ER Case Presentation CSF

of 30
-
Upload
melinda-joy -
Category
Documents
-
view
221 -
download
0
Transcript of ER Case Presentation CSF
-
7/31/2019 ER Case Presentation CSF
1/30
CASE PRESENTATION
-
7/31/2019 ER Case Presentation CSF
2/30
CC: my head hurts and Im afraid
I have meningitis again.
HPI: 31yo c/o headache and neck pain for 3
days, getting progressively worse, similar toprevious episode of meningitis in the past.Pain is pounding, all over, 5/10 today, no
exacerbating or alleviating factors. Admits
to N/V x 1 today, denies fever, chills, rash,SOB, CP
-
7/31/2019 ER Case Presentation CSF
3/30
PMHx
1) HIV with AIDS as of 16 months ago
2) h/o hospitalization for cryptococcal meningitis x 23) Visual impairment and hearing loss 2/2 #1
4) h/o oral thrush
5) h/o herpes zoster Allergies: fish
PSHx
1) s/p appendectomy
2) h/o facial fractures
-
7/31/2019 ER Case Presentation CSF
4/30
FHx non-contributory
SocHx Tobacco: 1ppd x 20 years
EtOH: denies
Drug use: admits to h/o IV cocaine use for ~5 years inthe past, no current use
Medications, noncompliant with all ARV (type unknown)
Dapsone
Fluconazole
Bactrim
-
7/31/2019 ER Case Presentation CSF
5/30
ROS
General: adenopathy, fatigue, chills+ fever, +night sweats, +weakness
HEENT: recent trauma, recent change in vision,
discharge, photophobia, lacrimation,dysphagia, vertigo, +neck stiffness, +b/l vision
loss, can distinguish light and dark, +hearing loss
L ear, unchanged
CV: CP, DOE, PND
-
7/31/2019 ER Case Presentation CSF
6/30
ROS contd
Pulm:
SOB,
hemoptysis,
pleuritic CP GI/GU: +N/V, diarrhea, constipation,hematochezia, dysuria, urethral discharge
Neuro: +depression, +HA, seizure, syncope,
weakness
MSK: arthralgia, myalgia
-
7/31/2019 ER Case Presentation CSF
7/30
PE
VS: T 98.4 HR 72 RR 18 BP 117/67 98% on RA
Gen: cachectic with temporal wasting, NAD,cooperative
HEENT: +occipital tenderness, +mild nuchal rigidity(but negative Kernigs and Brudzinskis), b/l TMclear, PERRL, oropharynx is clear without erythema
or oral thrush, no lymphadenopathy CV: RRR, no murmurs
-
7/31/2019 ER Case Presentation CSF
8/30
PE contd
Pulm: CTAB, no wheezes, no rhales, no rhonchi
Abd: NTND, normoactive BS
Neuro: A+O x 3, intact strength and sensation in allextremeties
Ext: no edema, no deformity, no lesions
-
7/31/2019 ER Case Presentation CSF
9/30
Labs
CBC 11.3
4.1 202
33.7
BMP 135 105 28
3.0 24 1.19 128
APTT 43
PT 13.7
UA Color Yellow
Clarity ClearGlucose Neg
Bilirubin SmallKetones Trace
Spec. G >1.030pH 6.0protein 30
Nitrite Neg
Leuk Est Neg
-
7/31/2019 ER Case Presentation CSF
10/30
CSF Appearance clear colorless
Glucose 55
Protein 65RBCs 96
WBC 3
Segs (%) 0Lymphs(%) 100
Mono (%) 0
Eosinphl (%) 0
Fungal Smear Negative
Crypt. Ag Positive
VDRL Negative
Gram Stain no WBCs, organisms
-
7/31/2019 ER Case Presentation CSF
11/30
Lymphocyte panel:
%Mature T cells (CD3) 94 [57-85]
Absolute CD3 1501 [840-3060]%CD4 (Helper cells) 3 [30-61]
Absolute CD4 52 [490-740]
-
7/31/2019 ER Case Presentation CSF
12/30
Lymphocyte panel:
%Mature T cells (CD3) 94 [57-85]
Absolute CD3 1501 [840-3060]%CD4 (Helper cells) 3 [30-61]
Absolute CD4 52 [490-740]
-
7/31/2019 ER Case Presentation CSF
13/30
-
7/31/2019 ER Case Presentation CSF
14/30
Head CT: no evidence of acute intracranialpathology
Cervical CT: No fracture or dislocation
-
7/31/2019 ER Case Presentation CSF
15/30
DDX
Cryptococcal Meningitis
CNS toxoplasmosis
Lymphoma Progressive multifocal encephalopathy
Herpes simplex encephalitis
CMV Brain abscess
-
7/31/2019 ER Case Presentation CSF
16/30
CNS Complications in HIV
Occur in >40% HIV patients
Presenting feature of AIDS in 10-20% of cases
Types of complications
Directly or indirectly from HIV
AIDS dementia complex
Vacuolar myelopathy
Peripheral neuropathies
Immunodeficiency leading to infectious, autoimmune,or neoplastic processes
-
7/31/2019 ER Case Presentation CSF
17/30
CNS Complications in HIV
Occur in >40% HIV patients
Presenting feature of AIDS in 10-20% of cases
Types of complications
Directly or indirectly from HIV
AIDS dementia complex
Vacuolar myelopathy
Peripheral neuropathies
Immunodeficiency leading to infectious, autoimmune,or neoplastic processes
Opportunistic Infections occur when CD < 200
-
7/31/2019 ER Case Presentation CSF
18/30
Immune Reconstitution
Inflammatory Syndrome (IRIS)
Collection of inflammatory disordersassociated with paradoxical worsening of pre-existing infectious processes or unmasking ofsubclinical infections following HAARTinitiation in HIV patients
30-100 days after HAART initiation
-
7/31/2019 ER Case Presentation CSF
19/30
Cryptococcal meningitis
Cryptococcus neoformans encapsulated yeast found in soil andpigeon droppings
Spore inhalation pulmonaryinfection latency reactivationand dissemination
+/- visible lesions on head CT
-
7/31/2019 ER Case Presentation CSF
20/30
Cryptococcal meningitis
1 million cases worldwide, with 700,000deaths
2-7 cases per 1000 HIV-infected patients in
USA 89% occur as CNS manifestation
4th most common OI (PCP, CMV,
mycobacteria) 6-14% mortality
Relapse rate 30-50%
-
7/31/2019 ER Case Presentation CSF
21/30
Clinical Presentation
Headache (73-81%)
Fever (62-88%)
Malaise (38-76%) Nausea and vomiting
(8-42%)
Stiff neck (22-44%)
Visual disturbances (30%)
AMS with somnolence(18-28%)
Photophobia (19%)
Papilledema (10%)
Cranial neuropathies,
including nystagmus andamblyopia (6%)
-
7/31/2019 ER Case Presentation CSF
22/30
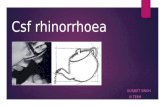
Neuroimaging
Cryptococcoma in medula
Cryptococcoma in basal ganglia
Bilateral visual loss due toarachnoiditis at level of optic
nerve or invasion of optic
nerve
-
7/31/2019 ER Case Presentation CSF
23/30
Diagnosis
Definitive diagnosis by CSF culture
Lumbar puncture with opening pressure
Neuroimaging first to r/o mass lesions, risk ofherniation
India Ink stain of CSF
Cryptococcal antigen test of CSF
93-100% sensitive; 93-98% specific
Serum testing if LP not feasible
-
7/31/2019 ER Case Presentation CSF
24/30
CSF analysis
May be normal in 25%, or minimally abnormal in 50%
identification by serology and India Ink are crucial
Normal Cryptococcus
Opening pressure 50200 mm H2O CSF Elevated >200mm H20 (may be
normal in 30%)
Color Colorless Clear
Turbidity Crystal clear Clear or viscous if numerous
cryptococci present
Mononuclear cells
-
7/31/2019 ER Case Presentation CSF
25/30
-
7/31/2019 ER Case Presentation CSF
26/30
-
7/31/2019 ER Case Presentation CSF
27/30
Treatment
Medical treatment: 3 phases
Induction
Consolidation
Maintenance
Manage ICP
-
7/31/2019 ER Case Presentation CSF
28/30
Elevated ICP
>200cm H20
Occurs in >50% cases
Mechanism?
Cytokine-induced inflammation increased vasulcarpermeability
Fungal antigen clogging arachnoid villi impairedresorption
Manage aggressively in symptomatic patients Daily LPs to reduce opening pressure to
-
7/31/2019 ER Case Presentation CSF
29/30
-
7/31/2019 ER Case Presentation CSF
30/30
References
Waxman SG. Chapter 24. Cerebrospinal Fluid Examination.In: Waxman SG, ed. Clinical Neuroanatomy. 26th ed. NewYork: McGraw-Hill; 2010.http://www.accessmedicine.com/content.aspx?aID=5275553. Accessed July 22, 2012.
NN Singh. CNS Cryptococcus in HIV. Medscape. UpdatedNovember 10, 2011.http://emedicine.medscape.com/article/1167389
Cox GM, Perfect JR. AIDS-associated cryptococcalmeningoencephalitis. In: UpToDate, Basow, DS (Ed),UpToDate, Waltham, MA, 2012.
Cox GM, Perfect JR. Microbiology and epidemiology ofcryptococcal infection. In: UpToDate, Basow, DS (Ed),UpToDate, Waltham, MA, 2012.