Enteric Gram Negative Rods

of 14
Transcript of Enteric Gram Negative Rods
-
8/13/2019 Enteric Gram Negative Rods
1/14
The Enterobacteriaceae are a large, heterogeneous groupof gram-negative rods whose natural habitat is theintestinal tract of humans and animals. The familyincludes many genera (escherichia, shigella, salmonella,enterobacter, klebsiella, serratia, proteus, and others).Some enteric organisms, eg, Escherichia coli, are part ofthe normal flora and incidentally cause disease, while
others, the salmonellae and shigellae, are regularly path-ogenic for humans. The Enterobacteriaceae are faculta-tive anaerobes or aerobes, ferment a wide range of car-bohydrates, possess a complex antigenic structure, andproduce a variety of toxins and other virulence factors.Enterobacteriaceae, enteric gram-negative rods, andenteric bacteria are the terms used in this chapter, butthese bacteria may also be called coliforms.
CLASSIFICATIONThe Enterobacteriaceae are the most common group ofgram-negative rods cultured in the clinical laboratoryand along with staphylococci and streptococci areamong the most common bacteria that cause disease.
The taxonomy of the Enterobacteriaceae is complex andrapidly changing since the introduction of techniquesthat measure evolutionary distance, such as nucleic acidhybridization and sequencing. More than 25 genera and110 species or groups have been defined; however, theclinically significant Enterobacteriaceae comprise 2025species, and other species are encountered infrequently.In this chapter, taxonomic refinements will be mini-mized, and the names commonly employed in the med-ical literature will generally be used. A comprehensiveapproach to identification of the Enterobacteriaceae ispresented in Chapters 41, 42, and 44 of Murray PR et al(editors):Manual of Clinical Microbiology, 8th ed. ASMPress, 2003.
The family Enterobacteriaceae have the following
characteristics: They are gram-negative rods, eithermotile with peritrichous flagella or nonmotile; theygrow on peptone or meat extract media without theaddition of sodium chloride or other supplements; grow
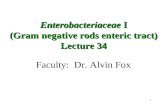
well on MacConkeys agar; grow aerobically and anaero-bically (are facultative anaerobes); ferment rather thanoxidize glucose, often with gas production; are catalase-positive, oxidase-negative, and reduce nitrate to nitrite;and have a 3959% G + C DNA content. Examples ofbiochemical tests used to differentiate the species ofEnterobacteriaceae are presented in Table 161. There
are many others in addition to the ones listed. In theUnited States, commercially prepared kits are used to alarge extent for this purpose.
The major groups of Enterobacteriaceae aredescribed and discussed briefly in the following para-graphs. Specific characteristics of salmonellae, shigellae,and the other medically important enteric gram-nega-tive rods and the diseases they cause are discussed sepa-rately later in this chapter.
Morphology & Identification
A. TYPICAL ORGANISMS
The Enterobacteriaceae are short gram-negative rods.Typical morphology is seen in growth on solid media invitro, but morphology is highly variable in clinical spec-imens. Capsules are large and regular in klebsiella, lessso in enterobacter, and uncommon in the other species.
B. CULTURE
E coliand most of the other enteric bacteria form circu-lar, convex, smooth colonies with distinct edges. Enter-obacter colonies are similar but somewhat moremucoid. Klebsiella colonies are large and very mucoidand tend to coalesce with prolonged incubation. Thesalmonellae and shigellae produce colonies similar to Ecolibut do not ferment lactose. Some strains of E coliproduce hemolysis on blood agar.
C. GROWTH CHARACTERISTICS
Carbohydrate fermentation patterns and the activity ofamino acid decarboxylases and other enzymes are usedin biochemical differentiation (Table 161). Some tests,eg, the production of indole from tryptophan, are com-
248
Enteric Gram-Negative
Rods (Enterobacteriaceae) 16
4010_1-16 2/11/04 9:28 AM Page 248
-
8/13/2019 Enteric Gram Negative Rods
2/14
D-SorbitolFermentation
L-ArabinoseFermentation
RaffinoseFermentation
L-RhamnoseFermentation
D-XyloseFermentation
MelibioseFermentation
Citrobacterfr
eundii
5
100
0
95
80
70
0
0
65
20
95
0
100
95
50
30
99
55
0
98
100
30
99
99
50
Enterobacter
aerogenes
0
5
98
95
0
2
0
98
0
98
97
0
100
100
95
100
100
5
98
100
100
96
99
100
99
Escherichiacoli
98
99
0
1
1
1
0
90
17
65
95
0
100
95
95
50
98
60
5
94
99
50
80
95
75
Klebsiellapneumoniae
0
10
98
98
0
95
0
98
0
0
0
0
100
97
98
99
99
30
90
99
99
99
99
99
99
Klebsiellaoxy
toca
99
20
95
95
0
90
1
99
0
0
0
0
100
97
100
100
99
55
99
99
98100
100
100
99
Morganellam
organii
98
97
0
0
5
98
95
0
0
98
95
0
100
90
1
0
0
0
0
0
0
0
0
0
0
Proteusmirabilis
2
97
50
65
98
98
98
0
0
99
95
90
100
96
2
15
0
0
0
0
0
1
1
98
0
SalmonellaC
holeraesuis
0
100
0
25
50
0
0
95
55
100
95
0
100
95
0
0
98
5
0
90
0
1
100
98
45
SalmonellaTyphi
0
100
0
0
97
0
0
98
3
0
97
0
100
0
1
0
100
0
0
99
2
0
0
82
100
Salmonella,mostserotypes
1
100
0
95
95
1
0
98
70
97
95
0
100
96
1
1
100
96
0
95
99
2
95
97
95
Serratiamarc
escens
1
20
98
98
0
15
0
99
0
99
97
90
100
55
2
99
99
0
40
99
0
2
0
7
0
Shigellasonn
ei
0
100
0
0
0
0
0
0
2
98
0
0
100
0
2
1
99
0
0
2
95
3
75
2
25
Sdysenteriae
,Sflexneri,S
boydii
50
100
0
0
0
0
0
0
5
1
0
0
100
2
0
0
93
2
0
30
60
50
5
2
50
1Adaptedfrom
FarmerJJIIIetal:Biochemicalidentificationofnew
speciesandbiogroupsofEnterobacteriaceaeisolatedfrom
clinicalspecime
ns.J
ClinMicrobiol
1984;21:46.
IndoleProduction
MethylRed
Voges-Proskauer
SimmonsCitrate
HydrogenSulfide
UreaHydrolysis
PhenylalanineDeaminase
LysineDecarboxylase
ArginineDihydrolase
OrnithineDecarboxylase
Motility(36C)
GelatinHydrolysis(22C)
D-Glucose,Acid
D-Glucose,Gas
LactoseFermentation
SucroseFermentation
D-MannitolFermentation
DulcitolFermentation
AdonitolFermentation
Table161
.
Examplesofbiochemicalreactionsof
selectedentericgram-negativerods.1
4010_1-16 2/11/04 9:28 AM Page 249
-
8/13/2019 Enteric Gram Negative Rods
3/14
monly used in rapid identification systems, while others,eg, the Voges-Proskauer reaction (production of acetyl-methylcarbinol from dextrose), are used less often. Cul-ture on differential media that contain special dyesand carbohydrates (eg, eosin-methylene blue [EMB],MacConkeys, or deoxycholate medium) distinguisheslactose-fermenting (colored) from non-lactose-ferment-ing colonies (nonpigmented) and may allow rapid pre-sumptive identification of enteric bacteria (Table 162).
Many complex media have been devised to help inidentification of the enteric bacteria. One such mediumis triple sugar iron (TSI) agar, which is often used tohelp differentiate salmonellae and shigellae from otherenteric gram-negative rods in stool cultures. Themedium contains 0.1% glucose, 1% sucrose, 1% lac-tose, ferrous sulfate (for detection of H2S production),tissue extracts (protein growth substrate), and a pHindicator (phenol red). It is poured into a test tube toproduce a slant with a deep butt and is inoculated by
stabbing bacterial growth into the butt. If only glucoseis fermented, the slant and the butt initially turn yellowfrom the small amount of acid produced; as the fermen-tation products are subsequently oxidized to CO2 andH2O and released from the slant and as oxidative decar-boxylation of proteins continues with formation ofamines, the slant turns alkaline (red). If lactose orsucrose is fermented, so much acid is produced that theslant and butt remain yellow (acid). Salmonellae andshigellae typically yield an alkaline slant and an acidbutt. Although proteus, providencia, and morganellaproduce an alkaline slant and acid butt, they can beidentified by their rapid formation of red color in Chris-tensens urea medium. Organisms producing acid on theslant and acid and gas (bubbles) in the butt are other
enteric bacteria.1. EscherichiaE colitypically produces positive testsfor indole, lysine decarboxylase, and mannitol fermenta-tion and produces gas from glucose. An isolate fromurine can be quickly identified as E coliby its hemolysis
on blood agar, typical colonial morphology with an iri-descent sheen on differential media such as EMB agar,and a positive spot indole test. Over 90% of E coliiso-lates are positive for -glucuronidase using the substrate4-methylumbelliferyl--glucuronide (MUG). Isolatesfrom anatomic sites other than urine, with characteristicproperties (above plus negative oxidase tests) often canbe confirmed as E coliwith a positive MUG test.
2. Klebsiella-enterobacter-serratia groupKlebsiellaspecies exhibit mucoid growth, large polysaccharidecapsules, and lack of motility, and they usually give pos-itive tests for lysine decarboxylase and citrate. Mostenterobacter species give positive tests for motility, cit-rate, and ornithine decarboxylase and produce gas fromglucose. Enterobacter aerogeneshas small capsules. Serra-tia produces DNase, lipase, and gelatinase. Klebsiella,enterobacter, and serratia usually give positive Voges-Proskauer reactions.
3. Proteus-morganella-providencia groupThemembers of this group deaminate phenylalanine, aremotile, grow on potassium cyanide medium (KCN),and ferment xylose. Proteus species move very activelyby means of peritrichous flagella, resulting in swarm-ing on solid media unless the swarming is inhibited bychemicals, eg, phenylethyl alcohol or CLED (cystine-lactose-electrolyte-deficient) medium. Proteus speciesandMorganella morganiiare urease-positive, while prov-idencia species usually are urease-negative. The proteus-providencia group ferment lactose very slowly or not atall. Proteus mirabilisis more susceptible to antimicrobialdrugs, including penicillins, than other members of thegroup.
4. CitrobacterThese bacteria typically are citrate-positive and differ from the salmonellae in that they donot decarboxylate lysine. They ferment lactose veryslowly if at all.
5. ShigellaShigellae are nonmotile and usually do notferment lactose but do ferment other carbohydrates,
250 / CHAPTER 16
Table 162. Rapid,presumptive identification of gram-negative enteric bacteria.
Lactose Fermented Rapidly Lactose Fermented Slowly Lactose Not Fermented
Escherichia coli: metallic sheen on Edwardsiella,serratia,citrobacter, Shigella species: nonmotile; no gas fromdifferential media; motile; flat, arizona, providencia, erwinia dextrosenonviscous colonies Salmonella species: motile; acid and
Enterobacter aerogenes: raised colonies, usually gas from dextroseno metallic sheen;often motile; more Proteus species:swarmingon agar;
viscous growth urea rapidly hydrolyzed (smell ofKlebsiella pneumoniae: very viscous, ammonia)
mucoid growth; nonmotile Pseudomonas species (see Chapter17):soluble pigments,blue-green andfluorescing; sweetish smell
4010_1-16 2/11/04 9:28 AM Page 250
-
8/13/2019 Enteric Gram Negative Rods
4/14
producing acid but not gas. They do not produce H2S.The four shigella species are closely related to E coli.Many share common antigens with one another and
with other enteric bacteria (eg, Hafnia alveiand Ple-siomonas shigelloides).
6. SalmonellaSalmonellae are motile rods that char-acteristically ferment glucose and mannose without pro-ducing gas but do not ferment lactose or sucrose. Mostsalmonellae produce H2S. They are often pathogenic forhumans or animals when ingested. Arizona is includedin the salmonella group.
7. Other EnterobacteriaceaeYersinia species are dis-cussed in Chapter 20. Other genera occasionally foundin human infections include edwardsiella and ewingella,hafnia, cedecea, and kluyvera.
Antigenic Structure
Enterobacteriaceae have a complex antigenic structure.
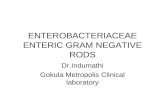
They are classified by more than 150 different heat-stable somatic O (lipopolysaccharide) antigens, morethan 100 heat-labile K (capsular) antigens, and morethan 50 H (flagellar) antigens (Figure 161). In Salmo-nella Typhi, the capsular antigens are called Vi antigens.
O antigens are the most external part of the cell walllipopolysaccharide and consist of repeating units ofpolysaccharide. Some O-specific polysaccharides con-tain unique sugars. O antigens are resistant to heat andalcohol and usually are detected by bacterial agglutina-tion. Antibodies to O antigens are predominantly IgM.
While each genus of Enterobacteriaceae is associatedwith specific O groups, a single organism may carry sev-
eral O antigens. Thus, most shigellae share one or moreO antigens with E coli. E colimay cross-react with someprovidencia, klebsiella, and salmonella species. Occa-sionally, O antigens may be associated with specifichuman diseases, eg, specific O types of E coliare foundin diarrhea and in urinary tract infections.
K antigens are external to O antigens on some butnot all Enterobacteriaceae. Some are polysaccharides,including the K antigens of E coli; others are proteins. Kantigens may interfere with agglutination by O antisera,and they may be associated with virulence (eg, E colistrains producing K1 antigen are prominent in neonatalmeningitis, and K antigens of E colicause attachment ofthe bacteria to epithelial cells prior to gastrointestinal orurinary tract invasion).
Klebsiellae form large capsules consisting of polysac-charides (K antigens) covering the somatic (O or H)antigens and can be identified by capsular swelling tests
with specific antisera. Human infections of the respira-
tory tract are caused particularly by capsular types 1 and2; those of the urinary tract, by types 8, 9, 10, and 24.
H antigens are located on flagella and are denaturedor removed by heat or alcohol. They are preserved bytreating motile bacterial variants with formalin. Such Hantigens agglutinate with anti-H antibodies, mainlyIgG. The determinants in H antigens are a function ofthe amino acid sequence in flagellar protein (flagellin).
Within a single serotype, flagellar antigens may be pres-ent in either or both of two forms, called phase 1 (con-ventionally designated by lower-case letters) and phase 2(conventionally designated by Arabic numerals), asshown in Table 164. The organism tends to changefrom one phase to the other; this is called phase varia-tion. H antigens on the bacterial surface may interfere
with agglutination by anti-O antibody.There are many examples of overlapping antigenicstructures between Enterobacteriaceae and other bacte-ria. Most Enterobacteriaceae share the O14 antigen of Ecoli. The type 2 capsular polysaccharide of klebsiellae isvery similar to the polysaccharide of type 2 pneumo-cocci. Some K antigens cross-react with capsular poly-saccharides of Haemophilus influenzae or Neisseriameningitidis. Thus, E coliO75:K100:H5 can induceantibodies that react with H influenzaetype b.
The antigenic classification of Enterobacteriaceaeoften indicates the presence of each specific antigen.Thus, the antigenic formula of an E coli may beO55:K5:H21; that of Salmonella Schottmlleri isO1,4,5,12:Hb:1,2.
Colicins (Bacteriocins)
Many gram-negative organisms produce bacteriocins.These virus-like bactericidal substances are produced bycertain strains of bacteria active against some other
ENTERIC GRAM-NEGATIVE RODS (ENTEROBACTERIACEAE) / 251
LipopolysaccharideO side chains (O)
Capsule (K)
Flagella (H)
Cell envelope (cytoplasmic membrane,peptidoglycan, outer membrane)
Figure 161. Antigenic structure of Enterobacteri-aceae.
4010_1-16 2/11/04 9:28 AM Page 251
-
8/13/2019 Enteric Gram Negative Rods
5/14
strains of the same or closely related species. Their pro-duction is controlled by plasmids. Colicins are producedby E coli, marcescens by serratia, and pyocins bypseudomonas. Bacteriocin-producing strains are resis-tant to their own bacteriocin; thus, bacteriocins can beused for typing of organisms.
Toxins & Enzymes
Most gram-negative bacteria possess complexlipopolysaccharides in their cell walls. These substances,endotoxins, have a variety of pathophysiologic effectsthat are summarized in Chapter 9. Many gram-negativeenteric bacteria also produce exotoxins of clinicalimportance. Some specific toxins are discussed in subse-quent sections.
DISEASES CAUSEDBY ENTEROBACTERIACEAE OTHERTHAN SALMONELLA & SHIGELLA
Causative Organisms
E coliis a member of the normal intestinal flora (seeChapter 11). Other enteric bacteria (proteus, enterobac-ter, klebsiella, morganella, providencia, citrobacter, andserratia species) are also found as members of the nor-mal intestinal flora but are considerably less commonthan E coli. The enteric bacteria are sometimes found insmall numbers as part of the normal flora of the upperrespiratory and genital tracts. The enteric bacteria gen-erally do not cause disease, and in the intestine they mayeven contribute to normal function and nutrition.
When clinically important infections occur, they areusually caused by E coli, but the other enteric bacteriaare causes of hospital-acquired infections and occasion-ally cause community-acquired infections. The bacteriabecome pathogenic only when they reach tissues outsideof their normal intestinal or other less common normalflora sites. The most frequent sites of clinically impor-
tant infection are the urinary tract, biliary tract, andother sites in the abdominal cavity, but any anatomicsite (eg, bacteremia, prostate gland, lung, bone,meninges) can be the site of disease. Some of the entericbacteria (eg, Serratia marcescens, Enterobacter aerogenes)
are opportunistic pathogens. When normal hostdefenses are inadequateparticularly in infancy or oldage, in the terminal stages of other diseases, afterimmunosuppression, or with indwelling venous or ure-thral catheterslocalized clinically important infectionscan result, and the bacteria may reach the blood streamand cause sepsis.
Pathogenesis & Clinical Findings
The clinical manifestations of infections with E coliandthe other enteric bacteria depend on the site of theinfection and cannot be differentiated by symptoms orsigns from processes caused by other bacteria.
A. E COLI
1. Urinary tract infectionE coliis the most commoncause of urinary tract infection and accounts for approx-
imately 90% of first urinary tract infections in youngwomen (see Chapter 48). The symptoms and signsinclude urinary frequency, dysuria, hematuria, andpyuria. Flank pain is associated with upper tract infec-tion. None of these symptoms or signs is specific for Ecoliinfection. Urinary tract infection can result in bac-teremia with clinical signs of sepsis.
Nephropathogenic E coli typically produce ahemolysin. Most of the infections are caused by E coliofa small number of O antigen types. K antigen appears tobe important in the pathogenesis of upper tract infec-tion. Pyelonephritis is associated with a specific type ofpilus, P pilus, which binds to the P blood group sub-stance.
2. E coli-associated diarrheal diseasesE coli thatcause diarrhea are extremely common worldwide. TheseE coliare classified by the characteristics of their viru-lence properties (see below), and each group causes dis-ease by a different mechanism. The small or large bowelepithelial cell adherence properties are encoded by geneson plasmids. Similarly, the toxins often are plasmid- orphage-mediated. Some clinical aspects of diarrheal dis-eases are discussed in Chapter 48.
Enteropathogenic E coli(EPEC) is an importantcause of diarrhea in infants, especially in developingcountries. EPEC previously was associated with out-breaks of diarrhea in nurseries in developed countries.EPEC adhere to the mucosal cells of the small bowel.Chromosomally mediated factors promote tight adher-ence. There is loss of microvilli (effacement), formationof filamentous actin pedestals or cup-like structures, and
occasionally, entry of the EPEC into the mucosal cells.Characteristic lesions can be seen on electron micro-graphs of small bowel biopsy lesions. The result ofEPEC infection is watery diarrhea, which is usually self-limited but can be chronic. EPEC diarrhea has been
Table 163. Pathogenic species of shigella.
Present Group and OrnithineDesignation Type Mannitol Decarboxylase
S dysenteriae A S flexneri B + S boydii C + S sonnei D + +
252 / CHAPTER 16
4010_1-16 2/11/04 9:28 AM Page 252
-
8/13/2019 Enteric Gram Negative Rods
6/14
associated with multiple specific serotypes of E coli;strains are identified by O antigen and occasionally byH antigen typing. A two-stage infection model usingHEp-2 cells also can be performed. Tests to identifyEPEC are performed in reference laboratories. Theduration of the EPEC diarrhea can be shortened and thechronic diarrhea cured by antibiotic treatment.
Enterotoxigenic E coli(ETEC) is a common causeof travelers diarrhea and a very important cause ofdiarrhea in infants in developing countries. ETEC colo-nization factors specific for humans promote adherenceof ETEC to epithelial cells of the small bowel. Somestrains of ETEC produce a heat-labile exotoxin(LT)(MW 80,000) that is under the genetic control of aplasmid. Its subunit B attaches to the GM1 gangliosideat the brush border of epithelial cells of the small intes-tine and facilitates the entry of subunit A (MW 26,000)into the cell, where the latter activates adenylyl cyclase.This markedly increases the local concentration of cyclic
adenosine monophosphate (cAMP), which results inintense and prolonged hypersecretion of water and chlo-rides and inhibits the reabsorption of sodium. The gutlumen is distended with fluid, and hypermotility anddiarrhea ensue, lasting for several days. LT is antigenicand cross-reacts with the enterotoxin of Vibrio cholerae.LT stimulates the production of neutralizing antibodiesin the serum (and perhaps on the gut surface) of personspreviously infected with enterotoxigenic E coli. Personsresiding in areas where such organisms are highly preva-lent (eg, in some developing countries) are likely to pos-sess antibodies and are less prone to develop diarrhea onreexposure to the LT-producing E coli. Assays for LTinclude the following: (1) fluid accumulation in theintestine of laboratory animals; (2) typical cytologic
changes in cultured Chinese hamster ovary cells or othercell lines; (3) stimulation of steroid production in cul-tured adrenal tumor cells; and (4) binding andimmunologic assays with standardized antisera to LT.These assays are done only in reference laboratories.
Some strains of ETEC produce the heat-stableenterotoxin STa(MW 15004000), which is under thegenetic control of a heterogeneous group of plasmids.STa activates guanylyl cyclase in enteric epithelial cellsand stimulates fluid secretion. Many STa-positivestrains also produce LT. The strains with both toxinsproduce a more severe diarrhea.
The plasmids carrying the genes for enterotoxins (LT,ST) also may carry genes for the colonization factorsthat facilitate the attachment of E colistrains to intestinalepithelium. Recognized colonization factors occur with
particular frequency in some serotypes. Certain serotypesof ETEC occur worldwide; others have a limited recog-nized distribution. It is possible that virtually any E colimay acquire a plasmid encoding for enterotoxins. Thereis no definite association of ETEC with the EPEC strains
causing diarrhea in children. Likewise, there is no associ-ation between enterotoxigenic strains and those able toinvade intestinal epithelial cells.
Care in the selection and consumption of foodspotentially contaminated with ETEC is highly recom-mended to help prevent travelers diarrhea. Antimicro-bial prophylaxis can be effective but may result inincreased antibiotic resistance in the bacteria and proba-bly should not be uniformly recommended. Once diar-rhea develops, antibiotic treatment effectively shortensthe duration of disease.
Enterohemorrhagic E coli(EHEC) produces vero-toxin, named for its cytotoxic effect on Vero cells, a lineof African green monkey kidney cells. There are at leasttwo antigenic forms of the toxin. EHEC has been asso-ciated with hemorrhagic colitis, a severe form of diar-rhea, and with hemolytic uremic syndrome, a diseaseresulting in acute renal failure, microangiopathichemolytic anemia, and thrombocytopenia. Verotoxin
has many properties that are similar to the Shiga toxinproduced by some strains of Shigella dysenteriaetype 1;however, the two toxins are antigenically and geneticallydistinct. Of the E coliserotypes that produce verotoxin,O157:H7 is the most common and is the one that canbe identified in clinical specimens. ETEC O157:H7does not use sorbitol, unlike most other E coli, and isnegative on sorbitol MacConkey agar (sorbitol is usedinstead of lactose); O157:H7 strains also are negative onMUG tests (see above). Specific antisera are used toidentify the O157:H7 strains. Assays for verotoxin aredone in reference laboratories. Many cases of hemor-rhagic colitis and its associated complications can beprevented by thoroughly cooking ground beef.
Enteroinvasive E coli(EIEC) produces a disease very
similar to shigellosis. The disease occurs most com-monly in children in developing countries and in travel-ers to these countries. Like shigella, EIEC strains arenonlactose or late lactose fermenters and are nonmotile.EIEC produce disease by invading intestinal mucosalepithelial cells.
Enteroaggregative E coli(EAEC) causes acute andchronic diarrhea (> 14 days in duration) in persons indeveloping countries. These organisms also are the causeof food-borne illnesses in industrialized countries. Theyare characterized by their characteristic pattern of adher-ence to human cells. EAEC produce ST-like toxin (seeabove) and a hemolysin.
3. SepsisWhen normal host defenses are inadequate,E colimay reach the bloodstream and cause sepsis. New-
borns may be highly susceptible to E colisepsis becausethey lack IgM antibodies. Sepsis may occur secondary tourinary tract infection.
4. MeningitisE coliand group B streptococci are theleading causes of meningitis in infants. Approximately
ENTERIC GRAM-NEGATIVE RODS (ENTEROBACTERIACEAE) / 253
4010_1-16 2/11/04 9:28 AM Page 253
-
8/13/2019 Enteric Gram Negative Rods
7/14
75% of E colifrom meningitis cases have the K1 anti-gen. This antigen cross-reacts with the group B capsularpolysaccharide of N meningitidis. The mechanism of vir-ulence associated with the K1 antigen is not under-stood.
B. KLEBSIELLA-ENTEROBACTER-SERRATIA; PROTEUS-MORGANELLA-PROVIDENCIA; AND CITROBACTER
The pathogenesis of disease caused by these groups ofenteric gram-negative rods is similar to that of the non-specific factors in disease caused by E coli.
1. KlebsiellaK pneumoniae is present in the respira-tory tract and feces of about 5% of normal individuals.It causes a small proportion (about 1%) of bacterialpneumonias. K pneumoniaecan produce extensive hem-orrhagic necrotizing consolidation of the lung. It occa-sionally produces urinary tract infection and bacteremia
with focal lesions in debilitated patients. Other entericsalso may produce pneumonia. K pneumoniaeand Kleb-
siella oxytocacause hospital-acquired infections. Twoother klebsiellae are associated with inflammatory con-ditions of the upper respiratory tract: Klebsiella ozaenaehas been isolated from the nasal mucosa in ozena, afetid, progressive atrophy of mucous membranes; andKlebsiella rhinoscleromatis from rhinoscleroma, adestructive granuloma of the nose and pharynx.
2. Enterobacter aerogenesThis organism has smallcapsules, may be found free-living as well as in theintestinal tract, and causes urinary tract infections andsepsis.
3. SerratiaS marcescensis a common opportunisticpathogen in hospitalized patients. Serratia (usually non-pigmented) causes pneumonia, bacteremia, and endo-carditisespecially in narcotics addicts and hospitalizedpatients. Only about 10% of isolates form the red pig-ment (prodigiosin) that has long characterized Serratiamarcescens. S marcescensis often multiply resistant toaminoglycosides and penicillins; infections can betreated with third-generation cephalosporins.
4. ProteusProteus species produce infections inhumans only when the bacteria leave the intestinal tract.They are found in urinary tract infections and producebacteremia, pneumonia, and focal lesions in debilitatedpatients or those receiving intravenous infusions. Pmirabiliscauses urinary tract infections and occasionallyother infections. Proteus vulgarisand Morganella mor-
ganiiare important nosocomial pathogens.Proteus species produce urease, resulting in rapid
hydrolysis of urea with liberation of ammonia. Thus, in
urinary tract infections with proteus, the urine becomesalkaline, promoting stone formation and making acidi-fication virtually impossible. The rapid motility of pro-teus may contribute to its invasion of the urinary tract.
Strains of proteus vary greatly in antibiotic sensitiv-
ity. P mirabilisis often inhibited by penicillins; the mostactive antibiotics for other members of the group areaminoglycosides and cephalosporins.
5. ProvidenciaProvidencia species (Providenciarettgeri, Providencia alcalifaciens, and Providencia stuar-tii) are members of the normal intestinal flora. All causeurinary tract infections and occasionally other infectionsand are often resistant to antimicrobial therapy.
6. CitrobacterCitrobacter can cause urinary tractinfections and sepsis.
Diagnostic Laboratory Tests
A. SPECIMENS
Urine, blood, pus, spinal fluid, sputum, or other mate-rial, as indicated by the localization of the diseaseprocess.
B. SMEARS
The Enterobacteriaceae resemble each other morpho-logically. The presence of large capsules is suggestive ofklebsiella.
C. CULTURE
Specimens are plated on both blood agar and differen-tial media. With differential media, rapid preliminaryidentification of gram-negative enteric bacteria is oftenpossible (see Chapter 47).
Immunity
Specific antibodies develop in systemic infections, but itis uncertain whether significant immunity to the organ-isms follows.
Treatment
No single specific therapy is available. The sulfon-amides, ampicillin, cephalosporins, fluoroquinolones,and aminoglycosides have marked antibacterial effectsagainst the enterics, but variation in susceptibility isgreat, and laboratory tests for antibiotic sensitivity areessential. Multiple drug resistance is common and isunder the control of transmissible plasmids.
Certain conditions predisposing to infection by theseorganisms require surgical correction, eg, relief of uri-nary tract obstruction, closure of a perforation in anabdominal organ, or resection of a bronchiectatic por-tion of lung.
Treatment of gram-negative bacteremia and impend-
ing septic shock requires rapid institution of antimicro-bial therapy, restoration of fluid and electrolyte balance,and treatment of disseminated intravascular coagula-tion. Administration of antiglycolipid antibody is exper-imental but can prevent shock and death.
254 / CHAPTER 16
4010_1-16 2/11/04 9:28 AM Page 254
-
8/13/2019 Enteric Gram Negative Rods
8/14
Various means have been proposed for the preven-tion of travelers diarrhea, including daily ingestion ofbismuth subsalicylate suspension (bismuth subsalicylatecan inactivate E colienterotoxin in vitro) and regulardoses of tetracyclines or other antimicrobial drugs forlimited periods. Because none of these methods areentirely successful or lacking in adverse effects, it is
widely recommended that caution be observed in regardto food and drink in areas where environmental sanita-tion is poor and that early and brief treatment (eg, withciprofloxacin or trimethoprim-sulfamethoxazole) besubstituted for prophylaxis.
Epidemiology, Prevention,& Control
The enteric bacteria establish themselves in the normalintestinal tract within a few days after birth and from thenon constitute a main portion of the normal aerobic (facul-tative anaerobic) microbial flora. E coliis the prototype.
Enterics found in water or milk are accepted as proof offecal contamination from sewage or other sources.Control measures are not feasible as far as the normal
endogenous flora is concerned. Enteropathogenic E coliserotypes should be controlled like salmonellae (seebelow). Some of the enterics constitute a major problemin hospital infection. It is particularly important to rec-ognize that many enteric bacteria are opportunists
which cause illness when they are introduced into debil-itated patients. Within hospitals or other institutions,these bacteria commonly are transmitted by personnel,instruments, or parenteral medications. Their controldepends on hand washing, rigorous asepsis, sterilizationof equipment, disinfection, restraint in intravenoustherapy, and strict precautions in keeping the urinarytract sterile (ie, closed drainage).
THE SHIGELLAE
The natural habitat of shigellae is limited to the intesti-nal tracts of humans and other primates, where theyproduce bacillary dysentery.
Morphology & Identification
A.TYPICAL ORGANISMS
Shigellae are slender gram-negative rods; coccobacillaryforms occur in young cultures.
B. CULTURE
Shigellae are facultative anaerobes but grow best aerobi-cally. Convex, circular, transparent colonies with intactedges reach a diameter of about 2 mm in 24 hours.
C. GROWTH CHARACTERISTICS
All shige llae ferment glucose. With the exception ofShigella sonnei, they do not ferment lactose. The inabil-
ity to ferment lactose distinguishes shigellae on differen-tial media. Shigellae form acid from carbohydrates butrarely produce gas. They may also be divided into thosethat ferment mannitol and those that do not (Table163).
Antigenic Structure
Shigellae have a complex antigenic pattern. There isgreat overlapping in the serologic behavior of differentspecies, and most of them share O antigens with otherenteric bacilli.
The somatic O antigens of shigellae are lipopolysac-charides. Their serologic specificity depends on thepolysaccharide. There are more than 40 serotypes. Theclassification of shigellae relies on biochemical and anti-genic characteristics. The pathogenic species are shownin Table 163.
Pathogenesis & Pathology
Shigella infections are almost always limited to the gas-trointestinal tract; bloodstream invasion is quite rare.Shigellae are highly communicable; the infective dose ison the order of 103 organisms (whereas it usually is105108 for salmonellae and vibrios). The essentialpathologic process is invasion of the mucosal epithelialcells (eg, M cells) by induced phagocytosis, escape fromthe phagocytic vacuole, multiplication and spread
within the epithelial cell cytoplasm, and passage to adja-cent cells. Microabscesses in the wall of the large intes-tine and terminal ileum lead to necrosis of the mucousmembrane, superficial ulceration, bleeding, and forma-tion of a pseudomembrane on the ulcerated area. Thisconsists of fibrin, leukocytes, cell debris, a necroticmucous membrane, and bacteria. As the process sub-sides, granulation tissue fills the ulcers and scar tissueforms.
Toxins
A. ENDOTOXIN
Upon autolysis, all shigellae release their toxiclipopolysaccharide. This endotoxin probably con-tributes to the irritation of the bowel wall.
B. SHIGELLA DYSENTERIAEEXOTOXIN
S dysenteriaetype 1 (Shiga bacillus) produces a heat-labileexotoxin that affects both the gut and the central nervoussystem. The exotoxin is a protein that is antigenic (stim-
ulating production of antitoxin) and lethal for experi-mental animals. Acting as an enterotoxin, it producesdiarrhea as does the E coliverotoxin, perhaps by the samemechanism. In humans, the exotoxin also inhibits sugarand amino acid absorption in the small intestine. Acting
ENTERIC GRAM-NEGATIVE RODS (ENTEROBACTERIACEAE) / 255
4010_1-16 2/11/04 9:28 AM Page 255
-
8/13/2019 Enteric Gram Negative Rods
9/14
as a neurotoxin, this material may contribute to theextreme severity and fatal nature of S dysenteriaeinfec-tions and to the central nervous system reactionsobserved in them (ie, meningismus, coma). Patients withShigella flexnerior Shigella sonneiinfections develop anti-toxin that neutralizes S dysenteriaeexotoxin in vitro. Thetoxic activity is distinct from the invasive property ofshigellae in dysentery. The two may act in sequence, thetoxin producing an early nonbloody, voluminous diar-rhea and the invasion of the large intestine resulting inlater dysentery with blood and pus in stools.
Clinical Findings
After a short incubation period (12 days), there is asudden onset of abdominal pain, fever, and watery diar-rhea. The diarrhea has been attributed to an exotoxinacting in the small intestine (see above). A day or solater, as the infection involves the ileum and colon, the
number of stools increases; they are less liquid but oftencontain mucus and blood. Each bowel movement isaccompanied by straining and tenesmus (rectal spasms),
with resulting lower abdominal pain. In more than halfof adult cases, fever and diarrhea subside spontaneouslyin 25 days. However, in children and the elderly, loss of
water and electrolytes may lead to dehydration, acidosis,and even death. The illness due to S dysenteriaemay beparticularly severe.
On recovery, most persons shed dysentery bacilli foronly a short period, but a few remain chronic intestinalcarriers and may have recurrent bouts of the disease.Upon recovery from the infection, most persons developcirculating antibodies to shigellae, but these do not pro-tect against reinfection.
Diagnostic Laboratory Tests
A. SPECIMENS
Fresh stool, mucus flecks, and rectal swabs for culture.Large numbers of fecal leukocytes and some red bloodcells often are seen microscopically. Serum specimens, ifdesired, must be taken 10 days apart to demonstrate arise in titer of agglutinating antibodies.
B. CULTURE
The materials are streaked on differential media (eg,MacConkeys or EMB agar) and on selective media(Hektoen enteric agar or salmonella-shigella agar),
which suppress other Enterobacter iaceae and gram-positive organisms. Colorless (lactose-negative) colonies
are inoculated into triple sugar iron agar. Organismsthat fail to produce H2S, that produce acid but not gasin the butt and an alkaline slant in triple sugar iron agarmedium, and that are nonmotile should be subjected toslide agglutination by specific shigella antisera.
C. SEROLOGY
Normal persons often have agglutinins against severalshigella species. However, serial determinations of anti-
body titers may show a rise in specific antibody. Serol-ogy is not used to diagnose shigella infections.
Immunity
Infection is followed by a type-specific antibody response.Injection of killed shigellae stimulates production of anti-bodies in serum but fails to protect humans against infec-tion. IgA antibodies in the gut may be important in lim-iting reinfection; these may be stimulated by liveattenuated strains given orally as experimental vaccines.Serum antibodies to somatic shigella antigens are IgM.
Treatment
Ciprofloxacin, ampicillin, doxycycline, and trimetho-
prim-sulfamethoxazole are most commonly inhibitoryfor shigella isolates and can suppress acute clinicalattacks of dysentery and shorten the duration of symp-toms. They may fail to eradicate the organisms from theintestinal tract. Multiple drug resistance can be trans-mitted by plasmids, and resistant infections are wide-spread. Many cases are self-limited. Opioids should beavoided in shigella dysentery.
Epidemiology, Prevention,& Control
Shigellae are transmitted by food, fingers, feces, andflies from person to person. Most cases of shigella infec-tion occur in children under 10 years of age. S dysente-riaecan spread widely. Mass chemoprophylaxis for lim-ited periods of time (eg, in military personnel) has been
tried, but resistant strains of shigellae tend to emergerapidly. Since humans are the main recognized host ofpathogenic shigellae, control efforts must be directed ateliminating the organisms from this reservoir by (1) san-itary control of water, food, and milk; sewage disposal;and fly control; (2) isolation of patients and disinfectionof excreta; (3) detection of subclinical cases and carriers,particularly food handlers; and (4) antibiotic treatmentof infected individuals.
THE SALMONELLA-ARIZONA GROUP
Salmonellae are often pathogenic for humans or animalswhen acquired by the oral route. They are transmittedfrom animals and animal products to humans, wherethey cause enteritis, systemic infection, and enteric fever.
Morphology & Identification
Salmonellae vary in length. Most isolates are motile withperitrichous flagella. Salmonellae grow readily on simple
256 / CHAPTER 16
4010_1-16 2/11/04 9:28 AM Page 256
-
8/13/2019 Enteric Gram Negative Rods
10/14
media, but they almost never ferment lactose or sucrose.They form acid and sometimes gas from glucose andmannose. They usually produce H2S. They survivefreezing in water for long periods. Salmonellae are resis-tant to certain chemicals (eg, brilliant green, sodiumtetrathionate, sodium deoxycholate) that inhibit otherenteric bacteria; such compounds are therefore usefulfor inclusion in media to isolate salmonellae from feces.
Classification
The classification of salmonellae is complex because theorganisms are a continuum rather than a definedspecies. The members of the genus salmonella were orig-inally classified on the basis of epidemiology, host range,biochemical reactions, and structures of the O, H, andVi (when present) antigens. The names (eg, Salmonellatyphi, Salmonella typhimurium) were written as if they
were genus and species; this form of the nomenclature
remains in widespread but incorrect use. DNA-DNAhybridization studies have demonstrated that there areseven evolutionary groups. Nearly all of the salmonellaserotypes that infect humans are in DNA hybridizationgroup I; there are rare human infections with groupsIIIa and IIIb. The species name Salmonella entericahasbeen widely accepted, and the organisms in DNAhybridization group I are S entericasubspecies enterica.The organisms in the other groups have other sub-species names. It seems probable that the widelyaccepted nomenclature for classification will be as fol-lows: S enterica subspecies enterica serotypeTyphimurium, which can be shortened to SalmonellaTyphimurium with the genus name in italics and theserotype name in roman type. National and interna-
tional reference laboratories may use the antigenic for-mulas following the subspecies name because theyimpart more precise information about the isolates (seeTable 164). An example would be S entericasubspeciessalamaeserotype 50:z:e,n,x, which can also be written Sentericaserotype II 50:z:e,n,x, with the roman numeralII representing the subspecies salamae of DNAhybridization group II.
There are more than 2500 serotypes of salmonellae,including more than 1400 in DNA hybridization groupI that can infect humans. Four serotypes of salmonellaethat cause enteric fever can be identified in the clinicallaboratory by biochemical and serologic tests. Theseserotypes should be routinely identified because of theirclinical significance. They are as follows: SalmonellaParatyphi A (serogroup A), Salmonella Paratyphi B
(serogroup B), SalmonellaCholeraesuis (serogroup C1),and SalmonellaTyphi (serogroup D). The more than1400 other salmonellae that are isolated in clinical labo-ratories are serogrouped by their O antigens as A, B, C1,C2, D, and E; some are nontypeable with this set of
antisera. The isolates are then sent to reference laborato-ries for definitive serologic identification. This allowspublic health officials to monitor and assess the epi-demiology of salmonella infections on a statewide andnationwide basis.
Variation
Organisms may lose H antigens and become nonmotile.Loss of O antigen is associated with a change fromsmooth to rough colony form. Vi antigen may be lostpartially or completely. Antigens may be acquired (orlost) in the process of transduction.
Pathogenesis & Clinical Findings
SalmonellaTyphi, SalmonellaCholeraesuis, and perhapsSalmonellaParatyphi A and SalmonellaParatyphi B are
primarily infective for humans, and infection with theseorganisms implies acquisition from a human source.The vast majority of salmonellae, however, are chieflypathogenic in animals that constitute the reservoir forhuman infection: poultry, pigs, rodents, cattle, pets(from turtles to parrots), and many others.
The organisms almost always enter via the oral route,usually with contaminated food or drink. The meaninfective dose to produce clinical or subclinical infectionin humans is 105108 salmonellae (but perhaps as few as103 SalmonellaTyphi organisms). Among the host fac-tors that contribute to resistance to salmonella infectionare gastric acidity, normal intestinal microbial flora, andlocal intestinal immunity (see below).
Salmonellae produce three main types of disease inhumans, but mixed forms are frequent (Table 165).
A. THE ENTERIC FEVERS (TYPHOID FEVER)
This syndrome is produced by only a few of the salmo-nellae, of which SalmonellaTyphi (typhoid fever) is themost important. The ingested salmonellae reach the
Table 164. Representative antigenic formulas
of salmonellae.
O Group Serotype Antigenic Formula
1
D S Typhi 9,12 (Vi):d:A S Paratyphi A 1,2,12:aC1 S Choleraesuis 6,7:c:1,5B S Typhimurium 1,4,5,12:i:1,2D S Enteritidis 1,9,12:g,m:
1O antigens: boldface numerals.
(Vi):Vi antigen if present.
Phase 1 H antigen: lower-case letter.
Phase 2 H antigen: numeral.
ENTERIC GRAM-NEGATIVE RODS (ENTEROBACTERIACEAE) / 257
4010_1-16 2/11/04 9:28 AM Page 257
-
8/13/2019 Enteric Gram Negative Rods
11/14
small intestine, from which they enter the lymphaticsand then the bloodstream. They are carried by the bloodto many organs, including the intestine. The organismsmultiply in intestinal lymphoid tissue and are excretedin stools.
After an incubation period of 1014 days, fever,malaise, headache, constipation, bradycardia, and myal-gia occur. The fever rises to a high plateau, and thespleen and liver become enlarged. Rose spots, usually onthe skin of the abdomen or chest, are seen briefly in rarecases. The white blood cell count is normal or low. Inthe preantibiotic era, the chief complications of entericfever were intestinal hemorrhage and perforation, andthe mortality rate was 1015%. Treatment with antibi-
otics has reduced the mortality rate to less than 1%.The principal lesions are hyperplasia and necrosis oflymphoid tissue (eg, Peyers patches), hepatitis, focalnecrosis of the liver, and inflammation of the gallblad-der, periosteum, lungs, and other organs.
B. BACTEREMIA WITH FOCAL LESIONS
This is associated commonly with S choleraesuisbut maybe caused by any salmonella serotype. Following oralinfection, there is early invasion of the bloodstream(with possible focal lesions in lungs, bones, meninges,etc), but intestinal manifestations are often absent.Blood cultures are positive.
C. ENTEROCOLITIS
This is the most common manifestation of salmonella
infection. In the USA, SalmonellaTyphimurium andSalmonellaEnteritidis are prominent, but enterocolitiscan be caused by any of the more than 1400 group Iserotypes of salmonellae. Eight to 48 hours after inges-tion of salmonellae, there is nausea, headache, vomiting,
and profuse diarrhea, with few leukocytes in the stools.Low-grade fever is common, but the episode usuallyresolves in 23 days.
Inflammatory lesions of the small and large intestineare present. Bacteremia is rare (24%) except inimmunodeficient persons. Blood cultures are usuallynegative, but stool cultures are positive for salmonellaeand may remain positive for several weeks after clinicalrecovery.
Diagnostic Laboratory Tests
A. SPECIMENS
Blood for culture must be taken repeatedly. In entericfevers and septicemias, blood cultures are often positivein the first week of the disease. Bone marrow culturesmay be useful. Urine cultures may be positive after thesecond week.
Stool specimens also must be taken repeatedly. Inenteric fevers, the stools yield positive results from thesecond or third week on; in enterocolitis, during the first
week.A positive culture of duodenal drainage establishes
the presence of salmonellae in the biliary tract in carri-ers.
B. BACTERIOLOGIC METHODS FOR ISOLATIONOF SALMONELLAE
1. Differential medium culturesEMB, Mac-
Conkeys, or deoxycholate medium permits rapid detec-tion of lactose nonfermenters (not only salmonellae andshigellae but also proteus, serratia, pseudomonas, etc).Gram-positive organisms are somewhat inhibited. Bis-muth sulfite medium permits rapid detection of salmo-
Table 165. Clinical diseases induced by salmonellae.
Enteric Fevers Septicemias Enterocolitis
Incubation period 720 days Variable 848 hours
Onset Insidious Abrupt Abrupt
Fever Gradual, then high plateau, Rapid rise, then spiking Usually lowwith typhoidal state septic temperature
Duration of disease Several weeks Variable 25 days
Gastrointestinal symptoms Often early constipation; Often none Nausea, vomiting, diarrhea atlater, bloody diarrhea onset
Blood cultures Positive in first to second Positive during high fever Negativeweeks of disease
Stool cultures Positive from 2nd week on; Infrequently positive Positive soon after onsetnegative earlier in disease
258 / CHAPTER 16
4010_1-16 2/11/04 9:28 AM Page 258
-
8/13/2019 Enteric Gram Negative Rods
12/14
-
8/13/2019 Enteric Gram Negative Rods
13/14
REVIEW QUESTIONS
typhoid become permanent carriers, harboring theorganisms in the gallbladder, biliary tract, or, rarely, theintestine or urinary tract.
B. SOURCES OF INFECTIONThe sources of infection are food and drink that havebeen contaminated with salmonellae. The followingsources are important:
1. WaterContamination with feces often results inexplosive epidemics.
2. Milk and other dairy products (ice cream, cheese,custard)Contamination with feces and inadequatepasteurization or improper handling. Some outbreaksare traceable to the source of supply.
3. ShellfishFrom contaminated water.
4. Dried or frozen eggsFrom infected fowl or conta-minated during processing.
5. Meats and meat productsFrom infected animals
(poultry) or contamination with feces by rodents orhumans.
6. Recreational drugsMarijuana and other drugs.
7. Animal dyesDyes (eg, carmine) used in drugs,foods, and cosmetics.
8. Household petsTurtles, dogs, cats, etc.
Prevention & Control
Sanitary measures must be taken to prevent contamina-tion of food and water by rodents or other animals thatexcrete salmonellae. Infected poultry, meats, and eggsmust be thoroughly cooked. Carriers must not beallowed to work as food handlers and should observestrict hygienic precautions.
Two injections of acetone-killed bacterial suspensionsof SalmonellaTyphi, followed by a booster injectionsome months later, give partial resistance to small infec-tious inocula of typhoid bacilli but not to large ones.Oral administration of a live avirulent mutant strain ofSalmonellaTyphi has given significant protection in areasof high endemicity. Vaccines against other salmonellaegive less protection and are not recommended.
1. A 20-year-old college student goes to the studenthealth center because of dysuria, frequency, andurgency on urination for 24 hours. She has
recently become sexually active. On urinalysis,many polymorphonuclear cells are seen.The mostlikely organism responsible for these symptomsand signs is
(A) Staphylococcus aureus(B) Streptococcus agalactiae(C) Gardnerella vaginalis
(D) Lactobacillus species(E) Escherichia coli
2. A 27-year-old woman is admitted to the hospitalbecause of fever, with increasing anorexia,headache, weakness,and altered mental status of2 daysduration.She works for an airline as a cabinattendant, flying between the Indian subconti-nent and other places in Southeast Asia and theWest Coast of the USA.Ten days prior to admissionshe had a diarrheal illness that lasted for about 36hours.She has been constipated for the last 3 days.Her temperature is 39 C,heart rate 68/min,bloodpressure 120/80 mm Hg, and respirations 18/min.She knows who she is and where she is but doesnot know the date. She is picking at the bed-clothes. Rose spots are seen on the trunk. Theremainder of the physical examination is normal.Blood cultures are done and an intravenous line isplaced.The most likely cause of her illness is(A) Enterotoxigenic Escherichia coli (ETEC)(B) Shigella sonnei(C) Salmonella enterica subspecies enterica
serotype Typhimurium (Salmonella Typh-imurium)
(D) Salmonella enterica subspecies entericaserotype Typhi (Salmonella Typhi)
(E) EnteroinvasiveEscherichia coli (EIEC)
3. Blood cultures from the patient in Question 2grow a non-lactose-fermenting gram-negativebacillus. Which of the following is likely to be aconstituent of this organism?
(A) O antigen 157,H antigen 7 (O157:H7)(B) Vi antigen (capsule;virulence antigen)(C) O antigen 139 (O139)(D) Urease(E) K1 (capsular type 1)
4. Four members of a migrant farmworker familymother, father, and two young childrencometo the emergency room because of diarrhea andfever of 612 hours duration. Their stools havebeen frequent and flecked with blood. Severalother people in the workers camp have been illwith a similar diarrheal disease.This included theperson who prepared the evening meal the pre-vious day. The parents had normal physicalexaminations. The children showed signs ofexcessive fluid and electrolyte loss. The likelycause of this outbreak is(A) Salmonella enterica subspecies enterica
serotype Typhimurium (Salmonella Typh-imurium)
260 / CHAPTER 16
4010_1-16 2/11/04 9:28 AM Page 260
-
8/13/2019 Enteric Gram Negative Rods
14/14
(B) Salmonella enterica subspecies entericaserotype Typhi (SalmonellaTyphi)
(C) Shigella flexneri
(D) Rotavirus(E) Enterotoxigenic Escherichia coli (ETEC)
5. In Medieval Europe,bread was often stored in thedamp basements of churches before use in theceremonies. Sometimes a red substanceappeared on the bread. The bacteria that werered and on the bread were(A) Serratia marcescens(B) Pseudomonas aeruginosa(C) Escherichia coli(D) Klebsiella pneumoniae(E) Proteus mirabilis
6. A 37-year-old woman with a history of urinarytract infections comes to the emergency roomwith burning on urination along with frequency
and urgency.She says her urine smells like ammo-nia.The cause of her urinary tract infection is likelyto be(A) Enterobacter aerogenes(B) Proteus mirabilis(C) Citrobacter freundii(D) Escherichia coli(E) Serratia marcescens
7. A 60-year-old man was admitted to the hospital2 weeks previously because of head trauma andother injuries that resulted from an automobileaccident.A urinary tract catheter was inserted atadmission and remains in place.The man devel-ops a urinary tract infection with a gram-nega-tive bacillus.The probable cause of this patientsinfection is
(A) Pseudomonas aeruginosa(B) Providencia rettgeri(C) Escherichia coli(D) Morganella morganii(E) Indeterminable without culture and identifi-
cation testing
8. An 18-year-old student has abdominal crampsand diarrhea.A plate of MacConkeys agar is inoc-ulated and grows gram-negative rods. Triplesugar iron (TSI) agar is used to screen the isolatesfor salmonellae and shigellae. A result suggestingone of these two pathogens would be(A) Production of urease(B) Motility in the medium(C) Inability to ferment lactose and sucrose(D)
Fermentation of glucose(E) Production of gas in the medium
9. An uncommon serotype of Salmonella entericasubspecies enterica was found by laboratories inthe health departments of adjacent states. The
isolates were all from a small geographic area oneither side of the border between the states, sug-gesting a common source for the isolates. (All the
isolates were from otherwise healthy youngadults who smoked marijuana; the same salmo-nella was isolated from a specimen of the mari-
juana.) By what method did the laborator iesdetermine that these isolates were the same?(A) Capsular (K antigen) typing(B) O antigen and H antigen typing(C) DNA sequencing(D) Sugar fermentation pattern determination(E) Decarboxylase reaction pattern determination
10. A 43-year-old diabetic man has a 4 cm nonhealingfoot ulcer.Culture of the ulcer yields Staphylococ-cus aureus, Bacteroides fragilis, and a gram-nega-tive bacillus that swarms across the blood agarplate covering the entire surface of the agar after36 hours.The gram-negative bacillus is a memberof the genus(A) Escherichia(B) Enterobacter(C) Serratia(D) Salmonella(E) Proteus
Answers1. E 6. B2. D 7. E3. B 8. C4. C 9. B5. A 10. E
REFERENCES
Abbott S: Klebsiella, Enterobacter, Citrobacter, Serratia, Plesiomonas,and Other Enterobacteriaceae. In:Manual of Clinical Microbi-ology, 8th ed. Murray PR et al (editors). ASM Press, 2003.
Bopp CA et al: Escherichia, Shigella, and Salmonella. In:Manual ofClinical Microbiology, 8th ed. Murray PR et al (editors). ASMPress, 2003.
Dupont HL: Shigellaspecies (bacillary dysentery). In:Mandell, Dou-glas, and Bennetts Principles and Practice of Infectious Diseases,5th ed. Mandell GL, Bennett JE, Dolin R (editors). ChurchillLivingstone, 2000.
Eisenstein BI, Azaleznik DF: Enterobacteriaceae. In: Mandell, Dou-glas, and Bennetts Principles and Practice of Infectious Diseases,5th ed. Mandell GL, Bennett JE, Dolin R (editors). ChurchillLivingstone, 2000.
Farmer JJ III: Enterobacteriaceae: Introduction and Identification. In:Manual of Clinical Microbiology, 8th ed. Murray PR et al (edi-tors). ASM Press, 2003.
Miller SI, Pegues DA: Salmonellaspecies, including Salmonella typhi.In:Mandell, Douglas, and Bennetts Principles and Practice ofInfectious Diseases, 5th ed. Mandell GL, Bennett JE, Dolin R(editors). Churchill Livingstone, 2000.
ENTERIC GRAM-NEGATIVE RODS (ENTEROBACTERIACEAE) / 261
4010_1-16 2/11/04 9:28 AM Page 261