Epilepsy in Inherited Metabolic and Mitochondrial Disorders Nordli Metabolic Genetic.pdf ·...
40
Epilepsy in Inherited Metabolic and Mitochondrial Disorders Douglas R. Nordli, Jr., MD Epilepsy Center, Children’s Memorial Hospital Chicago, Illinois, USA
Transcript of Epilepsy in Inherited Metabolic and Mitochondrial Disorders Nordli Metabolic Genetic.pdf ·...

Epilepsy in Inherited Metabolic and Mitochondrial Disorders
Douglas R. Nordli, Jr., MD Epilepsy Center, Children’s Memorial
Hospital Chicago, Illinois, USA

Metabolic Diseases
More than 11,000 characterized inherited disorders in man
200 associated with seizures and epilepsy 50 present in infancy

Metabolic Disorders
Prompt treatment Prognosis Genetic implications for family Reduce unnecessary testing Peace of mind Increase our understanding of physiology

How to Organize Material
Seizure type Myoclonic seizures, tonic seizures, spasms
General category of disease Peroxisomal, lysosomal, mitochondrial, etc.
Pathophysiological mechanisms

Pathophysiology: Energy Failure

Staring and Unresponsive

GLUT-1 DS: De Vivo’s Disease
Focal seizures in infancy Generalized seizures later Gen 2.5-3 Hz spike-wave discharges Ann Neurol 2003: PET study Thalamic involvement is hallmark (Generalized spike-waves also seen in
hyperammonemia / hypoglycemia)

Energy Failure Syndrome

Patient with Energy Failure Disorder

MELAS
With stroke-like episodes EEG shows focal features, including focal slowing,
attenuation, and spikes


Sabbagh et al. Epilepsia 2010 Respirtory Chain Disorders
Status Epilepticus in neonates with multiorgan failure (2) Neonatal myoclonic encephalopathy (3) Infantile Spasms (8) Recurrent status epilepticus (21) Epilepsia partialis continua (4) Myoclonic epilepsy (18)
In one third of patients abnl were only detected in the liver

Excitatory / Inhibitory Transmission
Note discontinuity; multifocal IEDs After Treatment

Excessive Excitation
Increased glutamate / GABA Glutamate GABA Requires B6 EEGs are discontinuous, multifocal IEDs

Accumulation of Toxic Substances After protein meal Baseline
Note attenuation of background, peculiar monorhythmic theta Multifocal spikes

OTC
Ornithine transcarbamylase deficiency Worsened by protein load Accumulation of ammonia EEG shows a low-voltage pattern, with diffuse slowing
and multifocal epileptiform discharges Two patients studied by Verma et al. in 1984
demonstrated episodes of sustained monorhythmic theta activity

Destructive Lesions
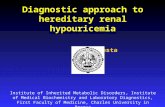
H E A D C I R C U M F E R E N C E
AGE (MONTHS)

Infant with Progressive Microcephaly
Background Attenuation Periodic
Brush-like pattern

Destructive Lesions
Erode complexity Some have peculiar EEG features Alpers- brush-like pattern NCL- vanishing EEG

Pathophysiology
Process Example EEG
Malformations PDH/PC, Zellweger Chaotic: B/S, hypsarhythmia
Destructive lesions NCL Reduced voltage (vanishing)
Toxins Urea Cycle Slowing, multiple IEDs, some unique patterns
Insufficient fuel GLUT-1 DS Gen S/W
Imbalance AA Pyridoxine Dep Chaotic: B/S

Metabolic Defect
Energy Failure
Disturbance of excitation / inhibition
Accumulation of toxic substances
Structural Damage

Seizure Types Associated with Metabolic Diseases in Infancy
Myoclonic seizures Infantile spasms Mixed seizures-combination of focal and
generalized elements Some tonic seizures

Problems Using Seizure Type to Identify Metabolic Disease
Limited repertoire in infants Seizures are etiologically non-specific

Organizing by Epilepsy Syndrome
Advantages Typical method of practice Incorporates more clinical information Some are caused by metabolic defects
Disadvantage Still not etiologically specific

Likely and Not-Likely Metabolic Disorders Likely Not-Likely
Early Myoclonic Encephalopathy (Aicardi) Benign Myoclonic Epilepsy
West Severe Myoclonic Epilepsy (Dravet)
Early Infantile Epileptogenic Encephalopathy (Ohtahara)
Benign Non-epileptic Infantile Spasms (Lombroso)
Neonatal Seizures Localization-related epilepsies with spasms
Multifocal epilepsies with focal seizures
Benign Infantile Partial Seizures (Watanabe)
Multifocal epilepsies with “generalized” seizures Localization-related epilepsies
Severe-Migrating Partial Seizures (Coppola et al.)

Age of Presentation Correlates with Epilepsy Syndrome
Age EEG Epilepsy
Neonatal Burst-suppression EME, EIEE
Early infantile Hypsarhythmia West
Late infantile Multifocal spikes/ more specific
Generalized myoclonic
Childhood Gen S/W, EPC, others (more specific) PME, EPC, others

Approach to Metabolic Disorders Presenting with Seizures
By epilepsy syndrome By age

Five Epilepsy Patterns
1. FAMILIAL EPILEPSIES
2. GENETIC GENERALIZED
EPILEPSIES
NORMAL
4a. EPILEPTOGENIC ENCEPHALOPATHIES
4b. SEVERE EPILEPTIC ENCEPHALOPATHIES
5. FOCAL STRUCTURAL
NAME
Normal
NORMAL
3. SELF-LIMITED EPILEPSY WITH FOCAL STEREOTYPED SPIKES
SLOWED
SLOWED, DISORGANIZED, AND
DISCONTINUOUS
FOCAL SLOWING/ATTENUATIO
N
EEG BACKGROUND
NONE
GENERALIZED AND STEREOTYPED
FOCAL OR MULTIFOACL AND STEROTYPED
MULTIFOCAL AND PLEOMOPRHIC
MULTIFOCAL AND PLEOMOPRHIC
FOCAL PLEOMORPHIC
SPIKES
Autosomal Dominant
SPIKES ARE STRONGLY GENETIC; EPILEPSY
ABOUT 30%
SPIKES ARE OFTEN AD; EPILEPSY LESS THAN
5%
MIXED
USUALLY DE NOVO, RARELY RECESSIVE
NONE
GENETICS
+/-
NO
NO
YES
YES
NO
GENETIC TESTING CLINICALLY
USEFUL
Mostly Favorable
VERY FAVORABLE, THOUGH SOME
REQUIRE LONG RX
VERY FAVORABLE
UNFAVORABLE
SEVERE
MIXED
OUTCOME

Electroclinical Syndromes
Nonsyndromic Epilepsies
- EME (Aicardi) - EIEE (Ohtahara)
- Benign familial neonatal epilepsy
-West syndrome -Late Infantile Epileptic Encephlopathy
-Benign familial infantile epilepsies
- Dravet; EFMR - Migrating focal seizures - Non-Progressive
Myoclonic Status
- **Febrile Seizures**
-Autosomal dominant nocturnal frontal lobe epilepsy
-Panayiotopoulos syndrome -Roladic Epilepsy -Late onset occipital (Gastaut)
-Lennox-Gastaut Syndrome
- No recognized syndromes
-With frontal foci
-Progressive Myoclonus Epilepsies
-AD with auditory features -AD familial temporal lobe
- No recognized syndromes
-Myoclonic infancy -**Febrile Seizures**
- Myoclonic atonic epilepsy -Childhood absence epilepsy -Epilepsy with myoclonic absence -Jeavons
- Juvenile absence -Juvenile myoclonic -Epilepsy with GTCs
- No recognized syndromes
1. Normal
2. Generalized stereotyped spikes; normal background
3. Focal/Multifocal Stereotyped Spikes; Normal Background
4a. Multifocal Spikes;
Background Slowing
4b. Multifocal spikes, discontinuity,
background slowing
-Epilepsies due to focal structural lesions -Can have homotopic EEG foci
5. Focal pleomorphic spikes; focal
slowing/attenuation
NEONATAL INFANCY
CHILDHOOD ADOLESCENCE
EEG FEAUTURES

Age EEG Features Screening Tests Disorders
Neonatal Burst-Suppression or Multifocal Spikes B6 Administration B6 Responsive Disorders
“ CSF Amino Acids Nonketotic Hypeglycinemia
“ Urinary Sulfite Dipstick/Serum Uric Acid
Molybdenum Cofactor Deficiency/Sulfite Oxidase Deficiency
“ Very Long Chain Fatty Acids (VLCFA) Peroxisomal Disorders
“ Lactate/Pyruvate Pyruvate Dehydrogenase Deficiency, Pyruvate Carboxylase Deficiency, Leigh syndrome
“ Serum Ammonia Early-Onset Multiple Carboxylase Deficiency
“ “ Urea Cycle Defects-neonatal citrullinemia
Low Amplitude Slowing “ Urea Cycle Defects- carbamoyl phosphate synthetase, ornithine transcarbamoylase, argininosuccinate synthetase
Comblike rhythm Serum Amino Acids/Urine Organic Acids Maple Syrup Urine Disease
Dysmature features during sleep Isovaleric Acidemia
Background slowing “ Proprionic Acidemia
Multifocal spikes, background slowing and depression “ Methylmalonic Acidemia

Early Infancy Burst-Suppression/ Multifocal spikes/slowed background
Serum Amino Acids Methylenetetrahydrofolate Reductase Deficiency
Hyposarhythmia Serum copper/ceruloplasmin Menke’s Disease
“ NONE PEHO Syndrome
“ Serum AminoAcids/Urine Organic Acids
Phenylketonuria and hyperphenylalaninemia, tyrosinemia type III, Hyperornithinemia-hyperammonemia-homocitrullinuria syndrome
“ “ Variety of organic acidurias including 3-mehtylglutaconic aciduria, 3-hyroxy- 3-mehtylglutaric aciduria, e-ydroxybutyric aciduria, 4-Hydroxybutyric aciduria
“ Lysosomal Hydrolases Tay-Sachs (hexosaminidase A)
“ “ Krabbe’s Disease (galactosylceramidase)
Multifocal spikes a-N-acetylgalactosaminidase (Schindler’s Disease)
Declining amplitude, very fast central spikes
Biotin Treatment/Biotinidase Screen
Biotinidase Deficiency
Background slowing, rhythmic temporal theta in type II (juvenile form)
Urinary oligosaccharides GM1 Gangliosidosis (Beta-Galactosidase)
Slowing/Posterior Spikes, Later 3 Hz spike-wave discharges
CSF glucose GLUT-1 Deficiency Syndrome

Late Infancy
Hypsarhythmia Serum electropheresis for CDG
Carbohydrate-deficient glycoprotein syndrome, CDG Type III
High Voltage, multifocal spikes
Lysosomal Hydrolases Metachromatic Leukodystrophy
low-amplitude fast activity (12 to 15 Hz) alternating with generalized slowing
Urine mucopolysaccharides Sanfilippo’s syndrome
Vanishing EEG in 1 Pseudoperiodic d/c in 2
Skin Biopsy with EM Infantile NCL; Late infantile NCL
continuous anterior high-voltage 1 to 3/s spike-wave-like activity
NONE Alper’s
LINCL Veneselli et al. 2001

Childhood and Adolescence
Background slowing, focal spikes Urine OA, Serum AA homocystinuria
Rhythmic trains of spike or sharp waves at 6 to 10/s
Gaucher cells in Bone Marrow Gaucher Type III
* Epilepsia Partialis Continua (EPC) Blood glucose Diabetes Mellitus with nonketotic hyperosmolar coma
* Focal slowing and spikes, 14- and 6-Hz positive bursts
Lactate MELAS
* EPC and Posterior attenuation/slowing
VLCFA Adrenoleukodsytrophy
Positive vertex spikes Urine oligosaccharides Sialidosis type I
4-6 Hz spike-wave discharges “ Sialidosis type II
Generalized 3-5 Hz SW, frontal predominance
DNA testing (no screen tests) Baltic Myoclonus
Generalized atypical spike-wave discharges
Lactate/Pyruvate MERRF
Generalized spike-wave and photoparoxysmal response
Triplet Repeats (no screening test available)
Dentatorubral-pallidoluysian atrophy
Generalized S/W, occipital spikes, with PPR
Skin Biopsy Lafora Disease
Multifocal spikes “ NCL type III
High-amplitude fast activity (16 to 24 Hz), unaltered by eye opening
Nerve Biopsy Neuroaxonal dystrophy

General Screening Tests
CBC with differential SMAC-20 Serum AA Urine OA Serum lactate / pyruvate Very long chain fatty acids Serum ammonia

Neonatal Seizures
Urea cycle defects Organic acidurias Biotin metabolism (multiple carboxylase,
holocarboxylase synthetase) Peroxisomal (Zellweger) Other: molybdenum cofactor / sulfite oxidase,
fructose, pyridoxine

Additional Neonatal Screening Tests
B6 administration CSF amino acids

Additional Infant Screening Tests
Lysosomal hydrolases Urine oligosaccharides / mucopolysaccharides Biotin treatment CSF glucose Serum copper / ceruloplasmin Lysosomal hydrolases Serum electropheresis for CDG Selective: skin biopsy

Additional Childhood Screening Tests
Urine oligosaccharides Selective
Bone marrow for Gaucher Nerve biopsy for neuroaxonal dystrophy Skin biopsy for NCL, Lafora Muscle biopsy for MELAS, MERRF DNA testing for MELAS, MERRF, DRPLA,
Baltic Myoclonus

Selected EEG Patterns and their Disorders
EEG pattern Disorder
Comb-like rhythm Maple Syrup Urine Propionic Acidemia
Fast central spikes Tay-Sachs Disease
Rhythmic vertex positive spikes
Sialidosis type I
Vanishing EEG Infantile NCL (type I)
High-amplitude 16-24 hertz activity
Infantile neuroaxonal dystrophy
Diminished spikes during sleep, giant SSEPS
PME
Marked photosensitivity PME and NCL, particularly type II

Conclusions
Rational approach is possible Several clues
Seizure types: myoclonic, spasms, tonic, mixed Epilepsies: NS, EME, West, Pleomorphic Clinical: unexplained encephalopathy
Organization by epilepsy syndrome / age EEG can be very useful Selective Diagnostic Testing