Epidémiologie et maîtrise de la tuberculose: situation...
27
Epidémiologie et maîtrise de la tuberculose: situation internationale Hans L Rieder Union Internationale Contre la Tuberculose et les Maladies Respiratoires Paris, 24 mars 2009
Transcript of Epidémiologie et maîtrise de la tuberculose: situation...
Epidémiologie et maîtrise de la tuberculose:
situation internationale
Hans L Rieder
Union Internationale Contre la Tuberculose et les Maladies Respiratoires
Paris, 24 mars 2009

GDP (in US$) per head (log scale)
Tube
rcul
osis
cas
espe
r 100
,000
(log
sca
le)
2.55
10
20
50
100 200 500 10,0005,000
100
1,000 2,000
500
200
1,000
20,000 50,000
IndiaChina
France
Janssens JP, Rieder HL. Eur Respir J 2008;32:1415-6
Relationship between estimated tuberculosis incidencerates 2004 and per capita gross domestic product 2005
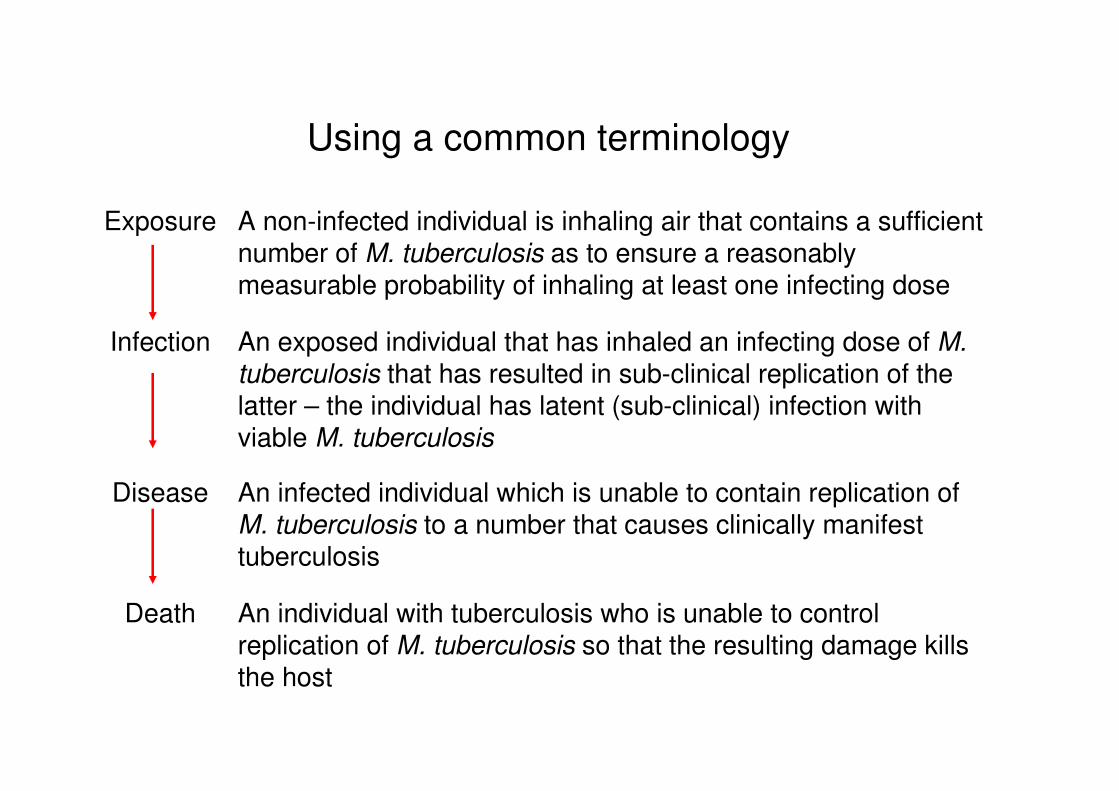
An individual with tuberculosis who is unable to control replication of M. tuberculosis so that the resulting damage kills the host
Death
An infected individual which is unable to contain replication ofM. tuberculosis to a number that causes clinically manifest tuberculosis
Disease
An exposed individual that has inhaled an infecting dose of M. tuberculosis that has resulted in sub-clinical replication of the latter – the individual has latent (sub-clinical) infection with viable M. tuberculosis
Infection
A non-infected individual is inhaling air that contains a sufficient number of M. tuberculosis as to ensure a reasonably measurable probability of inhaling at least one infecting dose
Exposure
Using a common terminology
In tuberculosis pathogenesis,
the incubation period
(between infection and manifest disease)
is not defined
and there is only
partial protective immunity against reinfection

Incident cases of tuberculosis emerge unpredictably fromthe population prevalently infected with M tuberculosis
Population including persons with and without infection with M tuberculosis

Subclinicalinfection
Infectioustuberculosis
Non-infectioustuberculosis
Prophylactictreatment
Preventivetherapy
Chemotherapy
BCGvaccination
Patient's delay
Doctor's delay
Transmission
DeathExposure
Component of the tuberculosis elimination strategy: identification and preventive chemotherapy for persons already infected
Reduction of the prevalence of tuberculous infection
Essence of the tuberculosis control strategy: identification and curative chemotherapy for cases transmitting M. tuberculosis
Reduction of the incidence of tuberculous infection
An Epidemiologic Approach to Tuberculosis Interventions
Mantoux C. La Presse Médicale 1910;2:10-15
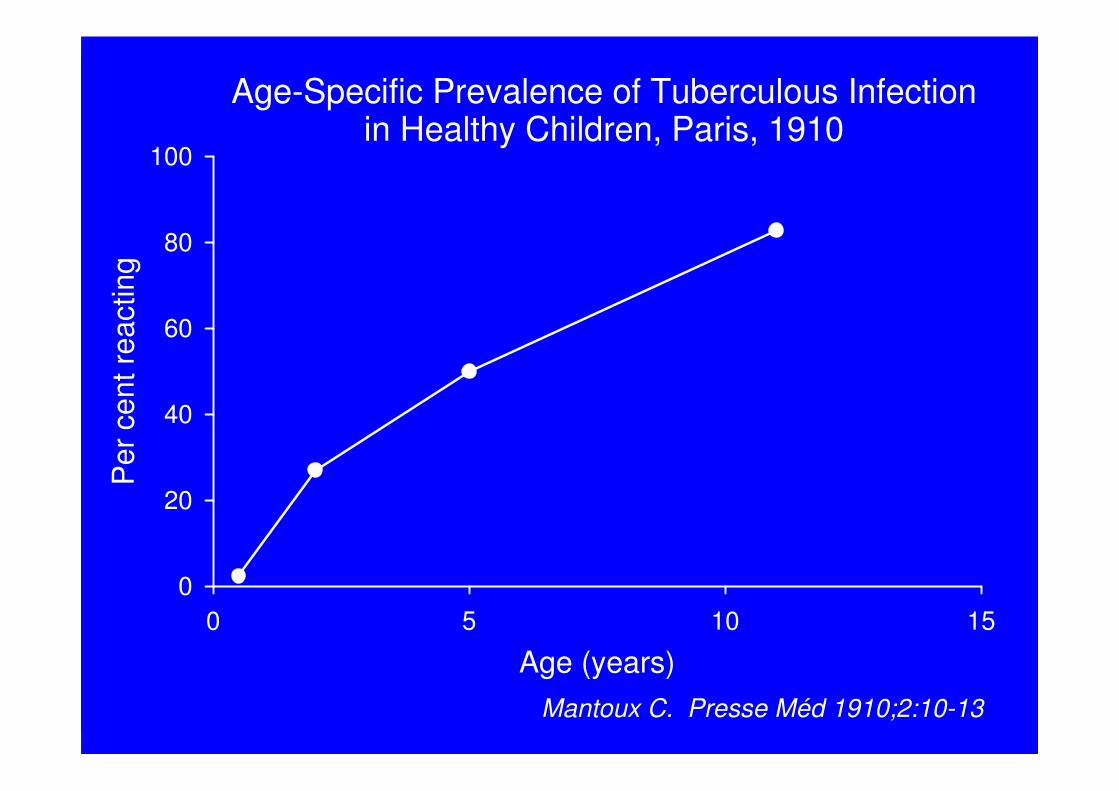
Age-Specific Prevalence of Tuberculous Infectionin Healthy Children, Paris, 1910
Age (years)0 5 10 15
Per
cen
t rea
ctin
g
0
20
40
60
80
100
Mantoux C. Presse Méd 1910;2:10-13

Childhood experience predicts adult experience in every birth cohort!
Andvord K F. Norsk Magasin for Lægevidenskaben 1930;91:642-60
Mortality
Canetti G. Paris: Vigot Frères, 1939, 305 pp
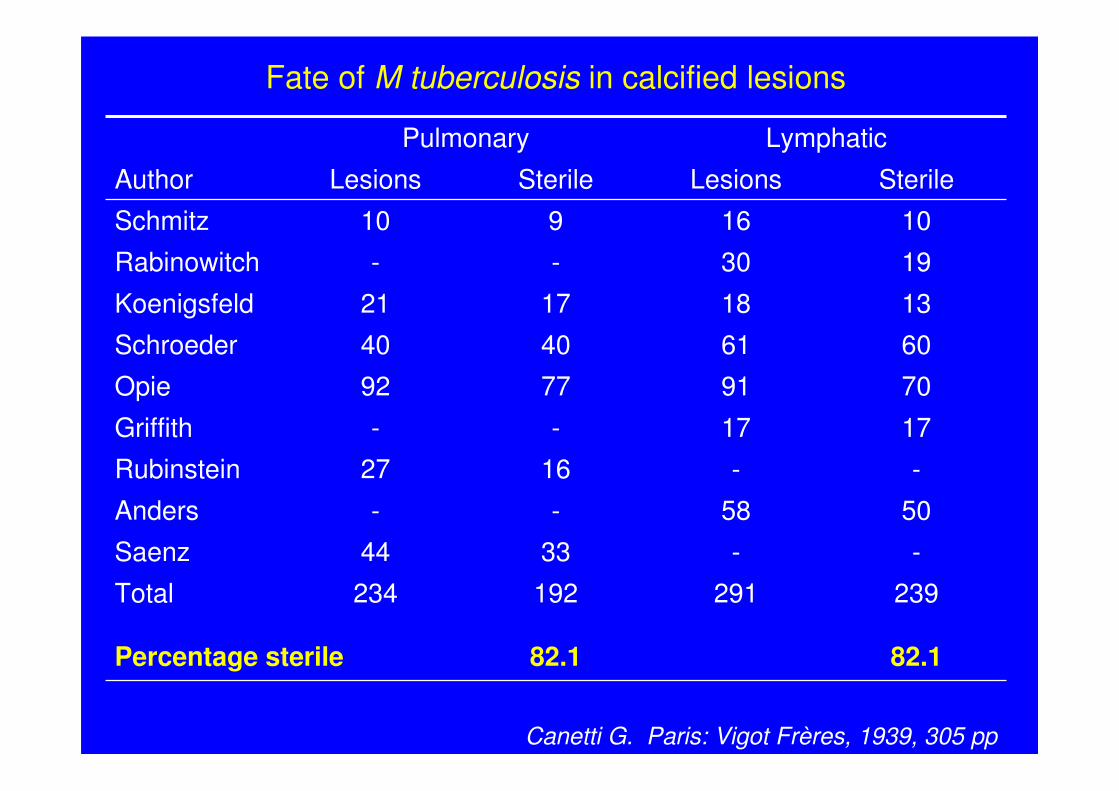
82.182.1Percentage sterile
239291192234Total
--3344Saenz
5058--Anders
--1627Rubinstein
1717--Griffith
70917792Opie
60614040Schroeder
13181721Koenigsfeld
1930--Rabinowitch
1016910Schmitz
SterileLesionsSterileLesionsAuthor
LymphaticPulmonary
Fate of M tuberculosis in calcified lesions

Kristian Andvord’s observation:
A case for prolonged latency with subsequent reactivation,
but….
George Canetti’s findings tell otherwise:
The immune system leads to killing of tubercle bacilli
“Once infected – always infected”:A hypothesis not borne out by facts

Growth of BCG in mice after sub-cutaneous vaccination
Month after BCG vaccination0 1 2 3 4 5
CFU
of B
CG
10
30
50
100
300
500
1000
Lymph nodes
Spleen
Lung
Olsen AW, et al. Scand J Immunol 2004;60:273-77

Protection Afforded by BCG Vaccinationin British School Children During Follow-up
Year of follow-up
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Pro
tect
ion
(%)
0
20
40
60
80
100
D'Arcy Hart P, et al. Br Med J 1977;2:293-5
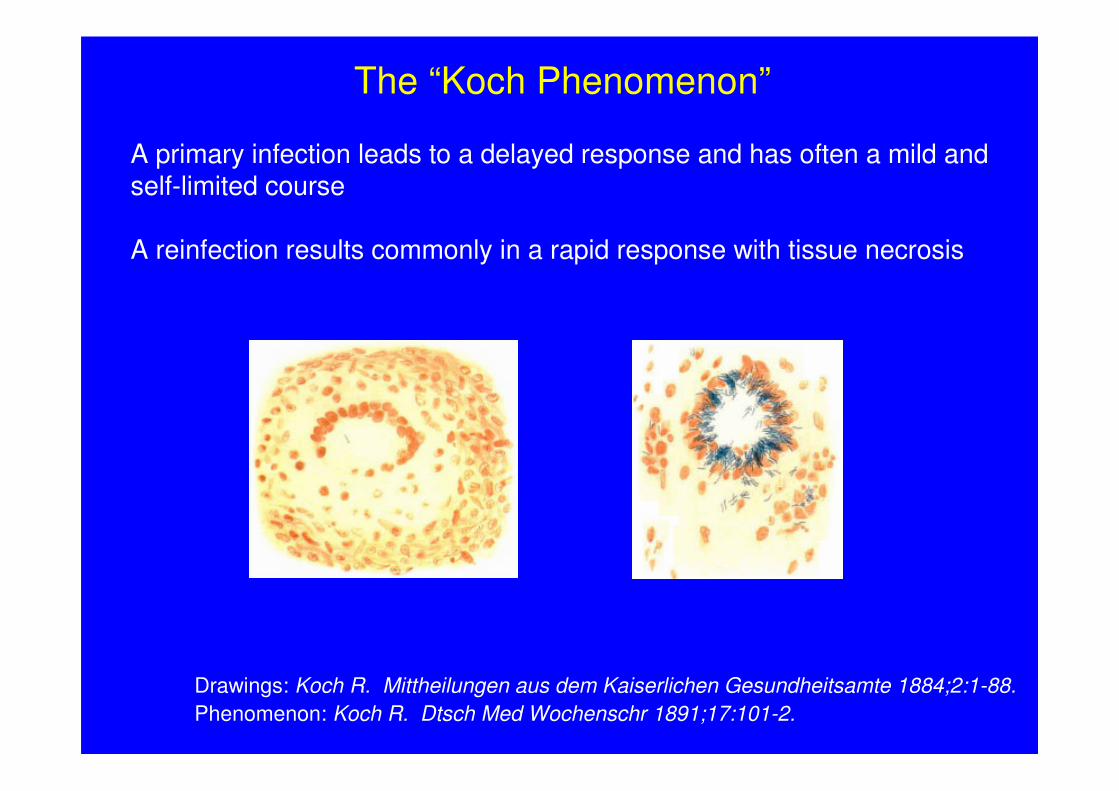
Drawings: Koch R. Mittheilungen aus dem Kaiserlichen Gesundheitsamte 1884;2:1-88.Phenomenon: Koch R. Dtsch Med Wochenschr 1891;17:101-2.
The “Koch Phenomenon”
A primary infection leads to a delayed response and has often a mild andself-limited course
A reinfection results commonly in a rapid response with tissue necrosis
Cross-sectional
Birth cohort
Age
Mor
bidi
ty /
mor
talit
y
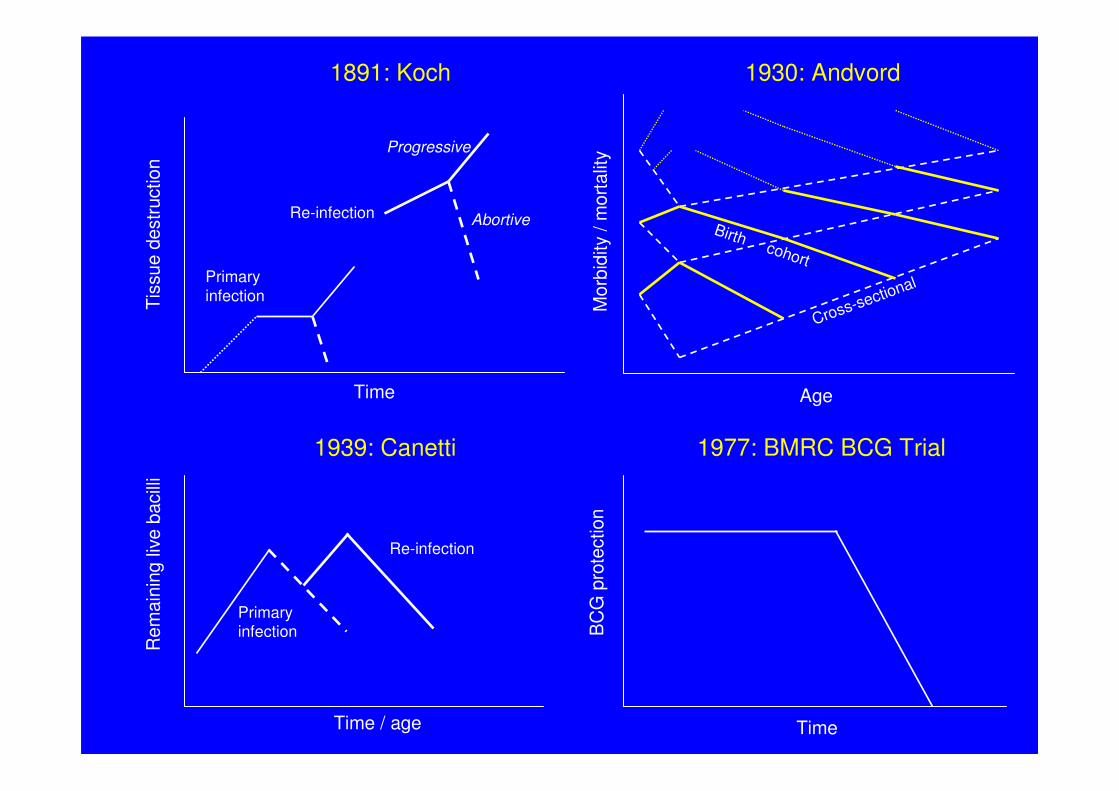
1930: Andvord
Time / age
Rem
aini
ng li
ve b
acill
i
Primaryinfection
Re-infection
1939: Canetti
Time
Tiss
ue d
estru
ctio
n
Primaryinfection
Re-infection
Progressive
Abortive
1891: Koch
Time
BC
G p
rote
ctio
n
1977: BMRC BCG Trial
A positive tuberculin skin test is neither expression of living bacilli nor of protective immunity, it only reflects the immunologic response following prior infection
o
A primed immune system may protect against subsequent re-infection or alternatively results in a severe tissue damaging response
o
A first infection is commonly overcome and frequently ends in the elimination of bacilli but primes the immune system for a decade or more
o
Occam’s razor?
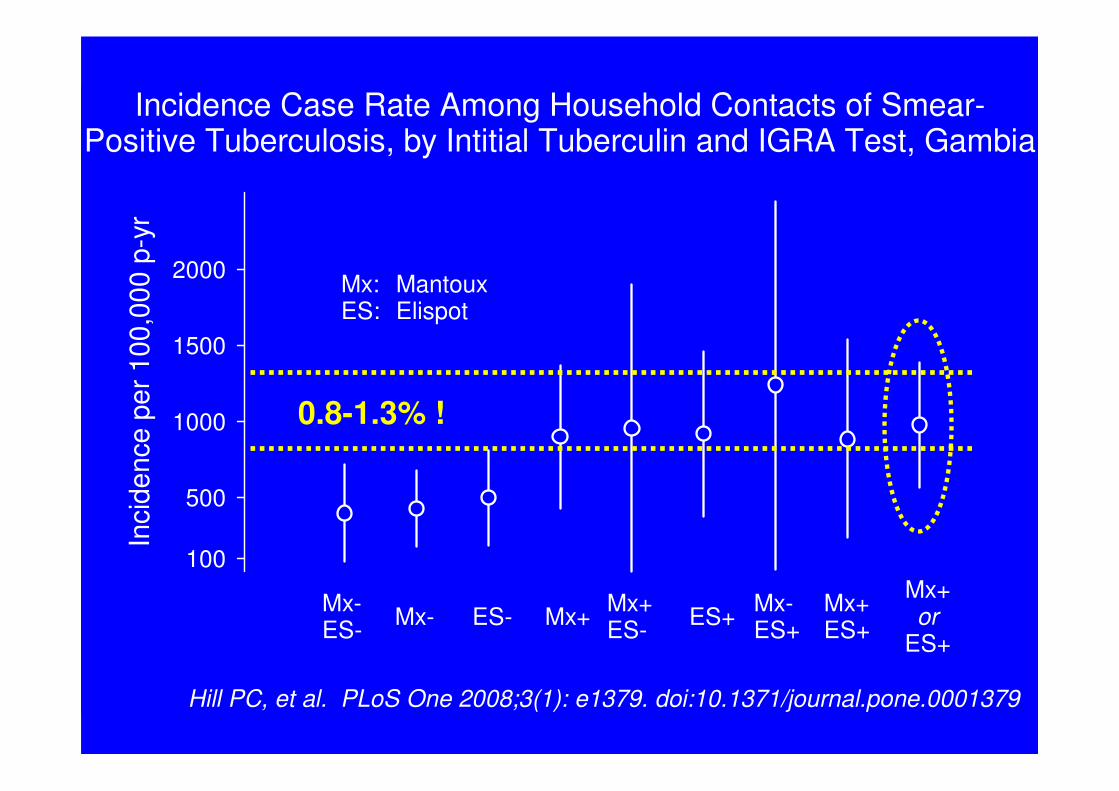
Incidence Case Rate Among Household Contacts of Smear-Positive Tuberculosis, by Intitial Tuberculin and IGRA Test, Gambia
Inci
denc
e pe
r 100
,000
p-y
r
100
500
1000
1500
2000
Mx-ES- Mx- ES- Mx+ Mx+
ES- ES+ Mx-ES+
Mx+ES+
Mx+or
ES+
Hill PC, et al. PLoS One 2008;3(1): e1379. doi:10.1371/journal.pone.0001379
Mx:ES:
MantouxElispot
0.8-1.3% !

A simplified view of a problem:Tuberculin skin test versus IGRAs
Both tests measure the wrong thing,but IGRAs do it more specifically
An immunologic response to mycobacterialantigens acquired in the past does notequate currently live bacilli ready to causedisease (BCG!)

Preventive Therapy for HIV Infected PoliceOfficers in Dar es Salaam, Tanzania
Num
ber o
f per
sons
0
100
200
300
400HIV+
Gotresult
AcceptPT
EvaluatedStarted
INH Adherent
Bakari M, et al. East Afr Med J 2000;77:494-7
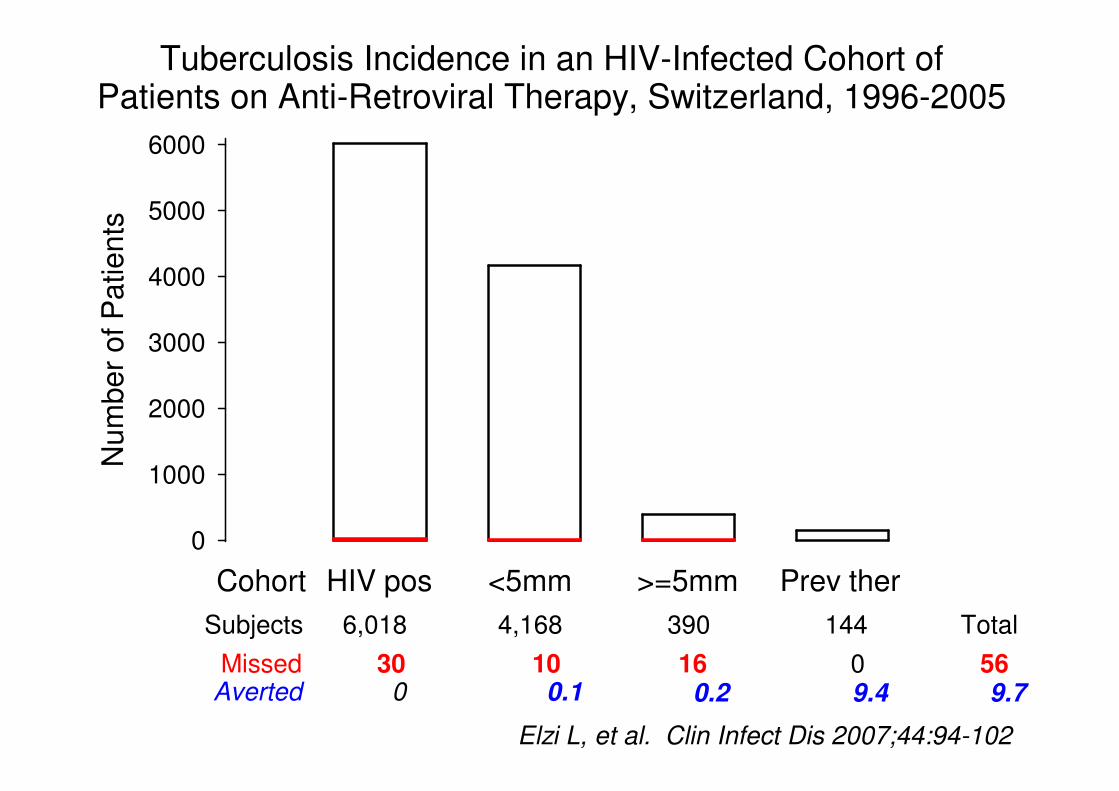
Tuberculosis Incidence in an HIV-Infected Cohort ofPatients on Anti-Retroviral Therapy, Switzerland, 1996-2005
Num
ber o
f Pat
ient
s
0
1000
2000
3000
4000
5000
6000
Missed 30 10 16 0Averted 9.4
Subjects 6,018 4,168 390 144
Cohort HIV pos <5mm >=5mm Prev ther
Elzi L, et al. Clin Infect Dis 2007;44:94-102
0.20.10
Total569.7
Subclinicalinfection
Infectioustuberculosis
Non-infectioustuberculosis
BCGvaccination
Exposure
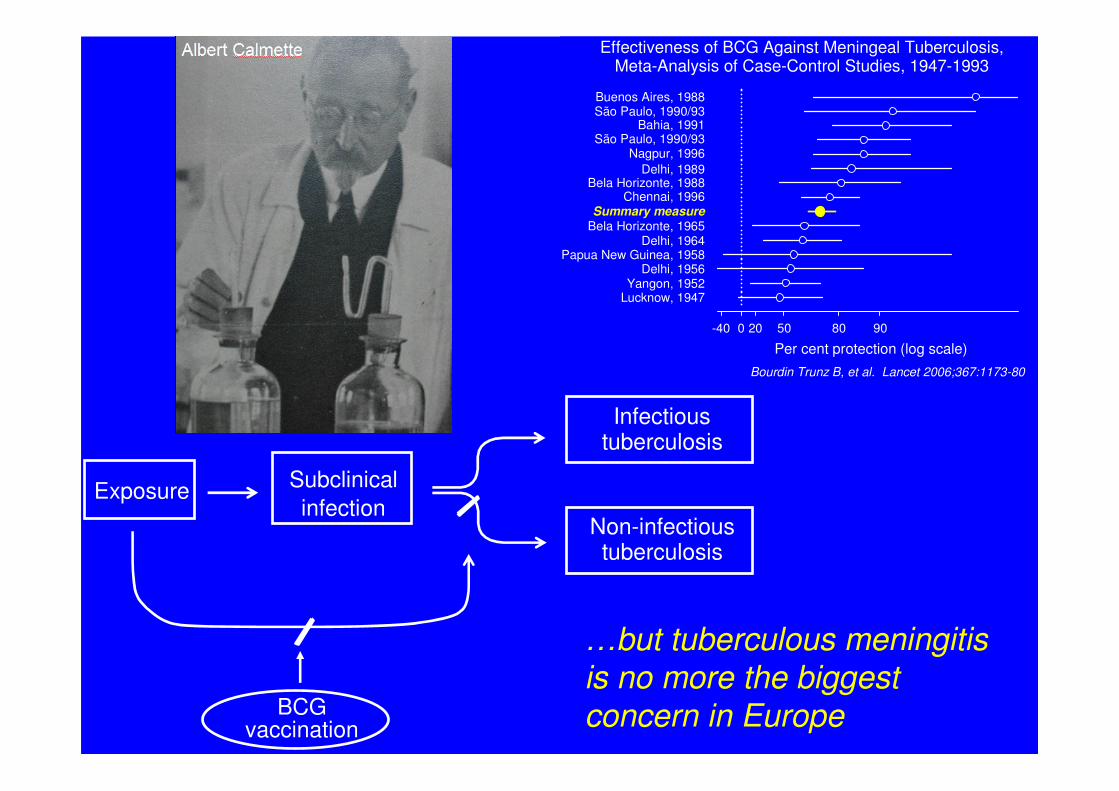
Effectiveness of BCG Against Meningeal Tuberculosis,Meta-Analysis of Case-Control Studies, 1947-1993
Per cent protection (log scale)0-40 50 80 9020
Buenos Aires, 1988
São Paulo, 1990/93
Delhi, 1989Bela Horizonte, 1988
Chennai, 1996Summary measure
São Paulo, 1990/93Bahia, 1991
Nagpur, 1996
Papua New Guinea, 1958
Lucknow, 1947Yangon, 1952
Bela Horizonte, 1965Delhi, 1964
Delhi, 1956
Bourdin Trunz B, et al. Lancet 2006;367:1173-80
…but tuberculous meningitisis no more the biggestconcern in Europe

Subclinicalinfection
Infectioustuberculosis
Non-infectioustuberculosis
Prophylactictreatment
Preventivetherapy
Chemotherapy
BCGvaccination
Patient's delay
Doctor's delay
Transmission
DeathExposure
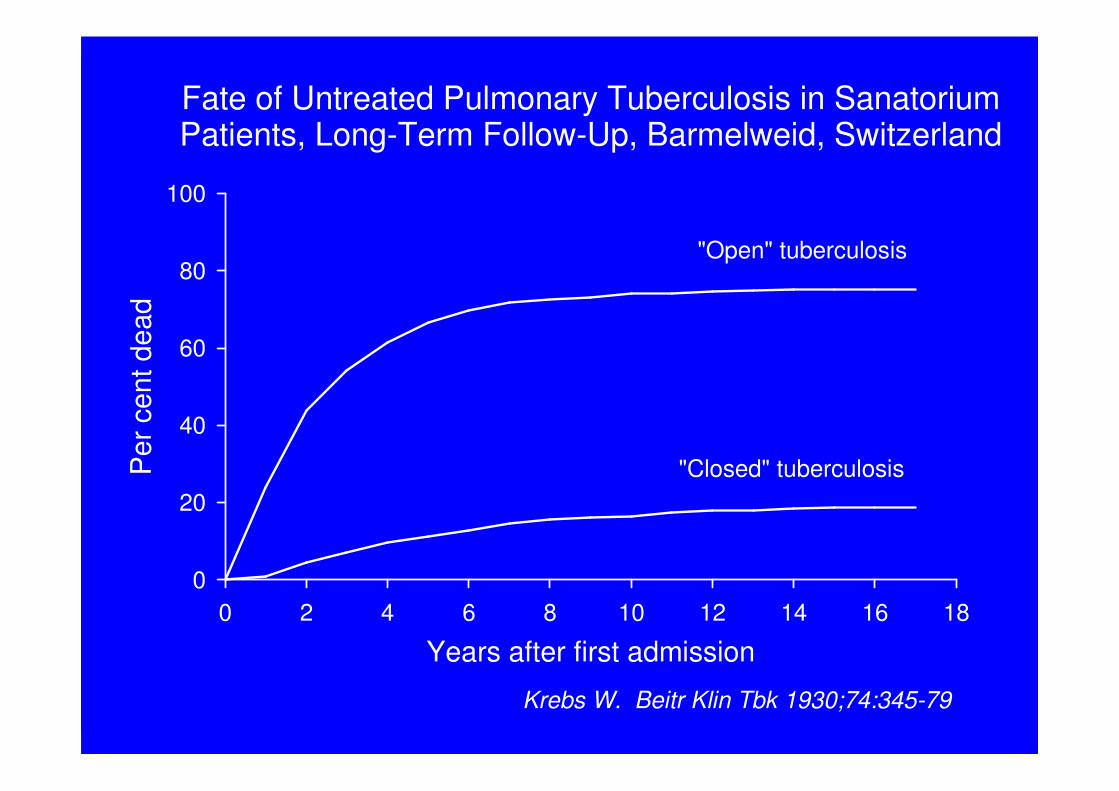
Fate of Untreated Pulmonary Tuberculosis in SanatoriumPatients, Long-Term Follow-Up, Barmelweid, Switzerland
Years after first admission0 2 4 6 8 10 12 14 16 18
Per
cen
t dea
d
0
20
40
60
80
100
"Open" tuberculosis
"Closed" tuberculosis
Krebs W. Beitr Klin Tbk 1930;74:345-79
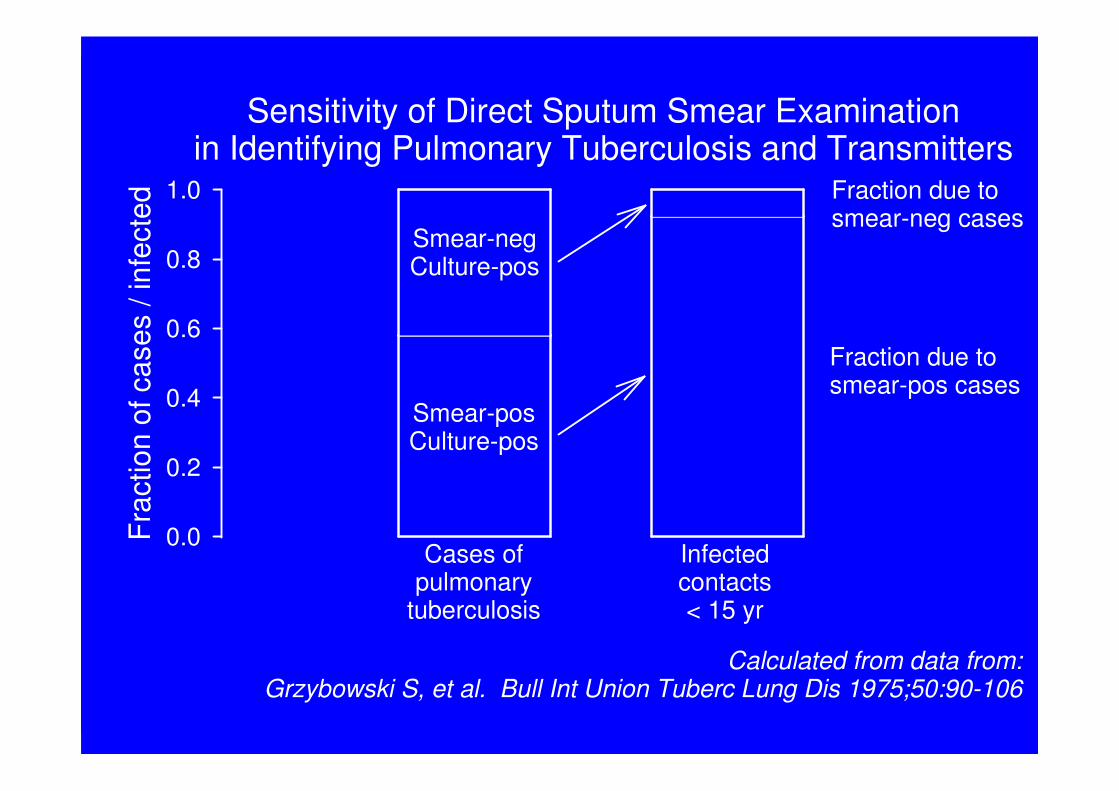
Sensitivity of Direct Sputum Smear Examinationin Identifying Pulmonary Tuberculosis and Transmitters
Frac
tion
of c
ases
/ in
fect
ed
0.0
0.2
0.4
0.6
0.8
1.0
Smear-negCulture-pos
Smear-posCulture-pos
Fraction due tosmear-neg cases
Fraction due tosmear-pos cases
Calculated from data from:Grzybowski S, et al. Bull Int Union Tuberc Lung Dis 1975;50:90-106
Cases ofpulmonary
tuberculosis
Infectedcontacts< 15 yr

0 1 10 100 1000 10.000 100.000 1.000.000AFB per ml of sputum
Freq
uenc
y
X-Ray and clinical (15%)
Poor microscopy (35%)
Excellent microscopy (65%)
PCR (80%)Culture (85%)
Slide courtesy: Van Deun A, November 22, 2007
Schematic Presentation of Relative Frequency of Patients,Number of bacilli, and Available Diagnostic Methods
Improve identification of transmitters:=
Improve microscopy
Improve identification of patients:=
Improve clinical skills

After 2 months chemotherapy After 6 months chemotherapy
Miliary Tuberculosis