New York Headache Center Headache Update Alexander Mauskop, MD.
Upload
mohamadrezaCategory
view
212download
0
ORIGINAL ARTICLE
Epidemiology and clinical characteristics of chronic dailyheadache in a clinic-based cohort of Iranian population
Seyed Mohammad Seyed Saadat • Mozaffar Hosseininezhad •
Babak Bakhshayesh • Mahsa Hoseini •
Mohamadreza Naghipour
Received: 8 June 2013 / Accepted: 12 September 2013
� Springer-Verlag Italia 2013
Abstract Although CDH is a major health care problem
encountered in headache clinics, our knowledge about the
epidemiological features of CDH is limited in developing
countries. The objective of this study was to survey the
frequency and clinical features of chronic daily headache
(CDH) and its subtypes among Iranian population pre-
senting to a referral tertiary Headache clinic in a University
Hospital. This cross-sectional survey was carried out
between September 2011 and March 2012. Data of patients
with CDH including their age, sex, educational level, and
marital status were recorded using structured face-to-face
interview. Subtypes of the CDH were determined by his-
tory, physical examination and appropriated laboratory or
imaging findings. A total number of 177 cases (32.71 %)
fulfilled the CDH criteria. The frequency of CDH was
higher in 40–49 age groups (n = 54) and among women
with a female to male ratio of 2.12/1. Chronic migraine was
the most common subtype of CDH in 75 cases (44.4 %).
Chronic tension-type headache and secondary causes were
second and third frequent subtypes of CDH in 27.8 and
20.1 % of cases, respectively. Cervicogenic headaches
(10.7 %) and medication overuse headache (4.1 %) were
the most common causes of secondary headaches. The
present study confirmed previous findings which showed a
high prevalence of CDH and chronic migraine in clinic
setting, with preponderance for women. In addition, we
found the highest prevalence of cervicogenic headaches
among secondary causes of CDH.
Keywords Chronic daily headache �Chronic tension-type headache � Migraine disorders �Tertiary care centers � Outpatient clinics � Iran
Abbreviations
CDH Chronic daily headache
CM Chronic migraine
CTTH Chronic tension-type headache
HC Hemicrania continua
NDPH New daily persistent headache
MOH Medication overuse headache
CH Cervicogenic headaches
ICHD International Classification of Headache
Disorders
Introduction
Chronic daily headache (CDH) is defined as a headache
that occurs on at least 15 days per month, for at least
3 months, and can be divided into primary and secondary
types [1–3]. Although CDH is a major health care problem
encountered in headache clinics, few studies have been
conducted regarding the epidemiological features of CDH
in developing countries, particularly in the Middle East and
Iran [4, 5], where environmental exposures, socioeconomic
condition, genetic background, availability of medical
services, trends in self-drug consumption, and geographic
S. M. Seyed Saadat � M. Hoseini
Medical Student Research Committee, Guilan University of
Medical Sciences, Rasht, Iran
M. Hosseininezhad � B. Bakhshayesh (&)
Department of Neurology, Poursina Hospital, Guilan University
of Medical Sciences, 41486-48476 Rasht, Iran
e-mail: [email protected]
M. Naghipour
Department of Social Medicine, Faculty of Medicine, Guilan
University of Medical Sciences, Rasht, Iran
123
Neurol Sci
DOI 10.1007/s10072-013-1550-2

characteristics are different. In the only population-based
study performed in Tehran, the capital of Iran and one of
the biggest cities in the Middle East [5], the prevalence of
CDH (7 %) among Iranian population was higher than
reported rates in most previous studies [6–9], and the
highest ever-reported prevalence rate of MOH (4.9 %) was
found among adult individuals of Tehran.
Considering that most previous studies were conducted
based on the old version of the CDH criteria [1], and given
that no clinic-based study have been performed on CDH
among Iranian population so far, therefore, we performed
this prospective study to survey the relative frequency of
CDH and its subtypes among Iranian patients attending to a
referral tertiary headache clinic in Rasht, the Capital city of
Guilan Province, northern Iran.
Materials and methods
This cross-sectional clinic-based study was performed in
the Headache outpatient Clinic of the Neurology Depart-
ment of Poursina University–Hospital in Rasht, which is
the main referral tertiary clinic in the province, from
September 2011 to March 2012. All patients attending to
our Headache Clinic for their first visit, with a chief
complaint of headache presented 15 days or more per
month in at least three consecutive months were recruited.
The study was approved by the Human Research Com-
mittee at the Guilan University of Medical Sciences
(GUMS). Our clinic patients mostly come from primary or
secondary care centers or refer from private centers or
offices. The purpose of the study was explained to all
participants, and written informed consent was obtained.
Patients with clinical presentation of CDH were further
evaluated to identify the specific causes of headache
according to the second edition of the 2004 International
Classification of Headache Disorders (ICHD-II) diagnostic
criteria [10].
Patients underwent structured face-to-face interview and
asked for baseline information including age, sex, educa-
tional level, marital status and a history of analgesic use or
overuse. Detailed history and complete general and neu-
rological examinations were carried out by two attending
neurologists. Routine laboratory tests as well as Brain CT
scan/MRI were performed where necessary. The body
mass index (BMI) of each patient was calculated. Data of
each patient were finally recorded in a questionnaire.
Further work-up using specific diagnostic laboratory tests
procedures or imaging tools (i.e., lumbar puncture, nerve
block, sinus radiographs, etc.) was attempted to rule out the
secondary causes in patients who presented with warning
signs and symptoms which were not consistent with the
diagnosis of primary headaches [3, 11, 12].
In patients with definite CDH, subtypes of CDH were
determined based on the ICHD-II. CDH was divided into
three main categorization including CM, CTTH and other
causes of primary CDH. Patients who did not meet the
criteria of ICHD-II were considered as ‘‘other CDH’’. We
considered secondary CDH as the main diagnosis if it was
accompanied by another subtype of CDH. We followed up
patients 2 months later using telephone call to confirm the
final diagnosis. The diagnosis of MOH was made accord-
ing to the revised ICHD-II criteria for 8.2 Medication
overuse headaches [13]. The diagnosis of MOH was ruled
out in patients whose headache was not resolved after
discontinuation of the overused or abused medication for a
period of 2 months. In those cases, the diagnosis of other
subtypes of headache syndrome was established based on
the ICHD-II classification.
Statistical analysis
The study data were analyzed using SPSS software. All
variables were normally distributed according to the Kol-
mogorov–Smirnov test. Descriptive data were reported
using mean ± SD and percentage. Due to normal distri-
butions, the parametric tests were used in the analyses. We
used test and one-way ANOVA to compare demographic
and clinical characteristics between different subgroups of
headache in this study. One-way ANOVA with post-hoc
Tukey test was performed to compare mean age between
different subtypes of CDH. P value B0.05 was considered
statistically significant.
Results
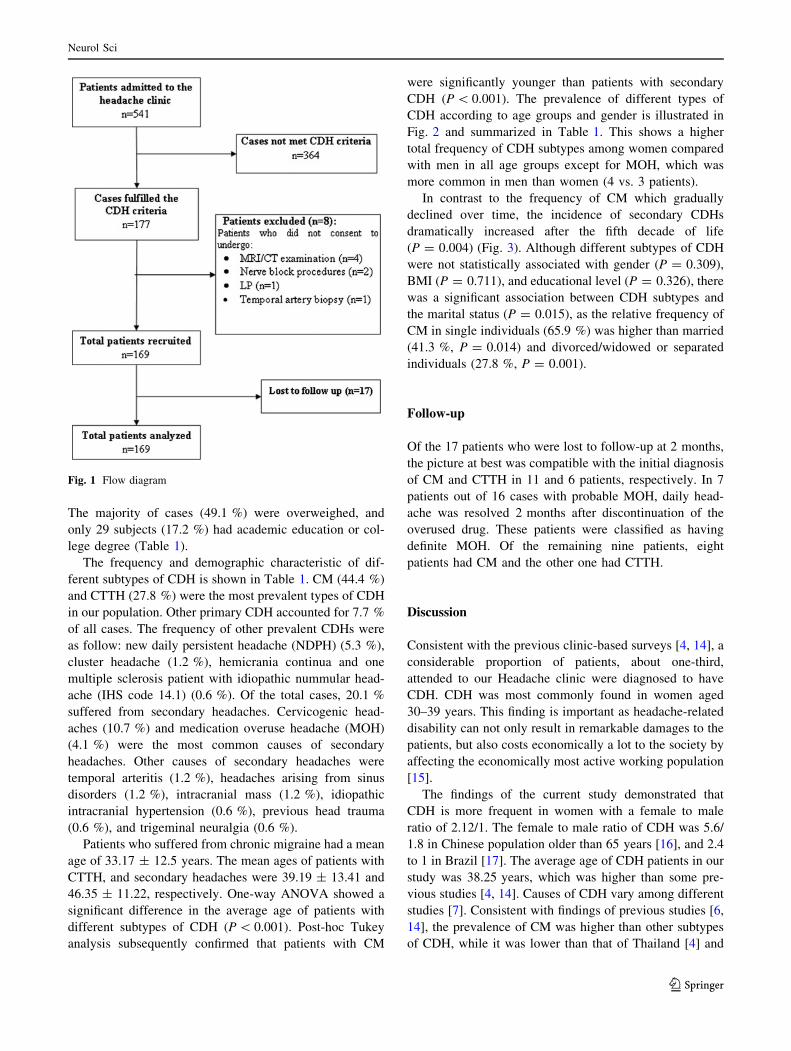
Of the 541 cases admitted to our headache clinic, 177 cases
(32.71 %) fulfilled the CDH criteria. Among 177 patients
with CDH, eight patients (4.5 %) with red flag signs and
symptoms were excluded from our study, because they did
not consent to undergo MRI/CT examination (n = 4),
nerve block procedures (n = 2), LP (n = 1), or temporal
artery biopsy (n = 1). After diagnostic work-up, 17
patients were lost to follow-up at 2 months, but included in
the final analysis based on their initial probable diagnosis.
Eventually, 169 patients were included in our study
(Fig. 1).
The prevalence of CDH was considerably higher in
female (68 %), with a female to male ratio of 2.12/1. The
mean age of patients was 38.25 ± 13.23 ranged from 11 to
76 years and the highest frequency of CDH was found in
the 40–49 age groups (n = 54). The mean age of male and
female patients with CDH was 37.96 ± 13.28 and
38.39 ± 13.26 years, respectively (P = 0.58). Thirty-six
subjects (21.3 %) were divorced, widowed or separated.
Neurol Sci
123
The majority of cases (49.1 %) were overweighed, and
only 29 subjects (17.2 %) had academic education or col-
lege degree (Table 1).
The frequency and demographic characteristic of dif-
ferent subtypes of CDH is shown in Table 1. CM (44.4 %)
and CTTH (27.8 %) were the most prevalent types of CDH
in our population. Other primary CDH accounted for 7.7 %
of all cases. The frequency of other prevalent CDHs were
as follow: new daily persistent headache (NDPH) (5.3 %),
cluster headache (1.2 %), hemicrania continua and one
multiple sclerosis patient with idiopathic nummular head-
ache (IHS code 14.1) (0.6 %). Of the total cases, 20.1 %
suffered from secondary headaches. Cervicogenic head-
aches (10.7 %) and medication overuse headache (MOH)
(4.1 %) were the most common causes of secondary
headaches. Other causes of secondary headaches were
temporal arteritis (1.2 %), headaches arising from sinus
disorders (1.2 %), intracranial mass (1.2 %), idiopathic
intracranial hypertension (0.6 %), previous head trauma
(0.6 %), and trigeminal neuralgia (0.6 %).
Patients who suffered from chronic migraine had a mean
age of 33.17 ± 12.5 years. The mean ages of patients with
CTTH, and secondary headaches were 39.19 ± 13.41 and
46.35 ± 11.22, respectively. One-way ANOVA showed a
significant difference in the average age of patients with
different subtypes of CDH (P \ 0.001). Post-hoc Tukey
analysis subsequently confirmed that patients with CM
were significantly younger than patients with secondary
CDH (P \ 0.001). The prevalence of different types of
CDH according to age groups and gender is illustrated in
Fig. 2 and summarized in Table 1. This shows a higher
total frequency of CDH subtypes among women compared
with men in all age groups except for MOH, which was
more common in men than women (4 vs. 3 patients).
In contrast to the frequency of CM which gradually
declined over time, the incidence of secondary CDHs
dramatically increased after the fifth decade of life
(P = 0.004) (Fig. 3). Although different subtypes of CDH
were not statistically associated with gender (P = 0.309),
BMI (P = 0.711), and educational level (P = 0.326), there
was a significant association between CDH subtypes and
the marital status (P = 0.015), as the relative frequency of
CM in single individuals (65.9 %) was higher than married
(41.3 %, P = 0.014) and divorced/widowed or separated
individuals (27.8 %, P = 0.001).
Follow-up
Of the 17 patients who were lost to follow-up at 2 months,
the picture at best was compatible with the initial diagnosis
of CM and CTTH in 11 and 6 patients, respectively. In 7
patients out of 16 cases with probable MOH, daily head-
ache was resolved 2 months after discontinuation of the
overused drug. These patients were classified as having
definite MOH. Of the remaining nine patients, eight
patients had CM and the other one had CTTH.
Discussion
Consistent with the previous clinic-based surveys [4, 14], a
considerable proportion of patients, about one-third,
attended to our Headache clinic were diagnosed to have
CDH. CDH was most commonly found in women aged
30–39 years. This finding is important as headache-related
disability can not only result in remarkable damages to the
patients, but also costs economically a lot to the society by
affecting the economically most active working population
[15].
The findings of the current study demonstrated that
CDH is more frequent in women with a female to male
ratio of 2.12/1. The female to male ratio of CDH was 5.6/
1.8 in Chinese population older than 65 years [16], and 2.4
to 1 in Brazil [17]. The average age of CDH patients in our
study was 38.25 years, which was higher than some pre-
vious studies [4, 14]. Causes of CDH vary among different
studies [7]. Consistent with findings of previous studies [6,
14], the prevalence of CM was higher than other subtypes
of CDH, while it was lower than that of Thailand [4] and
Fig. 1 Flow diagram
Neurol Sci
123

Ta
ble
1C
har
acte
rist
ics
of
chro
nic
dai
lyh
ead
ach
esan
dit
ssu
bty
pes
All
(n=
16
9)
CM
(n=
75
)C
TT
H(n
=4
7)
Oth
erty
pes
of
CD
H(n
=1
3)
Sec
on
dar
yC
DH
All
(n=
34
)M
OH
(n=
7)
CH
(n=
18
)O
ther
seco
nd
ary
cau
ses
(n=
9)
Mea
nag
eat
enro
lmen
t(±
SD
)*3
8.2
5(±
13
.23
)3
3.1
7(±
12
.15
)3
9.1
9(±
13
.41
)4
3(±
11
.40
)4
6.3
5(±
11
.22
)4
1.1
4(±
13
.49
)4
6.9
4(±
8.5
3)
49
.22
(±1
3.9
6)
Ag
eg
rou
ps
(%)*
*
10
–2
94
4(2
6%
)2
8(3
7.3
%)
12
(25
.5%
)2
(15
.4%
)2
(5.9
%)
2(2
8.6
%)
0(0
%)
0(0
%)
30
–3
94
4(2
6%
)2
2(2
9.3
%)
14
(29
.8%
)2
(15
.4%
)6
(17
.6%
)2
(28
.6%
)2
(11
.1%
)2
(22
.2%
)
40
–4
95
4(3
2%
)1
8(2
4%
)1
4(2
9.8
%)
7(5
3.8
%)
15
(44
.1%
)1
(14
.3%
)1
1(6
1.1
%)
3(3
3.3
%)
50
and
abo
ve
27
(16
%)
7(9
.3%
)7
(14
.9%
)2
(15
.4%
)1
1(3
2.4
%)
2(2
8.6
%)
5(2
7.8
%)
4(4
4.4
%)
Gen
der
(%)
Mal
e5
4(3
2%
)1
9(2
5.3
%)
18
(38
.3%
)6
(46
.2%
)1
1(3
2.4
%)
4(5
7.1
%)
4(2
2.2
%)
3(3
3.3
%)
Fem
ale
11
5(6
8%
)5
6(7
4.7
%)
29
(61
.7%
)7
(53
.8%
)2
3(6
7.6
%)
3(4
2.9
%)
14
(77
.8%
)6
(66
.7%
)
Ed
uca
tio
n(%
)a
Illi
tera
teo
rel
emen
tary
sch
oo
lA5
1(3
0.2
%)
21
(28
%)
13
(27
.7%
)5
(38
.5%
)1
5(4
4.1
%)
3(4
2.9
%)
7(3
8.9
%)
5(5
5.6
%)
Mid
dle
sch
oo
lB2
3(1
3.6
%)
9(1
2%
)7
(14
.9%
)0
(0%
)6
(17
.6%
)2
(28
.6%
)4
(22
.2%
)0
(0%
)
Hig
hsc
ho
olC
66
(39
.1%
)2
8(3
7.3
%)
19
(40
.4%
)5
(38
.5%
)1
1(3
2.4
%)
2(2
8.6
%)
7(3
8.9
%)
2(2
2.2
%)
Aca
dem
iced
uca
tio
no
rh
igh
erD
29
(17
.2%
)1
7(2
2.7
%)
8(1
7%
)3
(23
.1%
)2
(5.9
%)
0(0
%)
0(0
%)
2(2
2.2
%)
Mar
ital
stat
us
(%)*
**
Sin
gle
41
(24
.3%
)2
7(3
6%
)9
(19
.1%
)1
(7.7
%)
4(1
1.8
%)
2(2
8.6
%)
2(1
1.1
%)
0(0
%)
Mar
ried
92
(54
.4%
)3
8(5
0.7
%)
27
(57
.4%
)6
(46
.2%
)2
1(6
1.8
%)
2(2
8.6
%)
12
(66
.7%
)7
(77
.8%
)
Div
orc
ed,
sep
arat
edo
rw
ido
wed
36
(21
.3%
)1
0(1
3.3
%)
11
(23
.4%
)6
(46
.2%
)9
(26
.5%
)3
(42
.9%
)4
(22
.2%
)2
(22
.2%
)
Mea
nB
MI
(kg
/m2)
(±S
D)
26
.19
(±4
.03
)2
6.5
7(±
4.0
1)
25
.41
(±3
.95
)2
5.4
8(±
3.8
9)
26
.67
(±4
.24
)2
8.1
6(±
5.4
2)
26
.18
(±4
.37
)2
6.1
5(±
3.2
6)
BM
Ica
teg
ory
(%)
No
rmal
(%)b
55
(32
.5%
)2
1(2
8%
)1
8(3
8.3
%)
6(4
6.2
%)
10
(29
.4%
)1
(14
.3%
)6
(33
.3%
)3
(33
.3%
)
Ov
erw
eig
ht
(%)c
83
(49
.1%
)3
9(5
2%
)2
2(4
6.8
%)
6(4
6.2
%)
16
(47
.1%
)2
(28
.6%
)9
(50
%)
5(5
5.6
%)
Ob
ese
(%)d
31
(18
.3%
)1
5(2
0%
)7
(14
.9%
)1
(7.7
%)
8(2
3.5
%)
4(5
7.1
%)
3(1
6.7
%)
1(1
1.1
%)
Res
ult
sar
ere
po
rted
asm
ean
(±S
D)
or
asn
um
ber
(per
cen
tag
e)o
fp
atie
nts
CM
chro
nic
mig
rain
e,C
TT
Hch
ron
icte
nsi
on
-ty
pe
hea
dac
he,
MO
Hm
edic
atio
no
ver
use
sh
ead
ach
e,C
Hce
rvic
og
enic
hea
dac
hes
*P
\0
.00
1,
**
P=
0.0
4,
**
*P
=0
.01
5,
Pv
alu
ew
asn
ot
sig
nifi
can
tfo
ro
ther
par
amet
ers
aE
du
cati
on
alle
vel
was
defi
ned
asth
eh
igh
est
lev
elo
fed
uca
tio
nac
hie
ved
for
each
pat
ien
tan
dw
asca
teg
ori
zed
bas
edo
ny
ears
of
edu
cati
on
asfo
llo
ws:
Ail
lite
rate
or
elem
enta
rysc
ho
ol
(\6
yea
rs);
Bm
idd
lesc
ho
ol
(6–
8y
ears
);C
hig
hsc
ho
ol
(9–
12
yea
rs),
and
Dco
lleg
eo
rh
igh
er(m
ore
than
13
yea
rs)
bN
orm
alB
MI
isd
efin
edas
aB
MI
of\
25
cO
ver
wei
gh
tis
des
crib
edas
aB
MI
of
25
–2
9k
g/m
2
dO
bes
ity
isd
escr
ibed
asa
BM
Io
f3
0an
dm
ore
than
30
kg
/m2
Neurol Sci
123

elderly population of China [16], where CTTH was the
most common. A possible reason for this difference is
attributed to the study population. Since CM is accompa-
nied by higher intensity than other subtypes of CDH, it is
expected that patients with CM are more likely to seek for
medical care [15].
In our study there was no association between sex and
types of CDH. Although CM tended to occur more fre-
quently in women than CCTH [7], Both CM and CTTH
were more prevalent in our females’ cases. The distribution
of the CDH subtypes was different among our population
according to their age groups. In patients younger than
50 years, CM remained the most common cause of CDH.
Secondary causes of headaches were the common causes in
females older than 50 years. This pattern of distribution
was seen more predominantly in our female cases in their
6th decades of life or above. While no such a relationship
was seen among different age groups of male cases. In
accordance with the results of prior studies, most of our
patients who diagnosed to have CM and CTTM were in
their 4th decade of life [2, 18].
Secondary headaches caused one-fifth of all CDHs in
our study. Although MOH was the most common subtype
of secondary CDH in most previous studies [7, 14, 19],
cervicogenic (52.9 %) formed the most prevalent cause of
headache among our patients who diagnosed to have
secondary CDH. Moreover, MOH constituted 4 % of all
causes of CDH, which was less than our expectation.
However, this finding does not support the previous study
by Pascual et al. [14], who reported an 80 % prevalence of
analgesic overuse among individuals with CDH, and is in
contrary with results of a population-based study by Ca-
stillo who showed that 31 % of cases with CDH overuse
painkillers [19]. A possible explanation for this contra-
dictory result could be attributed to the use of different
diagnostic criteria for the definitions of MOH in prior
studies, resulted in substantial diversity in the reported
incidence and prevalence rates of MOH among studies. As
MOH was not considered as a single disorder in these
studies according to their used criteria; while, it is a
crucial criterion in the identification of CDH in new
revision of ICHD-II [4, 10, 13]. Cultural issues and a
lower tendency of patients to use medication for chronic
pain on their own in our area could explain other reasons
of such discrepancy. On the other hand, cervicogenic
headaches were responsible for 10.7 % of all causes of
CDH and 52.9 % of secondary causes in our study. This is
the highest ever-expressed frequency of CH compared
with previous similar studies [20–22], which reported the
prevalence of cervicogenic headaches ranged from 0.17 to
4.6 in different populations. This could be explained by
differences in designs and populations of studies, or use of
different diagnostic criteria, other than ICDH, in previous
studies [20]. Furthermore, new criteria do not have high
Fig. 2 Subtypes of CDH
stratified by age and gender.
Y number, X age (year)
Fig. 3 Frequencies of different subtypes of CDH according to the
age groups
Neurol Sci
123

specificity for the diagnosis of cervicogenic headaches, as
CM or CTTH may also respond to nerve block.
The current study had several limitations that should be
noted: (1) our study was conducted in a tertiary care center.
This could have resulted in selection bias of including only
severe cases in our study, and subsequently lead us to
overestimate the frequency of CDHs with higher severity
such as CM. As a result, we could not generalize our results
neither to the general population nor to primary care levels;
(2) as the data collection in our study was based on patient’s
self-reported information during face-to-face interview; the
analgesic overuse might not been reported properly by
individuals. Therefore, the rate of MOH in our study might
be underestimated; (3) as our Headache Clinic is a univer-
sity center that provides a cheaper service than private
centers; patients attending our center might have lower
socioeconomic status, which can influence the frequency of
CDH and its different subtypes among our study population.
Conclusion
In conclusion, CDH is among the leading causes of annual
visit to tertiary headache clinics, and CM remains as the
most common cause of CDH in both men and women
below 40 years of age. However, secondary causes should
always be considered, especially among women aged
above 40 years. Better understanding of the epidemiolog-
ical feature of CDHs helps general physicians and spe-
cialists of primary and secondary care settings to list
properly the differential diagnosis of chronic headaches
and choose the most effective treatment approach.
Acknowledgments We are grateful to all the patients for their
participation in the study. This work was financially supported by
grants from the Guilan University of Medical Sciences.
Conflict of interest The authors declare that there is no conflict of
interest.
References
1. Silberstein SD (2006) Chronic daily headache: classification,
epidemiology, and risk factors. Adv Stud Med 6:885–890
2. Vargas BB, Dodick DW (2009) The face of chronic migraine:
epidemiology, demographics, and treatment strategies. Neurol
Clin 27:467–479
3. Dodick DW (2006) Chronic daily headache. N Engl J Med
354:158–165
4. Srikiatkhachorn A, Phanthurachinda K (1997) Prevalence and
clinical features of chronic daily headaches in a headache clinic.
Headache 37:277–280
5. Shahbeigi S, Fereshtehnejad S-M, Mohammadi N, Golmakani
MM, Tadayyon S, Jalilzadeh G, Pakdaman H (2012) Epidemi-
ology of headaches in Tehran urban area: a population-based
cross-sectional study in district 8, year 2010. Neurol Sci
6. Lanteri-Minet M, Auray JP, El Hasnaoui A (2003) Prevalence
and description of chronic daily headache in the general popu-
lation in France. Pain 102:143–149
7. Lu SR, Fuh JL, Chen WT, Juang KD, Wang SJ (2001) Chronic
daily headache in Taipei, Taiwan: prevalence, follow-up and
outcome predictors. Cephalalgia 21(10):980–986
8. Ho KH, Ong BK (2003) A community-based study of headache
diagnosis and prevalence in Singapore. Cephalalgia 23(1):6–13
9. Yu S, Liu R, Zhao G, Yang X, Qiao X, Feng J, Fang Y, Cao X,
He M, Steiner T (2012) The prevalence and burden of primary
headaches in China: a population-based door-to-door survey.
Headache 52(4):582–591
10. The International Classification of Headache Disorders: 2nd
edition (2004) Cephalalgia 24 Suppl 1:9-160
11. Bigal ME, Lipton RB (2007) The differential diagnosis of chronic
daily headaches: an algorithm-based approach. J Headache pain
8:263–272
12. Goadsby PJ, Boes C (2002) Chronic daily headache. J Neurol
Neurosurg Psychiatry 72(Suppl II):ii2–ii5
13. Silberstein SD, Olesen J, Bousser MG, Diener HC, Dodick D,
First M, Goadsby PJ, Gobel H, Lainez MJ, Lance JW, Lipton RB,
Nappi G, Sakai F, Schoenen J, Steiner TJ (2005) The International
Classification of Headache Disorders, 2nd Edition (ICHD-II)–
revision of criteria for 8.2 Medication-overuse headache. Cepha-
lalgia 25(6):460–465. doi:10.1111/j.1468-2982.2005.00878.x
14. Pascual J, Colas R, Castillo J (2001) Epidemiology of chronic
daily headache. Curr Pain Headache Rep 5:529–536
15. Silva Junior A, Tavares R, Lara R, Faleiros B, Gomez R, Teixeira
A (2012) Frequency of types of headache in the tertiary care
center of the Hospital das Clı́nicas of the Universidade Federal de
Minas Gerais, MG, Brazil. Rev Assoc Med Bras 58(6):709–713
16. Wang SJ, Fuh JL, Lu SR (2000) Chronic daily headache in
Chinese elderly: prevalence, risk factors, and biannual follow up.
Neurology 54:314–319
17. Queiroz LP, Peres MFP, Kowacs F, Piovesan EJ, Ciciarelli MC,
Souza JA, Zukerman E (2008) Chronic daily headache in Brazil:
a nationwide population-based study. Cephalalgia 28:1264–1269
18. Bigal ME, Lipton RB (2009) The epidemiology, burden, and
comorbidities of migraine. Neurol Clin 27:321–334
19. Castillo J, Munoz P, Guitera V, Pascual J (1999) Epidemiology of
chronic daily headache in the general population. Headache
39:190–196
20. Knackstedt H, Bansevicius D, Aaseth K, Grande RB, Lundqvist
C, Russell MB (2010) Cervicogenic headache in the general
population: the Akershus study of chronic headache. Cephalalgia
30(12):1468–1476. doi:10.1177/0333102410368442
21. Nilsson N (1995) The prevalence of cervicogenic headache in a
random population sample of 20-59 year olds. Spine 20(17):
1884–1888
22. Bogduk N, Govind J (2009) Cervicogenic headache: an assess-
ment of the evidence on clinical diagnosis, invasive tests, and
treatment. Lancet neurol 8:959–968
Neurol Sci
123