Epatite C, fertilità ed aspetti terapeutici nelle donne · Epatite C, fertilità ed aspetti...
30
Erica Villa Azienda Ospedaliero-Universitaria di Modena, Università di Modena e Reggio Emilia Epatite C, fertilità ed aspetti terapeutici nelle donne Cagliari, 16 settembre 2017 Courtesy of Anne Schreivogl
Transcript of Epatite C, fertilità ed aspetti terapeutici nelle donne · Epatite C, fertilità ed aspetti...

Erica Villa
Azienda Ospedaliero-Universitaria di Modena, Università di Modena e Reggio Emilia
Epatite C, fertilità ed aspetti terapeutici nelle
donne
Cagliari, 16 settembre 2017
Courtesy of
Anne Schreivogl

Summary
Fertility in CLD
The HCV model: reproductive factors and
fertility
Clinical study
Epidemiological studies
Therapeutic options
Fertility in women with chronic liver disease
Sex hormone disturbances are common in women with CLD
They are mainly due to the abnormality of the physiology of the
hypothalamic-pituitary-gonadal axis and to the etiology of liver
disease.
In women with cirrhosis, chronic anovulation is a common problem,
and it is manifested as secondary amenorrhea, oligomenorrhea, or
irregular episodes of metrorrhagia.
LT leads to partial improvements in both sex hormone levels and
sexual function.
Women achieve normal menstruation and fertility a few months after
transplantation
Gavaler JS.. Recent Dev Alcohol 1995;12:199–208.Mass K, et al. Transplantation 1996;62:476–479; Madersbacher S et al. Clin
Endocrinol (Oxf) 1996;44:461–466; Parolin M et al Transpl Proc 2004;36:943–944.; Burra et al. Liver Ttanspl 2013; 19: 122-131; Burra
P. Liver Transpl 2009;15:S50–S56.

Reproductive factors and liver disease in HCV+
women
Response to antiviral therapy with IFN-based therapies is
much lower in menopausal women
Progression of fibrosis in slower in women in fertile age
Course of CLD is greatly accelerated by menopause
HCC risk after menopause becomes equivalent to that found
in males
Shimizu et al Liver 2001 ; Di Martino et al. Hepatology 2004; Codes et al. Gut 2007; Villa et al. Plos1
2012; Villa et al Gastroenterology 2011; Villa et al. JMV 2012

Mean serum levels of Anti-Mullerian Hormone levels in
HCV-positive women divided according to reproductive
phases
Plos1 2012, Karampatou et al. J Hep 2017
Reproductive Pre-menopausal Early Menop Late Menop
P<0001
Controls HCV+
< 40 anni
> 40 anni
No
Yes Menopause
Controls HCV+
HCV-positive women

Patients
Study groups:
Clinical group:
100 Hepatitis C Virus-positive women with CLD
50 Hepatitis B Virus-positive women CLD
100 healthy women without CLD matched by age
Two external validation group,
the Italian Platform for the Study of Viral Hepatitis
Therapies (PITER) cohort
a US insurance database

Age,
reproductive status,
serum levels of AMH were collected for all 3 groups.
The following additional data were collected for the HCV+ and HBV+ groups:
• virus genotype (HCV),
• body mass index (BMI),
• estrogen level,
• insulin-like growth factor-1 (IGF-1) level,
• presence of steatosis on ultrasound,
• liver stiffness
• histologic features,
• antiviral treatment and response,
• parity,
• age at first full-term pregnancy,
• and occurrence and number of spontaneous miscarriage(s)
Clinical group
Clinical and Laboratory Assessments

Characteristic HCV+
group (n = 100)
HBV+ group
(n = 50)
P value Age (y) 37.2 ± 8.5 35.1 ± 8.0 .209
Duration of HCV infection (y) 12 ± 7 12 ± 8 .972
Platelet count (×103/mm
3) 219 ± 70 202 ± 65 .144
Alanine aminotransferase (IU/L) 79 ± 30 89 ± 65 .305
Gamma-glutamyl transferase (IU/L) 35 ± 21 29 ± 22 .113
Cholesterol (mg/dL) 179 ± 50 189 ± 45 .219
Triglyceride (mg/dL) 99 ± 35 85 ± 55 .105
Ferritin (ng/mL) 89 ± 30 77 ± 54 .148
Blood glucose (mg/dL) 75 ± 22 80 ± 25 .233
HOMA 1.7 ± 1.5 1.5 ± 1.0 .715
Mean BMI (kg/m2) 23.6 ± 5.0 23.2 ± 4.6 .637
HCV genotype 1/2/3/4, n 56/15/21/8 NA
Grade of inflammation 3.6 ± 1.5 5.2 ± 0.5 .001
Stage 1.8 ± 1.3 2.4 ± 1.1 .043
Presence of steatosis, n (%) 40 (40) 10 (20) .014
Stiffness (kPa) 6.0 ± 3.0 5.7 ± 2.0 .468
Data are reported as the mean ± SD, unless otherwise noted. NA, not available.
Baseline Characteristics of Study Participants
Karampatou et al J Hep 2017

Hormonal and Reproductive Characteristics of Study
Participants
Characteristic HCV+
(n =
100)
HBV+
(n = 50)
Controls
(n = 100)
P, I vs. II P, I vs. III P, II vs. III
AMH, all women (ng/ml) 3.2 ± 3.1 2.8 ± 1.7 4.3 ± 2.5 .548 .0009 <.0001
AMH, 20–30 y (ng/ml) 3.4 ± 2.2 3.6 ± 1.4 5.5 ± 1.3 .271 <.0001 <.0001
AMH < 0.16 ng/ml, n (%) 34 (34) 2 (4)
6 (6) <.0001 <.0001 .6073
Estradiol (ng/ml) 77 ± 58 87 ± 33 86 ± 49 .219 .410 .8827
IGF-1 (ng/ml) 110 ± 58 126 ± 60 NA .145 - -
Parity, n (%) 52 (52) 21 (42) NA .248 - -
Age at first pregnancy (y) 30 ± 6 27 ± 7 NA .235 - -
History of miscarriage, n
(%)
35 (35) 4 (8) NA .0004 - -
History of miscarriage and AMH < 2.47 ng/ml, n
24 1 NA .0076 - -
History of multiple miscarriages
8 1 NA .1447 - -
Karampatou et al J Hep 2017

0
10
20
30
40
50
60
Pregnancies Miscarriages
HCV
HBV
Relative proportion of pregnancies and miscarriage in
HCV+ and HBV+ women
%
52 21 35 4
P=.001
Karampatou et al J Hep 2017

0
5
10
15
20
25
30
<2.47 ng/ml >2.47 ng/ml
HCV
HBV
Occurrence of miscarriages and median AMH level among
HCV+ and HBV+ women
P = .0049
24 111 3
Karampatou et al J Hep 2017

Relationship between circulating IGF-1 levels and AMH levels (A),
liver stiffness (B), grade of inflammation (C), and degree of fibrosis
(D) in HCV+ and HBV+ women

Data from the PITER HCV Cohort Study

273 women (42.0%) had a history of miscarriage
122/273 (44.6%) had a history of multiple
miscarriages: 71 women (26.0%) had 2 miscarriages,
26 women (0.9%) had 3 miscarriages,
5 women (1.8%) had 4 miscarriages,
4 women (1.4%) had 5 miscarriages,
2 women (0.7%) had 6 miscarriages,
2 women (0.7%) had 7 miscarriages,
1 woman (0.36%) had 8 miscarriages
Data on miscarriage available in 650 HCV+ women
Data from the PITER HCV Cohort Study
Karampatou et al J Hep 2017

Data from the PITER HCV Cohort Study
590 HCV+ women
between 15 and 49 years of age
HCV+ women
Total fertility rate
Whole Italian population
of the same age range 1.37
0.7
Karampatou et al J Hep 2017

Data from the US Insurance Cohort Study

HCV/HIV Infection No HCV/HIV Infection
Women with HCV and /or HIV diagnosisN=111,043
Women without HCV or HIV diagnosisN=30,733,127
Continuous plan ≥1 year post-index dateN=76,264
Continuous plan ≥1 year post-index date N=11,560,535
Continuous plan ≥9 months pre-index date N=35,570
Continuous plan ≥9 months pre-index date N=6,967,045
Women aged 18–45N=16,895
Women aged 18–45N=3,041,048
Cases: 13,264 Controls: 39,792
Only HCVN=9,010
HIV/HCVN=398
1:3 match
Only HIVN=7,487
Sample Selection: Infertility Analysis

0,2
0,3
1,4
3,3
2,4
2,5
6,2
8,7
15,8
27,2
1,4
1,9
2,9
5,3
5,5
11,3
11,9
20,5
26,3
35,3
2,3
1
7,9
2,3
3,6
5,3
9,5
23,3
30,8
28,9
0 5 10 15 20 25 30 35 40
Renal diseases
Alcohol abuse
Ovary dysfunction
Obesity
Diabetes
Drug abuse
Hypertension
Hematologic diseases
Metabolic diseases and immunity disorders
Diseases of the circulatory system
Patients, %
HIV/HCV HCV No HCV
Comorbidities of Women in Infertility Analysis
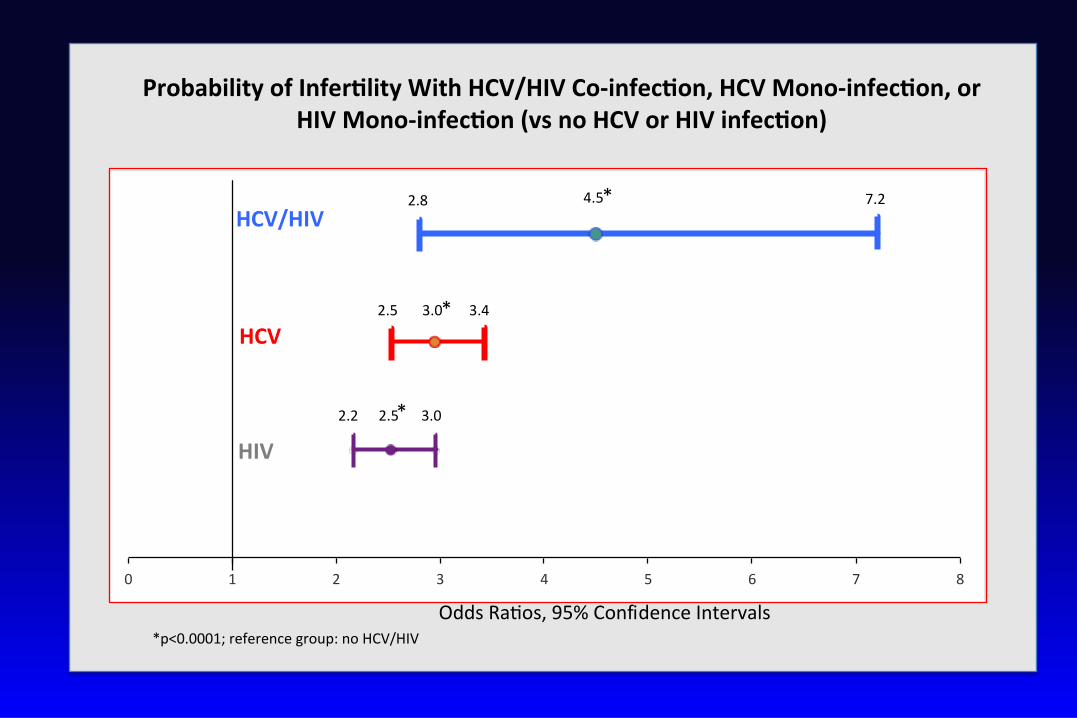
ProbabilityofInfer lityWithHCV/HIVCo-infec on,HCVMono-infec on,orHIVMono-infec on(vsnoHCVorHIVinfec on)
*p<0.0001;referencegroup:noHCV/HIV
4.52.8 7.2
3.02.5 3.4
2.52.2 3.0
0 1 2 3 4 5 6 7 8
HCV
HCV/HIV
HIV
*
*
*
OddsRa os,95%ConfidenceIntervals

Pregnant Women (N=2,647,993)
Women with continuous plan ≥6 months before and ≥1 year after index date N=880,058
Women without HIVN=875,975
HCV-infected womenN=3,198
Women without HCVN=872,777
Aged 18–45N=1,226
Cases: 1,225 Controls: 12,2501:10 match
HCV diagnosis before pregnancyN=1,512
Aged 18–45N=822,046
Sample Selection: Pregnancy Outcomes Analysis


Adjusted results- pregnancy outcomes
Outcomes Odds ratio Confidence Interval
Premature birth 1.336 1.059 1.685
Live birth 0.754 0.622 0.913
Stillbirth 1.252 0.491 3.188
Gestational diabetes 1.240 1.019 1.510
Pre-eclampsia 1.206 0.935 1.556
Miscarriage 1.106 0.885 1.383
• Adjusted results are consistent with unadjusted results.
• Premature and live birth results are significant.
Data from the US Insurance Cohort Study

Therapeutic options

AMH Levels and Response to IFN-based Antiviral Therapy
75 HCV+ women (36 ± 8 years) underwent antiviral treatment, all
with Peg IFN/R, associated with Telaprevir (n=2) or Boceprevir (n=6).
Mean age at therapy was 36±8 years.
SVR was achieved in 53 women (70.6%).
0
10
20
30
40
50
60
70
80
AMH<0.16ngml AMH>0.16 ng/ml
SVR
%
10/19 44/56
P = .030
Karampatou et al J Hep 2017
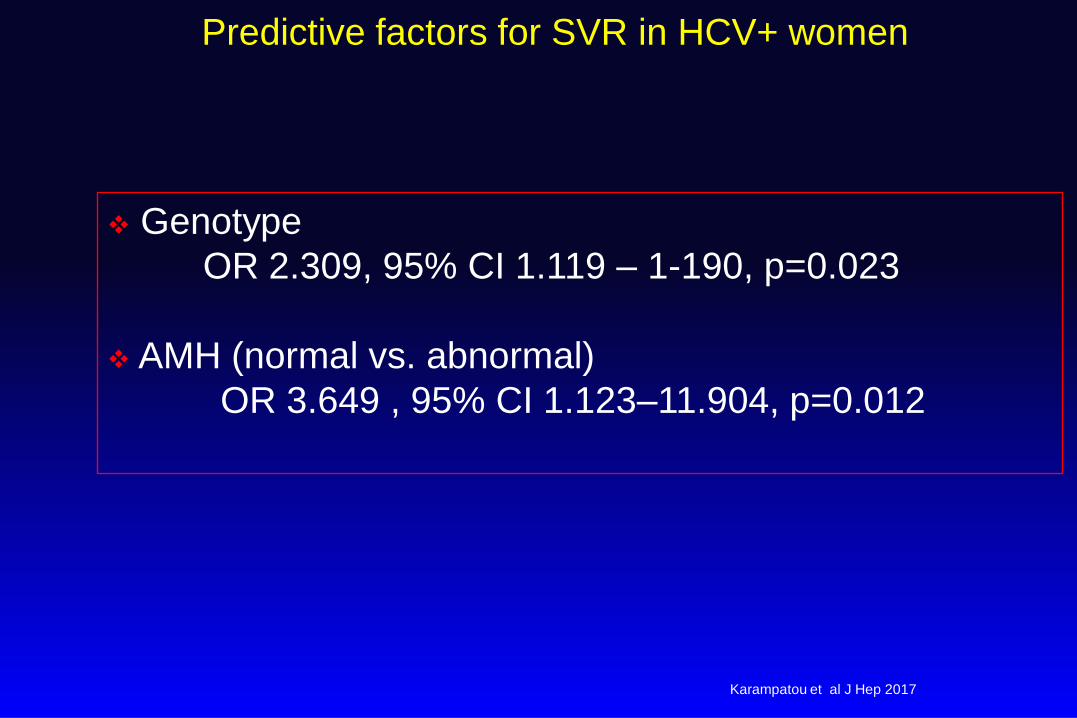
Predictive factors for SVR in HCV+ women
Genotype
OR 2.309, 95% CI 1.119 – 1-190, p=0.023
AMH (normal vs. abnormal)
OR 3.649 , 95% CI 1.123–11.904, p=0.012
Karampatou et al J Hep 2017

0
10
20
30
40
50
60
70
Miscarriage rate
SVR
No SVR
%
Response to Antiviral Therapy and Rate of
Miscarriage
17/53 14/22
P= .0102
Karampatou et al J Hep 2017

Prospective study of 3D in F0-F3 young (<35
years) HCV+ gt 1 or 4 women
Primary objective
The modification of AMH levels before and after successful
antiviral therapy in comparison with age-matched HCV-
positive women not undergoing antiviral treatment is the
primary endpoint.
Secondary objective
• Modification of the Estradiol (E2) levels
• Occurrene of miscarriage during the observation period
post-therapy.

Summary
In women with Hepatitis C infection, ovarian
senescence occurs early and negatively influences
reproductive function and response to therapy
Both prospective and cohort-based data indicate that
HCV+ women have strikingly impaired fertility and high
rate of miscarriages.
The role of antiviral therapy with DAA in reversing
ovarian senescence and improving fertility should be
explored.


WomenInHepatology
Courtesy of Anne Shreivogl
GENDER-C Project
Gastroenterology, Modena
Barbara Lei Mariagrazia Del Buono Veronica Bernabucci Filippo Schepis Anna Ferrari
Stefano Gitto Ranka Vukotic Aimilia Karampatou
Lab
Rosina Critelli Elena Turola Fabiola Milosa Francesca Faillaci, Rosario Condello
Pathology, AOU, Modena
Luisa Losi, Livia Maccio
Clinical Pathology, NOCSAE, Modena
Tommaso Trenti Enrica Baraldi Simonetta Tagliavini Annamaria Cenci
Istituto Superiore di Sanità
Loreta Kondili, Stefano Rosato, Stefano Vella and Piter Investigators: A. Craxi, S.Petta, V. Calvaruso (University Paolo Gioaccone Palermo); L. Chessa, M.C.Pasetto (University of Cagliari); E. Bigliotti, F. Tamburini (Sapienza University of
Rome); G. Montalto, A.R. Capitano (University Paolo Giaccone Palermo); D. Ieluzzi, G.Fattovich, S, Storato (University of Verona); A. L. Zignego ; M. Monti, L. Gragnani
(University of Florence); M. Zuin, E. Finati, A.Giorgini ( San Paolo Hospital Milano); G Angarano, M. Milella (University of Bari); F.Alessandro, M Dallio, C. Loguercio (2
nd University of Naples);G. Mazzella, G.Lazzarini, M Di Fine (University S. Orsola Malpighi, Bologna); F.P.Russo, I. Franceschet (Padua Hospital); F.Castelli, S. Zaltron
(Spedali Civili Brescia); G.Raimondo, R. Filomia , G.Martino University, Messina); M Puoti, E. Danieli (Niguarda Cà-Granda Hospital, Milano) M.Strazzabosco, M Gemma
(S. Gerardo, Hospital, Monza); M. Angelico, F. De Leonardis (Tor Vergata University, Rome); A. Gori, E. Cappelletti (S.Gerardo Hospital, Monza); R. Bruno S.Cima (S.
Matteo IRCCS, Pavia); C.Coppola, D.C Amoruso (Gragnano Hospital Napoli); P. Andreone, G.Simonetti (Sant’Orsola Malpighi University , Bologna); GB. Gaeta, V.Rizzo
(2 nd University Napoles); P. Toniutto, D.Dissegna (University of Udine); M.Mondelli S.Ludovisi (S. Matteo IRCCS, Pavia); M Persico, M.Masarone (G.da Procida
Hospital Salerno); C.Torti, A.Strazzulla (University Hospital Mater Domini, Catanzaro); F.Rosina,L.Framarin (Local Health District, Gradenigo, Torino); Maria Giovanna
Quaranta, Loredana Falzano, Alessandra Mallano (Istituto Superiore di Sanità).
★
The two meetings were held in Modena during the Women in Hepatology Meeting in May 2014 and in Naples during the AISF
Monothematic Conference in October 2014.
The Position Paper was generated by the Gender Committee of the Italian Association for the Study of the Liver (AISF) to provide an
official position paper in a setting characterized by uncertain clinical behavior and lack of uniform approach.
Digestive and Liver Disease 48 (2016) 120–137
★ Filomena Morisco, Raffaele Bruno, Elisabetta Bugianesi, Patrizia Burra,Vincenza Calvaruso, Alice Cannoni, Nicola Caporaso, Gian Paolo Caviglia,Alessia
Ciancio, Silvia Fargion, Alessandro Federico, Annarosa Floreani,Giovanni Battista Gaeta, Maria Guarino, Pietro Invernizzi, Anna Licata,Carmela Loguercio,
Giuseppe Mazzella, Felice Petraglia, Massimo Primignani,Kryssia Rodriguez-Castro, Antonina Smedile, Luca Valenti, Ester Vanni, SilviaVannuccini, Chiara
Voltolini,
★
Malattie Infettive, Università La Sapienza Gloria Taliani