Epigenetic changes in myelodysplastic syndrome and acute … · 2015. 12. 23. · Revista Român ă...
7
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008 Epigenetic changes in myelodysplastic syndrome and acute myeloid leukemia: novel targets for therapy Andrei M. Cucuianu 1* , Anca Bacârea 2 , Mariana PaŃiu 1 , Delia M. Dima 1 1. “Ion ChiricuŃă” Cancer Institute, Hematology Department, Cluj-Napoca, Romania 2. University of Medicine and Pharmacy Târgu Mureş, Clinical Laboratory Department Abstract Epigenetic modifications, defined as DNA changes other than changed nucleotide sequence consist mainly of hypermethylation of gene promoters and histone deacetylation. Through these mechanisms, genes, in- cluding tumor suppressor genes can have a functionally altered expression and therefore be “silenced”. Epige- netically silenced tumor suppressor genes are common events in myelodysplastic syndromes (MDS) and acute myeloid leukemia (AML), usually correlating with poor prognosis. Epigenetic modifications may be useful tar- gets for therapy in MDS and AML. Two groups of drugs, demethylating agents (azacytidine and decitabine) and histone deacetylase inhibitors (phenyl-butyrate, valproic acid and suberoylanilide hydroxamic acid) have recent- ly been proven effective, either alone or in combinations, by several clinical trials in high-risk MDS and elderly high-risk AML. These agents were able to induce responses, even complete responses in patients known to have an extremely poor prognosis. In conclusion, epigenetic changes are important events in MDS and AML patho- genesis and progression; targeting these mechanisms is one of the strategies that have lately been incorporated in the therapeutic armamentarium of high-risk MDS and AML patients. Rezumat Modificările epigenetice, definite ca modificările ADN-ului altele decât schimbarea secvenŃei nucleoti- dice constau în principal în hipermetilarea regiunilor promoter ale genelor şi în de-acetilarea histonelor. Prin aceste mecanisme, genele, inclusiv genele supresoare tumorale suferă alterări funcŃionale, expresia lor fiind practic “cenzurată”. Cenzurarea epigenetică a genelor supresoare tumorale este relativ frecventă în sindroame- le mielodisplazice (SMD) şi leucemiile acute mieloide (LAM), aceste evenimente corelându-se deseori cu un prognostic infaust. Modificările epigenetice constituie însă Ńinte utile pentru tratamentul acestor afecŃiuni. Două grupe de molecule, agenŃii demetilanŃi (azacitidina şi decitabina) şi inhibitorii histon-deacetilazelor (fenil-buti- ratul, acidul valproic şi acidul hidroxamic suberoilanilidic) s-au dovedit eficienŃi, atât ca monoterapie cât şi în combinaŃii, în tratamentul SMD şi LAM la batrâni, în cazurile cu risc crescut. Aceşti noi agenŃi terapeutici au fost capabili să inducă răspunsuri obiective, chiar remisiuni complete la aceşti pacienŃi, cunoscuŃi ca având un prognostic deosebit de grav. In concluzie, modificările epigenetice sunt evenimente importante în patogeneza şi progresia SMD şi LAM; tratamentul Ńintit pe aceste modificări a fost încorporat recent în arsenalul terapeutic al pacienŃilor cu SMD şi LAM cu risc crescut. * Adresa pentru corespondenŃă: “Ion ChiricuŃă” Cancer Institute, Hematology Department, Cluj-Napoca, Roma- nia, Bd. 21 Decembrie Nr 73, 400124, Cluj-Napoca, Romania Tel: 0264-592766, Fax: 0264-598606, E-mail: [email protected] 39
Transcript of Epigenetic changes in myelodysplastic syndrome and acute … · 2015. 12. 23. · Revista Român ă...
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
Epigenetic changes in myelodysplastic syndrome and acutemyeloid leukemia: novel targets for therapy
Andrei M. Cucuianu1*, Anca Bacârea2, Mariana PaŃiu1, Delia M. Dima1
1. “Ion ChiricuŃă” Cancer Institute, Hematology Department, Cluj-Napoca, Romania2. University of Medicine and Pharmacy Târgu Mureş, Clinical Laboratory Department
Abstract
Epigenetic modifications, defined as DNA changes other than changed nucleotide sequence consistmainly of hypermethylation of gene promoters and histone deacetylation. Through these mechanisms, genes, in-cluding tumor suppressor genes can have a functionally altered expression and therefore be “silenced”. Epige-netically silenced tumor suppressor genes are common events in myelodysplastic syndromes (MDS) and acutemyeloid leukemia (AML), usually correlating with poor prognosis. Epigenetic modifications may be useful tar-gets for therapy in MDS and AML. Two groups of drugs, demethylating agents (azacytidine and decitabine) andhistone deacetylase inhibitors (phenyl-butyrate, valproic acid and suberoylanilide hydroxamic acid) have recent-ly been proven effective, either alone or in combinations, by several clinical trials in high-risk MDS and elderlyhigh-risk AML. These agents were able to induce responses, even complete responses in patients known to havean extremely poor prognosis. In conclusion, epigenetic changes are important events in MDS and AML patho-genesis and progression; targeting these mechanisms is one of the strategies that have lately been incorporatedin the therapeutic armamentarium of high-risk MDS and AML patients.
Rezumat
Modificările epigenetice, definite ca modificările ADN-ului altele decât schimbarea secvenŃei nucleoti-dice constau în principal în hipermetilarea regiunilor promoter ale genelor şi în de-acetilarea histonelor. Prinaceste mecanisme, genele, inclusiv genele supresoare tumorale suferă alterări funcŃionale, expresia lor fiindpractic “cenzurată”. Cenzurarea epigenetică a genelor supresoare tumorale este relativ frecventă în sindroame-le mielodisplazice (SMD) şi leucemiile acute mieloide (LAM), aceste evenimente corelându-se deseori cu unprognostic infaust. Modificările epigenetice constituie însă Ńinte utile pentru tratamentul acestor afecŃiuni. Douăgrupe de molecule, agenŃii demetilanŃi (azacitidina şi decitabina) şi inhibitorii histon-deacetilazelor (fenil-buti-ratul, acidul valproic şi acidul hidroxamic suberoilanilidic) s-au dovedit eficienŃi, atât ca monoterapie cât şi încombinaŃii, în tratamentul SMD şi LAM la batrâni, în cazurile cu risc crescut. Aceşti noi agenŃi terapeutici aufost capabili să inducă răspunsuri obiective, chiar remisiuni complete la aceşti pacienŃi, cunoscuŃi ca având unprognostic deosebit de grav. In concluzie, modificările epigenetice sunt evenimente importante în patogeneza şiprogresia SMD şi LAM; tratamentul Ńintit pe aceste modificări a fost încorporat recent în arsenalul terapeutic alpacienŃilor cu SMD şi LAM cu risc crescut.
*Adresa pentru corespondenŃă: “Ion ChiricuŃă” Cancer Institute, Hematology Department, Cluj-Napoca, Roma-nia, Bd. 21 Decembrie Nr 73, 400124, Cluj-Napoca, RomaniaTel: 0264-592766, Fax: 0264-598606, E-mail: [email protected]
39
userrTextbox1. List2004 (cited)
userrTextbox2. Mufti2003 (cited)
userrTextbox7. Baylin2005 (not cited)
userrTextbox3. Kantarjian2006 (cited)
userrTextbox4. Gore2006 (cited)
userrTextbox5. Silverman2006 (cited)
userrTextbox6. Liu2007 (cited)
userrTextbox8. Martelin2004 (not cited)
userrTypewriterWeight of copy-paste or inappropriate paraphrased text: 67% (no abstract)
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter
userrTypewriter- Figure reproduction without permission -
userrTypewriter
userrTypewriter
AdministratorTextbox9. Fenaux2007 (not cited)
AdministratorTextbox10. Engelhardt2007 (not cited)
AdministratorLine
AdministratorTypewriter
AdministratorTypewriterFalse bibliographic insertions
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
Epigenetic modifications define po-tentially reversible DNA and chromatinchanges, transmitted from a cell to its progeny,able to induce altered gene expression withoutchanging DNA sequence and without adding ordeleting any genetic information.
DNA normally exists in a complex con-figuration with proteins such as histones. His-tones organize DNA into units named nucleo-somes, which basically consist of DNAwrapped around a histone core. A histone coreconsists of two copies of each of four differentcore proteins (H2A, H2B, H3, H4). Histonescan be acetylated and methylated at N-terminallysine residues. The protein-DNA interactionsmediate packaging of DNA from ultra compact(the visible chromosomes during mitosis) tomost relaxed (the fine chromatin observed un-der the microscope in immature cells). Thischromatin remodeling process is determinedlargely by the balance between histone acetyla-tion and DNA methylation. When histones, es-
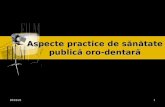
pecially H3 and H4 are hyper acetylated andDNA is not methylated the chromatin is “ac-tive”, the corresponding genes being ready fortranscription, whereas when H3 and H4 are notacetylated and DNA is methylated, the chro-matin is “inactive” leading to epigenetic silenc-ing of the corresponding genes, as shown inFigure 1 3,15.
Epigenetic silencing is essential for thenormal development of mammalian cells, asonly a certain genetic repertoire gets expressedin each cell type despite the common DNAblueprint9. However, over the past decades, ithas become apparent that cancer cells use theprocess of epigenetic silencing to their advan-tage by silencing the expression and function ofgenes that counteract the malignant phenotype,the so-called tumor-suppressor genes7. Regard-less of the underlying DNA defects, epigeneticsilencing has been found to be one of the com-mon downstream events in myelodysplasticsyndrome (MDS) and acute myeloid leukemia
40
Figure1. Impact of chromatin remodeling on gene transcription. Methylated cytosine residues in CpG(cytosine-guanosine) dinucleotides in promoter regions of genes recruit transcriptional repression complexesincluding histone deacetylases (HDAC), methyl CpG binding protein 2 (MeCP2) and Sin3. The deacetylatedlysine tails of the histones interact tightly with DNA, rendering the chromatin transcriptionally inactive (15).
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrRectangle
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrCalloutThis figure was lifted from Mufti2003 without author's permission
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
AdministratorSquiggly
AdministratorSquiggly
AdministratorSquiggly
userrHighlight
userrHighlight
AdministratorRectangle
AdministratorCalloutfalse text source
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
(AML) pathogenesis. Two interconnectedmolecular mechanisms are key to the process ofepigenetic silencing: DNA methylation of thepromoter regions of genes and histone modifi-cations.
DNA methylation occurs by covalentaddition of a methyl group at the 5’ carbon ofthe cytosine ring, resulting in 5-methylcytosine(Figure 2). These methyl groups project intothe major groove of DNA and effectively inhib-it transcription. In mammalian DNA, 5-methyl-cytosine is found in approximately 4% of ge-nomic DNA, primarily at cytosine-guanosinedinucleotides (CpG). CpG concentrations (is-lands) are typically found in or near promoterregions of genes. It was found that if such re-gions are heavily methylated the correspondinggenes do not get expressed. Hematologic malig-nancies demonstrate a link between methylationand the neoplastic phenotype8. AML and MDSare characterized by the hypermethylation andsilencing of multiple genes. This process canoccur early and may be detected in cases oflow-risk MDS but, in general, it is associatedwith disease progression. In MDS, for example,the cyclin-dependent kinase inhibitor P15 is afrequent target of aberrant methylation, and itsinactivation is associated with an increased riskof progression to AML12. A recent studyshowed that the gene encoding alpha-catenin(CTNNA1) is expressed at a much lower levelin leukemia-initiating stem cells from individu-als with AML or MDS with a 5q deletion than
in individuals with MDS or AML lacking a 5qdeletion or in normal haematopoietic stem cellsand that this is due to suppression by bothmethylation and histone deacetylation of theCTNNA1 promoter13. A number of other genesare similarly affected, including DAP kinase,regulators of apoptosis, SOCS1, involved in cy-tokine regulation, E-cadherin, involved in celladhesion and others. Methylation of these genesoccurs particularly in “high-risk” MDS and anincreased degree of methylation is associatedwith progression towards AML3.
Histone modifications include acetyla-tion, methylation, phosphorylation and ubiquiti-nation. Acetylation seems to be the most impor-tant histone-modulation process. In general,acetylation of lysine residues on histone tails isassociated with transcriptionally active chro-matin (euchromatin), whereas deacetylated his-tones are associated with transcriptionally inac-tive chromatin (heterochromatin). Histones areacetylated by enzymes which contain histoneacetyltransferase activity; in contrast, deacetyla-tion is mediated by histone deacetylases(HDAC). Several human HDACs have beenidentified to date, classified in 2 major classes:class I HDACs are almost exclusively nuclear,while class II HDACs shuttle in and out of thenucleus in response to specific cellular signals.HDACs are associated with specific chromatinloci in pairs and triplets. DNA methylation isfollowed by recruitment of histone deacety-lases, histone methylases, and eventually, a si-
41
N
0 N
NH2
N
0 N
NH2
cytosine 5-methylcytosine
CH3 N N
0 N
NH2
Ribose
N N
0 N
NH2
Deoxyribose
5-Azacytidine Decitabine
DeoxyriboseRibose
Figure 2. Chemical structure of cytosine, 5-methylcytosine and the demethylating cytosine analogs 5-azacytidine (AZA) and decitabine (DAC)
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
AdministratorSquiggly
AdministratorSquiggly
AdministratorSquiggly
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
lencing complex of proteins including hete-rochromatin protein 1 (HP1). By this mecha-nism, chromatin is remodeled such that it be-comes "invisible" to transcription factors,achieving a stable silenced state3,15.
Therapeutic implications of epigenet-ic changes in MDS and AML. Several com-pounds targeting DNA methylation and histonemodifications have so far proven beneficial inhigh-risk MDS and AML patients:
1. DNA Methylation Inhibitors inMDS and AML treatment
Two cytosine analogs, 5-azacytidine(AZA) and 5-aza-2'-deoxycitidine or decitabine(DAC) were found 25 years ago to specificallyinhibit DNA methylation by trapping DNA-methyltransferases (MTases). AZA can incor-porate into RNA and also is a pro-drug of DAC.DAC is phosphorylated by deoxycytidine ki-nase and incorporates efficiently into DNA. Thestructure of these compounds is presented inFigure 2. MTases, upon encountering DAC,form irreversible covalent bonds with the incor-porated base and are then targeted for degrada-tion in the proteosome. Cells then divide in theabsence of MTases, which results in progres-sive DNA hypomethylation and reactivation ofpreviously silenced genes. The covalent bindingof MTases to DNA can also result in cytotoxici-ty at high doses of DAC and/or high levels ofMTases10.
Clinical trials with azacytidine (AZA)were initiated two decades ago and revealed ef-ficacy at high doses in AML and at lower dosesin MDS. In a recent report, data from three se-quential trials comprising 309 patients wererecollected and reanalyzed. The dosage usedwas 75 mg/m2/d for 7 days every 28 days. Com-plete remissions were seen in 10% to 17% ofazacytidine-treated patients and 23% to 36% ofpatients had hematologic improvement. Themedian number of cycles to first response wasthree, and 90% of responses were seen by cycle6. The most frequent side effects consisted of
transient worsening of preexisting cytopenias.However, azacytidine did not increase the rateof infection or bleeding above the rate causedby the underlying disease18.
Decitabine (DAC) is more active thanAZA in vitro at equimolar doses and may havea different spectrum of activity and side effectscompared to AZA because it does not incorpo-rate into RNA. Clinical trials with DAC werealso initiated two decades ago and revealedpromising efficacy in hematologic malignan-cies20. In a phase III trial, 170 patients withMDS were randomized to receive either DACat a dose of 15 mg/m2, i.v., every 8 hours for 3days and repeated every 6 weeks, or best sup-portive care. Patients who were treated withDAC achieved a significantly higher overall re-sponse rate (17%), including 9% complete re-sponses, compared with supportive care (0%).Patients treated with decitabine had a trend to-ward a longer median time to AML progressionor death compared with patients who receivedsupportive care alone11. The most common ad-verse effects of decitabine, are due to myelo-suppression with transient grade 4 neutropeniaand thrombocytopenia being experienced by amajority of patients. Several studies are current-ly under way to test the effects of DAC inAML. A study on 51 elderly (median 72 years)AML patients, using the same dosage, showedobjective responses occurring in 31 % of pa-tients including complete remission in 14%. Be-sides the antileukemic effect, limited hospital-ization times, few adverse effects and the goodfeasibility of outpatient treatment, support DACtreatment in this subset of AML patients14.
Currently the hypomethylating agentsazacytidine (Vidaza R ) and decitabine (DacogenR) are commercially available. They have beenapproved for MDS treatment in USA and areunder clinical investigation in Europe and otherparts of the world. There are also several ongo-ing trials assessing the role of DAC in AMLHowever, it is still unclear which MDS andAML patients benefit most from the treatment
42
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
AdministratorRectangle
AdministratorCalloutfalse text source
AdministratorRectangle
AdministratorCalloutfalse text sources
AdministratorRectangle
AdministratorCalloutfalse text source
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
and which are the optimal drug schedules. Theresponse and survival data from the above men-tioned clinical trials seems to indicate that it isthe higher risk MDS patients, with un-favourable and intermediate karyotype and theelderly AML patients with unfavourable cyto-genetics who benefit mostly from hypomethy-lating agents. In fact in this groups of patientsthe other available therapeutic options are ex-tremely disappointing2.
An important issue is the fact that hy-pomethylating agents require 3 to 6 months oftreatment before response is obtained, thereforeone should not declare failure until at least 4courses of hypomethylating agents have beendelivered. Several trials also address the ques-tion of whether hypomethylating agents couldimprove the results of aggressive chemotherapyand allogeneic stem cell transplantation. Itseems that azacytidine and decitabine given asmaintenance therapy after intensive chemother-apy in high risk MDS may prolong the relapse-free survival with an acceptable toxicity pro-file3.
2. Histone deacetylase (HDAC) inhi-bitors in the treatment of MDS and AML
A variety of HDAC inhibitors (HDACi)are under clinical investigation. Interest in theuse of HDACi for the treatment of myeloid ma-lignancies dates back to the recognition of theactivity of butyrate derivatives and polar planarcompounds to induce differentiation. CertainAML fusion genes, such as AML1-ETO, PML-RAR , and PLZF-RAR specifically recruitnuclear corepression complexes which includeHDAC, thereby silencing expression of genesdownstream from the promoters bound by thefusion proteins. In such leukemias, HDACi maybe utilized to specifically reverse the transcrip-tional repression induced by the fusion prote-ins16. Among the several HDACi investigated,the following have been found most promising:
Small - chain fatty acids. A variety ofsmall-chain fatty acids inhibit HDAC activity at
submillimolar concentrations. These includesodium and arginine butyrate, sodiumphenylbutyrate, and valproic acid. Phase Istudies of continuous infusion phenylbutyrate(PB) demonstrated that the drug was well-toler-ated. The dosage was 375 mg/kg/day 21 daysevery 28 days, for a total of 12 weeks (three cy-cles). Lineage responses were achieved in sev-eral patients with MDS and AML5. Recent datademonstrating that valproic acid (VA) has sim-ilar HDAC inhibitory activity has raised hopesthat oral formulations of this drug, which iscommonly used for neuropsychiatric disorders,could be used to modulate gene expression. Thepharmacodynamic impact of VA on leukemiccells is similar to PB. VA is currently being in-vestigated in monotherapy and in combinationwith other drugs in MDS and in AML4.
Suberoylanilide hydroxamic acid(SAHA) also known as vorinostat is an oralHDAC inhibitor that modulates acetylation ofhistones and promotes apoptosis and differenti-ation in various leukemic cell lines in vitro.Clinical administration has also been associatedwith induction of histone acetylation. Severalphase I and phase II clinical trials have beenperformed, in a variety of hematological malig-nancies, including patients with AML andMDS. The doses used in these trials were be-tween 400 and 700 mg daily for 14 days, every21 days. In about 15-20% of patients partial ob-jective responses were observed, while the mostcommon toxicities were fatigue, diarrhea andthrombocytopenia17.
3. Combinations of drugs targetingepigenetic modifications in MDS and AML
Probably the best chance to improveclinical responses with epigenetic targeted ther-apy is by using combinations of active drugs.The recognition that HDAC recruitment ac-counted at least in part for the silencing ofgenes with methylated promoters led to thedemonstration that optimal reexpression of suchgenes required sequential exposure to a methyl-
43
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
AdministratorRectangle
AdministratorCalloutfalse text source
AdministratorRectangle
AdministratorRectangle
AdministratorCalloutfalse text sources
AdministratorCalloutfalse text sources
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
transferase inhibitor followed by an HDACi1.Following this encouraging in vitro data, sever-al investigators are presently testing the idea ofaugmenting the clinical activity of AZA andDAC through the subsequent addition of anHDACi. Gore et al6 evaluated a variety of dosesand schedules of AZA, followed by a 7-daycontinuous infusion of PB. The combinationhas been well-tolerated, and significant sus-tained clinical responses were achieved in 50%of patients. The responders, who had pretreat-ment methylation of p15 or CDH-1 promoters,reversed methylation during the first cycle oftherapy (methylation-specific PCR), whereasnone of nonresponders showed any demethyla-tion. Administration of both drugs was also as-sociated with induction of acetylation of his-tones H3 and H4. Garcia-Manero et al4 evaluat-ed DAC plus VA in a cohort of AML and MDSpatients, with an overall response rate of 53%(14% complete responses). Another direction isgiven by the fact that HDACi synergize withretinoids in a variety of systems. This has led tothe concept of potentially combining theseclasses of agents to build on the modest singleactivity of retinoids in MDS as single agents orin combination with growth factors. Studiescombining all trans-retinoic acid (ATRA) withPB and with VA are ongoing. In a recent phaseI/II study, the combination AZA, VA andATRA was tested in patients with AML orhigh-risk MDS. The overall response rate was42% and median remission duration was 26weeks19.
In conclusion, epigenetic changesseem to be important events in MDS and AMLpathogenesis and progression, especially inhigh risk patients. Targeting these mechanismshas become possible lately due to the incorpora-tion in treatment regimens of the demethylatingagents azacytidine and decitabine. Combiningthese agents with histone deacetylase inhibitorsand possibly with other molecules may redefinethe standard of care in high risk MDS and el-derly high-risk AML patients, who until recent-
ly have benefited mainly from supportive mea-sures.
References
1. Cameron EE, Bachman KE, Myohanen S, Her-man JG, Baylin SB. - Synergy of demethylation andhistone deacetylase inhibition in the re-expression ofgenes silenced in cancer. - Nat Genet 1999; 21:103–1072. Estey E. - Acute myeloid leukemia andmyelodysplastic syndromes in older patients. - J ClinOncol. 2007; 25:1908-19153. Fenaux P, Gardin C. - Epigenetic Therapy inmyelodysplastic syndromes. - Hematology Educa-tion: the education program for the annual congressof EHA, 2007;1:205-2134. Garcia-Manero G, Kantarjian HM, Sanchez-Gonzalez B, Yang H, Rosner G, Verstovsek S et al.-Phase 1/2 study of the combination of 5-aza-2'-de-oxycytidine with valproic acid in patients withleukemia. - Blood 2006;108:3271-32795. Gore SD, Weng LJ, Figg WD, Zhai S, Done-hower RC, Dover G et al. - Impact of prolonged in-fusions of the putative differentiating agent sodiumphenylbutyrate on myelodysplastic syndromes andacute myeloid leukemia. - Clin Cancer Res2002;8:963-9706. Gore SD, Baylin S, Sugar E, Carraway H, MillerCB, Carducci M et al. - Combined DNA methyl-transferase and histone deacetylase inhibition in thetreatment of myeloid neoplasms. - Cancer Res2006;66:6361-63697. Herman JG, Baylin SB. - Gene silencing in can-cer in association with promoter hypermethylation. -N Engl J Med. 2003;349:2042–20548. Issa JP. - CpG island methylator phenotype incancer. - Nat Rev Cancer. 2004;4:988–9939. Jones PA, Takai D. - The role of DNA methyla-tion in mammalian epigenetics. - Science.2001;293:1068–107010. Jones PA, Taylor SM. - Cellular differentiation,cytidine analogs and DNA methylation. - Cell.1980;20:85–93. 11. Kantarjian H, Issa JP, Rosenfeld CS, BennettJM, Albitar M, DiPersio J et al. - Decitabine im-proves patient outcomes in myelodysplastic syn-dromes: results of a phase III randomized study. -Cancer 2006;106:1794-1803.
44
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrRectangle
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrHighlight
userrRectangle
AdministratorSquiggly
AdministratorSquiggly
AdministratorRectangle
AdministratorCalloutfalse text sources
AdministratorRectangle
AdministratorCalloutfalse text sources
-
Revista Română de Medicină de Laborator Vol. 11, Nr. 2, Iunie 2008
12. List AF, Vardiman J, Issa JP, DeWitte T. -Myelodysplastic Syndromes. - Hematology2004:297-31713. Liu TX, Becker MW, Jelinek J et al. - Chromo-some 5q deletion and epigenetic suppression of thegene encoding alpha-catenin (CTNNA1) in myeloidcell transformation. - Nat Med. 2007;3:78-83. 14. Lübbert M, Rüter B, Schmid M, et al. - Contin-ued Low-Dose Decitabine (DAC) Is an Active First-Line Treatment of Older AML Patients: First Resultsof a Multicenter Phase II Study. - Blood (ASH An-nual Meeting Abstracts) 2005;106: Abstract 185215. Mufti G, List AF, Gore SD, Ho AY. -Myelodysplastic syndrome. - Hematology 2003:176-199.16. O’Connor O. - HDAC inhibitors: mechanismsof action and efficacy in the treatment of hematolog-ic malignancies. - Clinical Advances in Hematologyand Oncology 2006;4, Suppl 14: 3-417. O’Connor O, Heany ML, Schwartz L, Richard-son S, Willim R, MacGregor-Cortelli B et al. - Clini-cal experience with intravenous and oral formula-
tions of the novel histone deacetylase inhibitorsuberoylanilide hydroxamic acid in patients with ad-vanced hematologic malignancies. - J Clin Oncol2006;24:166-17318. Silverman LR, McKenzie DR, Peterson BLHolland JF, Backstrom JT, Beach CL, et al. - Furtheranalysis of trials with azacytidine in patients withmyelodysplastic syndrome: studies 8421, 8921, and9221 by the Cancer and Leukemia Group B. - J ClinOncol. 2006;24:3895-390319. Soriano AO, Yang H, Faderl S, Estrov Z, GilesF, Ravandi F et al. - Safety and clinical activity ofthe combination of 5-azacytidine, valproic acid andall-trans retinoic acid in acute myeloid leukemia andmyelodysplastic syndrome. - Blood. 2007;110:2302-2308 20. Wijermans PW, Lübbert M, Verhoef G,Klimek V, Bosly A. - An epigenetic approach to thetreatment of advanced MDS; the experience with theDNA demethylating agent 5-aza-2'-deoxycytidine(decitabine) in 177 patients. - Ann Hematol.2005;84, Suppl 13:9-17
45
userrRectangle
userrRectangle
userrRectangle
userrRectangle