EPIDEMIOLOGIC CHALLENGES IN MALIGNANT HYPERTHERMIA (MH) Department of Anesthesiology Children’s...
29
EPIDEMIOLOGIC CHALLENGES IN MALIGNANT HYPERTHERMIA (MH) Department of Anesthesiology Children’s Hospital of Pittsburgh/ University of Pittsburgh Jesus Apuya, MD Barbara Brandom, MD
-
Upload
kimberly-bruce -
Category
Documents
-
view
221 -
download
1
Transcript of EPIDEMIOLOGIC CHALLENGES IN MALIGNANT HYPERTHERMIA (MH) Department of Anesthesiology Children’s...

EPIDEMIOLOGIC CHALLENGES IN MALIGNANT
HYPERTHERMIA (MH)
Department of AnesthesiologyChildren’s Hospital of Pittsburgh/
University of Pittsburgh
Jesus Apuya, MDBarbara Brandom, MD

ACKNOWLEDGEMENTS
• Marilyn Larach
• Sheila Muldoon
• Henry Rosenberg
• Debra Merritt
• Bettina Dixon
• and the Board of Malignant Hyperthermia Association of US

AT A GLANCE...
• Epidemiology of MH• Pathogenesis of MH• 4 Different Case
Scenarios• The MH Clinical
Grading Scale• MH-like Anesthetic
Events
• Mimics of MH• Diseases Associated with MH
• Possibly MH-Related• Rhabdomyolysis but not MH
• Muscle Biopsy & IVCT• MHAUS, NAMHR, NMSIS
& MH Hotline• Bibliography
“Epidemiologic barriers” in defining the true incidence of MH”
• Difficulty in establishing diagnosis of MH
• No noninvasive diagnostic screening test

“Epidemiologic barriers” in defining the true incidence of MH” (cont.)
• All cases are not reported to MH Registry
• Triggering of MH in susceptible patients may not occur
• Lack of uniform criteria for MH diagnosis

Incidence of Different Forms of MH in Relation to Type of Anesthesia
Fulminant MH Abortive MH Overall incidence (all subgroups of suspected MH included)
Total number of anesthetics 1:251,063 1:17,435 1:16,303
General anesthesia 1:221,811 1:15,404 1:14,403
Anesthesia with potent inhalation agent 1:84,488 1:6,653 1:6,167
With succinylcholine 1:61,961 1:4,506 1:4,201
Without succinylcholine 1:174,597 1:20,541 1:18,379
Anesthesia with administration of succinylcholine 1:140,006 1:8,819 1:8,297

Pathogenesis: Key Concepts
• Heterogeneous disorder
• Genetically transmitted with variable expression/penetrance
• Can be triggered by volatile anesthetics and succinylcholine

Hereditary - multiple genes
Several chromosomes:– 19q11.2-13.2 Ryanodine (RyR1)
• Release of Ca2+ stores from sarcoplasmic reticulum
– 17q11.2-q24• Altered sodium channel functioning
– 7q21.1• Dihydropyridine (DHP), voltage sensor for RyR1
– 1q32• CACNL1A3 gene encoding the alpha 1-subunit of the voltage-
gated DHP receptor that interacts with RyR1

Non-specific clinical presentation
• hypercarbia
• tachycardia
• fever
• hyperventilation
• metabolic and respiratory acidoses
• cardiovascular collapse
• rhabdomyolysis

Case One in PACU
A large 13 year old boy underwent
2 hours of uncomplicated halothaneanesthesia.

Case Two in OR
A 10 year-old male was given propofol & mivacurium to facilitate tracheal intubation. Anesthesia was
continued with isoflurane/N2O.

Case Three Masseter Rigidity?
A 16 year-old male who refused spinal anesthesia for lower extremity surgery, was given propofol and succinyl-choline (no potent anesthetic gas).

Case Four Outside
A 12 year old male collapsed after rigorous exercise.
Tobin JR, Jason DR, Nelson TE, Sambuughin. Malignant Hyperthermia and Apparent Heat Stroke N. JAMA 2001; 286(2):168-169 http://jama.ama-assn.org/issues/v286n2/ffull/jlt0711-4.html
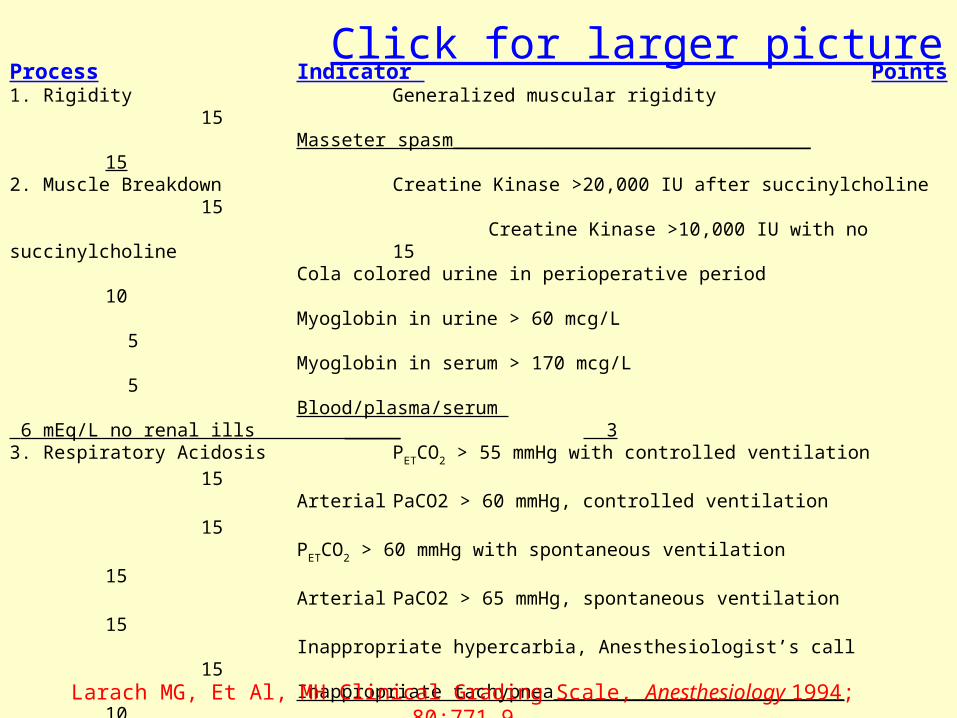
Process Indicator Points1. Rigidity Generalized muscular rigidity 15
Masseter spasm________________________________ 152. Muscle Breakdown Creatine Kinase >20,000 IU after succinylcholine 15
Creatine Kinase >10,000 IU with no succinylcholine 15Cola colored urine in perioperative period 10Myoglobin in urine > 60 mcg/L 5Myoglobin in serum > 170 mcg/L 5Blood/plasma/serum
6 mEq/L no renal ills _____ 33. Respiratory Acidosis PETCO2 > 55 mmHg with controlled ventilation
15 Arterial PaCO2 > 60 mmHg, controlled ventilation 15
PETCO2 > 60 mmHg with spontaneous ventilation 15
Arterial PaCO2 > 65 mmHg, spontaneous ventilation 15
Inappropriate hypercarbia, Anesthesiologist’s call 15Inappropriate tachypnea__________________________ 10
4. Temperature Increase Inappropriately rapid increase 15Inappropriately increased temperature > 38.8C_______ 10
5. Cardiac Involvement Inappropriate sinus tachycardia 3Ventricular tachycardia or fibrillation_________________ 3
6. Family History Positive family history in first degree relative 15 Positive family history, more distant relative ____ 5
7. Others Arterial base excess more negative than –8 mEq/L 10Arterial pH <7.25 10Rapid reversal of MH signs after iv dantrolene 5Positive MH family history with another indicator from the patient’s anesthetic experience other than increased CK 10Elevated CK and a family history of MH______________ 10Larach MG, Et Al, MH Clinical Grading Scale, Anesthesiology 1994; 80:771-9
Click for larger picture

CGS Sum and Probability of MH
Almost certain>50
Very likely35-49
Somewhat greater than likely
20-34

Clinical Grading Scores (CGS)
45303538 SUM
0 0 510Other
0 0 0 0Family History
15 0 0 3Cardiac
15 0 010Temperature
15 015 0Respiratory
0151515Muscle Injury
1515 0 0Rigidity
Case 4Case 3 Case 2Case 1

MH-Like Anesthetic Events
< 14 years 0.000135 Myotonia Dystrophica
12 (4-19) 0.00036 Becker
5 (<16) yrs 0.0020 Duchenne
AGE at DxINCIDENCEMYOPATHY

Differential Diagnosis
+-+++Acidosis
-+/-++Rigidity
++++++ BP
+++++++++ HR
+++++++ ETCO2
PheochromocytomaThyrotoxicosisMH

Some Mimics of MH
• Adverse drug reactions • Arthrogryposis• Carnitine palmitoyl
transferase deficiency• CNS diseases• Contrast media in CSF
• Elevated ETCO2 with laparoscopic cases
• Cystinosis • Glycogen storage
disease• Lymphoma• Mitochondrial disease• Neuroleptic malignant
syndrome• Viral myopathy• William’s syndrome

Diseases Associated with MHS
• Central core disease
• Isolated elevation of creatine kinase
• King Denborough syndrome

Possibly MH Related
• Dystrophinopathy
• Emery Dreifuss MD
• FascioScapuloHumeral MD
• Abnormal Muscle Enzymes
• Ion Channel Mutations– Na, K, Cl

Rhabdomyolysis, but NOT MH
• Brody’s disease• Deficient calcium adenosine triphosphatase
• McArdle’s disease• Myophosphorylase B deficiency

Muscle Biopsy and IVCT
• Nearly 100% sensitive
• 85% specific
Anesthesia for MH Susceptible Patients
• If your patient has had a muscle biopsy for MH contracture testing or is registered through the North American Malignant Hyperthermia Registry (NAMHR):– Call # 888-274-7899– Complete & return report of anesthetic

Bibliography1. Larach, MG for the North American Malignant Hyperthermia Group.
Standardization of the caffeine-halothane muscle contracture test. Anesth Analg 1989; 69:511-515
2. Laboratory diagnosis of malignant hyperpyrexia susceptibility (MHS). European MH Group. Br J Anaesth. 1985; 57(10):1038.
3. European Malignant Hyperpyrexia Group. A protocol for the investigation of malignant hyperpyrexia (MH) susceptibility. Br J Anaesth, 1984; 56: 1267-1269.
4. Allen, G, et al. The sensitivity and specificity of the caffeine-halothane contracture test. Anesthesiology 1998; 88:579-88.
5. Ording, H., et al. In-vitro contracture test for diagnosis of malignant hyperthermia following the protocol of the European MH Group: results of testing patients surviving fulminant MH and unrelated low-risk subjects. The European Malignant Hyperthermia Group. Acta Anesthesiol. Scand., 1997; 41: 955-966.

Bibliography, cont.6. Urwyler A., et.al. Guidelines for molecular genetic dectection of
susceptibility to malignant hyperthermia. And editorial III. Br J Anaesth. 2001; 86(2): 283-7.
7. Brandt, A., et al. Screening of the ryanodine receptor gene in 105 malignant hyperthermia families: novel mutations and concordance with the in-vitro contracture test. Hum. Mol. Genet. 1999; 8: 2055-2062.
8. Brown, R., et al. A novel ryanodine receptor and genotype-phenotype correlation in a large malignant hyperthermia New Zealand Maori pedigree. Hum. Mol. Genet. 2000; 9: 1515-1524.
10. Larach, MG, et al. MH Clinical Grading Scale. Anesthesiology 1994; 80:771-9.
11. Ording, H. Incidence of Malignant Hyperthermia in Denmark. Anesth Analg 1985; 64:700-4.12. Benumof, Jonathan. Muscle Diseases. Anesthesia & Uncommon Diseases. (4/e), Philadelphia, 1998.

Bibliography, cont..
13. Monnier N, et al. Malignant Hyperthermia susceptibility is associated with a mutation of the alpha 1 subunit of the human dihydropyridine-sensitive L-type voltage-dependent calcium channel receptor in skeletal muscle. Am J Hum Genet 1997;60(6):1316-25.
14. Tobin JR, Jason DR, Nelson TE, Sambuughin N. Malignant Hyperthermia and Apparent Heat Stroke, JAMA 2001; 286(2):168-169.
16. Larach, MG, et al. MH Clinical Grading Scale. Anesthesiology 1994; 80:771-9.
17. Dierdorf, Stephen. Anesthesia for Patients with Rare and Coexisting Diseases. Clinical Anesthesia (3/e), Philadelphia, 1996. p 461.
18. McPherson EW, Taylor CA Jr. The King Syndrome: MH, myopathy, and multiple anomalies. Am J Med Genet 8:159, 1981.
19. Loke JC, MacLennan DH. Bayesian modeling of muscle biopsy contracture testing for malignant hyperthermia susceptibility. Anesthesiology 1998;88(3):589-600.







![Malignant hyperthermia [final]](https://static.fdocuments.us/doc/165x107/58ceb1b71a28abb2218b5123/malignant-hyperthermia-final.jpg)