Equine performance products | Horse Care | Equine Health ...

EQUINE VETERINARY EDUCATION Equine uet. Educ. (2000) 12 (1) 35-44
35
Rtorial Article Chronic obstructive pulmonary disease: a review T. S. MAIRAND F. J. DERKSEN Bell Equine Veterinary Clinic, Mereworth, Maidstone, Kent ME18 5GS, UK and Department of Large Animal Clinical Sciences, Michigan State University, East Lansing, Michigan 48824, USA.
Introduction
Chronic obstructive pulmonary disease (COPD) is an inflammatory obstructive lower airway disease of the mature horse. It is a complex syndrome with variable clinical signs ranging from exercise intolerance in performance horses to chronic cough, mucopurulent or purulent nasal discharge, expiratory dyspnoea, and sometimes, weight loss in horses with severe disease.The term COPD was introduced by Sasse (1971) and is still the most commonly used name for the disease. The disease has also been known as heaves, broken wind, alveolar emphysema, chronic pulmonary disease, small airway disease, chronic obstructive lung disease, chronic bronchiolitis and recurrent airway obstruction.
A certain amount of confusion exists with regard to terminology of lower airway diseases in the horse. Inflammatory airway disease (IAD) is a term that has been introduced recently to describe a milder clinical syndrome observed in young horses, particularly racehorses in training (Moore 1996). At present it remains uncertain whether or not this milder inflammatory airway disease progresses to the more severe syndrome of COPD in the older horse. This article is restricted to a discussion of COPD in the mature horse.
Clinical signs of COPD are usually observed after exposure to hay and straw dust during stabling. Expiratory difficulty is caused by obstruction to airflow in both the large and the small airways. In the large airways this obstruction is caused primarily by bronchospasm, whereas in the small airways it is attributable mainly to inflammation and excessive secretions. The disease goes into remission when horses are pastured and not exposed to hay (unless they are also affected by summer pasture- associated obstructive pulmonary disease) (Derksen et al. 1985a). Although the exact pathogenesis of the disease is unclear, respiratory tract hypersensitivity to fungal and thermophilic actinomycete spores is believed to be involved. During periods of airway obstruction, affected horses demonstrate airway hyperresponsiveness (i.e. the airways show an abnormal tendency to narrow in response to a variety of stimuli), which wanes during periods of disease remission (Derksen et al. 1985a; Fairbairn 1993a).
Epizootology
COPD is a common respiratory tract disease of horses in temperate climates. It is a disease of the stabled horse and
is rare in climates where horses are kept outside all year round. The incidence of disease increases with age and it is uncommon in young horses. There is no particular breed or sex predisposition.
The prevalence of COPD varies around the world. It is reported to be most common in the northern hemisphere, where horses are fed hay that is produced during humid summer weather. In a survey of Swiss horses, the incidence of COPD was reported to be 54% (Bracher et al. 1991). The prevalence of COPD in the UK is unknown, although some clinicians believe that the incidence is increasing (Mair 1995).
Clinical signs
The clinical signs of COPD are extremely variable. In mild cases, there may be few or no overt clinical signs other than exercise intolerance. In severe cases, the horse may be debilitated and a respiratory cripple. In most cases the onset of disease is insidious, whereas in others the disease may appear suddenly following on from a viral respiratory infection, particularly influenza (Gerber 1973).
In mild cases, the horse may appear normal at rest, with a normal breathing pattern or slightly exaggerated end-expiratory effort. Such cases may demonstrate mild clinical signs of coughing and nasal discharge a t exercise, and there may be exercise intolerance in performance horses.
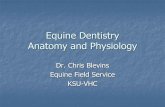
Horses with more severe COPD frequently demonstrate clinical signs at rest. These include a frequent, deep cough that is sometimes explosive and paroxysmal. A bilateral nasal discharge may be present (persistent or intermittent), and varies in nature from mucoid to mucopurulent to purulent (Fig 1). Obstruction of the small airways results in expiratory dyspnoea and increased expiratory effort. This causes a biphasic expiratory effort with the thoracic component of expiration followed by an abdominal component. This results in a ‘double expiratory effort’, which in long-standing and severe cases can cause hypertrophy of the abdominal musculature and the development of a ‘heave line’ (Gillespie and Tyler 1969; Cook 1976; McPherson et al. 1978; Littlejohn 1980). Horses with severe COPD may demonstrate marked exercise intolerance.
Clinical signs of COPD in individual horses vary. In many cases the severity of the clinical disease worsens with time unless prevented by treatment and management changes. The disease is usually worse when

36 Chronic obstructive pulmonary disease
Fig 1: Mild bilateral mucopurulent discharge typical of COPD.
horses are stabled, and improves if they are turned out to pasture. New batches of hay or straw may precipitate a worsening of the clinical signs, as may changes in the weather conditions.
Acute severe bouts of disease sometimes occur, resulting in severe dyspnoea and tachypnoea, with flaring of the nostrils (Fig 2), protrusion of the anus with each expiratory effort, an anxious facial expression, and paroxysmal coughing. Such acute exacerbations are often associated with sudden changes in management and environmental conditions.
Aetiology
Allergic responses to inhaled spores are the commonest cause of COPD. Acute exposure of an asymptomatic COPD sufferer to an environment containing mouldy feed and bedding will induce clinical signs of COPD (forced abdominal breathing, coughing and flared nostrils) (Derksen et al. 1985a; McGorum et al. 1993a). Over 50 species of moulds have been identified in stable air, with the primary source being hay and straw. Dust generated from mouldy hay and straw is a mixture of many different potential allergens (Webster et al. 1987; Clarke and Madelin 1987; Woods et al. 1993). Specific inhalation challenges of affected horses have suggested Aspergillus fumigatus, Faenia rectivirgula (formerly known as Micropolyspora faenia) and Thermoactinomyces vulgaris as potentially important allergens (McPherson et al. 1979; Derksen et al. 1988; McGorum et al. 1993a).
Other mould species are almost certainly involved in some cases and, less commonly, there may be involvement of other agents such as pollen. Heated hays and straws are very dusty, and the composition of the dust is primarily thermophilic fungal and actinomycete spores (Clarke and Madelin 1987). Many of these spores are aerodynamically small enough to reach and deposit in the bronchioles when breathed in by a horse.
The most critical factor in determining the
Fig 2: Flaring of the nostrils at rest associated with marked dyspnoea in a pony affected by an acute exacerbation of COPD.
microbial development of hay and straw is the water content at baling. Baling at 15 to 20% water content is associated with little heating. However, baling at 20 to 30% may result in heating and moderate mould contamination. Baling at 35 to 50% water content leads to spontaneous heating to 50 to 60°C and heavy mould contamination. Such contamination may result in respirable challenges of up to lo6 fungal and actinomycete spores per breath as the horse eats mouldy hay from a hay net (Clarke and Madelin 1987).
Since hay is the point source of offending spores, the concentration of these antigens is much higher near the hay than in the rest of the horse’s environment. The airspace around the horse’s nose is called the breathing zone. The characteristic feeding behaviour of the horse, such as shaking and eating hay for long periods, results in dust concentrations in the breathing zone that are very much higher than in the rest of the stable (Woods et al. 1993). This information has therapeutic implications, as it suggests that improving stable ventilation is less important than removing the point source of dust (hay) when treating horses with COPD.
McGorum and colleagues (1993a) and Fairbairn et al. (1993b) studied the effects of natural challenge (stabling and feeding poor quality hay) and challenge with Aspergillus fumigatus, Faenia rectivirgula and Thermoactinomyces vulgaris in control and COPD- affected horses. Within a few hours, natural challenge induced lung dysfunction in the COPD cases; hypoxaemia occurred by 5 h and there were increased numbers of neutrophils in bronchoalveolar lavage fluid

T. S. Mair and F. J. Derksen 37
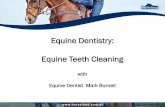
Fig 4: Histological section of lung stained with H&E from a pony affected by COPD. A bronchiole is shown demonstrating chronic bronchiolitis with epithelial hyperplasia and mucus plugging the airway lumen. A dense cuff ofpredominantly mononuclear cells is present in the peribronchiolar tissue.
Fig 3: Emphysematous change involving both apical lobes and the periphery of the diaphragmatic lung lobes in a long-standing case of COPD.
(BALF). Natural challenge had no effect on control horses. In COPD cases, Aspergillus fumigatus and Faenia rectivirgula challenge induced BALF neutrophilia, although this was less severe than that induced by.natura1 challenge and was unaccompanied by changes in lung function. These studies indicate that COPD is a pulmonary hypersensitivity t o specific antigens in hay and straw dust.
The precise immunological mechanisms associated with fungal and actinomycete spore deposition in the distal airways have not been elucidated, and probably vary from case to case. o p e s 1 (immediate), 3 (Arthus) and 4 (delayed) hypersensitivity reactions have been implicated. Inhaled spores and their metabolites that deposit on the mucosa of the small airways might also initiate inflammation by primary irritant effects. Inhaled endotoxin may also play a role in inducing airway inflammation, either directly, following inhalation of high concentrations, or indirectly by potentiating the effects of allergen inhalation (McGorum et al. 1998).
Further evidence for an immune-mediated basis of COPD is supported by studies of pulmonary lymphocyte populations (McGorum et al. 1993b), and immunoglobulin and specific antibody levels in respiratory tract secretions (Mair et al. 1988; Halliwell et al. 1993). Skin testing and measurements of serum precipitins have also been studied as a means of assessing immune mechanisms and identifylng antigens involved in COPD.
However, positive skin tests and serum precipitins to fungal and thermophilic actinomycete antigens are found
Fig 5: Dacheal aspirate stained with Giemsa from a horse with COPD showing a neutrophil influx and alveolar macrophages (one of which has phagocytosed some neutrophils).
in many normal as well as COPD-affected horses, and they probably reflect level of exposure of the horse rather than susceptibility to COPD (Eyre 1972; Halliwell et al. 1979; Beech and Merryman 1986; Madelin et al. 1991; Evans et al. 1992; McGorum et al. 1993~).
COPD is sometimes reported to develop after a preceding viral respiratory infection (Gerber 1973). This predisposition to the development of COPD following viral infections may be caused by increased antigen uptake across the damaged epithelial surfaces of the respiratory tract, altered immune responses induced by virus, and increased retention of particulate antigens due to damage to the mucociliary clearance mechanisms. Prevention of COPD by reducing airborne dust levels is an important consideration in the management of horses with viral infections.

38 Chronic obstructive pulmonary disease
Pathology
The severity of pathological changes in COPD is variable between cases, and is also variable between different regions of the lung in individual cases (Thurlbeck and Lowell 1964; Breeze 1979; Schoon and Deegen 1983; Vie1 1983; Winder and von Fellenberg 1986,1988).
In many cases of COPD, the lungs appear grossly normal, and gross destructive changes of emphysema only develop following long-term uncontrolled disease (Fig 3). Histology commonly shows bronchiolar epithelial cell hyperplasia, peribronchial infiltration by neutrophils, lymphocytes and plasma cells, and inflammatory cell accumulation in the airway lumen. Chronic bronchiolitis, sometimes with alveolar overinflation, is the most consistent histological abnormality in COPD (Fig 4). Epithelial cells in small airways often show changes, including loss of granulation of Clara cells, goblet cell metaplasia, and intraepithelial lamellar inclusion bodies.
In the peripheral lung tissues, some cases show alveolar fibrosis, necrosis of type I alveolar epithelial cells and replacement by type II alveolar epithelium (Kaup et al. 1990). Pores of Kohn are increased in number (Gillespie and Tyler 1967a; Kaup et al. 1990). Electron microscopy of areas of emphysema found in some horses shows loss of capillaries, more pores of Kohn, increased numbers of osmophilic inclusions, and more collagen in alveolar septa (Gillespie and Tyler 1967a,b).
Pathophysiology
Horses affected by COPD generally have an increased airway resistance and decreased dynamic compliance, and a prolongation of nitrogen washout (Gillespie et al. 1966; Muylle and Oyaert 1973; Willoughby and McDonnelll979; McPherson et al. 1978; Thomson and McPherson 1984; Derksen et al. 1985a; Armstrong et al. 1986; Broadstone et al. 1988). All of these changes are compatible with diffuse airway obstruction. The exacerbated regional differences in small airway resistance and lung compliance result in an uneven distribution of ventilation. The resulting inequalities in ventilatiodperfusion ratio may in turn cause hypoxaemia (Nyman et al. 1991). The increase in total pulmonary resistance and the impaired gas exchange decrease the exercise tolerance of affected horses.
Diffise airway obstruction of COPD is caused primarily by airway smooth muscle contraction. Evidence for this is the immediate bronchodilation (within 5-15 min) observed after aerosol administration of bronchodilators (Derksen et al. 1992, 1996). Airway obstruction remaining after bronchodilation is likely due to plugging of airways with mucus and exudate, and hyperplasia of airway epithelium.
Pathogenesis The pathogenesis of COPD has recently been reviewed (Robinson et al. 1996). Exposure of COPD-susceptible horses to hay and straw dust initiates inflammation in the
lower airways, and this plays a major role in the pathogenesis of the disease. Following natural challenge, neutrophils accumulate in the lungs between 3 and 5 h (Fairbairn et al. 1993b) and appear in BALF within 5 h (McGorum et al. 1993a). Neutrophils may be attracted into the lungs by either non specific or specific mechanisms. Nonspecific mechanisms, such as direct chemotactic activity of dust particles and activation of the alternate complement pathway, might account for the mild increase in BALF neutrophils that occurs in some normal horses and ponies exposed to dusty environments (Derksen et al. 1985b; Tremblay et al. 1993). In COPD-affected horses, specific immune responses to inhaled antigens probably result in cytokine production by alveolar macrophages and lymphocytes, which subsequently results in a neutrophil influx.
The role of inflammatory mediators in the pathogenesis of COPD is uncertain. Activation of the arachidonic acid cascade in COPD horses has been shown in several studies (Gray et al. 1989, 1992a,b,c; Watson et al. 1990, 1992). The balance between production of inflammatory and inhibitory prostanoids may play an important role in the pathogenesis of COPD, but further research is required in this area to elucidate the precise role of individual mediators in the disease. Recently, Marr and colleagues (1998) demonstrated in horses that leukotriene D4 (LTD41, but not LTB4, caused a dose-dependent airway obstruction. The potency of LTD4 was several hundred times that of methacholine. LTB4 induced neutrophil recruitment to the lung, suggesting that these mediators could contribute to the pathogenesis of COPD. The exact role of leukotrienes in this disease is still to be determined.
As long ago as 1885, Gresswell and Gresswell referred to broken wind as a ‘nervous inflammatory disease’. It is now clear that there is an intimate interaction between the inflammatory response and the nervous system that regulates smooth muscle tone, mucus secretion, and the cough reflex. Therefore, several studies of neural mechanisms in horses with COPD have shown potentially important roles of the parasympathetic, sympathetic and nonadrenergic noncholinergic nervous systems (Broadstone et al. 1991; LeBlanc et al. 1991; Yu et al. 1994a,b). The importance of these neural mechanisms in the disease has been reviewed (Robinson et al. 1996; Robinson 1999). These studies have made it clear that several inflammatory mediators can facilitate parasympathetically mediated bronchospasm, and studies by Olszewski et al. (1997, 1999) suggest that mast cell-derived rather than neutrophil-derived products are most important in this regard.
Diagnosis In many cases, COPD can be diagnosed on the basis of the history, clinical features and response to therapy. However, in mild cases there may be few overt clinical signs and the physical examination may be unremarkable. In these cases, the use of further diagnostic tests, such as endoscopic examination, respiratory cytology and lung function tests may be

T. S. Mair and F. J. Derksen 39
necessary to achieve a diagnosis. Abnormalities of lung sounds detected by
auscultation are frequently present in horses demonstrating overt clinical signs of respiratory disease. The ability to detect adventitious sounds may be enhanced by the use of a rebreathing bag. Abnormally harsh bronchial sounds, wheezing and crackling sounds may be heard alone or in combination. In severe cases, adventitious wheezing and crackling sounds may be audible to the naked ear at the nostrils. Airflow at the nostrils during during expiration will be biphasic. Fluid rattling sounds and referred pulmonary sounds may be heard over the cervical trachea, and the laryngeal cough reflex is often abnormally sensitive. Thoracic percussion is thought by some clinicians to be helpful to detect overinflation of the lungs, but it is likely that this will only be detected in advanced or severe cases.
Pulmonary function testing, including arterial blood gas analysis and measurement of intrapleural pressure, can be helpful to quantify the degree of pulmonary dysfunction, and to monitor the progress of the case. Horses with overt clinical signs of COPD frequently demonstrate a maximum change of intrathoracic pressure during breathing of greater than 6 mmHg, and a partial arterial oxygen pressure of less than 82 mmHg (McPherson et al. 1978). However, these tests are too insensitive to be helpful in low grade and subclinical COPD. Other physiological abnormalities in COPD include decreased dynamic compliance, increased pulmonary resistance, and prolongation of nitrogen washouts. These tests of pulmonary function require specialised equipment that is not generally available in practice, and may not be sensitive enough to detect low grade disease. Tidal breathing flow-volume loops have been investigated as a more sensitive physiological test to detect small airway obstruction (Petsche et al. 1994). A completely noninvasive measurement of lung function, using forced oscillatory mechanics, has also been recommended recently as a useful practical diagnostic aid for small airway disease (Hoffman 1999a).
Nuclear scintigraphy has had relatively limited value in the clinical investigation of COPD to date. The techniques and interpretation of pulmonary scintigraphic scans are discussed by Votion and Lekeux (1999). Lung perfusion and ventilation scans may show abnormalities in clinical COPD. Small airway obstruction results in patchy lung perfusion images; and ventilation scans may show a concentration of aerosol deposition in the larger airways as well as patchy reduction in the lung periphery. Whether nuclear imaging is useful in detecting abnormalities in early and low grade disease has yet to be determined. Radiographic abnormalities are inconsistent and usually only identifiable in severe, long-standing cases. Radiography is of little or no value in mild COPD.
High numbers of neutrophils and increased quantities of mucus in tracheal aspirates are typical of COPD (Fig 5). Spiral casts of inspissated mucus from the bronchioles (Curschmann’s spirals) are often present. The cytological characteristics of tracheal aspirates,
especially the number of neutrophils, are quite variable in normal horses (possibly reflecting the degree and type of environmental pollutants), and tracheal aspirate cytology need not necessarily reflect the nature of the cell population in the small airways and alveoli. Despite these limitations, tracheal aspirate cytology can be a useful screening test to identify airway inflammation (Whitwell and Greet 1984; Mair 1987).
Bronchoalveolar lavage (BAL) provides a more sensitive way of assessing inflammation in the small airways. The technique of BAL is described by Hoffman (1999b). The numbers of neutrophils in BALF is less variable than tracheal aspirates, and evaluation of BALF cytology may be more helpful than tracheal aspirate cytology. In some horses with COPD, BALF cytology will also show increased numbers of eosinophils andor mast cells. BALF neutrophilia subsides when affected horses are in clinical remission (Derksen et al. 198513).
Treatment and control
Treatment of COPD is purely palliative; there is no cure. The prognosis for an individual horse depends on the severity and chronicity of the disease, the ability to control the environment or eliminate the specific allergens, the types and dosages of medications required, and the work expected from the horse (Robinson 1997).
Environmental control
The most important component of treatment is environmental control to reduce exposure of the horse to the aeroallergens and other airborne pollutants that precipitate the disease. Airway hyperresponsiveness, which is a feature of the clinical disease, means that airborne environmental pollutants (e.g. inert dusts, ammonia, etc.) need to be controlled in addition to the specific allergens to which the horse is hypersensitive. Environmental control is the most effective method of alleviating the clinical signs of COPD and of achieving long-term control, but it may be the most difficult treatment in terms of obtaining owner compliance.
The optimal management of most COPD cases is to keep the horse totally at pasture with no access to hay or straw. If affected horses must be stabled, a bedding material other than straw (e.g. shredded paper, wood shavings, rubber mats or peat moss) should be used. Eliminating hay from the diet appears to be the most important aspect of environmental control (Vandenput et al. 1998). An alternative to dry hay should be fed, such as a cubed diet, vacuum-packed hay, or silage. In mild cases, soaking the hay prior to feeding may be sufficient. The ventilation of the box must be able to provide 8 to 10 air changes per hour. If possible, stalls adjacent to the one used by the affected horse should be similarly managed. The horse should be housed away from areas where hay and straw are used, and away from any manurdmuck heaps.
Medical treatment of COPD (Table 1) is indicated in horses demonstrating moderate or severe clinical signs.

40 Chronic obstructive pulmonary disease
TABLE 1: Medical treatments for COPD ~~ ~
Anticholinergic bronchodilators Atropine sulphate 0.02 pgkg bwt i.v. once only Glycopyrrolate Ipratropium bromide
2.2 pgkg bwt i.v. once or twice (8 h interval) 2-3 pgkg bwt by aerosol every 4-6 h
Sympathomimetic bronchodilators
Phosphodiesterase inhibitors
Corticosteroids
Clenbuterol
Pirbuterol Albuterol
0.8 pgkg bwt per 0s or i.v. twice a day (increase to 1.6 pgkg bwt and subsequently to 3.2 pgkg bwt twice a day if necessary) 1 or 2 pgkg bwt by aerosol 1 or 2 pgkg bwt by aerosol
Aminophylline
Prednisolone
Dexamethasone Beclomethasone diproprionate
4.5-6.5 mgkg bwtper 0s 3 times a day
1 or 2 mgkg bwt per 0s alternate mornings. Reduce dose after 2-3 weeks 0.04 mgkg bwt i.v. twice a day. Reduce dose after 2 or 3 days 1320 pg by aerosol twice a day
Mast cell stabilisers
Mucolytics
Disodium cromoglycate
Bromhexine hydrochloride Dembrexine
80 mg by aerosol once a day
0.1-0.3 mgkg bwtper 0s or i.v. once a day 0.3 mgkg bwtper 0s twice a day
In milder cases, environmental control alone may be sufficient. Medications that are most useful include bronchodilators and corticosteroids. Other drugs that are sometimes helpful include mucolytics and expectorants.
Bronchodilators
Specific bronchodilators that can be used include three groups of drugs: anticholinergics (such as atropine), sympathomimetics (P-adrenergic agonists) (such as clenbuterol), and phosphodiesterase inhibitors (methylxanthines such as aminophylline). In other species, bronchodilators are most effective when delivered by aerosol because this achieves a high concentration of the drug at the intended site (i.e. the small airways) with less problems of systemic side effects. A detailed discussion of inhalation therapy of equine respiratory disorders is given by Duvivier et al. (1999). Hypoxaemia is a possible complication of bronchodilator therapy caused by ventilation-perfusion mismatching; this is unlikely to be an important clinical problem in COPD but may be an important consideration in the treatment of some other pulmonary diseases, especially in foals.
Anticholinergic agents
Atropine is an effective bronchodilator which acts by blocking vagally induced bronchospasm (Broadstone et al. 1988). The effects of a single dose of atropine persists for up to 12 h, but side effects include decreased mucociliary clearance, tachycardia, mydriasis, ileus and excitement (especially in ponies). Despite these side effects, atropine can be useful in acute exacerbations of COPD where there is severe bronchospasm. Glycopyrrolate administered i.v. once or twice at an interval of 8 hours can be used as an alternative to atropine. Ipratropium bromide is an anticholinergic agent that can be administered by aerosol.
It can provide effective bronchodilation in horses with COPD for 4 to 6 h, with few or no systemic side effects and no effect on mucociliary clearance (Robinson et al. 1993).
Sympathomimetic agents
Sympathomimetic agents cause bronchodilation by stimulation of p2-receptors in the large and small airways. P2-receptors are also found in vascular beds and the uterus. PBreceptor specificity is not complete, and large doses of P2-receptor agonists can cause side effects such as trembling, excitement, sweating, ileus, colic and tachycardia by virtue of inadvertent stimulation of pl-receptors (Derksen et al. 1992). The P2-adrenergic compounds include clenbuterol, terbutaline, pirbuterol and albuterol.
Clenbuterol is a specific P2-agonist that is well absorbed when given orally, and has a relatively long half- life. It also stimulates mucociliary clearance. Twice a day oral or i.v. administration maintains blood levels in a therapeutic range. The standard dose of 0.8 pgkg bwt is not effective in all horses, and a graded treatment schedule is recommended. If the horse fails to demonstrate a clinical response after 2 or 3 days at the dose of 0.8 pgkg bwt, this can be increased to 1.6 pgkg bwt. If the horse fails to respond to this new dosage, it may be increased again to 3.2 pgkg bwt.
Horses should not begin their treatment with clenbuterol at these higher dose rates because they are likely to suffer side effects of sweating, trembling, tachycardia and excitement. A gradual, stepwise increase in dose rate should therefore be adopted.
An oral dose rate for terbutaline has not been established in the horse, and potential side effects (sweating, tremors and excitement) may limit its usefulness. Although oral albuterol is commonly used in clinical practice, there are no data in the literature to show

T. S. Mair and F. J. Derksen 41
efficacy at any dose. Indeed, a recent report demonstrated no detectable blood levels of albuterol following oral administration at a dose of 50 and 250 pgkg bwt (Ball 1998). This suggests that oral albuterol may be poorly absorbed and may not be efficacious in the horse.
Several P-agonists have been administered by nebulisation or dry powder inhalation. Pirbuterol and albuterol a t doses of 1 to 2 pgkg bwt cause effective bronchodilation, but the duration of action is only approximately 1 h (Derksen et al. 1992, 1996).
Phosphodiesterase inhibitors
The phosphodiesterase inhibitors, such as caffeine, theobromine and theophylline, promote bronchodilation by inhibiting the breakdown of intracellular CAMP in airway smooth muscle. Theophylline (or its soluble salt aminophylline) is the most commonly used bronchodilator in this group. It is an effective bronchodilator in horses when blood concentrations reach 10 pg/ml; however, excitement occurs when levels reach 15 pg/ml (McKiernan et al. 1990). Thus therapeutic and toxic levels are close to each other, and this, coupled with its erratic absorption from the gastrointestinal tract, means that the drug is difficult to use effectively in a clinical setting.
Corticosteroids
Corticosteroids are effective at reducing airway inflammation in COPD. However, the inflammation will return on cessation of therapy unless exposure to the offending allergens is reduced. Corticosteroids are potent anti-inflammatory agents with many actions.
Corticosteroids:
Decrease the number of circulating lymphocytes Inhibit the production of cytokines such as IL-2
0 Decrease production of eicosanoids and expression of leucocyte adhesion factors
0 Attenuate IgE-dependent histamine release.
Corticosteroids also increase P-receptor numbers and activity (Barnes and Pedersen 1993; Barnes 1996). Potential side effects of corticosteroids include immunosuppression, Cushings-like signs and laminitis. Laminitis is probably the commonest side effect of corticosteroid therapy seen in practice, however immunosuppression and bacterial infections, including pneumonia, occur occasionally. To reduce the risk of side effects, oral administration of prednisolone on an alternate day regime is advised. An initial dose of 1 to 2 mgkg bwt per 0s is administered every other morning. After 2 weeks therapy, response to treatment should be assessed and the dose rate should be dropped until the minimum effective dose is reached. The horse should eventually be weaned off the corticosteroid completely if possible.
In a recent study, the efficacy of prednisone in the treatment of COPD was questioned (Robinson et al.
1998). In this study, prednisone at a daily oral dose rate of 0.45 mgkg bwt failed to enhance disease recovery in response to removal of hay and straw from the horse’s environment.
In severe cases and horses with acute exacerbations of disease, dexamethasone therapy may be necessary, but this drug carries a greater risk of undesirable side effects. An initial dose of i.v. dexamethasone (0.04 mgkg bwt) may be administered b.i.d. for 2 to 3 days, followed by a reducing dose rate over the next 7 to 10 days (depending on the clinical response) (Seahorn and Beadle 1998).
Inhaled corticosteroid therapy has become an important form of treatment for human asthma, and this form of therapy will probably prove beneficial in the therapy of COPD in the horse. However, to date, inhalational therapy with corticosteroids has been insufficiently studied. Aerosol administration of beclomethasone b.i.d. has recently been shown to improve respiratory function in horses with COPD (Amman et al. 1998; Rush et al. 1998).
Disodium cromoglycate
Disodium cromoglycate is a mast cell-stabilising agent that has been shown to be an effective prophylactic treatment of COPD in some horses. The drug is administered by nebulisation. In one study, it was demonstrated that a single dose of the drug prevents the onset of clinical signs of disease for up to 3.6 days, whereas 4 successive daily treatments will prevent clinical disease for up to 24.3 days (Thomson and McPherson 1981). However, a subsequent study failed to show this activity (Soma et al. 1987). The drug is particularly useful in cases where unavoidable exposure to dusts may occur, for example when an affected horse is to be travelled to a show.
In clinical practice, disodium cromoglycate appears to work better in some cases of COPD than in others, which may relate to differences in the aetiopathogenesis between individual cases.
Mucolytics
In cases where there are excessive quantities of tenaceous mucus in the lower airways, mucolytics and expectorants may be helpful, along with bronchodilators, to decrease airway resistance. Acetylcysteine, dembrexine and bromhexine have been used for this purpose. However, there are no reports in the literature showing efficacy of mucolytics in equine airway disease.
Immunotherapy
Immunotherapy to produce hyposensitisation to the offending allergens may be helpful in some cases of COPD (Beech and Merryman 1986). However, difficulties associated with the identification of the relevant allergens and the presence of multiple allergies in individual horses limit the effectiveness of this treatment. There have been no well-controlled clinical studies to assess the efficacy of this form of therapy.

42 Chronic obstructive pulmonary disease
Antimicrobial drugs
Secondary lower airway bacterial infection may complicate COPD in some rare cases, producing additional signs of fever, purulent nasal discharge, anorexia, neutrophilia and hyperfibrinogenaemia. Streptococcus zooepidemicus is a common isolate in these patients, and procaine penicillin i.m. (22000 idkg bwt once or twice a day) o r oral trimethoprim-sulphadiazine (15 mgkg bwt b.i.d.1 is generally an effective treatment (Seahorn and Beadle 1998).
References
Amman, V.J., Vrins, A.A. and Lavoie, J.-P. (1998) Effects of inhaled beclomethasone diproprionate on respiratory function in horses with chronic obstructive pulmonary disease (COPD). Equine uet. J . 30, 152-157.
Armstrong, P.J., Derksen, F.J., Robinson, N.E. and Slocombe, R.F. (1986) Airway responses to aerosolized methacholine and citric acid in ponies with recurrent airway obstruction (heaves). Am. Rev. resp. Dis. 133,357-361.
Ball, M.A. (1998) Pharmacokinetics of orally administered albuterol in the horse. In: Proceedings of World Equine Airway Symposium, Guelph, Canada. p 5.
Barnes, P.J. (1996) Mechanisms of corticosteroids in asthma. Am. J . Respir. Care Med. 154, 521-527.
Barnes, P.J. and Pedersen, S. (1993) Efficacy and safety of inhaled corticosteroids in asthma. Am. Rev. respir. Dis. 148,51-526.
Beech, J. and Merryman, G.S. (1986) Immunotherapy for equine respiratory disease. Equine vet. Sci. 6, 6-10.
Bracher, V., von Fellenberg, R., Winder, C.N., Gruenig, G. and Hermann, M. (1991) An investigation of the incidence of chronic obstructive pulmonary disease (COPD) in random populations of Swiss horses. Equine uet. J . 23, 136-141.
Breeze, R.G. (1979) The problem of disease definition. Vet. Clin. N . Am.: Large Anim. Pract. 1, 219-230.
Broadstone, R.V., LeBlanc, P.H., Derksen, F.J. and Robinson, N.E. (1991) Zn vitro responses of airway smooth muscle from horses with recurrent airway obstruction. Pulm. Pharmacol. 4,191-202.
Broadstone, R.V., Scott, J.S., Derksen, F.J. and Robinson, N.E. (1988) Effects of atropine in ponies with recurrent airway obstruction. J. appl. Physiol. 65, 272-275.
Clarke, A.F. and Madelin, T. (1987) Technique for assessing respiratory health hazards from hay and other source materials. Equine vet. J . 19,442-447.
Cook, W.R. (1976) Chronic bronchitis and alveolar emphysema in the horse. Vet. Rec. 99, 448-451.
Derksen, F.J., Robinson, N.E. and Berney, C. (1992) Aerosol pirbuterol: bronchodilator activity and side effects in ponies with recurrent airway obstruction (heaves). Equine vet. J . 24,
Derksen, F.J., Robinson, N.E., Scott, J.S. and Stick, J.A. (1988) Aerosolized Micropolyspora faeni antigen as a cause of pulmonary dysfunction in ponies with recurrent airway obstruction (heaves). Am. J . uet. Res. 49, 933-938.
Derksen, F.J., Robinson, N.E., Armstrong, P.J., Stick, J.A. and Slocombe, R.F. (1985a) Airway reactivity in ponies with recurrent airway obstruction (heaves). J . appl. Physiol. 58,
107-112.
598-604.
Derksen, F.J., Scott, J.S., Miller, D.C., Slocombe, R.F. and Robinson,
N.E. (198513) Broncho-alveolar lavage in ponies with recurrent airway obstruction (heaves). Am. Rev. resp. Dis. 132, 1066-1070.
Derksen, F.J., Olszewski, M., Robinson, N.E., Berney, C., Lloyd, J.W., Hakala, J., Matson, C. and Ruth, D. (1996) Use of a hand-held, metered dose aerosol delivery device to administer pirbuterol acetate to horses with heaves. Equine vet. J . 28,
Duvivier, D.H., Votion, D., Roberts, C.A., Art, T. and Lekeux, P. (1999) Inhalation therapy of equine respiratory disorders. Equine vet. Educ. 11, 124-130.
Evans, A.G., Paradis, M.R. and OCallaghan, M. (1992) Intradermal testing of horses with chronic obstructive pulmonary disease and recurrent urticaria. Am. J. vet. Res. 53,203-208.
Eyre, P. (1972) Equine pulmonary emphysema: a bronchopulmonary mould allergy. Vet. Rec. 91, 134-140.
Fairbairn, S.M., Lees, P. and Page, C.P. (1993a) Duration of antigen-induced hyperresponsiveness in horses with allergic respiratory disease and possible links with early airway obstruction. J . vet. Pharmacol. Therap. 16,469-476.
Fairbairn, S.M., Page, C.P., Lees, P. and Cunningham, F.M. (199313) Early neutrophil but not eosinophil or platelet recruitment to the lungs of allergic horses following antigen exposure. Clin. Exp. Allergy 23, 821-828.
Gerber, H. (1973) Chronic pulmonary disease in the horse. Equine vet. J . 5,26-32.
Gillespie, J.R. and Tyler, W.S. (1967a) Quantitative electron microscopy of the interalveolar septa of the horse lung. Am. Rev. resp. Dis. 95, 477-483.
Gillespie, J.R. and Tyler, W.S. (196713) Capillary and cellular changes in alveolar walls of emphysematous horse lung: a quantitative electron microscope study. Am. Rev. resp. Dis. 95,
Gillespie, J.R. and Tyler, W.S. (1969) Chronic alveolar emphysema in the horse. Adv. vet. Sci. 13, 59-99.
Gillespie, J.R., Tyler, W.S. and Eberly, V.E. (1966) Pulmonary ventilation and resistance in emphysematous and control horses. J . appl. Physiol. 21,416-422.
Gray, P.R., Derksen, F.J., Robinson, N.E., Carpenter-Reyo, L.J., Johnson, H.G. and Roth, R.A. (1989) The role of cyclooxygenase products in the acute airway obstruction and airway hyperreactivity of ponies with heaves. Am. Reu. resp. Dis. 140,154-160.
Gray, P.R., Derksen, F.J., Broadstone, R.V., Robinson, N.E., Johnson, H.G. and Olson, N.C. (1992a) Increased pulmonary production of immunoreactive 15-hydroxyeicosatetraenoic acid in an animal model of asthma. Am. Rev. resp. Dis. 145, 1092-1097.
Gray, P.R., Derksen, F.J., Robinson, N.E., Slocombe, R.F. and Peters-Golden, M.L. (199210) Epithelial strips: an alternative technique for examining arachidonate metabolism in equine tracheal epithelium. Am. J . resp. Cell mol. Biol. 6, 29-36.
Gray, P.R., Derksen, F.J., Broadstone, R.V., Robinson, N.E. and Peters-Golden, M. ( 1 9 9 2 ~ ) Decreased airway mucosal prostaglandin E2 production during airway obstruction in an animal model of asthma. Am. Rev. resp. Dis. 146,586-591.
Gresswell, J.B. and Gresswell, A. (1885) A Manual of the Theory and Practice of Equine Medicine. Bailliere, Tindall and Cox, London. pp 164-172.
Halliwell, R.E.W., McGorum, B.C., Irving, P. and Dixon, P.M. (1993) Local and systemic antibody production in horses affected with chronic obstructive pulmonary disease. Vet. Immunol. Zmmunopathol. 38,201-215.
Halliwell, R.E.W., Fleischman, J.B., Mackay-Smith, M., Beech, J.
306-310.
484-490.

T. S. Mair and F. 3. Derksen 43
and Gunson, D.E. (1979) The role of allergy in chronic pulmonary disease of horses. J . Am. vet. med. Ass. 174,277-281.
Hoffman, A.M. (1999a) A programme of lung function testing for horses suspected with small airway disease. Equine vet. Educ.
Hoffman, A.M. (1999b) Bronchoalveolar lavage technique and cytological diagnosis of small airway inflammatory disease. Equine vet. Educ. ll, 330-336.
Kaup, F.-J., Drommer, W., Damsch, S. and Deegen, E. (1990) Ultrastructural findings in horses with chronic obstructive pulmonary disease (COPD) 11: pathomorphological changes of the terminal airways and the alveolar region. Equine vet. J . 22, 349-355.
LeBlanc, P., Broadstone, R.V., Derksen, F.J. and Robinson, N.E. (1991) In vitro responses of distal airways in horses with heaves. Am. J . vet. Res. 52, 999-1003.
Littlejohn, A. (1980) Studies on the pathophysiology of chronic obstructive pulmonary disease in horses. I. Clinical signs. Onderst. J . vet. Res. 47, 159-162.
Madelin, T.M., Clarke, A.F. and Mair, T.S. (1991) Prevalence of serum precipitating antibodies in horses to fungal and thermophilic actinomycete antigens: effects of environmental challenge. Equine vet. J . 23, 247-252.
Mair, T.S. (1987) Value of tracheal aspirates in the diagnosis of chronic pulmonary diseases in the horse. Equine uet. J . 19,
Mair, T.S. (1995) Changing concepts of COPD. Equine vet. J . 27,
Mair, T.S., Stokes, C.R. and Bourne, F.J. (1988) Increased local IgA production in chronic obstructive pulmonary disease. Equine uet. J . 20, 214-216.
Marr, K.A., Lees, P., Page, C.P. and Cunningham, F.M. (1998) Inhaled leukotrienes cause bronchoconstriction and neutrophil accumulation in horses. Res. Vet. Sci. 64, 219-224.
McGorum, B.C., Dixon, P.M. and Halliwell, R.E.W. (1993a) Responses of horses affected with chronic obstructive pulmonary disease to inhalation challenges with mould antigens. Equine vet. J . 25, 261-267.
McGorum, B.C., Dixon, P.M. and Halliwell, R.E.W. (199313) Phenotypic analysis of peripheral blood and bronchoalveolar lavage fluid lymphocytes in control and chronic obstructive pulmonary disease affected horses, before and after natural (hay and straw) challenges. Vet. Immunol. Immunopathol. 36,
McGorum, Dixon, P.M. and Halliwell, R.E.W. (1993~) Evaluation of intradermal mould antigen testing in the diagnosis of equine chronic obstructive pulmonary disease. Equine vet. J .
McGorum, B.C., Ellison, J and Cullen, R.T. (1998) Total and respirable airborne dust endotoxin concentrations in three equine management systems Equine vet. J . 30, 430-434.
McPherson, E.A., Lawson, G.H.K., Murphy, J.R., Nicholson, J.M., Breeze, R.G. and Pirie, H.M. (1979) Chronic obstructive pulmonary disease (COPD) in horses: aetiological studies: responses to intradermal and inhalation antigenic challenge. Equine vet. J . ll, 159-166.
McPherson, E.A., Lawson, G.H.K., Murphy, J.R., Nicholson, J.M., Fraser, J.A., Breeze, R.G. and Pine, H.M. (1978) Chronic obstructive pulmonary disease (COPD): identification of affected horses. Equine vet. J . 10,47-53.
McKiernan, B.C., Koritz, G.D., Scott, J.S., Berney, C. and Robinson, N.E. (1990) Plasma theophylline concentration and
11, 322-328.
463-465.
402-403.
207-222.
25, 273-275.
lung function in ponies with recurrent obstructive lung disease. Equine vet. J . 22, 194-197.
Moore, B.R. (1996) Lower respiratory tract disease. Vet. Clin. N . Am.: Equine Pract. 12,457-477.
Muylle, E. and Oyaert, W. (1973) Lung function tests in obstructive pulmonary disease in horses. Equine vet. J . 5,37-44.
Nynian, G., Lindberg, R., Wechner, D., Bjork, M., Kvart, C., Persson, S.G.B., Gustafsson, H. and Hedenstierna, G. (1991) Pulmonary gas exchange correlated to clinical signs and lung pathology in horses with chronic bronchiolitis. Equine vet. J . 23,253-260.
Olszewski, M.A., Robinson, N.E. and Derksen, F.J. (1997) In vitro responses of equine small airways and lung parenchyma. Resp. Physiol. 109, 167-176.
Olszewski, M.A., Robinson, N.E., Zhu, F.-X., Zhang, X.-Y. and Tithof, P.K. (1999) Mediators of anaphylaxis but not activated neutrophils augment cholinergic responses of equine small airways. Am. J . Physiol. 276, L522-L529.
Petsche, V.M., Derksen, F.J. and Robinson, N.E. (1994) Tidal breathing flow-volume loops in horses with recurrent airway obstruction (heaves). Am. J . vet. Res. 55, 885-891.
Robinson, N.E. (1997) Pathogenesis and management of airway disease. Proc. Am. Ass. equine Pract. pp 106-115.
Robinson, N.E. (1999) Lower airway obstruction, heaves or broken wind. In: Guardians of the Horse: Past, Present and Future, Romney Publications/British Equine Veterinary Association, Newmarket, Suffolk. pp 183-187.
Robinson, N.E., Derksen, F.J., Berney, C. and Goossens, L. (1993) The airway response of horses with recurrent airway obstruction (heaves) to aerosol administration of ipratropium bromide. Equine vet. J . 25, 299-303.
Robinson, N.E., Jackson, C., Berney, C. and Derksen, F.J. (1998) Interactions of environment and prednisone in the treatment of heaves. In: Proceedings of the World Equine Airway Symposium, Guelph, Canada. p 6.
Robinson, N.E., Derksen, F.J., Olszewski, M.A. and Buechner- Maxwell, V.A. (1996) The pathogenesis of chronic obstructive pulmonary disease of horses. Br. vet. J . 152,283-306.
Rush, B.R., Raub, E.S., Rhoads, W.S., Flaminio, M.J.B.F., Matson, C.J., Hakala, J.E. and Gillespie, J.R. (1998) Pulmonary function in horses with recurrent airway obstruction after aerosol and parenteral administration of beclomethasone dipropionate and dexamethasone, respectively. Am. J . vet. Res. 59,1039-1043.
Sasse, H.H.L (1971) Some Pulmonary Function Tests in Horses: a n Aid to Early Diagnosis of Chronic Obstructive Pulmonary Disease (heaves) in Horses. PhD Thesis, University of Utrecht.
Schoon, H.-A. and Deegen, E. (1983) Histopathologie der chronisch obstruktiven bronchitis bei klinisch manifest erkrankten Pferden. Tier. Praxis ll,213-221.
Seahorn, T.L. and Beadle, R.E. (1998) How I treat .... chronic obstructive pulmonary disease. Comp. cont. Educ. pract. Vet.
Soma, L.R., Beech, J. and Gerber, N.H. (1987) Effects of cromolyn in horses with chronic obstructive pulmonary disease. Vet. Res. Commun. 11, 339-351.
Thomson, J.R. and McPherson, E.A. (1981) Prophylactic effects of sodium cromoglycate on chronic obstructive pulmonary disease in the horse. Equine vet. J. 13,243-246.
Thomson, J.R. and McPherson, E.A. (1984) Effects of environmental control on pulmonary function of horses affected with chronic obstructive pulmonary disease. Equine vet. J. 16,3538.
20, 1266-1268.

44 Chronic obstructive pulmonary disease
Thurlbeck, W.M. and Lowell, F.C. (1964) Heaves in horses. Am. Rev. Resp. Dis. 89, 82-88.
Tremblay, G.M., Ferland, C., Lapointe, J.-M., Vrins, A., Lavoie, J.P. and Cormier, Y. (1993) Effect of stabling on bronchoalveolar cells obtained from normal and COPD horses. Equine vet. J. 25, 194-197.
Vandenput, S., Duvivier, D., Votion, D., Art, T. and Lekeux, P. (1998) Environmental control to maintain stabled COPD horses in clinical remission: effects on pulmonary function. Equine vet. J. 30, 93-96.
Viel. L. (1983) Structural-Functional Correlations of the Lung in Horses with Small Airway Disease. PhD Thesis, University of Guelph.
Votion, D. and Lekeux, P. (1999) Scintigraphy of the equine lung. Equine vet. Educ. U, 300-309.
Watson, E.D., Mair, T.S. and Sweeney, C.R. (1990) Immunoreactive prostaglandin production by equine monocytes and alveolar macrophages and concentrations of PGE2 and PGF in bronchoalveolar lavage fluid. Res. vet. Sci. 49,88-91.
Watson, E.D., Sweeney, C.R. and Steensma, K.A. (1992) Arachidonate metabolites in bronchoalveolar lavage fluid from horses with and without COPD. Equine vet. J. 24,379-381.
Webster, A.J.F., Clarke, A.F., Madelin, T.M. and Wathes, C.M. (1987) Air hygiene in stables I: effects of stable design,
ventilation and management on the concentration of respirable dust. Equine vet. J. 19, 448-453.
Whitwell, KE. and Greet, T.R.C. (1984) Collection and evaluation of tracheobronchial washes in the horse. Equine vet. J. 16,499-508.
Willoughby, R.A. and McDonnell, W.N. (1979) Pulmonary function testing in horses. Vet. Clin. N. Am: Large. Anim. Pract. 1,357- 361.
Winder, N.C. and von Fellenberg, R. (1986) Immunofluorescent evaluation of the lower respiratory tract of healthy horses with chronic bronchiolitis. Am. J. vet. Res. 47, 1271-1274.
Winder, N.C. and von Fellenberg, R. (1988) Chronic small airway disease in the horse: immunohistochemical evaluation of the lungs with mild, moderate and severe lesions. Vet. Rec. 122,
Woods, P.S.A., Robinson, N.E., Swanson, M.C., Reed, C.E., Broadstone, R.V. and Derksen, F.J. (1993) Airborne dust and aeroallergen concentration in a horse stable under two different management systems. Equine vet. J. 25,208-213.
Yu, M., Wang, Z., Robinson, N.E. and LeBlanc, P.H. (1994a) Inhibitory nerve distribution and mediation of NANC relaxation by nitric oxide in horse airways. J. appl. Physwl. 76,339-344.
Yu, M., Wang, Z., Robinson, N.E. and LeBlanc, P.H. (199413) Modulation of bronchial smooth muscle function in horses with heaves. J. appl. Physiol. 77,2149-2154.
181-183.
Guardians of the Horse: st, Present a d Future BRITISH EQUINE VETERINARY ASSOCIATION AND ROMNEY PUBLICATIONS
Editors: Peter Rossdale, T i m Greet, Pat Harris, Rachel Green and Sherwin Hall
**OUT NOW**
With the new millennium nearly upon us it was decided to produce a celebratory publication giving a unique view of the evolution of man's relationship with the horse; and the progression in knowledge and understanding of those responsible for its care and welfare.
By inviting contributors to cover the past, present and future of their subjects, our intention has been to provide the reader with the balance of progress and speculation about the fkture. The past forms the basis of experience and provides an opportunity to recognise those on whom progress has depended; the present is of immediate concern in the challenges of our own Mespan; and the future an intriguing vista.
Use this book as a reference, read it in sections or &om cover to cover to achieve a better understanding of the horse and the relevance of modern methods which have been adapted for its weKare.This book will make a fascinating read for all those who love and appreciate this magnificent animal.
Over 60 authors have contributed to t h i s book. These include: Alistair B a q Peter Burrell, Rex Butte$eld, Eddie Cauvin, Bob Cook, Kees Dik, Tom Divers, Sue Dyson, Barrie Edwards, Richard Greenwood, Duncan Hannant, Doug Herthel, John Hickman, David Hodgson, Wayne Kes tq Geofley Lane, A1 Merritt, Helmut M e y q Bill Muir, Sidney Ricketts, Reuben Rose, Harold Schott, Lawson Soulsby and many more.
324 pages
Hardback Price ~30.00/$48.00 (US) Plus p&p E3.00 (L4.50/$7.00 outside the UK)
Please send orders to: Romney Publications, 351 Exning Road, Newmarket CB8 OAU, UK Fax: +44 (0) 1638 668 665