including internal
organs, muscle, water and
connective tissue
Flushing Symptom of NET
characterised by redness of
the face
Functional tumour A tumour (e.g. NET) that
produces excessive
hormones, often leading to
symptoms
Inflammatory bowel disease IBD Condition causing
inflammation of the digestive
system, including ulcerative
colitis and Chron’s disease
Irritable bowel syndrome IBS Symptoms or condition often
characterised by a
combination of abdominal
pain, bloating, and
alternating constipation and
diarrhoea
285
Insulinoma Tumour located in the
pancreas that produces
excessive levels of insulin
Malnutrition Refers to imbalance (excess
or deficiency) in a person’s
intake of energy and/or
nutrients, associated with
adverse functional and
clinical outcomes
Malnutrition Universal Screening
Tool
MUST Type of malnutrition risk
screening tool
Malnutrition Screening Tool MST Type of malnutrition risk
screening tool
Neuroendocrine tumour NET Tumour arising from
neuroendocrine cells
Niacin Essential vitamin, also known
as vitamin B3
Nutrition Risk Screening tool NRS-2002 Nutrition risk screening tool
Patient-Generated Subjective Global
Assessment
PG-SGA Malnutrition assessment tool
Patient-Generated Subjective Global
Assessment Short Form
PG-SGA SF Nutrition risk screening tool
Peptide receptor radionucleotide
therapy
PRRT A type of radiation treatment
injected into the
bloodstream, targeting

286
somatostatin receptors on
NET cells
Subjective Global Assessment SGA Malnutrition assessment tool
Somatostatin analogue SSA A drug/treatment that has
anti-secretory effects
(reduces hormone
production of NETs)

Minerva Access is the Institutional Repository of The University of Melbourne
Author/s:
Laing, Erin Clare
Title:
Understanding nutrition-related symptoms, complications and health-related quality of life in
patients with gastroenteropancreatic neuroendocrine tumours
Date:
2020
Persistent Link:
http://hdl.handle.net/11343/265872
File Description:
Final thesis file
Terms and Conditions:
Terms and Conditions: Copyright in works deposited in Minerva Access is retained by the
copyright owner. The work may not be altered without permission from the copyright owner.
Readers may only download, print and save electronic copies of whole works for their own
personal non-commercial use. Any use that exceeds these limits requires permission from
the copyright owner. Attribution is essential when quoting or paraphrasing from these works.