Epilepsy Specialist Symposium Treatment Algorithms in...
39
Epilepsy Specialist Symposium Treatment Algorithms in the Diagnosis and Treatment of Epilepsy November 30, 2012 Fred Lado, MD, Chair Montefiore Medical Center Albert Einstein College of Medicine Bronx, NY American Epilepsy Society | Annual Meeting
Transcript of Epilepsy Specialist Symposium Treatment Algorithms in...

Epilepsy Specialist Symposium Treatment Algorithms in the Diagnosis
and Treatment of Epilepsy
November 30, 2012
Fred Lado, MD, Chair
Montefiore Medical Center
Albert Einstein College of Medicine
Bronx, NY
American Epilepsy Society | Annual Meeting

How To Vote via Texting
1. Standard texting rates only (worst case US $0.20) 2. We have no access to your phone number 3. Capitalization doesn’t matter, but spaces and spelling do
TIPS

How To Vote via PollEv.com
Capitalization doesn’t matter, but spaces and spelling do TIP

Epilepsy Specialist Symposium Treatment Algorithms in the Diagnosis
and Treatment of Epilepsy
November 30, 2012
Fred Lado, MD, Chair
Montefiore Medical Center
Albert Einstein College of Medicine
Bronx, NY
American Epilepsy Society | Annual Meeting

Disclosure
Nothing to disclose
American Epilepsy Society | Annual Meeting 2012

Learning Objectives • Manage patients with first seizure by applying risk/benefit
analysis using prediction of seizure recurrence based on presentation and ancillary tests
• Evaluate patients for epilepsy surgery weighing the advantages/disadvantages of different approaches and understanding the rationale for selecting a specific approach
• Appropriately refer patients for implantation of and will successfully treat them with neurostimulator devices
• Discuss SUDEP with patients/families utilizing knowledge of both indications for discussion and understanding of pathophysiology of SUDEP.
American Epilepsy Society | Annual Meeting 2012

• Diagnosis and treatment of a first seizure Sheryl Haut, MD
• Debate surgical planning for extratemporal non-lesional surgery? Ashesh Mehta, MD and Francois Dubeau, MD
• Patient selection for treatment by devices (VNS, DBS) to palliate seizures Barbara Jobst, MD
• Discussing SUDEP Jeff Buchhalter, MD, PhD
Agenda

8
First seizure: Diagnosis,
treatment and prognosis November 30th, 2012
Sheryl Haut, M.D. Associate Professor of Clinical Neurology
Director, Adult Epilepsy Montefiore Medical Center
Albert Einstein College of Medicine
American Epilepsy Society | Annual Meeting

9
Disclosure
Acorda
Vivus
Upsher-Smith
Neuronex
American Epilepsy Society | Annual Meeting 2012
Consultant
Consultant
Consultant
Consultant

10
Learning Objectives
• To become familiar with the epidemiology of a first seizure, including definitions and incidence
•To understand factors related to recurrence risk after a first seizure
• To recognize the role of treatment on recurrence risk and integrate this role into clinical practice
American Epilepsy Society | Annual Meeting 2012

11
7 year old girl presents after a first
convulsive seizure noted by her parents
Seizure Description
Nocturnal, during sleep
Self limited after 2 minutes
Medical history
Normal birth and early development
No medical problems
No recent infections
Family history
One first cousin with epilepsy

12
Definitions
First unprovoked seizure
A seizure occurring in a person >1 month of age with no prior
history of unprovoked seizures
Excludes neonatal seizure; febrile seizure; acute
symptomatic seizure
Newly diagnosed epilepsy
Second unprovoked
seizure First presenting unprovoked
seizure, history of prior events

13
Seizure or epilepsy?
Epilepsy: Two or more unprovoked seizures
Is the definition of epilepsy changing? ILAE conceptual definition: “Disorder of the brain characterized by an
enduring predisposition to generate epileptic seizures and by the
neurobiologic, cognitive, psychological, and social consequences of
this condition. The definition of epilepsy requires the occurrence of
at least one epileptic seizure (Fisher 2005) .”
What time frame of 2 seizures constitutes “epilepsy”?
Experts Split on Whether Chief Justice
Roberts Has Epilepsy

14
Epidemiology of first seizure
Challenges
• Most studies do not distinguish first seizure from newly diagnosed epilepsy
• The majority of patients do not present for medical attention after a first seizure unless the seizure was a convulsion
• Overall, only one-third to one half of children and adults with seizures present after a first unprovoked seizure.

15
Incidence and recurrence risk
Incidence Incidence of first unprovoked seizure OR newly diagnosed epilepsy is 50-70/100,000 person years
Recurrence risk across studies
In studies that carefully exclude prior seizures, recurrence risk after a first seizure ranges from 27-52%
Risk factors for recurrence across studies
While recurrence rates vary across studies, risk factors for recurrence are more highly preserved
Role of age Recurrence risk and risk factors are remarkably similar for children and adults
Hauser 82, Hirtz 84, Annegers 86, Stroink 98, Shinnar 90, Berg 91, Hauser 93, First
Seizure Trial Group 93, Lindsten 01, others

16
7 year old girl presents after a first
convulsive seizure noted by her parents
Seizure Description
Nocturnal, during sleep
Self limited after 2 minutes
Medical history
Normal birth and early development
No medical problems
No recent infections
Family history
One first cousin with epilepsy
Results of testing
EEG: Left temporal spikes
MRI: Normal
ETIOLOGY

17
Etiology is a significant risk factor for seizure
recurrence after a first seizure
• Seizures without an immediate cause but with an identifiable prior brain injury
Remote symptomatic
• Occurring in otherwise normal individuals with no clear etiology Cryptogenic
• Presumed genetic epilepsy Idiopathic
• The new ILAE classification has revised these terms
Important disclaimer

18
PROGNOSIS OF CHILDREN WITH A FIRST UNPROVOKED
SEIZURE
PI Shinnar: 1 April 1988 - 31 March 2005 N=407
0
20
40
60
80
100
120
< 3 3 - 6 6 - 9 9 - 12 12 - 15 > 15
Age Distribution

19
All ≥ 10yr F/U
Number of Children 407 368 Mean Age at First Seizure (yrs) 6.8 6.8 Recurrent Seizures 185 (45%) 175 (48%) Total Number of Seizures to Date 1 (no recurrences) 222 (55%) 193 (52%) 2 (one recurrence) 49 (12%) 45 (12%) 3 20 ( 5%) 19 ( 5%) 4 14 ( 3%) 14 ( 4%) 5 15 ( 4%) 15 ( 4%) 6-9 27 ( 7%) 24 ( 7%) ≥ 10 60 (15%) 58 (16%)
Time (yrs)
0 5 10 15 20
Ris
k o
f S
eiz
ure
Re
cu
rre
nce
0.0
0.2
0.4
0.6
0.8
1.0
Overall
recurrence risk Shinnar et al 05

20
Time (yrs)
0 5 10 15 20
Ris
k o
f S
eiz
ure
Re
cu
rre
nce
0.0
0.2
0.4
0.6
0.8
1.0
Idiopathic/Cryptogenic (n=328)
Remote Symptomatic (n=79)
p < 0.0001
Recurrence Risk Following First Unprovoked Seizure Etiology (N=407)

21
Recurrence Risk Following First Unprovoked Seizure Etiology (N=407)
Time (yrs)
0 5 10 15 20
Ris
k o
f S
eiz
ure
Re
cu
rre
nce
0.0
0.2
0.4
0.6
0.8
1.0
Idiopathic (n=75)
Cryptogenic (n=253)
Remote Symptomatic (n=79)
p < 0.0001

22
Remote symptomatic etiology is associated
with a uniformly higher risk of recurrence
(Hauser 90, Shinnar 96, Stroink 98, Lindsten 01, FIRST trial, MESS trial, others)

23
7 year old girl presents after a first
convulsive seizure noted by her parents
Seizure Description
Nocturnal, during sleep
Self limited after 2 minutes
Medical history
Normal birth and early development
No medical problems
No recent infections
Family history
One first cousin with epilepsy
Results of testing
EEG: Left temporal spikes
MRI: Normal
State of patient

24
Sleep state at time
of first seizure
• Higher risk of seizure during sleep, whether daytime nap or nocturnal sleep • 2 year recurrence risk: 53% (asleep) vs 30% awake
Children: Sleep state
• Nocturnal seizures confer a higher recurrence risk, whether asleep or awake
Adults: Time of day
• Results persist after controlling for etiology and EEG
Strength of association
• Many studies have not examined time of day or sleep state Limitation
(Shinnar et al 93,Hopkins et al 88, van Donselaar et al 90,Camfield et al 85, Lindsten 01, MESS Trial 2010)

25
7 year old girl presents after a first
convulsive seizure noted by her parents
Seizure Description
Nocturnal, during sleep
Self limited after 2 minutes
Medical history
Normal birth and early development
No medical problems
No recent infections
Family history
One first cousin with epilepsy
Results of testing
EEG: Left temporal spikes
MRI: Normal
EEG abnormalities

26
Abnormal EEG and recurrence risk
• All studies in children indicate increased recurrence risk
• Most studies in adults indicate increased risk
Recurrence risk
• Focal spikes
• Generalized spike/wave
• Any epileptiform activity
• Any EEG abnormality
Specifics of abnormalities vary by study
• Risk persists even after controlling for other variables
Strength of association
• Utility of abnormal EEG is higher in non-remote symptomatic cases
• EEGs should include both sleep and awake when possible
Important considerations
(Hauser 82, Camfield 85, , Annegers 86,, van Donselaar 92, FIRST 93, Shinnar 96,Stroink 98, Kim et al 2006, MESS 2010)


28
Prognosis Following First Unprovoked Seizure EEG Abnormalities and Recurrence Risk
Idiopathic/Cryptogenic Cases (N=328)
EEG N Recurred (%) .
Number of Subjects 328 129 (39%)
EEG Available 305 126 (41%)
Abnormal EEG 124 (41%) 71 (57%)
Epileptiform Abnormalities 97 (31%) 61 (64%)
Focal Spikes (No Slowing) 60 (20%) 35 (58%)
Benign Rolandic 35 (11%) 20 (57%)
Slowing and Focal Spikes 10 ( 3%) 5 (50%)
Generalized Spike and Wave 34 (11%) 25 (74%)
Nonepileptiform Abnormalities 27 ( 9%) 10 (37%)
Slowing (No spikes) 20 ( 7%) 8 (40%)
Nonspecific Abnormalities 10 ( 3%) 4 (40%)
Normal EEGs 181 (59%) 55 (30%)
No EEG Available 23 3 (13%)
Shinnar et al 2005 Shinnar et al 2005

29
Other risk factors History of febrile seizure
Appears to increase the recurrence risk in remote symptomatic epilepsy only (Shinnar et al 2005)
Multiple seizures at first presentation
Seizures in a cluster are not independent (Haut et al 1997)
Results for recurrence risk differ among studies (Hauser 90, Shinnar 96, Ramos et al 2000 , Camfield et al 2000, Kho et al 2006)
Duration of initial seizure
Prolonged first seizure or status epilepticus does not increase recurrence risk
If seizure recurs, it is likely to be of similar duration however (Shinnar 05)
Seizure Classification
Partial > generalized (Hirtz 84, Shinnar 90, Camfield 85, Annegers 88)
Family history Family history of unprovoked seizures is generally not significant
Significant for siblings in the setting of idiopathic epilepsy

30
Treatment after a first seizure: What is the
evidence?
First Seizure Trial Group (FIRST)
Randomized subjects within 7 days after a first witnessed tonic-clonic seizure with or without partial onset:
Immediate treatment (carbamazepine, phenytoin, phenobarbital, or sodium valproate) vs. treatment with the same drugs only after seizure recurrence.
Multicenter study of early Epilepsy and Single Seizures (MESS):
Pragmatic trial which randomized subjects presenting with one or more seizures, where both clinician and patient were uncertain whether to proceed
with treatment:
Treatment was immediate vs. deferred; Medication choice was made by clinician
•At least four other studies: Camfield 89, Chandra 92, Gilad 96, Das 2000

31
FIRST Trial
• 22% treated vs.41% untreated had a recurrence (more than half within 6 months)
• Treatment reduced recurrence but more than 50% of untreated did not recur
Recurrence risk within 24 months
(FIRST1993, Musico et al 1997)
• 2 year remission (79%): 81% treated vs 78% untreated
• 5 year remission (64%): 63% treated vs. 64% untreated)
Long term remission
(Musico et al 1997, Leone et al 2006)
• Treatment reduced early recurrence but did not affect long term remission Conclusions
32
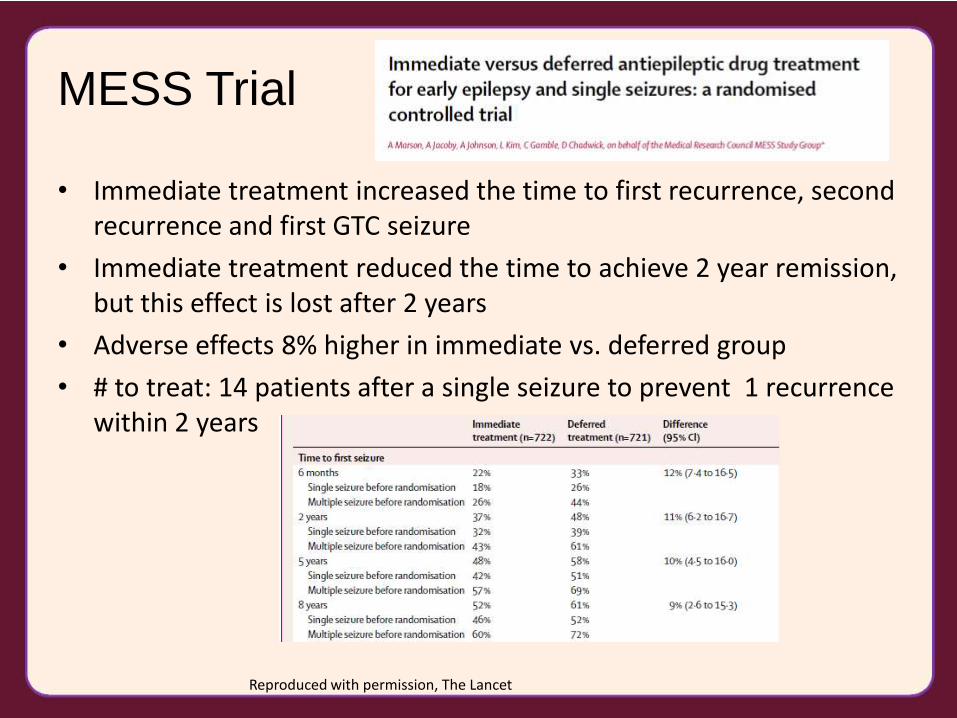
MESS Trial
• Immediate treatment increased the time to first recurrence, second recurrence and first GTC seizure
• Immediate treatment reduced the time to achieve 2 year remission, but this effect is lost after 2 years
• Adverse effects 8% higher in immediate vs. deferred group
• # to treat: 14 patients after a single seizure to prevent 1 recurrence within 2 years
Reproduced with permission, The Lancet

33
Recurrence risk and
implications for driving
Emerging European regulations allow driving after a single unprovoked seizure after six
months if recurrence risk is below 20%
Risk of recurrence within 12 months starting at the six
month point after a presenting seizure (if seizure free):
Treated group: 14% (CI 10-18%)
Untreated group: 18% (CI 13-23%)
Variables which increased the risk above 20%:
Remote symptomatic with abnormal EEG
Untreated non-remote
symptomatic with either abnormal
EEG and imaging
(Bonnett et al 2010 for MESS trial)

34
Risk allocation models
Camfield et al Neurology 1985, Reproduced with permission
Kim et al, Lancet Neurology 2006 Reproduced with permission

35
Other treatment considerations
Anxiety
• Patient may be very anxious about seizure recurrence; early treatment may alleviate anxiety
Injury
• Even a single seizure can cause injury
• Children are generally supervised at all times; risk of injury may be lower
• Adults may live alone, risk of injury may be higher
Duration of initial seizure
• If first seizure was prolonged or status epilepticus, recurrent seizure is more likely to be of similar duration

36
How long to treat?
• Medication withdrawal following treatment of a first seizure has not been well studied
• Studies of medication withdrawal in epilepsy demonstrate certain features reliably: – More successful in children than adults
– Success is higher when etiology is idiopathic; lowest when etiology is remote symptomatic
– Other Factors related to higher recurrence include lifetime # of seizures and presence of an abnormal EEG
• Available studies do not show an advantage of waiting more than 2 years of remission to withdraw AEDs
• Recommended rate of taper is typically 4-6 weeks
Gross- Tsur et al, 2004

37
Careful history: Prior seizure?
First unprovoked seizure
YES: Treat
No: Risk factors for recurrence?
No: Don’t treat
YES: Risk of recurrence >50%?
No: Other
considerations?
YES: Treat
YES: Treat
No: Don’t Treat
Sample treatment algorithm

38
Conclusions
• At least half of patients who present with a “first seizure” actually have newly diagnosed epilepsy
• Recurrence rates after a true first seizure in careful studies range from 27-52%
• Remote symptomatic etiology, abnormal EEG and seizure during sleep/night are among the strongest risk factors for recurrence
• Most recurrences occur during first 6 months
• Treatment after a first seizure reduces the rate of recurrence within the first 2 years but does not alter the long term prognosis
• Risk stratification modeling may help clinicians decide whom to treat

39
Acknowledgements
• Dr. Shlomo Shinnar
• Ruth Shinnar
• Montefiore-Einstein Epilepsy