Scarring patterns and relative mortality rates of Indian ...

Epilepsy update- September 2016
Kasia Sieradzan
Consultant Neurologist

Epidemiology of epilepsy
Epilepsy is the most common serious neurological condition within the general population
Incidence 50/ 100,000/ year
Prevalence 5-10/ 1000 persons
(excluding febrile convulsions, single seizures, inactive cases)
- Lifetime prevalence 5%
(chance of having a seizure at some point in life)
65 million people world wide diagnosed with epilepsy
There are as many people with active epilepsy as there are people with insulin- dependant diabetes

Causes of Epilepsy Head injury CNS infections Stroke Hippocampal sclerosis Cortical dysplasias/ neuronal migration disorders Brain tumours Anoxic brain injury Autoimmune Drugs and alcohol Genetic or presumed genetic Epilepsy Syndromes; Juvenile myoclonic epilepsy (JME), Dravet syndrome, Juvenile absence epilepsy, Rasmussen syndrome, Angelman syndrome, Lennox- Gastaut syndrome etc……
No cause found in about 50% of patients .

Definitions
An epileptic seizure is a transient occurrence of signs and/or symptoms due to abnormal excessive synchronous neuronal activity in the brain.
Epilepsy is a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures, and by the neurobiologic, cognitive, psychological, and social consequences.
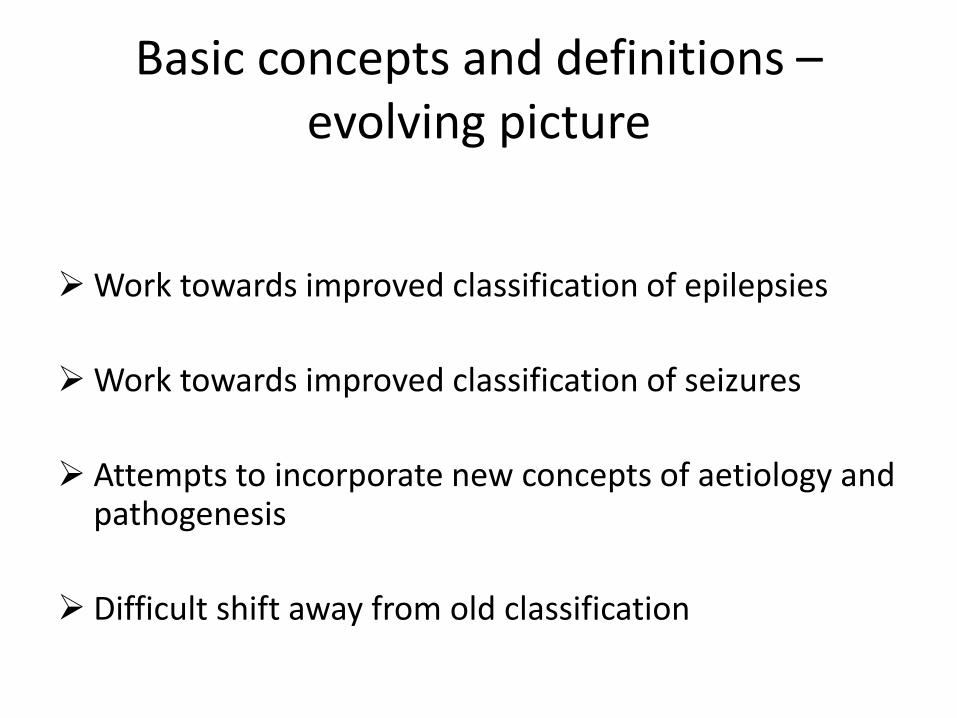
Basic concepts and definitions – evolving picture
Work towards improved classification of epilepsies
Work towards improved classification of seizures
Attempts to incorporate new concepts of aetiology and pathogenesis
Difficult shift away from old classification

Current International League Against Epilepsy definition – 2014
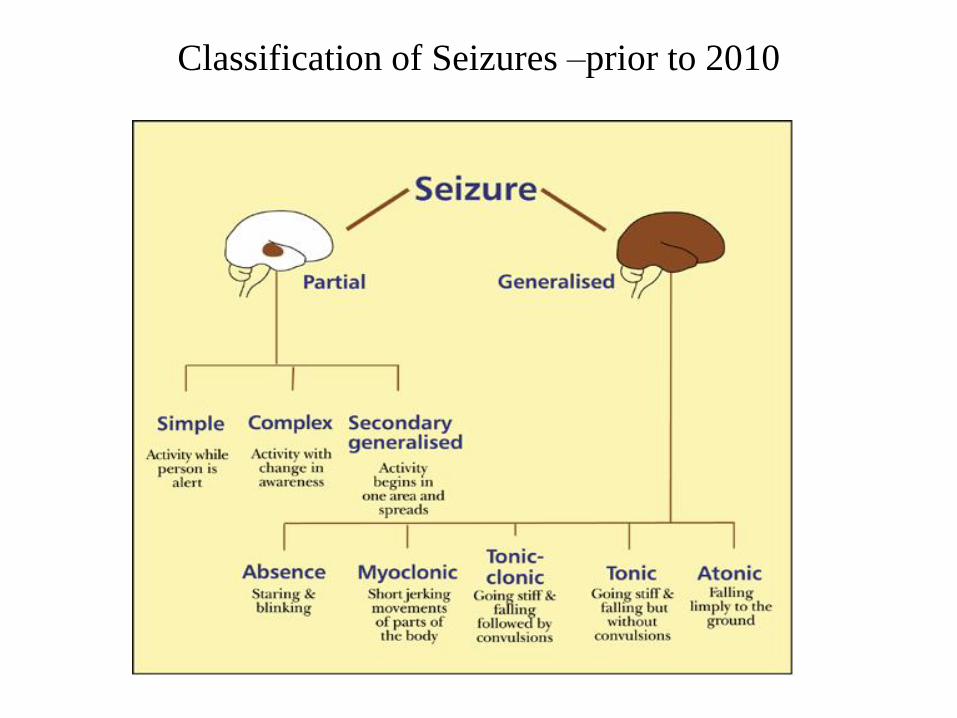
Classification of Seizures –prior to 2010
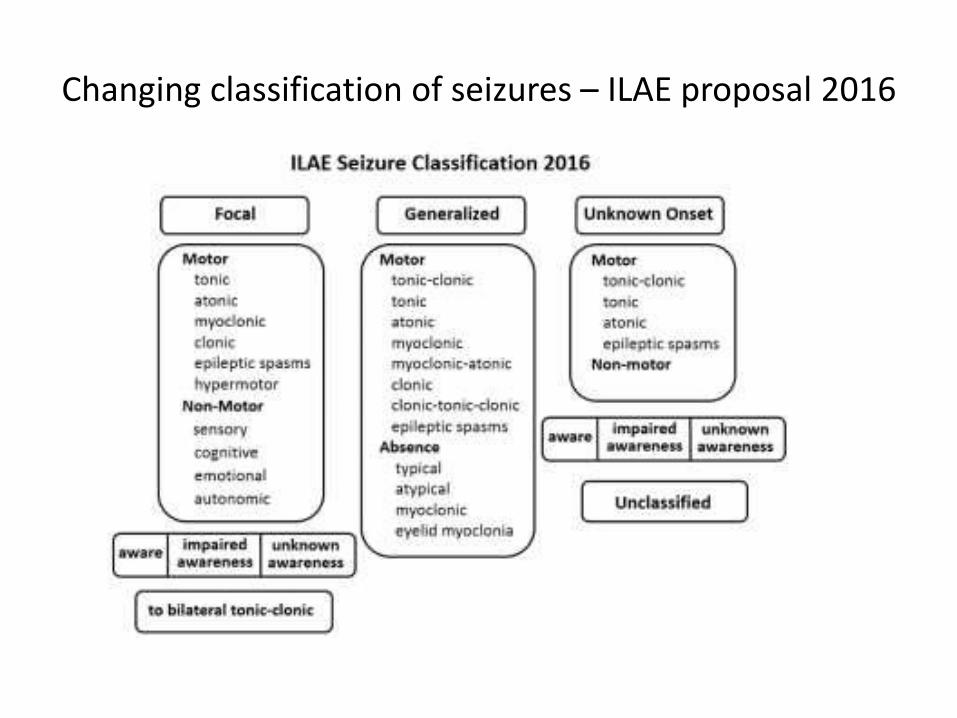
Changing classification of seizures – ILAE proposal 2016

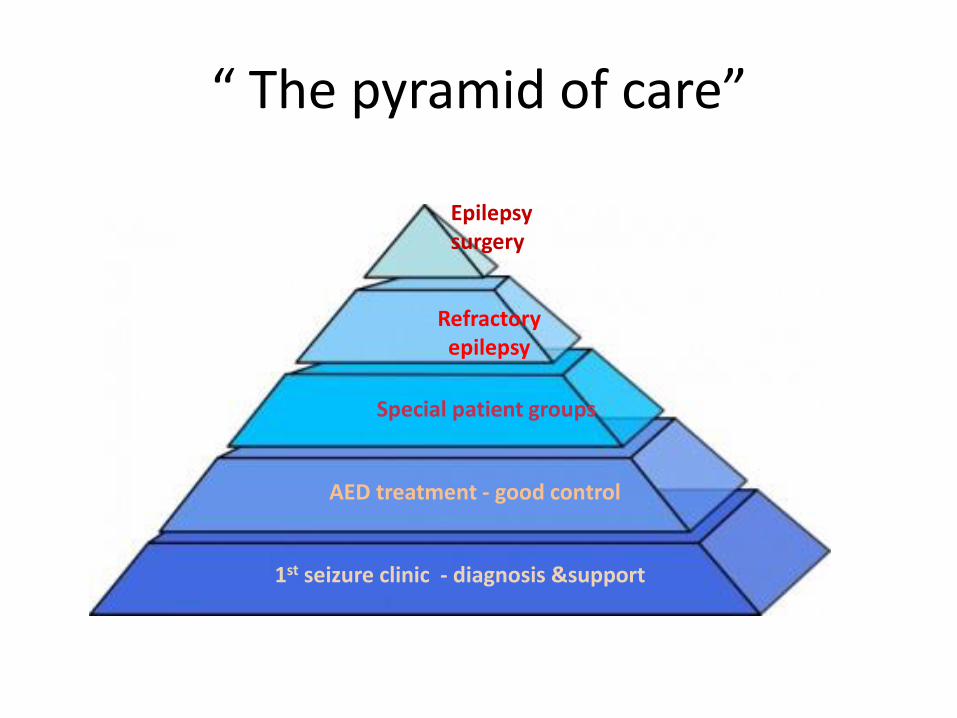
“ The pyramid of care”
1st seizure clinic - diagnosis &support
AED treatment - good control
Special patient groups
Refractory epilepsy
Epilepsy surgery
Comprehensive Epilepsy Service
• Epileptology • Neurophysiology • Neuropsychology • Neuropsychiatry • Neurosurgery • Epilepsy Nurses • Ketogenic diet • Full diagnostic
facilities • Research
• Transitional care • Women & Epilepsy • Epilepsy in Older Age • Epilepsy in Learning
Disability • Liaison with GPs and
community based-services

The essential service of the epilepsy specialist nurse
Medicines management
Education and training
Adviceand information
Specialised clinics
AssessmentCounselling And support
Liaison
Point of contact
Risk management
VNS, preoperative clinic, telephone clinics, Antenatal, Oncology
Empowerment
Increased awareness,
Ensuring adherence, reviewing and making changes in treatment, managing side effects
Current seizures, social and
Psychological situation, general
health and wellbeing
Improvement of quality of life
Continuity of care, liaison with, Epilepsy team,
paediatric service, GP’s allied health
professionals, LD service, charities, social services
etc
For Patients and other health
professionals, etc.
Fewer accidents, management of
prolonged seizures in community care,
reduction of admissions
Epilepsy Treatments
• AEDs
• SURGERY – Brain Surgery, VNS or DBS
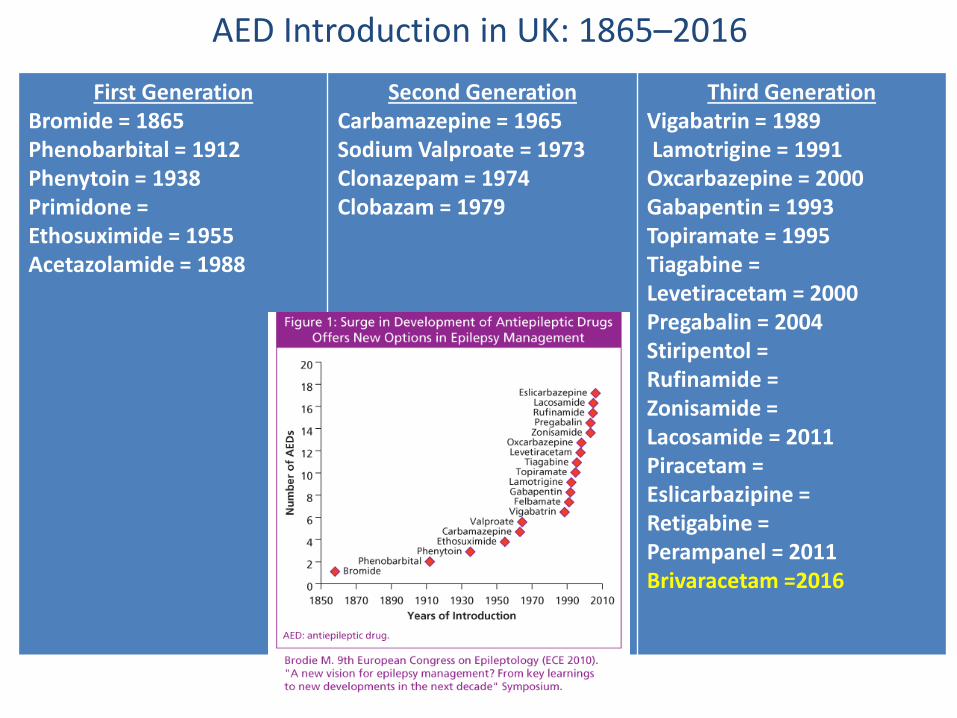
AED Introduction in UK: 1865–2016 First Generation
Bromide = 1865 Phenobarbital = 1912 Phenytoin = 1938 Primidone = Ethosuximide = 1955 Acetazolamide = 1988
Second Generation Carbamazepine = 1965 Sodium Valproate = 1973 Clonazepam = 1974 Clobazam = 1979
Third Generation Vigabatrin = 1989 Lamotrigine = 1991 Oxcarbazepine = 2000 Gabapentin = 1993 Topiramate = 1995 Tiagabine = Levetiracetam = 2000 Pregabalin = 2004 Stiripentol = Rufinamide = Zonisamide = Lacosamide = 2011 Piracetam = Eslicarbazipine = Retigabine = Perampanel = 2011 Brivaracetam =2016

Choosing an AED Primary criterion
Efficacy in particular seizure type Mechanism of action(s) may be an important criterion in the drug select process(s) may be an important criterion in
the drug selection process
Secondary criteria Ease of prescribing
Dose linearity – dosing straightforward
Time to steady state – allows rapid drug changes
Minimal interaction potential – co-medication not an
important consideration
Patient compliance
Elimination half-life of 12-24 hour – allows bid/od dosing
All dependent on AED Pharmacokinetics

Choice of 1st line AEDs
Focal epilepsies– Lamotrigine Levetiracetam Carbamazepine Lacosamide Eslicarbazepine Perampanel Pregabalin
Generalised epilepsy – Sodium Valproate (not in women of reproductive age)
Lamotrigine Levetiracetam Carbamazepine Perampanel Topiramate Zonisamide Ethosuximide (typical absence)

Shared care – traffic light system
• New AEDs introduced in the last 5 years
• Shared care protocols on SGNS
Brivaracetam – 2016
Lacosamide, Eslicarbazepine, Perampanel, Rufinamide, Tiagabine, Pregabaline
Carbamazepine; Levetiracetam, Lamotrigine; Topiramate; Valproate, Phenytoin, Clobazam, Clonazepam

SUDEP
Sudden Unexplained Death in Epilepsy “Sudden, unexpected, witnessed or unwitnessed, non traumatic and non
drowning death in patients with epilepsy, with or without evidence of a seizure,
and excluding documented status epilepticus, in which post mortem
examination does not reveal a toxicological or anatomic cause for death”
(Nashef 1997)
Probably accounts for approx 500 deaths a year in the UK
May account for 17% of all deaths of people with epilepsy

SUDEP – risk factors
• Early onset
• Male
• 20 – 40yrs old
• Tonic-clonic seizures
• Nocturnal
• Living alone
• Poor records
• Poor seizure control
• Non-compliance
• Polytherapy (more than one drug)
• Abrupt/frequent changes in AEDs
• Alcohol

Epilepsy in Women
Pregnancy

Epilepsy-related risks to the pregnancy outcome
• Effects of maternal seizures
• Effects of antiepileptic drugs
Core objectives: Prevent t-c seizures Reduce risk of foetal exposure
to AEDs major congenital
malformations neurocognitive &
behavioural toxicity
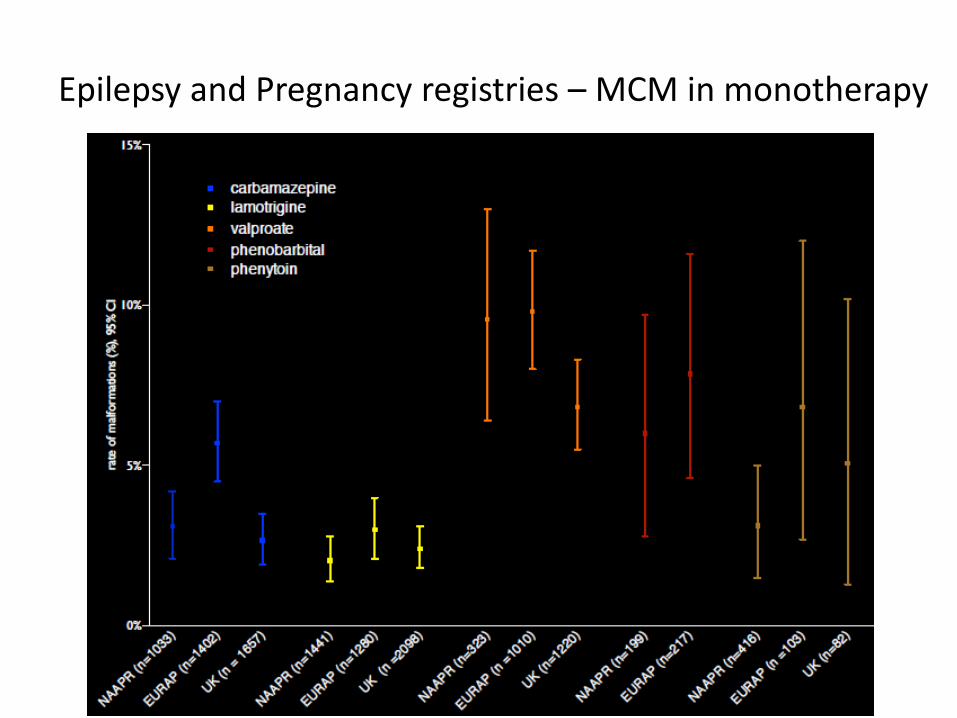
Epilepsy and Pregnancy registries – MCM in monotherapy
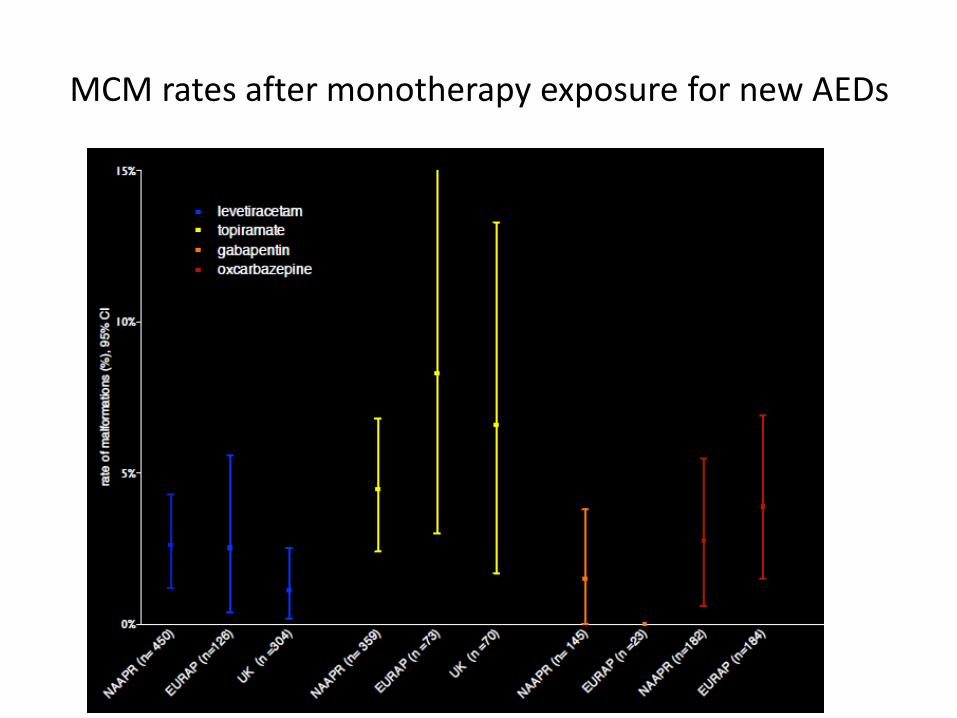
MCM rates after monotherapy exposure for new AEDs
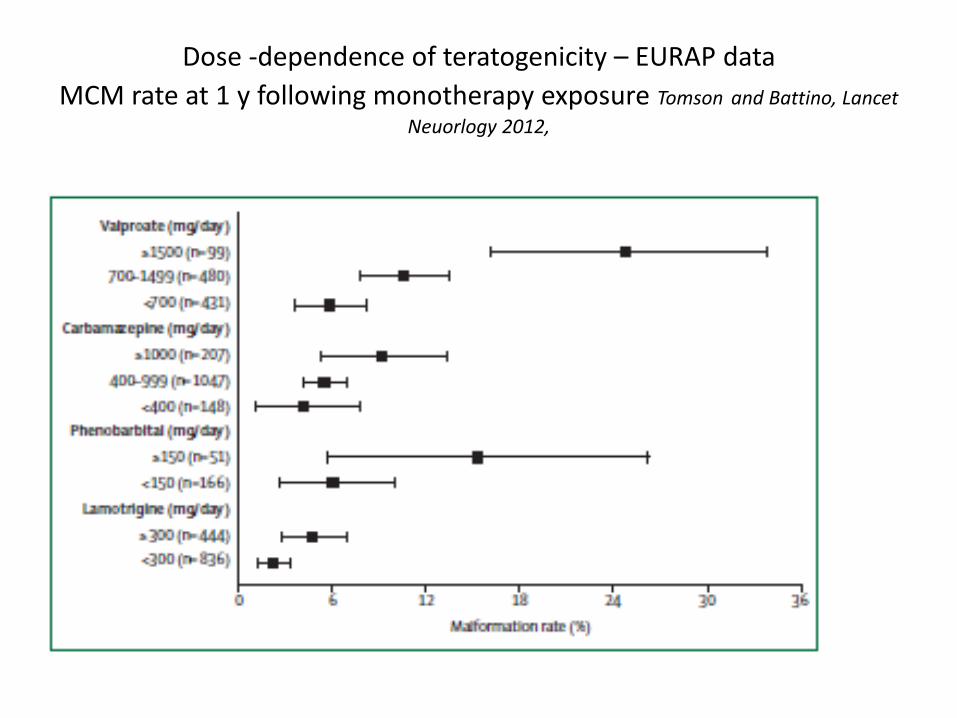
Dose -dependence of teratogenicity – EURAP data
MCM rate at 1 y following monotherapy exposure Tomson and Battino, Lancet
Neuorlogy 2012,

Dose dependence – UK Epilepsy &Pregnancy Register data 2014

Levetiracetam

Seizure control vs risk of MCM
Hernandez-Diaz Neurology 2012;78:1692-99

Neurocognitive Effects of
Antiepileptic Drugs (NEAD) Study
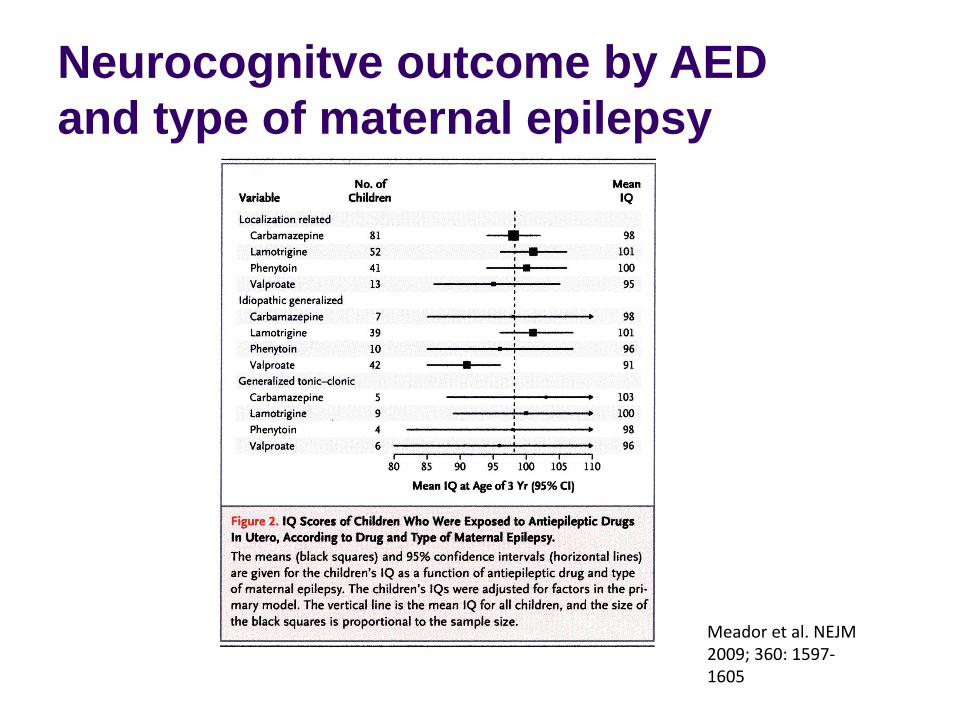
Neurocognitve outcome by AED
and type of maternal epilepsy
Meador et al. NEJM 2009; 360: 1597-1605

Neurocognitive outcomes by AED
and dose
Meador et al. NEJM 2009; 360: 1597-1605

Neurocognitive outcome in different monotherapy groups vs maternal intelligence
Meador et al. NEJM 2009; 360: 1597-1605


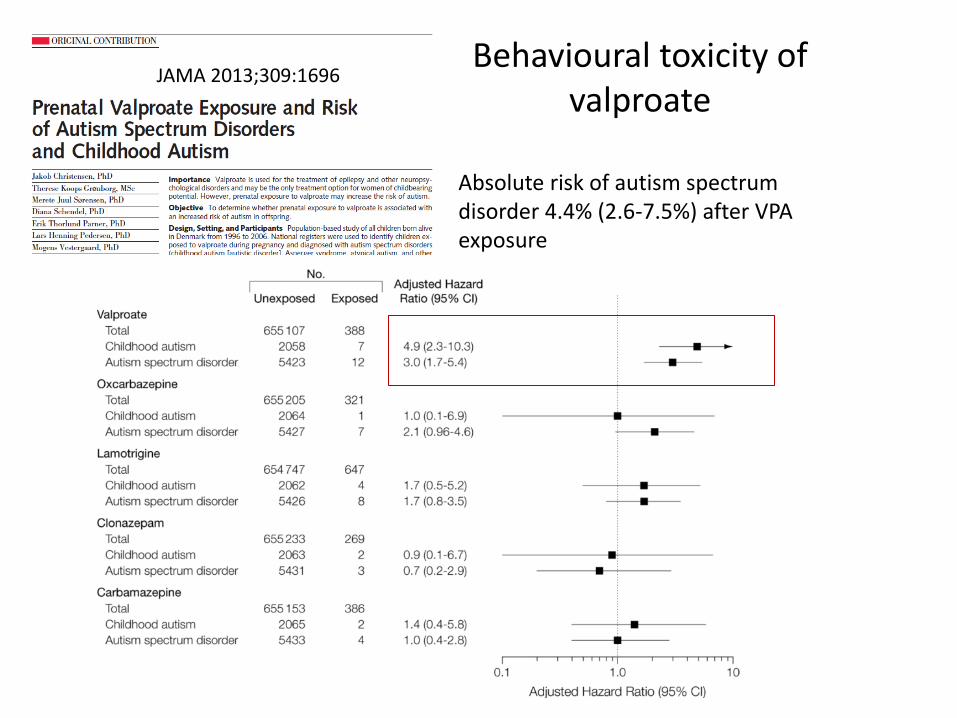
Behavioural toxicity of valproate
Absolute risk of autism spectrum disorder 4.4% (2.6-7.5%) after VPA exposure
JAMA 2013;309:1696


Physiological changes in AED concentrations during pregnancy
From Tomson, Pregnancy and Breastfeeding, EEC, Stockholm 2014

Lamotrigine – management in pregnancy
• Document individual pre-pregnancy plasma level • Monitor Ltg level monthly in pregnancy
– Problem with delayed reporting
• Increase dose empirically if seizures worsen and level not available
• Increase dose if level falls to 60-65% of pre-pregnancy value • Follow the experience of previous pregnancies • Anticipate post-partum Ltg toxicity – reduce dose (e.g. on days 3, 7, 10 to pre-conception dose + 50 mg extra to
compensate for sleep deprivation) Pennell et al. Neurology 2007; 70: 2130-36

Folic acid in pregnancy

Breast feeding and AEDs
• Levels in breast milk lower than maternal plasma levels except for levetiracetam, but v. low plasma levels in neonate
• V. small amonts of carbamazepine or valproate excreted in breast milk
• No significant problems with lamotrigine but some infants have 18-30% of maternal plasma level
• Potential for accumulation in some neonates due to immature liver (glucuronidation) and kidney function
• Adverse effects on the neonate generally not reported
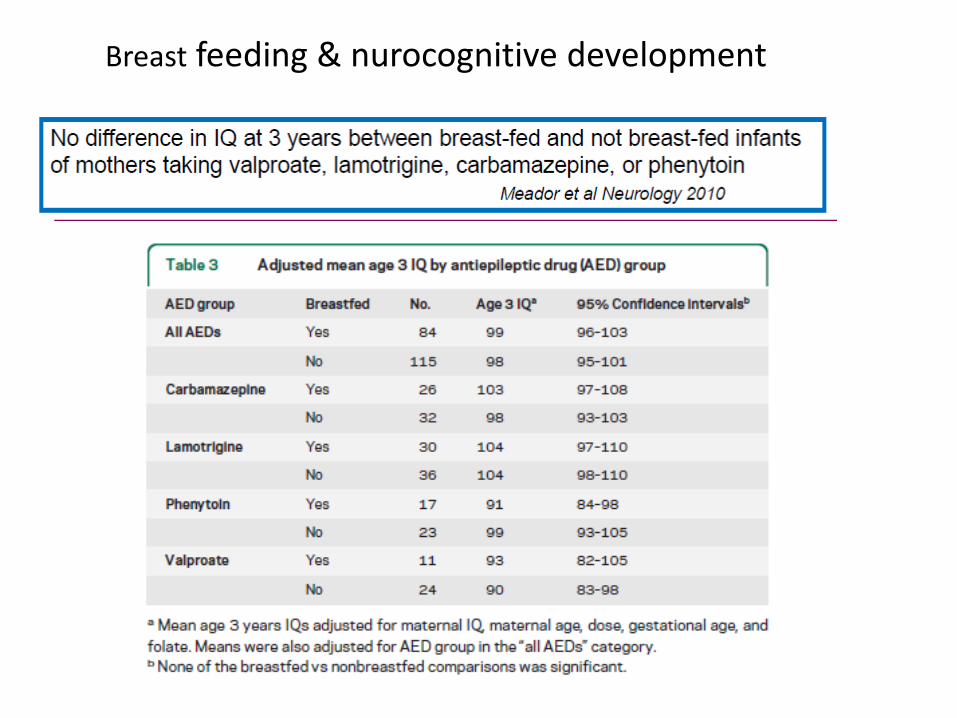
Breast feeding & nurocognitive development
Summary – management
– Effective liaison between GPs and specialist neurology and obstetric services
– Patient education from the stage of transition from the paediatric to adult service
– Consider elective transition to monotherapy
– Optimal AED therapy before conception
– Avoid valproate if alternatives exist
• make the patient aware of teratogenic risks
– Monitor Ltg plasma levels (? Other AEDs eg Lev)
– Support breast feeding

Epilepsy surgery
Resective surgery for patients with refractory epilepsy arising from a defined area of the brain that can be safely resected Criteria – medically refractory focal epilepsy -disabling, recurrent seizures - failed treatment for > 2 y on > 2 first line AEDs. Suitable patients: Hippocampal sclerosis in TLE patients Cortical dysplasias Benign tumours Small AVMs Postraumatic gliotic scarring Some non-lesional (“MRI-negative”) patients

Examples of “surgical” lesions causing epilepsy
Hippocampal
sclerosis
Low grade glioma
Focal cortical
dysplasia
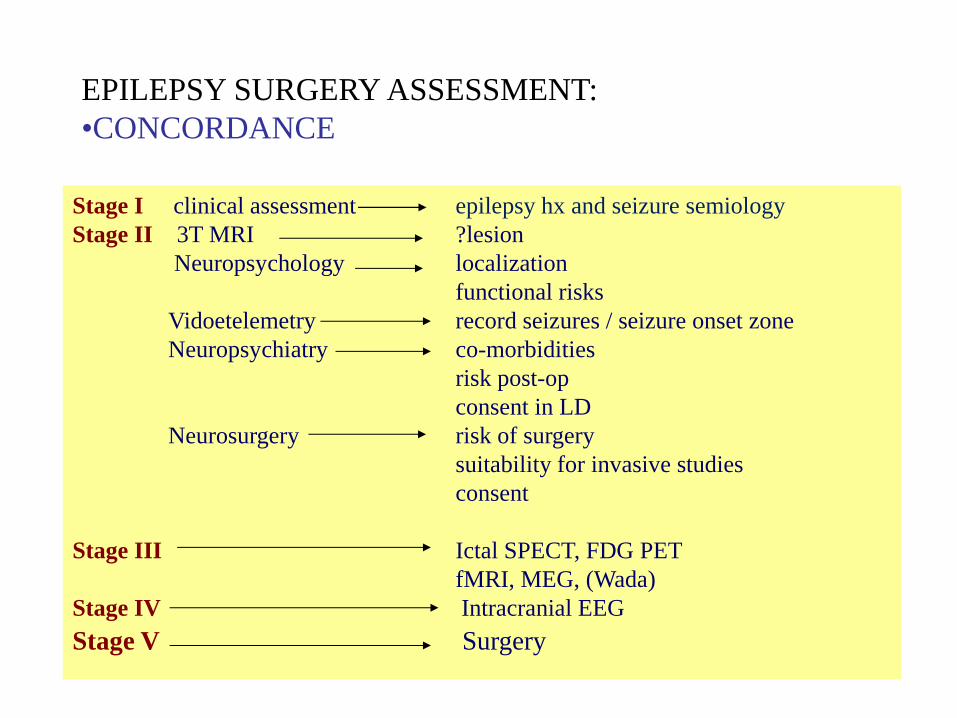
EPILEPSY SURGERY ASSESSMENT:
•CONCORDANCE
Stage I clinical assessment epilepsy hx and seizure semiology
Stage II 3T MRI ?lesion
Neuropsychology localization
functional risks
Vidoetelemetry record seizures / seizure onset zone
Neuropsychiatry co-morbidities
risk post-op
consent in LD
Neurosurgery risk of surgery
suitability for invasive studies
consent
Stage III Ictal SPECT, FDG PET
fMRI, MEG, (Wada)
Stage IV Intracranial EEG
Stage V Surgery

The Epilepsy Surgery Team Multidisciplinary team work
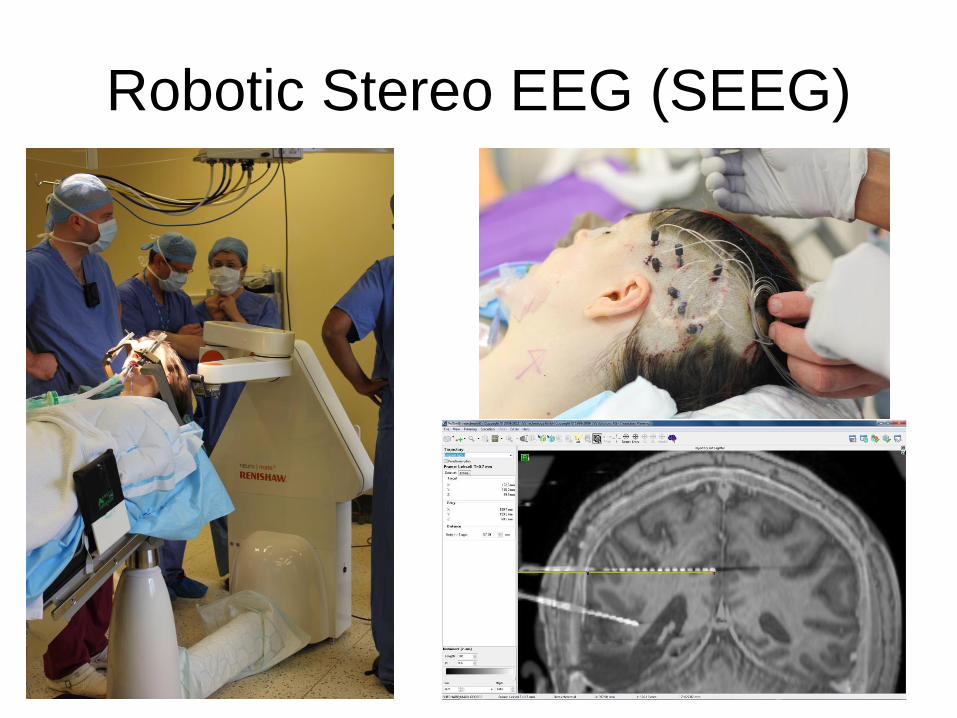
Robotic Stereo EEG (SEEG)

Depth electrode implantation 3D reconstruction – fusion of pre-operative MRI and post-operative CT – parietal epilepsy


Unsuitable for epilepsy surgery
Multifocal epilepsy
Primary generalized epilepsy
Seizure focus in eloquent cortical areas = high risk of postoperative deficits
May be suitable for vagus nerve stimulation (VNS) or disconnection procedures

Summary
• Vast topic clinically and scientifically
• Source of major disadvantage and stigma for patients
• Simple and complex epilepsy
• 70-80% achieve lasting remission and can be managed in primary care with re-referral/ specialist input as required
• Special needs of certain groups of patients
• Awareness of SUDEP
• Awareness of non-medical treatment options – too few patients referred for specialist assessment for surgery
• Cost effectiveness of treatment / utilisation of resources

Thank you
Questions ?