Erectile Dysfunction in 2010. Erectile Dysfunction Erectile dysfunction is defined as the consistent...
64
Erectile Dysfunction in 2010
-
Upload
darcy-conley -
Category
Documents
-
view
220 -
download
2
Transcript of Erectile Dysfunction in 2010. Erectile Dysfunction Erectile dysfunction is defined as the consistent...
Erectile Dysfunction in 2010
Erectile Dysfunction in 2010
Erectile DysfunctionErectile Dysfunction
Erectile dysfunction is defined as the consistent inability to attain or maintain a penile erection of sufficient quality to permit satisfactory sexual intercourse.
The prevalence of this condition increases with age.
It has been estimated that the worldwide prevalence of erectile dysfunction will be 322 million cases by the year 2025.
The risk of ED was 26 cases per 1000 men annually, which increased with age, lower education, DM, heart disease, and hypertension.
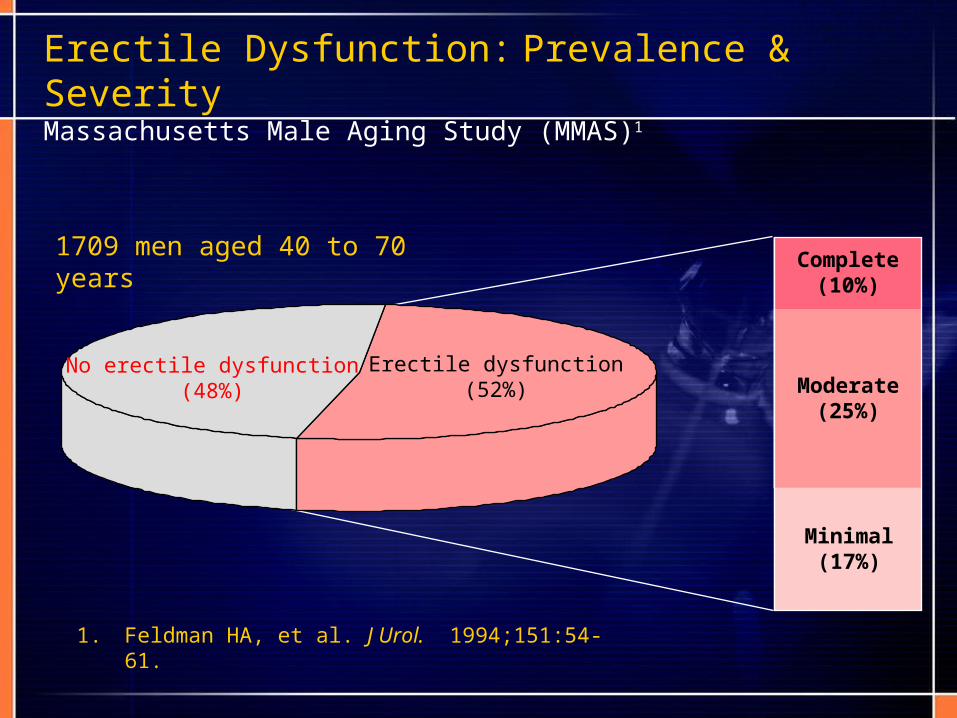
Erectile Dysfunction: Prevalence & SeverityMassachusetts Male Aging Study (MMAS)1
No erectile dysfunction(48%)
Erectile dysfunction(52%)
Complete(10%)
Moderate(25%)
Minimal(17%)
1709 men aged 40 to 70 years
1. Feldman HA, et al. J Urol. 1994;151:54-61.

(International Society of Impotence Research 1999)
Common risk factors for EDCommon risk factors for ED
Atherosclerosis • Caused Vasculogenic ED, whereas endothelial damage is the
proposed mechanism. Aging
• Alterations in the levels of NO that occur as a consequence of the aging endothelium.
• Chronic illness, depression, and lack of a sexual partner are all prevalent in this aging population.
Chronic tobacco use • Caused vasculogenic ED because of its effects on the vascular
endothelium. • Blood nicotine levels rise after smoking, which increases
sympathetic tone in the penis and leads to nicotine-induced, smooth-muscle contraction in the cavernosal body.
• leads to decreased penile NOS activity and neuronal NOS content.

Common risk factors for EDCommon risk factors for ED
Diabetes Mellitus • In the MMAS, the diabetic subset had a threefold increased prevalence of
ED compared with nondiabetic subjects (28% versus 9.6%). • The overall incidence rate of ED was 26 cases per 1000 man-years in
nondiabetics and 50 cases per 1000 man-years in the diabetic population. • The pathogenesis of ED in the diabetic patient is related to accelerated
atherosclerosis, alterations in the corporal erectile tissue, and neuropathy.Hypertension
• Both antihypertensive agents as well as the disease itself also contribute to ED.
• Certain classes of antihypertensive medications are notorious for their negative impact on erectile function, such as thiazides and β-blockers.
Hyperlipidemia• Contributed to ED by its relationship to endothelial dysfunction. • Study showed that decreasing total cholesterol to less than 200mg/dL by
using atorvastatin (Lipitor) led to significant improvement of ED.
Clinical assessment of ED patientsClinical assessment of ED patients
Differentiate between decreased libido and ED: assess whether the patient has one or bothTobacco use: type, amount, durationAlcohol intakeHistory of depression or anxiety disorderPresence of social/relationship stressorsAbility to have erections while masturbating versus when with partnerList of all prescription, over-the-counter, and herbal medicationsKnowledge of whether nocturnal erections are presentHistory of drug use: marijuana, cocaine, ketamine, other recreational drugsHistory of genitourinary traumaHistory of prostatic disease, or possible related symptomsHistory of hypertension, hyperlipidemia, CAD, peripheral vascular disease, cerebrovascular diseaseHistory of DMHistory of spinal cord injuryHistory of penile plaques: possible Peyronie's diseaseFrequency of intercourse or attempted intercourseAbility to ejaculate

Tools for ED evaluationTools for ED evaluation
International Index of Erectile Function (IIEF)
Sexual Encounter Profile (SEP)
Global Assessment Question (GAQ)
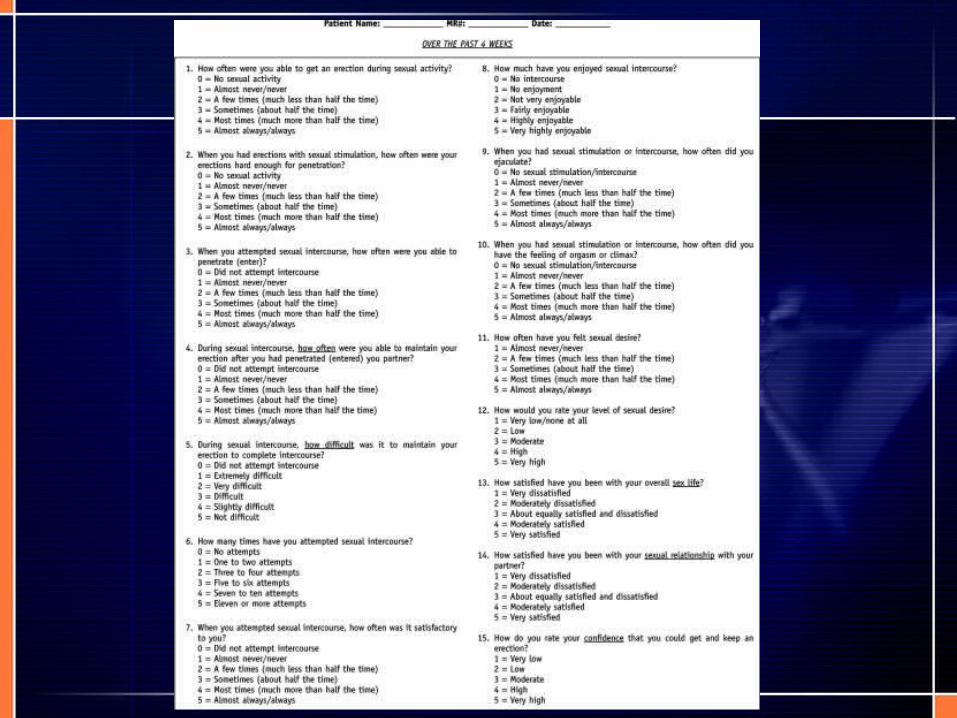
International Index of Erectile Function (IIEF)International Index of Erectile Function (IIEF)
a standardized questionnaire designed to measure ED and detect treatment-related changes reported by Rosen in 1997.
It is a 15-item questionnaire addressing 5 different domains: erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall satisfaction.
The IIEF is the most frequently used efficacy measurement employed in ED drug trials. Using a scale from 1 (never/almost never) to 5 (almost always/always), men grade each domain.
It is very sensitive and specific, and has been validated in 20 languages.
IIEF-5IIEF-5
To provide doctors with a “checklist” on erectile function that could be used in an office setting, an abridged 5-item version of the IIEF-15 has been developed by Rosen in 1999. 4 items are taken from the erectile function domain, plus another item addressing sexual intercourse satisfaction; it was chosen to reflect the central element in the NIH Consensus Panel (1992) definition of ED, which ties erectile function to satisfaction: “maintain erection of sufficient rigidity and duration to permit satisfactory sexual performance.” Perhaps the most important difference between the IIEF-15 and the IIEF-5 is that the latter asks patients to self-assess erectile function and satisfaction over the past 6 months, a more clinically relevant and practical time frame than 4 weeks. ED severity is classified into five categories based on the IIEF-5: severe (5 to 7), moderate (8 to 11), mild to moderate (12 to 16), mild (17 to 21), and no ED (22 to 25).
Sexual Encounter Profile (SEP)Sexual Encounter Profile (SEP)
SEP is a five-question survey provided to patients with ED in clinical studies of oral therapies. The survey is completed after each sexual attempt.
• 1. Were you able to achieve at least some erection?• 2. Were you able to insert your penis into your partner's
vagina?• 3. Did your erection last long enough to have successful
intercourse?• 4. Were you satisfied with the hardness of your erection?• 5. Were you satisfied with the overall sexual experience?
Answers to questions 2 and 3 are the ones most often used in the literature.
Global Assessment Questions (GAQ)Global Assessment Questions (GAQ)
GAQ is usually administered at the end of the treatment period during efficacy studies.
Question 1: Has the treatment taken during the study improved your erections?
Question 2: If yes, has the treatment improved your ability to engage in sexual activity?
This is very subjective, and its responses tend to be valued less than SEP and IIEF.
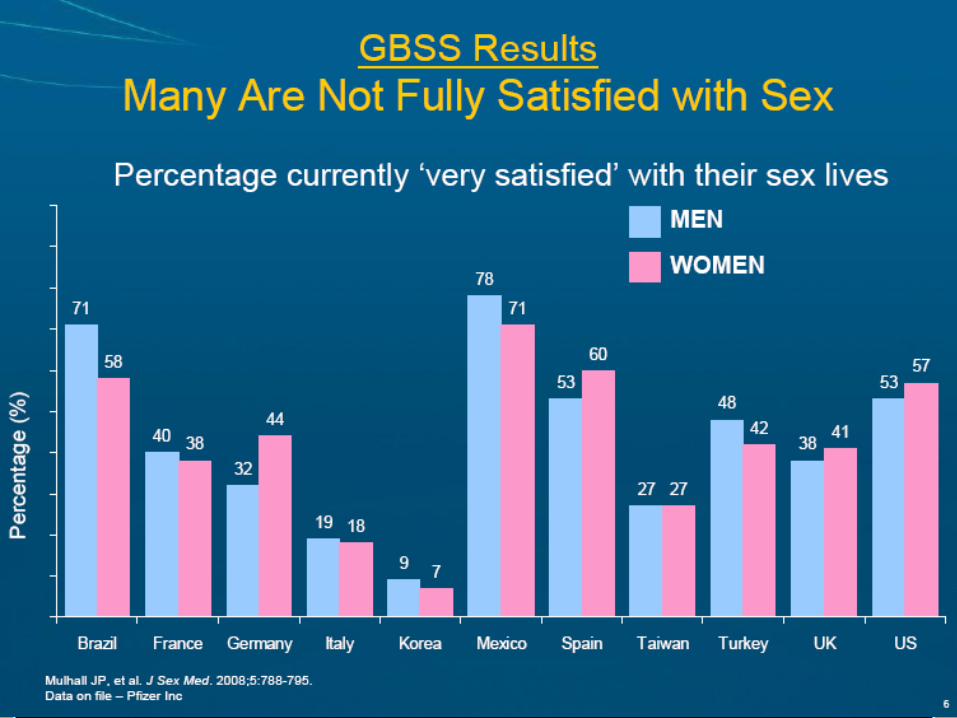
In 2005, There Was the GBSSIn 2005, There Was the GBSS
GBSS = Global Better Sex Survey
October 2005 – March 2006
Authoritative global survey focusing on sexual aspirations and unmet needs of men and women
12,563 sexually active adults, aged 25-74 years
27 countries, including Australia, Japan, South Korea, Hong Kong Singapore, Taiwan, Indonesia, Malaysia, Thailand
5Mulhall JP, et al. J Sex Med. 2008;5:788-795. Data on file – Pfizer Inc
The Next StepThe Next Step
GBSS
2005 2008
AP SHOWAP SHOW
Gather information on attitudes to sexual health, specifically for the Asia Pacific
• A diversity of cultural beliefs and practices
• Many people are uncomfortable talking about sexual health and many do not seek help
Help people understand the importance of sexual health to overall health and wellbeing
Encourage people to seek help for issues with sexual health
The erection hardness scale (EHS) is used
Asia Pacific Sexual Health and Overall Wellness (AP SHOW)
9
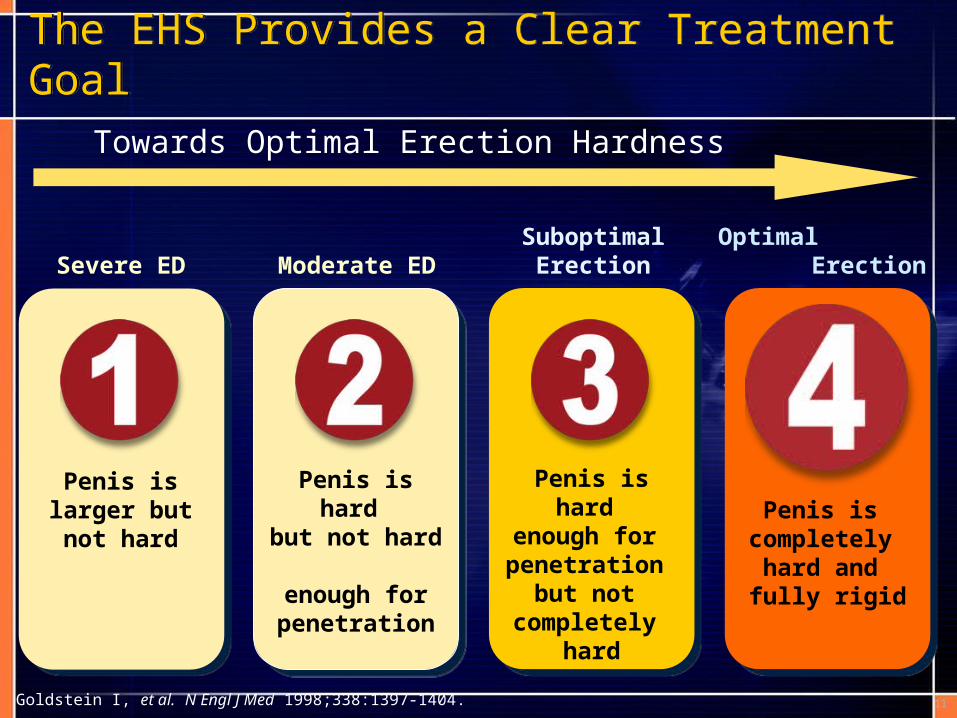
The EHS Provides a Clear Treatment Goal The EHS Provides a Clear Treatment Goal
Goldstein I, et al. N Engl J Med 1998;338:1397-1404.
Severe ED Moderate EDSuboptimal
ErectionOptimal
Erection
Penis is larger but not hard
Penis is hard but not hard enough for penetration
Penis is hard enough for penetration
but not completely
hard
Penis is completely hard and fully rigid
Towards Optimal Erection Hardness
11

Asia Pacific SHOWAsia Pacific SHOW
13 countries/regions
3,957 sexually active men (2,016) and women (1,941)
Face-to-face interviews (self-completed questionnaire) / online self-administered method
May to July 2008
The erection hardness scale (EHS) was used
12
COUNTRY
Australia
China
Hong Kong
India
Indonesia
Japan
South Korea
Malaysia
New Zealand
Philippines
Singapore
Taiwan
Thailand

Country Method Number Language
Australia Internet 209 English
China F-to-F* 600 Simplified Chinese
Hong Kong Internet 230 Traditional Chinese
India F-to-F* 400 English
Indonesia Internet 578 Bahasa Indonesia
Japan Internet 407 Japanese
S. Korea Internet 298 Korean
Malaysia Internet 202 Malay
New Zealand Internet 210 English
Philippines Internet 200 Tagalog/English
Singapore Internet 223 English
Taiwan Internet 200 Traditional Chinese
Thailand F-to-F* 200 Thai
Face-to-face or Internet Questionnaires
*subjects intercepted on street and handed a paper questionnaire to complete 13
150 males and 150 females
AP SHOW data : The Regional Results
AP SHOW data : The Regional Results
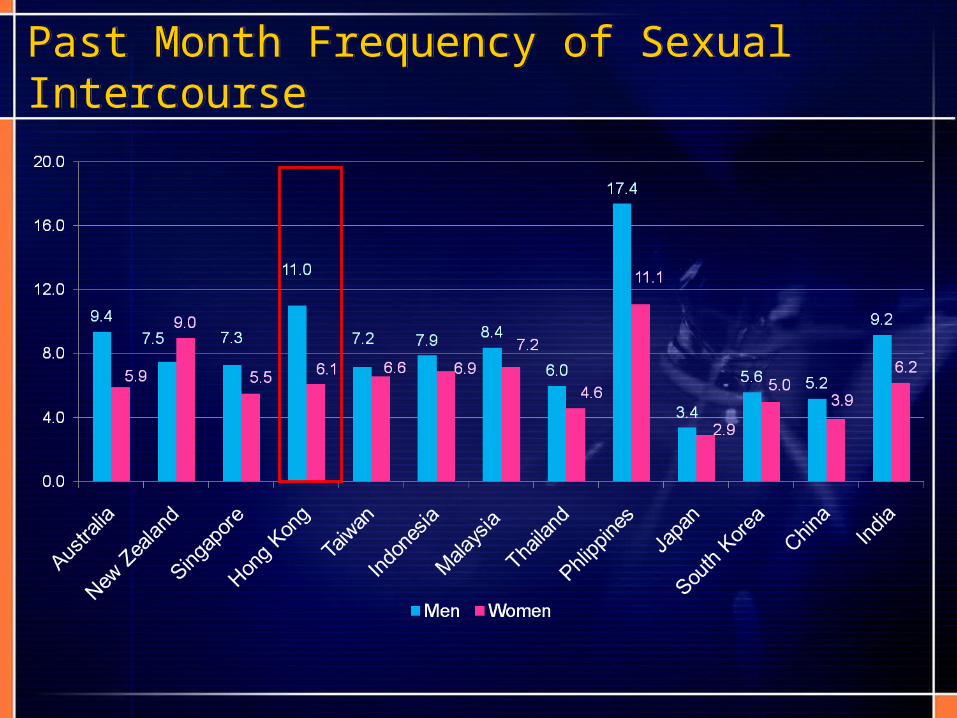
Past Month Frequency of Sexual Intercourse Past Month Frequency of Sexual Intercourse

Sex is very importantSex is very important
% of people who indicate sex as very important in their lives

People very satisfied with sexPeople very satisfied with sex
% of people are very satisfied with sex in their lives





AP SHOW : The Hong Kong Results
AP SHOW : The Hong Kong Results
AP SHOW – Key ResultsAP SHOW – Key Results
1) In Hong Kong, 66% of men and 69% of women are not very satisfied with sex.
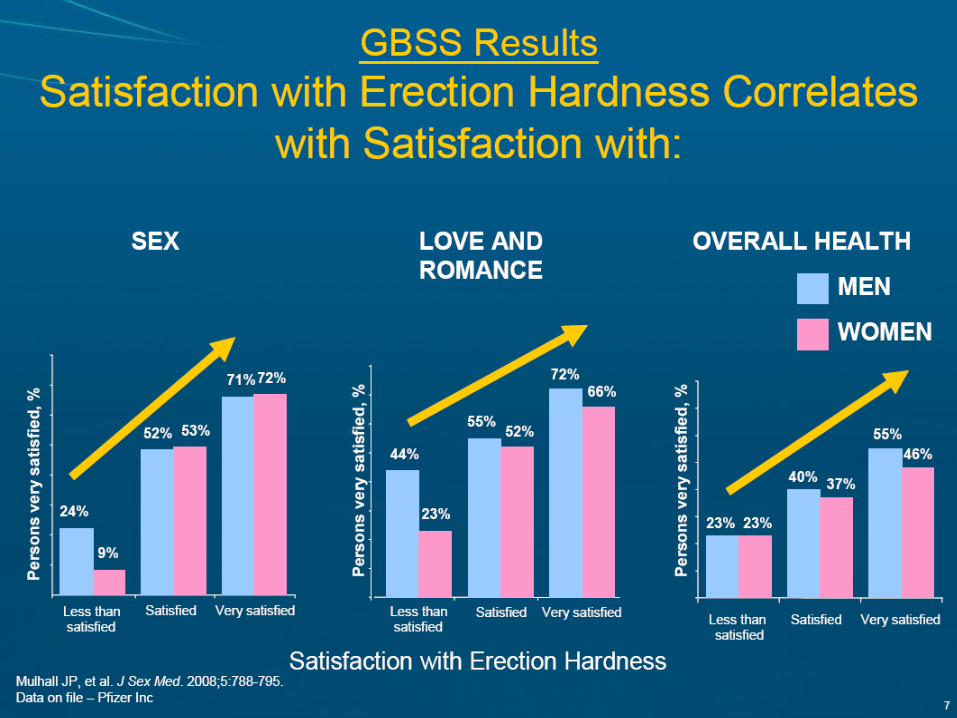
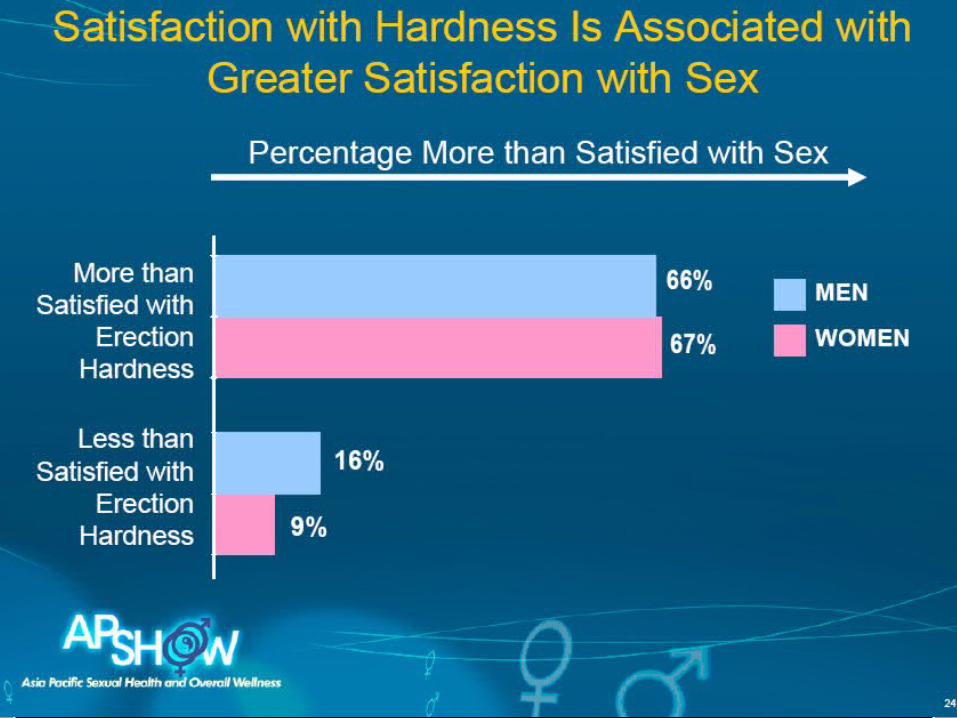
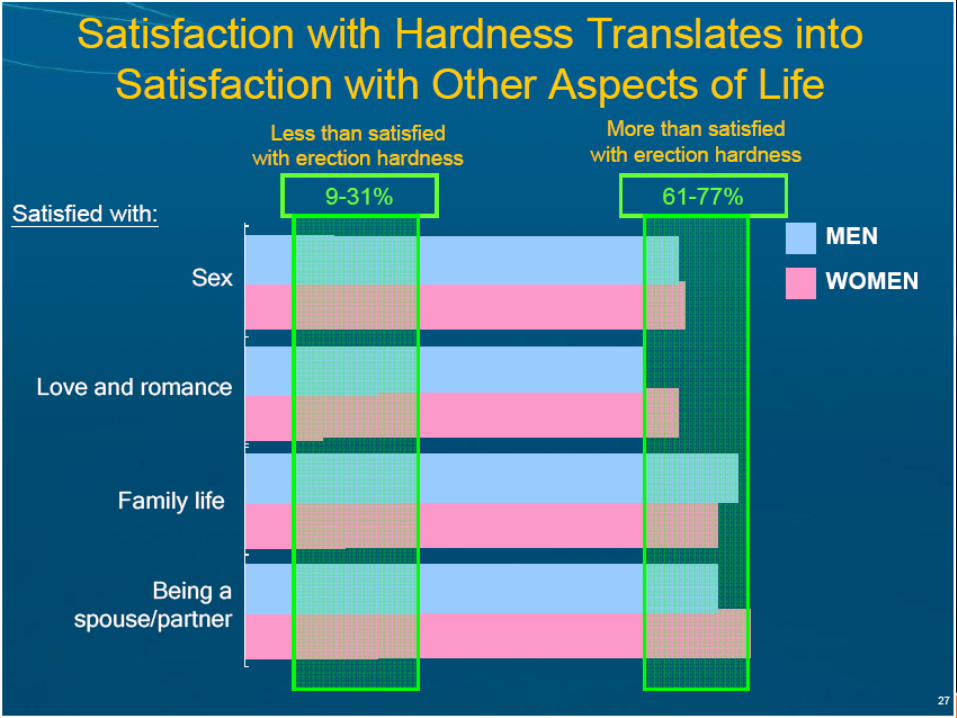
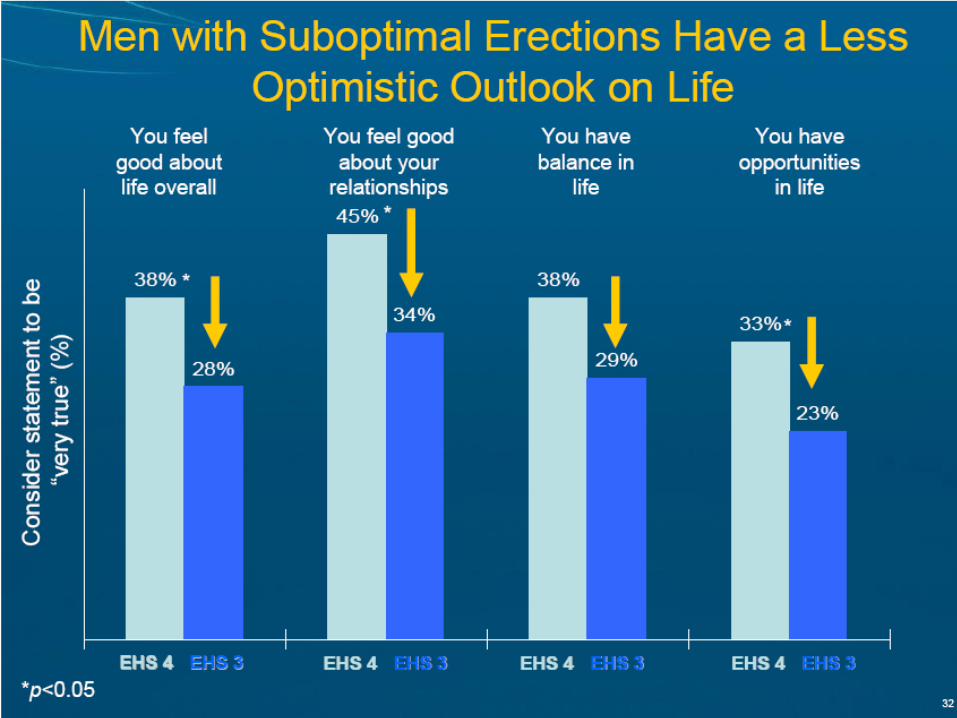
2) Greater satisfaction with sex is strongly associated with greater satisfaction with other aspects of life.
3) One in two men are not experiencing optimal erection hardness (EHS 4) during sexual activity. 60% of women report that their partners do not have optimal erection hardness (EHS 4) during sexual activity.
4) Men with and women whose partners have optimal erection hardness (EHS 4) are more satisfied with sex than men with and women whose partners have suboptimal erection hardness (EHS 3).
5) Men with suboptimal erection hardness (EHS 3) report they have less sex than they should, and are less satisfied with sex and other aspects of the sexual experience than men with optimal erection hardness (EHS 4).
15
In Hong Kong, 66% of men and 69% of women are not very satisfied with sex.
Greater satisfaction with sex is strongly associated with greater satisfaction with other
aspects of life.
16
1
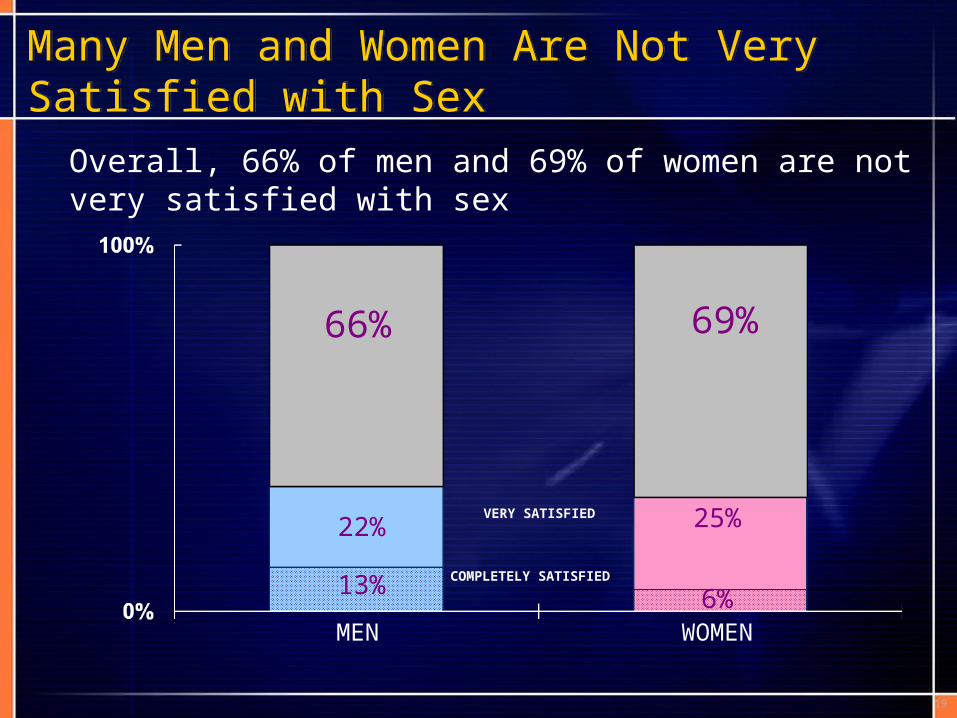
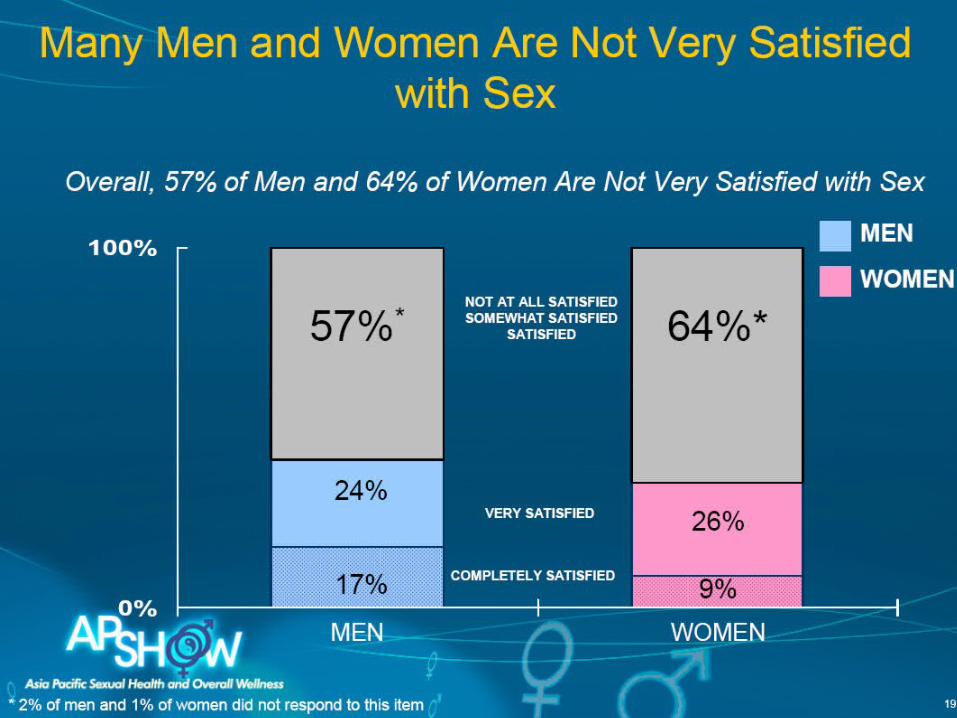
Many Men and Women Are Not Very Satisfied with SexMany Men and Women Are Not Very Satisfied with Sex
Overall, 66% of men and 69% of women are not very satisfied with sex
MEN WOMEN
66% 69%
COMPLETELY SATISFIED
VERY SATISFIED22%
13%
25%
6%
19

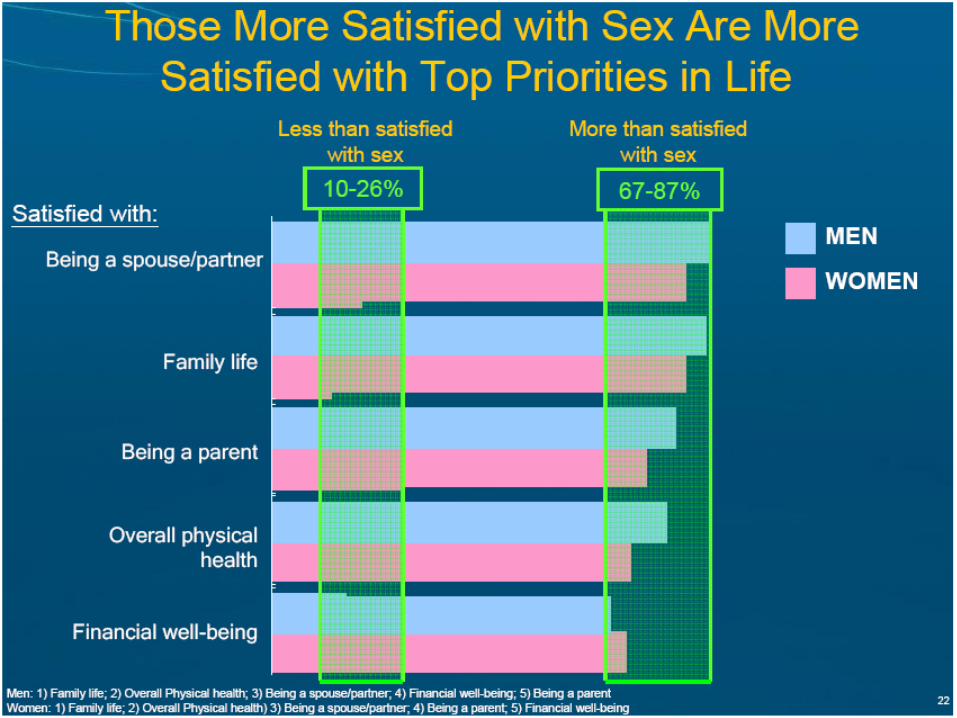
Those More Satisfied with Sex Are More Satisfied with Top Priorities in Life
Being a spouse/partner
Family life
Being a parent
Overall physical health
Financial well-being
Less than satisfied with sex
Satisfied with:
Men: 1) Being a spouse/partner; 2)Family life; 3) Overall Physical health; 4) Financial well-being ; 5) Being a parentWomen: 1) Overall Physical health; 2) Being a spouse/partner; 3) Family life and being a parent; 5) Financial well-being
21
60-93%
More than satisfied with sex
0-19%
MENWOMEN

One in two men are not experiencing optimal erection hardness (EHS 4) during sexual activity. 60% of women report that their partners do not have optimal erection
hardness (EHS 4) during sexual activity.
20
2
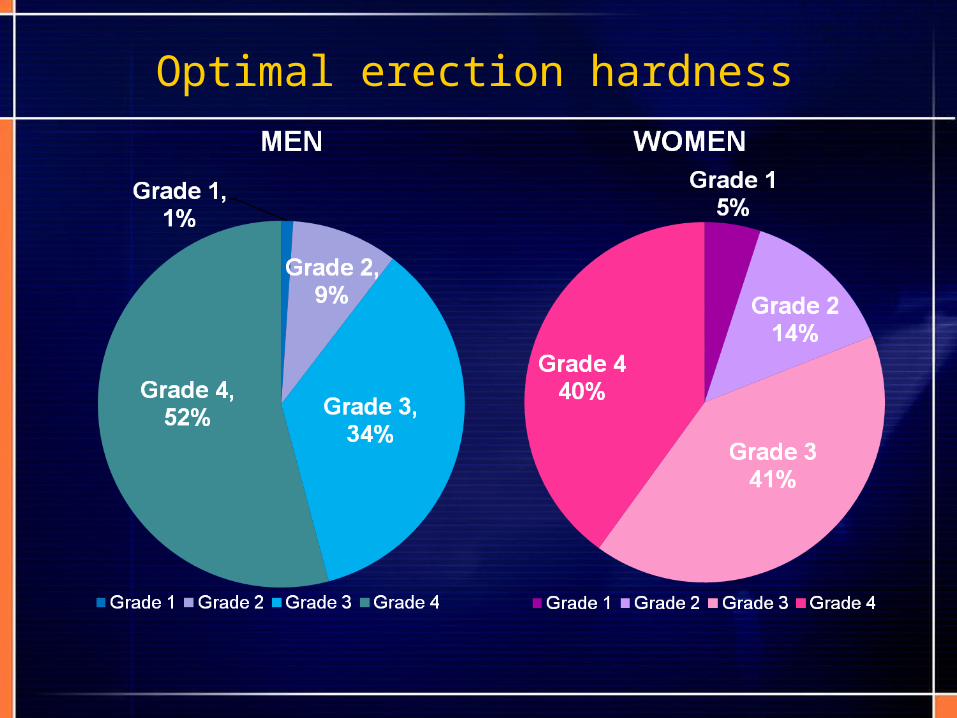
Optimal erection hardness

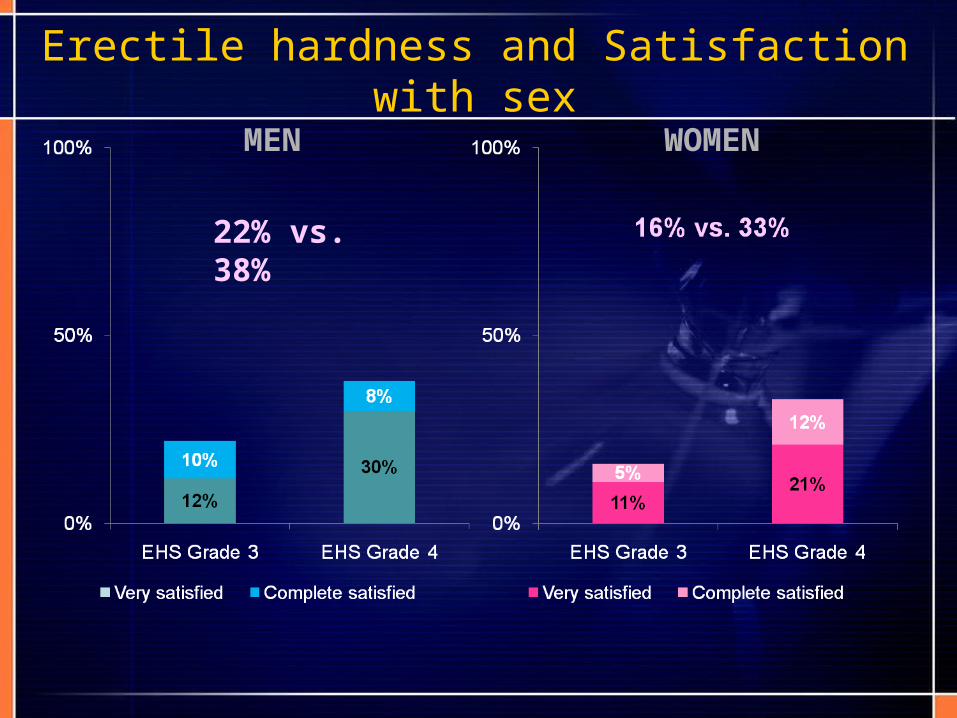
Men with and women whose partners have optimal erection hardness (EHS 4) are more satisfied with sex than men with and women
whose partners have suboptimal erection hardness (EHS 3)
22
3
MEN WOMEN
22% vs. 38%
Erectile hardness and Satisfaction with sex
Men with suboptimal erection hardness (EHS 3) report they have less sex than they should, and are less satisfied with sex and
other aspects of the sexual experience than men with optimal erection hardness (EHS 4)
25
4
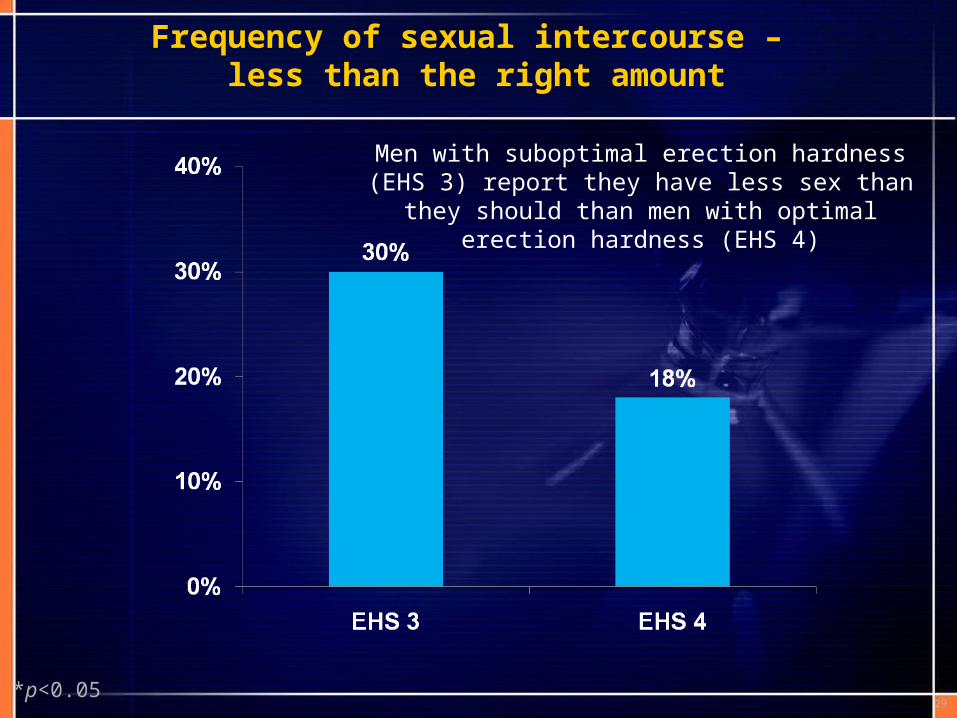
Frequency of sexual intercourse – less than the right amount
*p<0.0529
Men with suboptimal erection hardness (EHS 3) report they have less sex than they should than
men with optimal erection hardness (EHS 4)
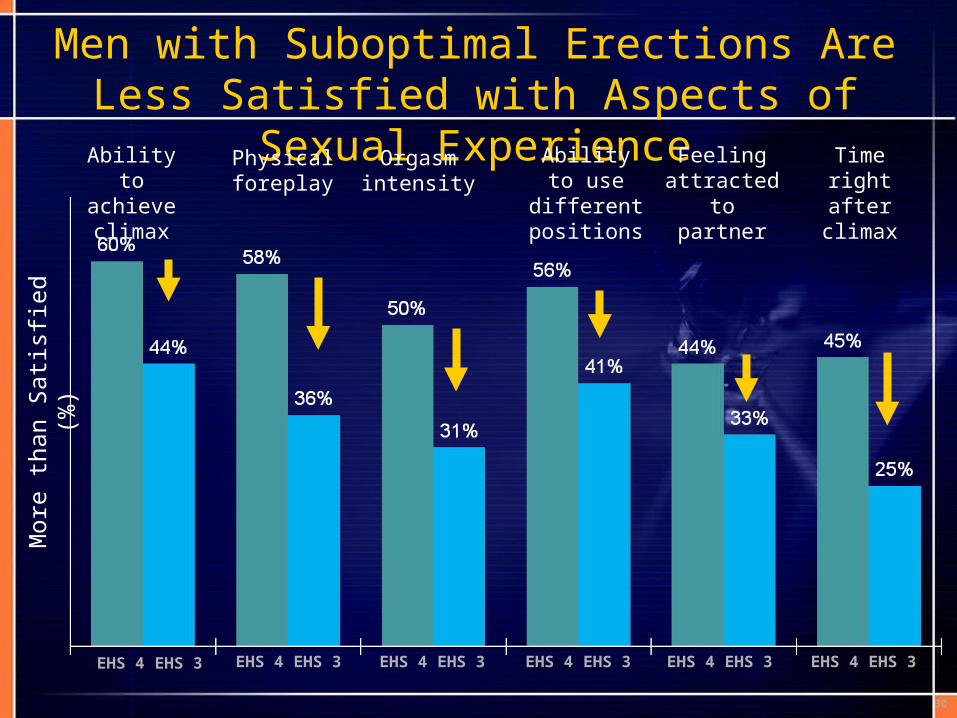
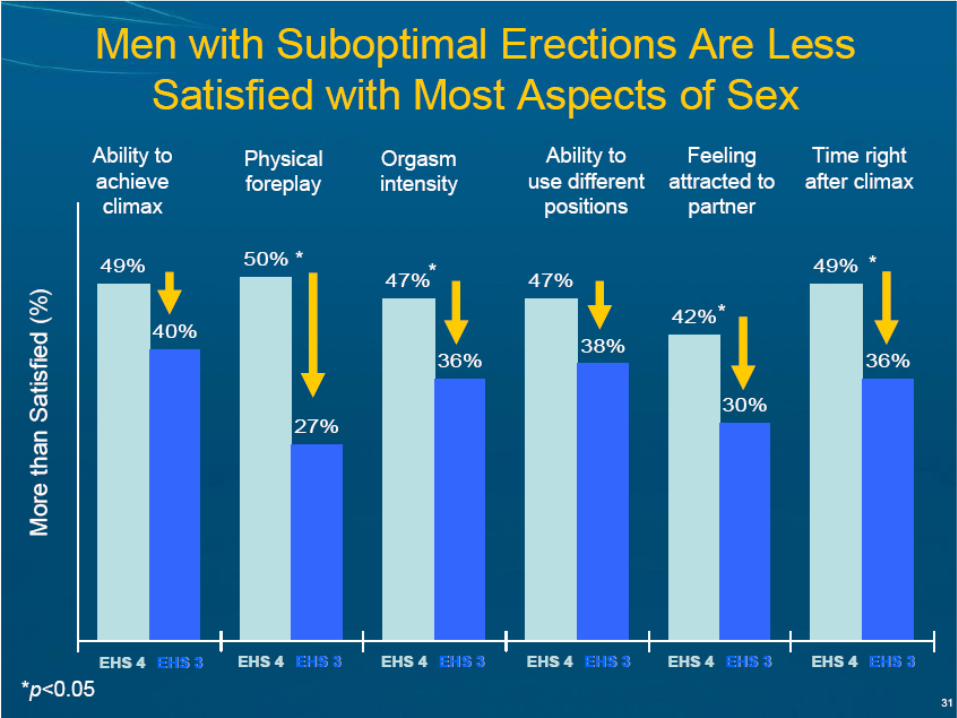
Men with Suboptimal Erections Are Less Satisfied with Aspects of Sexual Experience
Mor
e th
an S
atis
fied
(%)
Ability to achieve climax
Physical foreplay
Orgasm intensity
Feeling attracted to
partner
Ability to use different
positions
Time right after climax
EHS 4 EHS 3 EHS 4 EHS 3 EHS 4 EHS 3 EHS 4 EHS 3 EHS 4 EHS 3 EHS 4 EHS 3
30
AP show Hong Kong resultsAP show Hong Kong results
In Hong Kong, 66% of men and 69% of women are not very satisfied with sex.
Greater satisfaction with sex is strongly associated with greater satisfaction with other aspects of life.
48% men are not experiencing optimal erection hardness (EHS 4) during sexual activity. 60% of women report that their partners do not have optimal erection hardness (EHS 4) during sexual activity.
Men with and women whose partners have optimal erection hardness (EHS 4) are more satisfied with sex than men with and women whose partners have suboptimal erection hardness (EHS 3).
Men with suboptimal erection hardness (EHS 3) report they have less sex than they should, and are less satisfied with sex and other aspects of the sexual experience than men with optimal erection hardness (EHS 4).
ERECTILE DYSFUNCTION AND CARDIOVASCULAR DISEASESERECTILE DYSFUNCTION AND CARDIOVASCULAR DISEASES
Erectile Dysfunction = Endothelial DysfunctionErectile Dysfunction = Endothelial Dysfunction
DeBusk R et al. Am J Cardiol 2000 Jul 15;86(2):175–181.
1. Increasing age
2. Male
3. Hypertension
4. Diabetes mellitus
ED and cardiovascular disease share common risk factorsED and cardiovascular disease share common risk factors
5. Obesity
6. Cigarette smoking
7. Dyslipidemia
8. Sedentary lifestyle
ED and CVD often co-exist

There is now evidence that ED • is a risk factor for CAD
• may be the sentinel symptom of silent myocardial ischaemia
• is a potential predictor of subsequent cardiac events including death
ED and CADED and CAD
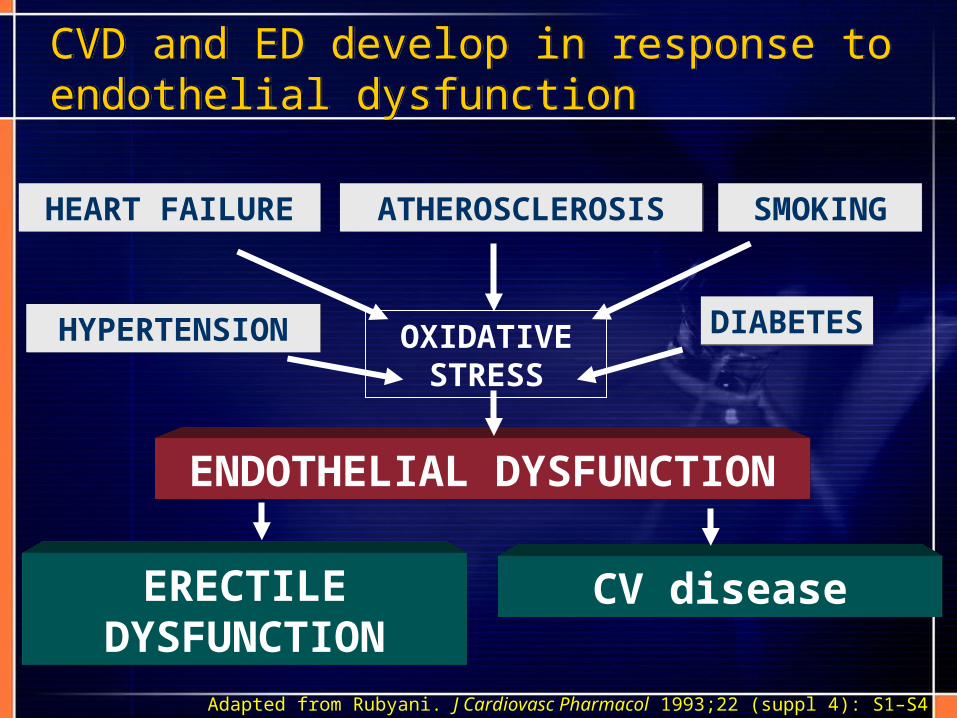
CVD and ED develop in response to endothelial dysfunctionCVD and ED develop in response to endothelial dysfunction
CV disease
ENDOTHELIAL DYSFUNCTION
OXIDATIVE STRESS
HYPERTENSIONHYPERTENSION
HEART FAILUREHEART FAILURE ATHEROSCLEROSISATHEROSCLEROSIS SMOKINGSMOKING
DIABETESDIABETES
Adapted from Rubyani. J Cardiovasc Pharmacol 1993;22 (suppl 4): S1–S4.
ERECTILE DYSFUNCTION
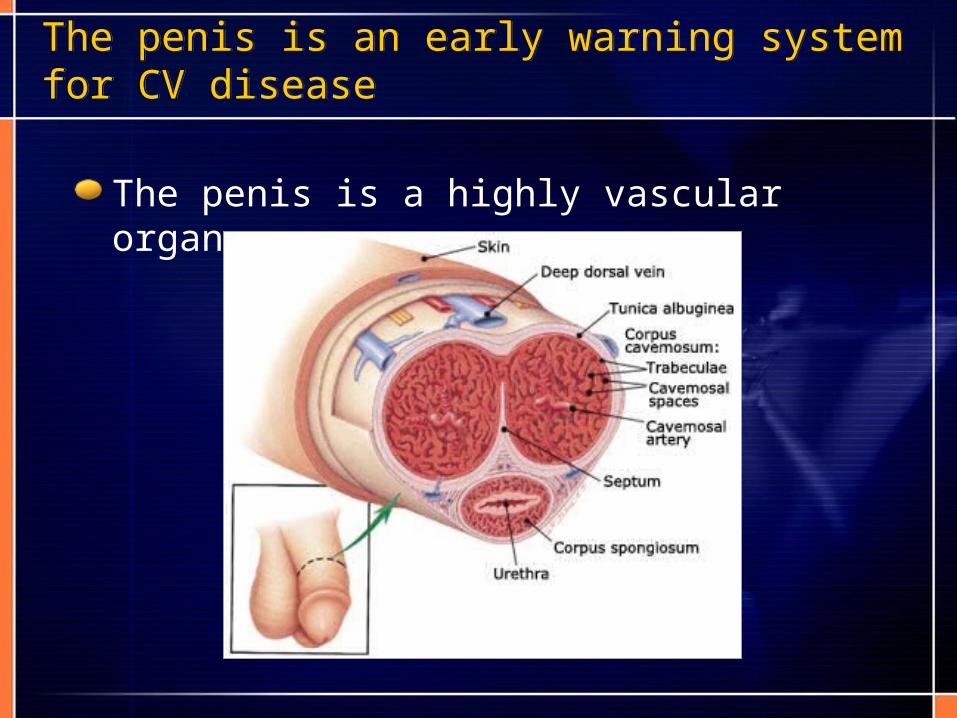
The penis is a highly vascular organ
The penis is an early warning system for CV diseaseThe penis is an early warning system for CV disease
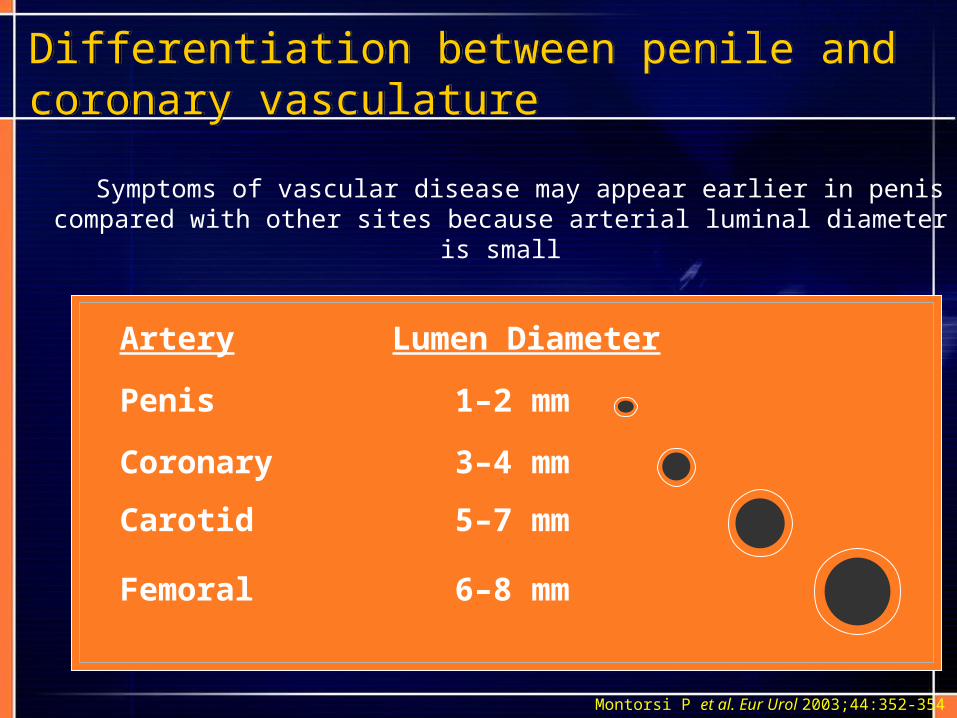
Symptoms of vascular disease may appear earlier in penis compared with other sites because arterial luminal diameter is small
Differentiation between penile and coronary vasculatureDifferentiation between penile and coronary vasculature
6–8 mmFemoral
5–7 mmCarotid
3–4 mmCoronary
1–2 mmPenis
Lumen DiameterArtery
Montorsi P et al. Eur Urol 2003;44:352-354
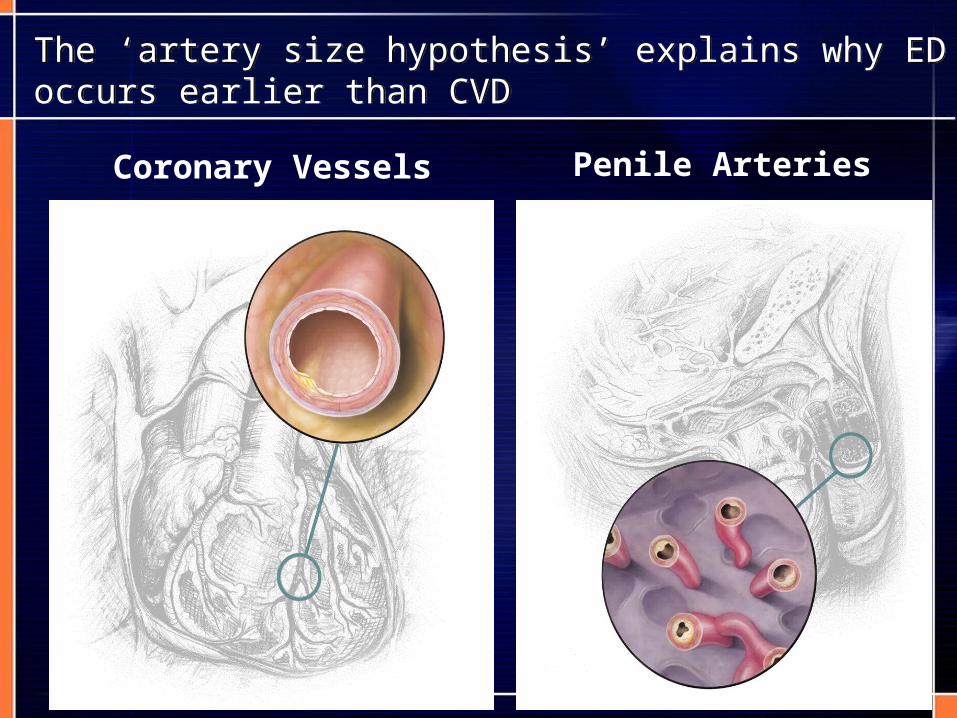
Coronary Vessels Penile Arteries
The ‘artery size hypothesis’ explains why ED occurs earlier than CVDThe ‘artery size hypothesis’ explains why ED occurs earlier than CVD
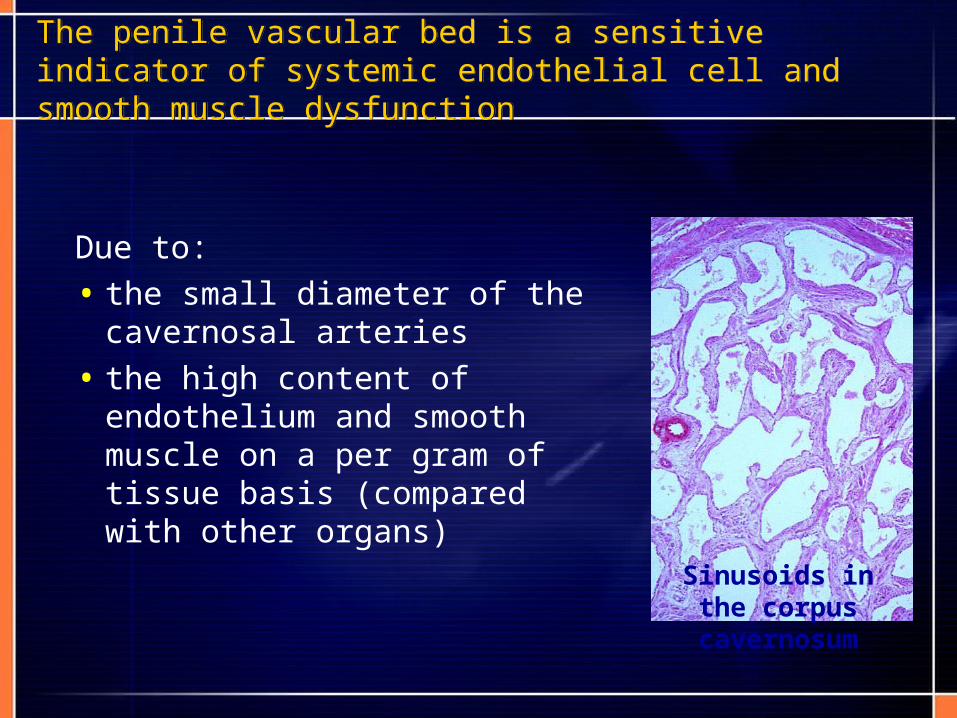
Due to:
• the small diameter of the cavernosal arteries
• the high content of endothelium and smooth muscle on a per gram of tissue basis (compared with other organs)
The penile vascular bed is a sensitive indicator of systemic endothelial cell and smooth muscle dysfunction The penile vascular bed is a sensitive indicator of systemic endothelial cell and smooth muscle dysfunction
Sinusoids in the corpus cavernosum
ED increases the risk of developing cardiovascular disease (CVD) by about 2 times the normal rate of incident CVD
The risk of CVD in men ages 40-60 with ED is greater than the risk of CVD in men older than 60
ED increases the risk of death from CVD by 50%
ED precedes the onset of CVD by about 2-5 years
ED is a potential predictor for cardiovascular disease as other common risk factors such as smoking, family history of CVD and dyslipidaemia
Take-Home MessagesTake-Home Messages